Back to Journals » Patient Preference and Adherence » Volume 19
Associations of Self-Management Care and Shared Decision-Making with Glycemic Control and Psychosocial Outcomes in Type 2 Diabetes Mellitus
Authors Jarrar M ![]() , Al-Bsheish M
, Al-Bsheish M ![]() , Alshahri BK, Bamashmoos MA, Alnaimi MI, Alsayil SA, Basager SA, Al Rawashdeh MA, Al-Rawashdeh AB
, Alshahri BK, Bamashmoos MA, Alnaimi MI, Alsayil SA, Basager SA, Al Rawashdeh MA, Al-Rawashdeh AB
Received 1 May 2025
Accepted for publication 23 July 2025
Published 2 August 2025 Volume 2025:19 Pages 2295—2307
DOI https://doi.org/10.2147/PPA.S534066
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Mu’taman Jarrar,1 Mohammad Al-Bsheish,2,3 Bashair Khalid Alshahri,4 Manar Abdulrahman Bamashmoos,5 Mona I Alnaimi,6 Shaykhah A Alsayil,7 Shymaa A Basager,8 Mohammad Ahmad Al Rawashdeh,9 Ahmad Bahjat Al-Rawashdeh1
1Nursing Department, Princess Aisha Bint Al Hussein College for Nursing and Health Sciences, Al-Hussein Bin Talal University, Ma’an, 71111, Jordan; 2Health Management Department, Batterjee Medical College, Jeddah, 21442, Saudi Arabia; 3Al-Nadeem Governmental Hospital, Ministry of Health, Amman, 11118, Jordan; 4Ophthalmology Department, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 5Pediatrics Department, King Fahad Military Medical Complex, Dammam, Eastern Province, Saudi Arabia; 6Otolaryngology Department, King Fahad University Hospital, Al-Khobar, Eastern Province, Saudi Arabia; 7Family Medicine Department, Dr.Sulaiman Al-Habib Hospital, Al-Khobar, Eastern Province, Saudi Arabia; 8Pediatrics Department, King Fahad University Hospital, Al-Khobar, Eastern Province, Saudi Arabia; 9Researcher/Biology, Pre-Med Track, University of Massachusetts Amherst, Amherst, MA, USA
Correspondence: Mu’taman Jarrar, Nursing Department, Princess Aisha Bint Al Hussein College for Nursing and Health Sciences, Al-Hussein Bin Talal University, Ma’an, 71111, Jordan, Email [email protected]; [email protected] Mohammad Al-Bsheish, Health Management Department, Batterjee Medical College, Jeddah, 21442, Saudi Arabia, Email [email protected]
Purpose: This study explored the associations of Self-Management Care (SMC) and Shared Decision-Making (SDM) with clinical outcomes, specifically glycated hemoglobin (HbA1c) levels, and non-clinical outcomes (psychosocial Outcomes) in patients with type 2 Diabetes Mellitus (T2DM).
Methods: A cross-sectional design was employed, involving 200 patients with T2DM, recruited through convenience sampling. Data were collected from the two healthcare facilities in Dammam, Saudi Arabia, between March and June 2020. Statistical analyses, including independent sample t-tests, one-way ANOVA, and multiple linear regression, were conducted using Statistical Package for the Social Sciences (SPSS) version 26.0.
Results: The findings showed that Increased SMC levels were associated with improved clinical outcomes, particularly lower HbA1c levels (p < 0.01). Additionally, SMC was positively associated with psychosocial outcomes (ie, quality of life and mental health; p < 0.05). In contrast, SDM was significantly associated with psychosocial outcomes (p < 0.05), its relationship with HbA1c was non-significant (p= 0.300), indicating only a minor explanatory effect. Additionally, demographic and clinical factors such as sex and lipid levels were found to influence glycemic outcomes, with males and patients with better lipid profiles showing lower HbA1c levels.
Conclusion: This study reinforces the pivotal role of SMC in achieving optimal glycemic control and improving the overall well-being of T2DM patients. While shared decision-making (SDM) enhances patient-reported outcomes, its impact on clinical outcomes such as HbA1c was not statistically significant. These findings support patient-centered approaches and highlight the need for further longitudinal research to confirm causal relationships. The results highlight the value of integrating comprehensive self-management support and patient-centered decision-making in diabetes care to optimize both clinical and psychosocial outcomes for patients.
Keywords: diabetes mellitus, DM, type 2 diabetes mellitus, T2DM, self-management care and shared decision-making, psychosocial outcomes, glycated hemoglobin, HbA1c
Introduction
Diabetes Mellitus (DM) is a long-term chronic illness characterized by impaired insulin secretion, insulin resistance, and persistent hyperglycemia. Type 2 Diabetes Mellitus (T2DM) is an important public health concern, representing 85–95% of adults with diabetes.1,2 Diabetes control and outcomes are an international issue as the prevalence and economic burden of Diabetes Mellitus are increasing. It affecting over 537 million adults worldwide, and from 1980 to 2014 the prevalence was quadrupled to 400 million cases due to worldwide aging and population growth, and estimated to reach over 700 million cases by 2045.1,3,4
Global health agenda and health system efforts are focused on diabetes management and prevention.1 Despite evidence of improved diabetic clinical outcomes with medical treatment,5–7 glycemic control is alarming because the prevalence of poor glycemic control is substantial.8–10 Inadequate glycemic management is linked to the increasing utilization of healthcare facilities and, subsequently, the cost of medical care.11 By 2045, diabetes is predicted to cost USD 958 billion compared to USD 850 billion in 2017. Most of these costs are attributed to undiagnosed and untreated cases.12 Despite improvements in pharmaceutical therapies, many individuals with T2DM struggle to preserve blood glucose levels, raising the possibility of severe complications such as heart disease, neuropathy, and nephropathy.13 Thus, patients with diabetes require appropriate care to successfully manage diabetes, avoid long-term complications, and improve their quality of life.
To successfully manage diabetes, a strategy that addresses both clinical biomarkers and patient-related outcomes (psychosocial outcomes). Given the complex interplay between physiological regulation and psychosocial factors, recent guidelines emphasize the integration of both clinical and non-clinical measures to provide a holistic assessment of diabetes management.14 Traditionally, DM care has focused on achieving optimal glycemic control, primarily determined using glycated hemoglobin (HbA1c) levels, a well-established indicator of sustained glycemic control.13,14 Lowering HbA1c levels is essential for lowering the risk of microvascular and macrovascular issues, such as nephropathy, neuropathy, cardiovascular disease, and stroke.15 However, although HbA1c remains a primary standard clinical marker, exclusive reliance on biochemical outcomes fails to capture the broader impact of diabetes on patient well-being and daily functioning.
In contrast, psychosocial outcomes include quality of life, treatment satisfaction and psychological health—are essential components of diabetes care that offer insightful information on patients’ experiences, challenges, and perceived effectiveness of management strategies.16,17 Evidence suggests that diabetes-related distress and depression significantly influence self-management care, such as adherence to treatment.18–20 For instance, high levels of diabetes distress are linked to a higher risk of complications and worse glycemic control, even after adjusting for HbA1c levels.18,19 Given these challenges, effective long-term management strategies that emphasize patient engagement in care are critical to improving patient outcomes.
Self-management care (SMC) and shared decision-making (SDM) have emerged as integral components of contemporary diabetes management. SMC involves patients actively participating in daily self-care activities, including physical activity, medication adherence, dietary regulation, and glucose monitoring, all of which contribute to better quality of life and glycemic control.17 SDM, in contrast, focuses on collaborative decision making between patients and medical professionals, ensuring that choices about treatments are in line with patient values, preferences, and individual circumstances.21 While both SMC and SDM have been independently associated with improved patient outcomes, their combined influence on both clinical (HbA1c levels) and non-clinical (psychosocial outcomes) indicators remains underexplored. Given these challenges, patient-centered approaches that enhance engagement in diabetes self-management are critical for long-term disease management. However, we acknowledge that examining such associations using a cross-sectional design does not permit causal inferences.
The self-management of diabetes is a complex, lifelong journey, and it may not always be easy to adopt and maintain self-management strategies.22 This requires the patient to actively participate and be responsible for achieving diabetes control.23 Motivation is a key aspect of self-management and plays a crucial role in adherence to lifestyle modifications, medication use, and glucose monitoring, particularly internal and external motivations.24 Intrinsic motivation, driven by personal goals, autonomy, and perceived competence, is more strongly associated with sustained behavioral changes in diabetes management.25 However, extrinsic motivation includes external encouragement from healthcare providers through patient-centered communication, adequate information provision, and fostering a supportive patient-provider relationship.26 Therefore, engaging in behaviors with long-term consequences, such as a balanced diet and regular exercise, with patient support and engagement, can have promising benefits.
The theoretical foundations of motivation in self-management and effective shared decisions in this study can be understood through Self-Determination Theory (SDT) and Patient Activation Theory (PAT). SDT posits that patients are prone to participate in and sustain self-care behaviors when they experience autonomy, relatedness, and competence.27 In relation to T2DM, patients who feel empowered in decision-making and perceive their actions as personally meaningful demonstrate greater adherence to self-management behaviors.28 Similarly, PAT suggests that higher patient activation is related to the ability, confidence, and understanding of managing one’s health, leading to better clinical and psychosocial outcomes.16 These theories underscore the importance of fostering intrinsic motivation and providing external support to encourage long-term diabetes management behavior.
Over the past few decades, there has been a need to evaluate non-clinical outcomes such as quality of life and psychosocial outcomes in addition to measuring clinical outcomes.29 Despite growing evidence supporting the importance of SMC and SDM, limited research has explored their combined influence on clinical outcomes, such as HbA1c levels, and non-clinical outcomes, including psychosocial outcomes. This knowledge gap hampers the development of effective patient-centered care strategies that address the full spectrum of challenges faced by individuals living with T2DM. Our study sought to fill this gap by exploring the relationship between SMC and SDM and both clinical and non-clinical outcomes in T2DM patients. By integrating insights from SDT and PAT, this study provides a deeper understanding of the motivational mechanisms underlying self-management and decision making in diabetic care. The findings of our study can inform strategies to enhance patient engagement, optimize diabetes management, improve patient outcomes, and provide comprehensive treatment that addresses the psychological and physical needs of individuals with T2DM.
Methodology
Design, Setting and Sampling
This study was a cross-sectional survey that examined the associations between SMC and SDM, and both HbA1c levels and psychosocial outcomes among T2DM. The survey was carried out over a three-month period from March to June 2020, in two healthcare facilities, tertiary care hospital at King Fahd Hospital of the University and diabetes clinics at Family and Community Medicine Center of Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia. The sample recruited in this study using a convenience sampling (A sample obtained for participants who meet study criteria), to recruit adult T2DM patients, given its feasibility in clinical settings.30 The inclusion criteria were as follows.
- Confirmed diagnosis of T2DM for at least one year based on the American Diabetes Association (ADA) criteria.14
- Age ≥ 18 years to ensure full autonomy in healthcare decisions, and
- Capacity to provide consent for participation in the study and to complete study questionnaires.
Patients were excluded if they had cognitive impairment or psychiatric disorders affecting self-care, pregnancy, gestational diabetes mellitus (GDM) due to distinct management pathways, acute illness, or hospitalization during data collection.
A robust justification for the sample size enhances the methodological rigor of this study. The minimum required sample size of 200 was determined using Epi Info 7 StatCalc, which is frequently employed in epidemiological research and sample size calculations based on the Centers for Disease Control and Prevention.31 Sample size was determined using Epi Info 7 StatCalc, based on a 0.3 effect size, 80% power, and 95% confidence level. A minimum of 200 participants was calculated, including a 10% buffer for potential non-response.32 The calculation accounted for a 10% non-response rate, which is critical in survey-based research to maintain adequate power and validity of the findings.33 The Epi Info 7 StatCalc tool applies rigorous statistical principles, ensuring that the sample size is sufficient for this type of study.31
Operationalization and Instruments
This study employed validated and standardized instruments to assess key study variables, including SMC, SDM, clinical outcomes (HbA1c levels), and non-clinical outcomes (psychosocial outcomes) among individuals with T2DM. Operationalizing these variables is essential to ensuring measurement accuracy, research validity, and replicability.34 SMC indicates the active involvement of T2DM patients in daily behaviors and practices to achieve optimal glycemic control. It involves multiple components including dietary control, glucose management, healthcare use, and physical activity.35 SMC was measured using the “Diabetes Self-Management Questionnaire (DSMQ)”, 16 items divided into four subscales: glucose management, dietary control, physical activity, and healthcare use. Each item was rated on a 4-point Likert scale, with higher scores indicating better self-management.35 Higher scores on the 4-point Likert scale used by the DSMQ indicated better self-management. The tool demonstrated strong construct reliability (Cronbach’s alpha = 0.89).
SDM refers to the collaborative process between the patient and the healthcare provider in making informed healthcare decisions that align with the patient’s preferences, values, and clinical evidence.36 SDM supports the selection of appropriate care and enhances treatment adherence.21 The Patient Version of the “Shared Decision-Making Questionnaire (SDMQ-9)” was used to assess the extent of SDM during clinical interactions.36 The SDMQ-9 is a 9-item instrument, and a 6-point scale was used to evaluate patient engagement and collaborative decision-making. The tool has a high degree of internal consistency (Cronbach’s alpha = 0.91). Negatively worded items were reverse-coded; therefore, a high score indicated a positive and preferable response.
Clinical factors such as Comorbidity, BMI, TC, HDL, LDL were extracted from the electronic medical records of patients with diabetes. Concerning the outcome in this study, the clinical outcome refers to the HbA1c level, which is a biomarker that represents the average blood sugar level throughout the previous two–three months, acting as a quantitative measure of glycemic control (HbA1c level below 7% is considered optimal for T2DM management, according to the ADA guidelines).14 Glycemic control was objectively measured using HbA1c levels extracted from patient medical records. The HbA1c test is the most reliable method for monitoring blood glucose levels over time and offers a robust evaluation of the impact of SMC and SDM on metabolic control.
Psychosocial outcomes represent self-reported measures of a patient’s condition such as quality of life, mental health, and perceived well-being.37 The new 5-level EQ-5D (EQ-5D-5L) tool was employed to assess health-related quality of life.38 The EQ-5D-5L is a standardized and widely validated tool that measures five dimensions: mobility, usual activities, self-care, pain/discomfort, and depression/anxiety.38 It demonstrates strong internal consistency (Cronbach’s alpha = 0.88) and is frequently used in clinical evaluations. Responses are used to calculate a composite health utility score, with higher scores indicating better perceived health status.
Ethical Considerations
The Institutional Review Board of Imam Abdulrahman Bin Faisal University approved this study (IRB- UGS-2019-294), ensuring complied with the Declaration of Helsinki (2013). All participants provided written informed consent to participate voluntarily in the survey before data collection. Confidentiality was maintained through de-identified coding of data, and all information was stored in secure, password-protected databases. Participants were guaranteed to leave at any time without facing any repercussions. Ethical approval for the use of the study tools was obtained from the authors.
Data Collection Procedure
Data collection was conducted systematically to ensure the reliability and validity of the findings. Participants were recruited from diabetes clinics in the Imam Abdulrahman Bin Faisal University healthcare facilities to ensure a representative sample of individuals diagnosed with T2DM. Prior to data collection, interested parties were made aware of the study’s objectives, procedures, and right to voluntary participation.
Data were collected using self-administered structured questionnaires (both in English and Arabic to accommodate language preferences and enhance comprehension) for Self-Management Care (SMC), Shared Decision-Making (SDM), and psychosocial outcomes, whereas, clinical information such as HbA1c and lipid levels were extracted from the electronic medical records of participants. Trained research assistants were available to provide clarification and assistance in completing the questionnaires, thus minimizing potential response bias. Completed questionnaires were collected and stored to ensure confidentiality. Data were gathered over a three-month period to ensure an adequate sample size, allowing for robust statistical analysis.
Data Analysis
Version 26.0 of the Statistical Package for the Social Sciences (SPSS) (IBM Corp., Armonk, NY) was used to analyze the data. Prior to the analysis, the data were checked for completeness, missing values, and outliers to maintain data integrity. The patients clinical and demographic data were compiled using standard deviations (SD) and means in descriptive statistics. Independent sample one-way analysis ANOVA and t-tests were used to compare HbA1c levels and psychosocial outcomes across the different demographic and clinical subgroups.39
To examine the associations between SMC, SDM, and both clinical (HbA1c) and non-clinical (psychosocial outcomes) outcomes, regression analysis was conducted to identify the independent determinants of HbA1c levels and psychosocial outcomes while adjusting for potential confounders such as age, sex, duration of diabetes, BMI, and comorbidities.40 All statistical tests were two-tailed, and statistical significance was set at p < 0.05. The findings are presented with 95% confidence intervals (CI), where applicable, ensuring robustness in inference. Model assumptions, including linearity, multicollinearity, and homoscedasticity, were verified before regression analyses.39 These analytical methods provide a deep understanding of the relationships between SMC, SDM, HbA1c and psychosocial outcomes, to provide meaningful insights for improving diabetes care and management.
Results
Patients’ Characteristics
A total of 200 patients with T2DM participated in the study, with the number of females and males distributed equally (50% each). The majority of participants were aged 50 years and above, with 34.5% in the 50–59 age group and 39.0% in the 60 years or older group. Most of the participants were unemployed (58.5%), 39.5% were employed, and 2.0% were students. The majority (76.0%) of patients had been diagnosed with T2DM for five years or more. Regarding nationality, most participants were Saudi (85.5%) and 83.0% were married. The socioeconomic status varied, with 37.5% earning more than 10,000 SR per month, 32.0% earning–5000–10,000 SR, and 30.5% earning less than 5000 SR. Educational attainment was diverse: 43.5% had a high school education, 24.0% held a bachelor’s degree, 14.0% had no formal education, 11.0% had a diploma, and 7.5% had postgraduate qualifications.
Analysis of HbA1c levels and psychosocial outcomes indicated notable variations based on demographic variables for certain variables, as shown in Table 1. Gender had a significant impact on HbA1c, with males having a lower mean HbA1c level (8.13±2.22) than females (8.81±2.03, p=0.039). However, there was no apparent sex disparity in psychosocial outcomes (p=0.636).
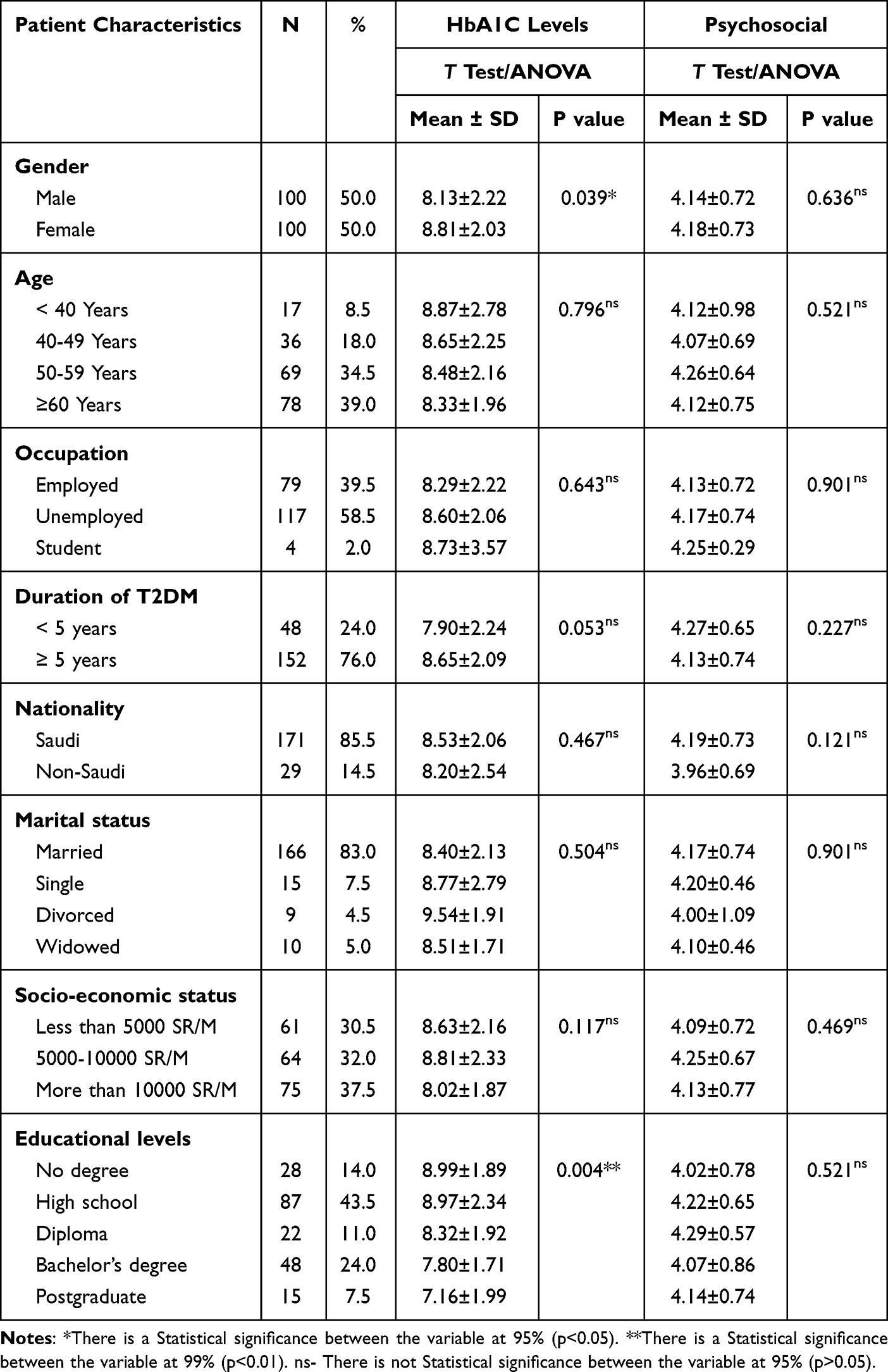 |
Table 1 Patient Demographic Characteristics and Their Association with Outcomes |
Age, occupation, T2DM, nationality, marital status, and socioeconomic status were not significantly associated with HbA1c level or psychosocial outcomes. However, patients who had diabetes for less than five years had a slightly lower mean HbA1c level (7.90±2.24) than those who had the disease for a longer period of time (8.65±2.09, p=0.053), although this result was not statistically significant.
Analysis of HbA1c levels and psychosocial outcomes based on patient clinical characteristics (Table 2) revealed, total cholesterol (TC) levels and low-density lipoprotein (LDL) levels were significantly associated with HbA1c levels. Patients with controlled TC (<200 mg/dL) had significantly lower HbA1c levels (8.24±1.92) than those with uncontrolled TC (≥200 mg/dL, 9.19±2.57, p=0.013). Similarly, patients with controlled LDL (<100 mg/dL) had a lower HbA1c level (8.05±1.71) than those with uncontrolled LDL (≥100 mg/dL, 8.80±2.38, p=0.021). However, no significant relationships were found between HbA1c levels and comorbidities, BMI, or high-density lipoprotein (HDL), or triglyceride (TG) levels. Furthermore, none of the clinical characteristics were significantly associated with psychosocial outcomes.
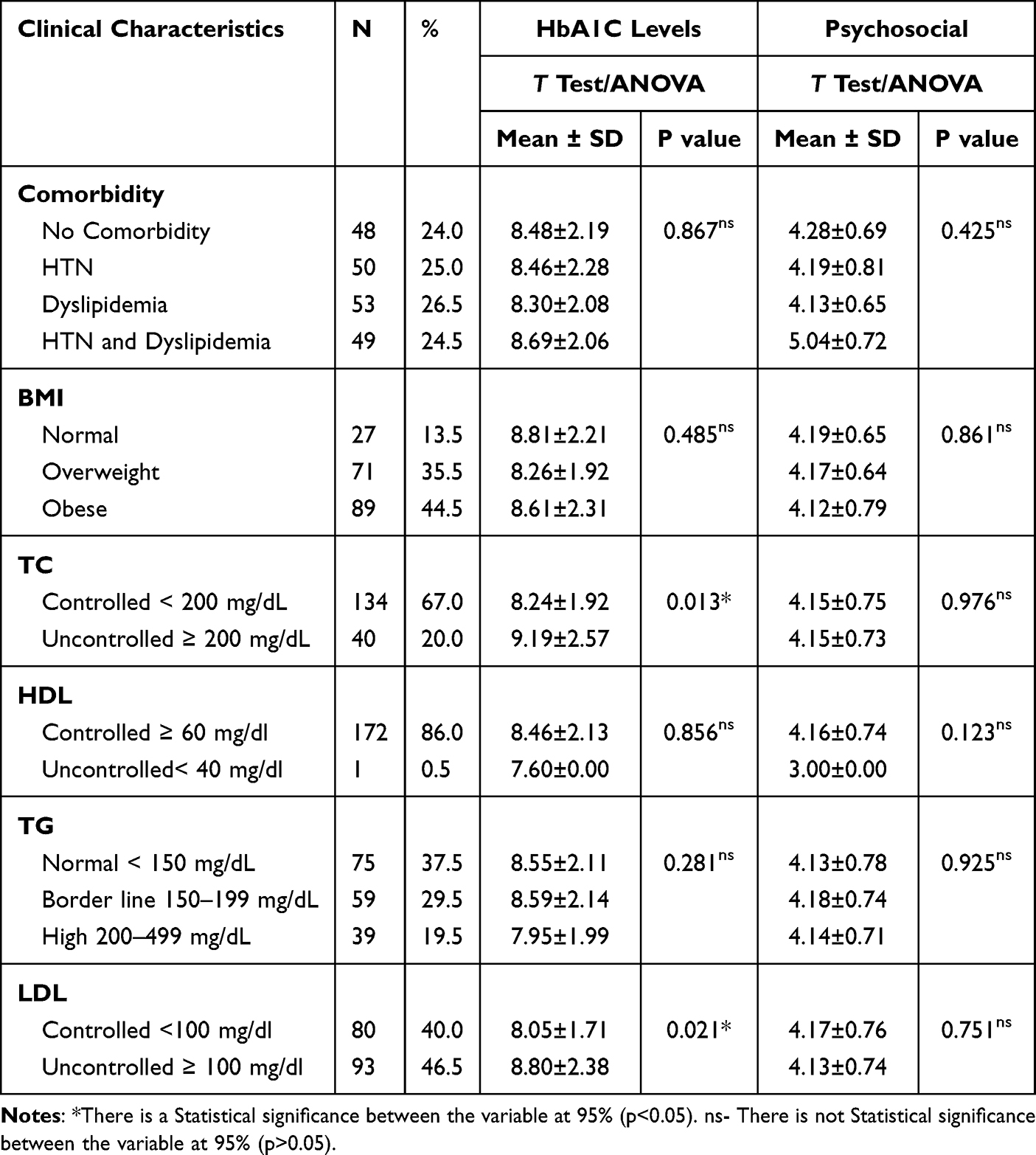 |
Table 2 Patient Clinical Characteristics and Associations with Outcomes |
Multivariate Assumptions, Reliability and Validity
Before conducting the multivariate analyses, key statistical assumptions were made to ensure the appropriateness of the regression model. Multivariate assumptions were made and the data were found to be normal and linear with no violation of multicollinearity or heteroscedasticity assumptions. The reliability of the study tools was evaluated using Cronbach’s alpha, and 0.70 was deemed acceptable for internal consistency.41 The study tools demonstrated strong reliability (Cronbach’s alpha = 0.89 DSMQ, 0.91 for SDMQ, and 0.89 for EQ-5D-5L). Factor analysis was performed, and the KMO and factor-loading results were reported. Items with factor loadings greater than 0.5 were retained in the study. KMO composite mean values were 0.85, 0.89 and 0.87 (p = 0.000) for SMC, SDM and EQ-5D-5L; respectively, which indicate the adequacy of sampling.40
The Influence of SDM and SMC on Patients’ Outcomes
As presented in Table 3, the linear regression analysis examined the relationships between SDM, SMC, HbA1c, and psychosocial outcomes. SMC demonstrated a significant inverse relationship with HbA1c levels (β = −0.156, p = 0.041), indicating that better SMC was associated with better glycemic control. However, SDM was not significantly associated with HbA1c level (β = 0.079, p = 0.300).
 |
Table 3 Influence of SMC and SDM |
For psychosocial outcomes, both SDM (β = 0.234, p = 0.001) and SMC (β = 0.153, p = 0.027) were significantly associated with better psychosocial outcomes, suggesting that greater participation of patients in the decision-making process and improved self-management practices contribute to an enhanced quality of life and mental health. These results underscore the critical role of SMC in improving glycemic control and psychosocial outcomes.
The overall regression model explained 7.6% of the variation in psychosocial (nonclinical) outcomes (p < 0.001) and 3.1% of the variation in clinical outcomes (p = 0.068), highlighting the relatively modest influence of SDM and SMC on psychosocial outcomes and the minimal impact on clinical outcomes, particularly HbA1c. Figure 1 provides a summary of the study results.
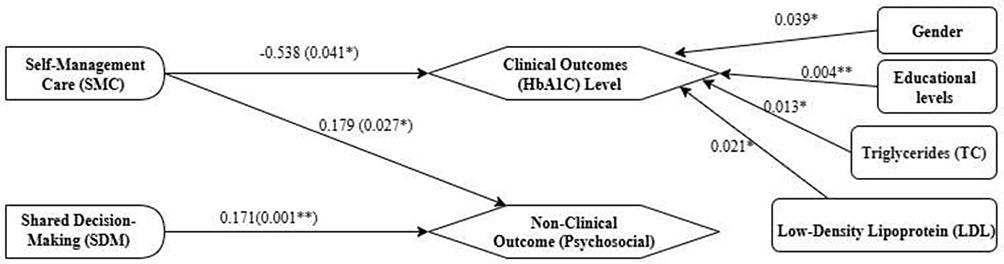 |
Figure 1 Summary of significant results. * There is a Statistical significance between the variable at 95% (p<0.05). ** There is a Statistical significance between the variable at 99% (p<0.01). |
Discussion
This study explored the relationship between SMC and SDM and both HbA1c levels and psychosocial outcomes in patients with T2DM. These findings suggest that SMC may play a modest role in improving glycemic control and psychosocial outcomes, whereas SDM appears to be more closely associated with psychosocial outcomes only. These results are consistent with previous research and contribute to growing evidence supporting patient-centered approaches, reinforcing the importance of patient engagement in diabetes management. These results align with the existing literature and can be explained through the lens of the two aforementioned theories (ie, SDT and PAT).27,42
Self-Management and Reported Outcomes
The significant association between SMC and HbA1c levels is consistent with previous studies that have emphasized the effectiveness of diabetes self-management interventions. Studies have shown that patients who engage in structured self-care activities, including medication adherence, dietary regulation, and physical activity, achieve better glycemic outcomes.43,44 A controlled, randomized study assessing the POWER2DM integrated e-health support system demonstrated that such interventions effectively improve quality of life and glycemic control in individuals with diabetes. The study highlighted that providing patients with tools to actively manage their condition helps improve clinical outcomes.45 Our findings align with research demonstrating that diabetes self-management education leads to sustained advancements in metabolic markers including HbA1c.46 These findings also align with SDT, which posits that when individuals experience autonomy, competence, and relatedness in managing their health, they are more likely to participate in sustained health-promoting behaviors.27 A scoping review assessing the application of SDT in diabetes management found that interventions grounded in SDT effectively enhance self-management practices, treatment adherence, and quality of life of patients with diabetes. The review concluded that fostering autonomy, competence, and relatedness in patients encourages proactive health behaviors, leading to improved clinical outcomes.47 Patients with high self-management skills are likely to feel more competent at controlling their diabetes, which in turn results in better metabolic outcomes.
Furthermore, the strong relationship between SMC and psychosocial outcomes such as quality of life and mental health, supports previous findings that self-efficacy in diabetes management reduces psychological distress.48 Studies suggest that patients with higher self-management skills report greater confidence in handling their condition, leading to lower levels of diabetes-related distress and depression.17 This can be explained through PAT, which suggests that individuals with higher activation levels have the knowledge, skills, and confidence to manage their health and improve their quality of life.42,49 Therefore, SMC is associated with improvements in the physical and psychological health of diabetic patients.
Decision-Making and Reported Outcomes
The study findings revealed that SDM is positively associated with psychosocial outcomes but does not significantly affect glycemic control. This is consistent with earlier studies that indicate that while SDM improves patient satisfaction and engagement, it may not directly translate into measurable clinical improvements such as HbA1c reduction.50 Similar results have been observed in studies where SDM enhanced treatment adherence and psychological well-being but did not significantly alter metabolic markers.51 One possible explanation is that SDM fosters a collaborative relationship between patients and healthcare professionals, improving care satisfaction and perceived control over their health, which in turn improves mental health and quality of life. However, achieving substantial HbA1c reduction often requires consistent and long-term self-care behaviors. Thus, SDM alone, especially in a cross-sectional context, may not have a direct or measurable influence on clinical biomarkers.
According to SDT, SDM fosters autonomy by allowing patients to play an active role in choosing their course of therapy, which enhances their quality of life and psychological well-being. However, because SDM does not directly alter behaviors such as medication adherence or lifestyle modifications, its influence on HbA1c levels may be limited. Additionally, from PAT perspective, SDM contributes to increased activation by empowering patients with information and fostering collaborative decision making.42 Empowerment improves patient confidence and reduces the stress related to disease management, thereby enhancing psychosocial outcomes.
Demographic and Clinical Predictors of Outcomes
This study also explored the impact of demographic and clinical characteristics on HbA1c levels and psychosocial outcomes. Sex differences in glycemic control, with males showing significantly lower HbA1c levels than females, are consistent with prior research indicating that women with T2DM often experience greater glycemic variability and poorer metabolic control.52 Potential factors contributing to this disparity include hormonal influences, differences in insulin sensitivity, and psychosocial stressors that affect diabetes self-management. Additionally, the non-significant association between age and HbA1c levels aligns with findings suggesting that while diabetes duration influences glycemic control, chronological age alone may not be a strong determinant.53 However, the observed trend of worse glycemic control in patients with longer disease duration supports the evidence that diabetes tends to progress over time and often requires more intensive management strategies (Holman et al, 2014).
Another key finding was the significant association between lipid levels and HbA1c levels, particularly among patients with uncontrolled total cholesterol (TC) and LDL cholesterol levels. This aligns with studies showing that dyslipidemia is a common comorbidity in T2DM and contributes to poor glycemic outcomes.54 The interplay between lipid metabolism and glucose regulation suggests that comprehensive management that addresses both glycemic and lipid control is necessary for optimal diabetes outcome.
Study Implications
Our findings have several important clinical implications. First, diabetes management programs should prioritize self-management education, as it plays a vital role in improving both clinical and psychosocial outcomes. Second, while SDM may not directly lower HbA1c levels, its positive impact on psychosocial outcomes underscores the need for patient-centered approaches in diabetes care. Healthcare providers should continue to engage patients in decision making to enhance treatment adherence and overall well-being. Finally, the relationship between dyslipidemia and poor glycemic control suggests that integrated treatment strategies targeting both metabolic parameters are essential.
Study Limitations
Despite the insightful information provided by this study, several limitations should be noted. First, we were unable to demonstrate causal linkages between SMC, SDM, HbA1c levels, and psychosocial outcomes due to the cross-sectional design. A longitudinal study is needed to determine whether these associations persist over time and to assess potential bidirectional effects.
Second, self-reported measures were used to assess SMC, SDM, and psychosocial outcomes. While these instruments are validated, recall and social desirability biases can affect self-reported data, possibly leading to over- or underestimation of engagement in self-care behaviors and decision-making processes. Objective assessments, such as digital tracking of medication adherence and lifestyle behaviors, could complement self-reported data in future studies.
Third, the study sample was drawn from a specific clinical setting, which restricts the generalization of the findings to broader populations, including individuals with different healthcare access, cultural backgrounds, and socioeconomic status. Future studies should examine these associations in diverse and representative cohorts to ensure their external validity.
Lastly, while we adjusted for demographic and clinical factors, unmeasured confounders, such as health literacy, provider communication styles, and psychological resilience, may have influenced the observed relationships. Incorporating qualitative research and mixed-methods approaches could offer a deeper understanding of the underlying mechanisms linking SMC and SDM to patient outcomes.
Future Directions
Future studies should examine the long-term impact of integrated SMC and SDM interventions on both clinical and psychosocial outcomes in T2DM patients. Randomized controlled trials (RCTs) assessing the effectiveness of structured educational programs, digital health tools, and personalized coaching models could provide stronger evidence for best practices in diabetes care. Additionally, investigating the role of emerging technologies such as mobile health (mHealth) applications and artificial intelligence-driven decision support systems could enhance patient engagement in self-care and decision-making. These tools have the potential to offer real-time feedback, facilitate personalized goal setting, and improve patient-provider communication. Furthermore, studies examining how demographic factors such as gender, socioeconomic status, and cultural beliefs interact with SMC and SDM could inform tailored interventions that address the unique needs of diverse patient populations. Special attention should also be paid to understanding the obstacles and enablers of SDM in individuals with low health literacy and limited access to healthcare. Finally, future research should assess how integrating multidisciplinary care teams including diabetes educators, psychologists, and nutritionists into routine diabetes management can influence patient outcomes. A holistic team-based approach may offer a more comprehensive approach to enhance T2DM patients’ metabolic control and quality of life.
By filling these gaps, subsequent research can help refine diabetes care models that not only optimize clinical outcomes but also enhance patient empowerment and well-being in the long term.
Conclusion
This study offers more evidence of the role of SMC in improving glycemic control and psychosocial outcomes in T2DM patients. While SDM plays an important role in enhancing psychosocial outcomes, its effect on clinical outcomes was not significant in our study. The results reinforcing the significance of patients’ involvement in diabetes treatment. Aligning diabetes management strategies with theoretical frameworks such as SDT and PAT can offer effective strategies to improve both clinical and psychosocial outcomes in individuals with T2DM. Future research should explore longitudinal effects and intervention strategies that integrate self-management support and SDM to optimize diabetes outcomes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhou B, Lu Y, Hajifathalian K, et al. Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet. 2016;387(10027):1513–1530. doi:10.1016/S0140-6736(16)00618-8
2. Goyal R, Jialal I. Diabetes Mellitus Type 2. Treasure Island (FL): StatPearls Publishing; 2019.
3. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the international diabetes federation diabetes atlas, 9th edition. Diabet Res Clin Pract. 2019;157(2019):107843. doi:10.1016/j.diabres.2019.107843
4. International Diabetes Federation (IDF). IDF diabetes atlas. 10th ed. 2021. Available from: https://diabetesatlas.org.
5. Rodbard HW, Rosenstock J, Canani LH, et al. Oral semaglutide versus empagliflozin in patients with type 2 diabetes uncontrolled on metformin: the PIONEER 2 trial. Diabetes Care. 2019;42(12):2272–2281. doi:10.2337/dc19-0883
6. Matthews DR, Paldánius PM, Proot P, Chiang YT, Stumvoll M, Del Prato S. Glycaemic durability of an early combination therapy with vildagliptin and metformin versus sequential metformin monotherapy in newly diagnosed type 2 diabetes (VERIFY): a 5-year, multicentre, randomised, double-blind trial. Lancet. 2019;394(10208):1519–1529. doi:10.1016/S0140-6736(19)32131-2
7. Axelsson AS, Tubbs E, Mecham B, et al. Sulforaphane reduces hepatic glucose production and improves glucose control in patients with type 2 diabetes. Sci Transl Med. 2017;9(394):1–13. doi:10.1126/scitranslmed.aah4477
8. Lipska KJ, Yao X, Herrin J, et al. Trends in drug utilization, glycemic control, and rates of severe hypoglycemia, 2006-2013. Diabetes Care. 2017;40(4):468–475. doi:10.2337/dc16-0985
9. Critchley JA, Carey IM, Harris T, DeWilde S, Hosking FJ, Cook DG. Glycemic control and risk of infections among people with type 1 or type 2 diabetes in a large primary care cohort study. Diabetes Care. 2018;41(10):2127–2135. doi:10.2337/dc18-0287
10. Basto-Abreu A, Barrientos-Gutiérrez T, Rojas-Martínez R, et al. Prevalencia de diabetes y descontrol glucemico en Mexico: resultados de la Ensanut 2016. Salud Publica Mex. 2020;62(1):50–59. doi:10.21149/10752
11. Seuring T, Archangelidi O, Suhrcke M. The economic costs of type 2 diabetes: a global systematic review. Pharmacoeconomics. 2015;33(8):811–831. doi:10.1007/s40273-015-0268-9
12. Cho NH, Shaw JE, Karuranga S, et al. IDF diabetes atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabet Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
13. Zheng Y, Ley SH, Hu FB. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Publ Gr. 2017;14(2):88–98. doi:10.1038/nrendo.2017.151
14. Care D. Standards of care in diabetes-2023 abridged for primary care providers American Diabetes Association. Am Diabetes Assoc. 2023;41(1):1–28.
15. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med. 2014;359(15):1577–1589. doi:10.1056/NEJMoa0806470
16. Hibbard JH, Greene J. What the evidence shows about patient activation: better health outcomes and care experiences; fewer data on costs. Health Aff. 2013;32(2):207–214. doi:10.1377/hlthaff.2012.1061
17. Powers MA, Bardsley J, Cypress M, et al. Diabetes self-management education and support in type 2 diabetes. Diabetes Educ. 2017;43(1):40–53. doi:10.1177/0145721716689694
18. Patra S, Patro BK, Padhy SK, Mantri J. Prevalence of diabetes distress and its relationship with self-management in patients with type 2 diabetes mellitus Suravi. Ind Psychiatry J. 2021;30(2):234–239. doi:10.4103/ipj.ipj
19. Park HS, Cho Y, Seo DH, et al. Impact of diabetes distress on glycemic control and diabetic complications in type 2 diabetes mellitus. Sci Rep. 2024;14(1):1–8. doi:10.1038/s41598-024-55901-0
20. Fisher L, Glasgow RE, Strycker LA. The relationship between diabetes distress and clinical depression with glycemic control among patients with type 2 diabetes. Diabetes Care. 2010;33(5):1034–1036. doi:10.2337/dc09-2175
21. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
22. Wang MJ, Lin HM, Hung LC, Lo YT. Non-health outcomes affecting self-care behaviors and medical decision-making preference in patients with type 2 diabetes: a cross-sectional study. BMC Med Inform Decis Mak. 2020;20(1):1–8. doi:10.1186/s12911-020-1095-2
23. Tang TS, Funnell MM, Oh M. Lasting effects of a 2-year diabetes self-management support intervention: outcomes at 1-year follow-up. Prev Chronic Dis. 2012;9(6):2012. doi:10.5888/pcd9.110313
24. Steffen PLS, Mendonça CS, Meyer E, Faustino-Silva DD. Motivational interviewing in the management of type 2 diabetes mellitus and arterial hypertension in primary health care: an RCT. Am J Prev Med. 2021;60(5):e203–e212. doi:10.1016/j.amepre.2020.12.015
25. Chen M, Yun Q, Lin H, et al. Factors related to diabetes self-management among patients with type 2 diabetes: a Chinese cross-sectional survey based on self-determination theory and social support theory. Patient Prefer Adherence. 2022;16:925–936. doi:10.2147/PPA.S335363
26. Ahola AJ, Groop PH. Barriers to self-management of diabetes. Diabet Med. 2013;30(4):413–420. doi:10.1111/dme.12105
27. Deci EL, Ryan RM. The “what” and “why” of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. 2000;11(4):227–268. doi:10.1207/S15327965PLI1104_01
28. Ng JYY, Ntoumanis N, Thøgersen-Ntoumani C, et al. Self-determination theory applied to health contexts: a meta-analysis. Perspect Psychol Sci. 2012;7(4):325–340. doi:10.1177/1745691612447309
29. McAllister M, Dunn G, Payne K, Davies L, Todd C. Patient empowerment: the need to consider it as a measurable patient-reported outcome for chronic conditions. BMC Health Serv Res. 2012;12(1). doi:10.1186/1472-6963-12-157
30. Melnyk BM, Fineout-Overholt E. Evidence-based practice in nursing and healthcare. Qual Manag Health Care. 2004;13(4):291. doi:10.1097/00019514-200410000-00011
31. Centers for Disease Control. Epi InfoTM 7. Centers for Disease Control and Prevention. 2023. Available from: https://www.cdc.gov/epiinfo.
32. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
33. Bujang MA, Sa’at N, Bakar TA, Joo LC. Sample size guidelines for logistic regression from observational studies with large population. Malaysian J Med Sci. 2018;25(4):122–130. doi:10.21315/mjms2018.25.4.12
34. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
35. Schmitt A, Gahr A, Hermanns N, Kulzer B, Huber J, Hakk T. The diabetes self-management questionnaire (DSMQ). J Heal Qual Life Outcomes. 2013;11(1):1.
36. Kriston L, Scholl I, Hölzel L, Simon D, Loh A, Härter M. The 9-item shared decision making questionnaire (SDM-Q-9). Development and psychometric properties in a primary care sample. Patient Educ Couns. 2010;80(1):94–99. doi:10.1016/j.pec.2009.09.034
37. Cella D, Hahn E, Jensen S, et al. Patient-Reported Outcomes in Performance Measurement. 2015. doi:10.3768/rtipress.2015.bk.0014.1509
38. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727–1736. doi:10.1007/s11136-011-9903-x
39. Field A. Discovering Statistics Using IBM SPSS Statistics. Sage publications limited; 2024. doi:10.5860/choice.50-2114
40. Tabachnick BG, Fidell LS. Using Multivariate Statistics.
41. Stevens JP. Applied Multivariate Statistics for the Social Sciences.
42. Greene J, Hibbard JH. Why does patient activation matter? An examination of the relationships between patient activation and health-related outcomes. J Gen Intern Med. 2012;27(5):520–526. doi:10.1007/s11606-011-1931-2
43. Moskowitz D, Thom DH, Hessler D, Ghorob A, Bodenheimer T. Peer coaching to improve diabetes self-management: which patients benefit most? J Gen Intern Med. 2013;28(7):938–942. doi:10.1007/s11606-013-2367-7
44. Nundy S, Dick JJ, Chou CH, Nocon RS, Chin MH, Peek ME. Mobile phone diabetes project led to improved glycemic control and net savings for Chicago plan participants. Health Aff. 2014;33(2):265–272. doi:10.1377/hlthaff.2013.0589
45. Ruissen MM, Torres-Peña JD, Uitbeijerse BS, et al. Clinical impact of an integrated e-health system for diabetes self-management support and shared decision making (POWER2DM): a randomised controlled trial. Diabetologia. 2023;66(12):2213–2225. doi:10.1007/s00125-023-06006-2
46. Chrvalaa CA, Sherrb D, Lipman RD. Diabetes education for Chinese adults with type 2 diabetes: a systematic review and meta-analysis of the effect on glycemic control. Patient Educ Couns. 2016;116:218–229. doi:10.1016/j.diabres.2016.04.001
47. Sarfo JO, Obeng P, Kyereh HK, Ansah EW, Attafuah PYA. Self-determination theory and quality of life of adults with diabetes: a scoping review. J Diabetes Res. 2023;2023(Cvd):1–12. doi:10.1155/2023/5341656
48. Aujoulat I, Marcolongo R, Bonadiman L, Deccache A. Reconsidering patient empowerment in chronic illness: a critique of models of self-efficacy and bodily control. Soc Sci Med. 2008;66(5):1228–1239. doi:10.1016/j.socscimed.2007.11.034
49. Hibbard JH, Stockard J, Mahoney ER, Tusler M. Development of the patient activation measure (PAM): conceptualizing and measuring activation in patients and consumers. Health Serv Res. 2004;39(4 I):1005–1026. doi:10.1111/j.1475-6773.2004.00269.x
50. Shay LA, Lafata JE. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med Decis Mak. 2015;35(1):114–131. doi:10.1177/0272989X14551638
51. Joosten EAG, DeFuentes-Merillas L, De Weert GH, Sensky T, Van Der Staak CPF, De Jong CAJ. Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence and health status. Psychother Psychosom. 2008;77(4):219–226. doi:10.1159/000126073
52. Kautzky-Willer A, Harreiter J, Pacini G. Sex and gender differences in risk, pathophysiology and complications of type 2 diabetes mellitus. Endocr Rev. 2016;37(3):278–316. doi:10.1210/er.2015-1137
53. Peters SAE, Huxley RR, Woodward M. Diabetes as risk factor for incident coronary heart disease in women compared with men: a systematic review and meta-analysis of 64 cohorts including 858,507 individuals and 28,203 coronary events. Diabetologia. 2014;57(8):1542–1551. doi:10.1007/s00125-014-3260-6
54. Cowie CC. Diabetes diagnosis and control: missed opportunities to improve health. Diabetes Care. 2019;42(June):994–1004. doi:10.2337/dci18-0047
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.