Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 14
Associations of GWAS-Identified Risk Loci with Progression, Efficacy and Toxicity of Radiotherapy of Head and Neck Squamous Cell Carcinoma Treated with Radiotherapy
Authors Li Q, Liang Y, Liu Z, Yu C
Received 17 June 2021
Accepted for publication 20 August 2021
Published 21 September 2021 Volume 2021:14 Pages 1205—1210
DOI https://doi.org/10.2147/PGPM.S325349
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Qinghuan Li,1,* Yi Liang,1,* Zeng Liu,2 Chuanyun Yu1
1Oncology Radiotherapy Center, Xiangyang Central Hospital, Affiliated Hospital of Hubei University of Arts and Science, Xiangyang, Hubei, 441021, People’s Republic of China; 2Department of Oncology, Xiangyang Central Hospital, Affiliated Hospital of Hubei University of Arts and Science, Xiangyang, Hubei, 441021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chuanyun Yu Tel/Fax +86-710-2813559
Email [email protected]
Zeng Liu Email [email protected]
Background: Head and neck squamous cell carcinoma (HNSCC) ranks the sixth most common cancer worldwide. This study aims to evaluate the associations of GWAS-identified HNSCC risk loci with progression, efficacy and toxicity of radiotherapy of HNSCC treated with radiotherapy.
Methods: Six GWAS-identified risk loci were genotyped and evaluated. Multivariate logistic regression was used to determine the associations of these SNPs with progression, efficacy and toxicity of radiotherapy of HNSCC treated with radiotherapy.
Results: We found that rs259919 was significantly associated with higher TNM stage (allele A vs G: OR=1.49; 95% CI: 1.09– 2.03; P=0.012), while rs3135001 was significantly associated with better efficacy of radiotherapy (allele T vs C: OR=1.80, 95% CIs=1.19– 2.73, P=0.005). Both SNP rs1265081 (allele A vs C: OR=1.41, 95% CIs=1.08– 1.86, P=0.012) and rs3135001 (allele T vs allele C: OR=0.53, 95% CIs=0.35– 0.79, P=0.002) were significantly associated with the occurrence of grade 3– 4 oral mucositis.
Conclusion: We identified that three GWAS-identified HNSCC risk loci were significantly associated with progression, efficacy and toxicity of radiotherapy of HNSCC. Our findings strengthen the understanding of the essential role of genetic background in the progression and therapeutic effects of HNSCC.
Keywords: progression, genetic, radiotherapy, HNSCC, efficacy, toxicity
Introduction
Head and neck squamous cell carcinoma (HNSCC), a group of malignant tumors originating in the head and neck, ranks the sixth most common cancer worldwide.1 Unlike the increased rates of HPV infection in the oropharynx in the United States and Western Europe, the high incidence of HNSCC in Southeast Asia and Australia is associated with the consumption of specific carcinogenic-containing products.2 The main methods of treatment for localized or locally limited HNSCC are resection, radiotherapy and systemic therapy.3 Despite the use of aggressive treatment, only about 40% of patients with the most common histologically altered type-HNSCC, could survive more than 5 years.4,5 Further, it is characterized by considerable heterogeneity in disease course and treatment outcome.6,7 Therefore, an in-depth understanding of the factors influencing the progression and therapeutic effects of HNSCC is urgently needed to support biomarkers development, early warning and personalized patient treatment.
There is a growing interest in finding genetic factors that can potentially help identify subgroups of patients at higher risk of disease progression and therapeutic effects. Against this backdrop, studies identified that there was a solid connection between single nucleotide polymorphisms (SNPs) of candidate genes/loci and progression of HNSCC.8–11 Recently, a two-phase genome-wide association study (GWAS) identified six loci, including 6p22.1, 18q22.2, 2p23.1, 5p15.33, 6p21.32, and 6p21.33, were associated with risk of HNSCC.12 These findings suggested that the immunologic mechanism was implicated in the etiology of HNSCC. It is assumed that these loci might explain inter-individual differences in the disease progression and sensitivity to standard anticancer treatment. However, whether these loci contribute to the progression and therapeutic effects of HNSCC was still unexplored, especially in Chinese population. The purpose of this study was to evaluate associations of these GWAS-identified HNSCC risk loci with progression, efficacy and toxicity of radiotherapy of HNSCC treated with radiotherapy.
Patients and Methods
Patient and Clinical Data
Totally included in this study were 500 newly diagnosed, histologically confirmed HNSCC cases treated with radiotherapy (RT) alone or in combination with chemotherapy (CHT). At recruitment, five milliliter of blood sample from the patients was collected. Written informed consent was obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Xiangyang Central Hospital.
Treatment Efficacy and Toxic Reaction
All patients were treated with radical external radiotherapy with or without cisplatin-based chemotherapy or both. Treatment efficacy were evaluated with magnetic resonance imaging (MRI) directly after finishing radiotherapy in line with the Response Evaluation Criteria in Solid Tumors (RECIST), which defined endpoint of treatment efficacy as complete remission (CR). Radiation-induced oral mucositis were evaluated according to the radiation toxicity grading criteria of the Radiation Therapy Oncology Group or European Organization for Research and Efficacy of Cancer (RTOG/EORTC). Patients were defined as grade 0–2 group and grade 3–4 group.
DNA Extraction and Genotyping
Germline DNA was extracted from 200 μL peripheral blood samples of patients using a commercial extraction kit (Tiangen Biotech Corporation, Beijing, China). Genotyping of six top signal SNPs (rs259919, rs3135001, rs1265081, rs142021700, rs10462706, and rs4318431) was performed using the Sequenom iPLEX MassARRAY system (Sequenom, Inc., San Diego, CA, USA). For quality control, a 10% random sample was repeated, and 100% concordance was achieved for all SNPs. All laboratory genotyping personnel were blind to the clinical outcomes of the patients’ samples.
Statistical Analysis
Continuous data was presented as mean ± standard deviation, while categorical data was presented as frequency and percentage. Univariate logistic regression was performed to determine the association of the GWAS-identified risk loci with the progression, efficacy and toxicity of radiotherapy of HNSCC treated with radiotherapy. Statistical Analysis System software (Version 9.4; SAS Institute, Cary, NC) was used for all of the statistical analyses.
Results
Characteristics of Study Patients
Table 1 presents the baseline demographics and clinical information of the 500 HNSCC cases. The mean age was 50.4 (SD=9.7) with 407 males (81.5%), and a mean BMI of 23.4 (SD=3.9). There were 203 smokers (40.6%) and 167 alcohol drinkers (33.4%). The tumor site included oropharynx (30.6%), hypopharynx (19.0%), and larynx (50.4%). Among them, 54.2% of the patients received radiotherapy alone. The TNM stage distribution of all HNSCC patients was 176 cases (35.2%) in stage I or II, 324 cases (64.8%) in stage III or IV, respectively. Overall, 349 (69.8%) patients reached CR after radiotherapy. Of the toxic reactions, 237 (47.4%) patients developed grade 3–4 oral mucositis.
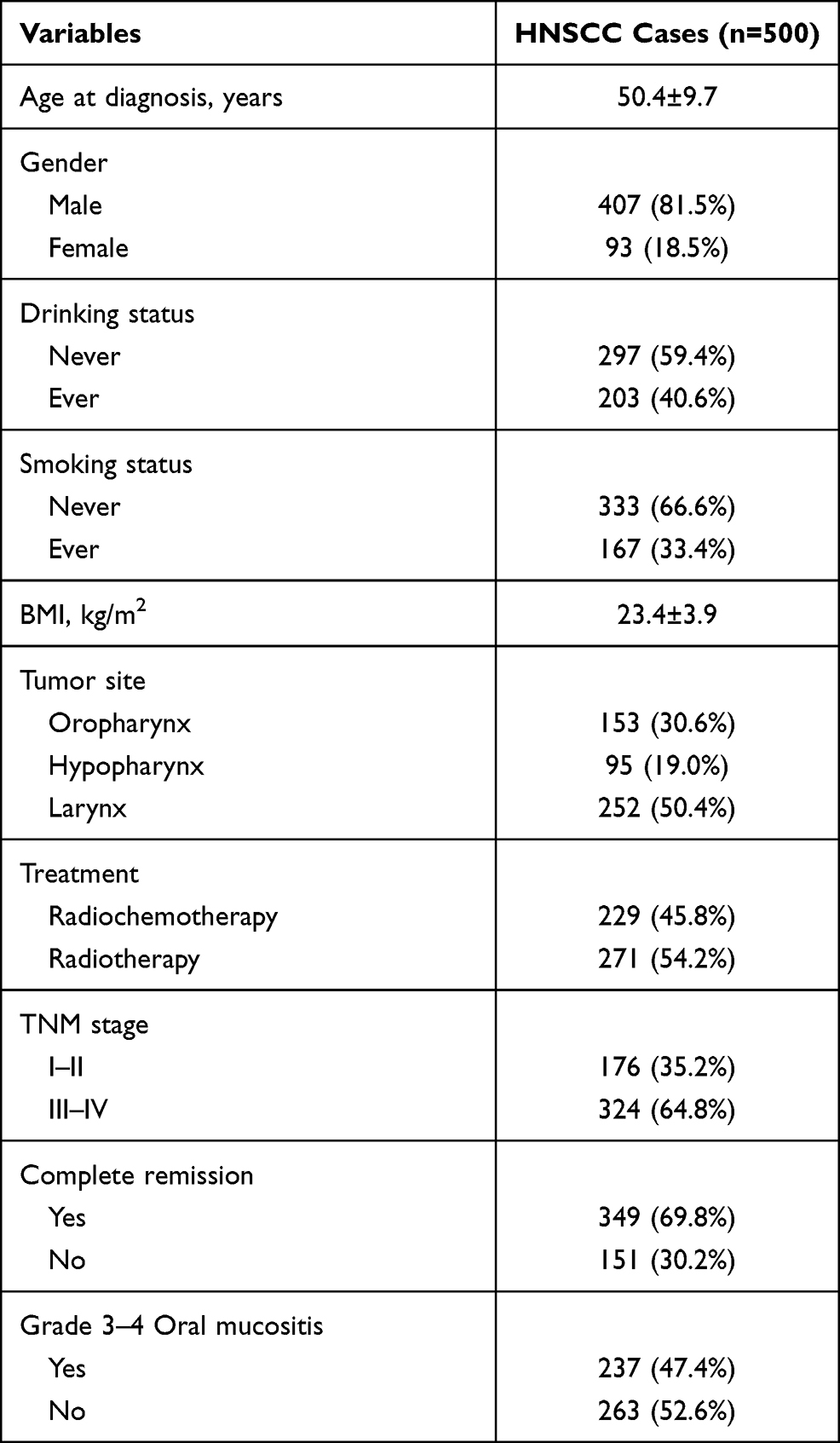 |
Table 1 Characteristics of the Patients |
Associations Between GWAS-Identified Risk Loci and the TNM Stage in HNSCC Patients
Table 2 presents the associations between GWAS-identified risk loci and the TNM stage in HNSCC patients. Only five variants (rs259919, rs3135001, rs1265081, rs10462706, and rs4318431) were analyzed, because the minor allele frequency of rs142021700 was small than 5%. We found rs259919 was significantly associated with higher TNM stage (allele A vs G: OR=1.49; 95% CI: 1.09–2.03; P=0.012). A significantly higher rs259919 AG/AA genotype distribution in the TNM (III–IV) group than in the TNM (I–II) subgroup was detected.
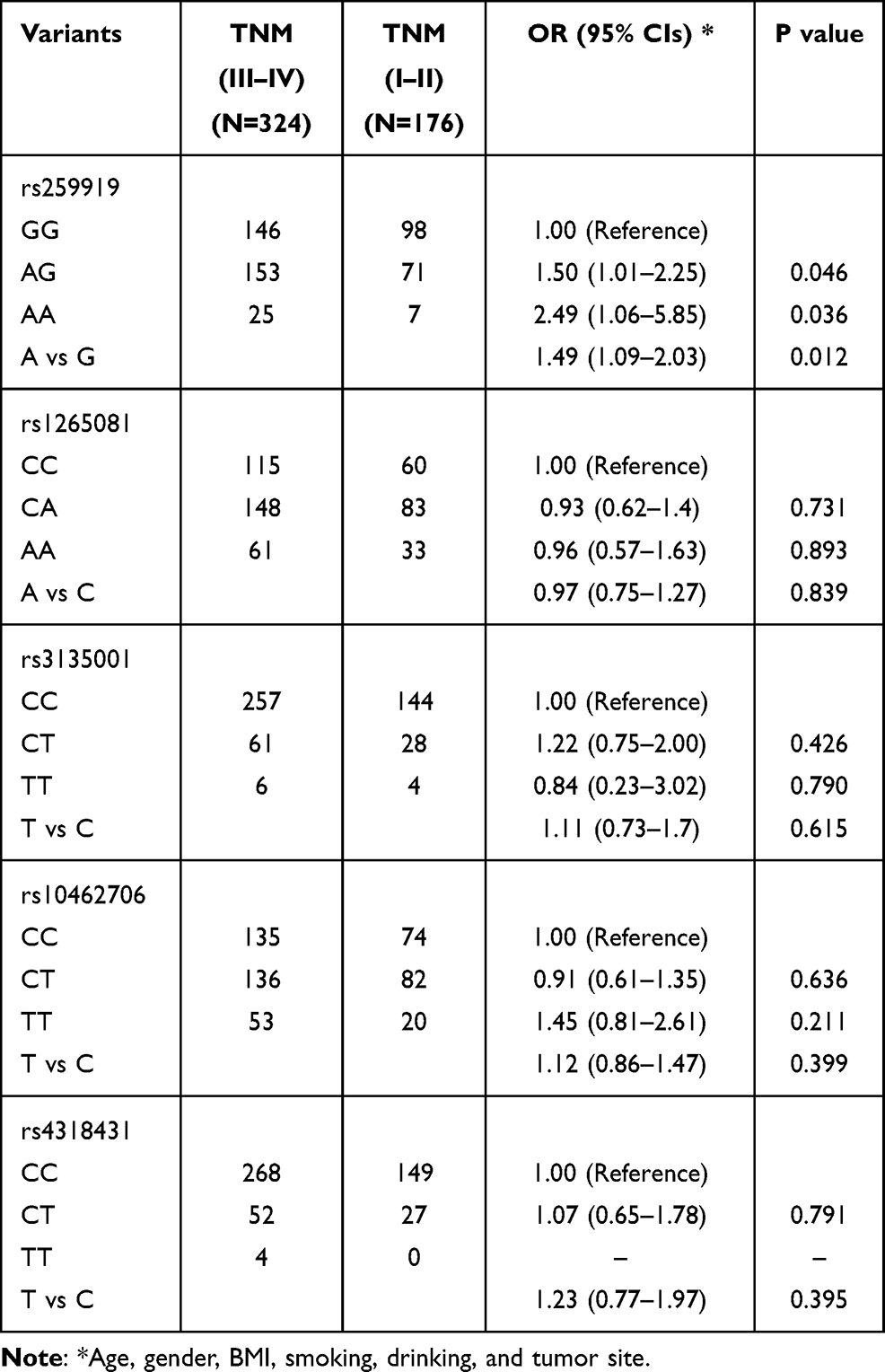 |
Table 2 Association Between GWAS-Identified Risk Loci and the TNM Stage in HNSCC Patients |
Associations Between GWAS-Identified Risk Loci and the Efficacy of Radiotherapy
Table 3 presents the associations between GWAS-identified risk loci and the efficacy of radiotherapy in HNSCC patients. We found rs3135001 was significantly associated with better efficacy of radiotherapy (allele T vs C: OR=1.80, 95% CIs=1.19–2.73, P=0.005).
 |
Table 3 Association Between GWAS-Identified Risk Loci and the Efficacy of Radiotherapy in HNSCC Patients (CR: Complete Remission) |
Associations Between the GWAS-Identified Risk Loci and Grade 3–4 Radiation-Induced Oral Mucositis
Table 4 presents the associations between GWAS-identified risk loci and grade 3–4 radiation-induced oral mucositis. Both SNP rs1265081 (allele A vs C: OR=1.41, 95% CIs=1.08–1.86, P=0.012) and rs3135001 (allele T vs allele C: OR=0.53, 95% CIs=0.35–0.79, P=0.002) were significantly associated with the occurrence of grade 3–4 oral mucositis.
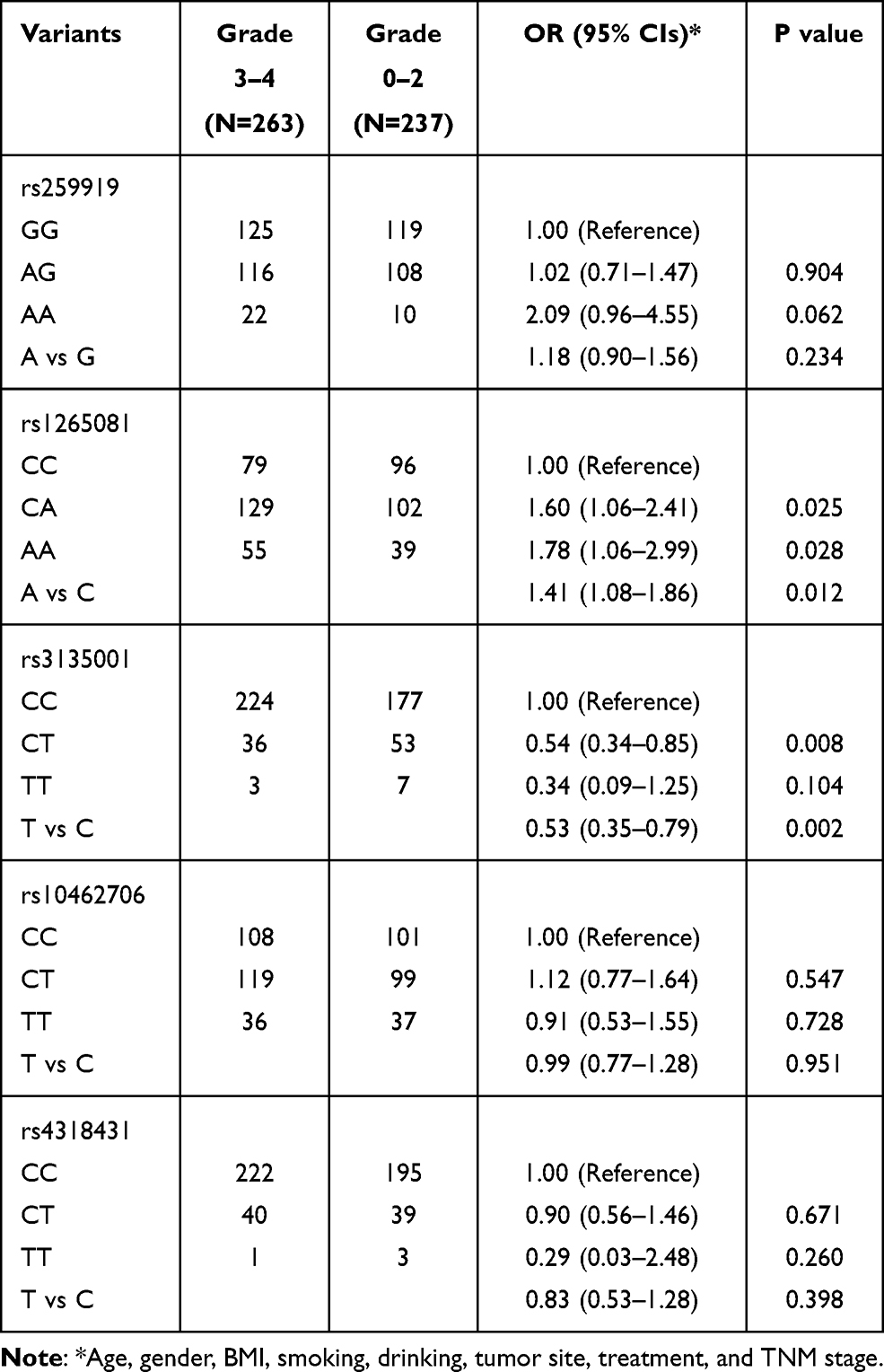 |
Table 4 Association Between GWAS-Identified Risk Loci and Grade 3–4 Radiation-Induced Oral Mucositis |
Discussion
In the past decades, combined radiotherapy and chemotherapy have been recognized as feasible in HNSCC treatment.13 However, its progression, efficacy and toxicity of radiotherapy was full of uncertainty. In the current study, we explored the associations between several GWAS-identified HNSCC risk loci with progression, efficacy and toxicity of radiotherapy of HNSCC. We revealed that: (1) rs259919 was significantly associated with higher TNM stage; (2) rs3135001 was significantly associated with better efficacy of radiotherapy; (3) both SNP rs1265081 and rs3135001 were significantly associated with the occurrence of grade 3–4 oral mucositis. Taking together, these loci might be useful biomarkers for predicting efficacy and toxicity of radiotherapy for HNSCC patients.
HNSCC is a heterogeneous disease, differing not only in clinical presentation and course, but also in genetic variation.14 Using candidate gene approach, Zhang et al have identified several loci for risk and progression of HNSCC.9–11 The study of these genetic variants has revealed not only underlying mechanisms but also clinically useful biomarkers that contribute to the personalization of treatment. In current study, 3 of the five GWAS-identified HNSCC risk loci was identified to be associated with either progression, efficacy or toxicity of radiotherapy of HNSCC. Among them, rs259919 not only increases the occurrence of the disease but also is related to the progress of HNSCC. SNP rs259919 was located in the lncRNA ZNRD1-AS1 region, which have reported to associated with bladder cancer, nasopharyngeal carcinoma, breast cancer, glioma, endometrial cancer, hepatocellular carcinoma, lung cancer, and cervical cancer.15–24 Interestingly, we found rs3135001 was significantly associated with better efficacy of radiotherapy and fewer grade 3–4 oral mucositis. Using RegulomeDB 2.0, we found rs3135001 was located in a TF binding or DNase peak region.25 SNP rs3135001 was located in the HLA-DQB1 domain, which exhibit a larger degree of allelic polymorphism than usually recognized by routine serology.26 It has been linked many diseases, including cancer, cardiovascular diseases, and autoimmune diseases.27–30 In addition, we also found rs1265081 was significantly associated with the occurrence of grade 3–4 oral mucositis. SNP rs1265081 was located in the CCHCR1 domain, and GTEX portal also showed allele A of rs1265081 was associated with higher expression level of CCHCR1 in whole blood and many tissues.31 CCHCR1 was identified to up-regulate in skin cancer and associated with EGFR expression.32
Although we have relative moderate sample size and systematic follow-up endpoint collection, several inherent limitations in this study need to be addressed. First, because of study time, funding, and staffing constraints, we are not currently following up on overall survival, just some short- to medium-term endpoints. Second, sample size was limited in relation to our stratification analysis. Third, further large-scale analysis with in-depth functional experiments are needed. Nevertheless, our results still provided new evidence and ideas for the prognostic study of HNSCC.
In conclusion, we identified three GWAS-identified HNSCC risk loci were significantly with progression, efficacy and toxicity of radiotherapy of HNSCC. Our findings strengthen the understanding of the essential role of genetic background in the progression and therapeutic effects of HNSCC. Further investigations of the underlying molecular mechanisms to explain how these polymorphisms affect disease progression, and response to radiotherapy are needed.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Ferlay J, Colombet M, Soerjomataram I, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144(8):1941–1953. doi:10.1002/ijc.31937
2. Hashibe M, Brennan P, Benhamou S, et al. Alcohol drinking in never users of tobacco, cigarette smoking in never drinkers, and the risk of head and neck cancer: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. J Natl Cancer Inst. 2007;99(10):777–789. doi:10.1093/jnci/djk179
3. Lee NCJ, Kelly JR, Park HS, et al. Patterns of failure in high-metastatic node number human papillomavirus-positive oropharyngeal carcinoma. Oral Oncol. 2018;85:35–39. doi:10.1016/j.oraloncology.2018.08.001
4. Leemans CR, Braakhuis BJ, Brakenhoff RH. The molecular biology of head and neck cancer. Nat Rev Cancer. 2011;11(1):9–22. doi:10.1038/nrc2982
5. Glazer CA, Chang SS, Ha PK, Califano JA. Applying the molecular biology and epigenetics of head and neck cancer in everyday clinical practice. Oral Oncol. 2009;45(4–5):440–446. doi:10.1016/j.oraloncology.2008.05.013
6. Ebrahimi A, Luk PP, Low H, et al. The American Joint Committee on Cancer staging for metastatic head and neck cutaneous squamous cell carcinoma: a multi-institutional study of within-stage heterogeneity and impact on prognostic performance. Head Neck. 2020;42(11):3235–3242. doi:10.1002/hed.26369
7. Mroz EA, Rocco JW. Intra-tumor heterogeneity in head and neck cancer and its clinical implications. World J Otorhinolaryngol Head Neck Surg. 2016;2(2):60–67. doi:10.1016/j.wjorl.2016.05.007
8. Sanguansin S, Petmitr S, O-charoenrat P, Pongstaporn W. Association of glutathione S-transferase omega gene polymorphisms with progression of head and neck cancer. Mol Biol Rep. 2012;39(12):10915–10920. doi:10.1007/s11033-012-1991-3
9. Zhang Z, Wang L, Wei S, et al. Polymorphisms of the DNA repair gene MGMT and risk and progression of head and neck cancer. DNA Repair (Amst). 2010;9(5):558–566. doi:10.1016/j.dnarep.2010.02.006
10. Zhang Z, Wang LE, Sturgis EM, et al. Polymorphisms of FAS and FAS ligand genes involved in the death pathway and risk and progression of squamous cell carcinoma of the head and neck. Clin Cancer Res. 2006;12(18):5596–5602. doi:10.1158/1078-0432.CCR-05-1739
11. Zhang Z, Shi Q, Sturgis EM, Spitz MR, Hong WK, Wei Q. Thymidylate synthase 5ʹ- and 3ʹ-untranslated region polymorphisms associated with risk and progression of squamous cell carcinoma of the head and neck. Clin Cancer Res. 2004;10(23):7903–7910. doi:10.1158/1078-0432.CCR-04-0923
12. Shete S, Liu H, Wang J, et al. A Genome-Wide Association Study identifies two novel susceptible regions for squamous cell carcinoma of the head and neck. Cancer Res. 2020;80(12):2451–2460. doi:10.1158/0008-5472.CAN-19-2360
13. Strigari L, Pinnaro P, Carlini P, et al. Efficacy and mucosal toxicity of concomitant chemo-radiotherapy in patients with locally-advanced squamous cell carcinoma of the head-and-neck in the light of a novel mathematical model. Crit Rev Oncol Hematol. 2016;102:101–110. doi:10.1016/j.critrevonc.2016.04.004
14. Gingerich MA, Smith JD, Michmerhuizen NL, et al. Comprehensive review of genetic factors contributing to head and neck squamous cell carcinoma development in low-risk, nontraditional patients. Head Neck. 2018;40(5):943–954. doi:10.1002/hed.25057
15. Gao Z, Li S, Zhou X, Li H, He S. Knockdown of lncRNA ZNRD1-AS1 inhibits progression of bladder cancer by regulating miR-194 and ZEB1. Cancer Med. 2020;9(20):7695–7705. doi:10.1002/cam4.3373
16. Wang Q, Hu X, Du M, et al. ZNRD1-AS1 promotes nasopharyngeal carcinoma cell invasion and metastasis by regulating the miR-335-ROCK1 axis. OncoTargets Ther. 2020;13:4779–4790. doi:10.2147/OTT.S250028
17. Kim HW, Jeong D, Ham J, et al. ZNRD1 and Its antisense long noncoding RNA ZNRD1-AS1 are oppositely regulated by cold atmospheric plasma in breast cancer cells. Oxid Med Cell Longev. 2020;2020:9490567. doi:10.1155/2020/9490567
18. Wang M, Yang C, Liu X, et al. An upstream open reading frame regulates vasculogenic mimicry of glioma via ZNRD1-AS1/miR-499a-5p/ELF1/EMI1 pathway. J Cell Mol Med. 2020;24(11):6120–6136. doi:10.1111/jcmm.15217
19. Peng JT, Li MC. A functional Cis-eQTL locus in lncRNA ZNRD1-AS1 contributes to the susceptibility of endometrial cancer. Eur Rev Med Pharmacol Sci. 2019;23(18):7802–7807.
20. Wang PY, Li JH, Liu YM, et al. Single nucleotide polymorphisms in ZNRD1-AS1 increase cancer risk in an Asian population. Oncotarget. 2017;8(6):10064–10070. doi:10.18632/oncotarget.14334
21. Liu Z, Song C, Wen J, et al. Hepatitis B virus genotypes, expression quantitative trait loci for ZNRD1-AS1 and their interactions in hepatocellular carcinoma. Oncotarget. 2016;7(28):44076–44083. doi:10.18632/oncotarget.9854
22. Li D, Song L, Wen Z, et al. Strong evidence for LncRNA ZNRD1-AS1, and its functional Cis- eQTL locus contributing more to the susceptibility of lung cancer. Oncotarget. 2016;7(24):35813–35817. doi:10.18632/oncotarget.8411
23. Guo L, Wen J, Han J, et al. Expression quantitative trait loci in long non-coding RNA ZNRD1-AS1 influence cervical cancer development. Am J Cancer Res. 2015;5(7):2301–2307.
24. Wen J, Liu Y, Liu J, et al. Expression quantitative trait loci in long non-coding RNA ZNRD1-AS1 influence both HBV infection and hepatocellular carcinoma development. Mol Carcinog. 2015;54(11):1275–1282. doi:10.1002/mc.22200
25. Boyle AP, Hong EL, Hariharan M, et al. Annotation of functional variation in personal genomes using RegulomeDB. Genome Res. 2012;22(9):1790–1797. doi:10.1101/gr.137323.112
26. Morel C, Zwahlen F, Jeannet M, Mach B, Tiercy JM. Complete analysis of HLA-DQB1 polymorphism and DR-DQ linkage disequilibrium by oligonucleotide typing. Hum Immunol. 1990;29(1):64–77. doi:10.1016/0198-8859(90)90070-6
27. David AL, Taylor GM, Gokhale D, Aplin JD, Seif MW, Tindall VR. HLA-DQB1*03 and cervical intraepithelial neoplasia type III. Lancet. 1992;340(8810):52. doi:10.1016/0140-6736(92)92464-Q
28. Reveille JD, Owerbach D, Goldstein R, Moreda R, Isern RA, Arnett FC. Association of polar amino acids at position 26 of the HLA-DQB1 first domain with the anticentromere autoantibody response in systemic sclerosis (scleroderma). J Clin Invest. 1992;89(4):1208–1213. doi:10.1172/JCI115704
29. Wank R, Meulen JT, Luande J, Eberhardt HC, Pawlita M. Cervical intraepithelial neoplasia, cervical carcinoma, and risk for patients with HLA-DQB1*0602,*301,*0303 alleles. Lancet. 1993;341(8854):1215. doi:10.1016/0140-6736(93)91043-L
30. Halle MK, Sodal M, Forsse D, et al. A 10-gene prognostic signature points to LIMCH1 and HLA-DQB1 as important players in aggressive cervical cancer disease. Br J Cancer. 2021;124(10):1690–1698. doi:10.1038/s41416-021-01305-0
31. Lonsdale J, Thomas J, Salvatore M. The genotype-tissue expression (GTEx) project. Nat Genet. 2013;45(6):580–585. doi:10.1038/ng.2653
32. Suomela S, Elomaa O, Skoog T, et al. CCHCR1 is up-regulated in skin cancer and associated with EGFR expression. PLoS One. 2009;4(6):e6030. doi:10.1371/journal.pone.0006030
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.