Back to Journals » Journal of Healthcare Leadership » Volume 17
Associations Between Work-Related Factors, Mental Well-Being, and Health Literacy Sensitivity: A Cross-Sectional Study Among Healthcare Personnel
Authors Stavdal MN ![]() , Hermansen Å, Sjetne IS
, Hermansen Å, Sjetne IS ![]() , Larsen MH, Wahl AK, Kohnen D, Gay CL, Lerdal A
, Larsen MH, Wahl AK, Kohnen D, Gay CL, Lerdal A ![]() , Borge CR
, Borge CR
Received 6 May 2025
Accepted for publication 1 August 2025
Published 13 August 2025 Volume 2025:17 Pages 383—394
DOI https://doi.org/10.2147/JHL.S533694
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Malene Nerbøvik Stavdal,1,2 Åsmund Hermansen,3 Ingeborg Strømseng Sjetne,4 Marie Hamilton Larsen,5 Astrid Klopstad Wahl,1 Dorothea Kohnen,6,7 Caryl L Gay,2,8 Anners Lerdal,1,2 Christine Råheim Borge1,2
1Department of Public Health and Interdisciplinary Health Sciences, University of Oslo, Oslo, Norway; 2Research Department, Lovisenberg Diaconal Hospital, Oslo, Norway; 3Faculty of Social Sciences, Department of Social Work, Child Welfare and Social Policy, OsloMet Oslo Metropolitan University, Oslo, Norway; 4Norwegian Institute of Public Health, Division for Health Services, Oslo, Norway; 5Department of Postgraduate Studies, Lovisenberg Diaconal University College, Oslo, Norway; 6Faculty of Psychology and Educational Sciences, Research Group Work, Organisational, and Personnel Psychology WOPP - O2L Van den Heuvelinstituut, KU Leuven, Leuven, Belgium; 7Faculty of Medicine Department of Public Health and Primary Care, Leuven Institute for Healthcare Policy, Leuven, Belgium; 8Department of Family Health Care Nursing, University of California, San Francisco, CA, USA
Correspondence: Malene Nerbøvik Stavdal, Department of Public Health and Interdisciplinary Health Sciences, University of Oslo, P.O. Box 1111 Blindern, Oslo, 0317, Norway, Tel +47 40223099, Email [email protected]
Objective: Explore possible associations between healthcare personnel’s work-related factors, mental well-being, and health literacy sensitivity. Few studies have investigated these factors. Thus, knowledge about their relationships may enhance healthcare personnel’s ability to meet patients’ health literacy needs, ultimately improving patient care.
Methods: This cross-sectional survey included interdisciplinary healthcare personnel (N = 288, 75% female, mean age 44 (SD = 11.8)) working in direct patient care at a medium-sized general hospital in Norway. Participants were recruited from May to June 2022 and asked to answer questions regarding work-related factors, mental well-being, and how they follow up on patients’ health literacy needs. Data were analyzed using hierarchical multiple regression.
Results: Greater health literacy sensitivity among healthcare personnel is associated with fewer work-related and mental well-being challenges. The work-related factors, teamwork (β = 0.138– 0.236, p < 0.05 – p < 0.001) and staffing (β = 0.178, p < 0.01), as well as the mental well-being variables, work engagement (β = 0.179– 0.288, p < 0.01 – < 0.001) and depression (β = 0.154, p < 0.05), show statistically significant associations with one or more of the nine health literacy domains.
Conclusion: Work-related factors and mental well-being, particularly work engagement, are associated with healthcare personnel’s health literacy sensitivity.
Practice Implications: Healthcare organizations should actively enhance healthcare personnel’s health literacy resources while ensuring that their efforts to follow up on patients’ health literacy needs do not adversely impact the healthcare personnel’s work-related factors or mental well-being.
Keywords: health literacy, health literacy sensitivity, work engagement, work-related factors, mental well-being, hospital
Introduction
A worldwide initiative to enhance citizens’ health literacy (HL) through improved healthcare systems is ongoing.1,2 In the Norwegian population,3 one in three have HL challenges, meaning they struggle to “gain access to, understand and use information in ways which promote and maintain good health for themselves, their families and their communities”.4 The European Health Literacy Survey5 shows significant HL challenges in the greater European population, with almost one in two (47%) Europeans having limited HL. People with HL challenges often lack disease knowledge, have communication barriers, and experience shame when interacting with healthcare personnel (HCP). Moreover, they may suffer from a lack of involvement in decision-making, and encounter difficulties navigating the healthcare system.3,6–8 In light of these known difficulties, it is worrisome that HCP often seem to overestimate both patients’ and their own HL knowledge. They may lack an understanding of the HL concept as well as the importance of following up on patients’ HL needs.9
Healthcare organizations should prioritize patients’ and HCP’s needs for information accessibility and appropriate health-related services. This approach is known as health literacy responsiveness (HLR), where healthcare organizations ensure that health information, resources, and environments are accessible to individuals with varying levels of HL.10 However, the complexity of healthcare systems can pose significant challenges for patients, particularly those with low HL. Individuals with low HL face higher hospital admission rates and extended hospital stays.11 For an organization to achieve HLR, it must employ HCPs who are HL-sensitive, meaning they have adequate knowledge, skills, and attitudes to follow up on patients’ HL needs.12,13 This can, for example, be done by checking for patients’ understanding, encouraging questions, and using communication techniques and visual aids that are appropriate for their patients’ HL level.13,14 HCP need to apply HL techniques and enable patient involvement in every patient encounter to maximize health outcomes and safety,15 even in stressful situations.12
However, it can be challenging for HCP to be HL-sensitive. It might be perceived as an extra job demand, given that HCP often experience stress, heavy workloads, staffing shortages, and inadequate organizational leadership.2,16,17 The Job Demands-Resources (JD-R) model demonstrates the job demand of HL sensitivity as possibly being associated with work-related factors (teamwork and staffing) and mental well-being (work engagement, anxiety, and depression). The JD-R model describes two psychological processes where employees facing excessive job demands lead – via burnout – to negative outcomes, and conversely, job resources – via work engagement – nurture positive outcomes and reduce burnout.18–20 Demerouti et al18 define job demands as “aspects of the job that require sustained physical or mental effort and are therefore associated with certain physiological and psychological costs”, ie, physical demands, time pressure, and shift work.19 Not all job demands are negative, but demands may turn into job stressors when they exceed the capacity of available resources.19 Job resources, in turn, are those aspects of the job that help achieve goals, reduce the impact of job demands, or promote personal growth and development. An example is interdisciplinary teamwork, which is crucial for enhancing HLR and creating a safe environment and good working conditions for HCP.21 Carthon et al22 show that well-functioning teamwork, adequate staffing levels, and positive work engagement are among the factors that create a good work environment for nurses and affect patient safety, which likely also applies to other HCP groups.
Work engagement and burnout represent opposing ends of a spectrum,19 where work engagement can evolve into burnout by turning employees’ energy into exhaustion, involvement to cynicism, and efficacy into ineffectiveness.19 Addressing how HCP follow-up on patients’ HL needs may be necessary to avoid employee burnout. HCP experiencing burnout, symptoms of depression, and anxiety have been observed to deliver diminishing quality of care, potentially compromising patient safety.16,23–27 The prevalence of work-related burnout and other mental health challenges, such as symptoms of anxiety and depression, is higher among HCP than among employees in other professions, with burnout being the primary cause of HCP leaving their professions.25,26 Work engagement and satisfaction are also crucial work performance indicators.28 Frequently, exposure to job stressors, such as heavy workloads, can impact HCPs’ mental and physical well-being, serving as essential organizational predictors for work engagement.22,23
These challenges related to work factors and mental well-being suggest a potential link to HCP HL sensitivity. A qualitative study exploring HCP experiences has shown that HL sensitivity can influence HCP work satisfaction and stress.17 However, to our knowledge, no studies have investigated the associations between HL sensitivity and the work-related factors of teamwork and staffing, and the mental well-being indicators of work engagement, anxiety and depression using an instrument that explicitly captures HCP's knowledge, skills, and attitudes in the follow-up of patients’ HL needs. Such research is essential to enhancing our understanding of HL sensitivity and illuminating working conditions for HCP so that they can be optimized for better patient care. Hence, the present study aims to explore possible associations between healthcare personnel’s work-related factors, mental well-being, and HL sensitivity.
Methods
Study Design
This was a cross-sectional study of interdisciplinary HCP working in direct patient care at a medium-sized general hospital in Oslo, Norway. The study was conducted from May to June 2022 and followed the STROBE29 checklist for reporting observational studies.
This study is an independent satellite of the Magnet4Europe (M4E) project, which aims to improve mental health and well-being in the healthcare workplace. A detailed protocol of M4E is available elsewhere.30
Sample and Recruitment
Inclusion Criteria
Interdisciplinary HCP with a bachelor’s degree or higher, working in direct patient care. HCP from all hospital departments (ie, medical, surgical, mental health and addiction, as well as the child and adolescent psychiatric outpatient clinic) were included. Information about the study was provided to all eligible employees via Email and the hospital’s intranet. All eligible HCP were invited to answer questions regarding work-related factors, mental well-being, and HL sensitivity. Data collection took place using online data collection platforms.
Ethical Considerations
The study was conducted in accordance with the Helsinki Declaration and was approved by the South East Norway Regional Committees for Medical and Health Research Ethics (REK, protocol 166980) as well as the hospitals’ data protection official for research. Upon questionnaire entry, written informed consent was obtained electronically from all participants. We informed HCP that participation was voluntary, with the option to withdraw at any time, and that participants’ confidentiality was safeguarded.
Instruments and Data Collection
The M4E project’s questionnaire packages included multiple instruments related to this study’s aim. In addition to the M4E questionnaires, this study included an additional instrument to capture HL sensitivity among HCP. All instruments included in this study were validated.
Health Literacy Sensitivity
The Instrument of Health Literacy Competencies (IOHLC) was used to assess health literacy sensitivity among HCP. The IOHLC14 is a multidimensional instrument recently translated into Norwegian; the Norwegian version consists of 36 items.31 The items are distributed across nine domains, each consisting of three to six items. Response options for each item are: (1) highly disagree, (2) disagree, (3) neither agree nor disagree, (4) agree, and (5) highly agree. The nine domains are: (1) Design teaching plan for low health literacy, (2) Simple and practical teaching, (3) Building a friendly environment, (4) Design of easy-to-use materials, (5) Life-oriented teaching, (6) Checking for understanding, (7) Encouraging questions, (8) Self-designed low-literacy materials to clients, and (9) Interdisciplinary collaboration. Each domain score is calculated as the mean score of the items on that domain, with high values (max 5.0) indicating that participants highly agree. Higher domain scores indicate higher HL sensitivity. In our study, the Cronbach’s alpha coefficients range from 0.56 in domain four to 0.89 in domain seven.
Work-Related Factors
To capture Teamwork and Staffing, two items from the Practice Environment Scale (PES-5)32 were used: (1) A lot of teamwork between nurses and physicians and (2) Enough staff to get the work done. Each item is rated on a four-point scale: (1) Strongly disagree, (2) Disagree, (3) Agree, or (4) Strongly agree. Higher values indicate better teamwork/staffing. The PES-5 has recently been validated by Lake et al32 to be used as single items.
Mental Well-Being
Work engagement was captured with three items from the Utrecht Work Engagement Scale (UWES-3).33 The questions were scored on a five-point scale: (1) Never, (2) Seldom, (3) Sometimes, (4) Often, or (5) Always. Higher scores indicate higher work engagement. The UWES-3 has previously been validated by Schaufeli et al,33 and the Cronbach’s alpha in our study was 0.81.
Anxiety was measured with the Generalized Anxiety Disorder-2 (GAD-2).34 The two items were rated on a four-point scale: (1) Not at all, (2) Several days, (3) More than half the days, or (4) Nearly every day was used. Higher values indicate more frequent symptoms of anxiety. The GAD-2 was validated by Kroenke et al,34 and the Cronbach’s alpha in this study was 0.84.
Depression was measured with the Patient Health Questionnaire-2 (PHQ-2).35 The two items were rated on a four-point scale: (1) Not at all, (2) Several days, (3) More than half the days, or (4) Nearly every day. Higher values indicate more frequent symptoms of depression. The PHQ-2 was validated by Kroenke et al.35 The Cronbach’s alpha in this study was 0.83.
HCP’s socio-demographic characteristics (ie, age, sex, occupation, and working conditions, such as years working within the profession and at the hospital) were collected to formulate the M4E questionnaire package.
Data Analysis
Statistical analyses were performed using STATA version 18.1. Frequencies were used to describe the HCP’s socio-demographic characteristics and work conditions, work-related factors, mental well-being, and HL sensitivity. Pearson correlations were used to check for multicollinearity using a cut point of 0.7 (Table 1).36 Hierarchical multiple regression was used to investigate associations between the different HL domains as dependent variables and socio-demographics, work-related factors, and mental well-being as independent variables. The order in which independent variables entered the regression model was determined based on previous literature (see introduction). Figure 1 shows the three-step hierarchical multiple regression analysis used to answer the research question. At least 10–20 participants per independent variable were included in each regression analysis to ensure adequate statistical power. Conventional labels for effect sizes for explained variance (R2) were used: small = 0.01–0.09, medium = 0.09 to 0.25, and large = 0.25 and higher.37
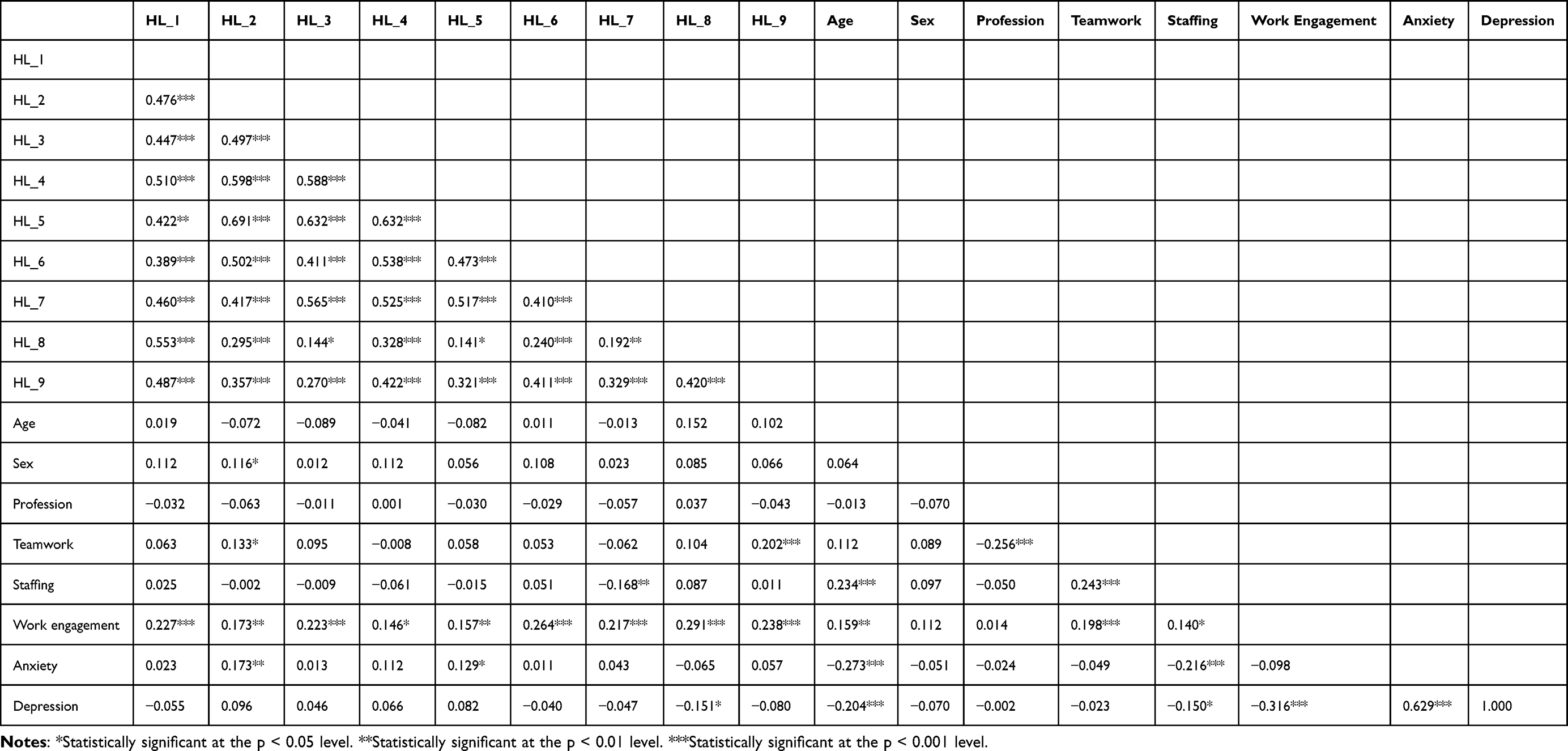 |
Table 1 Bivariate Correlation Matrix |
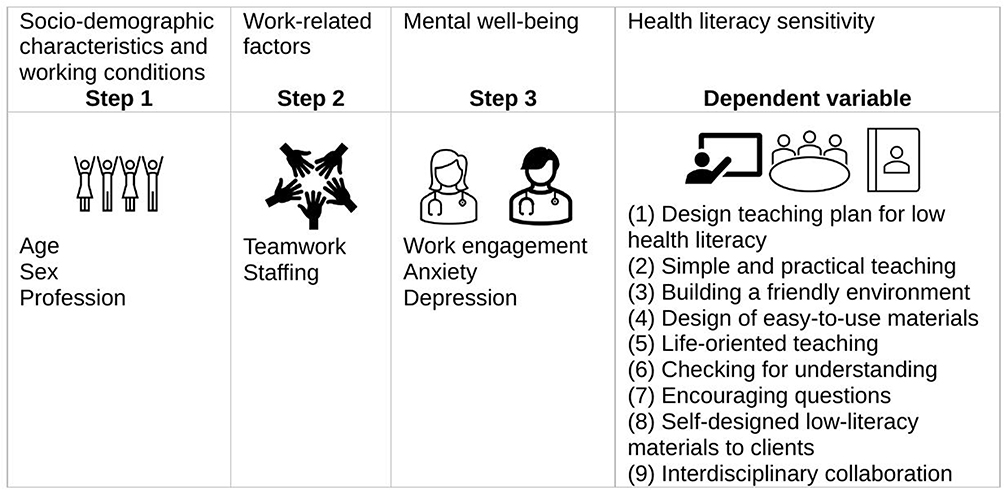 |
Figure 1 Theoretical model. |
Results
Of 1162 eligible healthcare personnel, 288 were recruited, yielding a 25% response rate.
Participant Demographics, Work-Related Factors, Mental Well-Being, and HL Sensitivity
Table 2 describes the 288 participants (216 females, 72 males) from the four hospital departments (ie, medical, surgical, mental health and addiction, and the child and adolescent psychiatric outpatient clinic). The average age of the participants was 44 years (SD = 12), while the average tenure working in the hospital was 11 years (SD = 9). Registered nurses (RNs) were the largest group of participants (41%), followed by medical doctors (MDs) and psychologists (30%), and other occupations (29%), such as physical therapists and social workers.
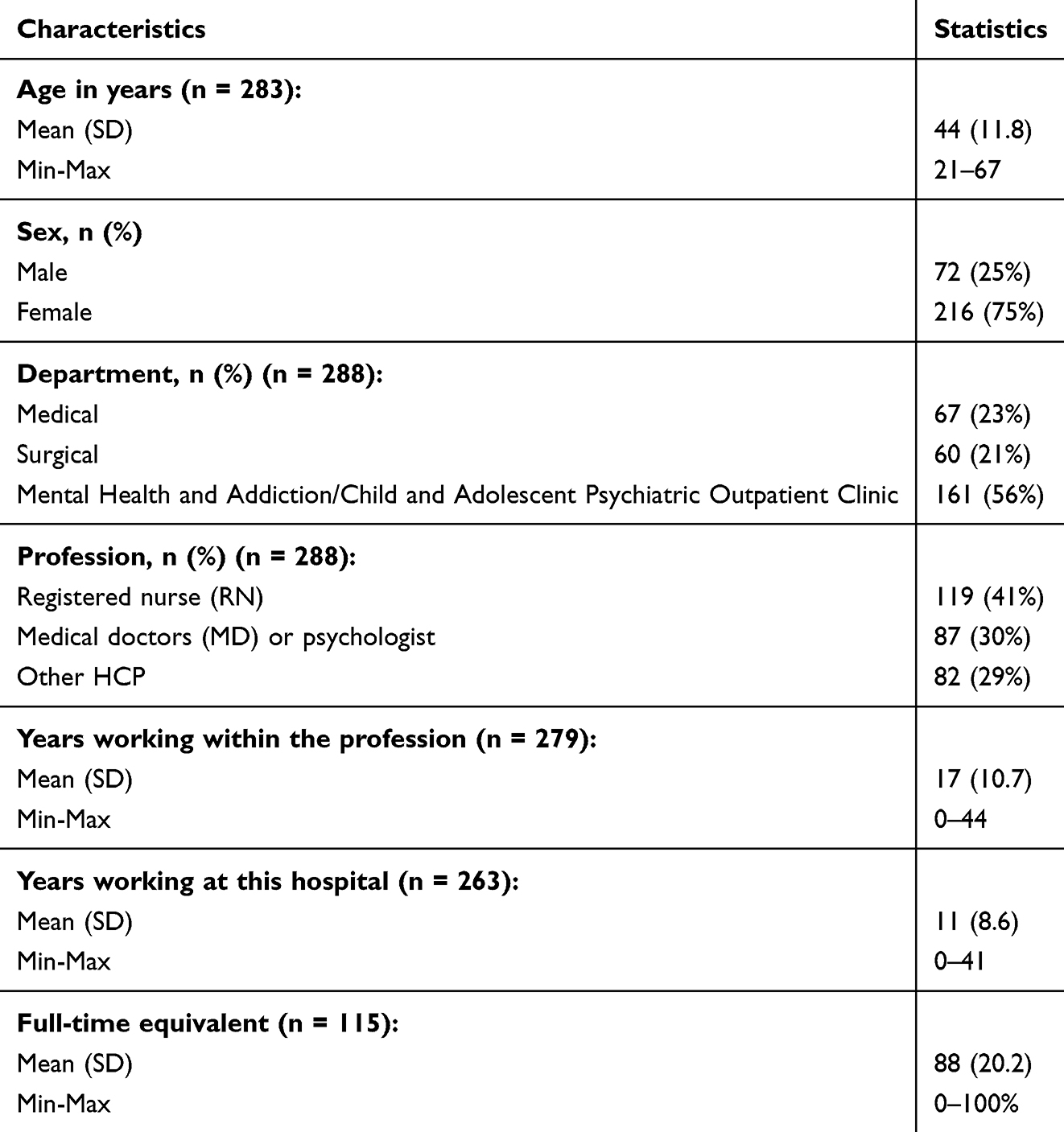 |
Table 2 Participant Socio-Demographic and Employment Characteristics and Job Descriptions (n = 288) |
Table 3 presents the descriptive statistics for measures of work-related factors, mental well-being, and HL sensitivity.
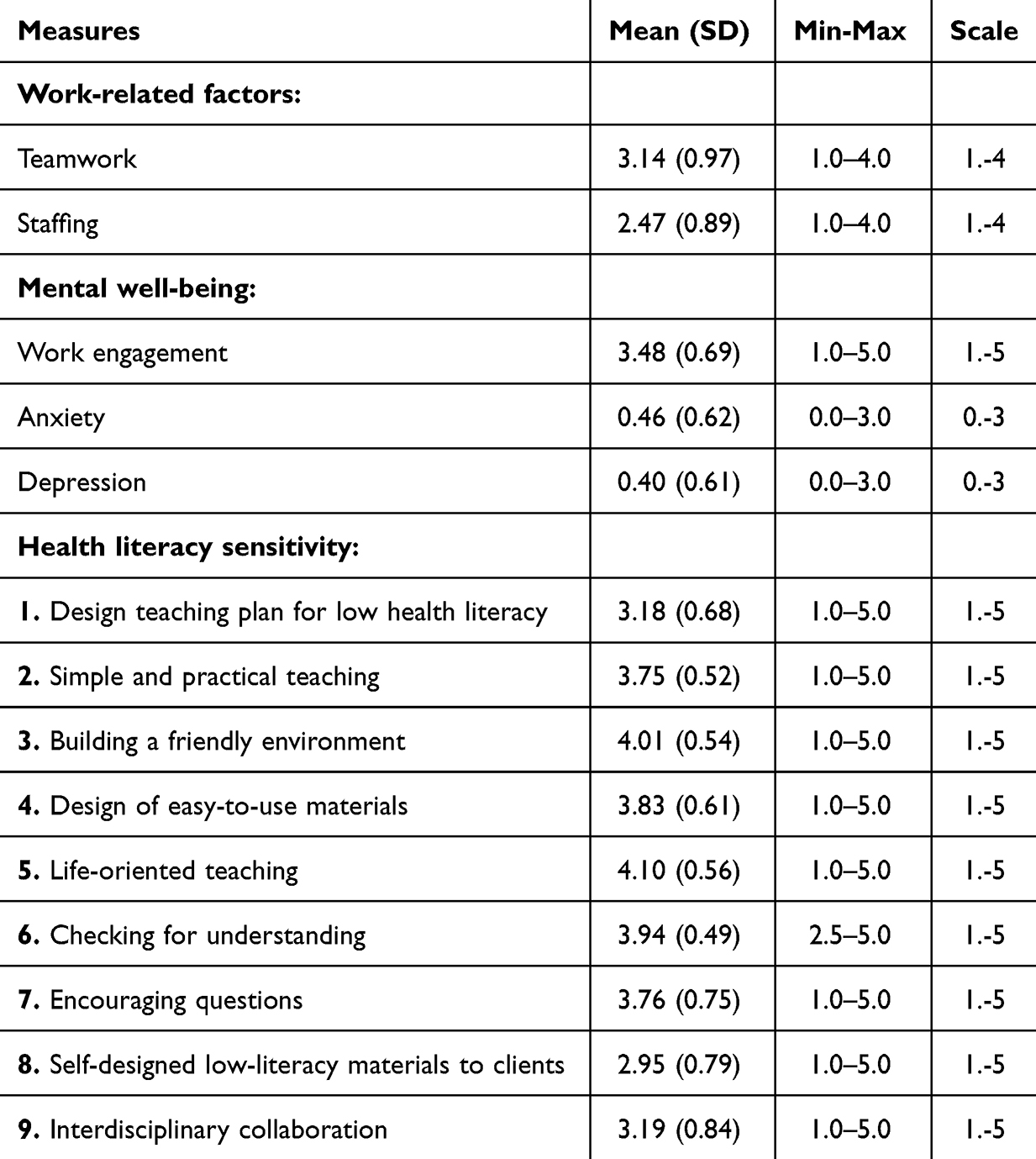 |
Table 3 Descriptive Statistics for Measures of Health Literacy Sensitivity, Work-Related Factors, and Mental Well-Being (n = 288). High Scores = Highly Agrees |
Associations Between Work-Related Factors, Mental Well-Being, and HL Sensitivity
Table 4 shows associations between work-related factors, mental well-being, and HCP HL sensitivity. HL domains 1–9 are the dependent variables throughout the hierarchical multiple regression, and in step 1 are the independent variables, age, sex, and profession included. However, the independent variables do not make significant contributions to the regression model and are not shown in Table 4. In step 2 of the regression model were, the work-related factor variables teamwork and staffing added as independent variables while also adjusting for step 1. The mental well-being variables work engagement, anxiety, and depression were added as independent variables in step 3, along with steps 1 and 2. The Pearson correlation (r) columns show that all independent variables correlated significantly with one or more of the nine HL domains (p < 0.05).
 |
Table 4 Hierarchical Multiple Regression Analysis of the Relationships of Work-Related Factors and HCP Mental Well-Being (Independent Variables) to the 9 Domains of Health Literacy Sensitivity (Dependent Variables), n = 288 |
As shown in Table 4, the hierarchical multiple regression illustrates the independent work-related factor variables – teamwork and staffing – in step 2. HCP experiencing high levels of teamwork are those who perform simple and practiced teaching (HL domain 2, r = 0.073, p < 0.05) and interdisciplinary collaboration (HL domain 9, r = 0.204, p < 0.001). HCP experiencing low staffing levels encourage patients to ask questions (HL domain 7, r = −0.150, p < 0.01). The multiple regression (step 2) analysis shows that high teamwork remains significantly associated with HL domain 2 (st.beta = 0.14, p < 0.05) and HL domain 9 (st.beta = 0.24, p < 0.001) and that staffing levels remain significantly associated with HL domain 7 (st.beta = 0.18, p < 0.01).
Step 3 of the regression analysis shows that the independent mental well-being variable, work engagement, is significantly associated with HCP being highly HL sensitive in all nine HL domains (p < 0.05) (Table 4). Work engagement remains significant in all nine equations in step 3 of the multiple regression analysis (st.β = 0.18–0.29, p < 0.05–0.001, R2= 6–11%).
The independent mental well-being variables anxiety and depression also show significance in step 3 (Table 4). HCP experiencing symptoms of anxiety work with HL in interdisciplinary collaborations (HL domain 9, r = 0.222, p < 0.05), and HCP experiencing symptoms of depression show associations with building-friendly environments (HL domain 3, r = 0.154, p < 0.05). The multiple regression analysis shows that anxiety remains significant in step 3 of HL domain 9 (st.beta = 0.16, p < 0.05), and depression remains significant in step 3 of HL domain 3 (st.beta = 0.18, p < 0.05). The significance shown in the work-related factor variable staffing in step 2 remains significant in step 3, HL domain 7 (st.beta = 0.19, p < 0.01).
Anxiety is included in the regression analysis because it correlates (r) with two HL domains (2, 5) in the bivariate correlation matrix (Table 1). Still, in step three of the multiple regression analysis (Table 4), anxiety only significantly correlates with HL domain 9. Notably, anxiety and depression share a correlation coefficient of 0.6, suggesting multicollinearity that likely influences these results. This could explain why depression´s inclusion in the model renders anxiety significant in HL domain 9, while it loses significance in HL domains 2 and 5. In the regression analysis, anxiety´s relationship with HL domain 9 may be masked by other variables or lack sufficient strength to emerge independently, underscoring the regression’s sensitivity to interrelationships among predictors. Depression was significantly correlated with HL domain 8 in the bivariate correlation matrix, but this association is lost in the regression analyses, where its only significant relationship is with HL domain 3.
Discussion and Conclusion
Discussion
This study aimed to explore possible associations between healthcare personnel’s work-related factors, mental well-being, and health literacy sensitivity. The findings show that engaged HCP are HL-sensitive. HCP who experience positive mental well-being through work engagement report high achievement addressing their patients’ HL needs. Work engagement is a positive, fulfilling, work-related state of mind characterized by vigor, dedication, and absorption,19 and engaged employees possess key attributes essential for effective HL follow-up with patients. Engaged employees identify with their work, leading them to invest considerable effort, remain physically active, and stay mentally alert.38
A recent study exploring associations with HCP work engagement has found links to work satisfaction, work overload, and emotional exhaustion.39 Within the JD-R model, where burnout and engagement are considered each other’s opposite, is work engagement considered a positive and energetic form of well-being.19 On the other hand, HL sensitivity is considered a job demand that can result in high work pressure, emotionally demanding interactions, and burnout for employees.40 HCP experiencing burnout may put patients at risk of worse patient outcomes, lower patient satisfaction, and reduced quality and safety.16,30 Fortunately, not all job demands are harmful, and engaged employees are motivated to stay involved and work to conserve and create new resources.40 Clinical HCP engagement for HL sensitivity should be viewed as a vital contribution to HLR, as all patients benefit from interactions with HL-sensitive HCP.9 Job resources are connected to organizational outcomes through engagement, functioning either as an intrinsic motivational role promoting employees’ growth, learning, and development or as an extrinsic motivational role, helping them achieve work goals.19 Employees who have intrinsic or extrinsic motivation for working with HL should be considered valuable assets to healthcare organizations, knowing that HCP must be held accountable for educating all patients, regardless of their illness and HL level.6
This study clearly establishes an important association between the work-related factor, teamwork, simple and practical teaching, and interdisciplinary collaboration. Carthon et al22 describe interdisciplinary teamwork as one of the most important factors for providing effective and efficient patient care. Moreover, collaborative HL follow-up can alleviate HCP workload and time constraints, thereby improving the effectiveness of HL sensitivity.2 Enhanced social support and a sense of community at work are connected to increased employee engagement and a reduced risk of burnout because these factors lessen the perceived demands of the job.23 Teamwork can be seen as a crucial job resource within the JD-R model, serving as a protective factor for HCP against emotional exhaustion and disengagement.41
Interestingly, this study also shows that HCP who report understaffing are willing to encourage patients to ask questions. One possible explanation could be that time constraints often hinder HL efforts,2 and understaffed HCP might not have time to be sufficiently HL sensitive, placing the responsibility of asking concrete questions on the patients. Understaffing is a significant challenge in today’s healthcare,42 and HCP can experience frustration when care is not person-centered or left incomplete due to work overload; these issues and low HL are perceived as threats to patient safety.27 However, it is enlightening that patient teaching is among the highest-prioritized activities HCP would focus on if staffing levels were improved.43 When considering HL sensitivity as a job demand within the JD-R model, we recognize that addressing patients’ HL needs can lead to increased time pressure and physical workload for HCP if organizational structures are lacking.
HCP experiencing symptoms of depression often work hard to create a friendly environment for patients and their families. Despite having little interest or pleasure in doing things and feeling down, depressed, or hopeless, these professionals manage to foster mutual trust and demonstrate understanding toward patients. These efforts may stem from a genuine desire to do good, allowing HCP who experience symptoms of depression to connect with patients differently and meet their need for a supportive environment. HCP face a higher risk than other professionals of developing depression and emotional distress related to their work,23 and HCP experiencing personal health challenges may relate to patients’ needs differently, recognizing the necessity of a supportive and friendly environment.
This study had several strengths and limitations. The study was strengthened by the participants’ interdisciplinarity and the fact that all hospital departments were included. This innovative study is the first to describe the association between HCP HL sensitivity, work-related factors (teamwork and staffing), and mental well-being (work engagement, depression, and anxiety). Our study will, therefore, serve as a basis for comparison for future investigations.
One study limitation is that all data were collected at a single time point and at a single hospital, with a relatively low response rate and small sample size. Our cross-sectional design provides a strong snapshot of associations between variables at one moment in time, but we acknowledge its limitation in establishing causation, as it cannot capture temporal relationships or consider potential confounding factors that may influence outcomes. In addition, the relatively low response rate and small sample size from a single hospital may introduce selection bias and limit the transferability of our results to other settings.
Another limitation is that two HL domains from the Norwegian version of the IOHLC questionnaire had Cronbach’s alpha coefficients below 0.7. This may be attributed to considerable variation among the items within those domains. As a result, we recommend interpreting the findings for HL domains 4 and 6 with caution, as the lower reliability scores could indicate limited internal consistency or the presence of heterogeneous constructs.44 Finally, for four of the regression analyses, the amount of explained variance indicated a small effect size. However, five of the equations showed a medium effect size, which has been reported to be good in cross-sectional studies.45
Conclusions
HCP who excel in addressing patients’ HL needs also demonstrate high levels of work engagement. Additionally, teamwork, staffing, and depression show associations with HCP HL sensitivity. Further research is needed to better understand these associations within hospitals and across the broader healthcare spectrum.
Practice Implications
Our findings suggest that healthcare organizations ought to pay more attention to HCP’s wishes when working to improve patients’ HL needs. Organizational interventions should be tested to enhance HL sensitivity in a way that does not negatively impact HCP work-related factors and mental well-being. The intervention should provide HCP with guidance and support to help them effectively meet patients’ and families’ needs for HL follow-up.
Acknowledgments
We want to thank the participating HCP for their valuable contributions.
Funding
The Norwegian Nurses Organisation and Kirsten Rønning Legacy supported this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Health literacy. Available from: https://www.who.int/teams/health-promotion/enhanced-wellbeing/ninth-global-conference/health-literacy.
2. Rajah R, Hassali MAA, Jou LC, Murugiah MK. The perspective of healthcare providers and patients on health literacy: a systematic review of the quantitative and qualitative studies. Perspect Public Health. 2018;138(2):122–132. doi:10.1177/1757913917733775
3. Le C, Finbråten HS, Pettersen KS, Joranger P, Guttersrud Ø. Befolkningens helsekompetanse, del I. The International Health Literacy Population Survey 2019–2021 (HLS19) – et samarbeidsprosjekt med nettverket M-POHL tilknyttet WHO-EHII. Rapport IS-2959. Helsedirektoratet; 2021.
4. World Health Organization. Health promotion. World Health Organization.
5. Sørensen K, Pelikan JM, Röthlin F, et al. Health literacy in Europe: comparative results of the European health literacy survey (HLS-EU). Eur J Public Health. 2015;25(6):1053–1058. doi:10.1093/eurpub/ckv043
6. Volandes AE, Paasche-Orlow MK. Health literacy, health inequality and a just healthcare system. Am J Bioeth. 2007;7(11):5–10. doi:10.1080/15265160701638520
7. Sorensen K, Brand H. Health literacy lost in translations? Introducing the European Health Literacy Glossary. Health Promot Int. 2014;29(4):634–644. doi:10.1093/heapro/dat013
8. Wynia M, Osborn CY. Health literacy and communication quality in health care organizations. J Health Commun. 2010;2. doi:10.1080/10810730.2010.499981
9. Toronto CE. Health literacy competencies for registered nurses: an e-Delphi Study. J Contin Educ Nurs. 2016;47(12):558–565. doi:10.3928/00220124-20161115-09
10. Trezona A, Dodson S, Osborne RH. Development of the Organisational Health Literacy Responsiveness (Org-HLR) self-assessment tool and process. BMC Health Serv Res. 2018;18(1):694. doi:10.1186/s12913-018-3499-6
11. Helseogomsorgsdepartementet. Strategi for å øke helsekompetansen i befolkningen 2019–2023 [Online]. Oslo: Helse-og omsorgsdepartementet; 2019. Available from: https://www.regjeringen.no/contentassets/97bb7d5c2dbf46be91c9df38a4c94183/strategi-helsekompetanse-uu.pdf.
12. Coleman C. Teaching health care professionals about health literacy: a review of the literature. Nurs Outlook. 2011;59(2):70–78. doi:10.1016/j.outlook.2010.12.004
13. Coleman C, Hudson S, Maine L. Health literacy practices and educational competencies for health professionals: a consensus study. J Health Commun. 2013;18:82–102. doi:10.1080/10810730.2013.829538
14. Chang L-C, Chen Y-C, Liao -L-L, Wu FL, Hsieh P-L, Chen H-J. Validation of the instrument of health literacy competencies for Chinese-speaking health professionals. PLoS One. 2017;12(3):e0172859. doi:10.1371/journal.pone.0172859
15. Ocloo J, Garfield S, Franklin BD, Dawson S. Exploring the theory, barriers and enablers for patient and public involvement across health, social care and patient safety: a systematic review of reviews. Health Res Policy Syst. 2021;19(1):8. doi:10.1186/s12961-020-00644-3
16. Salyers MP, Bonfils KA, Luther L, et al. The relationship between professional burnout and quality and safety in healthcare: a meta-analysis. J Gen Intern Med. 2016;32(4):475–482. doi:10.1007/s11606-016-3886-9
17. Stavdal MN, Larsen M, Wahl A, et al. Healthcare personnel experiences with health literacy sensitivity in relation to work satisfaction and stress: a qualitative study. J Multidiscip Healthc. 2025;18:1269–1280. doi:10.2147/JMDH.S493548
18. Demerouti E, Bakker AB, Nachreiner F, Schaufeli WB. The job demands-resources model of burnout. J Appl Psychol. 2001;86(3):499–512. doi:10.1037/0021-9010.86.3.499
19. Schaufeli WB, Bakker AB. Job demands, job resources, and their relationship with burnout and engagement: a multi-sample study. J Organiz Behav. 2004;25(3):293–315. doi:10.1002/job.248
20. Schaufeli WB, Taris TW. A critical review of the job demands-resources model: implications for improving work and health. Dordrecht: Springer Netherlands; 2014:43–68.
21. Rowland J, Hollar D. Promoting health literacy for people with disabilities and clinicians through a teamwork model. J Fam Strengths. 2015;15. doi:10.58464/2168-670X.1286
22. Carthon JM, Hatfield L, Plover C, et al. Association of nurse engagement and nurse staffing on patient safety. J Nurs Care Qual. 2019;34(1):40–46. (In English). doi:10.1097/ncq.0000000000000334
23. Fiabane E, Giorgi I, Sguazzin C, Argentero P. Work engagement and occupational stress in nurses and other healthcare workers: the role of organisational and personal factors. J Clin Nurs. 2013;22(17–18):2614–2624. doi:10.1111/jocn.12084
24. Thapa DR, Subedi M, Ekström-Bergström A, Areskoug Josefsson K, Krettek A. Facilitators for and barriers to nurses’ work-related health-a qualitative study. BMC Nurs. 2022;21(1):1–218. doi:10.1186/s12912-022-01003-z
25. Flowers S-LDA, Guillén-Solà M, Sansó N, Galiana L. Compassionate care: a qualitative exploration of nurses’ inner resources in the face of burnout. Nurs Rep. 2024;14(1):66–77. doi:10.3390/nursrep14010006
26. Aiken LH, Sermeus W, McKee M, et al. Physician and nurse well-being, patient safety and recommendations for interventions: cross-sectional survey in hospitals in six European countries. BMJ Open. 2024;14(2):e079931. doi:10.1136/bmjopen-2023-079931
27. Karlsson AC, Gunningberg L, Bäckström J, Pöder U. Registered nurses’ perspectives of work satisfaction, patient safety and intention to stay – a double‐edged sword. J Nurs Manag. 2019;27(7):1359–1365. doi:10.1111/jonm.12816
28. Wang KY, Chou CC, Lai JCY. A structural model of total quality management, work values, job satisfaction and patient‐safety‐culture attitude among nurses. J Nurs Manag. 2019;27(2):225–232. doi:10.1111/jonm.12669
29. von Elm ED, Altman DGP, Egger MP, Pocock SJP, Gøtzsche PCMD, Vandenbroucke JPP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
30. Sermeus W, Aiken LH, Ball J, et al. A workplace organisational intervention to improve hospital nurses’ and physicians’ mental health: study protocol for the Magnet4Europe wait list cluster randomised controlled trial. BMJ Open. 2022;12(7):e059159. doi:10.1136/bmjopen-2021-059159
31. Borge CR, Wahl AK, Larsen MH, Andersen MH, Stavdal MN, Hermansen Å. Validation of the Health Literacy Competencies (IOHLC) instrument in Norwegian interdisciplinary health care professionals in specialist health care service [Manuscript submitted for publication]. J Interprof Educ Pract. 2025.
32. Lake ET, Gil J, Moronski L, McHugh MD, Aiken LH, Lasater KB. Validation of a short form of the practice environment scale of the nursing work index: the PES‐5. Res Nurs Health. 2024;47(4):450–459. doi:10.1002/nur.22388
33. Schaufeli W, Shimazu A, Hakanen J, Salanova M, De Witte H. An ultra-short measure for work engagement: the UWES-3 validation across five countries. Eur J Psychol Assess. 2017;35:1–15. doi:10.1027/1015-5759/a000430
34. Kroenke K, Spitzer RL, Williams JB, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Internal Med. 2007;146(5):317–325. doi:10.7326/003-4819-146-5-200703060-00004
35. Kroenke K, Spitzer RL, Williams JB. The Patient Health Questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284–1292. (In English). doi:10.1097/01.Mlr.0000093487.78664.3c
36. Mindrila D, Balentyne P. Scatterplots and correlation. Based on Chapter 4 of the basic practice of statistics (6th ed.). Available from: https://www.westga.edu/academics/research/vrc/assets/docs/scatterplots_and_correlation_notes.pdf.
37. Gravetter FJ, Wallnau LB. Statistics for the Behavioral Sciences. Wadsworth, CA: Cengage Lerning; 2013.
38. García-Sierra R, Fernández-Castro J, Martínez-Zaragoza F. Relationship between job demand and burnout in nurses: does it depend on work engagement? J Nurs Manag. 2016;24(6):780–788. (In English). doi:10.1111/jonm.12382
39. Moreno-Martínez M, Sánchez-Martínez I. The associated factors of work engagement, work overload, work satisfaction, and emotional exhaustion and their effect on healthcare workers: a cross-sectional study. Healthcare. 2025;13(2):162. doi:10.3390/healthcare13020162
40. Bakker AB, Demerouti E, Chen PY. Job demands–resources theory: taking stock and looking forward. J Occup Health Psychol. 2017;22(3):273–285. doi:10.1037/ocp0000056
41. Mijakoski D, Karadzhinska-Bislimovska J, Stoleski S, Minov J, Atanasovska A, Bihorac E. Job demands, burnout, and teamwork in healthcare professionals working in a general hospital that was analysed at two points in time. Open Access Maced J Med Sci. 2018;6(4):723–729. doi:10.3889/oamjms.2018.159
42. World Health Organization. Health workforce. Available from: https://www.who.int/health-topics/health-workforce#tab=tab_1.
43. Cho SH, Lee JY, You SJ, Song KJ, Hong KJ. Nurse staffing, nurses prioritization, missed care, quality of nursing care, and nurse outcomes. Int J Nurs Pract. 2020;26(1):e12803–n/a. doi:10.1111/ijn.12803
44. Tavakol M, Dennick R. Making sense of Cronbach’s alpha. Int J Med Educ. 2011;2:53–55. doi:10.5116/ijme.4dfb.8dfd
45. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Updating Factors Influencing Nurse Work Engagement in the Hospital Settings: A Systematic Review
Aungsuroch Y, Gunawan J, Juanamasta IG, Montayre J
Journal of Healthcare Leadership 2024, 16:157-176
Published Date: 20 March 2024