Back to Journals » International Journal of Women's Health » Volume 18
Associations Among Parental Rearing Patterns, Psychological Resilience and Coping Styles in Adolescent Females with Endometriosis
Authors Zhang W, Ma D, Yang X, Gu Z ![]() , Yang H
, Yang H
Received 30 March 2026
Accepted for publication 18 June 2026
Published 3 July 2026 Volume 2026:18 613267
DOI https://doi.org/10.2147/IJWH.S613267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Wei Zhang1,*, Di Ma1,*, Xu Yang1, Zhihui Gu 2, Hong Yang1
1Department of Gynaecology and Obstetrics, General Hospital of the Northern Theater Command, Shenyang, People’s Republic of China; 2Department of Social Medicine, School of Health Management, China Medical University, Shenyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong Yang, Email [email protected]
Purpose: Adolescent endometriosis (EMs) imposes substantial physical and psychological burdens on young female patients, and adaptive coping strategies are vital for their health management. This study aimed to explore the latent classes of parental rearing patterns and coping styles among adolescent females with endometriosis, and examine the interrelationships between parental rearing, psychological resilience and coping styles. The findings intend to provide theoretical evidence and practical references for mental health intervention and public health services targeting this vulnerable group.
Methods: This cross-sectional study consecutively recruited participants from 2024 to 2026 at a tertiary Class A hospital in Shenyang. A total of 168 adolescents aged 12– 20 years were enrolled via convenience sampling. Parental Rearing Patterns Scale, the Resilience Scale, and the Coping Styles Scale were used to collect relevant data. Latent class analysis (LCA) was adopted to classify parental rearing patterns and coping styles. Independent samples t-test, one-way ANOVA and bias-corrected Bootstrap mediation analysis (5,000 resamples) were further performed for statistical testing.
Results: LCA identified two parenting subtypes (31.5% positive-empowering, 68.5% high-pressure restrictive) and three coping subtypes (58.9% active problem-solving, 28.0% passive-avoidant, 13.1% social support-seeking). Psychological resilience differed significantly across parenting patterns and coping styles (P< 0.05). Mediation analysis revealed that high-pressure restrictive parenting was negatively associated with psychological resilience, and resilience was correlated with coping styles (P< 0.05). The indirect effect was 0.295 (P< 0.05), and the direct effect was non-significant. As this was a cross-sectional study, the findings only indicate statistical indirect associations rather than causal mediation.
Conclusion: Different parenting styles and coping patterns lead to varied psychological and clinical outcomes. Positive-empowering parenting and active coping facilitate patients’ psychological adjustment and disease management. By contrast, high-pressure restrictive parenting, avoidant coping and low willingness to seek help tend to trigger negative emotions, reduce treatment adherence and delay intervention. Parenting styles affect coping behaviors partly through psychological resilience. Targeted improvement of psychological resilience can effectively enhance patients’ ability to cope with the disease.
Keywords: adolescent endometriosis, parental rearing patterns, psychological resilience, coping styles, mediation effect
Introduction
Endometriosis (EMs) is caused by the ectopic growth of endometrial tissues, which commonly leads to pelvic pain, dysmenorrhea, infertility and other symptoms, seriously impairing women’s reproductive health.1 It was previously believed that EMs predominantly affects women of childbearing age, yet its incidence among adolescents has long been underestimated.2 More than 60% of adult patients develop typical symptoms before the age of 20.3 A study including 1011 adolescents with chronic pelvic pain reported that 64% of the participants were diagnosed with EMs, and the disease can even occur in girls prior to menarche.4,5 The main clinical manifestations of adolescent EMs include pelvic pain and dysmenorrhea, accompanied by irregular menstruation, urinary discomfort, as well as gastrointestinal symptoms such as diarrhea and constipation.6 As a chronic disease unique to women, patients with EMs frequently experience neglected pain, misunderstanding and lack of trust during medical treatment. These adversities not only aggravate physical and mental distress, but also reduce their willingness to seek medical care and impair mental health.7,8 Influenced by conventional perceptions, patients and their families tend to regard pain as a normal phenomenon of adolescence, resulting in delayed diagnosis.9 Since the disease involves sensitive issues related to reproductive health, adolescent patients are prone to develop gender-related stigma.10 They may therefore conceal their condition and avoid social interaction, which further triggers social anxiety, body image disturbance and other problems, creating a vicious cycle between physical symptoms and poor social adaptation.11
Disease coping styles vary distinctly among patients with endometriosis, and coping strategies are closely correlated with physical and mental health status. Actively seeking support from family and peers and voluntarily disclosing one’s condition can effectively reduce stigma and enhance self-esteem. Accepting the disease and proactively acquiring relevant disease knowledge are also significantly positively correlated with a higher quality of life.12 In contrast, catastrophic thinking, excessive focus on physical discomfort and avoidant coping substantially reduce patients’ quality of life.13,14 Studies on adolescent patients in Europe and America have also confirmed that those who adopt cognitive restructuring, mindfulness regulation and other strategies experience milder pain and better recovery of social functions. By comparison, adolescents trapped in long-term avoidance and self-blame are at a remarkably higher risk of anxiety and depression.15,16 Communicating with fellow patients and obtaining emotional support serves as a vital way for adolescents to relieve negative emotions and build self-identity.17 Online and offline patient communities can disseminate disease knowledge, provide emotional companionship and alleviate loneliness; nevertheless, excessive engagement in online social interaction may exacerbate anxiety.18 Collectively, positive coping patterns relieve negative emotions and improve quality of life, whereas negative coping exacerbates psychological stress.
Against the backdrop of collectivist culture and traditional family values in China, adolescents’ behaviors and mental states are susceptible to family attitudes.19 Additionally, adolescents are more reluctant to take the initiative to confide in elders when facing gynecological diseases involving privacy. Parental parenting concepts and emotional attitudes shape adolescents’ disease cognition, psychological resilience and coping styles. Accordingly, family factors play an even more critical role among adolescent EMs patients in China.20,21 Multiple studies conducted in Europe and America have indicated that family interaction patterns and overall family functioning profoundly affect the mental health and medical-seeking behaviors of adolescents. Dysfunctional family interactions exacerbate psychological problems such as alexithymia and impair individuals’ psychological adjustment capacity.22 Moreover, the quality and operational status of the family environment are associated with health-related quality of life among adolescents. Parents’ psychological status and family functioning also directly affect parent-adolescent engagement, and further influence adolescents’ compliance with medical and psychological services as well as their medical choices.23 Sound family functioning and a supportive family environment are essential safeguards for maintaining adolescents’ mental health and encouraging them to actively seek and cooperate with medical treatment.24
Affected by the disease, adolescents experience a notable decline in psychological endurance and stress resistance, and frequently present with self-denial and social withdrawal, which may induce a range of psychological problems.25 A cohort study including 11,238 young women verified that EMs patients had a considerably higher risk of moderate to severe psychological problems within one year before and after disease onset compared with healthy individuals.26 Long-term psychological stress further reduces their willingness to seek help.27 As a chronic inflammatory disease, endometriosis acts as a major psychological stressor during adolescence. Some patients are able to mobilize internal and external resources to regulate physical and mental states and confront the disease and treatment with a positive mindset.28 This adaptive capacity in adversity is defined as psychological resilience, which refers to individuals’ comprehensive ability to conduct self-regulation and achieve positive adaptation by virtue of personal cognition, skills and internal and external resources when encountering stress and difficulties.29 Relevant studies in Hong Kong, China have shown that adolescents with higher levels of psychological resilience tend to adopt more active help-seeking behaviors.30
Theoretical Basis and Model Selection
The Rutter Developmental Model is a classic theory for explaining the formation mechanism of resilience.31 It posits that individuals’ adaptation to adversity is determined by the dynamic interplay between risk factors and protective factors, rather than a single factor.29 When protective factors prevail, they can effectively offset the adverse impacts of risks and help individuals maintain sound psychological adaptation under stress. The Family Systems Theory suggests that the family microenvironment profoundly shapes individual behavioral patterns.32 As a core environmental variable in adolescents’ socialization, parenting styles mold their stress response patterns through emotional support and behavioral regulation. According to the resilience theory, external environmental support does not exert direct effects on individual behaviors. Instead, it enhances internal resilience-a protective psychological resource-which reshapes individuals’ cognitive appraisal of stressors, and ultimately influences their coping strategies and adaptation outcomes. This study aims to explore the internal mechanism through which parenting styles affect disease adaptation among adolescent patients with EMs, and thus adopts the mediation model for empirical analysis. In contrast to the moderation model (which only tests moderating effects) and the bidirectional correlation model (which merely verifies correlations without clarifying causal pathways), the mediation model can clearly delineate the progressive relationships among independent, mediating and dependent variables, and accurately reveal the underlying mechanisms, making it well-suited for this research. Based on existing theories and previous empirical evidence, parenting styles, as a distal environmental factor, cannot directly affect the disease adaptation and mental status of adolescent EMs patients. Its influences operate sequentially through individuals’ internal psychological resources and behavioral strategies. Accordingly, this study employs a full mediation model to fit the pathways of variable effects, so as to verify the core hypothesis that environmental factors affect disease adaptation entirely via the psychological-behavioral pathways of individuals.
Research Hypotheses
H1: Parenting styles are associated with psychological resilience among adolescent patients with EMs. H2: Psychological resilience is associated with disease coping behaviors among adolescent patients with EMs. H3: The effect of parenting styles on disease coping behaviors of adolescent patients with EMs is mainly realized through the indirect pathway of psychological resilience, namely the pathway of parenting styles→psychological resilience→disease coping behaviors.
Methods
Study Subjects
This cross-sectional study continuously recruited adolescent patients with endometriosis from a tertiary Grade A hospital in Shenyang from 2024 to 2026 as the research subjects. The sample size of this study was determined based on the empirical rule for multivariate statistical analysis. Generally, the sample size should be 5 to 10 times the number of independent variables. With an additional 20% reserved to account for invalid questionnaires and participant dropouts, the initial target sample size was set at 100 to 200 cases. To further improve model stability and statistical power, we continuously enrolled eligible participants. A total of 192 questionnaires were distributed and 181 were retrieved. After excluding questionnaires with patterned responses, excessive missing data and inconsistent answers, 168 valid samples were obtained, yielding an overall valid response rate of 87.5%. Participants were recruited consecutively. Uniformly trained investigators initially screened patients attending the gynecological outpatient department in accordance with the inclusion and exclusion criteria. Eligible patients and their guardians were fully informed of the research objectives, survey content, questionnaire completion time, data usage and confidentiality principles. Questionnaires were administered after obtaining written informed consent from patients and their families. During the recruitment period, 217 suspected cases were screened in total. Among them, 195 met the enrollment criteria, and 192 voluntarily participated in the study. Three patients declined participation due to time constraints, and no passive dropout occurred.
The inclusion criteria were: (1) age between 12 and 20 years (consistent with WHO and national definitions of adolescence); (2) diagnosis of endometriosis confirmed by surgery and histopathology; (3) ability to communicate independently and complete the questionnaires; (4) awareness of their own medical condition; and (5) absence of psychiatric disorders or cognitive impairment. The exclusion criteria were: (1) presence of other severe organic diseases or malignant tumors; and (2) current participation in other psychological intervention studies.
Research Instruments
General Information Questionnaire
A self-designed form was used to collect demographic characteristics (age, only-child status), family background (monthly household income, parental education level), and disease-related cognition (eg, prior exposure to sexual health education).
Ways of Coping Questionnaire
The Ways of Coping Questionnaire was developed by Xiao Jihua33 et al in the early 1990s to construct an assessment tool for coping strategies suitable for the Chinese cultural context. Based on Lazarus and Folkman’s transactional theory of stress and coping, the questionnaire also incorporates characteristics of Chinese collectivist culture, such as an emphasis on interpersonal relationships and family support, achieving the localization of the theoretical framework. The questionnaire consists of 62 items, divided into six subscales: Problem-Solving, Self-Blame, Seeking Help, Fantasy, Avoidance, and Rationalization. Each subscale reflects a typical coping tendency when an individual faces stress. The questionnaire uses a “Yes/No” dichotomous scoring system, with higher scores on each subscale indicating a greater tendency to adopt that coping style. The scale has demonstrated good reliability and validity in domestic research and is widely used in the fields of mental health and stress research. The Cronbach’s alpha for each dimension is greater than 0.7.
Parenting Style Questionnaire
The Parenting Style Questionnaire was developed by Gong Yihua34 based on Diana Baumrind’s theoretical framework of parenting styles, combined with characteristics of Chinese family culture and parent-child interactions. This questionnaire aims to systematically assess the emotional attitudes, behavioral patterns, and interactive styles exhibited by parents in the process of raising children. The scale includes multiple dimensions, mainly covering Emotional Warmth, Authoritarian Control, Indulgence, Neglect, and Democratic Encouragement, comprehensively encompassing common parenting types in Chinese families. The questionnaire uses a Likert 5-point scoring method (1= “Very Inconsistent”, 5= “Very Consistent”), with higher scores indicating more pronounced characteristics in that dimension. This tool has demonstrated good applicability and psychometric properties in research on Chinese family education and child psychological development. The Cronbach’s alpha for each dimension is greater than 0.7.
Connor-Davidson Resilience Scale-10 (CD-RISC-10)
The Connor-Davidson Resilience Scale-10 (CD-RISC-10) was developed by Campbell-Sills et al35 as a simplified version of the Connor-Davidson Resilience Scale, designed for the rapid assessment of an individual’s psychological adaptation and recovery capacity in the face of adversity, stress, and trauma. The scale consists of 10 items covering core components of resilience such as Tenacity, Strength, and Optimism. It uses a Likert 5-point scoring system (1 = “Never”, 5 = “Almost Always”), with total scores ranging from 10 to 50. Higher scores indicate better levels of psychological resilience. Due to its concise items and ease of administration, the CD-RISC-10 is widely used in clinical, community, and general population research and has been validated in multiple cross-cultural studies for good reliability and validity. The Cronbach’s alpha for scale is greater than 0.8.
Statistical Analysis
Data Preprocessing and Missing Data Management
The unified dataset was imported into SPSS 26.0 for standardized data cleaning. Given the missing completely at random of questionnaire items, mean imputation was used when the missing proportion was less than 10%. Questionnaires with a missing proportion of 10% or above were eliminated. The above strategies reduce the bias caused by missing data and guarantee data quality.
Selection Criteria for Latent Class Analysis
Latent Class Analysis (LCA) was performed using Mplus 8.3 to identify population subgroups based on the core variables of parenting styles and coping styles. According to family systems theory and resilience theory, parenting styles act as distal environmental variables for adolescents’ illness adaptation, while coping styles represent core individual psychological and behavioral responses. Significant individual heterogeneity exists in these two variables, making LCA an appropriate approach to explore subgroup characteristics. This study focused on classifying participants by combined patterns of parenting styles and coping styles, which can accurately reveal psychological and behavioral differences among patients and align with the research objective of population stratification.
Starting with the one-class model, we gradually increased the number of latent classes and fitted models with 1 to 5 classes sequentially. The optimal classification was determined comprehensively based on multiple indicators.The model fit was evaluated using the following criteria: (1) Information criteria: Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and Sample-Size Adjusted BIC (aBIC), where lower values indicate better model fit; (2) Classification quality: Entropy values, where values closer to 1 indicate more precise classification (typically > 0.80 is considered ideal);36 (3) Model comparison tests: The Lo-Mendell-Rubin Likelihood Ratio Test (LMR-LRT) and the Bootstrap Likelihood Ratio Test (BLRT), where P<0.05 indicates that the k-class model is significantly superior to the (k−1)-class model.37 Model parsimony and clinical interpretability were also taken into account to determine the final optimal number of classes and avoid overfitting.
A total of 168 adolescents with endometriosis (EMs) were ultimately enrolled in this study. Although the sample size did not meet the criteria for large-sample epidemiological investigations, adolescent EMs is a rare and highly insidious disease with limited clinical recruitment accessibility and scarce cases, which is consistent with the sample characteristics of surveys targeting rare diseases. Multiple domestic and international latent class analysis (LCA) and latent profile analysis (LPA) studies on rare diseases and chronic gynecological conditions among adolescents have reported that exploratory subgroup analyses of this type generally adopted sample sizes ranging from 113 to 200. Small samples within this range have been widely proven feasible and capable of yielding stable results.38–42 Accordingly, the sample size of 168 participants is appropriate for this exploratory study. It can support the identification of heterogeneous subgroups among adolescents with EMs, and the findings are of statistical and clinical reference value.
Mediation Effect Analysis
Bias-corrected nonparametric percentile Bootstrap method implemented in SPSS 26.0 was adopted to test all mediation effects. The resampling was set for 5,000 iterations, and the 95% confidence intervals (CIs) for all path coefficients were calculated. The mediation effect was judged based on whether the 95% CI of the indirect effect contained zero. An indirect effect was considered statistically significant if its 95% CI did not include zero. The specific criteria were as follows: A full mediation effect was identified when the indirect effect was significant while the direct effect was non-significant; A partial mediation effect was determined when both the indirect and direct effects were significant. For cases with a significant indirect effect but a non-significant total effect, the results were interpreted based on the suppression (masking) effect theory. In multiple mediation or complex path models, indirect paths with opposite directions may counteract one another, resulting in a non-significant total effect close to zero, whereas individual mediation paths can remain independently significant. Methodological studies have confirmed that a significant total effect is not a prerequisite for a valid mediation effect, and the core criterion for mediation testing lies in the significance of the indirect effect (a×b). Accordingly, this study did not take a significant total effect as the precondition for establishing mediation paths. This approach is consistent with the mainstream analytical paradigm for mediation analysis.43,44 Previous studies have suggested that full mediation constitutes the strongest evidence for a mediation effect.45 Differentiating between full and partial mediation offers a qualitative description of the effect size within mediation models and facilitates the interpretation of results.46
Two-tailed tests were adopted throughout the analyses at α=0.05. All analyses met model assumptions of normality, independence, homogeneity of variance and linearity. Latent variable analyses satisfied requirements for model fit, residual independence and sample homogeneity. Quantitative data were described as mean ± standard deviation (M±SD), while categorical data were expressed as frequencies and percentages (%). Independent samples t-tests and one-way analysis of variance (ANOVA) were conducted to explore differences in resilience scores across different demographic and clinical characteristic groups.
Results
Latent Class Model Selection for Coping Styles and Parental Rearing Patterns
To determine the optimal number of latent classes for coping styles and parental rearing patterns, models ranging from 1–5 classes were estimated and compared (Table 1). As the number of latent classes increased, the information criteria—AIC,BIC, and aBIC—consistently exhibited a downward trend for both variables.
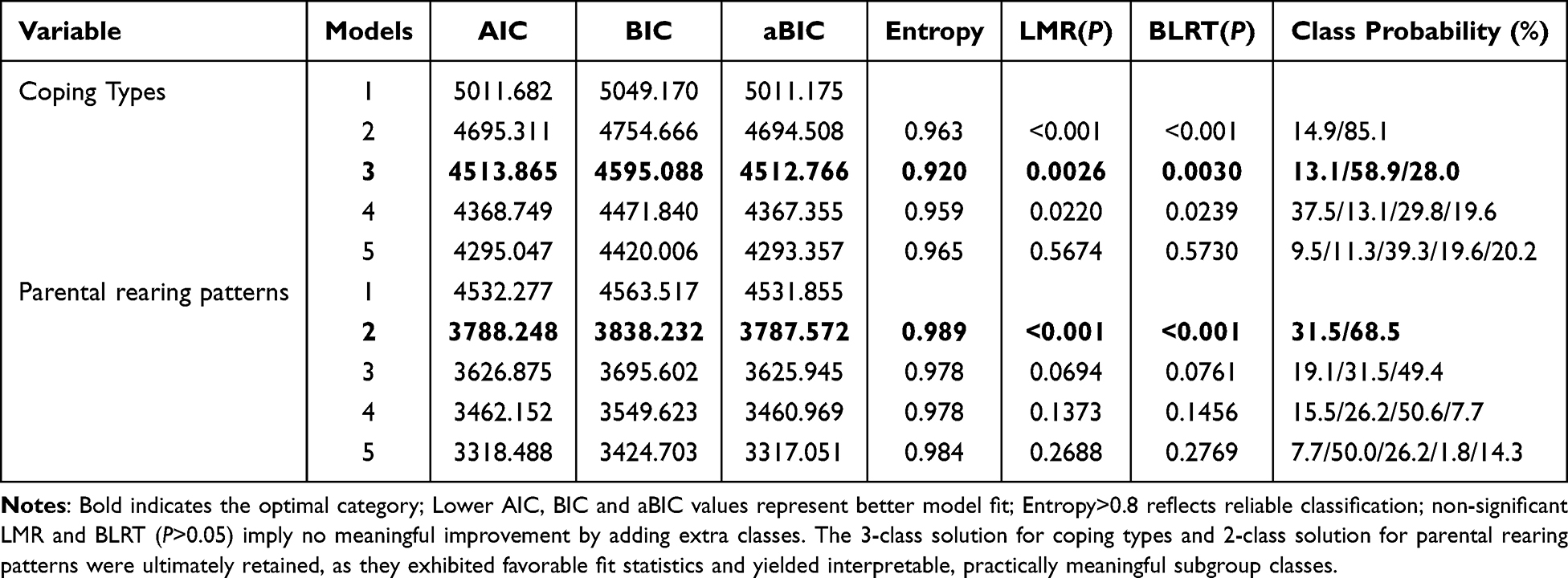 |
Table 1 Fit Indices of Latent Class Models for Coping Styles and Parental Rearing Patterns |
Model Selection for Coping Styles
The LMR and the BLRT indicated that the three-class model provided a significantly better fit than the two-class model (LMR P=0.0026, BLRT P=0.0030). Although the 4-class model also reached statistical significance (P<0.05), the LMR and BLRT values for the 5-class model were no longer significant (P>0.05), indicating that extracting a fifth class did not significantly improve the goodness-of-fit. Furthermore, the 3-class model yielded an entropy value of 0.920, which is well above the acceptable threshold of 0.80, demonstrating excellent classification accuracy. The latent class proportions were well-distributed (13.1%, 58.9%, and 28.0%), avoiding any overly small or conceptually meaningless classes. Considering both statistical significance and model parsimony, the 3-class model offered the best balance of adequate fit and interpretability, and was thus retained as the final model for coping styles.
Model Selection for Parental Rearing Patterns
The LMR and BLRT were utilized as critical indicators to determine the optimal number of classes. The results revealed that the 2-class model was significantly superior to the 1-class model, with both P-values being highly significant (P<0.001). However, when a 3-class model was estimated, the P-values for the LMR and BLRT were 0.0694 and 0.0761, respectively (both P>0.05), failing to reach statistical significance. This suggests that adding a third class did not yield a statistically significant improvement in model fit. The 2-class model demonstrated outstanding classification precision, with an entropy value of 0.989 (approaching 1.0). Additionally, the class probabilities for the 2-class model were well-balanced at 31.5% and 68.5%, providing practical significance for the research.
Characteristics of Coping Types Latent Classes
Based on the latent class analysis illustrated in the figure, three distinct coping profiles were identified (Figure 1): Active Problem-Solving Type (58.9%), Passive-Avoidant Type (28.0%), and Social Support-Seeking Type (13.1%). The Active Problem-Solving Type, which constituted the largest proportion of the sample, was characterized by the highest scores in problem-solving and relatively lower scores in avoidance-related strategies such as fantasy, self-blame, and withdrawal. In contrast, the Passive-Avoidant Type exhibited elevated scores across avoidance-oriented strategies (fantasy, rationalization, self-blame, and withdrawal), with moderate engagement in problem-solving and help-seeking. The Social Support-Seeking Type, representing the smallest subgroup, showed a distinct pattern of higher scores in help-seeking behaviors, while maintaining lower levels across other coping dimensions. These findings highlight the heterogeneity of coping strategies within the population, with the majority adopting an active problem-solving approach, while a substantial proportion relied on passive-avoidant strategies, and a minority primarily sought social support.
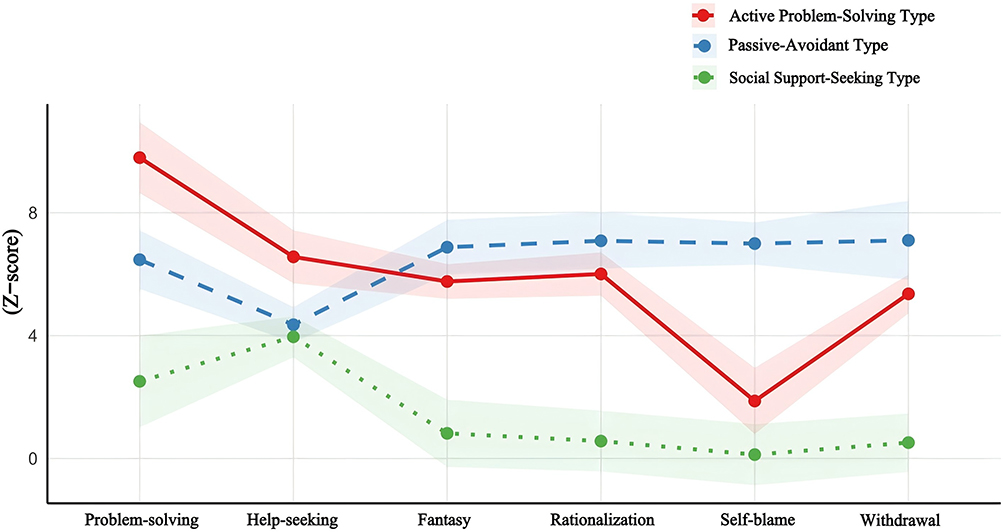 |
Figure 1 Characteristics of Coping Types Latent Classes. Notes: Classes were grouped by dimensional score patterns. The Active Problem-Solving Type had the highest problem-solving scores and low scores on avoidant tactics (fantasy, self-blame, withdrawal); the Passive-Avoidant Type scored highly across all avoidant strategies with moderate problem-solving and help-seeking scores; the Social Support-Seeking Type scored highest on help-seeking. |
Characteristics of Parenting Latent Classes
Latent class analysis identified two distinct parenting profiles (Figure 2): Positive-Empowering Parenting (31.5%) and High-Pressure Restrictive Parenting (68.5%). The Positive-Empowering Parenting group was characterized by higher scores in trust-encouraging and emotionally warm parenting, and lower scores in authoritarian, indulgent, and neglectful parenting. In contrast, the High-Pressure Restrictive Parenting group exhibited higher levels of authoritarian and neglectful parenting, but lower levels of trust-encouraging and emotionally warm parenting. Notably, the majority of the sample (68.5%) fell into the High-Pressure Restrictive Parenting category, while only 31.5% were classified as Positive-Empowering Parenting. These findings highlight a predominance of restrictive and high-pressure parenting styles within the sample, with a smaller proportion experiencing more positive and empowering parental approaches.
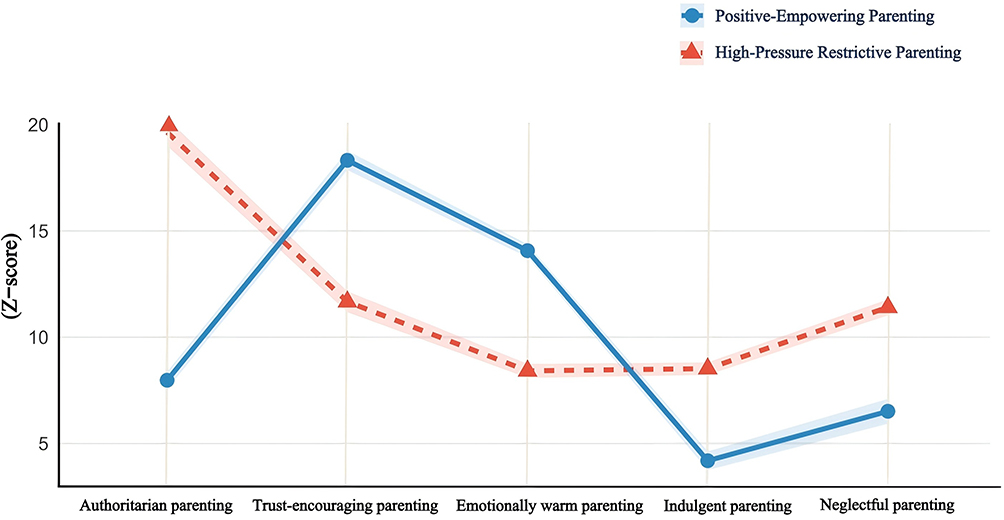 |
Figure 2 Characteristics of Parenting Latent Classes. Notes: Groups were divided by dimensional score patterns. Positive-Empowering Parenting: High scores on trust-encouraging and emotional warmth, low scores on authoritarian, indulgent and neglectful parenting; High-Pressure Restrictive Parenting: High authoritarian/neglectful scores, markedly low trust-encouraging and emotional warmth scores. |
Univariate Analysis of Factors Influencing Coping Styles
The results of the univariate analysis (Table 2) indicated significant differences in the selection of coping styles among individuals with varying demographic characteristics and family backgrounds. Significant differences in coping styles were observed across different educational stages (χ2=14.629, P=0.006). Specifically, high school students exhibited the highest proportion of “active problem-solving” (26.2%), whereas college students had the lowest proportion of “social support-seeking” (0%). Furthermore, being an only daughter had a highly significant impact on coping styles (χ2=23.756, P<0.001); only daughters were more inclined to adopt “active problem-solving” (47.0%), while non-only daughters showed a higher proportion of “social support-seeking” (9.5%) compared to only daughters (3.6%).
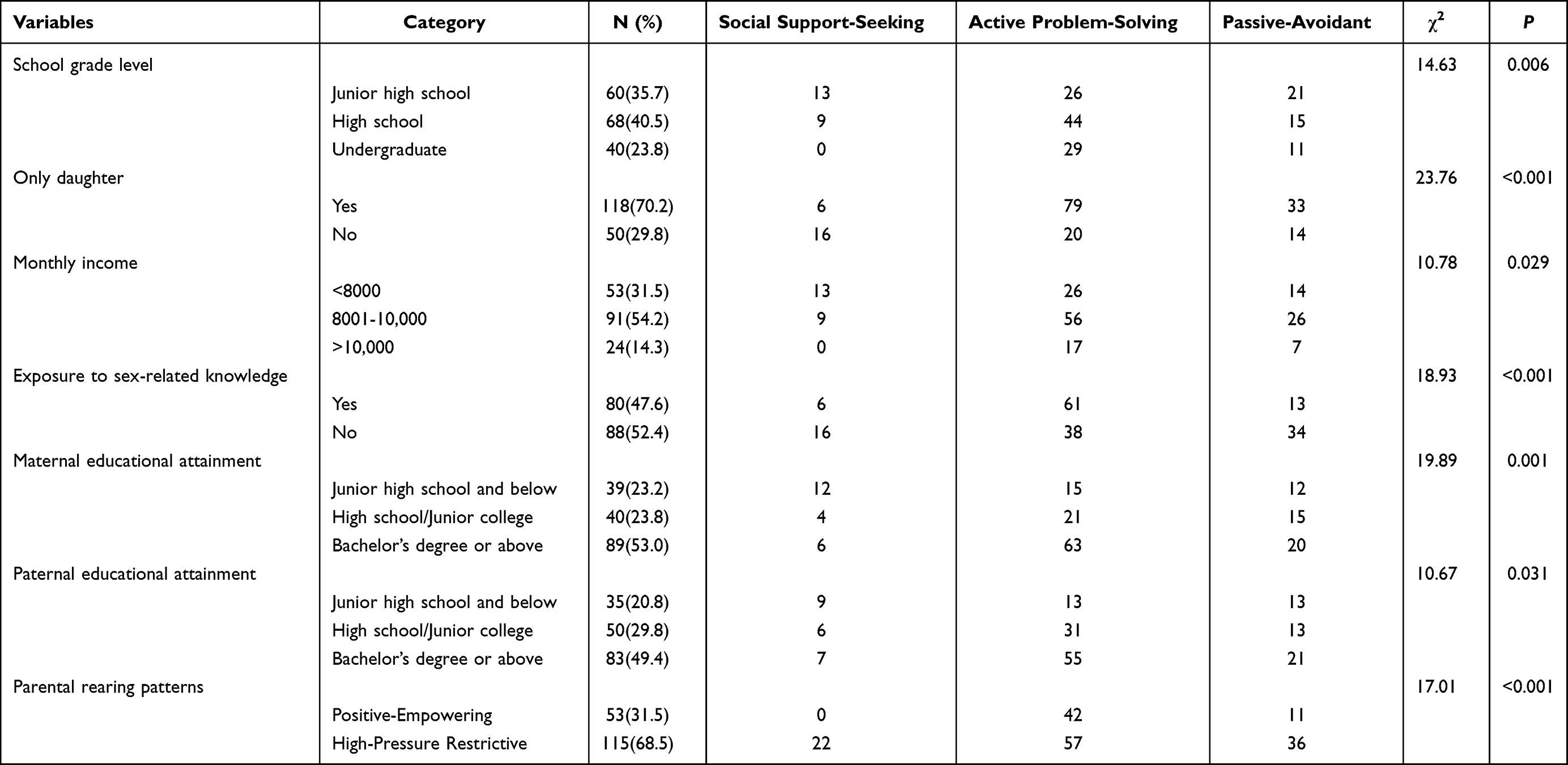 |
Table 2 Univariate Analysis of Coping Types Among Individuals with Different Demographic and Family Characteristics |
Monthly family income also significantly influenced coping strategies (χ2=10.776, P=0.029), with individuals from middle-income families (8,001–10,000 RMB) demonstrating a higher proportion of positive coping. Regarding exposure to sex-related knowledge, highly significant differences in coping styles were found between those who had been exposed to such knowledge and those who had not (χ2=18.934, P<0.001). Individuals with prior exposure were more prone to “active problem-solving” (36.3%), whereas those without exposure adopted “negative avoidance” at a significantly higher rate (20.2%) than their exposed counterparts (7.7%).
Both maternal and paternal educational levels exerted a significant impact on coping styles. Higher maternal education was associated with a greater likelihood of adopting “active problem-solving” (37.5% in the bachelor’s degree or higher group; χ2=19.885, P=0.001). The influence of paternal education was similarly significant (χ2=10.670, P=0.031), with individuals whose fathers had higher educational attainment being more inclined toward positive coping.
Finally, a highly significant association was identified between parental rearing patterns and coping styles (χ2=17.006, P<0.001). Under the “positive-empowering” parenting style, no individuals opted for “social support-seeking,” while a notable proportion (25.0%) utilized “active problem-solving.” In contrast, individuals subjected to a “high-pressure restrictive” parenting style exhibited a significantly higher proportion of “negative avoidance” (21.4%) compared to the positive-empowering group (6.5%).
Correlation Analysis Between Variables
In this study, a correlation matrix analysis was conducted to examine the relationships among coping styles (problem-solving, help-seeking, fantasy, rationalization, self-blame, and withdrawal), various parenting styles (authoritarian, trust-encouraging, emotionally warm, indulgent, and neglectful), and psychological resilience (Figure 3). The results indicated that positive coping styles, such as problem-solving and help-seeking, were significantly and positively correlated with trust-encouraging and emotionally warm parenting styles (r>0.4, P<0.05), suggesting that positive parenting styles facilitate the development of positive coping strategies in adolescents. Conversely, negative coping styles, such as self-blame and withdrawal, exhibited significant positive correlations with authoritarian and neglectful parenting styles (r>0.4, P<0.05), while showing significant negative correlations with trust-encouraging and emotionally warm parenting styles (r<-0.4, P<0.05). This indicates that negative parenting styles may increase the risk of adolescents adopting negative coping strategies.
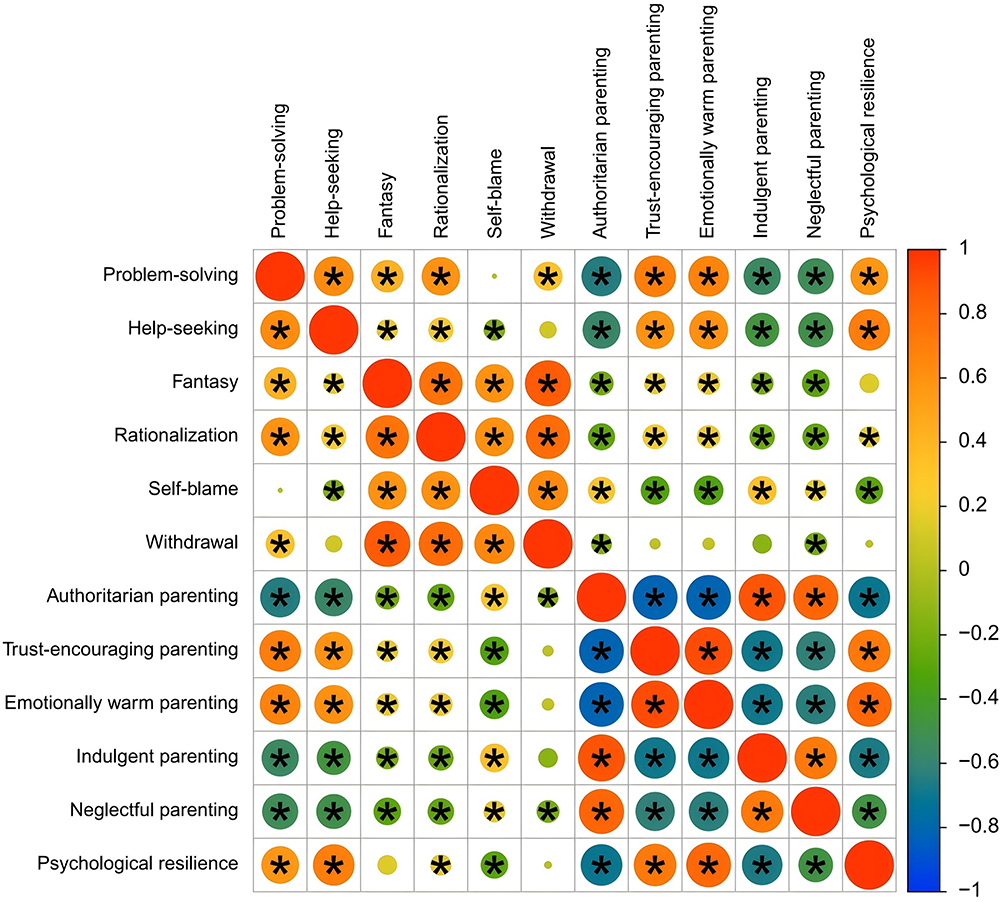 |
Figure 3 Correlation heatmap of coping styles, parenting styles, and psychological resilience. Notes: Red indicates positive correlation, blue indicates negative correlation. *P<0.05. |
Furthermore, psychological resilience was significantly and positively correlated with positive coping styles like problem-solving and help-seeking (r≈0.4~0.6, P<0.05), and significantly and negatively correlated with negative coping styles like self-blame and withdrawal (r≈-0.4~-0.6, P<0.05). Additionally, psychological resilience demonstrated significant positive correlations with trust-encouraging and emotionally warm parenting styles, and significant negative correlations with authoritarian and neglectful parenting styles.
In summary, positive parenting styles not only help adolescents develop positive coping strategies but also significantly enhance their psychological resilience. Conversely, negative parenting styles are closely associated with the adoption of negative coping strategies and lower levels of psychological resilience.
Analysis of the Impact of Parental Rearing Patterns and Coping Types on Resilience
Results of the independent samples t-test (Table 3) indicated that parental rearing patterns exerted a highly significant influence on individuals’ resilience levels (t=13.635, P<0.001). Specifically, individuals under the “Positive-Empowering” rearing pattern exhibited significantly higher resilience scores (44.13±7.79) compared to those under the “High-Pressure Restrictive” pattern (27.45±7.17). Furthermore, one-way analysis of variance (ANOVA) revealed significant differences in resilience scores across different coping types (F=7.592, P=0.001). Post-hoc comparisons further demonstrated that individuals with the “Active Problem-Solving” type achieved the highest resilience scores (35.21±10.18), which were significantly greater than those of the “Social Support-Seeking” (27.32±6.74) and “Passive-Avoidant” (29.98±11.77) groups.
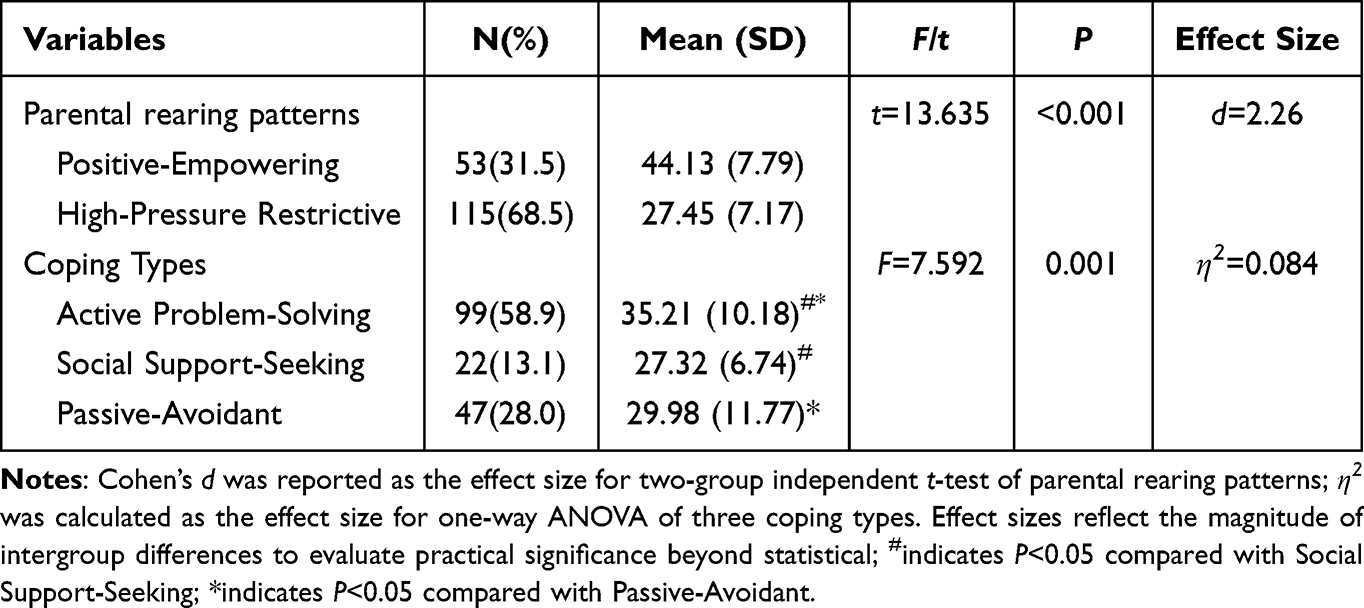 |
Table 3 Comparison of Resilience Across Different Parental Rearing Patterns and Coping Types |
Testing the Mediating Role of Psychological Resilience
The Bootstrap method was applied to examine the mediating role of psychological resilience (Table 4 and Figure 4). Path a (independent variable→mediator): High-pressure restrictive rearing was significantly negatively correlated with psychological resilience (β=−0.666, t=−7.58, P<0.001). Path b (mediator→dependent variable): After adjusting for the effect of rearing patterns, psychological resilience was significantly negatively correlated with illness coping styles (β=−0.185, t=−2.11, P= 0.040). The indirect effect of psychological resilience was 0.123 (SE=0.148). The 95% Bootstrap confidence interval (CI) was [0.005, 0.585]. The CI did not contain zero (P<0.05) demonstrating that the mediating effect of psychological resilience was statistically significant. After the mediator was included, the direct effect of high-pressure restrictive rearing on coping styles was not statistically significant (β=0.007, P=0.958), with a 95% CI of [−0.589, 0.621] which contained zero. These findings were interpreted based on the suppression effect. A significant total effect is not a prerequisite for a valid mediating effect. The significant indirect effect alongside the non-significant direct effect indicates that the association between high-pressure restrictive rearing and coping styles operates entirely through psychological resilience.
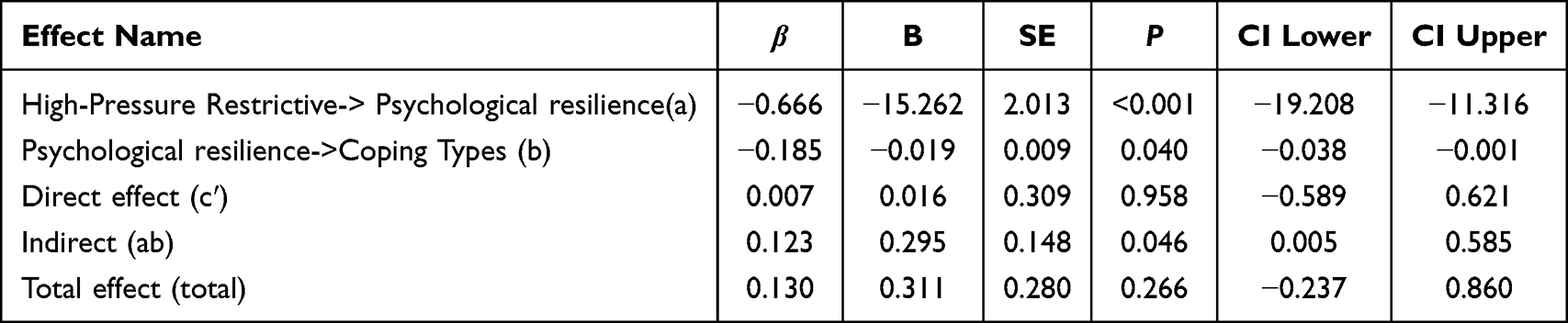 |
Table 4 Mediation Analysis of Psychological Resilience Between High-Pressure Restrictive Rearing and Coping Types |
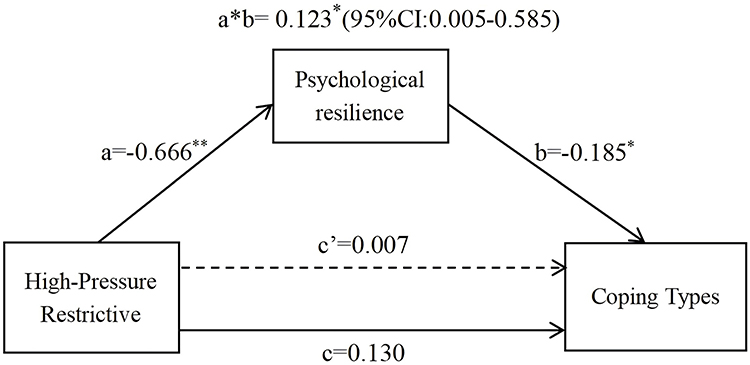 |
Figure 4 Path model for the mediating effect of psychological resilience. Notes: All path coefficients are standardized values; a: path coefficient from high-pressure restrictive parenting to psychological resilience; b: path coefficient from psychological resilience to coping types;c:total effect of high-pressure restrictive parenting on coping types; c′:direct effect of high-pressure restrictive parenting on coping types (controlling for psychological resilience); a*b: indirect effect via psychological resilience; **indicates P<0.01;*indicates P<0.05. |
Discussion
Current Status of Parenting Styles: Dominance of High-Pressure Restrictive Parenting in the Studied Sample
LCA identified two distinct parenting style profiles among families of the participating adolescents: positive-empowering (31.5%) and high-pressure restrictive (68.5%). In the present sample, parenting characterized by authoritarian control, emotional neglect, and high parental pressure was predominant, while parenting featuring emotional warmth, trust, and encouragement was less common. These descriptive findings suggest that excessive behavioral control and insufficient emotional support are prevalent in some families of adolescent patients in this study. The relatively high proportion of high-pressure restrictive parenting observed in the current sample reflects unique sample characteristics and contextual cultural features compared with previous domestic studies. Ren and Chen47 reported that warm-involved parenting accounted for 49.1% and rejecting-involved parenting for only 11.3% among Chinese adolescents. From a cultural perspective, Wang48 illustrated that Confucian collectivist cultural values and strong social emphasis on academic achievement may encourage Chinese parents to adopt more authoritarian and high-pressure disciplinary strategies, which may be associated with adolescents’ over-adaptive behaviors to meet external expectations. The high prevalence (68.5%) of the high-pressure restrictive profile in this study further supports the view that parents in similar social and academic contexts tend to adopt controlling parenting approaches rather than supportive and empowering parenting practices.
Current Status of Coping Styles: Prevalent Active Problem-Solving and Limited Social Support Utilization
Under the pressure related to illness, adolescents exhibit individual differences in their coping strategies towards illness.58.9% of participants predominantly adopted active problem-solving coping, indicating that most adolescents attempted to manage illness-related challenges through proactive engagement. Meanwhile, 28.0% of the adolescents exhibited negative avoidance coping, which may correspond to emotional suppression and psychological disengagement among this subgroup. Of note, only 13.1% of participants reported active social support-seeking. This observational result may be attributable to the private nature of endometriosis, potential disease-related stigma, and suboptimal family support functioning, which may limit adolescents’ willingness to seek external help from peers or professional institutions during illness. The typology of coping styles identified in this study is largely consistent with existing international evidence on adolescent coping. Global crisis-focused studies have documented that family connection, peer interaction, outdoor activity, and reasonable internet use are common and effective coping resources for children and adolescents.49,50 Youths with chronic somatic illnesses, such as celiac disease, also commonly employ proactive problem-solving and planning strategies to adapt to disease restrictions.51 Nevertheless, negative coping patterns are frequently observed among clinical adolescent populations. Suzer Gamli et al52 found elevated avoidant coping and impaired emotional regulation among adolescents with obsessive–compulsive disorder. Similarly, adolescents undergoing chronic disease management often report anxiety and persistent self-doubt as common negative coping manifestations.51 The present findings further indicate that negative coping tendencies are non-negligible among adolescents exposed to adverse family contexts, which highlights an important target for future adolescent mental health intervention research.
Associations Between Parenting Styles and Adolescent Coping Strategies
This study identified a significant association between parenting styles and coping strategy patterns among adolescents (P < 0.001). Specifically, adolescents in the positive-empowering parenting profile tended to adopt active problem-solving coping strategies, while those in the high-pressure restrictive parenting group were more likely to report negative avoidance coping. Consistent with existing evidence, family ecological factors are closely linked to adolescents’ coping patterns. Previous studies have well-documented that socioecological contexts, especially family communication modes and interpersonal roles, are correlated with adolescents’ cognitive appraisals and coping responses during disease adaptation.51 Global research conducted during the pandemic further indicated that family support serves as a primary protective resource for adolescent coping.50 In addition, appropriate family involvement, rather than excessive overprotection, has been recognized as an important factor supporting autonomous disease management among adolescents with chronic illnesses.53
In the current cross-sectional sample, adolescents exposed to high-pressure restrictive parenting tended to utilize more negative coping responses, including avoidance, self-blame, and withdrawal, and reported relatively lower levels of psychological resilience. Notably, 68.5% of participants in this study were categorized into the high-pressure restrictive parenting subgroup. This parenting pattern, characterized by high control and emotional neglect, may limit adolescents’ opportunities for independent problem-solving and trial-and-error learning. Individuals experiencing such family environments may have fewer internal psychological resources and limited external support, which could be accompanied by a higher tendency toward avoidant and self-blaming coping in stressful situations. These observations are consistent with prior empirical findings regarding adverse parenting styles. Longitudinal evidence has suggested that negative parenting characteristics are correlated with increased emotional and behavioral problems, including disordered eating and depressive symptoms.54 Authoritarian and permissive parenting have also been linked to higher rates of maladaptive behaviors such as internet addiction among youth.55 Excessive parental pressure and restriction may constrain adolescents’ independent development and correlate with maladaptive emotion regulation when facing interpersonal or environmental conflicts.54 In this study, none of the adolescents in the high-pressure restrictive group reported social support-seeking coping. This finding implies that parenting characterized by high control and emotional neglect may be associated with reduced willingness and ability to seek external support, potentially making adolescents more vulnerable to feelings of isolation and helplessness when encountering disease-related stressors.
The Role of Psychological Resilience Between High-Pressure Restrictive Parenting and Illness Coping Styles
The association between high-pressure restrictive family environments and adolescents’ illness coping patterns is not direct, and is largely linked through individuals’ internal psychological resources. High-pressure restrictive parenting correlates with lower psychological resilience among adolescents, and reduced resilience is further associated with maladaptive coping styles such as negative avoidance. Observations from the present sample indicate that high-pressure restrictive parenting is linked to poorer psychological resilience in adolescents, which is consistent with findings from domestic and international studies on family environments and resilience. Existing research has shown that authoritarian and rejecting parenting styles are closely correlated with decreased resilience in children and adolescents.56,57 From a neurocognitive and developmental perspective, excessive parental control may heighten individuals’ sensitivity to negative events and weaken their psychological adaptability.58 Rigid parental expectations and coercive control can also hinder the development of psychological plasticity and the capacity to cope with adversity.59 For adolescents with endometriosis, chronic family pressure combined with physical and psychological distress caused by the disease limits their capacity to adjust to stress, depletes internal psychological defense resources, and is associated with reduced psychological resilience.60
This study suggests that psychological resilience acts as a key intermediate variable connecting parenting characteristics and adolescents’ illness coping styles. As documented in previous literature, psychological resilience is a stable adaptive psychological resource across all developmental stages and correlates closely with individual coping tendencies.61–63 Adolescents with higher resilience tend to adopt active problem-solving strategies when faced with adversity,64,65 while those with low resilience are more likely to engage in negative and emotion-oriented coping.66 Coping actively with endometriosis demands substantial cognitive and emotional resources. In this sample, high-pressure restrictive parenting is associated with the depletion of psychological resources. Adolescents with insufficient resilience therefore tend to choose negative avoidance, a coping pattern that requires fewer psychological resources. The mediating pathway identified in this study differs from those reported in some previous studies, reflecting the unique clinical characteristics of adolescents with endometriosis. Prior research has commonly reported that psychological resilience mainly serves as a buffer or moderator between parental educational anxiety and adolescents’ mental health and negative coping behaviors,67,68 while some studies have identified partial mediating effects of resilience.57 Such discrepancies may be attributed to differences in the nature and intensity of stressors across studies. Parental educational anxiety discussed in earlier studies generally represents a persistent negative emotional atmosphere within the family, which adolescents with strong resilience can mitigate by mobilizing internal psychological resources.67 In contrast, the high-pressure restrictive parenting examined in this study is a long-term stressor characterized by persistent behavioral control and emotional deprivation. According to the Conservation of Resources theory, prolonged authoritarian parenting continuously erodes adolescents’ psychological coping resources. For adolescents living with chronic endometriosis, adverse family environments no longer serve a protective role and instead become a major source of stress. Under cumulative stress, variations in psychological resilience largely explain the association between parenting styles and illness coping patterns. Psychological resilience constitutes a core pathway linking high-pressure restrictive parenting to maladaptive coping among these adolescents. These findings provide clear implications for psychological interventions targeting adolescents with endometriosis. Since long-established high-pressure restrictive parenting patterns are difficult to change in the short term, clinical interventions may focus on improving psychological resilience. Approaches including cognitive behavioral therapy, mindfulness training, and the development of social support from schools and peers can effectively enhance adolescents’ psychological resilience and adaptive capacity.69,70 Even when adolescents remain in high-pressure family settings, improved internal resilience can alleviate the adverse impacts of unfavorable parenting, encourage the adoption of positive coping strategies amid disease-related challenges, and reduce negative avoidance and other maladaptive behaviors.
It should be noted that there are multiple alternative explanations for the associations among parenting styles, psychological resilience and illness coping styles observed in this study. Adolescents’ stress coping patterns and psychological adaptation are shaped by multiple factors, rather than family rearing environment alone. Apart from the core variables included in this research, a number of unmeasured confounding factors may interfere with the relationships between the study variables. Specifically, family socioeconomic status and parental educational attainment can indirectly affect adolescents’ psychological resilience and illness coping behaviors by influencing parenting concepts, parent-adolescent interaction quality and family stress atmosphere.71 Meanwhile, the severity and fluctuating symptoms of endometriosis directly affect patients’ physical and mental burden and adaptation status, and may alter their stress coping tendencies.72 In addition, other psychological traits not assessed in this study, such as negative cognitive bias, emotion regulation ability and illness acceptance, may also serve as potential psychological confounders and account for individual differences in adolescents’ coping styles. Therefore, the observed associations between variables cannot fully rule out the combined effects of other confounding pathways. The present findings only support the existence of correlations rather than definitive or exclusive causal mechanisms.
Limitations
This study redirects endometriosis-related psychosocial research to vulnerable adolescents, highlights the roles of family dynamics and psychological resources, and advances social psychological studies on adolescent chronic diseases and women’s health. Nevertheless, several notable limitations of the present study should be acknowledged. First, as a cross-sectional observational study, this work can only demonstrate correlations rather than clarify the temporal sequence and causal relationships between variables. Without longitudinal follow-up data, the causal directions of associations and the causal pathways underlying the mediating effect cannot be rigorously verified. Accordingly, the results of the mediation model merely reflect correlational pathways and should not be overinterpreted as definitive causal effects. Second, participants were recruited via convenience sampling from a single medical center. The homogeneous sample with restricted regional and cultural backgrounds, together with the relatively small sample size, limits the generalizability of the findings. Third, all core variables were measured using self-report questionnaires, which are susceptible to response biases such as recall bias and may interfere with the observed associations between variables. Fourth, several potential confounding factors, including family socioeconomic status, parental educational attainment, disease severity and other unmeasured psychological variables, were not included and controlled for in the analysis. Hence, alternative explanations for the observed relationships remain possible, and the influence of other underlying mechanisms cannot be fully ruled out. Future research should adopt a multicenter, large-sample longitudinal design with rigorous control of confounding variables. Longitudinal data can help clarify the temporal order of variables and further validate the mediating mechanism linking parenting styles, psychological resilience and illness coping styles, so as to generate more robust and widely applicable conclusions.
Conclusion
This study reveals that high-pressure restrictive parenting may undermine adolescents’ psychological resilience and subsequently lead to maladaptive coping styles. Clinically, psychological resilience can be set as a core intervention target. Considering the low willingness to seek help and the high prevalence of avoidant coping among the participants, medical institutions may launch specialized services: provide stress management and professional psychological counseling for patients to correct negative coping patterns. In view of the finding that high-pressure parenting accounts for 68.5% in this sample, targeted parenting guidance shall be delivered to family caregivers to improve inappropriate parenting practices. These dual measures help enhance patients’ psychological resilience and ability to cope with the disease. In the field of public health, family parenting guidance should be integrated into the routine health management of adolescents with chronic gynecological diseases as soon as possible. Local health authorities may leverage the maternal and child health service system to formulate standardized health education programs, offer personalized parenting support to families of adolescent patients with endometriosis, and promote positive and empowering parenting styles. This strategy can also be applied to adolescent females with other chronic illnesses to advance overall women’s health management. Due to traditional cultural norms, uneven distribution of medical resources across regions, the private nature of the disease and widespread disease-related stigma, the implementation effect of interventions varies from area to area. Relevant measures should be adjusted flexibly and implemented gradually in light of local conditions.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due the data also forms part of an ongoing study but are available from the corresponding author on reasonable request.
Ethical Approval
The study design was approved by the Committee on Human Experimentation of China Medical University (2024-BS-032). All methods were carried out in accordance with Declaration of Helsinki. An informed consent was scanned and signed by each participant before participating. For individuals younger than the age of 16, written consent was obtained from their parents or legal guardians. Personal privacy was protected when handling personal data, and we kept individual records completely secret.
Acknowledgments
The authors would like to thank all the researches and medical staff, who helped to obtain the written informed consent about the conduct of this survey and to interview or help explain the questionnaires, and thank all the participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by 2024 Liaoning Provincial Natural Science Foundation Program (Doctoral Research Initiation Project): Provincial Doctoral Research Initiation Fund Program (Project Number: 2024-BS-032). Funded person: Zhihui Gu. Project Name: Machine Learning-Based Prediction of Healthcare-Seeking Behavior among Adolescents with Endometriosis.
Disclosure
The authors reported no conflicts of interest in this work.
References
1. Lu J, Ling X, Liu L. et al. Emerging hallmarks of endometriosis metabolism: a promising target for the treatment of endometriosis. Biochim Biophys Acta Mol Cell Res. 2023;1870(1):119381. doi:10.1016/j.bbamcr.2022.119381
2. Khashchenko EP, Uvarova EV, Fatkhudinov TK, et al. Endometriosis in adolescents: diagnostics, clinical and laparoscopic features. J Clin Med. 2023;12(4):1678. doi:10.3390/jcm12041678
3. Liakopoulou MK, Tsarna E, Eleftheriades A, et al. Medical and behavioral aspects of adolescent endometriosis: a review of the literature. Children. 2022;9(3):384. doi:10.3390/children9030384
4. Hirsch M, Dhillon-Smith R, Cutner AS, et al. The prevalence of endometriosis in adolescents with pelvic pain: a systematic review. J Pediatr Adolesc Gynecol. 2020;33(6):623–18. doi:10.1016/j.jpag.2020.07.011
5. Lu MY, Niu JL, Liu B. The risk of endometriosis by early menarche is recently increased: a meta-analysis of literature published from 2000 to 2020. Arch Gynecol Obstet. 2023;307(1):59–69. doi:10.1007/s00404-022-06541-0
6. Viscardi MF, Piacenti I, Musella A, et al. Endometriosis in adolescents: a closer look at the pain characteristics and atypical symptoms: a prospective cohort study. J Clin Med. 2025;14(4):1392. doi:10.3390/jcm14041392
7. Wren G, Mercer J. Dismissal, distrust, and dismay: a phenomenological exploration of young women’s diagnostic experiences with endometriosis and subsequent support. J Health Psychol. 2022;27(11):2549–2565. doi:10.1177/13591053211059387
8. Katz C, Evans S, Mikocka-Walus A. ‘Listen to women as if they were your most cherished person’: Australian women’s perspectives on living with the pain of endometriosis: a mixed-methods study. J Health Psychol. 2025;30(8):1899–1914. doi:10.1177/13591053241250101
9. Panvino F, Paparella R, Pisani F, et al. Endometriosis in adolescence: a narrative review of the psychological and clinical implications. Diagnostics. 2025;15(5):548. doi:10.3390/diagnostics15050548
10. Reinhardt A, Eitze S. Breaking the endometriosis silence: a social norm approach to reducing menstrual stigma and policy resistance among young adults. Psychol Health. 2025;40(6):881–903. doi:10.1080/08870446.2023.2277838
11. Facchin F, Vercellini P, Somigliana E. The impact of endometriosis on educational and professional pathways: a cross-sectional online study. BMC Psychol. 2026;14(1):303. doi:10.1186/s40359-026-04112-5
12. Bień A, Pokropska A, Grzesik-Gąsior J, et al. Quality of life in women with endometriosis: the importance of socio-demographic, diagnostic-therapeutic, and psychological factors. J Clin Med. 2025;14(12):4268. doi:10.3390/jcm14124268
13. Spinoni M, Capano AU, Porpora MG, et al. Understanding the psychological factors linking pelvic pain and health-related quality of life in endometriosis: the influence of illness representations and coping strategies. Am J Obstet Gynecol. 2025;233(1):
14. Moore C, Cogan N, Williams L. A mixed-methods investigation of coping, adaptation and health-related quality of life in individuals experiencing endometriosis. Psychol Health. 2026;1–21. doi:10.1080/08870446.2026.2650778
15. González-Echevarría AM, Rosario E, Acevedo S, et al. Impact of coping strategies on quality of life of adolescents and young women with endometriosis. J Psychosom Obstet Gynaecol. 2019;40(2):138–145. doi:10.1080/0167482X.2018.1450384
16. Zarbo C, Santona A, Parolin L, et al. Stopping suffering: an exploration of suicidal ideation and its clinical, cognitive and relational correlates among women with a diagnosis of endometriosis. J Affect Disord. 2025;391:119964. doi:10.1016/j.jad.2025.119964
17. Gstoettner M, Wenzl R, Radler I, et al. “I think to myself ‘why now?’” - a qualitative study about endometriosis and pain in Austria. BMC Womens Health. 2023;23(1):409. doi:10.1186/s12905-023-02576-w
18. Loughran A, Daken K, Plessis CD, et al. how women with endometriosis use social media for support and self-management: an analysis of reddit content. Int J Environ Res Public Health. 2025;22(11):1706. doi:10.3390/ijerph22111706
19. Wang L, Xian Y, Dill SE, et al. Parenting style and the cognitive development of preschool-aged children: evidence from rural China. J Exp Child Psychol. 2022;223:105490. doi:10.1016/j.jecp.2022.105490
20. Dong Y. “Premature” girls with “illegitimate” diseases: a qualitative exploration of the stigma of gynecological diseases for unmarried Young Women in China. J Health Commun. 2023;28(2):111–120. doi:10.1080/10810730.2023.2185322
21. Xie QW, Fan XL, Sun Y, et al. The impact of neighborhood environment on adolescent anxiety and depression: a moderated mediation model involving screen time and family function. J Affect Disord. 2025;389:119751. doi:10.1016/j.jad.2025.119751
22. Coci C, Provenzi L, De Giorgis V, et al. Family dysfunctional interactive patterns and alexithymia in adolescent patients with restrictive eating disorders. Children. 2022;9(7):1038. doi:10.3390/children9071038
23. Roberts E, Zelikovsky N. Family environment, social support, and health-related quality of life in adolescents following kidney transplant. Pediatr Transplant. 2024;28(5):e14824. doi:10.1111/petr.14824
24. Wirehag Nordh EL, Grip K, Axberg U. The patient and the family: investigating parental mental health problems, family functioning, and parent involvement in child and adolescent mental health services (CAMHS). Eur Child Adolesc Psychiatry. 2025;34(7):2023–2034. doi:10.1007/s00787-024-02607-3
25. Berkelbach van der Sprenkel EE, van der Laan SEI, Finkenauer C, et al. Chronic conditions and adolescents’ psychosocial wellbeing: the impact of self-reporting. Eur J Pediatr. 2025;185(1):15. doi:10.1007/s00431-025-06616-5
26. Rowlands IJ, Teede H, Lucke J, et al. Young women’s psychological distress after a diagnosis of polycystic ovary syndrome or endometriosis. Hum Reprod. 2016;31(9):2072–2081. doi:10.1093/humrep/dew174
27. Ando S, Nishida A, Usami S, et al. Help-seeking intention for depression in early adolescents: associated factors and sex differences. J Affect Disord. 2018;238:359–365. doi:10.1016/j.jad.2018.05.077
28. Lubián-López DM, Moya-Bejarano D, Butrón-Hinojo CA, et al. Measuring Resilience in Women with Endometriosis. J Clin Med. 2021;10(24):5942. doi:10.3390/jcm10245942
29. Rutter M. Resilience as a dynamic concept. Dev Psychopathol. 2012;24(2):335–344. doi:10.1017/S0954579412000028
30. Sum MY, Chan SKW, Tsui HKH, et al. Stigma towards mental illness, resilience, and help-seeking behaviours in undergraduate students in Hong Kong. Early Interv Psychiatry. 2024;18(3):181–189. doi:10.1111/eip.13455
31. Rutter M. Psychosocial resilience and protective mechanisms. Am J Orthopsychiatry. 1987;57(3):316–331. doi:10.1111/j.1939-0025.1987.tb03541.x
32. Miller EA, Elder CR. Balanced parenting: proposing a differentiation-based parenting approach informed by Bowen family systems theory. Fam Process. 2025;64(1):e13092. doi:10.1111/famp.13092
33. Xiao JH, Xu XF. A study on the reliability and validity of the Coping Style Questionnaire. Chin Mental Health J. 1996;10(4):164–168.2.
34. Gong YH. Preliminary Development of the Parental Rearing Style Questionnaire. Southwest University; 2005.
35. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-davidson Resilience Scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019–1028. doi:10.1002/jts.20271
36. Liu Q, Charleston MA, Richards SA, Holland BR. Performance of akaike information criterion and bayesian information criterion in selecting partition models and mixture models. Syst Biol. 2023;72(1):92–105. doi:10.1093/sysbio/syac081
37. Kim SY. Determining the number of latent classes in single- and multi-phase growth mixture models. Struct Equation Model. 2014;21(2):263–279. doi:10.1080/10705511.2014.882690
38. Zhang H, Wei X, Liu W, et al. Latent class analysis identifies distinct pain phenotypes in newly diagnosed systemic juvenile idiopathic arthritis. Arthritis Res Ther. 2025;27(1):71. doi:10.1186/s13075-025-03534-7
39. Han HQ, Song JX, Han WP, et al. Latent profile analysis of flourishing in patients undergoing chemotherapy after ovarian cancer surgery: a single-center study in Shanxi. Cancer Manag Res. 2025;17:3025–3038. doi:10.2147/CMAR.S549590
40. Hammer MJ, Cooper BA, Chen LM, et al. Identification of distinct symptom profiles in patients with gynecologic cancers using a pre-specified symptom cluster. Support Care Cancer. 2023;31(8):485. doi:10.1007/s00520-023-07954-6
41. Fidler DJ, Prince MA, Van Deusen K, et al. Latent profiles of autism symptoms in children and adolescents with Down syndrome. J Intellect Disabil Res. 2022;66(3):265–281. doi:10.1111/jir.12910
42. Åkerblom S, Peppler Jönsson I, Ringqvist Å, et al. Identifying and characterizing clinical subgroups in individuals with endometriosis. Front Pain Res. 2025;6:1610109. doi:10.3389/fpain.2025.1610109
43. MacKinnon DP, Krull JL, Lockwood CM. Equivalence of the mediation, confounding and suppression effect. Prev Sci. 2000;1(4):173–181. doi:10.1023/a:1026595011371
44. Shrout PE, Bolger N. Mediation in experimental and nonexperimental studies: new procedures and recommendations. Psychol Methods. 2002;7(4):422–445.
45. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. doi:10.1037//0022-3514.51.6.1173
46. Preacher KJ, Kelley K. Effect size measures for mediation models: quantitative strategies for communicating indirect effects. Psychol Methods. 2011;16(2):93–115. doi:10.1037/a0022658
47. Ren Y, Chen H. The integrative influence of parental involvement and parenting style on adolescent psychological adjustment. Child Psychiatry Hum Dev. 2025;26. doi:10.1007/s10578-025-01887-3
48. Wang X. Parenting style on the over-adaptation of secondary school students: a moderated mediation model of self-esteem and gender. BMC Psychol. 2025;13(1):1136. doi:10.1186/s40359-025-03481-7
49. Solmi M, Thompson T, Cortese S, et al. Collaborative outcomes study on health and functioning during infection times (COH-FIT): global and risk-group stratified course of well-being and mental health during the COVID-19 pandemic in adolescents. J Am Acad Child Adolesc Psychiatry. 2025;64(4):499–519. doi:10.1016/j.jaac.2024.07.932
50. Agorastos A, Thompson T, Solmi M, et al. Mental health, coping and related risk factors during the first 2 years of the COVID-19 pandemic in children: nationally representative, multi-wave, cross-sectional results from 12 countries from the global COH-FIT study. Eur Neuropsychopharmacol. 2026;104:112741. doi:10.1016/j.euroneuro.2025.112741
51. Maddison-Roberts H, Jones C, Satherley RM. Gluten-free diet management and well-being in children with celiac disease: a qualitative study. Pediatr Allergy Immunol. 2025;36(3):e70061. doi:10.1111/pai.70061
52. Suzer Gamli I, Kacar A, Eyupoglu N, et al. Emotion regulation, coping, and alexithymia in adolescents with obsessive-compulsive disorder: a mediational analysis. Clin Psychol Psychother. 2025;32(3):e70083. doi:10.1002/cpp.70083
53. Roques MA, Rosso-Delsemme N, Celli A, et al. Navigating the transition from adolescence to adulthood among young people with severe haemophilia: the qualitative phase of the TRANSHEMO project. Haemophilia. 2025;31(6):1197–1208. doi:10.1111/hae.70101
54. Wu R, Huang Y, Shao L, et al. Negative parenting style and depressive symptoms among college students: a longitudinal moderated mediation model involving eating disorders, ethnicity and maladaptive cognitive emotion regulation strategies. BMC Psychology. 2025;13(1):371. doi:10.1186/s40359-025-02693-1
55. Liu SW, Chen S, Huang C, et al. Parenting style and child internet addiction in China: mediation effect of parental active meditation. Int J Environ Res Public Health. 2025;22(4):461. doi:10.3390/ijerph22040461
56. Zhang L, Xia Y, Zhu S, et al. The impact of family socioeconomic status on preschoolers’ anxiety: the serial mediation effects of parenting style and psychological resilience in preschoolers. Behav Sci. 2025;15(11):1443. doi:10.3390/bs15111443
57. Wang J, Huang X, Li Z, et al. Effect of parenting style on the emotional and behavioral problems among Chinese adolescents: the mediating effect of resilience. BMC Public Health. 2024;24(1):787. doi:10.1186/s12889-024-18167-9
58. Ding X, Zheng L, Liu Y, et al. Parenting styles and psychological resilience: the mediating role of error monitoring. Biol Psychol. 2023;180:108587. doi:10.1016/j.biopsycho.2023.108587
59. Feldman R. Father contribution to human resilience. Dev Psychopathol. 2023;35(5):2402–2419. doi:10.1017/S0954579423000354
60. Ou W, Yang Y, Chen Y, et al. Bridge symptoms between parenting styles and proximal psychological risk factors associated with adolescent suicidal thoughts: a network analysis. Child Adolesc Psychiatr Ment Health. 2023;17(1):129. doi:10.1186/s13034-023-00674-z
61. Taylor MG, Bruefach T, Carr DC. Measuring psychological resilience in aging: findings from the health and retirement study and national longitudinal study of adolescent to adult health. Innov Aging. 2024;8(3):igae013. doi:10.1093/geroni/igae013
62. Silveira S, Hecht M, Matthaeus H, et al. Coping with the COVID-19 pandemic: perceived changes in psychological vulnerability, resilience and social cohesion before, during and after lockdown. Int J Environ Res Public Health. 2022;19(6):3290. doi:10.3390/ijerph19063290
63. Yang M, Guo K, Liu W, et al. Coping tendency as a mediator in the relationship between psychological resilience and health problems among college students. Psychol Res Behav Manag. 2024;17:2619–2630. doi:10.2147/PRBM.S466150
64. Nowakowski K, Wróbel K. Psychopathic traits, psychological resilience and coping with stress in socially maladjusted youth. Psychiatr Pol. 2021;55(5):1157–1167. doi:10.12740/PP/OnlineFirst/118139
65. Beames JR, Li SH, Newby JM, et al. The upside: coping and psychological resilience in Australian adolescents during the COVID-19 pandemic. Child Adolesc Psychiatr Ment Health. 2021;15(1):77. doi:10.1186/s13034-021-00432-z
66. Ma A, Yang Y, Guo S, et al. Adolescent resilience and mobile phone addiction in Henan Province of China: impacts of chain mediating, coping style. PLoS One. 2022;17(12):e0278182. doi:10.1371/journal.pone.0278182
67. Lu Y, Zhao H, Zhu X, et al. How parental educational anxiety fuels adolescent depression: the mediating chain of moral disengagement and negative coping, and the buffering role of psychological resilience. BMC Psychol. 2025;13(1):1370. doi:10.1186/s40359-025-03718-5
68. Qiu Z, Guo Y, Wang J, et al. Associations of parenting style and resilience with depression and anxiety symptoms in Chinese Middle School Students. Front Psychol. 2022;13:897339. doi:10.3389/fpsyg.2022.897339
69. Chen M, Chen X, Jiang H, et al. Parent-adolescent family resilience and psychological adjustment in chronically ill adolescents: an actor-partner interdependence mediation model. J Adv Nurs. 2025;81(4):1864–1874. doi:10.1111/jan.16377
70. Li Y, Ren Y, Du Z, et al. Competitive pressure, psychological resilience, and coping strategies in athletes’ pre-competition anxiety. Sci Rep. 2025;15(1):35467. doi:10.1038/s41598-025-19213-1
71. Conger RD, Donnellan MB. An interactionist perspective on the socioeconomic context of human development. Annu Rev Psychol. 2007;58:175–199. doi:10.1146/annurev.psych.58.110405.085551
72. Osaki JD, Oliveira MAP. What is behind? Impact of pelvic pain on perceived stress and inflammatory markers in women with deep endometriosis. J Clin Med. 2024;13(10):2927. doi:10.3390/jcm13102927
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Mediating Effect of Perceived Social Support and Medical Coping Modes Between Psychological Resilience and Meaning in Life in COVID-19 Patients
Zhang L, Jiang M, Wang L, Zheng J, Wang W
Patient Preference and Adherence 2023, 17:571-582
Published Date: 7 March 2023