Back to Journals » Clinical Interventions in Aging » Volume 21
Association Rule Analysis of Cognitive Frailty Subtypes in Community-Dwelling Older Adults
Authors Liang S, Lai X, Chen H, Wang Q, Huo X
Received 22 October 2025
Accepted for publication 26 January 2026
Published 6 February 2026 Volume 2026:21 574258
DOI https://doi.org/10.2147/CIA.S574258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Shicong Liang,1 Xiaoxing Lai,2 Hongshuang Chen,3 Qingchi Wang,3 Xiaopeng Huo3
1School of Nursing, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Neurology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 3Nursing Department, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China
Correspondence: Xiaopeng Huo, Nursing Department, Peking Union Medical College Hospital, Beijing, People’s Republic of China, Email [email protected]
Purpose: In order to provide a foundation for identification and intervention strategies, this study intends to investigate the influencing factors and associative patterns of two subtypes of reversible cognitive frailty (RCF) and potential reversible cognitive frailty (PRCF) in older adults with cognitive frailty (CF) who live in the community.
Patients and Methods: From July to December 2023, we conducted a cross-sectional study in a Beijing community to recruit older adults with CF using convenience sampling. We conducted the survey using the General Information Questionnaire, the Montreal Cognitive Assessment, the Clinical Dementia Rating, the Fried Frailty Phenotype, the Geriatric Depression Scale-15, the Generalized Anxiety Disorder-7, the Athens Insomnia Scale, the Barthel index, the Tinetti Performance Oriented Mobility Assessment, and the Lubben social network scale. The participants were separated into two categories: RCF and PRCF, based on frailty and cognitive assessment. After screening variables with a random forest algorithm, we applied association rule analysis to examine the factors influencing CF and the strength of their interactions.
Results: The survey was completed by 529 older adults with CF who lived in the community. Among them, 145 participants (27.4%) were classified as PRCF and 384 (72.6%) as RCF. 24 association rules, 12 for each subtype, were developed using the Apriori algorithm and clinical practice experience. These rules identified polypharmacy, multimorbidity, low educational attainment, and high fall risk as significant factors. Furthermore, the association pattern for PRCF is more complex.
Conclusion: The influencing factors associative patterns of the two categories of CF differ. In order to better manage elderly individuals with CF in the community, improve the cognitive health of the elderly, and encourage healthy aging, medical professionals should upgrade the community evaluation system for CF.
Keywords: cognitive frailty, older adults, association rule analysis, apriori algorithm
Introduction
Population aging has become a major public health concern. By 2030, the proportion of the global population aged 60 and above is projected to reach 16.6%.1 Although promoting physical activity and enhancing social participation among older adults can improve their quality of life and facilitate active aging, the prevalence of geriatric syndromes and chronic illnesses rises sharply with age.2,3 These conditions not only compromise older adults’ health and quality of life, but also impose substantial burdens on healthcare systems and the economy.4,5 Therefore, early identification of geriatric syndromes can reduce adverse health outcomes among older adults, alleviate healthcare burdens, and improve quality of life. Cognitive frailty (CF) is a common issue among geriatric syndromes, defined as the coexistence of physical frailty and cognitive impairment in the absence of dementia.6 Physical frailty and cognitive impairment can influence each other, forming a vicious cycle.7 The overall prevalence of CF worldwide is 9%, and it is showing an upward trend year by year.8 According to studies, up to 26.16% of older adults in Chinese communities suffer from CF, significantly higher than the global average.9 As a transitional stage preceding dementia, CF is also associated with various adverse outcomes such as falls, disability, and hospitalization.10 Therefore, early identification of this condition can delay the progression of cognitive impairment and reduce the risk of adverse health outcomes.11
It is worth noting that CF can be divided into two subtypes: reversible cognitive frailty (RCF) and potential reversible cognitive frailty (PRCF). The two subtypes of CF differ in their underlying mechanisms, clinical manifestations, and adverse health outcomes, making their differentiation clinically significant. RCF is defined as either pre-frailty or frailty, both co-occurring with subjective cognitive decline (SCD). SCD refers to self-perceived decline in memory or other cognitive functions relative to one’s own baseline, despite normal performance on cognitive testing.12 PRCF is defined as either pre-frailty or frailty, both co-occurring with mild cognitive impairment (MCI). Specifically, MCI is characterized by an individual performing poorly on one or more cognitive measures, which indicates deficits in one or more cognitive domains.13 Regarding adverse outcomes, the risk disparity between the two subtypes was also confirmed. In a cohort of 3,200 community-dwelling older adults in China, 41.0% had RCF and were at significantly higher risk of falls (OR=1.302,95% CI:1.053~1.593). PRCF elderly individuals accounted for 12.5%, with an even higher risk of falls (OR=1.442, 95% CI:1.179~1.922).14 However, most current studies focus solely on the overall incidence and adverse outcomes of CF, lacking in-depth exploration of the distinctive patterns of association between risk factors for the two subtypes.10,15 The influencing factors and intervention methods differ between the two subtypes. Early accurate assessment and targeted interventions can slow, halt, or even reverse cognitive decline.16
The two subtypes of CF result from the interaction of multiple factors, but traditional statistical models often rely on assumptions such as linear relationships, limiting their ability to integrate this type of data. Random forests are an ideal choice for variable selection due to their ability to handle non-linear relationships and their variable importance assessment mechanism. Association rule analysis reveals potential associations between variables by mining frequent item sets in data. It is currently being applied in areas such as the management of elderly diabetic patients, venous thrombosis, and falls.17,18
Therefore, this study aims to identify key factors associated with two subtypes of CF. Through data analysis utilizing random forest and association rule analysis methods, we investigate the interactive relationships among demographic characteristics, lifestyle factors, and relevant indicators in community-dwelling older adults with CF. This research provides a reference for identifying intervention targets for precise differentiation between the two subtypes.
Methods
Study Design
This cross-sectional study was conducted in a community in Beijing from July 2023 to December 2023.
Study Population
Convenience sampling can be used to rapidly obtain a sample of community-dwelling CF older adults.
Inclusion criteria: (1) Meets the definition of cognitive frailty:16 CF screening was conducted using the Fried frailty phenotype, the Montreal Cognitive Assessment (MoCA), and the Clinical Dementia Rating (CDR) scale. Simultaneously meet the following three criteria: ① Fried frailty phenotype score ≥ 1 point, ② MoCA score < 26 points (individuals with less than 12 years of education receive an additional 1 point), ③ CDR ≤ 0.5 points. (2) Aged 65 and above. (3) The ability to cooperate in completing the survey.(4) Giving informed consent and volunteering to participate.
Exclusion criteria: (1) Clinically diagnosed with dementia or mental illness; (2) Severe organ dysfunction and in the final stage of the disease; (3) Hemiplegia or limb impairment.
Survey Tool
The selection of independent variables is based on the biopsychosocial model and draws upon relevant research on cognitive decline, geriatric syndromes, and other related topics. It encompasses dimensions such as demographic characteristics, health status, psychological factors, and social support.
General Information Questionnaire
A general information questionnaire was developed based on previous research and a literature review. It collected demographic data including age, sex, body mass index, educational attainment, healthcare payment method, living arrangement, marital status, multimorbidity, medication history, and smoking and alcohol use.
Fried Frailty Phenotype (FFP)
The Fried Frailty Phenotype, proposed by Fried19 in 2001, comprises five components: unintentional weight loss, reduced grip strength, self-reported exhaustion, slow gait speed, and low physical activity levels. Each criterion met is assigned 1 point, yielding a total score range of 0~5. Scores are interpreted as 0 = robust, 1~2 = pre-frailty, and 3~5 = frailty.
Montreal Cognitive Assessment (MoCA)
The Montreal Cognitive Assessment (MoCA), developed by Nasreddine in 2005, comprises eight items: visuospatial/executive function, naming, memory, attention, language, abstraction, delayed recall, and orientation, with a total score ranging from 0 to 30. For participants with ≤12 years of education, 1 point is added to the total score. For this study, a total scores ≥26 indicate normal cognitive function. The Cronbach’s alpha coefficient for this scale is 0.88.20
Clinical Dementia Rating (CDR)
The Clinical Dementia Rating (CDR), developed by Hughes21 in 1982, the assessment comprises six domains: memory, orientation, judgment and problem-solving, work and social functioning, family life and hobbies, and independent living skills. Scores range from 0 to 3, where 0 denotes normal cognition, 0.5 indicates possible dementia, and scores ≥1 signify dementia. In this study, participants with a CDR score of 0 were classified as RCF, and those with higher scores as PRCF.
Geriatric Depression Scale-15 (GDS-15)
The Geriatric Depression Scale-15 (GDS-15), developed by Sheikh in 1986, this 15-item scale assigns 1 point per item, with reverse scoring applied to specific entries. Total scores range from 0 to 15, where 0~4 denotes normal status, 5~8 suggests mild depressive symptoms, and scores ≥9 indicate moderate-to-severe depression. The Cronbach’s alpha coefficient for this scale is 0.793.22 For this study, a GDS cutoff score of ≥8 was defined as representing geriatric depressive state.
Generalized Anxiety Disorder-7 (GAD-7)
The Generalized Anxiety Disorder-7 (GAD-7), developed by Spizer in 2006, the scale comprises 7 items with a total score range of 0~21 points: 0~4 indicates normal status, 5~9 suggests mild anxiety, 10~14 represents moderate anxiety, and scores ≥15 denote severe anxiety. The Cronbach’s alpha coefficient for this scale is 0.898.23
Athens Insomnia Scale (AIS-8)
Developed by Soldatos in 2000, this scale comprises 8 items with each item scored on a 0~3 scale, yielding a total score range of 0~24. Scores below 4 indicate no sleep disturbance, 4~6 suggest possible insomnia, and scores above 6 signify insomnia. The Cronbach’s alpha coefficient for this scale is 0.881.24
Barthel Index (BI)
Developed by Mahoney and Barthel in the United States in 1965, this scale comprises 10 items, each scored at 0, 5, 10, or 15 points, with a total score ranging from 0 to 100. Higher scores reflect greater independence: scores ≤20 = total dependence, 25~45 = severe dependence, 50~70 = moderate dependence, 75~95 = mild dependence, and 100 points denote complete independence. The Cronbach’s alpha coefficient for this scale is 0.902.25
Tinetti Performance Oriented Mobility Assessment (POMA)
The Tinetti Performance Oriented Mobility Assessment (POMA), developed by Tinetti in 1986, the scale comprises two components: balance and gait assessments, totaling 16 items. Scores range from 0 to 28, with lower values indicating greater fall risk. Scores above 24 denote no risk, 19~24 represent fall risk present, and below 19 indicate high fall risk. The Cronbach’s alpha coefficient for this scale is 0.887.26
Lubben Social Network Scale- Revised (LSNS-R)
The Lubben social network scale- Revised (LSNS-R), developed by Lubben in 1988, the scale comprises two dimensions: family and friends, each containing 6 items. Scores range from 0 to 5 per item, with a total possible score of 0 to 60. Lower total scores indicate greater social isolation risk, with scores ≤19 denoting social isolation risk present. The Cronbach’s alpha coefficient for this scale is 0.7.27
Sample Size Estimation
The primary objective of this study is to analyze the association patterns and influencing factors of two subtypes of CF among community-dwelling older adults. The sample size was calculated as 10 times the number of study variables.28 With 16 variables included and a 10% allowance for invalid responses, the estimated sample size required is 178 participants. This study actually included 529 participants, which reduces sampling error and enhances the statistical power of the tests.
Determining RCF and PRCF
Individuals with CF exhibit heterogeneity in the degree of cognitive dysfunction and clinical manifestations. RCF refers to subjective cognitive decline preceding mild cognitive impairment, where daily functioning in older adults remains largely unaffected and overall functional capacity is well preserved.12,16 PRCF refers to older adults who have exhibited mild clinical cognitive decline, meeting the criteria for mild cognitive impairment (MCI) and remaining in a potentially reversible stage.13,16 The International Academy on Nutrition and Aging (IANA) and the International Association of Gerontology and Geriatrics (IAGG) consensus proposes a CDR score of 0.5 as the criterion for MCI.29 When CDR=0 and a positive response is given to one of the items, it indicates the presence of SCD.30 Based on the aforementioned consensus and relevant research, this study employs the CDR score to classify CF: CDR=0 is defined as RCF, and CDR=0.5 is defined as PRCF.31,32
Statistical Methods
Data preprocessing for this study comprised two steps: data cleaning and data coding. First, data cleaning was conducted. Any questionnaire containing three or more unanswered questions, obvious contradictions, or any instance of formulaic responses was deemed invalid and excluded from subsequent analysis. Subsequently, data coding was performed. For categorical variables in general information, values were assigned directly based on their categorical attributes. For continuous variables in general information, age and BMI were categorized according to commonly used standards in geriatric medicine and standards for the Chinese population. For continuous variables from each scale test, classification was based on their standardized scoring rules, followed by value assignment coding to meet the requirements for subsequent statistical analysis. See Table 1 for details.
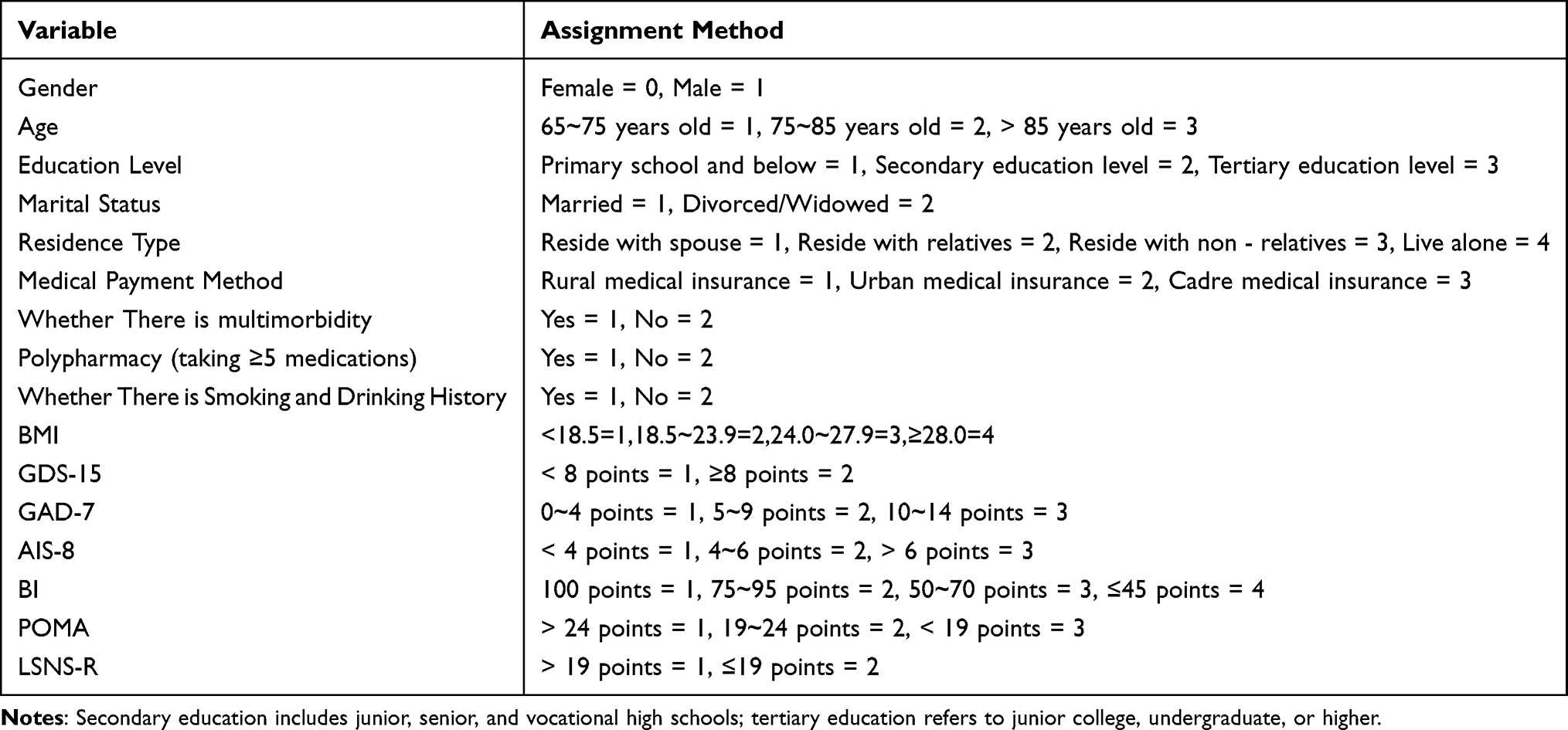 |
Table 1 Variable Assignment |
Data analysis was conducted using R software (version 4.3.1). Count data were expressed as frequencies and percentages. Intergroup comparisons were conducted using Pearson’s chi-square test or Fisher’s exact test (adjusted for cell frequency). In R, a random forest classification model was constructed using the randomforest package. A random seed of 10 was set to ensure reproducibility. The number of decision trees (ntree) was set to 500, while the number of candidate variables per node (mtry) used the default value. Variable importance calculation was enabled (importance=TRUE) to identify significant variables.
The selected significant variables were subsequently analyzed using the Apriori algorithm to examine association rules for CF subtypes. Association rules were expressed as X→Y, characterized by three metrics: support, confidence, and lift. Support represents the co-occurrence probability of both X and Y; higher values suggest stronger associations. Confidence indicates the conditional probability of Y given X, with greater values denoting more reliable rules. Lift quantifies whether X enhances the occurrence of Y: values >1 demonstrate positive correlation, =1 indicate independence, and <1 reflect negative correlation. In alignment with parameter configurations from comparable studies, this research established the maximum antecedent number as 5, minimum support at 0.04, and minimum confidence threshold of 0.6, while selecting association rules with lift values exceeding 1.17,18
Association rules are presented as unordered categorical data. Based on their sample distribution characteristics, Fisher’s exact test is applied to their antecedent and consequent items. Multiple comparisons between groups are adjusted using Bonferroni correction, with a significance level of α=0.05. An adjusted P value < 0.05 indicates statistical significance. Finally, this study performed univariate frequency statistics and visualization analysis on the antecedents of rules corresponding to the two subtypes. This clarified the distribution characteristics of common factors and subtype-specific factors, presented in bar charts.
Results
General Information of Community-Dwelling Older Adults with Cognitive Frailty
Of 5,253 community-dwelling older adults screened in Beijing, China, 529 met the criteria for CF and were included. Among the 529 older adults with CF, 384 cases (72.58%) belonged to RCF and 145 cases (27.42%) belonged to PRCF. Participants were classified into two subtypes, and the general data of the two groups of older adults are shown in Table 2.
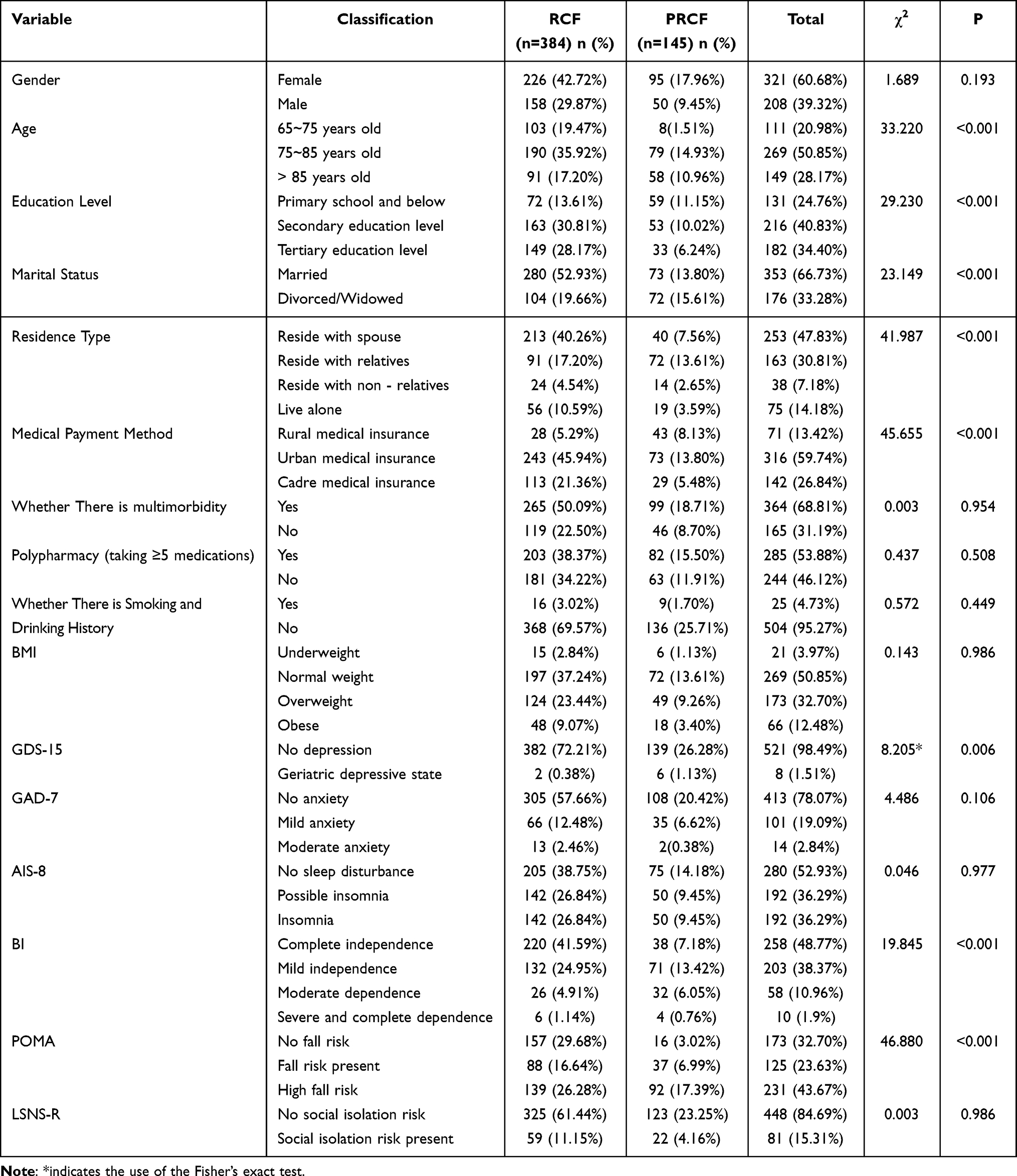 |
Table 2 General Information of Community-Dwelling Older Adults with CF |
Screening of Influencing Factors for Community-Dwelling Older Adults with CF
We used the two CF subtypes as dependent variables and entered 16 predictors into a random forest model implemented in R (version 4.3.1). The mean decrease in Gini index serves as a measure of dataset purity, with higher values indicating greater variable importance for the model. Figure 1 presents the importance ranking of influencing factors among community-dwelling older adults with CF. Based on clinical expertise and expert consensus, we selected the 10 most important variables plus 12 additional factors (including multimorbidity and polypharmacy) for association rule analysis.
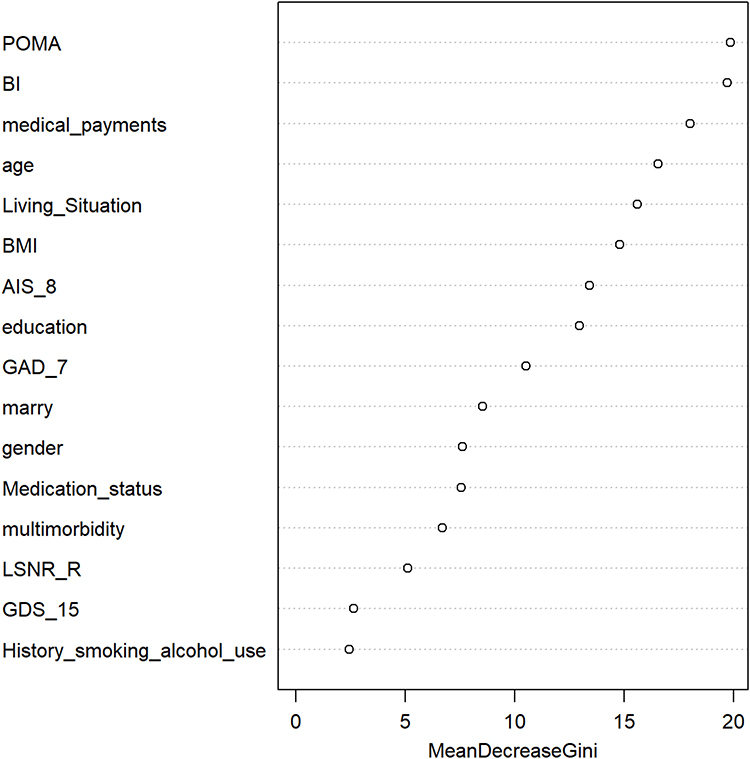 |
Figure 1 Importance ranking of influencing factors for community-dwelling older adults with cognitive frailty. |
Association Analysis results of Community-Dwelling Older Adults with CF
Using the Apriori algorithm, association rule analysis was performed on 12 variables, with RCF and PRCF as the consequents respectively. Rules with confidence >60% and lift >1 were screened, resulting in 24 association rules based on relevant professional knowledge and clinical practice experience, with 12 rules for each subtype. Association rules indicate that the antecedents of RCF are relatively simple, while those of PRCF are more complex; multimorbidity and polypharmacy are common risk factors for both RCF and PRCF. Differences exist in education level distribution between the two subtypes in older adults. Rules 13 and 19–24 indicate that older adults with PRCF predominantly received primary education or below, while those with RCF (Rules 6, 7, 9, 10, 12) mostly attained secondary education. Additionally, most PRCF rules (except Rules 13 and 22) included high fall risk, whereas only one RCF rule encompassed high fall risk. See Table 3 and Figure 2 for details.
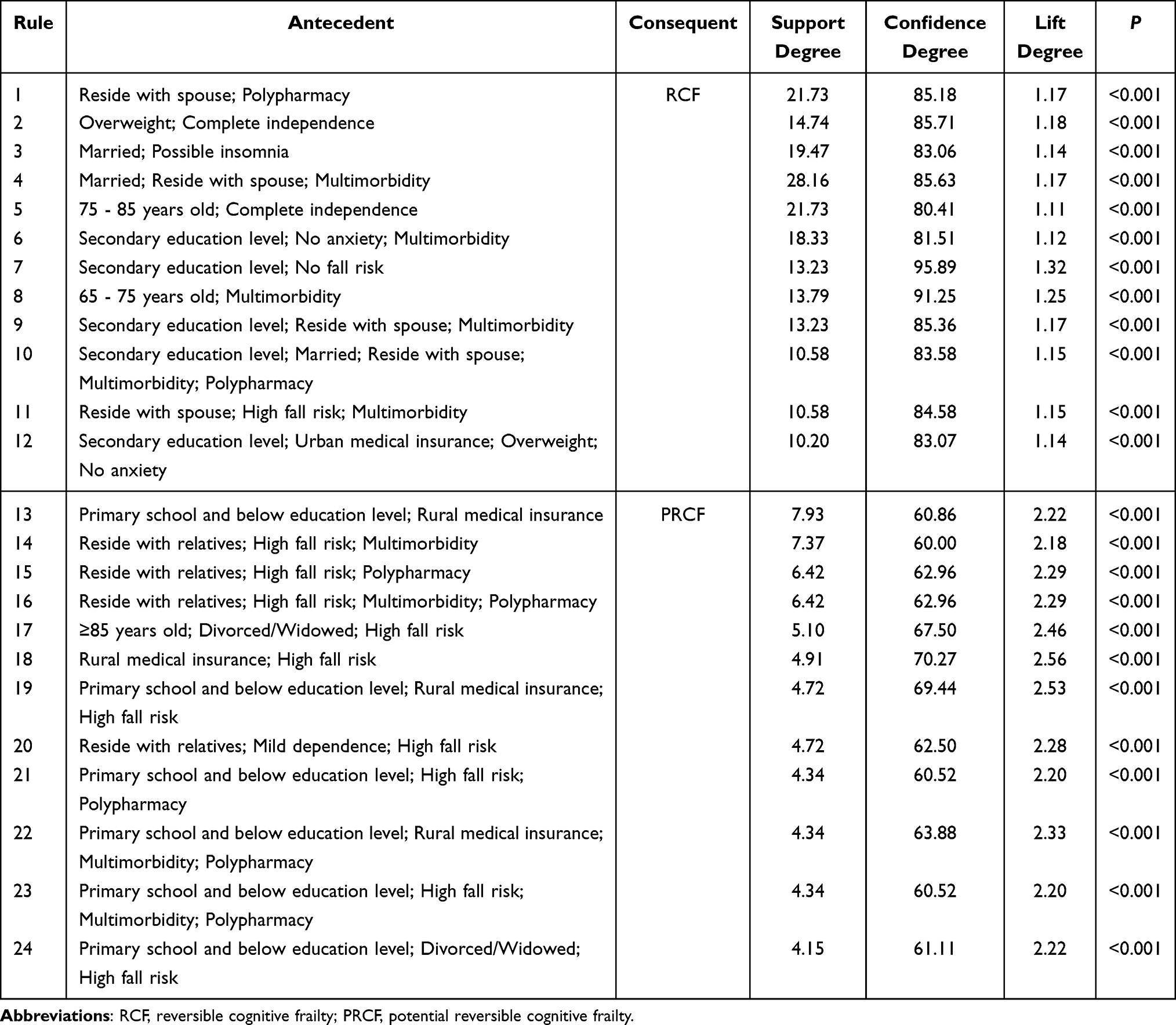 |
Table 3 Association Rules of Two Subtypes of Community-Dwelling Older Adults with Cognitive Frailty |
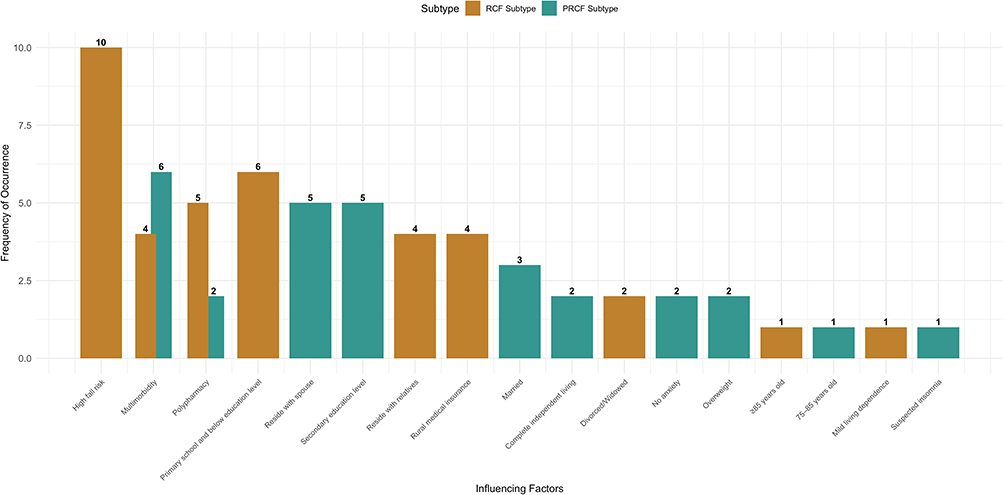 |
Figure 2 Frequency Analysis of Influencing Factors for RCF and PRCF. |
Discussion
Current Status of Community-Dwelling Older Adults with CF
The proportion of older adults with RCF in this study was higher than those with PRCF, which differs slightly from the findings of Zhao.33 The analysis suggests that differences in educational attainment among study participants and regional economic development levels may account for these variations. Higher educational levels are associated with greater self-care capacity among older adults while improved economic conditions indicate greater access to care resources for this demographic.34
The primary distinction between the RCF and PRCF subtypes lies in the mechanisms underlying cognitive impairment and its reversibility. The former manifests as diminished subjective cognitive abilities and markedly reduced functional connectivity within the cerebellum. By enhancing connectivity through functional compensation between the brain and cerebellum, overall cognitive function can be maintained. Thus, RCF exhibits reversible characteristics, presenting a critical window for cognitive intervention.16,35 The latter manifests as mild cognitive impairment, potentially linked to structural neuronal damage. At this stage, neuronal cell loss may exceed the brain’s physiological compensatory capacity, potentially leading to irreversible cognitive impairment.36 Therefore, enhancing early identification of RCF and PRCF and implementing timely interventions are crucial for slowing the progression of cognitive decline in older adults and optimizing long-term cognitive outcomes.
Association Rule Analysis of Community-Dwelling CF Older Adults
Association rule algorithms aim to uncover frequent co-occurrence patterns within datasets but cannot establish causal relationships. This study found that educational attainment, high fall risk, multimorbidity, and polypharmacy are associated with both subtypes.
Among these, educational attainment is positively correlated with cognitive function. Older adults with higher education levels possess greater cognitive reserve, which stimulates neural network plasticity mechanisms and enhances information processing capabilities, thereby delaying cognitive decline.37 High fall risk is a significant indicator of cognitive decline, likely because it often signifies deficits in cognitive functions such as attention, processing speed, and executive function, suggesting cognitive frail or even impairment in the elderly.38 A US cohort study examining the association between multimorbidity and cognitive decline in older adults reported that multimorbidity accelerates the rate of cognitive decline.39 Possible causes include vascular lesions and the release of inflammatory factors due to underlying conditions such as diabetes and hypertension, which elevate systemic inflammation levels. Patients with multimorbidity conditions often require multiple medications. A meta-analysis examining polypharmacy and cognitive impairment in older adults found that polypharmacy increases the risk of cognitive decline, with the risk escalating as the number of medications increases.40 Due to age-related declines in glomerular filtration and hepatic clearance,41 which slow down pharmacokinetics in the body, thereby increasing the risk of adverse drug reactions and the prevalence of cognitive impairment. Concurrently, higher medication counts elevate the risk of drug interactions. Compared to monotherapy, polypharmacy can accumulate multiple side effects and amplify neurotoxicity, leading to drug-related cognitive impairment. Additionally, certain medications such as anticholinergics can cause cognitive decline by antagonizing central acetylcholine receptors and disrupting neural transmission.42 Finally, the diminished self-management abilities of older adults with cognitive impairment also increase the likelihood of inappropriate medication use, creating a vicious cycle.
In RCF association rules, most antecedents are relatively simple, comprising two factors: a single risk factor and a single protective factor. This suggests that a risk factor can offset the protective effect of a protective factor, increasing the risk of cognitive impairment. Therefore, patients with RCF require assessment of specific risk factors and targeted interventions. In contrast, the antecedents in PRCF association rules are more complex, typically involving combinations of multiple risk factors with interactions among them. Consequently, it is essential to establish a multidimensional, comprehensive intervention system to achieve holistic care.
Management of Community-Dwelling CF Older Adults
Improve Community-Based Assessment of CF
《Expert consensus on neuropsychological assessment for mild cognitive impairment (2025 edition)》proposes that comprehensive and accurate evaluation of cognitive function, coupled with targeted interventions, constitutes an effective measure for delaying cognitive decline.43 This study revealed distinct patterns of risk factor associations between the two subtypes. Early identification of CF subtypes in older adults is essential to focus on risk factors and provide timely interventions. Community health centers can establish cognitive screening teams comprising physicians and nurses to assess cognitive decline using scales such as Fried, MoCA, and CDR. These teams should create dedicated cognitive profiles and conduct regular follow-ups.
Enhance the Management of Polypharmacy in Older Adults
This study found that multimorbidity conditions and polypharmacy are significant risk factors for cognitive impairment, consistent with previous research findings.40,44 Therefore, healthcare professionals should regularly organize physical examinations for community older adults, provide periodic health education, monitor their underlying conditions, actively manage these conditions, promptly detect changes in their health status, and minimize the impact on their cognitive function.
Furthermore,when prescribing medications, healthcare providers should tailor treatment plans to the specific circumstances of elderly patients, refer to the Beers criteria, and comprehensively evaluate the efficacy and adverse effects of various drugs to optimize medication regimens. Special attention should be given to elderly patients taking multiple medications. Provide medication education to explain the risks of polypharmacy, remind patients to take medications regularly and in prescribed doses, monitor for adverse reactions, and seek medical attention promptly.
Expand the Formats and Content of Health Education to Promote Healthy Lifestyles
The findings of this study indicate that older adults with lower educational attainment experience a more rapid decline in cognitive function, consistent with the results of previous research.45 Older adults with higher levels of education possess greater knowledge reserves, indicating higher activation levels in their brain’s neural networks, which in turn delays or mitigates the effects of cognitive decline.46 At the same time, older adults with higher levels of education possess greater knowledge about disease-related matters, enabling them to proactively identify risk factors and make adjustments to enhance their self-management capabilities.47 Therefore, community healthcare providers should consider the educational background of older adults and adopt personalized health education approaches. They should flexibly choose methods such as on-site education, home visits, and mobile notifications to enhance their disease knowledge and strengthen their self-management awareness. Additionally, health education content should be diversified, encompassing not only disease knowledge but also cognitive function intervention methods, balanced diets, and appropriate exercise. This will guide older adults in establishing healthy lifestyles and improving their quality of life.
Develop a Multidimensional Intervention System
The risk factors and mechanisms underlying the two subtypes of CF differ, necessitating distinct intervention strategies. For RCF older adults, interventions should target primary risk factors to prevent progression to PRCF or cognitive impairment. In contrast, PRCF older adults require attention to a range of risk factors and their interactions, necessitating multidimensional, comprehensive intervention measures.48 The management of CF older adults relies on multidisciplinary collaborative care (involving teams from geriatrics, nutrition, rehabilitation, and nursing) and follow-up monitoring by community health service centers. Research indicates that multicomponent interventions--incorporating cognitive training, physical exercise, nutritional support, and health education--significantly improved cognitive function in community-dwelling older adults and delayed the progression of CF.49 With the deep integration of artificial intelligence technology in the medical field, cognitive training games developed using AI technology can dynamically adjust difficulty levels based on users’ actual conditions. This enhances user adherence and positively impacts their cognitive function.50 Additionally, leveraging “Internet Plus” technologies can empower patients through features such as mobile notifications and wristband vibration alerts. This approach reduces the implementation costs of intervention measures, enhances patient adherence, and ultimately improves cognitive function.51 Cognitive function undergoes dynamic changes, which requires close monitoring. By leveraging smart wearable devices to collect physiological data such as blood pressure, sleep cycles, physical activity, and emotional states from older adults, combined with standardized cognitive assessment scale results, a CF risk prediction model is established to identify risk factors and develop personalized intervention measures.52,53 It is worth noting that the application of artificial intelligence and internet technologies in CF interventions may be hindered by factors such as insufficient digital literacy among older adults and limited access channels. This underscores the need for communities to tailor the implementation of such technological tools to the actual circumstances of older adults and to provide complementary support measures, including digital skills training.
Limitations
First, this study employed self-report instruments for data collection, which are susceptible to subjectivity among participants. This may lead to discrepancies between reported outcomes and actual results, introducing bias. Second, the Apriori algorithm was selected for association rule analysis. This algorithm can only identify co-occurrence patterns among variables and cannot reveal underlying causal relationships. Finally, the analysis did not account for missing data, potentially introducing selection bias that may compromise the robustness of the findings.
Conclusion
This study employed the Apriori algorithm to perform association rule analysis on data from community-dwelling older adults with cognitive frailty. It revealed distinct patterns in risk factor associations between RCF and PRCF, indicating differing intervention windows and approaches. Based on these findings, communities can focus on addressing cognitive frailty in the elderly and implement risk stratification, providing a theoretical basis for personalized cognitive interventions. This study addresses the need for cognitive health in an aging society, laying preliminary groundwork for reducing the public health burden associated with cognitive impairment-related diseases.
Data Sharing Statement
Current research data can be obtained from the corresponding author (Huo Xiaopeng, [email protected]) upon reasonable request.
Ethics Approval and Consent to Participate
The study design and procedures strictly adhered to the ethical principles outlined in the Declaration of Helsinki (2013 revision).This study was approved by the Ethics Committee of Peking Union Medical College Hospital, with the ethics review approval number ZS-2943.
Consent for Publication
All subjects understood and signed the informed consent form.
Acknowledgments
Thank you to all subjects who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National High Level Hospital Clinical Research Funding (2022-PUMCH-B-130).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Organization WH. World report on ageing and health. World Health Organization; 2015.
2. Parra Rizo MA, López Marin P. Efecto y adecuación del ejercicio para la mejora cardiovascular de la población mayor de 65 años. Revista de Psicología de la Salud. 2020;8(1). doi:10.21134/pssa.v8i1.670
3. Rizo MAP, Cigarroa I, Sánchez SO, et al. Sociodemographic profile of physically active older adults according to the type of physical activities practiced: gymnastic exercises, aquatic activities, yoga, Pilates and dance. Retos. 2024;56(56):280–13. doi:10.47197/retos.v56.102223
4. Ye X, Wang M, Xia Y, He P, Zheng X. Direct economic burden attributable to age-related diseases in China: an econometric modelling study. J Glob Health. 2023;13:04042. doi:10.7189/jogh.13.04042
5. Kingston A, Wohland P, Wittenberg R, et al. Is late-life dependency increasing or not? A comparison of the cognitive function and ageing studies (CFAS). Lancet. 2017;390(10103):1676–1684. doi:10.1016/S0140-6736(17)31575-1
6. Salvioli S, Basile MS, Bencivenga L, et al. Biomarkers of aging in frailty and age-associated disorders: state of the art and future perspective. Ageing Res Rev. 2023;91:102044. doi:10.1016/j.arr.2023.102044
7. Nader MM, Cosarderelioglu C, Miao E, et al. Navigating and diagnosing cognitive frailty in research and clinical domains. Nat Aging. 2023;3(11):1325–1333. doi:10.1038/s43587-023-00504-z
8. Qiu Y, Li G, Wang X, et al. Prevalence of cognitive frailty among community-dwelling older adults: a systematic review and meta-analysis. Int J Nurs Stud. 2022;125:104112. doi:10.1016/j.ijnurstu.2021.104112
9. Ruan Q, Xiao F, Gong K, et al. Prevalence of cognitive frailty phenotypes and associated factors in a community-dwelling elderly population. J Nutr Health Aging. 2020;24(2):172–180. doi:10.1007/s12603-019-1286-7
10. Zhang XM, Wu XJ, Cao J, Jiao J, Chen W. Association between cognitive frailty and adverse outcomes among older adults: a meta-analysis. J Nutr Health Aging. 2022;26(9):817–825. doi:10.1007/s12603-022-1833-5
11. Cozza M, Boccardi V. Cognitive frailty: a comprehensive clinical paradigm beyond cognitive decline. Ageing Res Rev. 2025;108:102738. doi:10.1016/j.arr.2025.102738
12. Rabin LA, Smart CM, Amariglio RE. Subjective cognitive decline in preclinical Alzheimer’s disease. Ann Rev Clin Psychol. 2017;13(1):369–396. doi:10.1146/annurev-clinpsy-032816-045136
13. Petersen RC, Caracciolo B, Brayne C, Gauthier S, Jelic V, Fratiglioni L. Mild cognitive impairment: a concept in evolution. J Intern Med. 2014;275(3):214–228. doi:10.1111/joim.12190
14. Xu X, Ding N, He J, et al. Associations between reversible and potentially reversible cognitive frailty and falls in community-dwelling older adults in China: a longitudinal study. BMC Geriatr. 2025;25(1):224. doi:10.1186/s12877-025-05872-2
15. Liu J, Xu S, Wang J, et al. Prevalence of cognitive frailty among older adults in China: a systematic review and meta-analysis. BMJ Open. 2023;13(4):e066630. doi:10.1136/bmjopen-2022-066630
16. Ruan Q, Yu Z, Chen M, Bao Z, Li J, He W. Cognitive frailty, a novel target for the prevention of elderly dependency. Ageing Res Rev. 2015;20:1–10. doi:10.1016/j.arr.2014.12.004
17. Li XL, Guo XH, Wang N, et al. Association rules analysis of diabetic distress in elderly patients with type 2 diabetes mellitus in the community. Chin Nurs res. 2024;38(23):4152–4158.
18. Xu Y, Wei H, Zhao Q, et al. Characteristic of dehydration in stroke patients based on the association rule. J Nurs Sci. 2024;39(15):15–18.
19. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–56. doi:10.1093/gerona/56.3.M146
20. Yu J, Li J, Huang X. The Beijing version of the montreal cognitive assessment as a brief screening tool for mild cognitive impairment: a community-based study. BMC Psychiatry. 2012;12(1):156. doi:10.1186/1471-244X-12-156
21. Hughes CP, Berg L, Danziger WL, Coben LA, Martin RL. A new clinical scale for the staging of dementia. Br J Psychiatry. 1982;140(6):566–572. doi:10.1192/bjp.140.6.566
22. Tang D. Use of the 15-item geriatric depression scale (GDS-15) in Chinese elderly individuals. Chin J Clin Psychol. 2013;21(3):402–405. doi:10.16128/j.cnki.1005-3611.2013.03.036
23. He XY, Li CB, Qian J, Cui HS, Wu WY. Reliability and validity study of the generalized anxiety disorder scale in general hospitals. Shanghai Arch Psychiatry. 2010;22(4):200–203.
24. Elbi H, Batum M, Ozturk EO, et al. Validation and discriminant analysis of the athens insomnia scale in older adults. Int J Methods Psychiatr Res. 2025;34(2):e70017. doi:10.1002/mpr.70017
25. Zhang C, Zhang X, Zhang H, et al. Psychometric properties of the Barthel index for evaluating physical function among Chinese oldest-old. JCSM Clinical Reports. 2022;7(2):33–43. doi:10.1002/crt2.47
26. Gao J, Wu CX, Bai DX, et al. Reliability and validity study of the tinetti balance and gait scale for fall risk assessment in elderly individuals. Chinese J Prac Nurs. 2014;30(5):61–63. doi:10.3760/cma.j.issn.1672-7088.2014.05.022
27. Fang EF, Xie C, Schenkel JA, et al. A research agenda for ageing in China in the 21st century (2nd edition): focusing on basic and translational research, long-term care, policy and social networks. Ageing Res Rev. 2020;64:101174. doi:10.1016/j.arr.2020.101174
28. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
29. Kelaiditi E, Cesari M, Canevelli M, et al. Cognitive frailty: rational and definition from an (I.A.N.A./I.A.G.G.) international consensus group. J Nutr Health Aging. 2013;17(9):726–734. doi:10.1007/s12603-013-0367-2
30. Hwang H-F, Suprawesta L, Chen S-J, Yu W-Y, Lin M-R. Predictors of incident reversible and potentially reversible cognitive frailty among Taiwanese older adults. BMC Geriatr. 2023;23(1):24. doi:10.1186/s12877-023-03741-4
31. Solfrizzi V, Scafato E, Seripa D, et al. Reversible cognitive frailty, dementia, and all-cause mortality. The Italian longitudinal study on aging. J Am Med Dir Assoc. 2017;18(1):89e1–89e8. doi:10.1016/j.jamda.2016.10.012
32. Bian J, Chen Z, Gao Y, et al. Prevalence of cognitive frailty, reversible and potentially reversible cognitive frailty among older adults without dementia: a systematic review and meta-analysis. J Gerontol B Psychol Sci Soc Sci. 2025. doi:10.1093/geronb/gbaf228
33. Zhao XR, Huang L, Cao LC, et al. Status and influencing factors of reversible and potentially reversible cognitive frailty among the community-dwelling elderly. Chinese General Prac. 2025;28(7):824–830,843.
34. Nielsen J, Bahendeka SK, Bygbjerg IC, Meyrowitsch DW, Whyte SR. Accessing diabetes care in rural Uganda: economic and social resources. Glob Public Health. 2017;12(7):892–908. doi:10.1080/17441692.2016.1172100
35. Tao W, Lu X, Yuan S, et al. Unstable functional brain states and reduced cerebro-cerebellar modularity in elderly individuals with subjective cognitive decline. Neuroimage. 2025;305:120969. doi:10.1016/j.neuroimage.2024.120969
36. Wang W, Si H, Yu R, et al. Effects of reversible cognitive frailty on disability, quality of life, depression, and hospitalization: a prospective cohort study. Aging Mental Health. 2022;26(10):2031–2038.
37. Hachinski V, Avan A. A new definition of brain reserve. Alzheimers Dement. 2022;18(3):535–537. doi:10.1002/alz.12562
38. Liu J, Wu Y, Long Z, Zhang S, Wu S. The association between cognitive frailty and the risk of fall occurrence in older adults: a meta-analysis of cohort studies. Front Med Lausanne. 2025;12:1537240. doi:10.3389/fmed.2025.1537240
39. Wei MY, Levine DA, Zahodne LB, Kabeto MU, Langa KM. Multimorbidity and cognitive decline over 14 years in older Americans. J Gerontol a Biol Sci Med Sci. 2020;75(6):1206–1213.
40. Yu X, Qian Y, Zhang Y, Chen Y, Wang M. Association between polypharmacy and cognitive impairment in older adults: a systematic review and meta-analysis. Geriatr Nurs. 2024;59:330–337.
41. Mangoni AA, Jackson SH. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6–14. doi:10.1046/j.1365-2125.2003.02007.x
42. Pieper NT, Grossi CM, Chan W-Y, et al. Anticholinergic drugs and incident dementia, mild cognitive impairment and cognitive decline: a meta-analysis. Age Ageing. 2020;49(6):939–947. doi:10.1093/ageing/afaa090
43. The Dementia and Cognitive Disorders Group of the Chinese Society of Neurology. Expert consensus on neuropsychological assessment for mild cognitive impairment (2025 edition). Zhonghua yi xue za zhi. 2025;105(3):204–218. doi:10.3760/cma.j.cn112137-20240612-01322 Danish
44. Wu RK, Wang MW, Han ZF, et al. Influencing factors of common chronic diseases on mild cognitive impairment in elderly inpatients with multiple comorbidities. Chin J Mult Organ Dis Elderly. 2025;24(01):26–31.
45. Iraniparast M, Shi Y, Wu Y, et al. Cognitive reserve and mild cognitive impairment: predictors and rates of reversion to intact cognition vs progression to dementia. Neurology. 2022;98(11):e1114–e1123. doi:10.1212/WNL.0000000000200051
46. Paap KR. Cognitive reserve? Cognitive capacity! Brain Sci. 2024;14(12):1265. doi:10.3390/brainsci14121265
47. Wang S, Niu W, Wang Y, et al. The current status and influencing factors of the coexistence of multiple frailty domains in patients with chronic heart failure. Chin J Nurs. 2025;60(03):311–318.
48. Peng J, Chang R, Wei X, Yin Z, Liu Q. Effect of non-pharmacological interventions in people with cognitive frailty: a systematic review and network meta-analysis. BMC Public Health. 2024;24(1):2684. doi:10.1186/s12889-024-20079-7
49. Zhong SM, Wu MQ, Li FF, et al. Application of the mobile health technology for home rehabilitation in older adults with cognitive impairment: a scoping review. Chin Nurs Manage. 2024;24(11):1717–1722.
50. Zhang Y, Zhou JJ, Zhang XM, et al. Management of cognitive frailty: a network meta-analysis of randomized controlled trials. Int J Geriatr Psychiatry. 2023;38(9):e5994.
51. Eun S-J, Kim EJ, Kim JY, Kim H-J. Development and evaluation of an artificial intelligence–based cognitive exercise game: a pilot study. J Environ Public Health. 2022;2022(1):4403976. doi:10.1155/2022/4403976
52. Gavriilaki M, Anyfanti P, Mastrogiannis K, et al. Association between ambulatory blood pressure monitoring patterns with cognitive function and risk of dementia: a systematic review and meta-analysis. Aging Clin Exp Res. 2023;35(4):745–761. doi:10.1007/s40520-023-02361-7
53. Lucey BP, Wisch J, Boerwinkle AH, et al. Sleep and longitudinal cognitive performance in preclinical and early symptomatic Alzheimer’s disease. Brain. 2021;144(9):2852–2862. doi:10.1093/brain/awab272
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Relationship Between Social Isolation and Cognitive Frailty Among Community-Dwelling Older Adults: The Mediating Role of Depressive Symptoms
Bai Y, Chen Y, Tian M, Gao J, Song Y, Zhang X, Yin H, Xu G
Clinical Interventions in Aging 2024, 19:1079-1089
Published Date: 17 June 2024
Development and Evaluation of Content Validity and Acceptance of a Multidomain Intervention Module for Reversal of Cognitive Frailty Among Older Adults
Mustafa Khalid N, Ponvel P, Ibrahim AM, Mohd Safien A, Md Fadzil NH, Singh DKA, Mat Ludin AF, Ibrahim N, Subramaniam P, Haron H, Rajikan R, Vanoh D, Shahar S
Clinical Interventions in Aging 2024, 19:1189-1202
Published Date: 1 July 2024