Back to Journals » ClinicoEconomics and Outcomes Research » Volume 7
Association of persistent and transient worsening renal function with mortality risk, readmissions risk, length of stay, and costs in patients hospitalized with acute heart failure
Authors Palmer J, Friedman H, Waltman Johnson K, Navaratnam P, Gottlieb S
Received 5 February 2015
Accepted for publication 5 March 2015
Published 19 June 2015 Volume 2015:7 Pages 357—367
DOI https://doi.org/10.2147/CEOR.S82267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio L Colombo
Jacqueline B Palmer,1 Howard S Friedman,2 Katherine Waltman Johnson,1 Prakash Navaratnam,2 Stephen S Gottlieb3
1Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA; 2DataMed Solutions, LLC, New York, NY, USA; 3Department of Medicine, University of Maryland School of Medicine, Baltimore, MD, USA
Background: Data comparing effects of transient worsening renal function (WRFt) and persistent WRF (WRFp) on outcomes in patients hospitalized with acute heart failure (AHF) are lacking. We determined the characteristics of hospitalized AHF patients who experienced no worsening renal function (non-WRF), WRFt, or WRFp, and the relationship between cohorts and AHF-related outcomes.
Methods and results: A patient’s first AHF hospitalization (index) was identified in the Cerner Health Facts® database (January 2008-March 2011). Patients had WRF if serum creatinine (SCr) was ≥0.3 mg/dL and increased ≥25% from baseline, and they were designated as WRFp if present at discharge or WRFt if not present at discharge. A total of 55,436 patients were selected (non-WRF =77%, WRFp =10%, WRFt =13%). WRFp had greater comorbidity burden than WRFt. At index hospitalization, WRFp patients had the highest mortality, whereas WRFt patients had the longest length of stay (LOS) and highest costs. These trends were observed at 30, 180, and 365 days postdischarge and confirmed by multivariable analyses. WRF patients had more AHF-related readmissions than non-WRF patients. In sensitivity analyses of the patient subset with live index hospitalization discharges, postdischarge LOS and costs were highest in WRFt patients, whereas mortality associated with a HF hospitalization was significantly higher for WRF patients vs non-WRF patients, with no difference between WRFp and WRFt.
Conclusion: In patients hospitalized for AHF, WRFp was associated with the highest mortality, whereas WRFt was associated with the highest LOS and costs. WRF patients had higher readmissions than non-WRF patients. Transient increases in SCr appear to be associated with detrimental outcomes, especially longer LOS and higher costs.
Keywords: renal function, acute heart failure, mortality rate, health outcomes, serum creatinine, cost
Introduction
The development of worsening renal function (WRF) occurs in approximately 25% of patients hospitalized for acute heart failure (AHF).1,2 Several studies have demonstrated that WRF in AHF patients is associated with increased mortality, length of stay (LOS), heart failure (HF)-associated hospital readmissions, and cost.2–7 A meta-analysis of 23 cohort, registry, and randomized controlled studies found that AHF patients with WRF had almost a 2-fold higher rate of all-cause mortality than those without WRF (unadjusted OR [odds ratio]: 1.75–95% CI [confidence interval]: 1.47–2.08, P<0.001).1
Previous studies have used varying definitions of WRF, and populations have generally been limited to small groups of selected patients or have had limited access to complete data and follow-up. Furthermore, previous studies have rarely distinguished between transient WRF (WRFt) and persistent WRF (WRFp). The three studies that have directly compared outcomes associated with WRFt vs WRFp in patients hospitalized for AHF had somewhat contradictory results.7–9 One study found that 6-month postdischarge events (combined all-cause mortality or AHF-related readmission) were increased in patients with WRFt and WRFp.7 The second study found that only WRFp led to a significant increase in all-cause mortality at 6 months.8 In the third study, both WRFt and WRFp were associated with a higher risk of 90-day all-cause mortality, but the risk was significantly higher with WRFp vs WRFt.9 Similar to many other studies, these studies had different methods of defining WRF, and only one of the studies assessed LOS. None of the studies assessed cost outcomes based on WRF persistence.
Using contemporary data from a large multicenter database, the current analysis assessed short- and long-term AHF-related outcomes by WRF status using a rigorous clinically-based definition for WRF. The objective of this retrospective cohort analysis was to describe the characteristics of patients hospitalized for AHF who experienced no WRF (non-WRF), WRFt, or WRFp and to determine the association of these groups with in-hospital, 30-, 180-, and 365-day postdischarge mortality, risk of AHF readmission, LOS, and costs.
Methods
Study design
This was a retrospective longitudinal database analysis with a study period between January 2008 and March 2012. The index hospitalization was defined as the earliest valid inpatient hospital admission for AHF during the study period; index hospitalizations were determined up to March 30, 2011, and readmissions were tracked until March 30, 2012. AHF diagnosis was identified as hospitalization with a primary or secondary discharge International Classification of Diseases, 9th Edition (ICD-9) code for AHF (428.xx, 398.91, 402.x1, 404.x1, 404.x3, 415.0, 416.x, 417.x, 425.x, 429.0, 429.1, or discharge diagnosis-related group of 127, 291, 292, and 293). These same diagnoses criteria were used for all assessed time points. The database used in the analysis was the Cerner Health Facts® (Kansas City, MO, USA) inpatient claims database, which contains deidentified patient data from Cerner and non-Cerner participating facilities. Patient demographics, diagnoses, prescriptions, procedures, laboratory testing, hospital information, service location, and billing data from >480 contributing facilities throughout the United States were captured in the database (http://www.bridgetodata.org/node/1789). The data set used in this analysis included patients with AHF-related admissions. All-cause outcomes were not explored in this study, since only AHF-related data were captured and tracked in the data set. At the index AHF-related hospitalization, mortality due to any cause was captured. Any mortality during a HF hospitalization was captured at the 30, 180, and 365-day post-discharge follow-ups.
Patients
To be included in the analysis, patients must have had ≥1 record of an inpatient stay for AHF (primary or secondary diagnoses) between January 1, 2008, and March 30, 2011; had ≥3 records of reported serum creatinine (SCr) values for the index hospitalization, including an admission (or baseline) SCr value within the same day or day after admission; and were ≥18 years of age at the index hospitalization. Patients with any of the following were excluded from the analysis: record of elective or planned HF-related hospitalization, record of a heart transplantation procedure, diagnosis of chronic kidney disease stage 5 or end-stage renal disease requiring dialysis, diagnosis of cachexia or sarcopenia, record of death with LOS ≤1 day at index hospitalization, missing cost or utilization data, unknown sex or age indicators, missing LOS data, or hospitalization for AHF within 1 year before the index hospitalization.
Definition of WRF
Eligible patients were divided into three renal function status cohorts based on SCr measurements during the index hospitalization. Currently, there is no expert consensus on how to define WRF. In the past, many studies have utilized a SCr cutoff relative to baseline.2–5,10,11 However, there have been growing concerns that small changes in SCr could be associated with greater decreases in estimated glomerular filtration rate (eGFR).12 To adjust for this, some studies have explored using a combination of absolute SCr and a ≥25% increase from baseline to define WRF.6,13 The current study will be the first to investigate outcomes such as LOS and costs using this more comprehensive definition of WRF. The last SCr measure before discharge was considered the discharge SCr. The WRFp cohort consisted of patients who had ≥0.3 mg/dL and a ≥25% increase from baseline SCr that persisted at discharge of the index hospitalization. The WRFt cohort consisted of patients who had ≥0.3 mg/dL and a ≥25% increase from baseline SCr that did not persist at discharge from the index hospitalization. The non-WRF cohort consisted of patients not identified as either WRFp or WRFt.
Assessments
Information at the index hospitalization was collected on patient demographics, hospital characteristics, comorbidities, and HF medication utilization. The primary analysis evaluated the relationship between WRF cohorts and mortality, LOS, and inpatient service costs for the index hospitalization and all subsequent AHF-related readmissions at cumulative postdischarge time points of 30, 180, and 365 days from the index hospitalization. In addition, the relationship between WRF cohorts and the number of AHF-related readmissions within 30, 180, and 365 days postdischarge from the index hospitalization was evaluated. Secondary analyses evaluated the relationship between AHF outcomes with index admission SCr and the index admission blood urea nitrogen (BUN)/SCr ratio. Furthermore, the relationship between WRF status and eGFR threshold (< or ≥60 mL/min/1.73 m2) was determined.
Statistical analyses
Using the inclusion/exclusion criteria, a feasibility assessment determined that the sample size was large enough to ensure the study was well powered. Descriptive statistics of patient demographics, hospital characteristics, comorbidities, HF medication utilization, and secondary analyses were performed for comparison among WRF cohorts. Comparisons among all three cohorts (WRFt, WRFp, and non-WRF) and just two cohorts (WRFt and WRFp) were performed using Kruskal–Wallis or Wilcoxon Rank Sum for continuous variables and χ-square test for categorical variables.
Multivariate modeling was conducted for the primary analysis. Covariates for all models were patient demographics, comorbidities, index admission SCr, index admission BUN/SCr ratio, hospital characteristics (including the number of beds, teaching status indicator, catheterization laboratory present indicator, and diagnostic catheterization laboratory indicator), and admission source and type. Logistic regression models were constructed to compare mortality among all three cohorts, or WRFt vs WRFp, at the index hospitalization, and mortality associated with all subsequent AHF-related readmissions within 30, 180, and 365 days of discharge. Negative binomial models were constructed to compare the number of AHF-related readmissions among all three cohorts, or WRFt vs WRFp, within 30, 180, and 365 days of discharge. Generalized linear models assuming gamma distribution were constructed to compare LOS and costs among all three cohorts, or WRFt vs WRFp, at the index hospitalization and all subsequent AHF-related readmissions within a cumulative (index + readmission) 30, 180, and 365 days of discharge. Costs were normalized to 2012 US dollars using the US Medical Care Services Consumer Price Index for All Urban Consumers.
Sensitivity analyses and model diagnostics
A sensitivity analysis was conducted to account for the potential impact of early mortality that could lead to biased estimates. This analysis used the same multivariate modeling described earlier for mortality, LOS, and costs, using only the subset of patients with a live discharge from the index hospitalization.
Regression diagnostics for the negative binomial and logistic regression models included an assessment of collinearity and influence diagnostics. Robustness analyses were conducted by constructing reduced models with significant variables only (retention fixed at P<0.05) and full models with outliers/heavy influence data points removed. The results of the robustness analyses were in agreement with those of the full analyses (data not shown). Analyses were conducted using the SAS software version 9.3 (SAS Institute Inc., Cary, NC, USA).
Results
Patients
The selection process identified 55,436 patients for inclusion in the analysis, with the most critical criterion being the requirement for ≥3 records of SCr values (Figure 1). The majority of patients (n=42,507, 77%) were categorized as having non-WRF; 13% (n=7,366) and 10% (n=5,563) of patients were categorized as having WRFt and WRFp, respectively, with a total WRF prevalence of 23%.
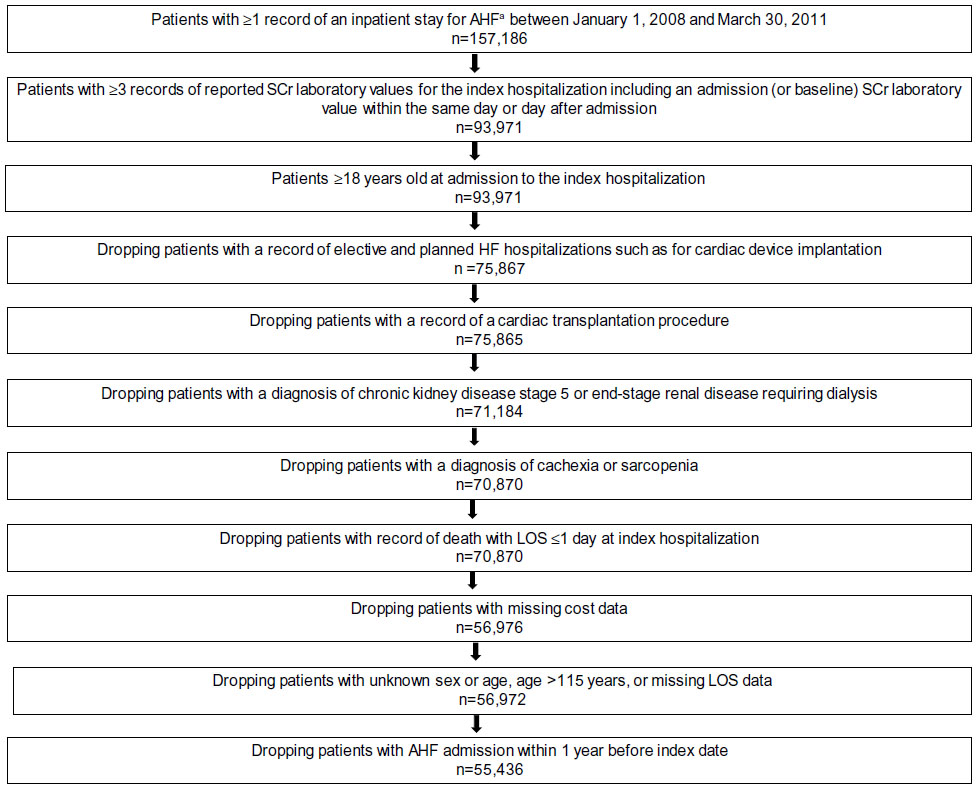 | Figure 1 Patient selection. |
For the total population, the mean age was 72.4±14.3 years, and 53% of patients were women. Patients with WRFp were older than patients with WRFt, but there was no difference in the sex distribution across cohorts (Table 1). Mean index admission SCr levels were similar among the cohorts, whereas the proportion of patients with eGFR of <60 mL/min/1.73 m2 at admission was higher in the WRFp (53.9%) and WRFt (54.3%) patients compared with the non-WRF patients (51.4%; Table 1). No meaningful conclusions could be made regarding differences among cohorts for vital signs, since these data were available only for a small percentage of patients. A higher overall comorbidity burden based on the Charlson Comorbidity Index was present in patients with WRFp compared to patients in the non-WRF and WRFt cohorts (Table 2). Patients with WRFp had significantly higher rates of cancer, sepsis, chronic liver disease, and impaired immune function, and lower rates of asthma and other respiratory conditions compared to patients with WRFt (Table 2). Non-WRF patients used fewer HF-related medications such as loop diuretics compared to patients with WRF. Patients with WRFp used less angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, and β-blockers compared to patients with WRFt (Table 2).
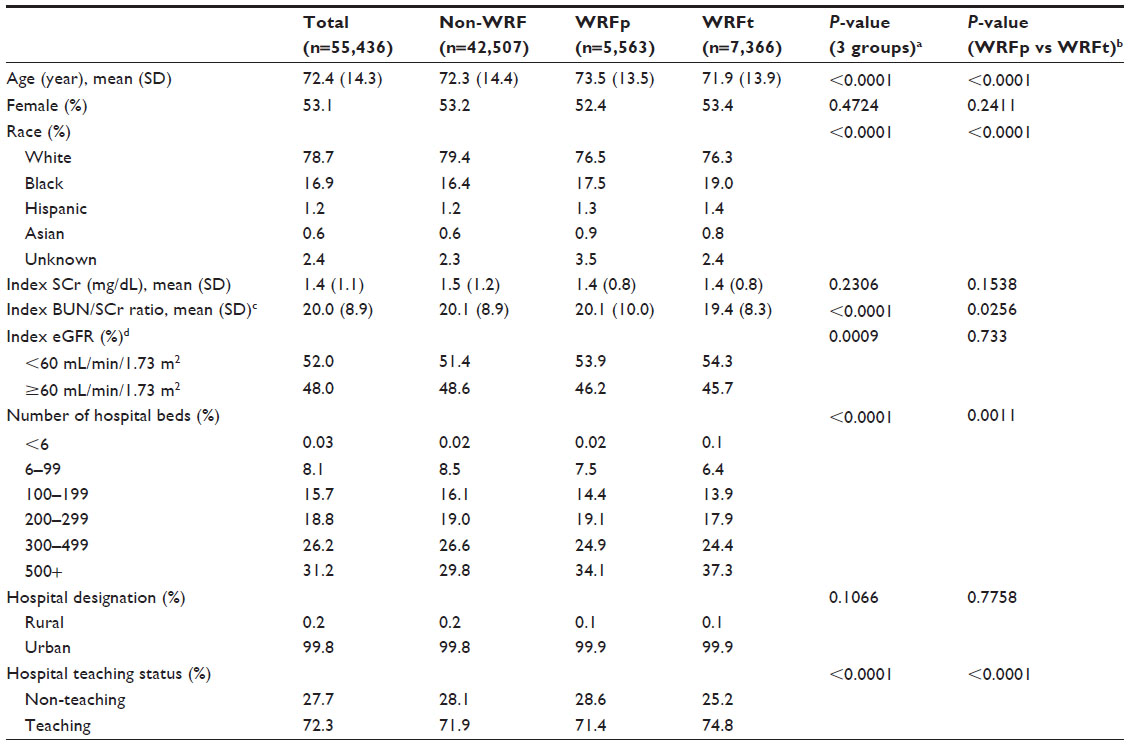 | Table 1 Patient and hospital characteristics by WRF cohort |
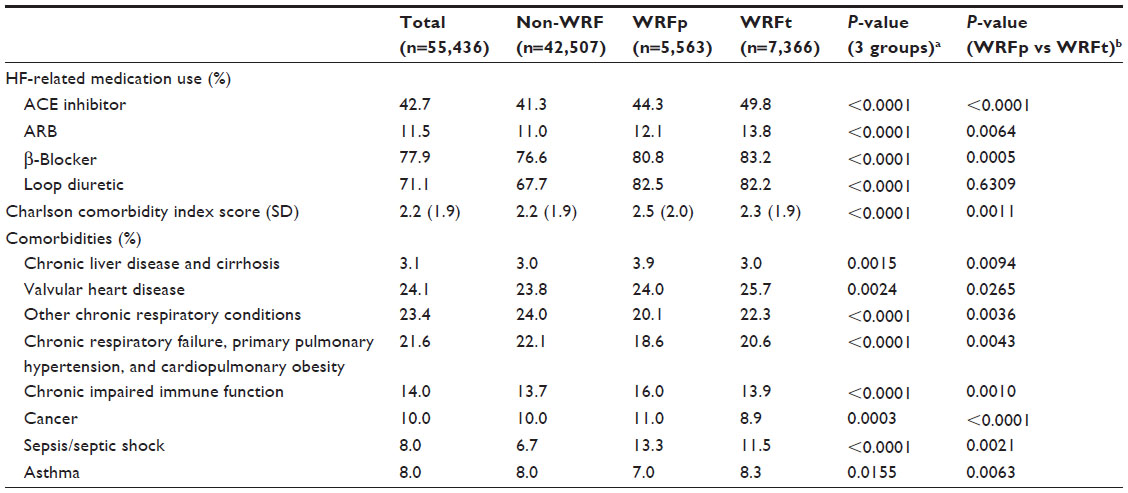 | Table 2 Medication utilization and comorbidities by WRF cohort |
Mortality
Patients with WRF had higher mortality rates than non-WRF at all time points (index, 30, 180, and 365 days postdischarge; Figure 2). The mean mortality rate at the index hospitalization was 23.6%, 5.7%, and 3.9% for the WRFp, WRFt, and non-WRF cohorts, respectively (Figure 2). When compared with the non-WRF cohort in multivariate models, the OR for mortality during the index hospitalization was 7.76 (95% CI: 7.09–8.50; P<0.0001) in the WRFp cohort and 1.20 (95% CI: 1.06–1.36; P=0.0030) in the WRFt cohort (Table 3). Patients in the WRFp cohort had greater than six times higher odds of mortality compared to those with WRFt (OR: 6.43; 95% CI: 5.63–7.34) at the index hospitalization. The greater odds with WRFp vs WRFt persisted up to a year later when looking at death during a HF-associated hospitalization (Table 3). Other significant multivariable predictors for index hospitalization mortality and HF-associated hospitalization mortality included WRFp, sepsis, cardiogenic shock, pneumonia, index admission SCr, and index admission BUN/SCr ratio. Most of the deaths (70%) occurred during the index hospitalization, which drove the cumulative mortality results.
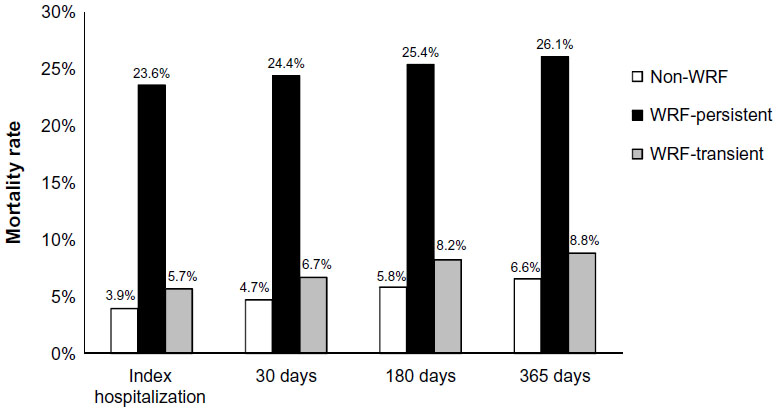 | Figure 2 Mortality rate by WRF cohort. |
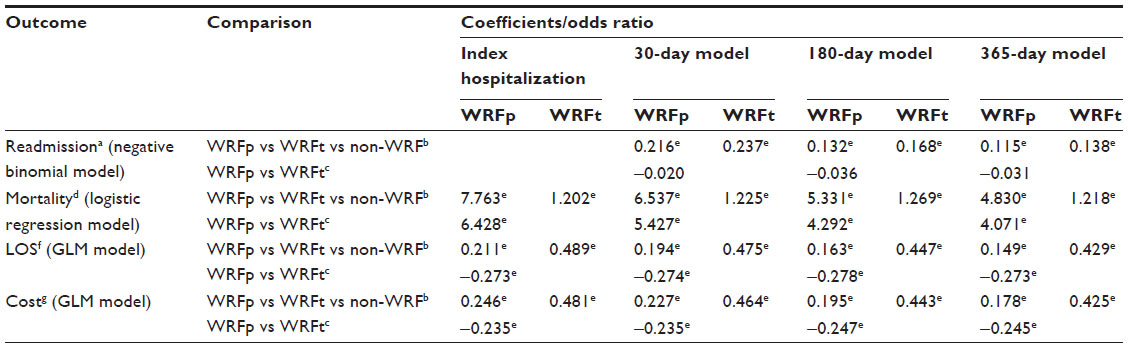 | Table 3 Statistical modeling summary |
In the sensitivity analysis, in which only the subset of patients with live discharge from the index hospitalization were evaluated, patients in the WRFt cohort had significantly higher odds ratios for mortality associated with a HF hospitalization at all time points than the reference non-WRF cohort (OR ≥1.24; P≤0.032). There was a numeric trend toward higher odds ratios for mortality associated with a HF hospitalization for the WRFp cohort as well, but statistical significance was not always reached (OR ≤1.30; P≤0.146). When patients with any WRF were combined together, they had significantly higher odds ratios for mortality associated with a HF hospitalization at 30, 180, and 365 days postdischarge compared to patients in the non-WRF cohort (OR ≥1.22; P<0.05). However, there were no significant differences in mortality associated with a HF hospitalization rates between the WRFp and WRFt cohorts at any time point in this mortality model, evaluating a subset of patients with live discharge from the index hospitalization.
Length of stay
Patients with WRFp had significantly shorter LOS at all time points compared with patients in the WRFt cohort, but had longer LOS compared with patients in the non-WRF cohort (Figure 3). The mean LOS at the index hospitalization was 10.2, 13.6, and 7.5 days for the WRFp, WRFt, and non-WRF cohorts, respectively (Figure 3). Compared with the non-WRF cohort in multivariate models, the index hospitalization LOS was significantly longer for the WRFp cohort (P<0.0001) and for the WRFt cohort (P<0.0001; Table 3). Compared with the WRFp cohort, the index hospitalization LOS was significantly longer for the WRFt cohort (P<0.0001; Table 3). This longer LOS for WRFt patients was observed at all time points (Table 3). Other significant multivariable predictors for LOS included WRFp, sepsis, pneumonia, acute cerebrovascular disease, WRFt, and cardiogenic shock. As with the mortality results, most of the inpatient stay (75%) during the 365-day follow-up occurred during the index hospitalization, which drove the cumulative LOS results.
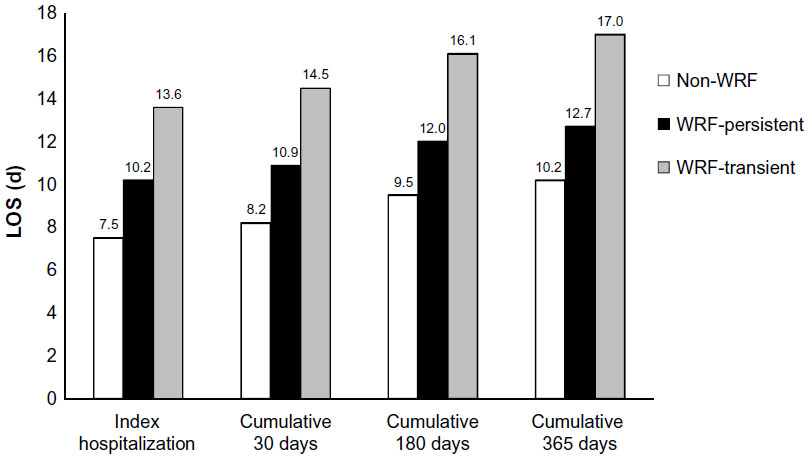 | Figure 3 LOS by WRF cohort. |
In the sensitivity analyses, the same LOS pattern (WRFt > WRFp > non-WRF) with respect to cohort was observed in patients with live index discharges and for the total population. Compared with the non-WRF cohort, the LOS was significantly longer for both WRFp and WRFt patients at all time points (P<0.0001). Compared with the WRFp cohort, LOS was significantly longer for the WRFt cohort at all time points (P<0.0001).
Costs
Patients with WRFp had significantly lower costs at all time points compared to patients with WRFt, but higher costs compared to patients in the non-WRF cohort (Figure 4). The mean index hospitalization costs were $29,252, $38,412, and $20,137 for the WRFp, WRFt, and non-WRF cohorts, respectively (Figure 4). Compared with the non-WRF cohort in multivariate models, the index hospitalization costs were significantly higher for the WRFp cohort (P<0.0001) and for the WRFt cohort (P<0.0001; Table 3). Compared with the WRFp cohort, the index hospitalization costs were significantly higher for patients in the WRFt cohort (P<0.0001; Table 3). Similar results were seen for the other time points (Table 3). Other significant multivariable predictors for cost included WRFt, sepsis, cardiogenic shock, pneumonia, emergency admission, geographic region, and index year. As with mortality and LOS, most of the costs (78%) occurred during the index hospitalization, which drove the cumulative cost results.
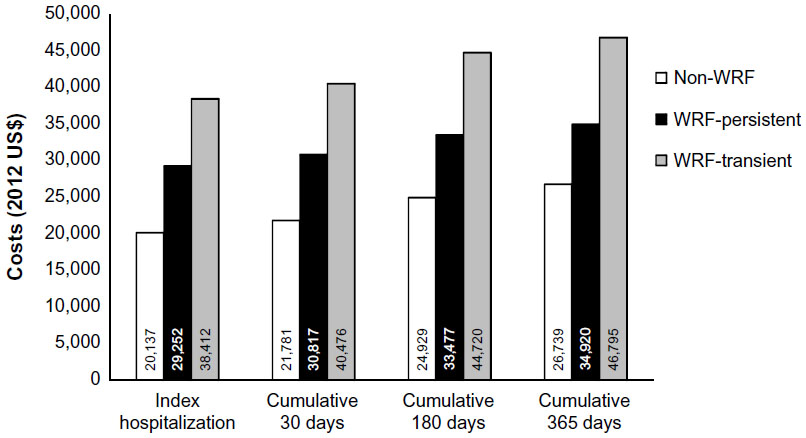 | Figure 4 Cost by WRF cohort. |
In the sensitivity analyses, the same cost pattern (WRFt >WRFp >non-WRF) with respect to cohort was observed in patients with live index discharges and for the total population. Compared with the non-WRF cohort, the costs were significantly higher for both WRFp and WRFt patients at all time points (P<0.0001). Compared with the WRFp cohort, costs were significantly higher for the WRFt cohort at all time points (P<0.0001).
Hospital readmissions
Patients with WRFp and WRFt had a significantly higher number of AHF-related readmissions at all time points compared to patients in the non-WRF cohort; however, there was no difference between the WRFp and WRFt cohorts (Figure 5). The mean number of readmissions at 30 days postdischarge was 0.12, 0.12, and 0.09 for the WRFp, WRFt, and non-WRF cohorts, respectively (Figure 5). Compared with the non-WRF cohort in multivariate models, the readmission count at 30 days postdischarge was significantly higher for the WRFp cohort (P<0.0001) and the WRFt cohort (P<0.0001; Table 3). Other significant multivariable predictors for readmission included WRFp, WRFt, atrial fibrillation, BUN/SCr ratio, index year, and admission source. Nearly one-quarter (24%) of the readmissions occurred during the first 30 days postdischarge.
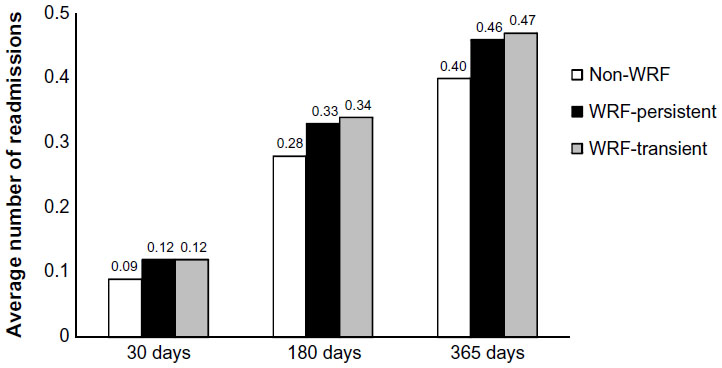 | Figure 5 AHF-related hospital readmissions by WRF cohort. |
Secondary analyses
Results from the secondary analyses showed that there was no difference in the average index admission (within the same day or the day after admission) SCr among cohorts (Table 1), although the distribution was significantly different, with non-WRF having a higher percentage of patients at the extremes of higher and lower index admission levels. Index admission SCr was a significant predictor of mortality, LOS, and costs after controlling for other factors. The average index admission BUN/SCr ratio was significantly higher in the WRFp and non-WRF cohorts compared with the WRFt cohort (Table 1), and was a significant predictor for mortality, LOS, costs, and readmissions. The index admission eGRF was available only for 48% of patients. This parameter was significantly higher in the non-WRF cohort than in the WRFp and WRFt cohorts; however, there was no significant difference in the probability of belonging to the higher eGFR (≥60 mL/min/1.73 m2) group between the WRFp and WRFt cohorts (Table 1).
Discussion
In this retrospective analysis of patients hospitalized for AHF, patients in the WRFp cohort had significantly higher mortality rates compared with patients in the non-WRF and WRFt cohort, whereas patients in the WRFt cohort had significantly longer LOS and costs compared with patients in the non-WRF and WRFp cohorts. Although any WRF was associated with a higher number of AHF-related readmissions, there was no difference between the WRFp and WRFt cohorts.
The mortality rate was strikingly higher in the WRFp cohort compared with the other cohorts. This finding may have been driven by the definitions used to characterize the WRF status cohorts. In 2002, Gottlieb et al11 demonstrated that a definition for WRF of change from baseline SCr ≥0.3 mg/dL was both sensitive and specific for mortality and LOS. Since then, many studies have used this definition, but due to the exponential relationship between eGFR and SCr, absolute changes in SCr are not equivalent in scale to changes in eGFR.12 To address this issue, we used an updated and more clinically rigorous definition for WRF that used both an absolute change in SCr ≥0.3 mg/dL and a relative change in SCr ≥25%.6 The use of this definition may have resulted in fewer patients being identified as having WRF. It is also possible that unmeasured factors that were not specifically addressed in this analysis (ie, concomitant chemotherapy, high- or low-protein diets, certain medications, etc) may have altered SCr levels, which would have affected WRF status.
Although the mortality rate was much higher in the WRFp cohort compared with the WRFt cohort, it is still notable that the mortality risk in the WRFt cohort was also significantly higher than the non-WRF cohort. This result is in agreement with that of a retrospective database study of Medicare patients reported by Krishnamoorthy et al,9 who found that both WRFt and WRFp (WRF defined as increase of SCr ≥0.3 mg/dL) were associated with a significant risk of 90-day all-cause mortality, although the risk with WRFp was 46% higher compared with WRFt. A study reported by Logeart et al7 also determined that both WRFt and WRFp (WRF defined as increase of SCr ≥25 μmol/L [>0.28 mg/dL]) in patients hospitalized for AHF were significantly predictive of worse outcomes (outcome of combined death and readmissions) 6 months postdischarge. Our findings on the increased risk of mortality in the WRFt cohort is in contrast to those of Aronson and Burger,8 who found that patients hospitalized for AHF with WRFt (WRF defined as increase of SCr ≥0.5 mg/dL) did not have significantly increased mortality 6 months postdischarge. In the current study, we also demonstrated that WRFt was associated with significantly higher LOS and costs compared with non-WRF and WRFp. These data indicate that negative outcomes are associated with WRFt and not just WRFp, and further investigation is needed for this population.
Patients in the WRFt and WRFp cohorts had higher rates of 30-day readmissions compared with patients in the non-WRF cohort. In agreement with these results, in another retrospective claims database analysis of 20,063 patients, WRF was shown to increase the 30-day readmission risk in patients hospitalized for AHF.14 In contrast, a prospective study of 299 patients found no association between WRF and 30-day readmission in patients hospitalized for AHF.4 Per the Patient Protection and Affordable Care Act, Medicare reimbursement funds are decreased for hospitals with excessive 30-day readmission rates for AHF. The only other study that has investigated readmissions based on WRF persistence found no significant difference by adjusted analyses for either WRFt or WRFp in 90-day all-cause readmission or HF-related readmission.9 Although the published data seem contradictory, the discrepancies may be due to the slightly varying definitions used for WRF; the definition in the current study was more stringent than the other three studies that investigated readmissions, requiring both an absolute and percentage increase in SCr. The results of the current study add to previous studies by showing that WRF status may be a possible indicator of risk for 30-day readmission for AHF.
Most of the observed deaths, costs, and inpatient stay days occurred during the index hospitalization, which drove the cumulative results for the 30, 180, and 365 day time points. In sensitivity analyses that excluded patients who died during the index hospitalization, the presence of any WRF remained (postindex hospitalization) significantly associated with increased mortality associated with a HF hospitalization at all time points. However, although WRFp was highly associated with index hospitalization mortality, there was no longer a difference in postindex mortality associated with a HF hospitalization between the WRFp and WRFt cohort. The pattern of LOS and costs among cohorts in patients with live discharge remained the same as the total population (ie, significantly higher for patients in the WRFt cohort compared with the other cohorts), indicating that differences in mortality rates at the index hospitalization did not drive the LOS and cost results. The observation that cost and LOS were similar in the total population and patients with live discharge was not unexpected since 94% of all patients had a live discharge. These data indicate that even transient increases in SCr appear to be associated with detrimental outcomes, such as longer LOS and higher costs when compared to patients with persistent increases. Post hoc analyses of a randomized, multicenter trial found that any change in renal function (either improved or worsened) with AHF was associated with longer LOS and increased mortality compared with stable renal function.15 Thus, any change in renal function, regardless of improved, worsened, transient, or persistent, appears to be associated with poor outcomes.
There are several strengths of this study including the use of data from a large multicenter database, the use of a stringent definition for WRF, and the assessment of both short- and long-term outcomes. Another notable strength of this study is the characterization of WRFt vs WRFp. The results of this study indicate that there is indeed a difference in outcomes based on persistence of WRF; however, both WRFp and WRFt were associated with negative outcomes.
In a meta-analysis of 16 studies, a significant linear relationship was found between SCr levels and mortality risk in patients with AHF.16 To determine if this relationship also applied to other biomarkers of renal function, we conducted secondary analyses of outcomes using index BUN/SCr ratio. After controlling for WRF status and other covariates, the index BUN/SCr ratio appeared to be a strong predictor of all outcomes.
This study was limited by issues that apply to all retrospective database analyses, including the inability to determine and account for clinical factors, and the potential for miscoding of diagnoses or resource utilization procedures. The database is also limited, in that only data from patients that went to Cerner reporting hospitals were captured, and the majority of these reporting hospitals are teaching hospitals where the patient mix and practice patterns may be different than other hospitals. Furthermore, no data from hospitalizations outside the Cerner reporting hospitals were captured. An additional limitation is that only the inpatient experience of the patient was captured. Thus, if a patient died after discharge, additional data could not be captured and the patient was lost to follow-up. Furthermore, the data set used in this analysis was only for patients hospitalized for AHF; therefore, no data on all-cause outcomes were assessed, which may have shed some additional light on the impact on outcomes due to renal dysfunction. Finally, other AHF physiologic processes other than renal status that were not assessed in this study may be driving outcomes.
Conclusion
In patients hospitalized for AHF, WRFp was associated with the highest mortality rate, whereas WRFt was associated with the highest costs and LOS. WRF patients had higher readmission rates than non-WRF patients. Notably, transient increases in SCr appear to be associated with detrimental outcomes, especially longer LOS and higher costs. Further research is needed to understand the basis for these findings.
Acknowledgments
Medical writing and editorial assistance was provided by Erin P Scott, PhD, of Scott Medical Communications, LLC. This assistance and study were funded by Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA. The study sponsor participated in the study design, interpretation of the data, and critical review of the manuscript. The final decision to submit the manuscript was made by the authors.
Author contributions
JBP, KWJ, and SSG contributed to the study design and interpretation of the data. HSF and PN contributed to data analysis and interpretation of the data. All authors participated in critically reviewing the manuscript for intellectual content, approved the final version for submission, and agreed to be accountable for all aspects of the work.
Disclosure
JBP and KWJ are employees of Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA. HSF and PN are paid consultants for Novartis Pharmaceuticals Corporation. SSG received grant support from Novartis and has served as a consultant for Novartis, BMS, and Gambro. The authors report no other conflicts of interest in this work.
References
Damman K, Valente MA, Voors AA, et al. Renal impairment, worsening renal function, and outcome in patients with heart failure: an updated meta-analysis. Eur Heart J. 2014;35(7):455–469. | |
Forman DE, Butler J, Wang Y, et al. Incidence, predictors at admission, and impact of worsening renal function among patients hospitalized with heart failure. J Am Coll Cardiol. 2004;43(1):61–67. | |
Breidthardt T, Socrates T, Noveanu M, et al. Effect and clinical prediction of worsening renal function in acute decompensated heart failure. Am J Cardiol. 2011;107(5):730–735. | |
Cowie MR, Komajda M, Murray-Thomas T, et al. Prevalence and impact of worsening renal function in patients hospitalized with decompensated heart failure: results of the prospective outcomes study in heart failure (POSH). Eur Heart J. 2006;27(10):1216–1222. | |
Herout PM, Harshaw Q, Phatak H, et al. Impact of worsening renal function during hospital admission on resource utilization in patients with heart failure. Am J Cardiol. 2010;106(8):1139–1145. | |
Metra M, Nodari S, Parrinello G, et al. Worsening renal function in patients hospitalised for acute heart failure: clinical implications and prognostic significance. Eur J Heart Fail. 2008;10(2):188–195. | |
Logeart D, Tabet JY, Hittinger L, et al. Transient worsening of renal function during hospitalization for acute heart failure alters outcome. Int J Cardiol. 2008;127(2):228–232. | |
Aronson D, Burger AJ. The relationship between transient and persistent worsening renal function and mortality in patients with acute decompensated heart failure. J Card Fail. 2010;16(7):541–547. | |
Krishnamoorthy A, Greiner MA, Sharma PP, et al. Transient and persistent worsening renal function during hospitalization for acute heart failure. Am Heart J. 2014;168(6):891–900. | |
Amin AP, Spertus JA, Reid KJ, et al. The prognostic importance of worsening renal function during an acute myocardial infarction on long-term mortality. Am Heart J. 2010;160(6):1065–1071. | |
Gottlieb SS, Abraham W, Butler J, et al. The prognostic importance of different definitions of worsening renal function in congestive heart failure. J Card Fail. 2002;8(3):136–141. | |
Stevens LA, Coresh J, Greene T, Levey AS. Assessing kidney function – measured and estimated glomerular filtration rate. N Engl J Med. 2006;354(23):2473–2483. | |
Damman K, Jaarsma T, Voors AA, et al. Both in- and out-hospital worsening of renal function predict outcome in patients with heart failure: results from the Coordinating Study Evaluating Outcome of Advising and Counseling in Heart Failure (COACH). Eur J Heart Fail. 2009;11(9):847–854. | |
Patel UD, Greiner MA, Fonarow GC, et al. Associations between worsening renal function and 30-day outcomes among Medicare beneficiaries hospitalized with heart failure. Am Heart J. 2010;160(1):132–138. e1. | |
Testani JM, McCauley BD, Kimmel SE, Shannon RP. Characteristics of patients with improvement or worsening in renal function during treatment of acute decompensated heart failure. Am J Cardiol. 2010;106(12):1763–1769. | |
Smith GL, Lichtman JH, Bracken MB, et al. Renal impairment and outcomes in heart failure: systematic review and meta-analysis. J Am Coll Cardiol. 2006;47(10):1987–1996. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.