Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 13
Association of MDM4 Gene rs4245739 Polymorphism with the Risk and Clinical Characteristics of Colorectal Cancer in a Chinese Han Population
Authors Zhao DM, Diao YE, Xu Q
Received 28 April 2020
Accepted for publication 7 September 2020
Published 26 November 2020 Volume 2020:13 Pages 673—678
DOI https://doi.org/10.2147/PGPM.S260209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
De-Ming Zhao,1 Yu-E Diao,2 Qing Xu3
1Department of Gastrointestinal Surgery, Dalian Municipal Central Hospital, Dalian, People’s Republic of China; 2Department of General Surgery, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China; 3Department of Anorectal Surgery, Nantong Third People’s Hospital, Nantong University, Nantong, Jiangsu, People’s Republic of China
Correspondence: Qing Xu Tel/Fax +86-513-89093902
Email [email protected]
Background: Studies show that MDM4 may play a pivotal role in colorectal cancer (CRC). Recently, a host of studies suggest that MDM4 gene rs4245739 polymorphism may modify the risk of different cancers.
Methods: In this study, we were interested whether MDM4 gene rs4245739 polymorphism correlated with the risk and clinical characteristics of CRC. Logistic regression was adopted to estimate the association of rs4245739 polymorphism and CRC risk.
Results: We enrolled 444 CRC patients and 530 controls and found MDM4 gene rs4245739 polymorphism may decrease the risk of CRC. Stratified analyses uncovered that this variant was connected to a less risk of CRC in females, non-drinkers, non-smokers, and people under 60 years old. Additionally, rs4245739 polymorphism was related to TNM staging, pathological type, tumor size, and location of CRC. Furthermore, this polymorphism was significantly linked with the survival of CRC.
Conclusion: Totally, this study suggests that MDM4 rs4245739 polymorphism is linked with the risk and clinical characteristics of CRC.
Keywords: MDM4, colorectal cancer, case–control study, rs4245739, polymorphism
Introduction
Colorectal cancer (CRC) is one of the most frequently diagnosed cancers and is the fourth most mortal cancer with an annual rate of almost 900,000 CRC-related deaths worldwide.1 The global new CRC patients are predicted to roar by 60% to above 2,200,000 in 2030, with 1,100,000 deaths caused by CRC.2 CRC ranks the 5th and 4th most dominant cancer in males and females in China, respectively.3 Up to date, the pathogenesis of CRC is still unclear. Both genetic factors and environmental risk factors including poor diets, obesity, alcohol consumption, smoking, and lacking of exercise were reportedly associated with CRC risk.4,5 A host of studies have identified novel gene loci associated with CRC susceptibility.6–11
P53, a tumor suppressor gene, plays a crucial role in multiple physiological processes, including cell cycle initiation and arrest, DNA lesion repair, signal pathway of apoptosis, autophagy, metabolism, and oxidative status.12,13 The main process of p53 degradation is ubiquitin-mediated proteolysis. One of the ubiquitin-labeled p53 enzymes is mouse double minute (MDM)-2 protein. MDM2 and its homolog MDM4 have very similar protein structures and both have an N-terminus, a region containing p53-binding domain.14 The activity of p53 is negatively regulated by the interaction between MDM2 and MDM4.15–17 MDM4 can directly connect to MDM2 to suppress its decomposition, which impacts the inhibitory effects of MDM2 on p53 activity.18 MDM4 is associated with tumor formation via restraining p53 tumor suppressor activity.19–21 Double knockdown of MDM4 and MDM2 can enhance the antitumor activity of 5-fluorouracil in colon cancer cells.22 MDM4 may be critical in colorectal carcinogenesis.23
MDM4 gene is located on chromosome 1q32. Recently, some studies investigated the potential link between MDM4 gene rs4245739 polymorphism and the risk of various cancers.24,25 Among these studies, only the Norwegian study by Gansmo et al probed into the connection between MDM4 gene rs4245739 polymorphism and CRC risk; however, they found no connection.26 In addition, no Chinese study interpreted the relationship between CRC risk and MDM4 gene rs4245739 polymorphism among Chinese individuals. Thus, we performed this study to address the connection between this variant and CRC susceptibility in a Chinese population.
Patients and Methods
Subjects
Totally 444 CRC patients and 530 volunteers were enrolled from Dalian Municipal Central Hospital and Nantong Third People’s Hospital. No CRC patient had undergone radio- or chemo-therapy. Diagnosis of CRC was made histopathologically. Clinicopathologic data of all participants were acquired from medical records. Qualified controls were chosen from the same area within the same period. All enrolled participants were more than 18 years old. Approval was given by the Ethics committees of the tested Hospitals, and Declaration of Helsinki was followed. All subjects provided written informed consent.
Blood Collecting and Genotyping
Peripheral blood (2 mL) was collected from all participants, and DNA was isolated from its leukocytes using a DNA purifying Kit (Tiangen Biotech) as instructed by the manufacturer. A matrix-supported laser desorption/ionization time-of-flight mass spectrometer on a MassARRAY system (Sequenom, San Diego, CA, USA) was adopted for genotyping. The primers of GTAGTACGAACATAAAAATGCATT TATCCA (forward) and ATTTTCAAATAATGTGGTAAGTGAGCG (reverse) were used for nucleotide extension. Each PCR involved a mixture (25 ul) of genotyping assays (20×, 1.25 ul), DNA (20 ng) and genotyping master mix (2×, 12.5 ul). PCR procedures were denaturing at 96 °C, 5 min; 35 cycles, 96 °C for 30 s, annealing at 57 °C, 40 s; elongating at 72 °C for 5 min. Genotyping accuracy was guaranteed by randomly choosing 1/10 of the specimens for secondary testing.27 The results were 100% consistent.
Statistical Analyses
All statistical analyses were carried out on SPSS 22.0 (SPSS Inc., Chicago, USA) at the significance level of P < 0.05. Categorical and continuous data were examined by Chi-square (χ2) test and Student’s t-test, respectively. Hardy–Weinberg equilibrium (HWE) was assessed using χ2-test. The genotype and allele type allocations between groups were compared via logistic regression by calculating the odds ratios (ORs) and 95% confidence intervals (CIs) with or without adjustment. Stratification was done by sex, age, drinking and smoking status. Additionally, the exposure combined models were assessed by logistic regression. Overall survival (OS) was defined by the Kaplan–Meier approach.
Results
Characteristics of Subjects
Demographic and clinical information of the subjects is listed in Table 1. No differences between the two groups were identified for age, smoking, sex, or alcohol. In terms of site of cancer, there were 290 with rectal cancer and 154 patients with colon cancer. The 444 CRC patients consisted of 95.4% adenocarcinoma (424), 3.2% squamous cell carcinoma (14), and 1.4% other types (6). We also investigated tumor node metastasis (TNM) stage, tumor size, and family history of CRC patients.
 |
Table 1 Demographic Information and Risk Factors for Colorectal Cancer and Control |
Connection Between CRC Risk and MDM4 Gene rs4245739 Polymorphism
The genotype and allele allocations of the tested polymorphism differed considerably between the CRC patients and controls (Table 2). The HWE test showed no evident bias in genotypic frequency among the controls. Individuals with AC and CC genotype were at lower risk of developing CRC (AC vs AA: OR, 0.76; 95%CI, 0.57-1.00; P = 0.046; CC vs AA: OR, 0.47; 95% CI, 0.23–0.97; P = 0.036). The presence of CC+AC genotype or C allele demonstrated a significantly lower risk for CRC. These results were also true in dominant and homozygote models after age and gender adjustment. We then further evaluated the role of MDM4 gene rs4245739 in the risk of CRC stratified by sex, age, alcohol and smoking (Table 3). Non-drinkers, non-smokers, women, and youngsters (age <60 years) were found with significantly less risk of CRC.
 |
Table 2 Genotype Frequencies of MDM4 Gene Rs4245739 Polymorphism in Cases and Controls |
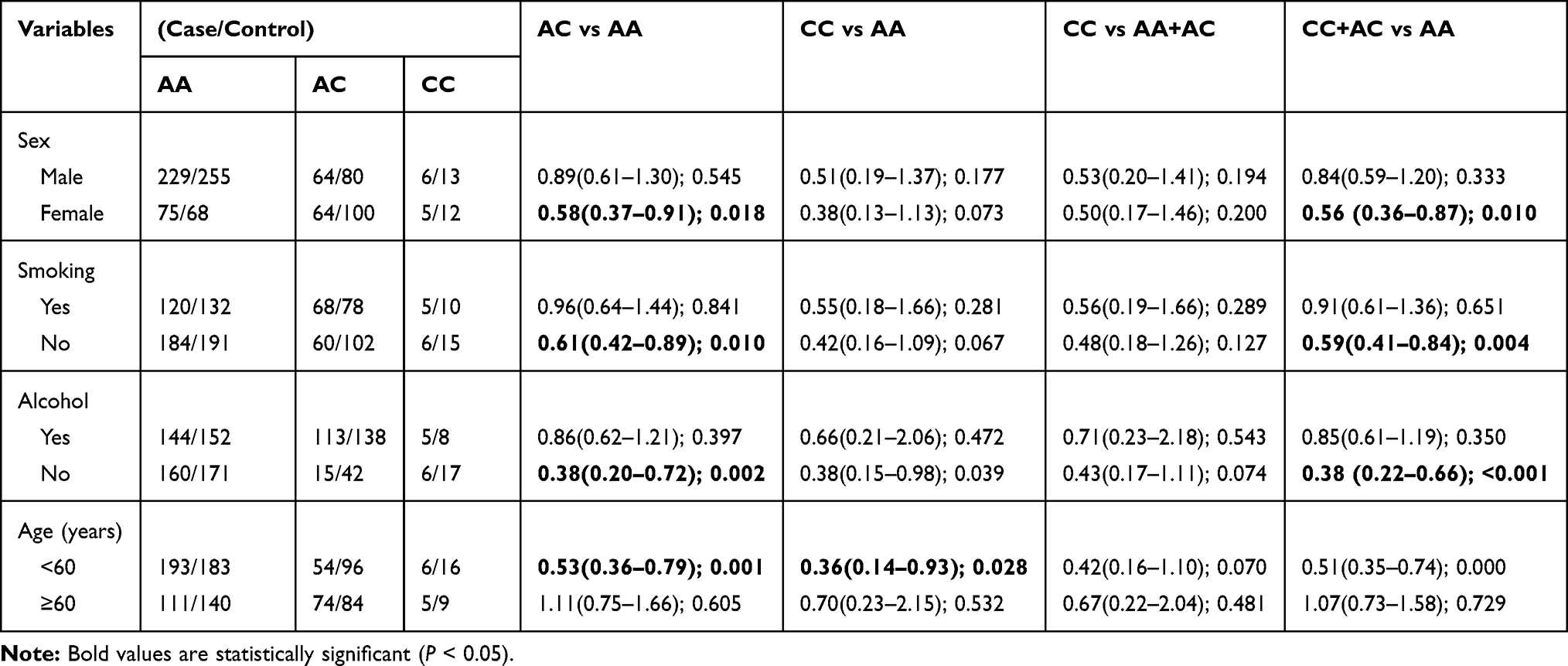 |
Table 3 Stratified Analyses Between MDM4 Gene Rs4245739 Polymorphism and the Risk of Colorectal Cancer |
Correlation Between MDM4 Gene rs4245739 and Clinicopathological Data of CRC Patients
Then, the connection between the tested polymorphism and clinical data of CRC patients was assessed. MDM4 gene rs4245739 polymorphism was connected to the histological grade, TNM stage, and tumor size of CRC (Table 4).
 |
Table 4 The Associations Between MDM4 Rs4245739 Polymorphism and Clinical Characteristics of Colorectal Cancer |
Survival Analysis of MDM4 Gene rs4245739 Polymorphism with CRC Patients
We explored the relationship between this variant and the prognosis of CRC patients. For the tested polymorphism, Kaplan-Meier single-factor analysis showed AC genotype carriers relative to AA genotype enjoyed significantly better OS (HR, 0.66, 95% CI, 0.47–0.93; log-rank P = 0.018, Figure 1).
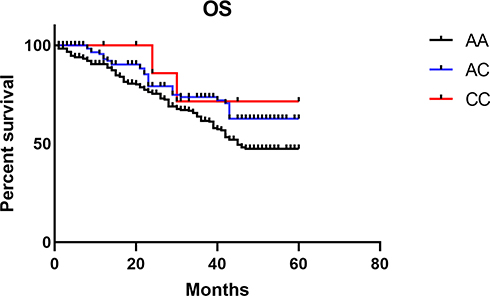 |
Figure 1 Kaplan–Meier analysis of overall survival of CRC patients with MDM4 gene rs4245739 polymorphism. |
Discussion
Herein, this study showed that MDM4 gene rs4245739 polymorphism was related to decreased risk and prognosis for CRC in Chinese subjects. Stratified analyses indicated the C allele from this single nucleotide polymorphism (SNP) has a protective role in CRC among females, non-drinkers, non-smokers, and those at age <60 years. Furthermore, the tested polymorphism was linked with the survival of CRC.
Several studies focused on the connection between MDM4 gene rs4245739 polymorphism and cancer risk. Zhou et al firstly observed that MDM4 rs4245739 polymorphism decreased the risk of esophageal squamous cell carcinoma (ESCC) and assumed that rs4245739 polymorphism can interrupt the miRNA-regulated gene regulation, which can modify ESCC risk.28 They subsequently reported an association between MDM4 rs4245739 polymorphism and a lower risk of breast cancer (BC) in a study with 1,100 BC patients and 1,400 controls in China.29 As for BC, conflicting results were obtained in other studies. Gansmo et al indicated that C allele of rs4245739 polymorphism reduced the risk for BC marginally in a population from Norway.26 Two studies from Iran did not obtain any association between this SNP and BC risk.30,31 However, a genome-wide association study with 10,707 BC and 76,646 controls identified rs4245739 polymorphism as an important estrogen receptor (ER) negative–specific BC risk locus.32 Differences in BC types, sample sizes and races may contribute to these inconsistent findings regarding BC. As for other types of cancers, Fan et al showed MDM4 rs4245739 polymorphism decreased the risk of non-Hodgkin lymphoma.33 Gao et al observed that this SNP increased susceptibility to small cell lung cancer.34 Mohammad Khanlou et al. revealed that MDM4 rs4245739 polymorphism did not associate with the risk of thyroid cancer among Iranian-Azeri patients.35 Different from the study by Gansmo et al from Norway,26 we recognized a relationship of MDM4 rs4245739 polymorphism with decreased risk for CRC in Chinese Han population. Gansmo et al suggested this SNP was not associated with CRC risk,26 but they only investigated colon cancer and ignored rectal cancer.26 Obviously, the sample sizes and ethnicities were both different between our study and the Norwegian study. Another point was that eating habits and living environments were different. These above factors may explain the conflicting findings. Due to these paradoxical results, Wang et al conducted a meta-analysis to address this issue and found that rs4245739 polymorphism decreased the risk of overall cancer,36 which was in line with our study.
Next, the stratified analyses of some factors found that MDM4 rs4245739 polymorphism correlated with a lower risk of CRC in females, non-smokers, non-drinkers, and those at age <60 years old, which suggested these exposure risk factors probably interact with the rs4245739 polymorphism. In addition, we evaluated the link of this polymorphism with clinicopathological data of CRC patients. The tested polymorphism in CRC patients was correlated to the tumor size, TNM stage, pathological type, and location of CRC. Reportedly, the MDM-4 oncogene rs4245739 SNP set up an unsuitable miR-191 target location and was related to both overall and disease-free survivals of ovarian cancer among Caucasians.37 MDM4 rs4245739 AC/CC genotypes were also significantly related to better overall, disease-specific, and disease-free survival.38 We observed that AC genotype carriers showed better OS compared with AA genotype carriers. As far as we know, we uncover a connection of rs4245739 polymorphism with the survival of CRC for the first time.
This study harbors some limitations. First, the moderately large sample size may decrease the power value of this study. Second, only one SNP in the MDM4 gene was investigated. Third, there were insufficient follow-up data of CRC patients. Fourth, we only recruited the Han Chinese population. Last, functional experiments should be conducted to further investigate the roles of this SNP in the pathogenesis of CRC.
To sum up, MDM4 gene rs4245739 polymorphism is linked with the risk and prognosis of CRC, and the C allele has a protective role in CRC risk and prognosis particularly. Further researches in other populations are warranted to validate these findings.
Acknowledgments
No funds.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019;394(10207):1467–1480. doi:10.1016/S0140-6736(19)32319-0
2. Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut. 2017;66(4):683–691. doi:10.1136/gutjnl-2015-310912
3. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
4. Wong SH, Yu J. Gut microbiota in colorectal cancer: mechanisms of action and clinical applications. Nat Rev Gastroenterol Hepatol. 2019;16(11):690–704. doi:10.1038/s41575-019-0209-8
5. Keum N, Giovannucci E. Global burden of colorectal cancer: emerging trends, risk factors and prevention strategies. Nat Rev Gastroenterol Hepatol. 2019;16(12):713–732. doi:10.1038/s41575-019-0189-8
6. Huyghe JR, Bien SA, Harrison TA, et al. Discovery of common and rare genetic risk variants for colorectal cancer. Nat Genet. 2019;51(1):76–87. doi:10.1038/s41588-018-0286-6
7. Zhang B, Jia WH, Matsuda K, et al. Large-scale genetic study in East Asians identifies six new loci associated with colorectal cancer risk. Nat Genet. 2014;46(6):533–542. doi:10.1038/ng.2985
8. Law PJ, Timofeeva M, Fernandez-Rozadilla C, et al. Association analyses identify 31 new risk loci for colorectal cancer susceptibility. Nat Commun. 2019;10(1):2154. doi:10.1038/s41467-019-09775-w
9. Lu Y, Kweon SS, Tanikawa C, et al. Large-scale genome-wide association study of east asians identifies loci associated with risk for colorectal cancer. Gastroenterology. 2019;156(5):1455–1466. doi:10.1053/j.gastro.2018.11.066
10. Wan Q, Zhang D, Zhou Q, et al. Association of CD44 gene rs187115 polymorphism with colorectal cancer risk and prognosis in Chinese Han population: a case-control study. Aging (Albany NY). 2019;11(21):9616–9625. doi:10.18632/aging.102408
11. Qian H, Zhang D, Bao C. Two variants of Interleukin-1B gene are associated with the decreased risk, clinical features, and better overall survival of colorectal cancer: a two-center case-control study. Aging (Albany NY). 2018;10(12):4084–4092. doi:10.18632/aging.101695
12. Hafner A, Bulyk ML, Jambhekar A, Lahav G. The multiple mechanisms that regulate p53 activity and cell fate. Nat Rev Mol Cell Biol. 2019;20(4):199–210. doi:10.1038/s41580-019-0110-x
13. Brady CA, Attardi LD. p53 at a glance. J Cell Sci. 2010;123(Pt15):2527–2532. doi:10.1242/jcs.064501
14. Marine JC, Dyer MA, Jochemsen AG. MDMX: from bench to bedside. J Cell Sci. 2007;120(Pt 3):371–378. doi:10.1242/jcs.03362
15. Li H, Zhang J, Tong JHM, et al. Targeting the oncogenic p53 mutants in colorectal cancer and other solid tumors. Int J Mol Sci. 2019;20:23. doi:10.3390/ijms20235999
16. Junttila MR, Evan GI. p53–a Jack of all trades but master of none. Nat Rev Cancer. 2009;9(11):821–829. doi:10.1038/nrc2728
17. Shvarts A, Steegenga WT, Riteco N, et al. MDMX: a novel p53-binding protein with some functional properties of MDM2. EMBO J. 1996;15(19):5349–5357.
18. Tanimura S, Ohtsuka S, Mitsui K, Shirouzu K, Yoshimura A, Ohtsubo M. MDM2 interacts with MDMX through their RING finger domains. FEBS Lett. 1999;447(1):5–9. doi:10.1016/s0014-5793(99)00254-9
19. Danovi D, Meulmeester E, Pasini D, et al. Amplification of Mdmx (or Mdm4) directly contributes to tumor formation by inhibiting p53 tumor suppressor activity. Mol Cell Biol. 2004;24(13):5835–5843. doi:10.1128/MCB.24.13.5835-5843.2004
20. Xiong S, Pant V, Suh YA, et al. Spontaneous tumorigenesis in mice overexpressing the p53-negative regulator Mdm4. Cancer Res. 2010;70(18):7148–7154. doi:10.1158/0008-5472.CAN-10-1457
21. Valentin-Vega YA, Barboza JA, Chau GP, El-Naggar AK, Lozano G. High levels of the p53 inhibitor MDM4 in head and neck squamous carcinomas. Hum Pathol. 2007;38(10):1553–1562. doi:10.1016/j.humpath.2007.03.005
22. Imanishi M, Yamamoto Y, Wang X, et al. Augmented antitumor activity of 5-fluorouracil by double knockdown of MDM4 and MDM2 in colon and gastric cancer cells. Cancer Sci. 2019;110(2):639–649. doi:10.1111/cas.13893
23. Suda T, Yoshihara M, Nakamura Y, et al. Rare MDM4 gene amplification in colorectal cancer: the principle of a mutually exclusive relationship between MDM alteration and TP53 inactivation is not applicable. Oncol Rep. 2011;26(1):49–54. doi:10.3892/or.2011.1270
24. Wang MY, Jia M, He J, et al. MDM4 genetic variants and risk of gastric cancer in an Eastern Chinese population. Oncotarget. 2017;8(12):19547–19555. doi:10.18632/oncotarget.14666
25. Xu C, Zhu J, Fu W, et al. MDM4 rs4245739 A > C polymorphism correlates with reduced overall cancer risk in a meta-analysis of 69477 subjects. Oncotarget. 2016;7(44):71718–71726. doi:10.18632/oncotarget.12326
26. Gansmo LB, Romundstad P, Birkeland E, et al. MDM4 SNP34091 (rs4245739) and its effect on breast-, colon-, lung-, and prostate cancer risk. Cancer Med. 2015;4(12):1901–1907. doi:10.1002/cam4.555
27. Zhang J, Zhuo Z, Li W, Zhu J, He J, Su J. XRCC1 gene polymorphisms and risk of neuroblastoma in Chinese children. Aging (Albany NY). 2018;10(10):2944–2953. doi:10.18632/aging.101601
28. Zhou L, Zhang X, Li Z, et al. Association of a genetic variation in a miR-191 binding site in MDM4 with risk of esophageal squamous cell carcinoma. PLoS One. 2013;8(5):e64331. doi:10.1371/journal.pone.0064331
29. Liu J, Tang X, Li M, et al. Functional MDM4 rs4245739 genetic variant, alone and in combination with P53 Arg72Pro polymorphism, contributes to breast cancer susceptibility. Breast Cancer Res Treat. 2013;140(1):151–157. doi:10.1007/s10549-013-2615-x
30. Hashemi M, Sanaei S, Hashemi SM, Eskandari E, Bahari G. Association of single nucleotide polymorphisms of the MDM4 gene with the susceptibility to breast cancer in a southeast iranian population sample. Clin Breast Cancer. 2018;18(5):e883–e891. doi:10.1016/j.clbc.2018.01.003
31. Pedram N, Pouladi N, Feizi MA, Montazeri V, Sakhinia E, Estiar MA. Analysis of the association between MDM4 rs4245739 single nucleotide polymorphism and breast cancer susceptibility. Clin Lab. 2016;62(7):1303–1308. doi:10.7754/Clin.Lab.2016.151128
32. Garcia-Closas M, Couch FJ, Lindstrom S, et al. Genome-wide association studies identify four ER negative-specific breast cancer risk loci.. Nat Genet. 2013;45(4):
33. Fan C, Wei J, Yuan C, et al. The functional TP53 rs1042522 and MDM4 rs4245739 genetic variants contribute to Non-Hodgkin lymphoma risk. PLoS One. 2014;9(9):e107047. doi:10.1371/journal.pone.0107047
34. Gao F, Xiong X, Pan W, et al. A regulatory MDM4 genetic variant locating in the binding sequence of multiple MicroRNAs contributes to susceptibility of small cell lung cancer. PLoS One. 2015;10(8):e0135647. doi:10.1371/journal.pone.0135647
35. Mohammad Khanlou Z, Pouladi N, Hosseinpour Feizi M, Pedram N. Lack of associations of the mdm4 rs4245739 polymorphism with risk of thyroid cancer among Iranian-Azeri patients: a case-control study. Asian Pac J Cancer Prev. 2017;18(4):1133–1138. doi:10.22034/APJCP.2017.18.4.1133
36. Wang MJ, Luo YJ, Shi ZY, et al. The associations between MDM4 gene polymorphisms and cancer risk. Oncotarget. 2016;7(34):55611–55623. doi:10.18632/oncotarget.10877
37. Wynendaele J, Bohnke A, Leucci E, et al. An illegitimate microRNA target site within the 3ʹ UTR of MDM4 affects ovarian cancer progression and chemosensitivity. Cancer Res. 2010;70(23):9641–9649. doi:10.1158/0008-5472.CAN-10-0527
38. Zhang Y, Sturgis EM, Wei P, et al. A genetic variant within MDM4 3ʹUTR miRNA binding site is associated with HPV16-positive tumors and survival of oropharyngeal cancer. Mol Carcinog. 2019;58(12):2276–2285. doi:10.1002/mc.23116
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.