Back to Journals » Vascular Health and Risk Management » Volume 21
Association of High Sensitivity C-Reactive Protein/Albumin Ratio for Coronary Artery Disease in a Southern Arab Peninsula Population: A Cross-Sectional Study Among Yemeni Adults
Authors Al-Fakih HA, Munibari A, Al-Motarreb A, Al-Wather NA, Al-Nono O, Al-Zaazaai AA
Received 8 August 2025
Accepted for publication 12 December 2025
Published 23 December 2025 Volume 2025:21 Pages 1121—1130
DOI https://doi.org/10.2147/VHRM.S559346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Akash Batta
Hesham A Al-Fakih,1 Abdulnasser Munibari,1 Ahmed Al-Motarreb,1 Nawar A Al-Wather,1 Osama Al-Nono,1 Ali A Al-Zaazaai2
1Department of Cardiology, Faculty of Medicine and Health Sciences, Sana’a University, Sana’a, Yemen; 2Department of Pharmacy, Faculty of Medicine and Health Sciences, Sana’a University, Sana’a, Yemen
Correspondence: Hesham A Al-Fakih, Department of Cardiology, Faculty of Medicine and Health Sciences, Sana’a University, Sana’a, Yemen, Tel +967 772037324, Email [email protected]
Background: Coronary artery disease (CAD) is a leading global health concern, with inflammation playing a pivotal role in its pathogenesis. The high-sensitivity C-reactive protein/albumin ratio (CAR) has emerged as a novel marker reflecting both systemic inflammation and physiological reserve. However, its predictive value in specific populations, particularly in the Southern Arab Peninsula, remains underexplored.
Objective: To evaluate the association of CAR in identifying CAD among Yemeni adults referred for coronary computed tomography angiography (CCTA), by assessing its association with coronary artery calcium (CAC) and CAD-RADS scores.
Methods: This cross-sectional study included 249 Yemeni patients with suspected CAD who underwent CCTA. High-sensitivity C-reactive protein and albumin levels were measured to calculate CAR. CAD severity was assessed using CAC and CAD-RADS scoring systems. Statistical analyses explored correlations and predictive performance.
Results: CAR demonstrated a significant positive correlation with CAC scores (r = 0.357, p < 0.001) and CAD-RADS levels (p < 0.001). ROC curve analysis yielded an AUC of 0.708, with an optimal CAR cut-off value of 0.0285, achieving 67.9% sensitivity and 63.6% specificity. Multivariable logistic regression confirmed CAR as an independent predictor of CAD (AOR = 11.28, p < 0.001), alongside diabetes, hypertension, dyslipidemia, and smoking.
Conclusion: CAR is a promising, cost-effective inflammatory marker for early CAD risk stratification, especially in resource-limited settings. Its strong correlation with CAC and CAD-RADS supports its clinical utility in identifying high-risk individuals who may benefit from further cardiovascular evaluation.
Keywords: C-reactive protein, albumin, coronary artery disease, CAR, CAD-RADS, CCTA, inflammation
Introduction
Ischemic heart disease (IHD) is a leading cause of death globally accounting for 13% of the world’s total deaths. Since 2000, deaths from ischemic heart disease have seen the largest increase, rising by 2.7 million to 9.0 million deaths in 2021.1 Owing to the 20–40% prevalence of angina pectoris symptoms, millions of individuals annually present for medical assessment of coronary artery patency.2 Atherosclerosis is the most common etiology of coronary artery obstruction, that caused by lipid buildup in large arteries. Inflammatory pathways are activated as a result of endothelial dysfunction, leading to plaque enlargement, necrotic core formation, and plaque calcification.3 CRP is an inflammation-associated protein,4 and is primarily synthesized in hepatocytes.5 Coronary computed tomography angiography (CCTA), on the other hand, is an imaging modality that visualizes calcium in coronary artery obstructive plaques and assesses artery patency. The American Heart Association has recommended the utilization of hs-CRP in the overall assessment of cardiovascular risk.6 High sensitive C reactive protein is a test measuring same CRP but it is much more sensitive and can detect very low levels of CRP in the blood, often in the range of 0.3 to 10 mg/L.The American College of Cardiology Foundation recommended that evaluating CRP levels is a logical approach for individuals at intermediate risk of cardiovascular events7 but recently a meta-analysis study revealed an elevated levels of CRP did not emerge as a valuable prognostic maker for CAC incidence and progression prediction.8 To increase sensitivity, CAR was utilized as comprehensive marker. The reason behind this combination is that both inflammation and nutritional/functional reserve are involved. CRP (numerator) increases with inflammation, while albumin (denominator) decreases with inflammation and poor nutritional status/chronic disease. Therefore, an elevated CAR signifies both heightened inflammation and a compromised physiological reserve or nutritional status. This dual information makes CAR a more comprehensive indicator of systemic stress and disease severity than hs-CRP alone. However, much of the existing evidence regarding CAR’s predictive utility in CAD originates from diverse populations, and there remains a significant gap in validating these findings within specific regional cohorts. Data from the Southern Arab Peninsula population, particularly those of Yemeni origin, are scarce, yet crucial, as genetic predispositions, environmental factors, and healthcare practices may influence the manifestation and progression of CAD and the utility of biomarkers. Understanding CAR’s role in this specific demographic can offer unique insights and enhance risk stratification strategies tailored to the region.
CCTA is an advanced imaging modality for coronary arteries, providing high diagnostic accuracy with positive predictive values ranging from 59% to 94% and negative predictive values ranging from 83% to 98%.9 The European Society of Cardiology Chronic Coronary Syndromes guidelines recommend CCTA as an appropriate test to exclude obstructive CAD in low-to intermediate-risk patients presenting with chest pain or chest pain equivalents.10 The CAD-RADS, which aims to classify and standardize the severity of CAD in CCTA, has been recently published and updated to CAD-RADS 0.2.11,12
The results of the CAC score, calculated by CCTA, are obtained promptly. For patients presenting with chest pain, a zero-calcium score is a strong negative risk predictor for coronary artery disease, demonstrating a negative predictive value of 99%, sensitivity of 91%, and specificity of 64%.13,14
Methodology and Patient Sample
This cross-sectional study was conducted between January 2023 and May 2025 at a tertiary cardiac center within an 800-bed tertiary hospital in Sana’a City, Yemen. We included 249 consecutive adult patients referred for coronary computed tomography (CT) angiography due to very low (less than 5% pretest probability (PTP)) or low pretest probability of chest pain or dyspnea (>5%- less than 15% PTP) as determined by the risk factors clinical Likelihood according to 2024 ESC Guidelines for the management of chronic coronary syndromes.
A formal sample size calculation was not performed; instead, a non-consecutive, convenience sample of all eligible patients who met the inclusion and exclusion criteria within the specified study period was utilized.The diagnosis and classification of CAD in these patients were primarily established through CCTA using CAD-RADS 0.2 classification, alongside CAC scoring.
Exclusion Criteria
Exclusion criteria included acute coronary syndrome, decompensated heart failure, severe valvular heart disease, malignancy, hepatic or renal malfunction, acute or chronic infection, anemia or hematologic disease, autoimmune disease or receipt of immunosuppression therapy, and chronic obstructive pulmonary disease. The study protocol was approved by the local ethics committee at Sana’a Faculty of Medicine and the study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Clinical Data and Laboratory Measurements
Baseline clinical and demographic characteristics were evaluated, including history of smoking, khat chewing (Catha Edulis herbal), diabetes mellitus (DM), hypertension (HTN), IHD, and dyslipidemia. Venous blood samples were obtained on the same day as the CCTA procedure from each patient for albumin and C-reactive protein (CRP) level measurements. High-sensitivity CRP (hs-CRP) was tested using standard hospital laboratory protocol with a latex turbidimetric assay on the Mindray BS-200 automatic analyzer. Albumin was measured using standard hospital laboratory protocol with the same device, which utilizes the Bromocresol Green (BCG) method. CAR was calculated by dividing hs-CRP (mg/L) by albumin (g/L).
Coronary Computed Tomography Angiography and Image Analysis: Prior to CCTA, patients underwent evaluation of their blood pressure and heart rate. To optimize scan conditions, a single oral dose of 5 mg Bisoprolol was administered to achieve target heart rates, and 0.5 mg of nitroglycerin was given sublingually to induce coronary vasodilation, facilitating optimal contrast filling and enhancing vessel readability. CCTA scans were performed using a Philips 128-multidetector CT scanner. For contrast enhancement, 100 milliliters of non-osmolar iodinated contrast medium was intravenously injected via an 18-gauge peripheral venous cannula at a rate of 5.5 mL/minute. All acquired imaging data were subsequently transferred to a workstation equipped with Philips Intelli Space PACS (Picture Archiving and Communication System) Version 12 for analysis.The cardiologists interpreting the CCTA images were blinded to the patients’ laboratory results and CAR scores to exclude bias.Data interpretation included the assessment of CAC scores, measured according to the Agatston classification, and CAD-RADS interpretations. Obstructive coronary lesions were estimated visually.
Results
A total of 249 patients were included; their baseline demographic and clinical characteristics are summarized in Table 1. The mean age of the patients was 50.3 years (SD ±13.7). Males predominated (n = 168, 67.5%), and the majority of patients were overweight, with a mean BMI of 26.9 kg/m2 (SD ±5.7). There were 158 (63.5%) current khat chewers, and 21 (8%) ex-khat chewers. A notable proportion of participants were current smokers (46.6%), and 14.1% were ex-smokers. Ninety-four patients (37.8%) were diabetic. Additionally, 110 patients (44.2%) were hypertensive. Furthermore, 69 patients (27.7%) had a history of dyslipidemia. CAC score demonstrated a highly skewed distribution, with a median of 0.00 (Interquartile Range [IQR]: [0, 1.1]. This indicates that at least half of the study participants had no detectable coronary artery calcification.
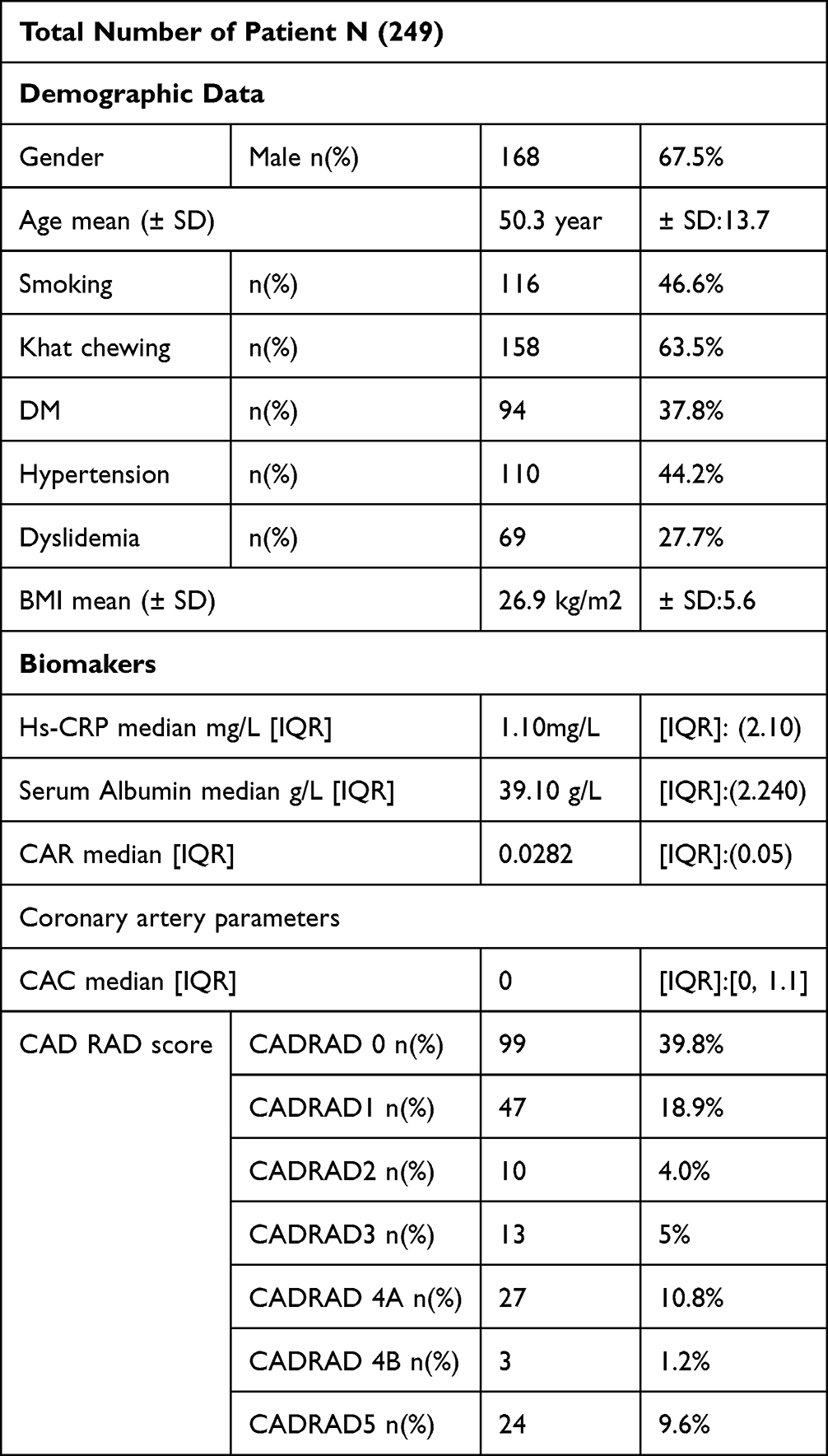 |
Table 1 Baseline Demographic and Clinical Characteristics of the Study Population (N=249) |
The distribution of patients across CAC score categories was as follows: 68.7% had a CAC score of 0, 6.8% had CAC (1–99), 13.7% had CAC (100–399), 6.4% had CAC (400–990), and 4.4% had CAC (>1000).
Association Between CAR and CAC Score
A statistically significant positive correlation was found between CAR and CAC score (Agatston score). Spearman’s rho indicated a moderate positive correlation (ρ = 0.357, p < 0.001), consistent with the Kendall’s tau-b coefficient (τ = 0.273, p < 0.001). By log-transforming the calcium score to overcome severely skewed data, the linear regression model revealed a weak positive linear correlation (R = 0.235), with CAR explaining 5.5% of the variance in CAC (R2 = 0.055, Adjusted R2 = 0.051), as shown in Figure 1. The standard error of the estimate was 2.60788. The ANOVA table demonstrated that the overall regression model was statistically significant (F(1, 240) = 14.055, p < 0.001), indicating that CAR is a significant predictor of CAC. Examination of the coefficients revealed that CAR was a statistically significant positive predictor of CAC (B = 8.998, Std. Error = 2.400, Beta = 0.235, t = 3.749, p < 0.001), indicating that higher CAR values are associated with higher CAC values. The constant (intercept) was 1.214 (t = 5.447, p < 0.001).
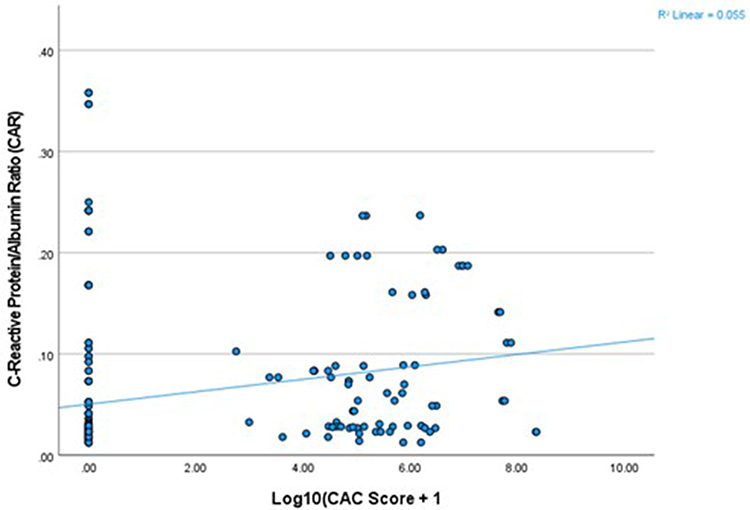 |
Figure 1 Positive correlation between C-Reactive Protein/Albumin Ratio (CAR) and Log-transformed Coronary Artery Calcium (CAC) score in Yemeni patients suspected of CAD (r=0.357,p<0.001). The solid line represents the linear regression fit. |
The Association Between the CAR and the CAD-RADs Score
An ordinal logistic regression was performed. The results demonstrated that CAR was a highly significant predictor of CAD-RADS level (Estimate = 11.924, Wald χ2 = 47.411, p < 0.001). For every 0.1 unit increase in CAR, the odds of being in a higher CAD-RADS category increased by approximately 1500 times (exp(B) = 150965.7). The model significantly improved prediction over an intercept-only model (Chi-Square = 50.202, df = 1, p < 0.001), with a Nagelkerke Pseudo R-square of 0.187, indicating that CAR explained 18.7% of the variance in CAD-RADS ordinal score. The assumption of parallel lines was met (Chi-Square = 12.044, df = 8, p = 0.149), confirming the validity of the proportional odds assumption. The model’s goodness-of-fit was also supported by a non-significant Deviance Chi-Square (p = 0.675). Further supporting this finding, a Kruskal–Wallis H-test also revealed a statistically significant difference in CAR levels across the CAD-RADS ordinal categories (H (9) = 57.080, p < 0.001), with mean ranks of CAR generally increasing with higher CAD-RADS severity (eg, CAD-RADS 0 mean rank = 93.74 vs CAD-RADS 5 mean rank = 184.33). The median CAR values generally increased with higher CAD-RADS categories. For instance, the median CAR for patients with CAD-RADS 0 was 0.0235 (IQR: 0.01), while for those with CAD-RADS 5, it was 0.0769 (IQR: 0.20), indicating a progressive rise in CAR with disease severity. This tendency is visually represented in Figure 2.
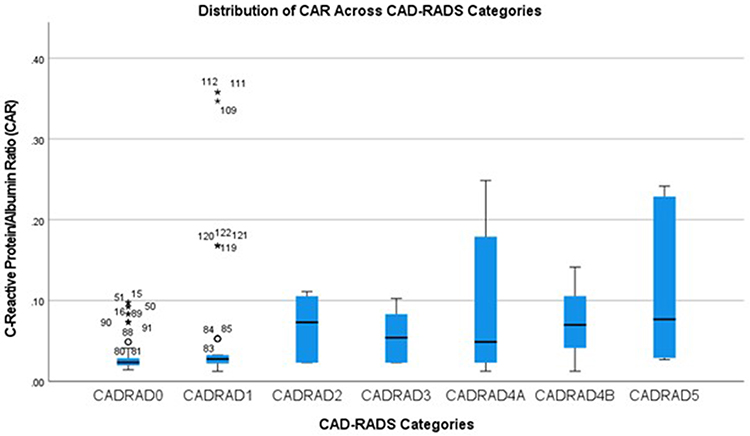 |
Figure 2 Box plot showing the distribution of the High-Sensitivity C-reactive protein to Albumin Ratio (CAR) for each CAD-RADS ordinal category. The central line within each box represents the median CAR, while the box itself indicates the interquartile range (25th to 75th percentiles). Whiskers extend to the minimum and maximum values within 1.5 times the interquartile range. Outliers are marked by “o” (circles) or “*” (asterisks). The plot visually suggests a trend of increasing median CAR values with higher CAD-RADS ordinal categories, though significant variability and outliers are present within several groups. |
Receiver Operating Characteristic (ROC) Curve Analysis and Diagnostic Accuracy of CAR
Receiver Operating Characteristic (ROC) curve analysis was performed to evaluate the diagnostic utility of CAR in distinguishing the presence of coronary artery disease (CAD-RADS > 0) from its absence (CAD-RADS = 0). The optimal cut-off for CAR was determined to be 0.0285. The area under the curve (AUC) was 0.708 (95% CI: 0.633–0.776), indicating acceptable discriminatory ability. The ROC curve visually representing this performance is shown in Figure 3. At this optimal cut-off, the sensitivity for detecting CAD was 67.86% (95% CI: 56.78–77.64%), and the specificity was 63.64% (95% CI: 55.80–70.97%). Further detailed diagnostic metrics, including the positive predictive value (PPV) of 48.72% (95% CI: 42.53–54.95%) and a negative predictive value (NPV) of 79.55% (95% CI: 73.63–84.42%), are summarized in Table 2.
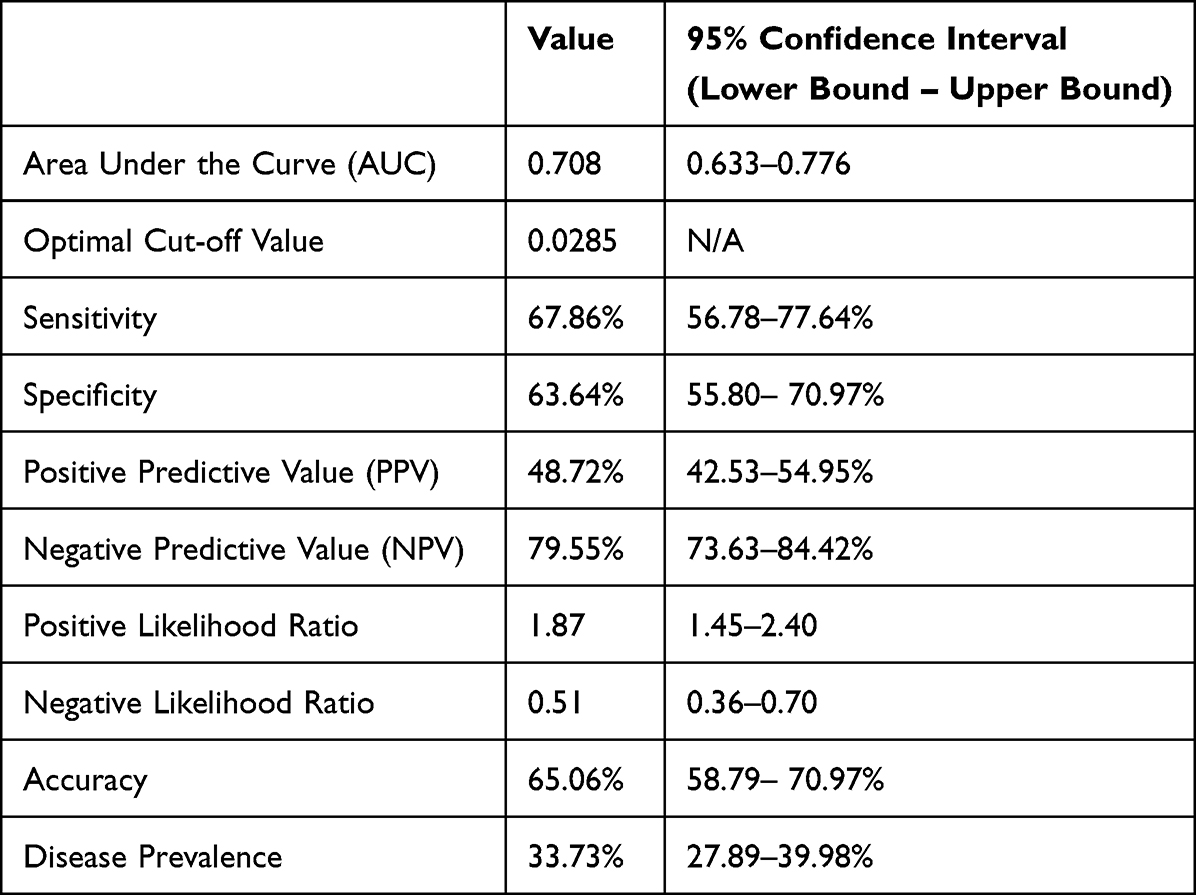 |
Table 2 Diagnostic Performance of C-Reactive Protein/Albumin Ratio (CAR) for Distinguishing Coronary Artery Disease (CAD-RADS > 0 Vs CAD-RADS = 0) at Optimal Cut-off (0.0285), with 95% Confidence Intervals |
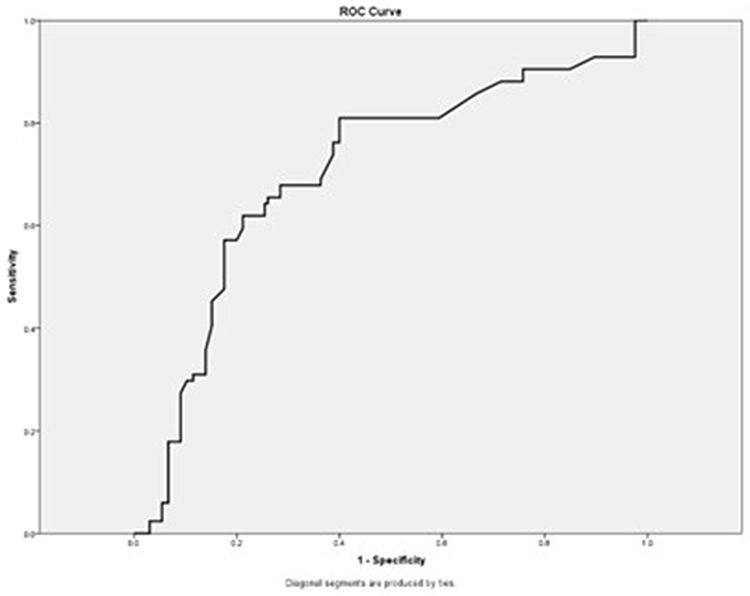 |
Figure 3 Receiver Operating Characteristic (ROC) curve for C-reactive protein/albumin ratio (CAR) distinguishing between the presence (CAD-RADS > 0) and absence (CAD-RADS = 0) of Coronary Artery Disease. The Area Under the Curve (AUC) is 0.708. |
Predictors of Coronary Artery Disease: Multi-Variable Logistic Regression Analysis
To identify independent predictors of coronary artery disease (CAD-RADS > 0), a multivariable binary logistic regression model was performed. The model included CAR, gender, khat use, smoking status, diabetes mellitus, history of hypertension, history of dyslipidemia, and body mass index as covariates. The analysis revealed that CAR (Adjusted Odds Ratio [AOR] = 11.282, 95% CI: 3.611–35.249, p < 0.001), diabetes mellitus (AOR = 5.850, 95% CI: 2.342–14.613, p < 0.001), history of hypertension (AOR = 3.870, 95% CI: 1.538–9.736, p = 0.004), and history of dyslipidemia (AOR = 5.469, 95% CI: 2.168–13.797, p < 0.001) were independently and significantly associated with increased odds of CAD. Smoking status was also found to be an independent predictor of CAD (overall p = 0.011). Specifically, current smokers had significantly higher odds of CAD compared to the reference group (eg, never smokers) (AOR = 19.274, 95% CI: 2.561–145.036, p = 0.004). Gender, khat chewing, and body mass index were not found to be significant independent predictors of CAD in this multivariable model. The full results of the multivariable logistic regression analysis are presented in Table 3.
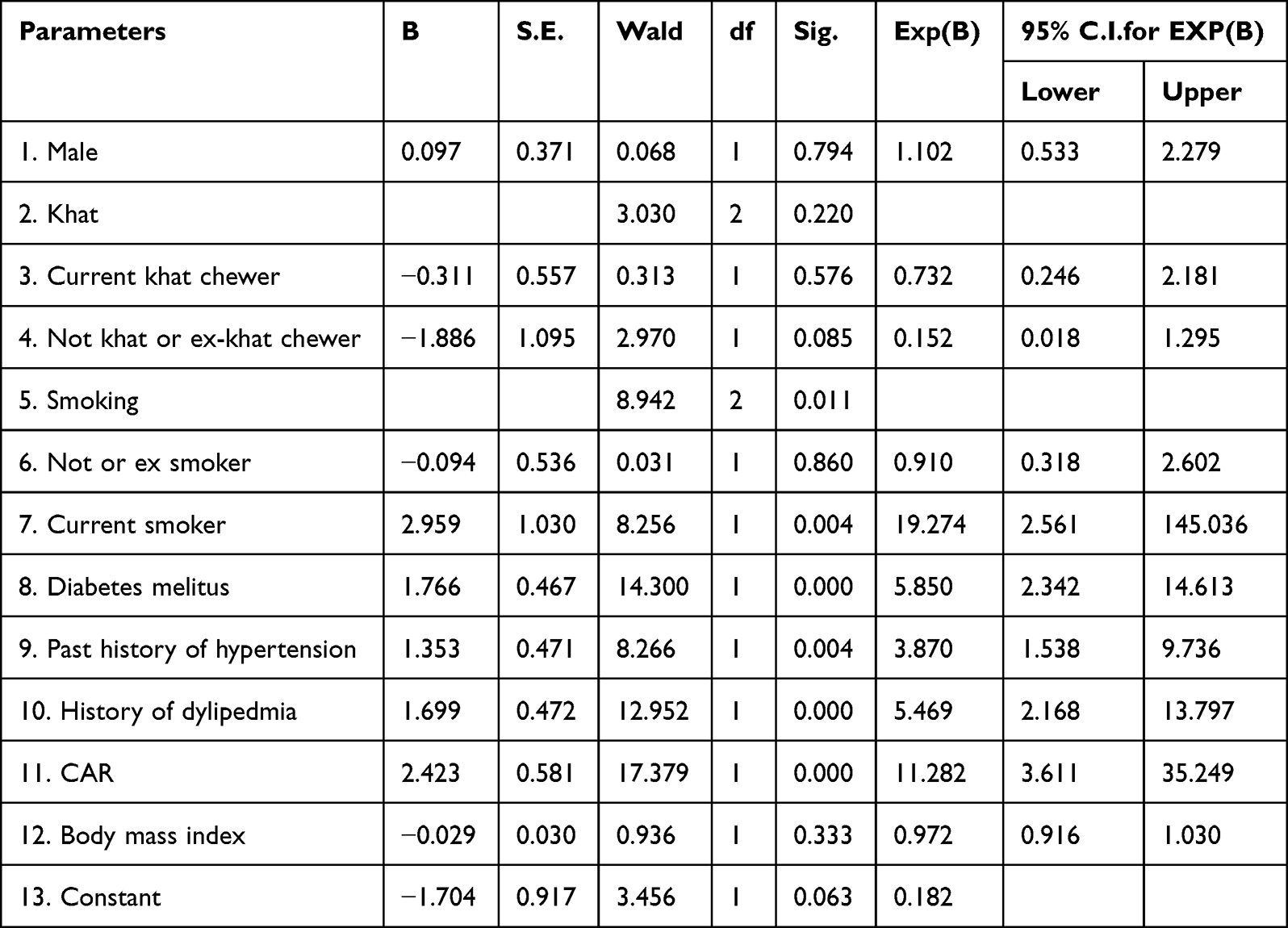 |
Table 3 Multivariable Logistic Regression Analysis of Predictors for Coronary Artery Disease (CAD-RADS > 0) |
Discussion
The findings of this study demonstrate a significant association between CAR and the severity of coronary artery disease (CAD), as determined by CAC and CAD-RADS scores. These results are consistent with existing studies that have shown a correlation between CAR and various indicators of cardiovascular risk and disease severity.15–18 Our study, however, further contributes to the literature by validating CAR’s potential as a valuable inflammatory biomarker for complementary CAD risk stratification specifically within a Southern Arab Peninsula population, thereby addressing a crucial regional data gap.
It is the first to investigate the CAR-CAD association (using CAC and CAD-RADS 2.0 scores) specifically among Yemeni adults in the Southern Arab Peninsula.
Our findings, specifically within this Yemeni population, align with other studies demonstrating CAR’s superiority over individual CRP or albumin levels in predicting outcomes across various inflammatory conditions.19 The strong association observed between CAR and both CAC scores and CAD-RADS ordinal levels in our study further solidifies CAR’s effectiveness as a valuable biomarker for quantifying the extent and severity of atherosclerotic disease, consistent with prior research on its utility in predicting myocardial ischemia and CAD severity quantified by the SYNTAX score.20 Similarly, recent studies have demonstrated the prognostic value of related immunonutritional indices, such as the HALP (Hemoglobin, Albumin, Lymphocyte, and Platelet) score21 and the CALLY (C-Reactive Protein-Albumin-Lymphocyte) index,22 in patients with myocardial infarction, further validating the clinical relevance of combining inflammatory and nutritional biomarkers A key strength of our study lies in the integration of CAR with CCTA-derived measures. While CCTA offers detailed anatomical assessment of coronary arteries, including plaque burden and calcification, CAR provides a dynamic snapshot of ongoing inflammatory activity. This combination offers a more comprehensive risk assessment, linking the systemic inflammatory state to the actual presence of coronary artery disease. Clinically, the identification of a relatively low optimal CAR cut-off value (0.0285) for distinguishing the presence of CAD (CAD-RADS > 0) with acceptable discriminatory ability suggests its effectiveness as a simple, accessible, and cost-effective screening tool, potentially serving as an initial indicator of disease or risk. This is particularly relevant in resource-limited settings, such as Yemen, where access to advanced imaging like CCTA may be challenging. It is important to note that this diagnostic cut-off differs from the generally higher CAR values reported in studies focused on predicting adverse cardiovascular outcomes or disease prognosis in established CAD, reflecting the influence of distinct clinical endpoints on biomarker thresholds. Patients identified with elevated CAR levels have a significantly higher likelihood of CAD; therefore, this finding mandates further diagnostic evaluation, such as advanced imaging (eg, CCTA), to confirm the diagnosis and guide management. While our study specifically focused on patients with suspected CAD referred for CCTA, it’s important to recognize that CAR’s potential as a risk stratification tool extends to various clinical scenarios, including patients with asymptomatic CAD or those with established acute coronary syndromes, as indicated by other research.23,24 The finding that elevated CAR is an independent predictor of CAD implies a differential treatment approach: patients with a high CAR should be prioritized for intensive risk factor modification, including lifestyle changes, smoking cessation, and aggressive management of associated comorbidities (DM, HTN, Dyslipidemia), alongside the mandatory consideration for advanced diagnostic evaluation (CCTA). Future studies should aim to further investigate CAR’s predictive performance across these diverse patient subsets to fully delineate its comprehensive applicability in CAD management. Furthermore, the identification of elevated CAR as a significant marker in CAD opens avenues for exploring therapeutic interventions. Future prospective studies are warranted to investigate whether targeted treatments, such as Statins or ACE inhibitors, could potentially lower CAR levels and, more importantly, if such reductions translate into improved clinical outcomes and regression of CAD progression in patients with high CAR, especially within this specific population.
Limitations of the Study
Despite promising findings, this study has several limitations, including its single-center design in Sana’a, Yemen, and a relatively small, specific patient cohort with low pretest probability, which limits generalizability to broader populations. Furthermore, the exclusion of sicker patients, the visual estimation of obstructive lesions, and the potential for unmeasured confounders suggest a need for caution. Thus, the optimal CAR cut-off value requires external validation in larger, diverse prospective cohorts to confirm its robustness and broader clinical applicability, paving the way for personalized clinical approaches.
Conclusion
According to aforementioned results, CAR holds promise as an accessible and cost-effective tool for CAD risk stratification, particularly in settings where advanced imaging such as CCTA faces limitations in terms of expense and availability. While CCTA remains a highly accurate diagnostic modality, CAR’s independent predictive capability supports its utility as a marker for identifying patients who may warrant further investigation. Continued large-scale validation is essential to confirm its broader clinical applicability.
Acknowledgments
The authors would like to express their sincere gratitude to all the patients who participated in this study, whose willingness to contribute made this research possible. We extend our appreciation to the staff and administration of the tertiary cardiac center for their invaluable support in data collection and providing the necessary facilities. We also wish to acknowledge the assistance of Gemini AI for its contributions to the rephrasing, grammar correction, and for providing guidance on the structure and content development of this manuscript. This assistance was used to enhance clarity and readability, and its role is disclosed here for full transparency. This research received no specific fund from any agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Leading causes of death. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death.
2. Gulati M, Levy PD, Mukherjee D, et al. 2021AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144:e368–e454.
3. Jebari-Benslaiman S, Galicia-García U, Larrea-Sebal A, et al. Pathophysiology of atherosclerosis. Int J Mol Sci. 2022;23(6):3346. doi:10.3390/ijms23063346
4. Tillett WS, T F. Serological reactions in pneumonia with a nonprotein somatic fraction of pneumococcus. J Exp Med. 1930;52(4):561. doi:10.1084/jem.52.4.561
5. Calabró P, Willerson JT, Yeh ET. Inflammatory cytokines stimulated C-reactive protein production by human coronary artery smooth muscle cells. Circulation. 2003;108(16):1930–1932. doi:10.1161/01.CIR.0000096055.62724.C5
6. Pearson TA, Mensah GA, Alexander RW, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice. Circulation. 2003;107(3):499–511. doi:10.1161/01.CIR.0000052939.59093.45
7. Greenland P, Alpert JS, Beller GA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults. J Am Coll Cardiol. 2010;56(25):e50–103. doi:10.1016/j.jacc.2010.09.001
8. Tajani A, Sadeghi M, Omidkhoda N, et al. The association between C-reactive protein and coronary artery calcification: a systematic review and meta-analysis. BMC Cardiovasc Disord. 2024;24:204. doi:10.1186/s12872-024-03856-5
9. Meijboom WB, Meijs MF, Schuijf JD, et al. Diagnostic accuracy of 64-slice computed tomography coronary angiography: a prospective, multicenter, multivendor study. J Am Coll Cardiol. 2008;52(25):2135–2144. doi:10.1016/j.jacc.2008.08.058
10. Knuuti J, Wijns W, Saraste A, et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407–477. doi:10.1093/eurheartj/ehz425
11. Cury RC, Abbara S, Achenbach S, et al. CAD-RADS: coronary artery disease–reporting and data system. J Am Coll Radiol. 2016;13(12 Pt A):1458–66.e9. doi:10.1016/j.jacr.2016.04.024
12. Cury RC, Abbara S, Achenbach S, et al. CAD-RADS™ 2.0 – 2022 coronary artery disease–reporting and data system. J Cardiovasc Comput Tomogr. 2022;16(6):536–557. doi:10.1016/j.jcct.2022.07.002
13. Huang W, Lim LMH, Aurangzeb AS, et al. Performance of the coronary calcium score in an outpatient chest pain clinic and strategies for risk stratification. Clin Cardiol. 2021;44(2):267–275. doi:10.1002/clc.23539
14. Fernandez-Friera L, Garcia-Alvarez A, Bagheriannejad Esfahani F, et al. Diagnostic value of coronary artery calcium scoring in low-intermediate risk patients evaluated in the emergency department for acute coronary syndrome. Am J Cardiol. 2011;107(1):17–23. doi:10.1016/j.amjcard.2010.08.037
15. Lou X, Wen N, Wang Y, Fang L. Relationship between CRP/ALB ratio and severity of coronary artery lesions in hypertensive patients with acute myocardial infarction. Med Sci Monit. 2025;
16. Zhang R, Wang Y, Liao L, et al. The relationship between C-reactive protein/albumin ratio and mortality in hypertensive patients: a national cohort study. Nutr Metab Cardiovasc Dis. 2024;34(7):1601–1609. doi:10.1016/j.numecd.2024.02.011
17. Tang C, Xu S, Lu Z, Yan J, Yu C. Association of hs-CRP/albumin ratio with all-cause and cardiac death in coronary heart disease individuals: a retrospective NHANES study. Front Cardiovasc Med. 2022;9:1062060.
18. Yan G, Zhang P, Yang M, et al. Systemic immune-inflammation index and CRP/albumin ratio for predicting all-cause mortality in patients with coronary artery disease. J Inflamm Res. 2022;15:4395–4404. doi:10.2147/JIR.S369963
19. Gharbia OM, Gomaa D, Hawas S, Abdel Twab H. Serum CRP/albumin ratio in Egyptian rheumatoid arthritis patients and its relation to disease activity, physical function and psychological status. Med J Cairo Univ. 2024;92(9):815.
20. Tascilar E, Simsek H, Kalkan S, Cengiz M, Akyel A. CRP/albumin ratio predicts severity of coronary artery disease and ischemia. Eur Rev Med Pharmacol Sci. 2023;27(1):164–170.
21. Tekin YK, Tekin G. The prognostic value of HALP score in predicting in-hospital mortality in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Coron Artery Dis. 2023;34(7):483–488. doi:10.1097/MCA.0000000000001271
22. Gunes M, Dinc C, Kaya A, et al. The prognostic value of C-Reactive Protein-Albumin-Lymphocyte (CALLY) index in predicting in-hospital mortality after primary percutaneous coronary intervention in patients With ST-Elevation Myocardial Infarction (STEMI). Catheter Cardiovasc Interv. 2025.
23. Menekse G, Yilmaz Y. Relationship between CRP/albumin ratio and long-term mortality in acute coronary syndrome patients. Cureus. 2023;15(11):e48906. doi:10.7759/cureus.48906
24. Zou J, Yu Y, Yu K, Xia W, Song J, Pan X. Usefulness of CRP/albumin ratio in predicting adverse cardiovascular events in chronic total occlusion undergoing PCI. Front Cardiovasc Med. 2021;8:731261. doi:10.3389/fcvm.2021.731261
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.