Back to Journals » International Journal of Women's Health » Volume 17
Association Between Weight Change Pelvic Organ Prolapse and Weight Change During the Perinatal Period Among Chinese Women
Authors Wang G, Zhou L, Yu R, Wang X, Cui H
Received 23 July 2025
Accepted for publication 19 November 2025
Published 24 December 2025 Volume 2025:17 Pages 5623—5630
DOI https://doi.org/10.2147/IJWH.S550259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Matteo Frigerio
Guan Wang,1 Li Zhou,2 Rao Yu,3 Xiaoqin Wang,3 Hongyan Cui1
1Department of Obstetrics,Tianjin Central Hospital of Gynecology Obstetrics, Tianjin, People’s Republic of China; 2Department of Gynecology, Tianjin Central Hospital of Gynecology Obstetrics, Tianjin, People’s Republic of China; 3Department of Obstetrics and Gynecology, First People’s Hospital of Wanzhou District, Chongqing, People’s Republic of China
Correspondence: Xiaoqin Wang, Department of Obstetrics and Gynecology, First People’s Hospital of Wanzhou District, No. 388, Tiancheng East Road, Zhoujiaba Street, Wanzhou District, Chongqing, 404000, People’s Republic of China, Tel +86 023 58376705, Email [email protected] Hongyan Cui, Department of Obstetrics,Tianjin Central Hospital of Gynecology Obstetrics, No. 156, the Nankai Third Road, Tianjin, 300100, People’s Republic of China, Tel +86 022 58287057, Email 18920196039/[email protected]
Background: Pelvic organ prolapse (POP) is a global problem that severely affects a woman’s quality of life. This study aimed to investigate the association between weight change during pregnancy and post-pregnancy POP.
Methods: This study retrospectively enrolled 640 participants from Tianjin Central Hospital of Gynecology Obstetrics (institution 1, n = 363 cases) in northern China and First People’s Hospital of Wanzhou District, Chongqing (institution 2, n = 277 cases) in southwestern China. The participants were grouped into POP-Q I–II (n = 288), POP-Q III–IV (n = 132), and non-POP groups (control group, n = 220). Pre-pregnancy body mass index (BMI), weight gain during pregnancy, and weight retention at 6 months postpartum were compared among the three groups after eliminating confounding factors.
Results: No statistically significant differences were detected in the pre-pregnancy BMI in the POP-Q I–IV, POP-Q I–II, and POP-Q III–IV groups compared to the control group (P > 0.05). Significant statistical differences (P < 0.05) were observed in weight gain during pregnancy (≥ 14 kg) in the POP-Q I–IV, POP-Q I–II, and POP-Q III–IV groups compared with the control group. Significant statistical differences (P < 0.05) were observed in weight retention (≥ 5 kg) at 6 months postpartum among the POP-Q I–IV, POP-Q I–II, and POP-Q III–IV groups compared to the control group.
Conclusion: Weight change during the perinatal period is the risk factor of postpartum POP. Specifically, a pre-pregnancy BMI < 23 kg/m2 did not increase the risk of POP, whereas gestational weight gain ≥ 14 kg and weight retention ≥ 5 kg at 6 months postpartum significantly increased the risk of postpartum POP. Weight management programs during and after pregnancy may help reduce the risk of POP.
Keywords: perinatal period, pre-pregnancy BMI, weight gain during pregnancy, weight retention postpartum, pelvic organ prolapse
Introduction
Pelvic organ prolapse (POP) is a common disorder that is associated with pelvic floor dysfunction. POP is influenced by various factors, such as age, hormones, pregnancy, and childbirth, and POP results in changes in the anatomical positions of the bladder, uterus, and rectum. Different prevalence rates have been reported between different racial/ethnic groups: White women, 10.76%; Hispanic women, 6.55%; Black women, 3.80%; and Asian-American women, 3.40%.1 East Asian women have a lower risk of POP than other races.1,2 The following factors add to the risk of POP: hysterectomy, being overweight, and ≥3 vaginal deliveries.3–5
The effect of body weight on pelvic floor function has consistently been a focal area of research and is considered an independent risk factor for POP.4–6 Body mass index (BMI) of obese patients was positively correlated with increased intra-abdominal and bladder pressure. For every 1 kg/m2 incremental increase in BMI, the incidence of POP increased by 3%. Ninety% of overweight/obese women (BMI > 25 kg/m2), 90% of obese women have different degrees of POP severity, and POP adversely affects 50% of overweight/obese women.7 Moreover, the combination of pregnancy and weight change further increases the risk of POP in women.8,9 A meta-analysis has indicated that excessive gestational weight gain is a risk factor for pelvic floor dysfunction.8 The prevalence of pelvic floor dysfunction is positively correlated with excessive gestational weight gain during pregnancy.9,10
Previous studies have mostly focused on pre-pregnancy BMI and POP, pregnancy BMI and POP, or postpartum BMI and POP. The connection between POP and BMI at these three timepoints (pre-pregnancy, at pregnancy and postpartum) was not continuously studied. The impact of pre-pregnancy BMI on POP and the association between weight change during pregnancy and POP development of POP have not been established, especially on Asian (Chinese) population. Our study aimed to retrospectively explore the association between pre-pregnancy BMI, weight gain during pregnancy, weight recovery at six months postpartum, and postpartum POP among populations from two distinct regions in northern and southwestern China.
Patients and Methods
Participants
Patients with POP admitted to Tianjin Central Hospital of Gynecology Obstetrics (institution 1) in northern China and the First People’s Hospital of Wanzhou District, Chongqing (institution 2) in southwestern China were retrospectively reviewed from January 2020 to December 2024. All the clinical data of these patients were checked according to the inclusion criteria. This study was approved by the Ethics Committees of both institutions and was proceeded in compliance with the Declarations of Helsinki. The requirement for written informed consent was waived by the ethics committee owing to the retrospective design of the study. All the data were anonymized or removed the personally identifiable information and securely stored to maintain with patient data confidentiality.
The inclusion criteria for patients with POP were set according to the Chinese Guidelines for the Diagnosis and Treatment of Pelvic Organ Prolapse (2020 edition) as follows:11 age at onset, 50–70 years; last delivery between 25 and 35 years of age; full-term singleton vaginal delivery without instrumental assistance; parity ≤ 2; newborn birth weight between 2500 and 3500 g; duration of the second stage of labor ≤ 2 h; perineal laceration ≤ II; no standardized pelvic floor function rehabilitation treatment after childbirth; breastfeeding duration of ≥6 months; and POP diagnosed by both symptomatic reports and POP quantitative grading (POP-Q).11 Symptomatic reports included the patients self-reported of symptoms of a feeling of heaviness, pelvic pressure or heaviness, prolapse of a mass, problems with urination, defecation, and sexual function issues, etc. Patients who visited a gynecological clinic for the evaluation of POP during the same period were also enrolled using the same criteria set for POP patients. The same two obstetrician-gynecologists in our author team with more than 8 years’ work experiences performed POP quantitative grading (POP-Q) [11] for the participants included.
The exclusion criteria were as follows: pelvic organ-related malignant tumors; severe primary diseases, such as heart (heart function grade III–IV), brain (intracranial infection, cerebral hemorrhage, metabolic encephalopathy, and intracranial tumors), and kidney disease (rapidly progressive nephritis, membranous nephropathy, polycystic kidney disease, lupus nephritis, and uremia); incomplete clinical data; a history of delivering a macrosomic infant; women with frequent vigorous physical activity; connective tissue disorders; obesity occurs 6 months after giving birth; chronic constipation; lung diseases that cause chronic coughing, or a history of pelvic organ-related surgery.
Grouping
A total of 687 participants (394 from institution 1 and 293 from institution 2) were enrolled in this study. However, 23 cases with incomplete data (11 cases from institution 1 and 12 cases from institution 2), 9 cases involving instrument-assisted delivery from institution 1, 7 cases with multiple pregnancies (5 cases from institution 1 and 2 cases from institution 2), and 8 cases with macrosomia (6 cases from institution 1 and 2 cases from institution 2) were excluded. A total of 47 participants were excluded, and 640 patients (93.16% [640/687]) completed this study as follows: Tianjin Central Hospital of Gynecology Obstetrics (363 cases [168 cases with POP-Q I–II and 75 cases with POP-Q III–IV] and 120 patients with non-POP) in northern China, and First People’s Hospital of Wanzhou District, Chongqing (277 cases [120 cases with POP-Q I–II, 57 cases with POP-Q III–IV], and 100 cases of non-POP) in southwestern China.
The POP group included 420 patients with POP-Q I–IV and the control group included 220 patients without POP. The participants were grouped into the POP-Q I–II group (n = 288), POP-Q III–IV group (n = 132), and the control group (non-POP group, n = 220) and compared.
Research Methods
Basic information on the participants included in the study was collected through an electronic medical record system and a self-constructed questionnaire survey. The electronic medical record system provided the information including age of onset, age at last childbirth, number of full-term singleton vaginal deliveries, newborn birth weight, duration of the second stage of labor, degree of perineal laceration, whether or not there was regular postpartum pelvic floor rehabilitation treatment, duration of breastfeeding, pre-pregnancy BMI within 3 months, weight gain during pregnancy, and weight recovery 6 months postpartum (Δ=weight at 6 months postpartum - pre-pregnancy weight), symptomatic reports and POP quantitative grading. The questionnaire survey mainly explored the patients’ age, weight changes half a year or one year after giving birth, menopausal status, whether hormone therapy or not, occupation, whether surgery for POP, etc. The self-constructed questionnaire was designed based on the core ideas of Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire-Short Form (POPIQ) and Pelvic Floor Distress Inventory-Short Form 20 Simple version.
Two centers each assigned three physicians who were blinded to this study to organize, input, proofread, and validate the data.
Statistical Methods
SPSS 28.0 statistical software was used for data analysis. Measurement data are presented as the mean ± standard deviation, and independent sample t-tests were used for intergroup comparisons. Chi-square tests were used to analyze categorical data. Statistical significance was set at P-value < 0.05.
Results
Basic Information
The basic patient information is presented in Table 1. The baseline data for the POP I–IV group showed no significant differences from the control group, as follows: overall age of onset (61.55 ± 5.56 vs 60.41 ± 5.49 y, P > 0.05); age at last delivery (28.93 ± 2.90 vs 29.11 ± 2.96 y, P > 0.05); parity (X2 = 1.71, P > 0.05), newborn birth weight (3406.67 ± 263.48 vs 3353.09 ± 266.24 g, P > 0.05); duration of the second stage of labor (36.63 ± 9.64 vs 33.57 ± 9.71 h, P > 0.05); and degree of perineal laceration (X2 = 0.003, P > 0.05). In addition, none of the patients had undergone standardized pelvic floor function rehabilitation treatment, and the breastfeeding duration was ≥6 months.
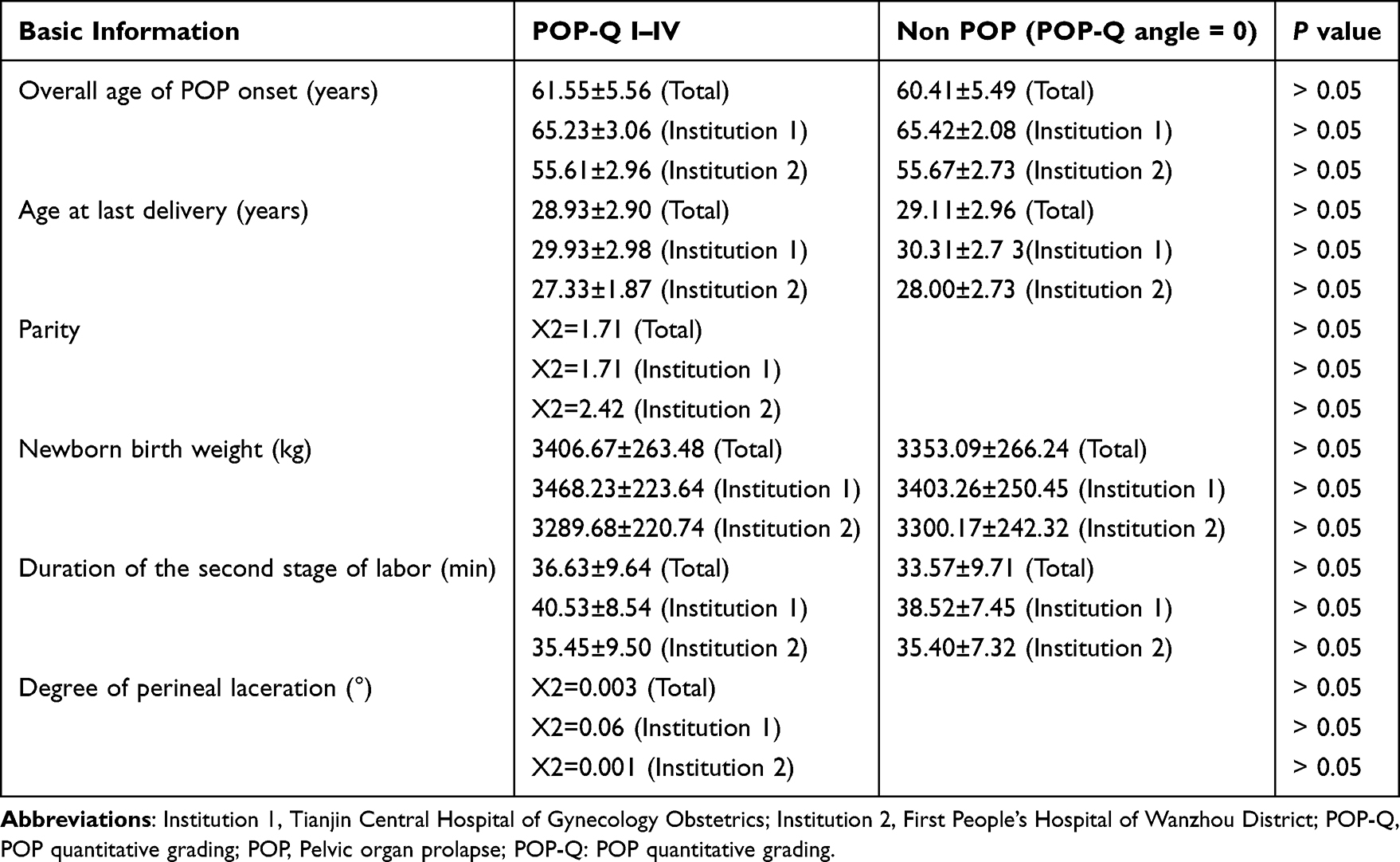 |
Table 1 Basic Information of Patients Enrolled in Two Research Centers |
Association Between Pre-Pregnancy BMI and POP
The pre-pregnancy BMI for the POP-Q I–IV and control groups was 21.87 ± 2.10 kg/m2 and 21.47 ± 1.52 kg/m2, respectively (P = 0.13; Figure 1A). The pre-pregnancy BMI of the POP-Q I–II and POP-Q III–IV groups were 21.75 ± 2.12 kg/m2 and 22.03 ± 2.06 kg/m2, respectively, and showed no significant difference when compared to the control group (21.47 ± 1.52 kg/m2, P = 0.31 and P = 0.06, respectively; Figure 1A).
 |
Figure 1 Association between pre-pregnancy body mass index (BMI) and POP. (A) The pre-pregnancy BMI of the POP-Q I–IV, POP-Q I–II, POP-Q III–IV, and non-POP groups in the 2 research centers (21.87 ± 2.10 vs 21.47 ± 1.52, P > 0.05; 21.75 ± 2.12 vs 21.47 ± 1.52, P > 0.05; 22.03 ± 2.06 vs 21.47 ± 1.52, P > 0.05). (B) The pre-pregnancy BMI of the POP-Q I–IV, POP-Q I–II, POP-Q III–IV, and non-POP groups from Institution 1 were compared (22.49 ± 2.31 vs 21.96 ± 1.85, P > 0.05; 22.35 ± 2.33 vs 21.96 ± 1.85, P > 0.05; 22.69 ± 2.26 vs 21.96 ± 1.85, P > 0.05). (C) The pre-pregnancy BMI between the POP-Q I–IV, POP-Q I–II, POP-Q III–IV, and non-POP groups from Institution 2 were compared (20.86 ± 1.11 vs 21.01 ± 0.91, P > 0.05; 20.73 ± 1.08 vs 21.01 ± 0.91, P > 0.05; 21.03 ± 1.13 vs 21.01 ± 0.91, P > 0.05). Abbreviations: POP-Q, POP quantitative grading; POP-Q 0°, 0 angle when proceeding POP-Q. |
The results from the two research centers were analyzed simultaneously and independently. The results from Institution 1 showed that the pre-pregnancy BMI of the POP-Q I–IV, POP-Q I–II, and POP-Q III–IV groups were 22.49 ± 2.31 kg/m2, 22.35 ± 2.33 kg/m2, and 22.69 ± 2.26 kg/m2, respectively, and were not statistically difference from the non-POP group (21.96 ± 1.85 kg/m2, P = 0.62, P = 0.37, and P = 0.12, respectively; Figure 1B). The results from Institution 2 also indicated that the pre-pregnancy BMI of the POP-Q I–IV, POP-Q I–II, and POP-Q III–IV groups were 20.86 ± 1.11 kg/m2, 20.73 ± 1.08 kg/m2, and 21.03 ± 1.13 kg/m2, respectively, which did not differ from the non-POP group (21.01 ± 0.91 kg/m2, P = 0.45, P = 0.20, and P = 0.93; Figure 1C).
Analysis of the Association Between Weight Gain During Pregnancy and POP
The weight gain during pregnancy in the POP-Q I–IV and control groups was 16.60 ± 2.72 kg and 13.46 ± 2.06 kg, respectively. A statistically significant difference was observed between the two groups (P < 0.001; Figure 2A). The overall weight gain during pregnancy in the POP-Q I–II and POP-Q III–IV groups was 15.81 ± 2.38 kg and 17.73 ± 2.77 kg, respectively, showing significant statistical differences compared to the control group (P < 0.001; Figure 2A).
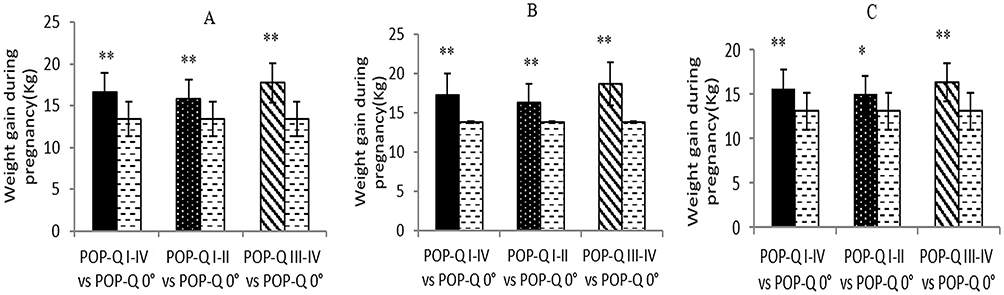 |
Figure 2 Analysis of the association between weight gain during pregnancy and POP. (A) The overall POP-Q I–IV groups from the two research centers are shown. Weight gain during pregnancy was compared among the POP-Q I–IV, POP-Q I–II, POP-Q III–IV, and non-POP groups (16.60 ± 2.72 vs 13.46 ± 2.06, **P < 0.01; 15.81 ± 2.38 vs 13.46 ± 2.06, **P < 0.01; 17.73 ± 2.77 vs 13.46 ± 2.06, **P < 0.01). (B) Weight gain during pregnancy among the POP-Q I–IV, POP-Q I–II, POP-Q III–IV, and non-POP groups from Institution 1 is presented (17.21 ± 2.80 vs 13.82 ± 1.93, **P < 0.01; 16.26 ± 2.41 vs 13.82 ± 1.93, **P < 0.01; 18.64 ± 2.73 vs 13.82 ± 1.93, **P < 0.01). (C) Weight gain during pregnancy among the POP-Q I–IV, POP-Q I–II, POP-Q III–IV, and non-POP groups from Institution 2 is presented (15.60 ± 2.24 vs 13.12 ± 2.11, **P < 0.01; 15.03 ± 2.10 vs 13.12 ± 2.11, *P < 0.05; 16.37 ± 2.20 vs 13.12 ± 2.11, **P < 0.01). Abbreviations: POP-Q, POP quantitative grading; POP-Q 0°, 0 angle when proceeding POP-Q. |
Weight gain during pregnancy in the POP-Q I–IV, POP-Q I–II, and POP-Q III–IV groups from Institution I respectively was 17.21 ± 2.80 kg, 16.26 ± 2.41 kg, and 18.64 ±2.73 kg, respectively. The POP groups exhibited significant statistical differences compared to the control group (13.82 ± 1.93 kg, P < 0.001; Figure 2B). Weight gain during pregnancy in the POP-Q I–IV, POP-Q I–II, and POP-Q III–IV groups from Institution 2 was 15.60 ± 2.24 kg, 15.03 ± 2.10 kg, and 16.37 ± 2.20 kg, respectively. The POP groups exhibited significant statistical differences compared to the control group (13.12 ± 2.11 kg, P < 0.001; Figure 2C).
Association Between Weight Retention 6 Months Postpartum and POP
The POP-Q I–IV group Δ = 7.28 ± 2.06 kg, whereas the control group Δ = 4.36 ±1.81 kg. A significant difference was observed between the two groups (P < 0.001; Figure 3A). The overall Δ values of the POP-Q I–II and POP-Q III–IV groups were 6.63 ± 1.71 kg and 8.23 ± 2.14 kg, respectively, with significant statistical differences compared to the control group (P < 0.001; Figure 3A).
 |
Figure 3 Association between weight retention at 6 months postpartum and POP. (A) Weight changes in the POP-Q I–IV, POP-Q I–II, POP-Q III–IV, and non-POP groups at 6 months postpartum in two research centers are shown. The comparison results are as follows: 7.28 ± 2.06 vs 4.36 ± 1.81, **P < 0.01; 6.63 ± 1.71 vs 4.36 ± 1.81, **P < 0.01; and 8.23 ± 2.14 vs 4.36 ± 1.81, **P < 0.01. (B) Weight changes at 6 months postpartum among the POP-Q I–IV, POP-Q I–II, POP-Q III–IV, and non-POP-Q groups from Institution 1 are presented (7.77 ± 2.19 vs 4.69 ± 1.99, **P < 0.01; 6.99 ± 1.94 vs 4.69 ± 1.99, **P < 0.01; 8.96 ± 1.99 vs 4.69 ± 1.99, **P < 0.01). (C) Weight changes at 6 months postpartum among the POP-Q I–IV, POP-Q I–II, POP-Q III–IV, and non-POP groups from Institution 2 are presented (6.50 ± 1.53 vs 4.05 ± 1.57; **P < 0.01; 6.03 ± 0.96 vs 4.05 ± 1.57, **P < 0.01; 7.13 ± 1.87 vs 4.05 ± 1.57, **P < 0.01). Abbreviations: POP-Q, POP quantitative grading; POP-Q 0°, 0 angle when proceeding POP-Q. |
The findings from Institution 1 indicated that the POP-Q I–IV, POP-Q I–II, and POP-Q III–IV group Δ values were 7.77 ± 2.19 kg, 6.99 ±1.94 kg, and 8.96 ± 1.99 kg, respectively. These values exhibited significant statistical differences compared to the control group (4.69 ± 1.99 kg, P < 0.001; Figure 3B). The Institution 2- POP-Q I–IV, POP-Q I–II, and POP-Q III–IV group Δ values were 6.50 ± 1.53 kg, 6.03 ± 0.96 kg, and 7.13 ± 1.87 kg, respectively. These values exhibited significant statistical differences compared to the control group (4.05± 1.57 kg, P < 0.001; Figure 3C).
Discussion
The association between perinatal weight changes (pre-pregnancy BMI, weight gain during pregnancy, and weight retention at six months postpartum) and the occurrence of POP in populations from two distinct regions in northern and southwestern China was examined. The findings of the current study support the conclusion that a pre-pregnancy BMI < 23 kg/m2 does not increase the risk of POP; however, gestational weight gain ≥14 kg and weight retention ≥5 kg at 6 months postpartum can significantly increase the risk of POP.
Association Between Pre-Pregnancy BMI and POP
Studies have demonstrated a positive association between BMI and POP incidence, indicating that overweight women are 8.5-fold more likely to develop POP than normoweight women.3,12,13 Both centrally and non-centrally obese women can experience collagen metabolism imbalance and pelvic floor tissue relaxation due to sustained increased intra-abdominal pressure and mechanical traction on pelvic floor support structures such as ligaments, fascia, and muscles.14 The current study revealed no statistically significant difference in the pre-pregnancy BMI between the experimental and control groups. This finding supports the notion that BMI is not significantly correlated with the development of POP, as in the meta-analysis by Zenebe et al.15
BMI has a threshold effect on POP. Fitz et al16 reported a positive association between BMI ≥ 30 kg/m2 and POP occurrence, whereas BMI ≤ 25 kg/m2 was not considered a risk factor for POP. Ashikari et al16 have also reported a positive association between a BMI ≥ 23.1 kg/m2 and the occurrence of POP. Our findings are highly consistent with those of Ashikari et al,16 indicating that a pre-pregnancy BMI of <23 kg/m2 does not increase the risk of POP.
Association Between Weight Gain During Pregnancy and POP
Perinatal weight gain plays a significant role in POP development. A significant association has been observed between weight gain during pregnancy and pelvic floor functional disorders in postpartum women.10,17,18 Excessive weight gain during pregnancy leads to excessive fat accumulation in the abdomen and an increase in uterine volume, which elevates intra-abdominal pressure and exerts sustained pressure on the pelvic floor muscles and bladder.17,18 Long-term compression of the pelvic floor ligaments, nerves, blood vessels, and other tissues results in weakened pelvic floor muscle strength and fascial damage, thereby altering the normal structure and anatomical position of the urethra and bladder, which leads to a loss of original support and POP.8,18
Exceeding the weight gain range recommended for pregnancy by the Institute of Medicine (<18 kg) has been shown to significantly increase the incidence of POP.19 The overall weight gain during pregnancy (≥14 kg) among patients with POP was notably higher than that among women without POP in the current study. Women in the two geographic regions of China who gained ≥14 kg during pregnancy had a significantly increased risk of POP despite not exceeding the Institute of Medicine. Therefore, the current study emphasized that it is crucial to develop tailored weight management plans for different regional populations throughout pregnancy to effectively promote pelvic health.19,20
Association Between Weight Retention 6 Months Postpartum and POP
Research has shown that postpartum weight retention is significantly associated with pelvic floor dysfunction (PFD) and serves as an independent risk factor for PFD.21 The association between weight retention at 6 months postpartum and POP was determined in the current study, which revealed that the experimental group exhibited significantly higher weight retention at 6 months postpartum (≥5 kg) than the control group. This association was consistent between the two sub-institutional analyses. These results indicate that the impact of postpartum weight retention is ubiquitous. This finding aligns with previous research findings.21,22 Postpartum weight retention leads to continuous accumulation of abdominal fat, which increases intra-abdominal pressure and causes long-term compression of pelvic floor muscles and nerves. This process delays postpartum pelvic floor tissue repair and exacerbates functional damage.23 Therefore, postpartum weight retention can increase the risk of developing POP. Postpartum weight management is a crucial aspect of POP prevention, and the 6-month period following childbirth is a critical stage for postpartum weight recovery.
Although the current study did not directly explore the interaction between weight gain during pregnancy and weight retention at six months postpartum, it has been previously reported that women who gain excessive weight during pregnancy are more prone to postpartum fat retention, regardless of pre-pregnancy BMI.24 Effective control of weight gain during pregnancy can reduce the risk of postpartum weight retention and indirectly improve the pelvic floor prognosis. Therefore, it is imperative to integrate the ongoing weight management before, during, and after pregnancy into a comprehensive management plan to prevent and control POP. It is recommended that obstetricians and gynecologists prevent the occurrence of POP through weight management during pregnancy. Based on the pre-pregnancy BMI of Chinese women and the results of this study, it is recommended to provide a weight gain management plan during pregnancy. It is suggested that women’s weight gain during pregnancy be controlled within <14 Kg and within <7 Kg in the first and second trimesters, which can effectively prevent the occurrence of POP.
The limitations of the current study are as follows. First, this was a retrospective study which only included patients from two medical centers, limiting the generalization to other population groups. Second, the association between BMI gain during pregnancy and POP was studied without analyzing other factors that may be complex to the overall health status of women; confounding factors such as occupation, sedentary behaviors, delivery methods, and menopause may lead to a degree of bias to the results. Third, the current study did not analyze the treatment of POP after production. Fourth, the use of questionnaire for collecting part of the information may lead to some recall bias on the results. Fifth, the lack of long-term follow-up beyond 6 months postpartum weakened the validity of the evidence. Randomized trial from multi-centers with large samples and long-term follow up is needed to validate the results. Further studies should take consideration of the controlling or the confounding factors like occupation, sedentary behaviors, delivery methods, and menopause, and the treatment of POP after production when analyzing the data.
Conclusion
The current study continuously analyzed the impact of pre-pregnancy BMI, weight gain during pregnancy, and weight retention at six months postpartum on POP in populations from two distinct regions in northern and southwestern China. A pre-pregnancy BMI < 23 kg/m2 does not increase the risk of POP; however, gestational weight gain ≥14 kg and weight retention ≥5 kg at 6 months postpartum can significantly increase the risk of POP. Women should be advised to limit gestational weight gain to <14 kg and avoid >5 kg weight retention by 6 months postpartum to lower POP risk.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
This study was approved by the Ethics Committees of both institutions and was proceeded in compliance with the Declarations of Helsinki. The requirement for written informed consent was waived by the ethics committee owing to the retrospective design of the study. All the data were anonymized or removed the personally identifiable information, and securely stored to maintain with patient data confidentiality.
Funding
There is no funding to report.
Disclosure
Not conflict of interest was reported by the authors.
References
1. Mou T, Warner K, Brown O, et al. Prevalence of pelvic organ prolapse among US racial populations: a systematic review and meta-analysis of population-based screening studies. Neurourol Urodyn. 2021;40(5):1098–1106. doi:10.1002/nau.24672
2. Mukwege A, Harlow SD, Hood MM, Reed BD, Dugan SA, Miller JM. Race/ethnicity and incidence of pelvic organ prolapse in midlife women: the study of Women’s health across the nation. J Womens Health. 2024;33(8):1042–1051. doi:10.1089/jwh.2023.0804
3. Kato J, Nagata C, Miwa K, Ito N, Morishige KI. Pelvic organ prolapse and Japanese lifestyle: prevalence and risk factors in Japan. Int Urogynecol J. 2022;33(1):47–51. doi:10.1007/s00192-021-04672-7
4. Bilgic D, Gokyildiz S, Kizilkaya Beji N, Yalcin O, Gungor Ugurlucan F. Quality of life and sexual function in obese women with pelvic floor dysfunction. Women Health. 2019;59(1):101–113. doi:10.1080/03630242.2018.1492497
5. Friedman T, Dietz HP. Does obesity change the perception of pelvic organ prolapse? Arch Gynecol Obstet. 2022;305(6):1491–1495. doi:10.1007/s00404-022-06430-6
6. Tian Z, Wang X, Hu X, Sun Z. Effect of surgically induced weight loss on pelvic organ prolapse: a meta-analysis. Obes Surg. 2023;33(11):3402–3410. doi:10.1007/s11695-023-06867-x
7. Lee UJ, Kerkhof MH, van Leijsen SA, Heesakkers JP. Obesity and pelvic organ prolapse. Curr Opin Urol. 2017;27(5):428–434. doi:10.1097/MOU.0000000000000428
8. Wang K, Xu X, Jia G, Jiang H. Risk factors for postpartum stress urinary incontinence: a systematic review and meta-analysis. Reprod Sci. 2020;27(12):2129–2145. doi:10.1007/s43032-020-00254-y
9. Zhou Y, Luo Y, Zhou Q, Xu J, Tian S, Liao B. Effect of gestational weight gain on postpartum pelvic floor function in twin primiparas: a single-center retrospective study in China. BMC Pregnancy Childbirth. 2023;23(1):273. doi:10.1186/s12884-023-05602-9
10. Sun S, Li H, Liu M, Shang Q, Tan Q, Yin W. An evaluation of the effects of gestational weight gain on the early postpartum pelvic floor using transperineal ultrasound. J Ultrasound Med. 2023;42(10):2331–2338. doi:10.1002/jum.16257
11. Gynecological Pelvic Floor Group. Obstetrics and Gynecology Branch of Chinese Medical Association. Chinese guideline for the diagnosis and management of pelvic orang prolapse (2020 version). Chin J Obstet Gynecol. 2020;55(05):300–306.
12. Gabra MG, Tessier KM, Fok CS, Nakib N, Oestreich MC, Fischer J. Pelvic organ prolapse and anal incontinence in women: screening with a validated epidemiology survey. Arch Gynecol Obstet. 2022;306(3):779–784. doi:10.1007/s00404-022-06510-7
13. Edmealem A, Ademe S, W/Selassie M. Determinants of pelvic organ prolapse among gynecologic patients, Northeastern Ethiopia, 2020: a case-control study. Womens Health. 2023;19:17455057231164549.
14. Si K, Yang Y, Liu Q, et al. Association of central and general obesity measures with pelvic organ prolapse. Obstet Gynecol. 2025;145(1):108–114. doi:10.1097/AOG.0000000000005758
15. Zenebe CB, Chanie WF, Aregawi AB, Andargie TM, Mihret MS. The effect of women’s body mass index on pelvic organ prolapse: a systematic review and meta analysis. Reprod Health. 2021;18(1):45. doi:10.1186/s12978-021-01104-z
16. Fitz FF, Bortolini MAT, Pereira GMV, Salerno GRF, Castro RA. PEOPLE: lifestyle and comorbidities as risk factors for pelvic organ prolapse-a systematic review and meta-analysis PEOPLE: PElvic Organ Prolapse Lifestyle comorbiditiEs. Int Urogynecol J. 2023;34(9):2007–2032. doi:10.1007/s00192-023-05569-3
17. Gao Q, Wang M, Zhang J, et al. Pelvic floor dysfunction in postpartum women: a cross-sectional study. PLoS One. 2024;19(10):e0308563. doi:10.1371/journal.pone.0308563
18. Falah-Hassani K, Reeves J, Shiri R, Hickling D, McLean L. The pathophysiology of stress urinary incontinence: a systematic review and meta-analysis. Int Urogynecol J. 2021;32(3):501–552. doi:10.1007/s00192-020-04622-9
19. Truong YN, Yee LM, Caughey AB, Cheng YW. Weight gain in pregnancy: does the Institute of Medicine have it right? Am J Obstet Gynecol. 2015;212(3):362.e1–e8. doi:10.1016/j.ajog.2015.01.027
20. Shao FX, He P, Mao YJ, et al. Association of pre-pregnancy body mass index and gestational weight gain on postpartum pelvic floor muscle morphology and function in Chinese primiparous women: a retrospective cohort study. Int J Gynaecol Obstet. 2025;168(2):680–692. doi:10.1002/ijgo.15870
21. Nygaard IE, Bardsley T, Sheng X, Murtaugh MA, Shaw JM. Habitus and pelvic floor symptoms and support 1 year postpartum. Obstet Gynecol. 2021;137(5):821–830. doi:10.1097/AOG.0000000000004349
22. Liang CC, Tseng LH, Horng SG, Lin IW, Chang SD. Correlation of pelvic organ prolapse quantification system scores with obstetric parameters and lower urinary tract symptoms in primiparae postpartum. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(5):537–541. doi:10.1007/s00192-006-0195-6
23. Chen Y, Johnson B, Li F, King WC, Connell KA, Guess MK. The effect of body mass index on pelvic floor support 1 year postpartum. Reprod Sci. 2016;23(2):234–238. doi:10.1177/1933719115602769
24. Subhan FB, Shulman L, Yuan Y, et al. Association of pre-pregnancy BMI and gestational weight gain with fat mass distribution and accretion during pregnancy and early postpartum: a prospective study of Albertan women. BMJ Open. 2019;9(7):e026908. doi:10.1136/bmjopen-2018-026908
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.