Back to Journals » International Journal of Women's Health » Volume 17
Association Between Short Birth Interval and Immediate Adverse Perinatal Outcomes Among Women Delivering at a Tertiary Hospital in South-Western Uganda
Authors Yel YAA, Kanyesigye H ![]() , Kato PK, Tibaijuka L
, Kato PK, Tibaijuka L ![]() , Akandwanaho G, Turanzomwe S
, Akandwanaho G, Turanzomwe S ![]() , Akello RA, Ngonzi J, Kayondo M, Byamukama O
, Akello RA, Ngonzi J, Kayondo M, Byamukama O ![]()
Received 26 May 2025
Accepted for publication 18 September 2025
Published 23 September 2025 Volume 2025:17 Pages 3167—3177
DOI https://doi.org/10.2147/IJWH.S531698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Yel Akol Akol Yel,1 Hamson Kanyesigye,1,* Paul Kalyebara Kato,1 Leevan Tibaijuka,1,2 Gideon Akandwanaho,1 Stuart Turanzomwe,1 Rebecca Agness Akello,1 Joseph Ngonzi,1 Musa Kayondo,1 Onesmus Byamukama1,2,*
1Department of Obstetrics and Gynecology, Mbarara University of Science and Technology, Faculty of Medicine, Mbarara, Uganda; 2Department of Obstetrics and Gynecology, Mbarara Regional Referral Hospital, Mbarara, Uganda
*These authors contributed equally to this work
Correspondence: Onesmus Byamukama, Department of Obstetrics and Gynaecology, Mbarara University of Science and Technology, P.O. Box 1410, Mbarara, Uganda, Tel +256 784124742, Email [email protected]
Purpose: Immediate adverse perinatal outcomes (IAPO) are more likely to occur in women with short inter-birth birth intervals (SIBI) compared to optimal inter-birth interval (OIBI). This study determined the association between short inter-birth interval and immediate adverse perinatal outcomes among women delivering at Mbarara Regional Referral Hospital (MRRH).
Patients and Methods: We conducted a cross-sectional study among mother-baby pairs admitted to MRRH postnatal ward within 24 hours after delivery from the period running from March 2023 to June 2023. The primary exposure variable was birth interval and the primary outcome was IAPO. Data was collected using a structured questionnaire. Modified Poisson Regression analysis was used to determine the relationship between birth interval and immediate adverse perinatal outcomes.
Results: Of the 688 participants enrolled, the mean age was 28.06 ± 5.04 years. Majority were married (97.8%) and referred to in (44.6%). Low birth weight was significantly higher among women with SIBI compared to OIBI ((9.9% versus 5.8%, p=0.047), while other adverse outcomes (preterm birth, stillbirth, and NICU admissions) were more frequent but not statistically significant. A SIBI was significantly associated with IAPO (aPR): 1.46; 95% C. I [1.02, 2.09], p=0.038). Other factors independently associated with adverse perinatal outcomes were maternal age< 20 years ([aPR]: 2.66; 95% C.I [1.05,6.73], p=0.039), obstetric complications (aPR: 2.16; 95% C.I [1.34, 3.48], p=0.002), having a diagnosis of fetal distress (aPR: 2.61; 95% C.I [1.80, 3.79], p< 0.001), and a history of malaria in pregnancy (aPR: 1.66; 95% C.I [1.12, 2.48], p=0.013).
Conclusion: A SIBI significantly increases the risk of IAPO. Additionally, maternal age below 20 years, the presence of obstetric complications, a diagnosis of fetal distress, and a history of malaria in pregnancy independently contribute to these unfavorable outcomes. We recommend health education and advocacy with emphasis for the utilization of family planning services so as to have OIBI.
Keywords: birth intervals, adverse perinatal outcomes, Uganda
Introduction
A birth interval is defined by WHO (World Health Organization) as the time between two consecutive births, recommending that a birth interval is between 33 and 69 months for ideal maternal and neonatal outcomes, and an interval less than 33 months is considered as short. Globally, 25% of child births occur at an interval below 33 months with comparatively higher proportions in central Asia (33%) and Sub-Saharan Africa (57%).2 There is a variation in the burden of short birth intervals in African countries and it ranges from 18 to 54.2–4 In Uganda, the burden has been found to range from 33% to 54%.5,6
Multiple studies have shown an increased occurrence of immediate adverse perinatal outcomes like; stillbirth, small for gestational age (SGA), low birth weight, low 5-minute APGAR score neonatal intensive care unit admission, and early neonatal deaths in women with a short birth interval compared to those with an optimal birth interval.7–9 These adverse perinatal outcomes have been reported in studies done in Tanzania, Egypt, South Africa, and Sudan and their occurrence ranges from 4% to 29%.10,11 However, a study done in Nigeria showed no association between short birth intervals and adverse perinatal outcomes.8 Optimal inter-birth intervals (OIBI) in obstetric care promote good perinatal outcomes.12
There are various reasons why women with short birth intervals have a high chance of having adverse perinatal outcomes. This can be because of the partially healed genital tract, unresolved inflammation from the prior pregnancy which leads to increased release of mediators like IL 1, 6, 8, and tumor necrotic factors which can initiate early rupture of membranes and preterm labor. The inadequate restoration of macro- and micronutrient depletions which results in a reduction of the availability of these nutrients to the fetus can lead to intrauterine growth retardation, hypoxia, and acidosis causing low APGAR score or perinatal death in severe forms.13–15 The relationship between short birth intervals and adverse perinatal outcomes is moderated by several other factors including socio-demographic, clinical, and obstetrics factors.16–19
Uganda has a higher number of women with short birth intervals (33–52%) which is much more than the global average prevalence (25%).4,6,7 Previous studies in our settings have concentrated on estimating the magnitude of short birth intervals. However, it is not documented in our setting whether these observed immediate adverse perinatal outcomes occur more among women with short birth intervals as compared to those with optimal birth intervals. The relationship between immediate adverse perinatal outcomes and short birth intervals is also not known in our setting. This study therefore assessed the relationship between birth intervals and immediate adverse perinatal outcomes of women delivering at Mbarara Regional Referral Hospital.
Methods
Study Setting, Study Design, and Study Population
This was a correlative, cross-sectional study among mother-baby pairs admitted to Mbarara Regional Referral hospital postnatal ward within 24 hours after delivery. This study was conducted in the postnatal ward of Mbarara Regional Referral Hospital (MRRH). It is situated in the southwestern part of Uganda, Mbarara city and it is a public, government-owned, tertiary hospital and while it is also a teaching hospital for Mbarara University of Science and Technology. It was funded by the Government of Uganda through the Ministry of Health. The hospital has a bed capacity of 350, 40 of which are on post-natal wards. The hospital conducts approximately 11,000 deliveries every year. The burden of SIBI in Uganda ranges from 33% to 52%.5,6 Majority of the patients that come to the hospital, from who we sampled are from Ankole and Kigezi sub-regions of Uganda, and commonly speak Runyankole and Rukiga. Some of the patients come from Lyantonde, Toro and Rwenzori sub-regions and speak Luganda, Rutoro and Rukonjo languages.
Our study population was mother-baby pairs with short or optimal birth intervals. We included all mother-baby pairs delivered at MRRH with short or optimal inter-birth intervals within 24 hours after delivery. We excluded mothers who had multiple pregnancies.
Sample Size and Sampling
We used Open Epi Version 3 to determine the sample size following sample size determination for comparative cross-sectional studies. Dean AG, Sullivan KM, Soe MM. OpenEpi: Open-Source Epidemiologic Statistics for Public Health, Version. Www.OpenEpi.com. We considered findings from a study done in Khartoum Hospital, Sudan considering proportions of low birth weight among women with short birth intervals and optimal birth intervals (12.9% versus 6.0%, p-value=0.004).20 Assuming a 95% confidence interval. Adjustment for the 10% non-response rate, we estimated the final sample size of 688 participants. The sample size was stratified into, 344 women with short birth intervals and 344 women with optimal birth intervals.
We used stratified sampling by dividing participants into short and optimal inter-birth interval groups, then applied simple random sampling (lottery method) to select 4 participants from each group daily over 3 months, achieving a total sample of 688 (344 per group).
Data Collection and Study Variables
The data collection process consisted of a principal investigator and two (2) research assistants who used interviewer-guided questionnaires that were structured in line with the research study. The research assistants who collected the data were midwives, who trained on the data collection tool and study procedures. Our primary exposure variable was the birth interval which was dichotomized as optimal if the birth interval was between 33 and 69 months and short if it was less than 33 months.
The dependent variable was immediate adverse perinatal outcomes as defined by the occurrence of one or more of these outcomes; stillbirth, preterm birth, birth weight of less than 2,500g, Apgar score less than 7 at 5 minutes, immediate neonatal death (death of the newborn within 24 hours after birth), and intensive-neonatal care unit admission. These were selected based on literature which had shown that these are most common perinatal outcomes within 24 hours of delivery. Data were captured on independent variables including socio-demographic, and obstetric factors, and medical factors. With the socio-demographic characteristics including Age, Education level, Referral status, marital status, Place of Residence, and Religion while Obstetric factors included Level of the facility, number of ANC visits, gestational age at delivery, prior cesarean delivery, history of stillbirth, parity, Mode of delivery, use of uterotonic, fetal presentation, fetal distress, a cadre of birth attendant, and use of labor care guide/partograph for labor monitoring, and presence of medical conditions which included HIV/AIDS, Diabetes mellitus, Heart disease, Malaria, Renal disease, Anemia.
Data Management and Analysis
Data collected was entered into pen Epi and exported to STATA software, version 17 for cleaning and analysis. There was comparison between the proportion of immediate adverse perinatal outcomes among women with optimal birth intervals and those with short birth intervals, we tabulated the frequencies of the immediate adverse perinatal outcome in each group, the chi-square test was used to compare the frequencies among the two groups and the level of significance.
To ascertain the association between birth interval and the immediate adverse perinatal outcomes, we used the modified Poisson Regression analysis. We reported Corresponding prevalence ratios (PRs) with their 95% confidence intervals (CIs) as our measures of association. Odds ratios were not used in this study as measure of association because of their potential to overestimate the effect size if the prevalence of the outcome of interest is high. Biologically plausible independent variables and those with a p-value of less than 0.2 during bivariate analysis were added to a final multivariable model. The statistically significant factors were those with a p-value of 0.05 or less at this level. Depending on the p-value short birth interval was considered to be associated with immediate adverse perinatal outcomes. Other variables that had a p-value of less than 0.05 were considered to be significantly associated with immediate adverse perinatal outcomes. 95% confidence intervals, prevalence ratios, and p-values that corresponded were also reported.
Results
Mother-baby pairs of 693 admitted to the postnatal ward within twenty-four hours after giving birth were screened for eligibility. A total of 688 mothers were screened and enrolled in the study. Three hundred and forty-four had SIBI, while 344 had OIBI. Of these, 109 newborns had at least one immediate adverse perinatal outcome (Figure 1).
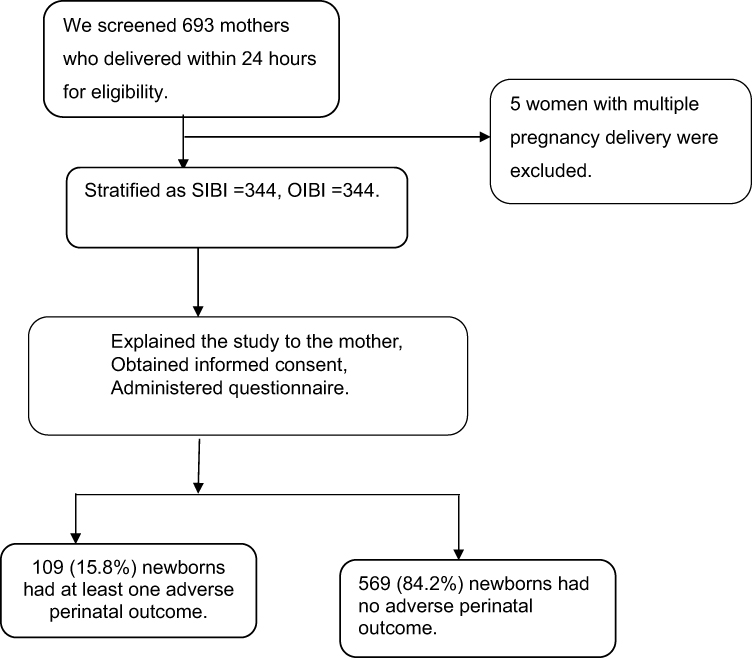 |
Figure 1 Flow chart for recruitment of study participants at Mbarara Regional Referral Hospital, southwestern Uganda. |
Socio-Demographic Characteristics of the Study Participants
The participants’ mean age was 28.06 ±5.04 years. With most of them married (97.8%), and had a secondary level of education (42.4%), were referred in (44.6%) and were Anglicans (49.7%). There was no significant difference in socio-demographic components of the participants (Table 1).
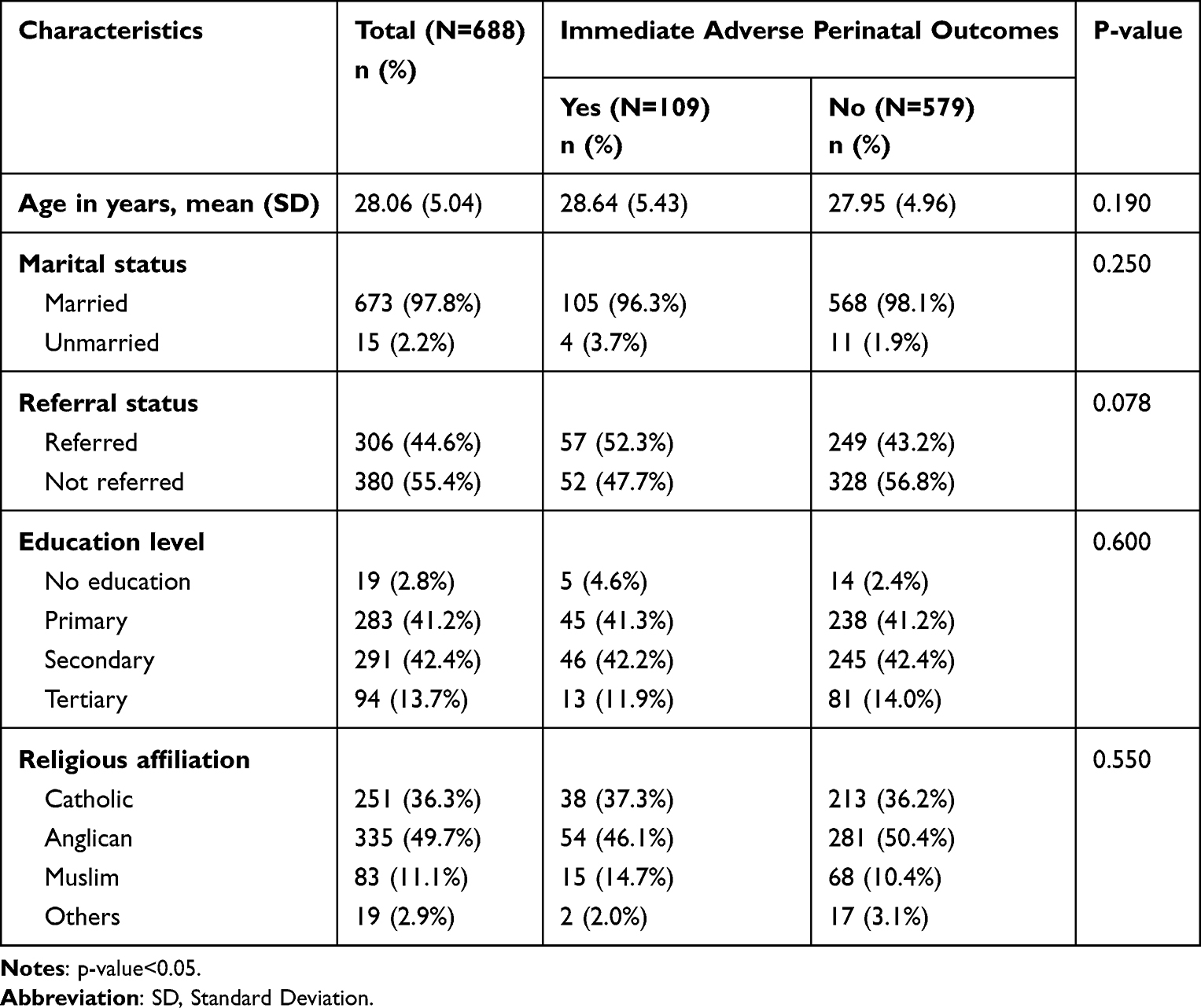 |
Table 1 Socio-Demographic Characteristics of Women That Delivered From Mbarara Regional Referral Hospital |
Obstetric Characteristics of Study Participants
The mean birth interval (SD) was 35.54 months (13.71). The participants who had immediate adverse perinatal outcomes tended to have short birth intervals (32.65±12.81 months) compared to those who had no immediate adverse perinatal outcomes (36.09±13.82 months) and this difference was statistically significant. The majority of participants had attended four or more ANC visits (75.7%), were multigravidae (83.0%) and delivered by caesarean section (59.7%). Eleven percent (11.5%) had a diagnosis of fetal distress, 7.8% had an obstetric complication in the current pregnancy, and 15.1% had suffered malaria in pregnancy. There was a significant difference in the proportions of adverse perinatal outcomes in the characteristics of interdelivery interval, parity, history of stillbirth, obstetric complications, mode of delivery, HIV status and history of malaria in the current pregnancy (Table 2).
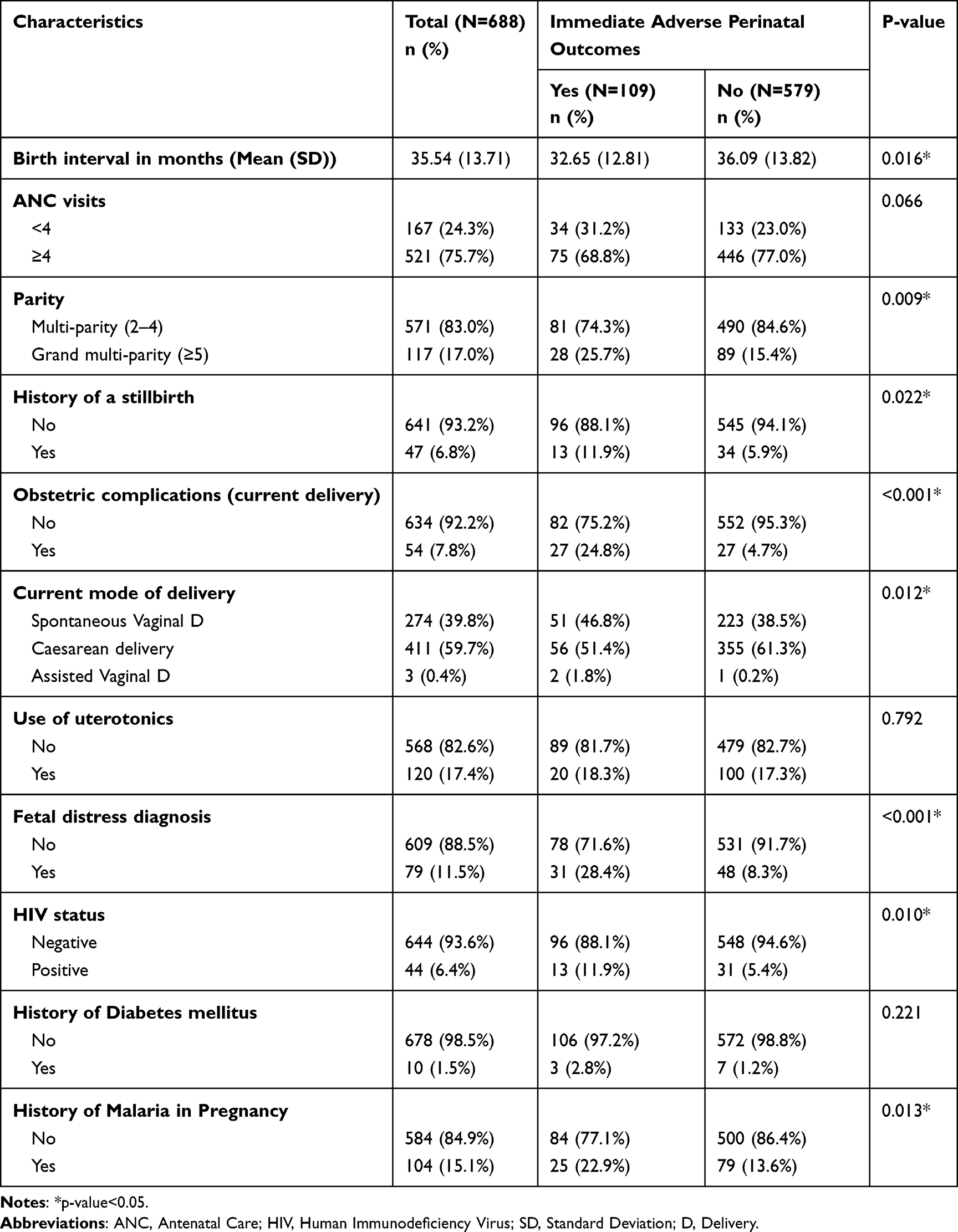 |
Table 2 Obstetric Characteristics of Women Who Had Delivery at Mbarara Regional Referral Hospital |
Immediate Adverse Perinatal Outcomes
Compared to women with optimal inter-birth interval (OIBI), women with a short inter-birth intervals (SIBI) had a significantly higher proportion of adverse perinatal outcomes (18.9% versus 12.8%, p=0.028). Low birth weight (<2.5 kilograms) was statistically significantly higher among women with SIBI compared to the OIBI (9.9% versus 5.8%, p=0.047). Other adverse outcomes were higher among those with SIBI compared to those with OIBI [preterm births (10.8% versus 7.3%), still births (6.1% versus 4.1%) and NICU admissions (11.0 versus 10.2%]; however, these were not statistically significant (Table 3).
 |
Table 3 Immediate Adverse Perinatal Outcomes |
Factors Associated with Immediate Adverse Perinatal Outcomes Among Participants
At multivariable analysis, immediate adverse perinatal outcomes were significantly associated with a short birth interval. Women with short birth intervals had 1.46 times more chances to have immediate adverse perinatal outcomes compared to women with optimal birth intervals (aPR): 1.46; 95% C.I [1.02, 2.09], p=0.038.
Other factors that were independently associated with immediate adverse perinatal outcomes included maternal age<20 years, obstetric complications, and having a diagnosis of fetal distress, and a history of malaria in pregnancy. Women aged <20 years were more likely about 2.66 times to have adverse perinatal outcomes in comparison to those aged 20–34 years ([aPR]: 2.66; 95% C.I [1.05,6.73], p=0.039). Women with obstetric complications were about 2.16 times more likely to have immediate adverse perinatal outcomes compared to those without obstetric complications, (aPR: 2.16; 95% C.I [1.34, 3.48], p=0.002). Having a diagnosis of fetal distress was about 2.16 times associated with immediate adverse perinatal outcomes compared to those without a diagnosis of fetal distress (aPR: 2.61; 95% C.I [1.80, 3.79], p<0.001). Women with a history of malaria in pregnancy were about 1.66 times more likely to have immediate adverse perinatal outcomes in comparison to those without a history of malaria (aPR: 1.66; 95% C.I [1.12, 2.48], p=0.013) (Table 4).
 |
Table 4 Factors Associated with Immediate Adverse Perinatal Outcomes Among Women Delivering at Mbarara Regional Referral Hospital |
Discussion
This study found that the proportion of immediate adverse perinatal outcomes was significantly higher among women with short birth intervals compared to those with optimal birth intervals (18.9% vs 12.8%, p=0.028). The overall high proportion of IAPO may reflect the referral nature of Mbarara Regional Referral Hospital (MRRH), which manages high-risk pregnancies, including 52% of participants referred in. Limited studies have specifically quantified adverse perinatal outcomes in short birth intervals. Our findings align with proportions reported in Denmark, Tanzania, and Ethiopia (22.4%, 21%, and 24%, respectively).21,22 The higher proportions in these studies may be attributable to differences in study design, such as population-based registers and prospective cohorts.
Low birth weight was significantly associated with SIBI in our study (9.9% vs 5.8%, p=0.047), consistent with findings from Sudan (12.9% vs 6.0%); [20] and Pakistan (2.6 times higher among short birth interval group).23 This association is attributed to inadequate restoration of maternal micronutrients, leading to intrauterine growth restriction.13–15 Although not statistically significant, other adverse perinatal outcomes such as stillbirths (6.1% vs 4.1%), preterm births (10.8% vs 7.3%), and NICU admissions (11.0% vs 10.2%) were more frequent in short birth interval group. Similar trends were noted in Tanzania, where preterm births (12.57% vs 10.51%) and perinatal deaths (4.14% vs 2.92%) were higher among women with SIBI.24 Systematic reviews in high-resource settings also report higher proportions of adverse outcomes, despite a lack of significant associations with NICU admissions or low Apgar scores.8 Contrasting findings in Nigeria and Spain showed no significant association between short birth interval and adverse outcomes.25 This discrepancy could stem from methodological differences, including smaller sample sizes and differing definitions of SIBI.
Maternal age <20 years was significantly associated with IAPO (OR 2.66). This is similar to findings in a multi-country study that indicated a two-fold risk of IAPO among adolescents.26 Adolescent pregnancies are often associated with insufficient antenatal care and a higher risk of complications such as hypertensive disorders, contributing to adverse outcomes.27,28 Obstetric complications (eg, uterine rupture, antepartum hemorrhage hypertensive disorders) were also significantly associated with IAPO (OR 2.16). Similar findings were reported in studies from South Korea and MRRH, highlighting the role of reduced uteroplacental perfusion in adverse outcomes.29,30 Fetal distress was strongly associated with IAPO (OR 2.16). This finding aligns with studies in India and by Gluck et al, which documented increased risks of perinatal complications due to fetal acidemia and meconium aspiration.29 Finally, malaria in pregnancy increased the risk of IAPO by 1.66 times. This is consistent with studies in Uganda, which identified placental injury and insufficiency caused by malaria as contributors to low birth weight.31,32
Strengths and Limitations
This study had notable strengths, including a relatively large sample size with equal representation of women with short and optimal birth intervals, which enhanced the validity of comparisons between groups. The use of stratified random sampling minimized selection bias and ensured representativeness, while data triangulation with medical records reduced recall and reporting errors. The application of modified Poisson regression provided robust estimates of association for outcomes with relatively high prevalence. However, the study also had limitations. Being cross-sectional in design, it could only demonstrate associations rather than causal relationships. Some data, particularly socio-demographic and past obstetric history, were self-reported, raising the possibility of social desirability and recall bias. In addition, the study was hospital-based at a tertiary referral facility, which typically receives high-risk pregnancies, potentially limiting generalizability to the wider community.
Conclusion
The proportion of immediate adverse perinatal outcomes is higher among women with short birth intervals compared to those with optimal birth intervals delivered at Mbarara Regional Referral Hospital. A short birth interval is significantly associated with these outcomes, emphasizing its role as a risk factor. Additionally, other factors that were independently linked to adverse perinatal outcomes included maternal age below 20 years, a diagnosis of fetal distress, obstetric complications, and a history of malaria during the current pregnancy.
These outcomes highlight the urgent demand for interventions targeted to address high-risk groups such as women with short birth intervals, adolescent pregnancies, and obstetric complications. Strengthening and scaling up postpartum child-spacing programs is essential to prevent short birth intervals and reduce detrimental perinatal outcomes in this population.
Abbreviations
IAPO, Immediate Adverse perinatal outcomes; ANC, Antenatal Care; IBI, Inter-birth intervals; MRRH, Mbarara Regional Referral Hospital; MUST, Mbarara University of Science and Technology NICU, Neonatal Intensive care unit; OIBI, Optimal Inter-Birth Interval; PIBI, Prolonged Inter-birth interval; PROM, Premature Rupture Of Membranes; REC, Research Ethics Committee; SGA, Small for Gestational Age; SIBI, Short Inter-birth Interval; TNF, Tumor Necrotic Factors; UB, University of Bahri; UNCST, Uganda National Council of Science and Technology; WHO, World Health Organization.
Data Sharing Statement
The datasets for this study are available on request from the corresponding author.
Ethical Approval and Consent of Participation
The protocol for the research was ethically reviewed and authorized by the institutional ethics bodies, specifically the Research Ethics Committee, Mbarara University (approval reference MUST- 2022-747) and with reference number HS3043ES with Uganda National Council for Science and Technology. Additionally, authorization from the administration of Mbarara Regional Referral Hospital was secured before the initiation of any research activities. Participants provided voluntary, written informed consent prior to enrollment, with assurances of privacy maintained by assigning anonymized codes rather than personal identifiers. Participation remained voluntary throughout, and participants retained the right to exit the study without repercussions. Participants experiencing neonatal loss were provided access to professional counseling services for emotional and psychological assistance. Upon completion of data collection, participants received education on reproductive health and options for postpartum contraception if interested. The ethical principles of the Declaration of Helsinki and the CIOMS-2002 (Council for International Organizations of Medical Sciences) guidelines were strictly adhered to, ensuring that participants faced no physical or psychological risks during the research.
Acknowledgment
This paper is based on the thesis of Yel Akol Akol Yel, which has been published in the Institutional Repository of Mbarara University of Science and Technology, accessible at: https://med.must.ac.ug/wp-content/uploads/2023/11/ABSTRACT-Yel-Akol.pdf. We thank all the women voluntarily accepted to participate in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received funding from the Maternal Newborn and Child health Institute (MNCHI) of Mbarara University of Science and Technology.
Disclosure
The authors declare that they have no conflicts of interest related to the publication of this work.
References
1. Organization WH. Report of a WHO technical consultation on birth spacing: Geneva, Switzerland 13–15 June 2005; 2007.
2. Rutstein SO. Trends in Birth Spacing. ICF Macro; 2011.
3. Ajayi AI, Somefun OD. Patterns and determinants of short and long birth intervals among women in selected sub-Saharan African countries. Medicine. 2020;99(19):e20118. doi:10.1097/MD.0000000000020118
4. Damtie Y, Kefale B, Yalew M, Arefaynie M, Adane B. Short birth spacing and its association with maternal educational status, contraceptive use, and duration of breastfeeding in Ethiopia. A systematic review and meta-analysis. PLoS One. 2021;16(2):e0246348. doi:10.1371/journal.pone.0246348
5. Aleni M, Mbalinda S, Muhindo R. Birth intervals and associated factors among women attending young child clinic in Yumbe Hospital, Uganda. Int J Reprod Med. 2020;2020(1):1326596. doi:10.1155/2020/1326596
6. Byamukama O, Migisha R, Kalyebara PK, et al. Short interbirth interval and associated factors among women with antecedent cesarean deliveries at a tertiary hospital, Southwestern Uganda. BMC Pregnancy Childbirth. 2022;22(1):268. doi:10.1186/s12884-022-04611-4
7. Bauserman M, Nowak K, Nolen TL, et al. The relationship between birth intervals and adverse maternal and neonatal outcomes in six low and lower-middle income countries. Reprod Health. 2020;17:1–10. doi:10.1186/s12978-020-01008-4
8. Onwuka C, Ugwu E, Obi S, et al. Effects of short inter‑pregnancy interval on maternal and perinatal outcomes: a cohort study of pregnant women in a low‑income country. Niger J Clin Pract. 2020;23(7):928–933. doi:10.4103/njcp.njcp_423_19
9. Yee L, Truong Y, Caughey A, Cheng Y. The association between interdelivery interval and adverse perinatal outcomes in a diverse US population. J Perinatol. 2016;36(8):593–597. doi:10.1038/jp.2016.54
10. Abozeid I, Salem HA-D, Aly Elboghdady A. Effects of a short interpregnancy interval on pregnancy outcomes. Al-Azhar Int Med J. 2021;2(5):12–17.
11. Lilungulu A, Matovelo D, Kihunrwa A, Gumodoka B. Spectrum of maternal and perinatal outcomes among parturient women with preceding short inter-pregnancy interval at Bugando Medical Centre, Tanzania. Maternal Health Neonatol Perinatol. 2015;1:1–7. doi:10.1186/s40748-014-0002-1
12. Randel A. Interpregnancy care: guidelines from ACOG and SMFM. Am Family Phys. 2019;100(2):121–123.
13. Conde-Agudelo A, Rosas-Bermúdez A, Kafury-Goeta AC. Birth spacing and risk of adverse perinatal outcomes: a meta-analysis. JAMA. 2006;295(15):1809–1823. doi:10.1001/jama.295.15.1809
14. Conde‐Agudelo A, Rosas‐Bermudez A, Castaño F, Norton MH. Effects of birth spacing on maternal, perinatal, infant, and child health: a systematic review of causal mechanisms. Stud Fam Plann. 2012;43(2):93–114. doi:10.1111/j.1728-4465.2012.00308.x
15. Tessema ZT, Teshale AB, Tesema GA, Tamirat KS. Determinants of completing recommended antenatal care utilization in sub-Saharan from 2006 to 2018: evidence from 36 countries using Demographic and Health Surveys. BMC Pregnancy Childbirth. 2021;21:1–12. doi:10.1186/s12884-021-03669-w
16. Liyew EF, Yalew AW, Afework MF, Essén B. Maternal near-miss and the risk of adverse perinatal outcomes: a prospective cohort study in selected public hospitals of Addis Ababa, Ethiopia. BMC Pregnancy Childbirth. 2018;18:1–8. doi:10.1186/s12884-018-1983-y
17. Yeshialem E, Abera M, Tesfay A. Determinants of adverse pregnancy outcomes among mothers who gave birth from jan 1-dec 31/2015 in jimma university specialized hospital, case control study, 2016. Ethiopian J Reprod Health. 2019;11(1):10. doi:10.69614/ejrh.v11i1.235
18. Bilano VL, Ota E, Ganchimeg T, Mori R, Souza JP. Risk factors of pre-eclampsia/eclampsia and its adverse outcomes in low-and middle-income countries: a WHO secondary analysis. PLoS One. 2014;9(3):e91198. doi:10.1371/journal.pone.0091198
19. Getaneh A, Tegene B, Belachew T. Knowledge, attitude and practices on cervical cancer screening among undergraduate female students in University of Gondar, Northwest Ethiopia: an institution based cross sectional study. BMC Public Health. 2021;21:1–9. doi:10.1186/s12889-021-10853-2
20. Adam I, Ismail MH, Nasr AM, Prins MH, Smits LJ. Low birth weight, preterm birth and short interpregnancy interval in Sudan. J Matern Fetal Neonatal Med. 2009;22(11):1068–1071. doi:10.3109/14767050903009222
21. Hegelund ER, Urhoj SK, Andersen A-MN, Mortensen LH. Interpregnancy interval and risk of adverse pregnancy outcomes: a register-based study of 328,577 pregnancies in Denmark 1994–2010. Maternal Child Health J. 2018;22:1008–1015. doi:10.1007/s10995-018-2480-7
22. Ilyas S, Latif F, Yasmeen N. Association of short inter-pregnancy interval with adverse perinatal outcome. Pak Postgrad Med J. 2015;26(1):11–17. doi:10.51642/ppmj.v26i1.173
23. Mahande MJ, Obure J. Effect of interpregnancy interval on adverse pregnancy outcomes in northern Tanzania: a registry-based retrospective cohort study. BMC Pregnancy Childbirth. 2016;16:1–9. doi:10.1186/s12884-016-0929-5
24. Ahrens KA, Nelson H, Stidd RL, Moskosky S, Hutcheon JA. Short interpregnancy intervals and adverse perinatal outcomes in high‐resource settings: an updated systematic review. Paediatric Perinatal Epidemiol. 2019;33(1):O25–O47. doi:10.1111/ppe.12503
25. Althabe F, Moore JL, Gibbons L, et al. Adverse maternal and perinatal outcomes in adolescent pregnancies: the Global Network’s Maternal Newborn Health Registry study. Reprod Health. 2015;12:1–9. doi:10.1186/1742-4755-12-S2-S8
26. Kaur J, Kaur K. Obstetric complications: primiparity vs. multiparity. Eur JExp Biol. 2012;2(5):1462–1468.
27. Chami HW, Gueye M, Ndiaye MD, et al. Relation between obstetric outcome and parity. Open J Obst Gynecol. 2019;9(6):894–903. doi:10.4236/ojog.2019.96087
28. Im DH, Kim YN, Cho EH, Kim DH, Byun JM, Jeong DH. Risk factors and pregnancy outcomes of antepartum hemorrhage in women with placenta previa. Reprod Sci. 2023;30(9):2728–2735. doi:10.1007/s43032-023-01191-2
29. Lugobe HM, Muhindo R, Kayondo M, et al. Risks of adverse perinatal and maternal outcomes among women with hypertensive disorders of pregnancy in southwestern Uganda. PLoS One. 2020;15(10):e0241207. doi:10.1371/journal.pone.0241207
30. Gluck O, Kovo M, Tairy D, Herman HG, Bar J, Weiner E. The effect of meconium thickness level on neonatal outcome. Early Human Dev. 2020;142:104953. doi:10.1016/j.earlhumdev.2020.104953
31. De Beaudrap P, Turyakira E, White LJ, et al. Impact of malaria during pregnancy on pregnancy outcomes in a Ugandan prospectivecohort with intensive malaria screening and prompt treatment. Malaria J. 2013;12:1–11. doi:10.1186/1475-2875-12-139
32. Kapisi J, Kakuru A, Jagannathan P, et al. Relationships between infection with Plasmodium falciparum during pregnancy, measures of placental malaria, and adverse birth outcomes. Malaria J. 2017;16:1–11. doi:10.1186/s12936-017-2040-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.