Back to Journals » International Journal of General Medicine » Volume 10
Association between serum concentration of 25-hydroxyvitamin D and community-acquired pneumonia: a case-control study
Authors Mamani M, Muceli N, Ghasemi Basir HR ![]() , Vasheghani M
, Vasheghani M ![]() , Poorolajal J
, Poorolajal J ![]()
Received 13 August 2017
Accepted for publication 5 October 2017
Published 13 November 2017 Volume 2017:10 Pages 423—429
DOI https://doi.org/10.2147/IJGM.S149049
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mojgan Mamani,1,2 Neda Muceli,2 Hamid Reza Ghasemi Basir,3 Maryam Vasheghani,4 Jalal Poorolajal5
1Brucellosis Research Centre, Hamadan University of Medical Sciences, Hamadan, Iran; 2Department of Infectious Disease, Hamadan University of Medical Sciences, Hamadan, Iran; 3Department of Pathology, Hamadan University of Medical Sciences, Hamadan, Iran; 4Chronic Respiratory Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran; 5Research Center for Health Sciences, Department of Epidemiology, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran
Background: Community-acquired pneumonia (CAP) is a common disease with significant morbidity and mortality. There is evidence that vitamin D deficiency can be associated with infectious diseases. The aim of this study was to compare the levels of vitamin D between patients with CAP and healthy controls.
Methods: In a case-control study on 73 patients with CAP and 76 healthy controls, the serum concentration of 25-hydroxyvitamin D (25[OH]D) was measured. Severity and outcomes of disease and also duration of hospital stay were compared in patients with different levels of 25(OH)D. The severity of CAP was assessed using the CURB-65 score (confusion, uremia, respiratory rate, low blood pressure, age ≥65 years) and was also reflected by the length of hospital stay, admission to intensive care unit (ICU), and 30-day mortality.
Results: In total, 81.2% of the study population had vitamin D levels <30 ng/dL. The risk of pneumonia among subjects with deficient vitamin D levels was 3.69 (95% CI: 1.46, 9.31) times of those with sufficient vitamin D level (P=0.006). Prevalence of severe deficiency of vitamin D in scores three and four of CURB-65 (59.38%), was far more than scores one and two (31.71%). Also, results indicated patients with severe deficiency had a higher risk for ICU admission, 30-day mortality, and longer hospitalization stay, but these were not statistically significant.
Conclusion: According to findings, a low level of 25(OH)D is associated with a higher incidence of CAP and more severe disease. It is recommended to pay more attention to vitamin D deficiency in infectious diseases, particularly in CAP patients.
Keywords: vitamin D deficiency, community-acquired infections, pneumonia
Introduction
Pneumonia is the sixth leading cause of death in the United States and the most frequent infectious factor associated with mortality.1 It is one of the most frequent reasons for hospitalization and one of the leading causes of death in elderly populations.2 It is also one of main causes of death in children under 5 years of age in developed countries.3
Pulmonary host defenses involve anatomical and mechanical barriers, humoral immune activity, cell-mediated immune function, and phagocyte activity. Alteration of consciousness, smoking, alcohol consumption, underlying systemic and pulmonary diseases, HIV infection, or old age may lead to impaired lung defense mechanism, and these patients are at risk for pulmonary infection.4
Traditionally, pneumonia is categorized by epidemiologic factors into community-acquired pneumonia (CAP), hospital-acquired pneumonia or nosocomial pneumonia, and ventilator-associated pneumonia. CAP is categorized into typical and atypical pneumonia depending on the type of causative agent. The most common typical pathogens include Streptococcus pneumoniae, Haemophilus influenzae, and Staphylococcus aureus. The major etiologic atypical pathogens of CAP are specific respiratory pathogens, i.e., Chlamydia, Mycoplasma, or Legionella species.5,6
The disease is prevalent among cases aged 50–60 years and usually occurs in winter and early spring. Although the most common clinical features of pneumonia include fever, cough, sputum production, abnormal chest auscultation, and dyspnea in a typical clinical model, elderly patients (especially over 80 years of age) may present with only tachypnea and loss of consciousness. Chest X-ray is a valuable diagnostic method for pneumonia.7,8
Pneumonia is an important disease with significant morbidity and mortality rates, and emotional and financial burden to family, society, and the government, so it is helpful to identify ways aimed at reducing its incidence or severity.
Vitamin A and zinc supplementation is used for the prevention of respiratory infections in developed countries.9,10 Moreover, vitamin C is used despite the little knowledge about its efficacy on respiratory infections.11 Recent research suggested the role of vitamin D in the prevention of pneumonia and increasing the individual’s immunity.12,13
Vitamin D is important for the normal activity of skeletal and nonskeletal tissues, immune cells and immunity, bone calcification, and brain processes.14
Further, vitamin D metabolites play an important role in the body’s immunity by induction of phagocyte migration, modulation of the Th1–Th2-cell balance, and the differentiation of T regulatory cells.15 Some studies showed that vitamin D may be helpful in the treatment of tuberculosis, psoriasis, and multiple sclerosis, as well as for prevention of cancers.14,15
It is shown that vitamin D deficiency (<20 ng/mL) is a prevalent condition and may be a key contributor to both acute and chronic infectious diseases including sepsis, pneumonia, urinary tract infections, and surgical site infections. Most cells, such as B and T lymphocytes, monocytes, and dendritic cells, have specific vitamin D receptors (VDRs). Vitamin D demonstrates its immunomodulatory effects on these cell lines through its effects on the VDR. Deficiency is associated with reduced innate immunity and an increased risk for infections. Vitamin D deficiency can positively affect a wide variety of microbial infections such as Gram-positive and Gram-negative bacteria, fungi, mycobacteria, and viruses.13
Recently, the role of vitamin D has been highlighted in various gene studies. One of the major components of the innate immune system is a diverse combination of cationic antimicrobial peptides that include the α- and β-defensins and cathelicidins. It is shown that vitamin D induced the expression of human cathelicidin antimicrobial peptide (CAMP) gene.15
Given the importance of pneumonia and because vitamin D deficiency is one of the possible factors involved in susceptibility to pneumonia, further studies on the possible role of vitamin D deficiency in the prevalence or severity of the disease can be useful.
High prevalence of vitamin D deficiency is reported among Iranian population in several studies.16–23 Considering the high incidence of pneumonia in Iran, we aimed to investigate the association between serum concentration of 25-hydroxyvitamin D (25[OH]D) and CAP in a case-control study in Hamadan, Iran.
Methods
It is a case-control study designed on adult patients who were diagnosed with CAP and hospitalized in the infectious ward to investigate the association between serum concentration of 25(OH)D and CAP. The data were gathered during patient hospitalization at Sina Hospital, a tertiary referral center in Hamadan. The sex-matched control subjects were recruited from the general population and usually were selected from patient’s companions. A diagnosis of CAP was established by symptoms of pneumonia in combination with physical examination and appropriate radiological changes on the chest X-ray. Also, sputum samples were analyzed to identify the etiologic pathogens.
The inclusion criteria were as follows: patients should be aged over 18 years with a confirmed diagnosis of CAP, pneumonia has not been established 48 hours after hospitalization, the patient has not been admitted to hospital for the last 3 months or do not have to go to the hospital for frequent visits due to chronic diseases, did not reside in nursing homes, were not pregnant, did not take supplemental calcium and vitamin D for the last 3 months, and with no history of malabsorption diseases or medicines that might influence vitamin D absorption and metabolism including chronic liver or renal disease.
Individuals with no history of pneumonia during the past 1 year, no history of calcium and vitamin D consumption 3 months before the study, no current use of inhaled or systemic steroid, and not having chronic liver or renal failure were considered for control group. Samples were collected in each season, and the same number of control samples was also obtained in the same season.
The protocol of this study was approved by the Ethics committee of Hamadan University of Medical Sciences, and written informed consent was obtained from all individuals involved. A blood sample was drawn from participants in the morning, and serum samples were stored at 20°C. Serum 25(OH)D concentration was measured by chemiluminescence immunoassay method, using LIASON autoanalyzer and DiaSorin kit (Stillwater, MN, USA). Vitamin D insufficiency, moderate deficiency, and severe deficiency were, respectively, defined as 25(OH)D levels of 21–29, 10–20, and <10 ng/mL.24
The data collection tools comprised an information form on demographic characteristics, signs and symptoms, physical examination, and the report of radiography. Also, severity of pneumonia was measured by CURB-65 score (confusion, uremia, respiratory rate, low blood pressure, age 65 years or greater).25
According to the results of a case-control study conducted by McNally et al in 2009,26 the prevalence of vitamin D deficiency among cases and non-cases of severe acute lower respiratory infection was reported to be 50% and 20%, respectively. On the basis of these results, we arrived at a sample size of 74 for each group and a total sample size of 148 at 98% significance level and 94% statistical power.26
Statistical analyses were performed using Stata SE 12.1 (StataCorp LP, College Station, TX, USA). Continuous variables were summarized using mean and standard deviation (mean ± SD). For the bivariate analysis, when the variables were parametric, the difference of averages test (Student’s t-test) was used; in the case of variables with more than two categories, the one-way ANOVA test was carried out. Also, chi-square tests were used for categorical variables. Simple and multiple logistic regression analysis was performed to assess the association between vitamin D deficiency and pneumonia. Significance levels were determined using two-tailed tests, and also 95% CIs for relative risks were calculated. P-value of less than 0.05 was considered statistically significant in all tests.
Results
A total of 149 subjects were studied, among them 69.9% were male. Of all the cases investigated, 73 patients with CAP were included in the case group and 76 healthy subjects in the control group.
The mean age in case and control groups was 67.75±10.25 and 71.97±14.27 years, respectively. The two groups were similar with respect to all demographic characteristics, except age (Table 1).
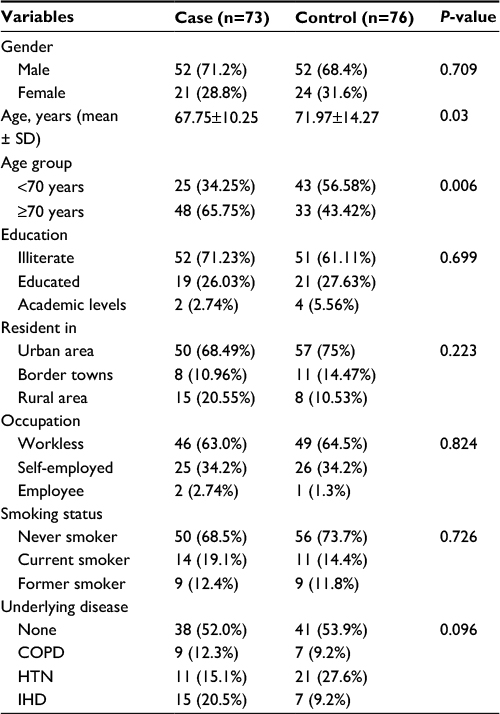 | Table 1 Demographic information and past medical history in case and control groups Abbreviations: HTN, hypertension; IHD, ischemic heart disease. |
Mean serum level of vitamin D was 21.96±24.87 and 19.31±11.15 ng/mL in patients and controls, respectively (P=0.400). Comparison between cases and controls demonstrated that while age group and education level had significant effects on the mean level of 25(OH)D, other demographic factors had no such effect (Table 2).
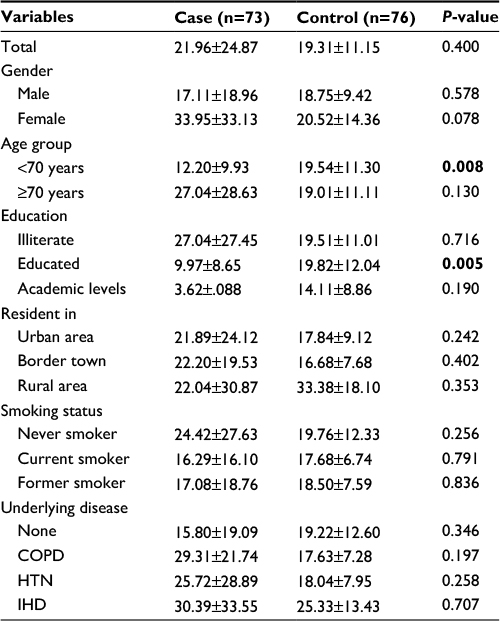 | Table 2 The mean vales of 25(OH)D in two groups based on different variables Note: Bold P-values are significant. Abbreviations: HTN, hypertension; IHD, ischemic heart disease; 25(OH)D, 25-hydroxyvitamin D. |
The association between vitamin D levels and CAP is given in Table 3, considering the sufficiency, insufficiency, and deficiency as 25(OH)D levels of >20, 10–20, and <10 ng/mL, respectively. Although there was no significant difference between the two groups for the mean of 25(OH)D, cases had a significant higher rate of deficiency than controls. According to these results, after controlling for age, the risk of CAP among individuals with insufficient vitamin D level was almost a half of individuals with sufficient levels. However, the risk of pneumonia among subjects with deficient vitamin D levels was 3.69 (95% CI: 1.46, 9.31) times of those with sufficient vitamin D levels (Table 3).
 | Table 3 The association between vitamin D levels and community-acquired pneumonia Note: aAdjusted for age and smoking. |
Also, regarding the odds ratio (OR) index, the relative chance (OR) of severe vitamin D deficiency in the case group was 4.16 (95% CI: 1.82, 9.85) times that of the control group.
The severity of CAP was assessed using the CURB-65 score and was also reflected by the length of hospital stay, admission to intensive care unit (ICU), and 30-day mortality rate. Although, when entering all of the vitamin D levels, there was no difference between the low- and high-risk patients identified based on CURB-65 (P=0.120); however, a significant impact of severe vitamin D deficiency on CURB-65 score was found with an OR of 3.15 (59.38% vs 31.71%, OR =3.15, 95% CI: 1.20, 8.25; P=0.018). The level of 25(OH)D was not significantly associated with ICU admission and death (Table 4). The mean length of hospital stay was 11.03±7.48 days in patients with severe deficiency compared with 9.47±6.06 days in patients with sufficient levels of 25(OH)D.
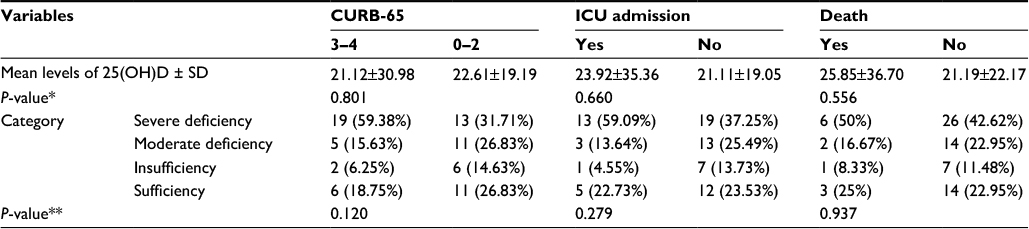 | Table 4 Comparison of the mean values as well as the categorized levels of 25(OH)D based on CURB-65 score, ICU admission, and 30-day mortality in CAP patients Notes: *t-test; **chi-square test. Abbreviations: 25(OH)D, 25-hydroxyvitamin D; CURB-65, confusion, uremia, respiratory rate, low blood pressure, age 65 years or greater; ICU, intensive care unit; CAP, community-acquired pneumonia. |
Discussion
The purpose of this case-control study was to investigate the relationship between vitamin D levels and severity of CAP in a total of 149 subjects (73 cases and 76 controls). The overall prevalence of vitamin D deficiency in the case group was not greater than in the control group; however, patients with CAP had a higher rate of severe vitamin D deficiency in comparison with healthy participants. Furthermore, CAP patients with severe vitamin D deficiency had more severe disease (higher CURB-65 score). Although not statistically significant, patients with severe deficiency had a higher rate of ICU admission and a longer duration of hospital stay.
The results of our study showed that there was a significant association between severe vitamin D deficiency and CAP. Individuals with severe deficiency were 4.16 times more susceptible in acquiring CAP when compared to the people with higher levels of vitamin D. Our result is consistent with the recent studies conducted in other countries,27–30 although this relationship was observed for different levels of vitamin D in other studies. Kim et al in a study on hospitalized patients with CAP in South Korea found that vitamin D deficiency, which was defined as 25(OH)D less than 20 ng/mL, was observed in about 80% of patients.27 In a hospital-based case-control study by Wayse et al on 150 Indian children under 5 years of age, one of factors associated with significantly higher OR for having severe acute lower respiratory infection was serum 25(OH)D less than 10 ng/mL (OR =11).30 Aregbesola et al investigated the effect of 25(OH)D on the risk of incident hospitalized pneumonia in an aging general population in eastern Finland. They found that the subjects with the lowest level of serum 25(OH)D had a significant 2.6-fold (95% CI: 1.4, 5.0) higher risk of developing pneumonia compared to the subjects with the highest levels.29 They concluded that there was an inverse effect of serum 25(OH)D concentration on the risk of incident pneumonia in the aging population. Quraishi et al reported the result of the third National Health and Nutrition Examination Survey in a large nationally representative cohort of noninstitutionalized adults in the United States. They showed that after adjusting for demographic factors, clinical data, and season, 25(OH)D levels less than 30 ng/mL were associated with 56% higher risk for CAP.28 Holter et al investigated the vitamin D status and long-term mortality in CAP. They showed that high prevalence of vitamin D deficiency and inadequacy among hospitalized adults with CAP and patients with vitamin D deficiency at hospital admission resulted in a 91% increase in risk of death during long-term follow-up after discharge, but no significant difference in survival was observed in patients with vitamin D inadequacy, compared to patients with vitamin D sufficiency.31
Our results demonstrated that the severity of CAP using the CURB-65 score was associated with severe vitamin D deficiency, and the OR of patients with severe deficiency for severe disease based on CURB-65 score was 3.15. Similarly, Pletz et al in a study on randomly selected patients with CAP in Germany found that there was a significant inverse correlation between serum 25(OH)D concentration and CURB-65 score.32 Although we found no significant association between vitamin D levels and both ICU admission and mortality in CAP, some studies indicated a significant relationship; for instance, Remmelts et al in a prospective cohort study on hospitalized patients with CAP stated that vitamin D deficiency was associated with an increased risk of ICU admission and 30-day mortality.33 Also, they showed that 25(OH)D status was an independent predictor of 30-day mortality and concluded that there was a relationship between deficiency and adverse outcome in CAP. An another study by Leow et al in a prospective cohort of 112 patients admitted with CAP during winter in New Zealand found that 25(OH)D deficiency is associated with increased mortality in their patients.34 Similar results were obtained in studies by McNally et al and Wayse et al.26,30
The results of our study indicated that low levels of 25(OH)D may lead to longer hospitalization, and there was a negative correlation between serum concentration of 25(OH)D and the length of hospital stay. Thus, patients with severe deficiency were hospitalized, on average, for 11.03 days, in comparison with 9.47 days in patients with sufficient levels of vitamin D. However, Choudhary and Gupta evaluated the role of oral vitamin D supplementation (1000–2000 IU per day for 5 days) for resolution of severe pneumonia in a randomized controlled trial on 200 children under 5 years of age.35 They found that median duration for the resolution of severe pneumonia was similar in both the groups (vitamin D supplementation vs placebo). Also, the two groups did not differ in duration of hospitalization and time to resolution of tachypnea, chest retractions, and inability to feed. They stated that short-term supplementation with oral vitamin D has no beneficial effect on resolution of severe pneumonia in under-five children.35 The fact that the short-term supplement of vitamin D cannot produce results in patients with CAP can be due to the long-term effects of vitamin D on the maturation and development of lymphocytes and other mononuclear cells in the immune system.
Limitations
In this study, sexes were matched for cases and controls, but this was not feasible for age. Also, we did not take into account the etiologies (bacterial or viral or both) of pneumonia to compare the impact of vitamin D deficiency. As some of our study participants probably ignored or forgot their supplementations and this might have influenced the results. In addition, the lack of documented information about treatment history and also administration of over-the-counter medications are the main drawbacks in all studies conducted in Iran. Furthermore, some outlier values were not excluded that resulted in high SD values, although we calculated the confidence intervals for these data.
Conclusion
Based on our study, patients with vitamin D deficiency may develop more severe CAP, as well as longer hospital stay, higher rates of ICU admission, and 30-day mortality compared to patients with vitamin D sufficiency. It is suggested that more attention be paid to vitamin D deficiency in infectious diseases, particularly in CAP. Further studies with larger sample sizes are needed to confirm the allegation of higher incidence of CAP in vitamin D-deficient individuals.
Acknowledgments
This paper was extracted from a PhD thesis by Neda Muceli. Acknowledgment is given to Razi Pathobiology Laboratory for performing 25(OH)D tests.
Disclosure
The authors report no conflicts of interest in this work.
References
Vilar J, Domingo ML, Soto C, Cogollos J. Radiology of bacterial pneumonia. Eur J Radiol. 2004;51(2):102–113. | ||
Kardas P, Ratajczyk-Pakalska E. Reasons for elderly patient hospitalization in departments of internal medicine in Lodz. Aging Clin Exp Res. 2003 ;15(1):25–31. | ||
Wallihan R, Ramilo O. Community-acquired pneumonia in children: current challenges and future directions. J Infect. 2014; 69(Suppl 1):S87–S90. | ||
Quinton LJ, Mizgerd JP. Dynamics of lung defense in pneumonia: resistance, resilience, and remodeling. Annu Rev Physiol. 2015;77:407–430. | ||
Avni T, Shiver-Ofer S, Leibovici L, et al. Participation of elderly adults in randomized controlled trials addressing antibiotic treatment of pneumonia. J Am Geriatr Soc. 2015;63(2):233–243. | ||
Cunha BA. The atypical pneumonias: clinical diagnosis and importance. Clin Microbiol Infect. 2006;12(Suppl 3):12–24. | ||
Chong CP, Street PR. Pneumonia in the elderly: a review of the epidemiology, pathogenesis, microbiology, and clinical features. South Med J. 2008;101(11):1141–1145; quiz 32, 79. | ||
Fung HB, Monteagudo-Chu MO. Community-acquired pneumonia in the elderly. Am J Geriatr Pharmacother. 2010;8(1):47–62. | ||
Barnett JB, Hamer DH, Meydani SN. Zinc: a new risk factor for pneumonia in the elderly? Nutr Rev. 2010;68(1):30–37. | ||
Fawzi WW, Mbise RL, Fataki MR, et al. Vitamin A supplementation and severity of pneumonia in children admitted to the hospital in Dar es Salaam, Tanzania. Am J Clin Nutr. 1998;68(1):187–192. | ||
Hemilä H, Louhiala P. Vitamin C may affect lung infections. J R Soc Med. 2007;100(11):495–498. | ||
Watkins RR, Lemonovich TL, Salata RA. An update on the association of vitamin D deficiency with common infectious diseases. Can J Physiol Pharmacol. 2015;93(5):363–368. | ||
Youssef DA, Ranasinghe T, Grant WB, Peiris AN. Vitamin D’s potential to reduce the risk of hospital-acquired infections. Dermatoendocrinol. 2012;4(2):167–175. | ||
Holick MF. Vitamin D deficiency. N Engl J Med. 200719;357(3):266–281. | ||
Gombart AF, Borregaard N, Koeffler HP. Human cathelicidin antimicrobial peptide (CAMP) gene is a direct target of the vitamin D receptor and is strongly up-regulated in myeloid cells by 1,25-dihydroxyvitamin D3. FASEB J. 2005;19(9):1067–1077. | ||
Alipour S, Saberi A, Seifollahi A, Shirzad N, Hosseini L. Risk factors and prevalence of vitamin d deficiency among Iranian women attending two university hospitals. Iran Red Crescent Med J. 2014;16(10):e15461. | ||
Faghih S, Abdolahzadeh M, Mohammadi M, Hasanzadeh J. Prevalence of vitamin d deficiency and its related factors among university students in shiraz, iran. Int J Prev Med. 2014;5(6):796–799. | ||
Ebrahimi M, Khashayar P, Keshtkar A, et al. Prevalence of vitamin D deficiency among Iranian adolescents. J Pediatr Endocrinol Metab. 2014;27(7–8):595–602. | ||
Habibesadat S, Ali K, Shabnam JM, Arash A. Prevalence of vitamin D deficiency and its related factors in children and adolescents living in North Khorasan, Iran. J Pediatr Endocrinol Metab. 2014;27(5–6):431–436. | ||
Hovsepian S, Amini M, Aminorroaya A, Amini P, Iraj B. Prevalence of vitamin D deficiency among adult population of Isfahan City, Iran. J Health Popul Nutr. 2011;29(2):149–155. | ||
Neyestani TR, Hajifaraji M, Omidvar N, et al. High prevalence of vitamin D deficiency in school-age children in Tehran, 2008: a red alert. Public Health Nutr. 2012;15(2):324–330. | ||
Kaykhaei MA, Hashemi M, Narouie B, et al. High prevalence of vitamin D deficiency in Zahedan, southeast Iran. Ann Nutr Metab. 2011;58(1):37–41. | ||
Moussavi M, Heidarpour R, Aminorroaya A, Pournaghshband Z, Amini M. Prevalence of vitamin D deficiency in Isfahani high school students in 2004. Horm Res. 2005;64(3):144–148. | ||
Hossein-nezhad A, Holick MF. Optimize dietary intake of vitamin D: an epigenetic perspective. Curr Opin Clin Nutr Metab Care. 2012; 15(6):567–579. | ||
Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax. 2003;58(5):377–382. | ||
McNally JD, Leis K, Matheson LA, Karuananyake C, Sankaran K, Rosenberg AM. Vitamin D deficiency in young children with severe acute lower respiratory infection. Pediatr Pulmonol. 2009;44(10):981–988. | ||
Kim HJ, Jang JG, Hong KS, Park JK, Choi EY. Relationship between serum vitamin D concentrations and clinical outcome of community-acquired pneumonia. Int J Tuberc Lung Dis. 2015;19(6):729–734. | ||
Quraishi SA, Bittner EA, Christopher KB, Camargo CA, Jr. Vitamin D status and community-acquired pneumonia: results from the third National Health and Nutrition Examination Survey. PloS One. 2013;8(11):e81120. | ||
Aregbesola A, Voutilainen S, Nurmi T, Virtanen JK, Ronkainen K, Tuomainen TP. Serum 25-hydroxyvitamin D3 and the risk of pneumonia in an ageing general population. J Epidemiol Community Health. 2013;67(6):533–536. | ||
Wayse V, Yousafzai A, Mogale K, Filteau S. Association of subclinical vitamin D deficiency with severe acute lower respiratory infection in Indian children under 5 y. Eur J Clin Nutr. 2004;58(4):563–567. | ||
Holter JC, Ueland T, Norseth J, et al. Vitamin D status and long-term mortality in community-acquired pneumonia: secondary data analysis from a prospective cohort. PLoS One. 2016;11(7):e015856. | ||
Pletz MW, Terkamp C, Schumacher U, et al. Vitamin D deficiency in community-acquired pneumonia: low levels of 1,25(OH)2 D are associated with disease severity. Respir Res. 2014;15:53. | ||
Remmelts HH, van de Garde EM, Meijvis SC, et al. Addition of vitamin D status to prognostic scores improves the prediction of outcome in community-acquired pneumonia. Clin Infect Dis. 2012;55(11):1488–1494. | ||
Leow L, Simpson T, Cursons R, Karalus N, Hancox RJ. Vitamin D, innate immunity and outcomes in community acquired pneumonia. Respirology. 2011;16(4):611–616. | ||
Choudhary N, Gupta P. Vitamin D supplementation for severe pneumonia – a randomized controlled trial. Indian Pediat. 2012;49(6):449–454. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.