Back to Journals » Vascular Health and Risk Management » Volume 21
Association Between Revascularization and 30-Day Survival of Ischemic Cardiomyopathy Patients in Dr. Hasan Sadikin General Hospital
Authors Raharjo PP ![]() , Suhendro AS, Yahya AF
, Suhendro AS, Yahya AF ![]() , Dewi TI
, Dewi TI
Received 25 February 2025
Accepted for publication 21 August 2025
Published 3 September 2025 Volume 2025:21 Pages 719—728
DOI https://doi.org/10.2147/VHRM.S524863
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Mirna N Chahine
Pradana Pratomo Raharjo, Adrian Sebastian Suhendro, Achmad Fauzi Yahya, Triwedya Indra Dewi
Department of Cardiology and Vascular Medicine, Universitas Padjadjaran/Dr. Hasan Sadikin General Hospital, Bandung, Indonesia
Correspondence: Pradana Pratomo Raharjo, Department of Cardiology and Vascular Medicine, Universitas Padjadjaran, Hasan Sadikin General Hospital, Bandung, Indonesia, Tel +62 81299200032, Email [email protected]
Introduction: Ischemic cardiomyopathy is the leading cause of heart failure and associated with increased morbidity and mortality. The role of percutaneous coronary intervention (PCI) in term of increasing survival and cardiovascular outcomes in ischemic cardiomyopathy remains unclear.
Purpose: To evaluate whether revascularization is associated with 30-day survival in ischemic cardiomyopathy in Dr. Hasan Sadikin General Hospital.
Patients and Methods: This was a single center, observational, retrospective cohort study. Subject data was taken from the CABG and PCI database of Cardiology and Vascular Medicine Department, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital from January 2021 to December 2022. Study outcome was 30-day survival after revascularization procedure. Survival analysis was done using Kaplan–Meier analysis then bivariate analysis with log rank test and cox regression analysis. Cox regression analysis was also done for multivariate analysis of confounding factors.
Results: A total of 67 ischemic cardiomyopathy patients were included in the final analysis of this study with balance proportion except for age, complete revascularization, and chronic total occlusion (CTO) variables. CABG group tends to be younger with more proportion in age ≤ 65 years old compared with PCI group (92.6% vs. 65%. p = 0.01). Complete revascularization had reached dominantly in the CABG group compared with PCI group (85.2% vs. 15%. p < 0.001). In coronary anatomy characteristic, CTO was found more in the CABG group (81.5% vs. 52.5%. p = 0.02). In 30-day follow up, overall survival rate was 91% with 81.5% in the CABG group compared with 97.5% in the PCI group (p = 0.03). Multivariate analysis was done to exclude confounding factors with adjusted hazard ratio of revascularization was 4.02 (CI95% 0.27– 60.3. p = 0.31).
Conclusion: There is no association between revascularization and 30-day survival in ischemic cardiomyopathy in Dr. Hasan Sadikin General Hospital. However, wide confidence intervals highlight uncertainty.
Keywords: coronary artery bypass grafting, ischemic cardiomyopathy, percutaneous coronary intervention, revascularization, survival, PCI
Introduction
Ischemic cardiomyopathy is a leading cause of heart failure with LVEF ≤ 40% and associated with increased morbidity and mortality.1 Those with history of myocardial infarction (MI) and left ventricular ejection fraction (LVEF) ≤35% had two times risk of heart failure hospitalization and four times risk of death.2 Along with optimal medial therapy (OMT), revascularization is a treatment choice to increase survival in ischemic cardiomyopathy.3 Successful revascularization will lead to improvement of left ventricular function and prognosis in heart failure patient due to reduction of ischemia burden in viable but hibernating myocardium.4 Revascularization can be achieved by coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI).5
Although revascularization is beneficial in improving prognosis and symptoms control, study comparing treatment choice in ischemic cardiomyopathy population is limited.3,6 STICH and STICHES trial which compare CABG along with OMT showed benefit in the CABG arm in terms of reducing all causes of mortality, cardiovascular mortality, or hospitalization due to cardiovascular causes.7,8 However, the utilization of CABG is limited, especially in high-risk patient such those with advanced age and comorbidities, PCI is thought to be alternative in this subset of patient.9,10 The role of PCI in improving survival and cardiovascular outcomes in this population is not clearly known.11 Recently, a randomized controlled trial (RCT) comparing PCI and OMT in ischemic cardiomyopathy named REVIVED study showed that there is no significant difference in outcomes.12
Prunea et al emphasized that although both CABG and PCI have their roles, decision-making must consider myocardial viability, anatomical complexity, and procedural risk. This review noted the scarcity of data in low- and middle-income countries, supporting the relevance of local studies to guide regional clinical decisions.13 Buszman et al reported that while CABG offered superior improvements in ventricular function compared to PCI, it was also associated with higher perioperative risk, particularly in patients with severely reduced LVEF.14 Liga et al stressed the importance of tailoring revascularization approaches, including the completeness of revascularization, to individual patient characteristics. They also highlighted a gap in short-term outcome data, such as 30-day survival, especially in high-risk groups.15 These publications demonstrate the complexity and individualized nature of revascularization decisions in ischemic cardiomyopathy, while also exposing gaps in short-term outcome data, particularly within Southeast Asian populations.
To this date, there is no RCT comparing short- and long-term outcomes of CABG and PCI in ischemic cardiomyopathy population with observational studies showed different results.16–22 There is no data regarding such outcomes in Indonesian population especially in our center. Therefore, this study aims to assess association between revascularization and 30-day survival of ischemic cardiomyopathy patients in Dr. Hasan Sadikin General Hospital.
Materials and Methods
Study Design and Patient Selection
This study is a single-center, observational, retrospective cohort study conducted in Dr. Hasan Sadikin General Hospital from January 2021 until December 2022. Subjects of this study were ischemic cardiomyopathy patients who had been registered in the PCI and CABG database of Cardiology and Vascular Medicine Department, Faculty of Medicine Universitas Padjadjaran/ Dr. Hasan Sadikin General Hospital that fulfill inclusion and exclusion criteria. This study waived individual informed consent because data were analyzed anonymously. Study procedures complied with the Declaration of Helsinki, and patient confidentiality was maintained throughout.
Inclusion criteria in this study are age more than 18 years old, fulfill diagnostic criteria of ischemic cardiomyopathy defined as LVEF ≤40%, history of symptomatic heart failure at least NYHA functional class II, and one of three criteria: (1) history of MI or revascularization by CABG or PCI; (2) ≥75% stenosis of left main or proximal LAD; and (3) ≥ 75% stenosis of two or more epicardial vessels. In addition, patients were required to have a moderate or severe anatomical SYNTAX score with anatomical SYNTAX score > 22, and to have undergone revascularization (PCI or CABG) electively at study period with available data regarding 30-day survival after intervention. Patients with acute coronary syndrome, LV aneurysm, significant valve dysfunction, mechanical complication, congenital heart disease, and history of device implantation such as ICD or CRT were excluded in this study. The minimum required sample size was calculated using the formula for two independent proportions. Based on prior studies, the proportion of the primary outcome in the intervention group was 0.99, with an assumed proportion of 0.79 in the control group. A significance level (α) of 5% and a power (1–β) of 80% were applied, with an expected minimum difference of 20%. The resulting calculation indicated that a minimum of 23 subjects was required per group. A total sampling method was applied consecutively using secondary data from the PCI and cardiac surgery registry at Dr. Hasan Sadikin General Hospital between January 2021 and December 2022.12,23,24
Data Collection
Subject was carried out consecutively from PCI and CABG database of Cardiology and Vascular Medicine Department, Faculty of Medicine Universitas Padjadjaran/ Dr. Hasan Sadikin General Hospital with total sampling method. Data collected consisted of baseline characteristic such as age, sex, body mass index (BMI), traditional coronary artery disease (CAD) risk factors (hypertension, type 2 diabetes mellitus, dyslipidemia, smoking, family history), history of MI, CKD, LVEF, IABP usage, complete revascularization, and medication status for both groups. Intervention selection including stent strategy using Drug-Eluting Stent (DES) or no stent strategy and intracoronary imaging were included in the PCI arm and CABG methods (on-pump or off-pump) was included in the CABG arm. Complete revascularization refers to the revascularization of all major epicardial coronary arteries with functionally or anatomically significant stenosis—defined as ≥ 50% luminal narrowing in the LAD, LCx, or RCA, or lesions identified as ischemia-producing through invasive or non-invasive functional testing. In contrast, incomplete revascularization denotes a strategy in which not all significant coronary territories are revascularized according to these criteria. The reasons for incomplete revascularization may include patient-related comorbidities, anatomical complexities, and technical or procedural considerations that limit the feasibility of achieving complete revascularization.25 The data regarding number of vessels involved, left main CAD, chronic total occlusion (CTO), bifurcation lesion, trifurcation lesion, and anatomical SYNTAX score were included in coronary artery characteristic. To address missing data, a complete-case analysis was applied, resulting in the exclusion of patients lacking complete 30-day follow-up (n = 9).
Statistical Analysis
Baseline characteristic and coronary artery characteristic were all presented in categorical variable. Intergroup difference was analyzed with descriptive analysis using chi square test (if expected count less than 5) or fisher exact test. Variable with intergroup difference was thought as a confounder and will be included in bivariate and multivariate analysis. Survival analysis was done using Kaplan–Meier analysis. Intergroup difference was calculated using log rank test if proportional hazard assumption is fulfilled. Bivariate and multivariate analysis were done using cox regression test if proportional hazard assumption is fulfilled. Significance level in this study cut-off was less than equal 0.05 (p < 0.05). Statistical analysis was done using IBM SPSS 27.0 for Windows software.
Results
From 114 ischemic cardiomyopathy patients undergone revascularization with CABG or PCI in period of January 2021 to December 2022, a total of 46 patients were excluded in this study. Seven patients were excluded due to repeated data. Thirty patients with low anatomical SYNTAX score (less than 23) were also excluded. Nine patients without 30-day follow-up were also excluded. A total of 67 patients were included in final analysis with 27 patients in the CABG arm and 40 patients in the PCI arm. Study flow was described in Figure 1.
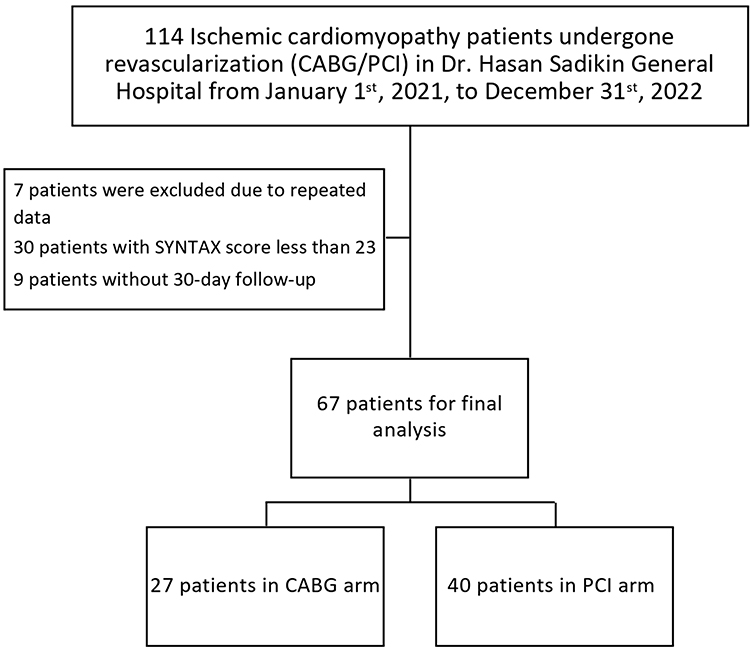 |
Figure 1 Study Flow. |
Baseline characteristic in this study was described in Table 1. A majority of male patients (81.5% in the CABG arm and 82.5% in the PCI arm) was included in this study with smoker as a major traditional CAD risk factor (81.5% in the CABG arm and 72.5% in the PCI arm). History of MI was found in 70.4% patient from the CABG group and 57.5% patient from PCI group with no intergroup difference. Most of patients had LVEF ≤ 35% (55.6% in the CABG arm and 65% in the PCI arm). IABP was used only in minority (25.9% in the CABG arm and 10% in the PCI arm). Almost all intervention in the PCI arm was done using DES (97.5%) with only one patient using Drug-Coated Ballon (DCB) (2.5%). Intracoronary imaging utilization is high in this study proven with 62.5% patients undergoing PCI were supported by using intravascular ultrasound (IVUS) or optical coherence tomography (OCT). On-pump CABG was method of choice in majority ischemic cardiomyopathy who undergone CABG with a total of 85.2%. Age and complete revascularization had a significant intergroup difference and included as a confounder. Patients in CABG group were younger compared with PCI group with more proportion of ≤ 65 years old (92.6% vs. 65%. p = 0.01). Complete revascularization was observed mostly in CABG group compared with PCI group (85.2% vs. 15%. p < 0.001). Only minority patient is optimally treated in both group (18.5% vs. 20%. p = 0.98)
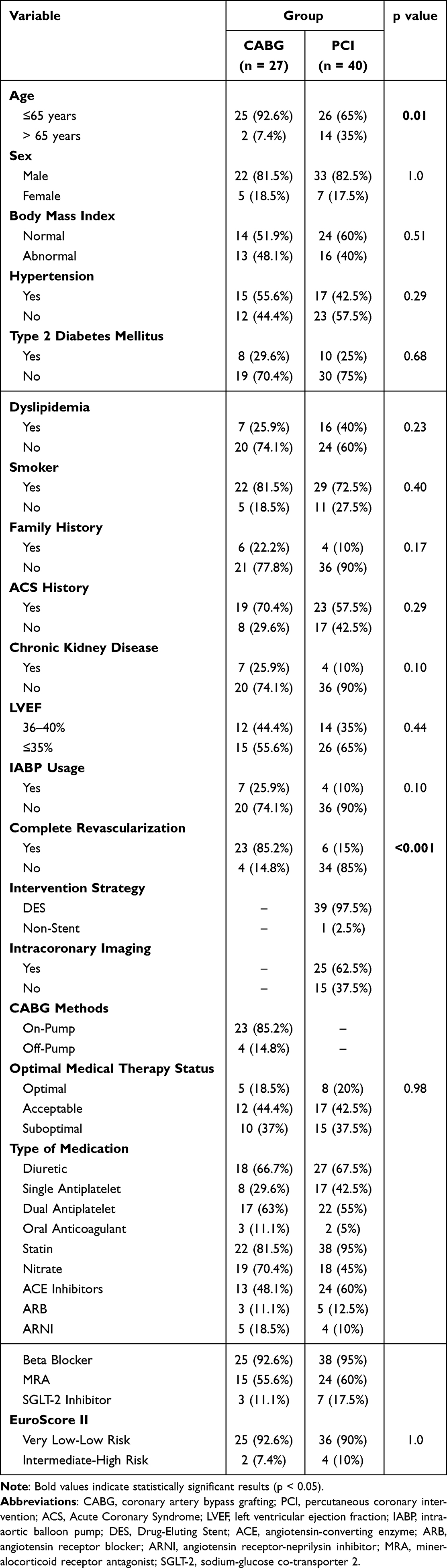 |
Table 1 Baseline Characteristic |
Coronary artery characteristic was described in Table 2. In term of vessel involved in this study, almost all included were three vessel disease CAD (85.2% in the CABG group and 82.5% in the PCI group). CTO had a significant difference in proportion with more CTO was found in the CABG group compared with PCI group (81.5% vs. 52.5%. p = 0.02).
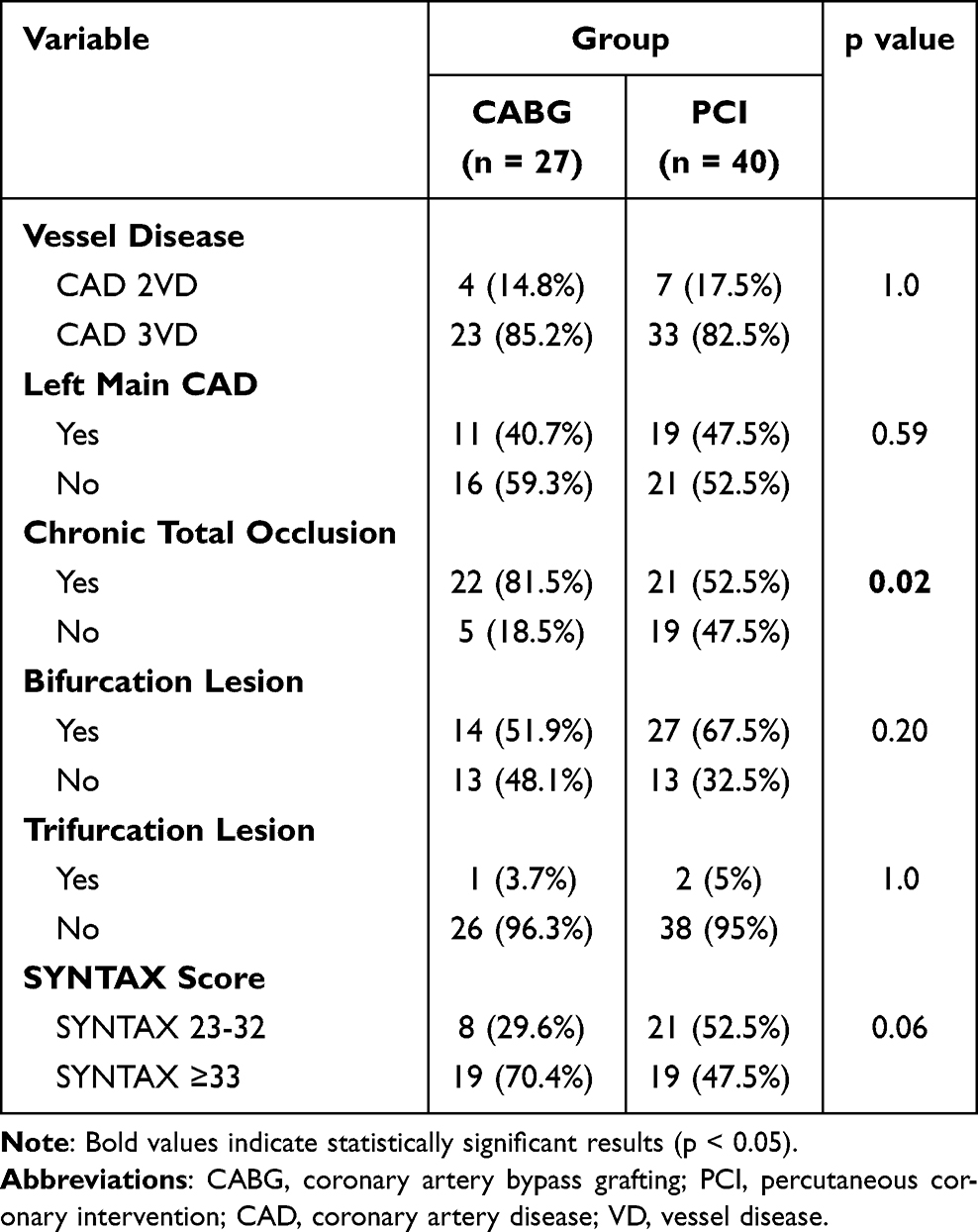 |
Table 2 Coronary Anatomy Characteristic |
Survival analysis was done to evaluate time to event with time of revascularization (CABG or PCI) as the starting point. Kaplan–Meier analysis was done to evaluate proportional hazard assumption (as shown in Figure 2). Event was found in 5/27 (81.5%) patients in the CABG arm and 1/40 (97.5%) patients in the PCI arm at 30-day follow up. In the PCI arm, event was observed in one patient due to cardiogenic shock at time of revascularization. In the CABG arm, an event was observed in 5 patients in day 0, 1, 2 and 5 after revascularization. One patient was death in day 0 due to hemorrhagic shock, one patient was death in day 1 due to cardiogenic shock, two patient was death in day 2 due to cardiogenic shock, other due to acute circulatory collapse, and last patient was death in day 5 due to septic shock due to ventilator associated pneumonia. All events were in-hospital events, and no event was observed out-of-hospital.
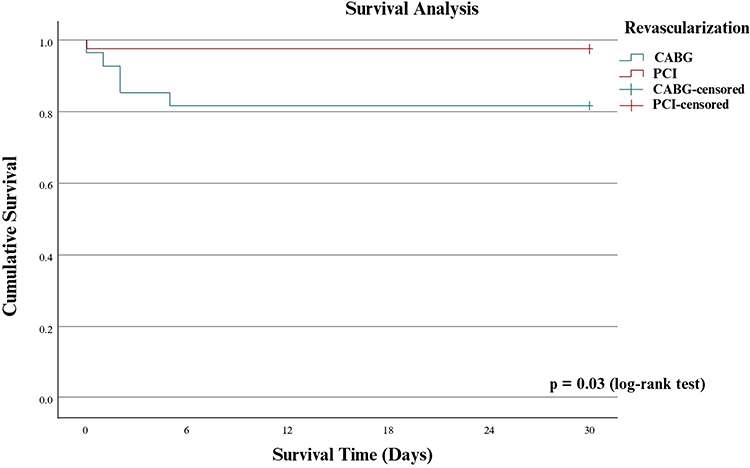 |
Figure 2 Survival Analysis in 30 Days According Intervention Group. |
Log rank test was done to evaluate association between revascularization and 30-day survival with significant result (p = 0.03). Bivariate and multivariate analysis to exclude confounders was done using cox regression analysis if the criteria of proportional hazard assumption was fulfilled. The result of bivariate and multivariate analysis was shown in Table 3. After controlling confounding, revascularization is not associated with 30-day survival in ischemic cardiomyopathy (adjusted HR 4.02; CI95% 0.27–60.3. p = 0.31). However, wide confidence intervals highlight uncertainty. Larger prospective studies are required to clarify the impact of revascularization strategy and completeness in Indonesian patients with ischemic cardiomyopathy.
 |
Table 3 Bivariate and Multivariable Analysis for Association Between Revascularization and 30-Day Survival |
Discussion
This is the first study conducted to assess association between revascularization and 30-day survival of ischemic cardiomyopathy in Dr. Hasan Sadikin General Hospital. The main finding of this study showed that revascularization is not associated with 30-day survival in ischemic cardiomyopathy (LVEF ≤ 40%). From a total of 67 patients enrolled in this study, PCI had better survival rate compared with CABG (97.5% vs. 81.5%) but statistically insignificant with adjusted Hazard Ratio (HR) of 4.02 (CI95% 0.27–60.3. p = 0.31). This finding was in line with previous study from Zhang et al, Pei et al, Khan et al and Sun et al that showed no significant difference of short-term mortality between CABG and PCI in ischemic cardiomyopathy population.17,19,21,26
Non-significant association between revascularization and 30-day survival in this study might be due to low mortality rate after 30-day follow up. In the PCI arm, event was observed in one patient due to cardiogenic shock at time of revascularization. Prunea et al emphasized the nuanced indications for CABG and PCI based on myocardial viability, surgical risk, and anatomical complexity. Our findings complement this, suggesting no short-term survival benefit of CABG over PCI in high-risk patients.13
Lower 30-day survival rate in the CABG group was in line with previous study from STICH trial that showed that CABG was associated with increased risk of all-cause mortality until 2 years after revascularization due to surgical intervention in patients with LV dysfunction.8 Study from Khalili et al showed that CABG in ischemic cardiomyopathy with LVEF < 35% had high perioperative mortality rate with reduced survival.27 Buszman et al showed better left ventricular function improvement with CABG but also higher perioperative risk, consistent with our observed CABG group mortality (18.5%).14 Heart failure, MI, and stroke are the most common cause of mortality in first 30-day after CABG. Bleeding (10%) and pulmonary embolism (4%) are less common causes of mortality in first 30-day.28 Sepsis after CABG had lower incidence but related with increased intensive care length of stay and 30-day mortality.29 Thirty day mortality was also influenced by hospital surgical volume with cut-off of 415 cases per year.30 However, 30-day mortality reflects only early mortality after CABG and observation should be prolonged to observe long-term mortality.31
Higher 30-day survival rate in the PCI group justify PCI as alternative choice of revascularization in ischemic cardiomyopathy with lower mortality and morbidity, especially in high-risk CABG candidate.9 Another study from Sheiban et al showed that from 77 ischemic cardiomyopathy patients, event was observed in 1 patient (1.3%).32 This might be due to improvement of contemporary PCI with advanced team, usage of potent antiplatelet, better stent technology, intracoronary imaging, usage of invasive functional test and mechanical circulatory support.9 Liga et al advocated tailored strategies in ischemic cardiomyopathy, particularly stressing the role of complete revascularization, which in our study did not reach independent significance in 30-day survival.15
The study has several limitations. The relatively small sample size and low number of mortality events reduce the statistical power and increase the uncertainty of the estimates, as reflected by the wide confidence intervals. This study is an observational retrospective cohort study with no randomization for each group without clear selection criteria in selecting revascularization method in ischemic cardiomyopathy patient. This study is a single-center study with uniform ethnic and race. Intervention was done by specialized interventionist and cardiothoracic surgeon with different skill that operator-dependent so this study result cannot be reproducible to other population. This study is a short-term follow up in term of survival outcome. Study result cannot be extrapolated to long-term outcome so that long-term follow up study is required to evaluate overall outcome in this subset of patient. Ischemia and viability data were not analyzed in this study. Role of myocardial viability in myocardial improvement after revascularization is unclear.33–35
Conclusion
There is no association between revascularization and 30-day survival in ischemic cardiomyopathy in RSUP Dr. Hasan Sadikin. However, the wide confidence interval and small number of events suggest statistical uncertainty, highlighting the need for larger studies to confirm these findings.
Data Sharing Statement
Available on reasonable request.
Ethical Approval
This research has received ethical approval from the Research Ethics Comittee of Dr. Hasan Sadikin General Hospital, Bandung, with ethical approval number LB.02.01/X.6.5/116/2023. Study procedures complied with the Declaration of Helsinki, and patient confidentiality was maintained throughout.
Acknowledgments
There are no acknowledgements in this review.
Funding
There is no funding in this review.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Velagaleti RS, Vasan RS. Heart failure in the 21st century: is it a coronary artery disease problem or hypertension problem? Cardiol Clin. 2007;25(4):487. doi:10.1016/j.ccl.2007.08.010
2. Elgendy IY, Mahtta D, Pepine CJ. Medical therapy for heart failure caused by ischemic heart disease. Circ Res. 2019;124(11):1520–1535. doi:10.1161/CIRCRESAHA.118.313568
3. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87–165. doi:10.1093/eurheartj/ehy394
4. Neumann FJ, Sechtem U, Banning AP, et al. 2019 ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 2020;41(3):407–477. doi:10.1093/eurheartj/ehz425
5. Gaudino MFL, Spadaccio C, Taggart DP. State-of-the-art coronary artery bypass grafting: patient selection, graft selection, and optimizing outcomes. Interv Cardiol Clin. 2019;8(2):173–198. doi:10.1016/j.iccl.2018.11.007
6. Wolff G, Dimitroulis D, Andreotti F, et al. Survival benefits of invasive versus conservative strategies in heart failure in patients with reduced ejection fraction and coronary artery disease: a meta-analysis. Circ Heart Fail. 2017;10(1). doi:10.1161/CIRCHEARTFAILURE.116.003255
7. Velazquez EJ, Lee KL, Jones RH, et al. Coronary-artery bypass surgery in patients with ischemic cardiomyopathy. N Engl J Med. 2016;374(16):1511–1520. doi:10.1056/NEJMoa1602001
8. Velazquez EJ, Lee KL, Deja MA, et al. Coronary-artery bypass surgery in patients with left ventricular dysfunction. N Engl J Med. 2011;364(17):1607–1616. doi:10.1056/NEJMoa1100356
9. Ahmad Y, Petrie MC, Jolicoeur EM, et al. PCI in patients with heart failure: current evidence, impact of complete revascularization, and contemporary techniques to improve outcomes. J Soc Cardiovasc Angiography Interventions. 2022;1(2):100020. doi:10.1016/j.jscai.2022.100020
10. Doshi D, Ben-Yehuda O, Bonafede M, et al. Underutilization of coronary artery disease testing among patients hospitalized with new-onset heart failure. J Am Coll Cardiol. 2016;68(5):450–458. doi:10.1016/j.jacc.2016.05.060
11. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American college of cardiology/American heart association joint committee on clinical practice guidelines. J Am Coll Cardiol. 2022;79(2):e21–129. doi:10.1016/j.jacc.2021.09.006
12. Perera D, Clayton T, O’Kane PD, et al. Percutaneous revascularization for ischemic left ventricular dysfunction. N Engl J Med. 2022;387(15):1351–1360. doi:10.1056/NEJMoa2206606
13. Prunea DM, Homorodean C, Olinic M, Achim A, Olinic DM. Optimizing revascularization in ischemic cardiomyopathy: comparative evidence on the benefits and indications of CABG and PCI. Life. 2025;15(4):575. doi:10.3390/life15040575
14. Buszman P, Szkróbka I, Gruszka A, et al. Comparison of effectiveness of coronary artery bypass grafting versus percutaneous coronary intervention in patients with ischemic cardiomyopathy. Am J Cardiol. 2007;99(1):36–41. doi:10.1016/j.amjcard.2006.07.056
15. Liga R, Colli A, Taggart DP, Boden WE, De Caterina R. Myocardial revascularization in patients with ischemic cardiomyopathy: for whom and how. J Am Heart Assoc. 2023;12(6). doi:10.1161/JAHA.122.026943
16. Bangalore S, Guo Y, Samadashvili Z, Blecker S, Hannan EL. Revascularization in patients with multivessel coronary artery disease and severe left ventricular systolic dysfunction: everolimus-eluting stents versus coronary artery bypass graft surgery. Circulation. 2016;133(22):2132–2140. doi:10.1161/CIRCULATIONAHA.115.021168
17. Pei J, Wang X, Xing Z, Zheng K, Hu X. Short-term and long-term outcomes of revascularization interventions for patients with severely reduced left ventricular ejection fraction: a meta-analysis. ESC Heart Fail. 2021;8(1):634–643. doi:10.1002/ehf2.13141
18. Redfors B, Volz S, Angeras O, et al. Comparative effectiveness of CABG versus PCI in patients with ischemic heart disease: insights from SWEDEHEART registry. Eur Heart J. 2020;41(Supplement_2). doi:10.1093/ehjci/ehaa946.2521
19. Khan MR, Kayani WT, Pelton J, et al. Coronary artery bypass grafting versus percutaneous coronary intervention in patients with left ventricular systolic dysfunction. Cardiovasc Drugs Ther. 2020;35(3):575–585. doi:10.1007/s10557-020-07063-0
20. Cui K, Zhang D, Lyu S, et al. Meta-analysis comparing percutaneous coronary revascularization using drug-eluting stent versus coronary artery bypass grafting in patients with left ventricular systolic dysfunction. Am J Cardiol. 2018;122(10):1670–1676. doi:10.1016/j.amjcard.2018.08.002
21. Sun LY, Gaudino M, Chen RJ, Bader Eddeen A, Ruel M. Long-term outcomes in patients with severely reduced left ventricular ejection fraction undergoing percutaneous coronary intervention vs coronary artery bypass grafting. JAMA Cardiol. 2020;5(6):631–641. doi:10.1001/jamacardio.2020.0239
22. Nusca A, Lipinski MJ, Varma A, et al. Safety of drug-eluting stents in patients with left ventricular dysfunction undergoing percutaneous coronary intervention. Am J Cardiol. 2008;102(6):679–682. doi:10.1016/j.amjcard.2008.04.049
23. Madiyono B, Moeslichan Mz S, Sastroasmoro S, Budiman I, Purwanto S. Perkiraan Besar Sampel. In: Dasar-Dasar Metodologi Penelitian Klinis.
24. Dahlan MS. Besar Sampel Dalam Penelitian Kedokteran Dan Kesehatan.
25. Gaba P, Gersh BJ, Ali ZA, Moses JW, Stone GW. Complete versus incomplete coronary revascularization: definitions, assessment and outcomes. Nat Rev Cardiol. 2021;18(3):155–168. doi:10.1038/s41569-020-00457-5
26. Zhang D, Lyu S, Song X, et al. Coronary artery bypass grafting versus percutaneous coronary intervention in patients with left ventricular systolic dysfunction. Angiology. 2016;68(1):19–28. doi:10.1177/0003319716639197
27. Khalili A, Rahimi M, Khezerlouy-aghadam N, Akbarzadeh F, Taban-sadeghi M. In-hospital mortality of patients with severe left ventricular dysfunction undergoing coronary artery bypass grafting in Iranian population. J Cardiothorac Surg. 2022;17(1):1–5. doi:10.1186/s13019-022-01906-7
28. Adelborg K, Horváth-Puhó E, Schmidt M, et al. Thirty-year mortality after coronary artery bypass graft surgery: a Danish nationwide population-based cohort study. Circ Cardiovasc Qual Outcomes. 2017;10(5). doi:10.1161/CIRCOUTCOMES.116.002708
29. Howitt SH, Herring M, Malagon I, McCollum CN, Grant SW. Incidence and outcomes of sepsis after cardiac surgery as defined by the sepsis-3 guidelines. Br J Anaesth. 2018;120(3):509. doi:10.1016/j.bja.2017.10.018
30. Gutacker N, Bloor K, Cookson R, et al. Hospital surgical volumes and mortality after coronary artery bypass grafting: using international comparisons to determine a safe threshold. Health Serv Res. 2017;52(2):863. doi:10.1111/1475-6773.12508
31. Siregar S, Groenwold RHH, de mol BAJM, et al. Evaluation of cardiac surgery mortality rates: 30-day mortality or longer follow-up? Eur J Cardiothorac Surg. 2013;44(5):875–883. doi:10.1093/ejcts/ezt119
32. Sheiban I, Moretti C, Biondi Zoccai G, et al. Short- and long-term outcomes of percutaneous coronary interventions in patients with severe left ventricular dysfunction. EuroIntervention. 2007;3(3):359–364. doi:10.4244/EIJV3I3A65
33. Bonow RO, Maurer G, Lee KL, et al. Myocardial viability and survival in ischemic left ventricular dysfunction. N Engl J Med. 2011;364(17):1617–1625. doi:10.1056/NEJMoa1100358
34. Panza JA, Ellis AM, Al-Khalidi HR, et al. Myocardial viability and long-term outcomes in ischemic cardiomyopathy. N Engl J Med. 2019;381(8):739–748. doi:10.1056/NEJMoa1807365
35. Panza JA, Chrzanowski L, Bonow RO. Myocardial viability assessment before surgical revascularization in ischemic cardiomyopathy: JACC review topic of the week. J Am Coll Cardiol. 2021;78(10):1068–1077. doi:10.1016/j.jacc.2021.07.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.