Back to Journals » International Journal of Women's Health » Volume 17
Association Between Progesterone Level on Trigger Day to Basal Progesterone Ratio and in vitro Fertilization-Embryo Transfer Outcomes in Antagonist Protocols
Authors Xu MY, Wang YT, Liu YF ![]()
Received 29 November 2024
Accepted for publication 20 February 2025
Published 8 March 2025 Volume 2025:17 Pages 663—671
DOI https://doi.org/10.2147/IJWH.S506574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Miao-Yi Xu, Yu-Ting Wang, Yao-Fang Liu
Department of Reproductive Technology, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan Province, 646000, People’s Republic of China
Correspondence: Yao-Fang Liu, Department of Reproductive Technology, The Affiliated Hospital of Southwest Medical University, No. 25 of Taiping Street, Luzhou, Sichuan Province, 646000, People’s Republic of China, Tel +860830-3165649, Email [email protected]
Objective: To investigate the relationship between the progesterone level on trigger day (Ptrigger) to basal progesterone (bP) ratio and the outcomes of in vitro fertilization-embryo transfer (IVF-ET).
Methods: A retrospective analysis was conducted on women who received an antagonist protocol, with a Ptrigger less than 1.5 ng/mL and who underwent fresh embryo transfer. Based on the Ptrigger/bP ratio, participants were categorized into four groups: group A (Ptrigger/bP < 1, n = 284), group B (Ptrigger/bP ≥ 1 and < 2, n = 363), group C (Ptrigger/bP ≥ 2 and < 3, n = 165), and group D (Ptrigger/bP ≥ 3, n = 118). Recombinant follicle-stimulating hormone was used to stimulate ovulation. Receiver operating characteristic curve analysis was used to analyze the accuracy of the Ptrigger/bP ratio in predicting clinical pregnancy following fresh embryo transfer.
Results: A decreasing trend in bP levels was observed across groups (A > B > C > D), while Ptrigger levels showed an increasing trend (A < B < C < D). Groups A and B included significantly younger women and required lower doses of gonadotropin (Gn) compared to Groups C and D. The embryo implantation and clinical pregnancy rates in Group A were 34.93% and 49.30%, respectively, significantly higher than those in Group D (23.19% and 33.90%, respectively). After propensity score matching for age, the differences in implantation and clinical pregnancy rates were not statistically significant between Group A and D. The Ptrigger/bP ratio had limited accuracy in predicting clinical pregnancy, with an area under the curve of 0.538 (95% CI [confidence interval]: 0.501– 0.575, P = 0.044).
Conclusion: A Ptrigger/bP ratio of less than 1 was associated with relatively favorable pregnancy outcomes in women undergoing IVF-ET with an antagonist protocol for ovulation induction.
Keywords: antagonist protocol, basal progesterone, bP, IVF-ET outcome, in vitro fertilization-embryo transfer, IVF-ET, progesterone level on trigger day, Ptrigger
Introduction
The gonadotropin-releasing hormone antagonist (GnRH-ant) protocol is a commonly used protocol for ovulation induction in in vitro fertilization-embryo transfer (IVF-ET), offering several advantages such as shorter duration of ovulation induction, reduced total Gn usage, and a lower risk of ovarian hyperstimulation syndrome (OHSS).1 However, GnRH-ant cycles have been associated with a higher likelihood of elevated progesterone levels on trigger day (Ptrigger) compared to agonist protocols.2 At present, the most widely used threshold to indicate elevated Ptrigger is 1.5 ng/mL.3–5 Some researchers demonstrated that a Ptrigger level of 1.5 ng/mL or higher negatively affects endometrial receptivity, thereby diminishing the success rate of fresh embryo transfers, and they recommend replacing fresh embryo transfers with a full embryo freeze in such cases.6,7
The Ptrigger level is influenced by factors such as the basal progesterone (bP) levels, defined as progesterone levels measured on Days 2 or 3 of the menstrual cycle, multiple follicular development, and the total dose of Gn administered.8,9 bP, which is primarily produced by the adrenal glands, varies between individuals. Adrenal gland-derived progesterone remains relatively stable throughout the follicular phase.10 Therefore, changes in Ptrigger levels are inherently linked to bP levels. However, whether the extent of Ptrigger elevation and IVF-ET outcomes are correlated remains unclear. If such a correlation exists, different participant profiles may have varying Ptrigger thresholds.
The Ptrigger/bP ratio reflects the extent of change in Ptrigger levels relative to bP. Based on this, our aim in this study was to explore the relationship between the Ptrigger/bP ratio and IVF-ET outcomes, with the goal of providing a reference for informing clinical decision-making.
Materials and Methods
Clinical Data
The clinical data of women who underwent IVF-ET assisted reproduction at the Reproductive Medicine Department of our hospital between January 2019 and December 2023 were retrospectively analyzed.
The inclusion criteria were as follows: (1) Women aged below 35 years with normal ovarian reserve function who were undergoing their first IVF-ET for assisted reproduction. (2) Women receiving the antagonist protocol for controlled ovarian hyperstimulation (COH). (3) Women with a Ptrigger level < 1.5 ng/mL. (4) Women who received at least one high-quality embryo during the fresh embryo transfer.
The following were the exclusion criteria: (1) Women with ovarian diseases, a history of ovarian surgery, polycystic ovary syndrome, or diminished ovarian reserve. (2) Women with uterine abnormalities or malformations. (3) Women with a history of endocrine-related diseases, such as adrenal cortical hyperplasia, hypothyroidism, or hyperthyroidism. (4) Women with chromosomal abnormalities or a history of recurrent miscarriage.
All study participants signed the informed consent form. This study was approved by the Ethics Committee of the institution (No. 20190184).
Study Methods
Detection of Antral Follicle Count (AFC) and Sex Hormone Levels
On day 2 or 3 of the menstrual cycle, B-mode ultrasound was utilized to measure the size of antral follicles and antral follicle count (AFC) in the participants. On the same day, venous blood samples were collected to measure the levels of basal estradiol (bE2), bP, basal follicle stimulating hormone (bFSH), and basal luteinizing hormone (bLH). All hormone measurements were performed using the chemiluminescence assay method.
Ovulation Induction Regimen and Embryo Transfer
A daily subcutaneous injection of recombinant follicle-stimulating hormone (Serono, Merck, Switzerland) at a dose of 125–300 U/day was initiated from day 3 of the menstrual cycle to stimulate ovulation. The dosage was adjusted as needed according to follicular development and serum levels of estradiol (E2), luteinizing hormone (LH), and progesterone. The blood progesterone was measured on the ovulation trigger day. The hormone levels on the ovulation trigger day were measured using fasting blood samples collected at 8:00 AM on the trigger day. Starting on day 5 or 6 of ovulation induction, subcutaneous injection of an antagonist, cetrorelix acetate (Baxter Oncology GmbH, Germany), at 0.25 mg/day was added.
Trigger criteria: Ovulation was triggered when at least one follicle reached a diameter of ≥ 18 mm or at least three follicles measured ≥ 16 mm in diameter. On the trigger day, participants received a subcutaneous injection of 250 ug of recombinant human chorionic gonadotropin (hCG) (Serono, Merck, Switzerland). Oocyte retrieval was performed 36 to 37 hours post-trigger.
Three days after oocyte retrieval, the decision to proceed with fresh embryo transfer, freezing, or extended culture to the blastocyst stage was made based on the participants’ endometrial condition, embryo quality, and other clinical factors. Luteal phase support was provided to participants who underwent fresh embryo transfer.
Judgement of Pregnancy Outcome
A β-human chorionic gonadotropin (hCG) level > 10 U/L, measured 14 days post-embryo transfer, was defined as hCG-positive. For individuals with positive hCG results, a transvaginal ultrasound was performed between 28 and 35 days post-embryo transfer to confirm a clinical pregnancy, indicated by the presence of a gestational sac within the uterine cavity.
Observation Indicators
Indicators compared between the groups in the study included general data such as age of the participants, bFSH, and anti-Müllerian hormone (AMH); indicators of ovulation induction status such as the estradiol (E2) level on the trigger day, the total dose of Gn administered, and the number of oocytes retrieved; and the outcome of fresh embryo transfer. Embryo implantation rate = number of gestational sacs / total number of embryos transferred × 100%. Clinical pregnancy rate = number of clinical pregnancy cycles / number of transfer cycles × 100%.
Experimental Setting
Based on the Ptrigger/bP ratio, the cycles were categorized into four groups: group A (Ptrigger/bP < 1, n = 284), group B (Ptrigger/bP ≥ 1 and < 2, n = 363), group C (Ptrigger/bP ≥ 2 and < 3, n = 165), and group D (Ptrigger/bP ≥ 3, n = 118). Participants were divided into a pregnant group and a non-pregnant group based on whether they achieved clinical pregnancy after embryo transfer. Each patient underwent a single transfer, and the number of embryos transferred ranged from one to two.
Statistical Analysis
Statistical analyses were performed using SPSS version 23.0 software. The normality of distribution for measurement data was assessed using the Kolmogorov–Smirnov test. Normally distributed measurement data were presented as the mean ± standard deviation  and analyzed using independent-samples t-tests or one-way analysis of variance (ANOVA). Non-normally distributed measurement data were expressed as the median and interquartile range (M [P25, P75]) and analyzed using the Mann–Whitney U-test. Categorical data were reported as percentages (%) and compared using the chi-squared test or Fisher’s exact test.
and analyzed using independent-samples t-tests or one-way analysis of variance (ANOVA). Non-normally distributed measurement data were expressed as the median and interquartile range (M [P25, P75]) and analyzed using the Mann–Whitney U-test. Categorical data were reported as percentages (%) and compared using the chi-squared test or Fisher’s exact test.
Logistic regression analysis was employed to explore associations between various factors and clinical pregnancy following fresh embryo transfer. The predictive power of each influencing factor was evaluated using receiver operating characteristic (ROC) curve analysis, with an area under the curve (AUC) value > 0.5 indicating that the factor had diagnostic utility. A statistically significant difference was defined as a P value < 0.05 (P < 0.05).
Results
Comparison of Clinical Characteristics Between Pregnant and Non-Pregnant Women
A total of 930 assisted reproduction cycles were included in this study. Baseline characteristics: age: 30.49 ± 3.41 years (range: 20–34 years); duration of infertility: 4.55 ± 3.69 years (range: 1–16 years); bP level: 0.64 ± 0.47 ng/mL (range: 0.10–2.84 ng/mL); and Ptrigger level: 0.76 ± 0.36 ng/mL (0.10–1.49 ng/mL). Compared to the non-pregnant group, women in the pregnant group were significantly younger, had a shorter duration of infertility, received a lower total Gn dose, had a higher AFC, and more oocytes were retrieved (P < 0.05). The two groups did not show any statistically significant differences in AMH, body mass index (BMI), or basal hormone levels (P > 0.05) (Table 1).
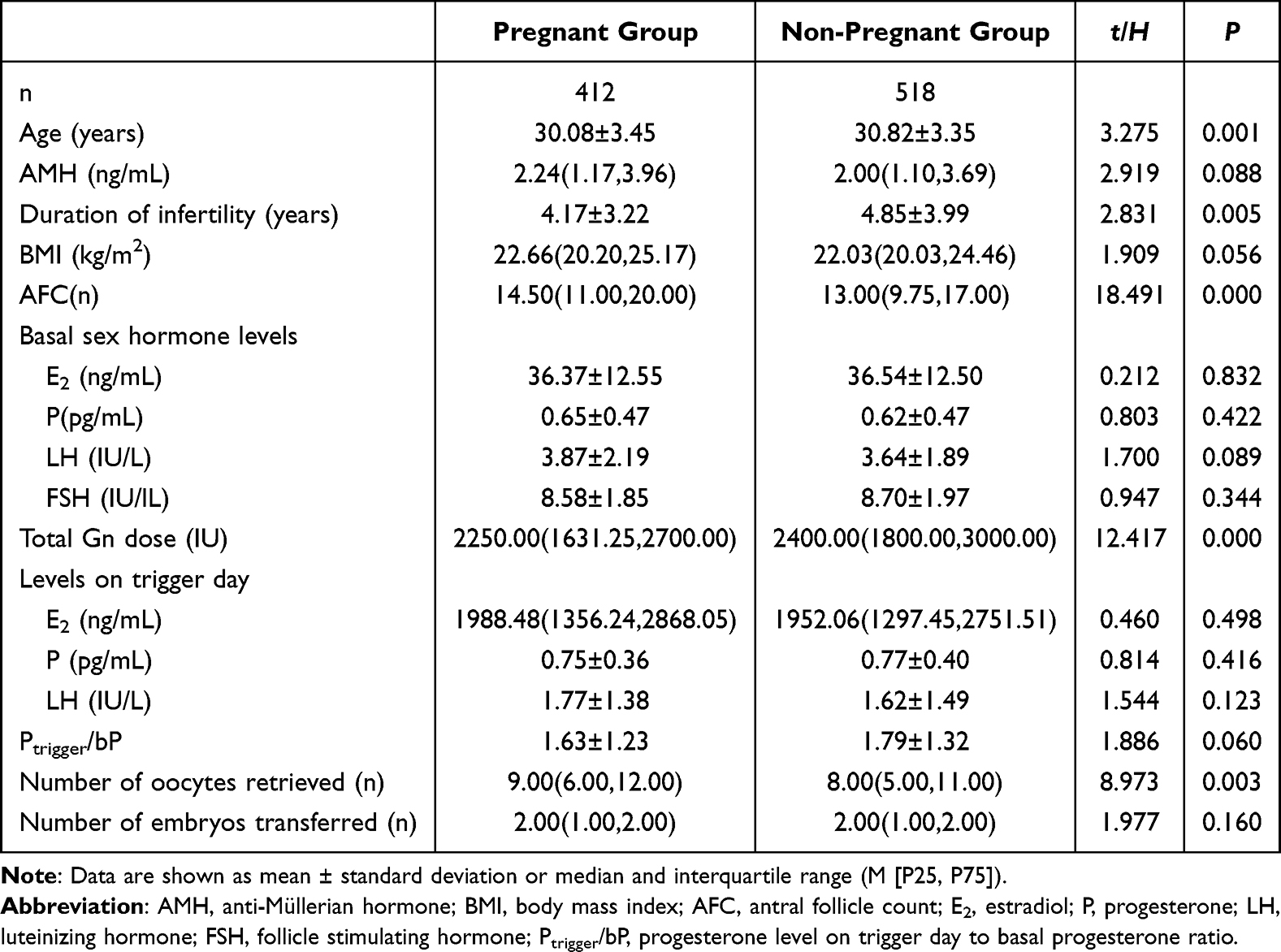 |
Table 1 Comparison of Clinical Characteristics of Women in the Pregnant and Non-Pregnant Groups |
Multivariate Logistic Regression Analysis of Factors Linked to Clinical Pregnancy in IVF-ET Cycles
A multivariate logistic regression model was constructed using factors with statistically significant differences identified in the univariate analysis. These factors included age, duration of infertility, AFC, total Gn dose, and number of oocytes retrieved. The analysis showed that age was a significant factor associated with clinical pregnancy outcomes (P < 0.05) (Table 2).
 |
Table 2 Logistic Regression Analysis of Factors Linked to Clinical Pregnancy |
Comparison of Clinical Characteristics Between Groups with Varying Ptrigger/bP Ratios
After categorizing participants based on their Ptrigger/bP ratio, it was observed that bP levels followed a descending order across the groups: group A > group B > group C > group D. Conversely, Ptrigger levels followed an ascending order: group A < group B < group C < group D. Groups A and B had significantly younger women, and their dose of total Gn was lower than those in groups C and D (P < 0.05). Additionally, E2 levels on trigger day in groups A and B were significantly lower than those in groups C and group D (P < 0.05). The number of oocytes retrieved in groups A, B, and C was significantly lower than that in group D. The embryo implantation rate and clinical pregnancy rate among women in group A were significantly higher than those in group D (P < 0.05). No significant differences were found between Groups A, B, C, and D with respect to AMH, duration of infertility, or BMI (P > 0.05) (Table 3).
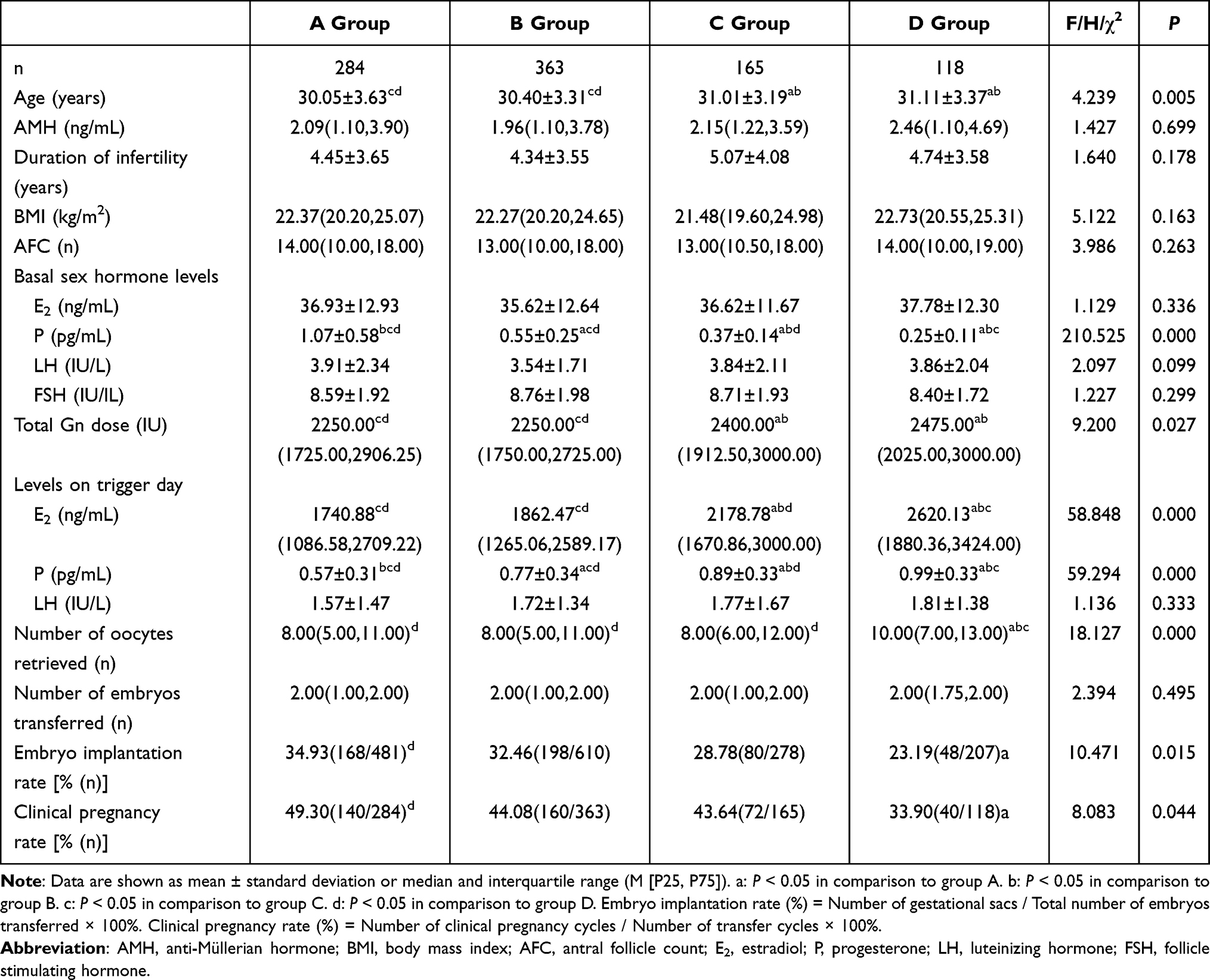 |
Table 3 Comparison of Clinical Characteristics Among Groups with Varying Ptrigger/bP Ratios |
Comparison of Clinical Characteristics After Age Matching Between Groups A and D
Given the aforementioned significant differences between groups A and D with respect to pregnancy outcomes, as well as the observed difference in age, a 1:1 propensity score matching was performed between groups A and D to control for age-related confounding factors. Propensity score matching was conducted using R 4.1.1 software with a caliper value of 0.1 to analyze the relationship between Ptrigger/bP and assisted reproduction outcomes.
The results showed that, prior to matching, women in group A were younger, received a lower total Gn dose, had lower trigger day E2 levels, lower Ptrigger levels, and fewer oocytes retrieved, compared to group D. Additionally, women in group A had higher bP levels, embryo implantation rates, and clinical pregnancy rates (P < 0.05). After matching, compared to group D, women in group A still had lower trigger day E2 and Ptrigger levels but higher bP levels (P < 0.05). The embryo implantation and clinical pregnancy rates were higher in group A than in group D, but the differences were not significant (P > 0.05).
Analysis of the Predictive Power of Ptrigger/bP Ratio for Clinical Pregnancy After Fresh Embryo Transfer Using ROC Curve Analysis
An ROC curve was plotted to evaluate the diagnostic accuracy of the Ptrigger/bP ratio for predicting clinical pregnancy after fresh embryo transfer. The analysis revealed that the AUC was 0.538, indicating limited predictive ability. The sensitivity and specificity were 0.850 and 0.270, respectively, with a 95% CI of 0.501–0.575, (P = 0.044) (Figure 1).
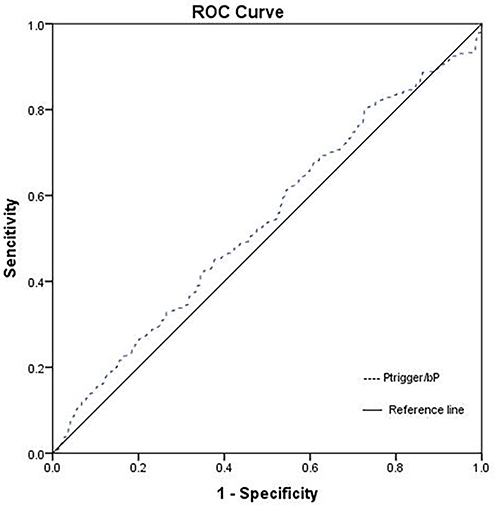 |
Figure 1 ROC curve analysis of the predictive power of Ptrigger/bP ratio for clinical pregnancy after fresh embryo transfers. |
Discussion
Most studies suggest that elevated Ptrigger levels in antagonist protocols exert a negative impact on the success rate of fresh embryo transfer in IVF-ET.11 The underlying mechanism proposed is that elevated Ptrigger levels cause premature progression of the endometrium into the secretory phase, leading to a developmental asynchrony between the embryo and the endometrium. This disrupts the implantation process, thereby reducing clinical pregnancy rates and potentially lowering live birth rates.12
Various thresholds for elevated Ptrigger levels have been reported in the literature, including 0.8 ng/mL, 1.4 ng/mL, and 1.5 ng/mL, among others,11,13,14 with 1.5 ng/mL being the most frequently used. The discrepancies in threshold values reported across studies may relate to differences in basal progesterone levels, individual variations in progesterone secretion, heterogeneity in baseline characteristics of study populations, and differences in ovarian response to stimulation among women undergoing ovulation induction. Since bP levels vary among individuals, Ptrigger levels change in accordance with bP. However, the relationship between the extent of Ptrigger elevation and the outcome of IVF assisted reproduction remains poorly understood.
In this study, women with Ptrigger values uniformly below 1.5 ng/mL were included to evaluate the success rate of fresh embryo transfer. The Ptrigger/bP ratio was used to reflect changes in Ptrigger relative to bP. Participants were divided into four groups based on the Ptrigger/bP ratios of <1, ≥1 to ≤2, ≥2 to ≤3, and ≥3, respectively. Differences in assisted reproduction outcomes among different groups were analyzed. Our analysis revealed that with increases in the Ptrigger/bP ratio, bP levels progressively decreased (group A > group B > group C > group D), while Ptrigger levels simultaneously rose (group A < group B < group C < group D). Women with Ptrigger/bP < 2 (groups A and B) were significantly younger, required less total Gn, and had lower trigger day E2 levels compared to those with Ptrigger/bP ≥ 2 (groups C and D). Furthermore, women with Ptrigger/bP < 3 (groups A, B, and C) had significantly fewer oocytes retrieved compared to those with Ptrigger/bP ≥ 3 (group D).
During controlled ovarian hyperstimulation (COH), large doses of exogenous gonadotropins promote the simultaneous development of multiple follicles. Granulosa cells within these follicles synthesize significantly higher amounts of progesterone compared to natural cycles,15,16 leading to elevated progesterone levels, including Ptrigger, in the late follicular phase.17 In this study, we found that, with variations in the Ptrigger/bP ratio, significant inter-group differences in Ptrigger levels were observed. Notably, the groups with a Ptrigger/bP ratio of ≥ 2, especially those reaching a ratio of 3, showed a consistent trend of significantly higher levels of total Gn doses, E2 levels on trigger day, and more retrieved oocytes than other groups.
We also found that an increase in the Ptrigger/bP ratio was associated with a gradual decline in both the implantation rates (34.93%, 32.46%, 28.78%, and 23.19% in each group, respectively) and the clinical pregnancy rates (49.30%, 44.08%, 43.64%, and 33.90% in each group, respectively). Group D, where the Ptrigger/bP ratio was ≥ 3, had significantly lower embryo implantation and clinical pregnancy rates than Group A, where the Ptrigger/bP ratio was < 1. This result indicates a potential link between lower Ptrigger/bP ratios and better outcomes in fresh embryo transfer (IVF-ET). Women with a Ptrigger/bP ratio < 3, especially those with a Ptrigger/bP ratio < 1, achieved favorable outcomes, while those with a Ptrigger/bP ratio ≥ 3 tended to have poorer post-transfer outcomes. However, our analysis also highlighted the presence of various confounding factors, such as age and total Gn dosage, among other factors across the groups. Therefore, to isolate the effect of the Ptrigger/bP ratio on embryo transfer outcomes, the influence of these other variables needs to be considered and controlled.
It is well established that the outcome of fresh embryo transfers is related to several factors. In this study, participants were categorized into pregnant and non-pregnant groups to investigate factors related to clinical pregnancy. The results revealed that, compared to the non-pregnant group, women in the pregnant group were significantly younger, had a shorter duration of infertility, required lower total Gn, and had significantly higher AFC and more retrieved oocytes. Subsequent logistic regression analysis confirmed that age was a significant predictor of clinical pregnancy among women undergoing IVF. This finding is consistent with published reports.18–20
Propensity score matching was utilized to control for the confounding effect of age between groups A and D. After matching, the results showed that women in group A (Ptrigger/bP < 1) exhibited lower trigger day E2 levels, lower Ptrigger, and higher bP levels compared to those in group D (Ptrigger/bP ≥ 3). Women in group A demonstrated higher embryo implantation and clinical pregnancy rates compared to those in group D (Ptrigger/bP ≥ 3), but these differences were not statistically different (Table 4). Furthermore, ROC curve analysis showed that the AUC for the predictive power of Ptrigger/bP ratio for clinical pregnancy after fresh embryo transfer was 0.538, indicating limited diagnostic utility. These findings suggest that a Ptrigger/bP ratio < 1 may be associated with improved assisted reproduction outcomes, but the ratio’s overall ability to predict clinical pregnancy success in fresh embryo transfer cycles, particularly under an antagonist protocol, appears limited.
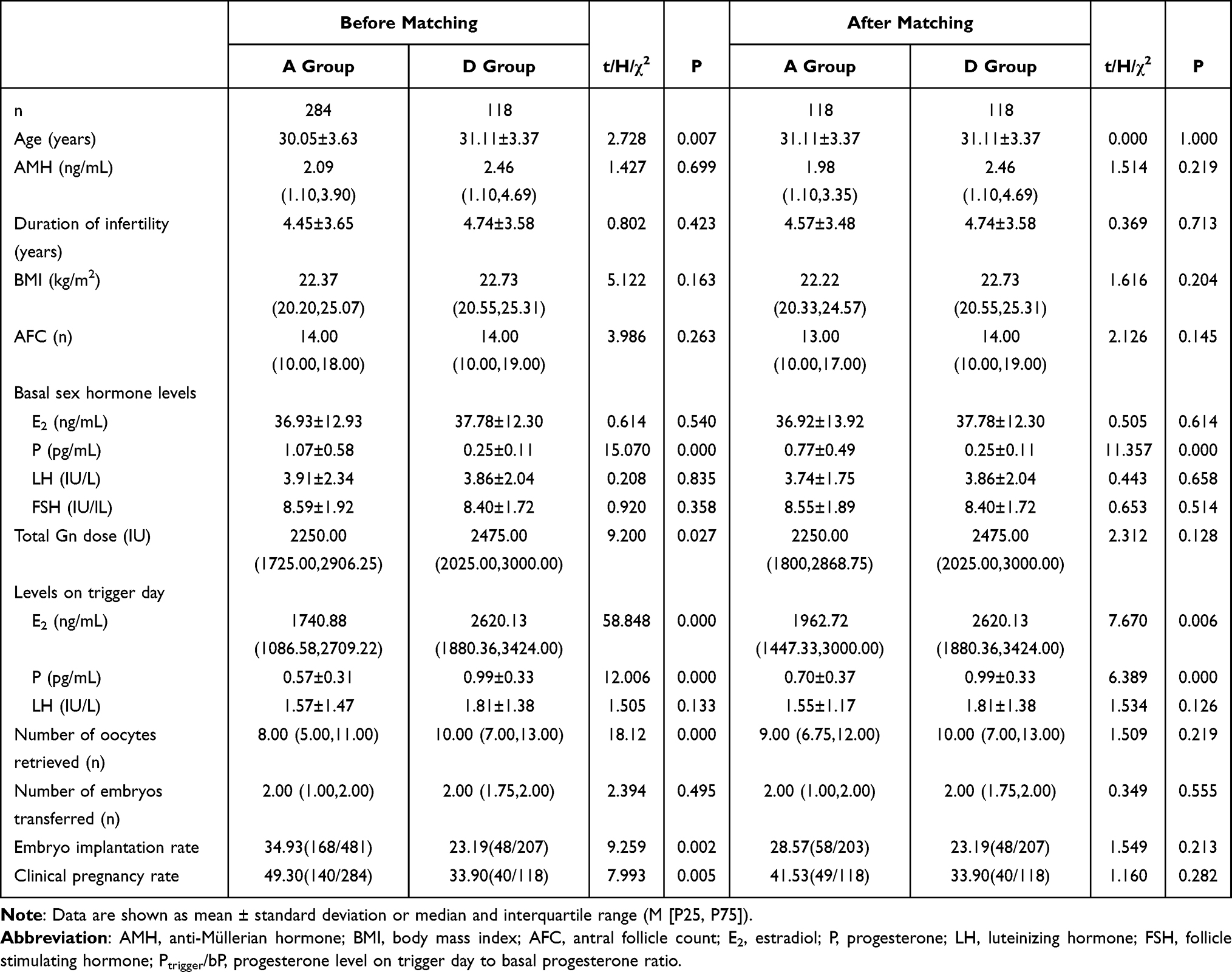 |
Table 4 Comparison of Clinical Characteristics After Age Matching Between Groups A and D |
Conclusion
In conclusion, in this study among women with normal ovarian reserve undergoing ovulation induction with an antagonist protocol, those with a Ptrigger/bP ratio < 1 tended to have better assisted reproductive outcomes. However, the predictive accuracy of the Ptrigger/bP ratio for clinical pregnancy following fresh embryo transfer was found to be relatively low, highlighting the need for further investigation. This study has several limitations. 1) As a retrospective analysis, the results may be subject to inherent bias. 2) Study participants were not stratified based on bP levels, and this may not fully reflect the impact of Ptrigger/bP on fresh embryo transfer outcomes. Future research should involve larger sample sizes and continued observation to further clarify the relationship between the Ptrigger/bP ratio and IVF-ET outcomes in antagonist protocols.
Data Sharing Statement
The datasets used or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of The Affiliated Hospital of Southwest Medical University (No. 20190184). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Funding
This research was supported by The Sichuan Provincial Department of Science and Technology (NO. 2022YFS0082).
Disclosure
The authors declare that they have no conflict of interest regarding this work.
References
1. Si M, Qi X, Zhen X, et al. Dose nomogram of individualization of the initial follicle-stimulating hormone dosage for patients with polycystic ovary syndrome undergoing IVF/ICSI with the GnRH-ant protocol: a retrospective cohort study. Adv Ther. 2023;40(9):3971–3985. Epub 2023 Jul 3. PMID: 37395872; PMCID: PMC10427540. doi:10.1007/s12325-023-02582-2
2. Sun Y, Zhu A. Effect of body mass index on progesterone level on trigger day in gonadotropin-releasing hormone antagonist cycles. Gynecol Endocrinol. 2024;40(1):2364892. Epub 2024 Jun 30. PMID: 38946240. doi:10.1080/09513590.2024.2364892
3. Tokgoz VY, Ekici GC, Tekin AB. The efficiency of progesterone/estradiol and progesterone/follicle ratio without elevated trigger-day progesterone levels on the reproductive outcomes of GnRH antagonist IVF/ICSI cycles. Gynecol Endocrinol. 2021;37(10):885–890. Epub 2021 Feb 1. PMID: 33517800. doi:10.1080/09513590.2021.1878137
4. Lee CI, Chen HH, Huang CC, Lin PY, Lee TH, Lee MS. Early progesterone change associated with pregnancy outcome after fresh embryo transfer in assisted reproduction technology cycles with progesterone level of >1.5 ng/ml on human chorionic gonadotropin trigger day. Front Endocrinol. 2020;11:653. PMID: 33042015; PMCID: PMC7522275. doi:10.3389/fendo.2020.00653
5. Golbasi H, Ince O, Golbasi C, Ozer M, Demir M, Yilmaz B. Effect of progesterone/estradiol ratio on pregnancy outcome of patients with high trigger-day progesterone levels undergoing gonadotropin-releasing hormone antagonist intracytoplasmic sperm injection cycles: a retrospective cohort study. J Obstet Gynaecol. 2019;39(2):157–163. Epub 2018 Oct 3. PMID: 30280612. doi:10.1080/01443615.2018.1504204
6. Gurunath S. Premature progesterone elevation in in vitro fertilisation cycles - current perspectives. J Hum Reprod Sci. 2022;15(4):325–336. Epub 2022 Dec 30. PMID: 37033132; PMCID: PMC10077738. doi:10.4103/jhrs.jhrs_162_22
7. George JS, Keefe KW, Lanes A, Yanushpolsky E. Premature progesterone elevation during the early and mid-follicular phases in fresh in vitro fertilization (IVF) cycles is associated with lower live birth, clinical pregnancy, and implantation rates. J Assist Reprod Genet. 2023;40(5):1029–1035. Epub 2023 Apr 4. PMID: 37012450; PMCID: PMC10239424. doi:10.1007/s10815-023-02786-z
8. Koo HS, Cha SH, Kim HO, et al. A high response to controlled ovarian stimulation induces premature luteinization with a negative impact on pregnancy outcomes in a gonadotropin-releasing hormone antagonist cycle. Clin Exp Reprod Med. 2015;42(4):149–155. Epub 2015 Dec 31. PMID: 26816874; PMCID: PMC4724599. doi:10.5653/cerm.2015.42.4.149
9. Oktem O, Akin N, Bildik G, et al. FSH Stimulation promotes progesterone synthesis and output from human granulosa cells without luteinization. Hum Reprod. 2017;32(3):643–652. PMID: 28158500. doi:10.1093/humrep/dex010
10. Yadav A, Noor N, Mahey R, Singh N, Dwarakanathan V, Malhotra N. Serum progesterone on the day of human chorionic gonadotropin (hCG) trigger as a predictor of in-vitro fertilization (IVF) outcome - a retrospective analysis of seven years. JBRA Assist Reprod. 2023;27(2):156–162. PMID: 35916460; PMCID: PMC10279434. doi:10.5935/1518-0557.20220023
11. Wei L, Zhao Y, Xu C, Zhang C. Slightly elevated progesterone on HCG trigger day has an impact on pregnancy outcomes of fresh single blastocyst transfer cycles under an early follicular phase prolonged protocol cycle. Int J Womens Health. 2022;14:1761–1768. PMID: 36568124; PMCID: PMC9784381. doi:10.2147/IJWH.S385362
12. Kalakota NR, George LC, Morelli SS, Douglas NC, Babwah AV. Towards an improved understanding of the effects of elevated progesterone levels on human endometrial receptivity and oocyte/embryo quality during assisted reproductive technologies. Cells. 2022;11(9):1405. PMID: 35563710; PMCID: PMC9105155. doi:10.3390/cells11091405
13. Zhao J, Hao J, Xu B, Wang Y, Li Y. Effect of slightly elevated progesterone on hCG trigger day on clinical pregnancy rate in GnRH-ant IVF/ICSI cycles. Reprod Health. 2022;19(1):66. PMID: 35287707; PMCID: PMC8919624. doi:10.1186/s12978-022-01371-4
14. Liu R, Zhou L, Chen X, He H, Cai Z. Letrozole supplementation and the increased risk of elevated progesterone levels on trigger day. Front Endocrinol. 2022;13:904089. PMID: 35957830; PMCID: PMC9359123. doi:10.3389/fendo.2022.904089
15. Cortés-Vazquez A, Veliz-Figueroa D, Vargas-Estrada K, Moreno-García JD, Cortés-Algara A. Progesterone levels on hCG day and oocyte maturation in a Mexican IVF program. JBRA Assist Reprod. 2024;28(2):247–253. PMID: 38289204; PMCID: PMC11152430. doi:10.5935/1518-0557.20240001
16. Manna PR, Stetson CL, Slominski AT, Pruitt K. Role of the steroidogenic acute regulatory protein in health and disease. Endocrine. 2016;51(1):7–21. Epub 2015 Aug 14. PMID: 26271515; PMCID: PMC4707056. doi:10.1007/s12020-015-0715-6
17. Elnashar AM. Progesterone rise on the day of HCG administration (premature luteinization) in IVF: an overdue update. J Assist Reprod Genet. 2010;27(4):149–155. Epub 2010 Feb 23. PMID: 20177771; PMCID: PMC2854984. doi:10.1007/s10815-010-9393-8
18. Shingshetty L, Cameron NJ, Mclernon DJ, Bhattacharya S. Predictors of success after in vitro fertilization. Fertil Steril. 2024;121(5):742–751. Epub 2024 Mar 16. PMID: 38492930. doi:10.1016/j.fertnstert.2024.03.003
19. Pathare ADS, Loid M, Saare M, et al. Endometrial receptivity in women of advanced age: an underrated factor in infertility. Hum Reprod Update. 2023;29(6):773–793. PMID: 37468438; PMCID: PMC10628506. doi:10.1093/humupd/dmad019
20. Homer HA. Understanding oocyte ageing. Minerva Obstet Gynecol. 2024;76(3):284–292. Epub 2024 Mar 27. PMID: 38536027. doi:10.23736/S2724-606X.24.05343-0
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.