Back to Journals » International Journal of Women's Health » Volume 18
Association Between Peripheral Blood Lymphocyte Count and HER2 Status in Breast Cancer: A Retrospective Study
Authors Liang H, Lin Y, Pan K, Wang J, Xie X, Ding M, Lin J
Received 8 December 2025
Accepted for publication 12 February 2026
Published 18 February 2026 Volume 2026:18 582468
DOI https://doi.org/10.2147/IJWH.S582468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Huikai Liang,1,2,* Yongming Lin,1,2,* Kelun Pan,1,2,* Jiayi Wang,1,2 Xinru Xie,1,2 Mingji Ding,1,2 Jianqing Lin1,2
1Department of Breast Surgery, The Second Affiliated Hospital of Fujian Medical University, Quanzhou, People’s Republic of China; 2The Second Clinical College of Fujian Medical University, Quanzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mingji Ding, Email [email protected] Jianqing Lin, Email [email protected]
Background: Overexpression of human epidermal growth factor receptor 2 (HER2) in breast cancer is associated with aggressive tumor biology and a distinct immune microenvironment. Although the absolute lymphocyte count (ALC) in peripheral blood is widely used as a routine indicator of systemic immune function, its relationship with HER2 status remains insufficiently explored.
Methods: This retrospective study investigated the association between pretreatment peripheral ALC and HER2 status in a cohort of breast cancer patients. Multivariate logistic regression, random forest modeling, and restricted cubic spline (RCS) analyses were employed to assess this relationship. Subgroup analyses were conducted across major clinical and pathological variables to evaluate their robustness. In parallel, tumor immune infiltration profiles were analyzed using the TIMER 2.0 platform.
Results: A robust and consistent inverse association was observed between ALC and HER2-positive status across all analytical approaches. In fully adjusted logistic regression models, higher ALC was independently associated with lower odds of HER2 positivity (OR= 0.53, 95% CI: 0.37– 0.77, P< 0.001), with consistent effects across all examined subgroups. Further immune profiling using the TIMER 2.0 platform demonstrated that ERBB2 (HER2) expression was negatively correlated with the infiltration of key anti-tumor lymphocytes, including CD8⁺ T cells, activated memory CD4⁺ T cells, and natural killer (NK) cells, while showing relative enrichment of immature B cells and non-regulatory CD4⁺ T cells. Collectively, these findings suggest that HER2-overexpressing tumors are associated with concurrent systemic immune alterations and a locally suppressed tumor immune microenvironment.
Conclusion: Peripheral blood ALC levels are negatively correlated with HER2 expression in breast cancer. Given its accessibility and cost-effectiveness, ALC may serve as a complementary systemic immune indicator for contextual assessment of HER2-related immune characteristics and immune heterogeneity at the population level.
Keywords: peripheral blood, absolute lymphocyte count, breast cancer, HER2, TIMER 2.0
Introduction
Breast cancer remains the most common malignancy among women worldwide and continues to pose a substantial global public health challenge.1 Human epidermal growth factor receptor 2 (HER2), encoded by the ERBB2 gene, is overexpressed or amplified in approximately 15%–20% of breast cancer patients.2 This molecular alteration is associated with increased tumor aggressiveness, poorer prognosis, and response to specific targeted therapies.3 The introduction of HER2-targeted agents, such as trastuzumab and pertuzumab, has markedly improved clinical outcomes in patients with HER2-positive breast cancer.4,5
Emerging evidence further suggests that crosstalk between HER2 signaling and the immune system plays a pivotal role in disease progression, therapeutic response, and resistance mechanisms.6–8 Understanding these interactions is therefore essential for optimizing treatment strategies and developing novel therapeutic approaches.
Tumor-infiltrating immune cells, particularly lymphocytes, have been extensively investigated in breast cancer and are recognized as key components of the tumor microenvironment.9 In HER2-positive breast cancer, higher tumor-infiltrating lymphocytes (TILs) density has been associated with better clinical prognosis and enhanced responses to HER2-targeted therapies.10,11 However, while the local immune response within the tumor has been extensively studied, the systemic immune status, particularly as reflected by peripheral immune markers like lymphocyte counts, remains less explored in the context of HER2 expression.
Absolute lymphocyte count (ALC) in peripheral blood is a routine, cost-effective, and easily obtainable biomarker that reflects systemic immune function. A reduced ALC has been associated with poor prognosis in various malignancies, including breast cancer.12,13 However, the relationship between HER2 expression and peripheral immune cell levels, such as ALC, remains poorly understood. Investigating this association may enhance our understanding of tumor–host immune interactions and help identify accessible immunological markers linked to HER2-driven tumor biology.
From a clinical practice perspective, particularly in resource-limited settings or primary care environments, breast cancer patients often cannot immediately obtain complete pathological and molecular profiling results at the time of initial diagnosis or during the preoperative period. Prior to the availability of routine pathology and HER2-related immunohistochemistry or fluorescence in situ hybridization (IHC/FISH) results, clinicians may face an information gap regarding a patient’s HER2 status, which can constrain early risk stratification and preliminary clinical decision-making.
Within this context, the present study explores ALC as a potential early, systemically accessible immune indicator. Importantly, ALC is not intended to replace standard HER2 testing methods, but rather to serve as supplementary immunological information. In selected clinical scenarios, ALC may provide preliminary contextual insight into HER2 status and the tumor immune milieu. In particular, when pathological results are pending or diagnostic resources are limited, ALC may assist in initial risk assessment and overall immune status evaluation, thereby offering complementary background information to support subsequent standardized testing and treatment decisions.
This study investigates the association between HER2 expression and peripheral blood ALC in breast cancer patients, aiming to assess whether HER2-positive tumors are associated with systemic immune suppression. To further interrogate the tumor immune microenvironment, we performed immune infiltration analysis using the TIMER2.0 database, which integrates multiple deconvolution algorithms.14 By combining peripheral and intratumoral perspectives, we seek to delineate a comprehensive immune profile of HER2-positive breast cancer and provide new insights into its immunological characteristics.
Materials and Methods
Study Population
Clinical data were retrospectively extracted from the institutional electronic medical record system, with all personal identifiers removed to protect patient confidentiality. A total of 789 patients were consecutively enrolled from the Department of Breast Surgery at The Second Affiliated Hospital of Fujian Medical University between July 1, 2021, and June 30, 2025.
Inclusion criteria were as follows: (1) female patients aged 20 years or older; (2) those who underwent primary surgical treatment for breast cancer; (3) histologically confirmed primary breast cancer as the first and only malignancy; (4) no evidence of distant metastasis at the time of diagnosis; and (5) no receipt of neoadjuvant therapy.
Exclusion criteria included: (1) incomplete data for key clinical covariates; (2) history of severe infection or active inflammation within one month before diagnosis; (3) presence of pre-existing immune system disorders; (4) severe dysfunction of major organs.
The detailed patient selection flowchart is presented in Figure 1. All clinical data were extracted after the completion of patient enrollment, and the dataset was locked prior to statistical analysis and manuscript submission.
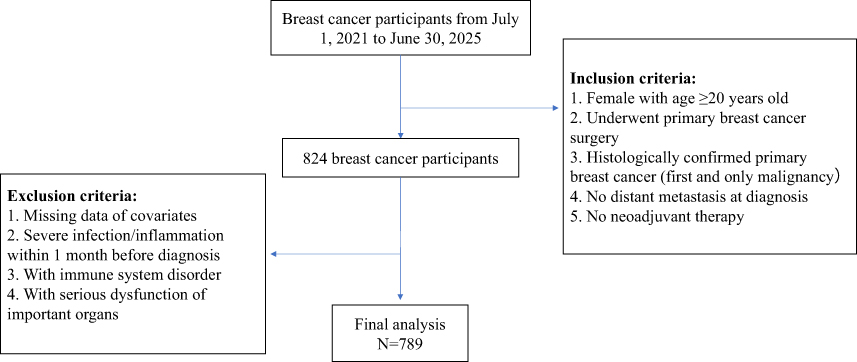 |
Figure 1 Flowchart of participant selection. |
HER2 Status Assessment
HER2 protein expression was evaluated using immunohistochemistry (IHC). For cases with equivocal IHC results (2+), fluorescence in situ hybridization (FISH) was performed to assess HER2 gene amp lification and determine the final HER2 status.
The interpretation criteria were as follows: IHC scores of 0 or 1+ were classified as HER2-negative, IHC scores of 3+ were classified as HER2-positive, IHC scores of 2+ were considered equivocal and required FISH testing. If FISH indicated HER2 gene amplification, the case was deemed HER2-positive; if no amplification was detected, the case was classified as HER2-negative.
Assessment of Absolute Lymphocyte Count
All preoperative blood samples were collected in the morning as part of routine clinical assessment. Peripheral blood samples were collected from all participants within two weeks prior to breast cancer surgery. ALC was measured as part of routine preoperative laboratory testing in the hospital’s clinical laboratory.
Covariate Adjustment
Covariates were selected based on prior research and clinical relevance. The following variables were adjusted for in the analysis: age, body mass index (BMI), hypertension (yes/no), diabetes (yes/no), marital status (unmarried/married), history of childbirth (yes/no), menopausal status (yes/no), tumor laterality (left/right), tumor multiplicity (single/multiple), histological grade (I, II, III), presence of perineural or vascular invasion (yes/no), estrogen receptor (ER) status (positive/negative), progesterone receptor (PR) status (positive/negative), and axillary lymph node metastasis (ALNM) (yes/no).
Due to the very low prevalence (fewer than ten cases) of smoking and alcohol consumption in the study population, these two variables were excluded from the final analysis.
Statistical Analysis
All statistical analyses were conducted using R software (version 4.5.1). Participants were stratified into two groups based on HER2 status for comparison of baseline characteristics. Continuous variables were tested for normality using the Kolmogorov–Smirnov test. Variables with normal distribution were expressed as mean ± standard deviation (SD) and compared using independent-samples t-tests. Categorical variables were presented as frequencies and percentages, with between-group differences assessed using the chi-square test or Fisher’s exact test, as appropriate.
To investigate the association between ALC and HER2 status, we employed a series of rigorous analytical approaches: First, multivariate logistic regression models were constructed with HER2 status as the dependent variable and ALC as the primary independent variable. These models were sequentially adjusted for potential confounders. Second, a random forest machine learning algorithm was implemented to assess the predictive importance of ALC for HER2 status, with importance quantified by mean decrease in accuracy and mean decrease in Gini index. Third, restricted cubic spline (RCS) modeling was applied to explore potential nonlinear associations between ALC and HER2 expression. Additionally, subgroup analyses were performed based on predefined stratification factors to validate the robustness of the observed associations.
To further explore the immunological context of HER2 expression, we utilized the TIMER2.0 online platform to analyze the correlations between HER2 gene expression and levels of immune cell infiltration (including T cells, B cells, and NK cells) in the breast cancer tumor microenvironment.
A two-tailed p-value < 0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 789 breast cancer patients were included in this study, comprising 580 cases (73.51%) in the HER2-negative group and 209 cases (26.49%) in the HER2-positive group.
Compared with the HER2-negative group, the HER2-positive group had a significantly higher Ki67 proliferation index (45.77 ± 17.23 vs 34.06 ± 21.56, P < 0.001) and a significantly lower ALC (1.79 ± 0.50 vs 1.93 ± 0.54, P = 0.002). Statistically significant differences were also observed between groups in histological grade, estrogen receptor (ER) status, and progesterone receptor (PR) status (P < 0.001 for all). In addition, differences in marital status (P = 0.040), parity history (P = 0.027), and menopausal status (P = 0.037) were statistically significant.
In contrast, no significant differences were found between the two groups with respect to age, tumor size, body mass index (BMI), tumor laterality, number of tumors, perineural invasion, vascular invasion, axillary lymph node metastasis (ALNM), hypertension, or diabetes (P > 0.05 for all). Baseline characteristics of the study population are summarized in Table 1.
 |
Table 1 The Baseline Characteristics of 789 Breast Cancer Participants |
Association Between ALC and HER2-Positive Status
Table 2 presents the results of logistic regression analyses evaluating the association between ALC and HER2-positive status. A consistent and statistically significant inverse association was observed across all models.
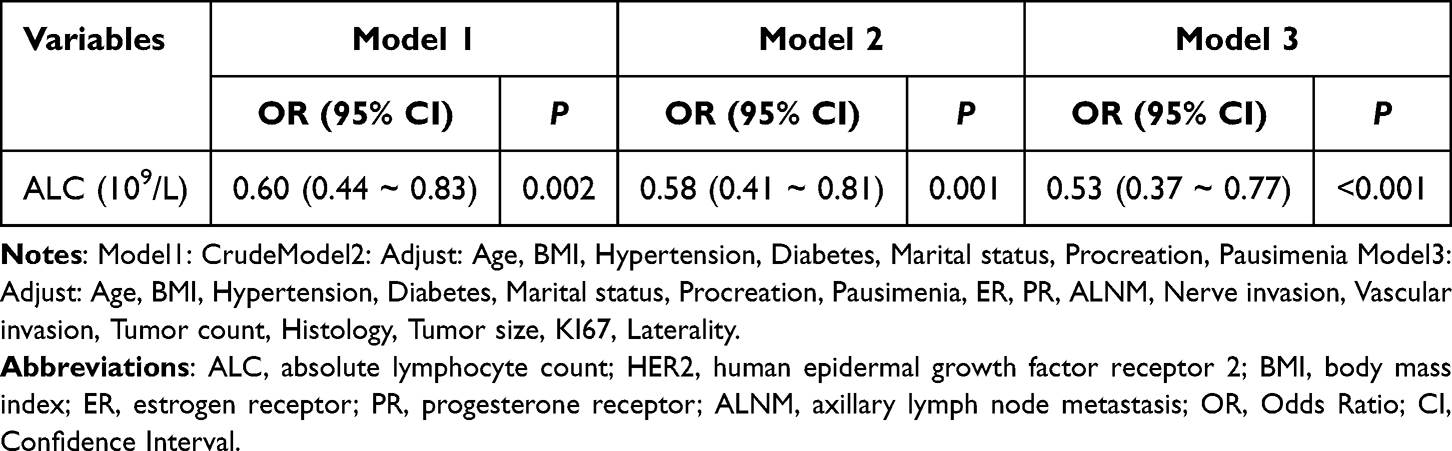 |
Table 2 Association Between Peripheral Blood Lymphocyte Count and HER2-Positive Status in Breast Cancer Patients |
In the unadjusted model (Model 1), higher ALC was significantly associated with lower odds of HER2 positivity (odds ratio [OR] = 0.60; 95% confidence interval [CI]: 0.44–0.83; P = 0.002).In Model 2, after adjustment for baseline demographic and clinical variables including age, body mass index (BMI), hypertension, diabetes, marital status, parity, and menopausal status, the association remained statistically significant (OR = 0.58; 95% CI: 0.41–0.81; P = 0.001).In Model 3, which further adjusted for tumor-related characteristics such as estrogen receptor (ER) status, progesterone receptor (PR) status, axillary lymph node metastasis (ALNM), perineural invasion, vascular invasion, tumor multiplicity, histological grade, tumor size, Ki67 index, and tumor laterality, the inverse association persisted (OR = 0.53; 95% CI: 0.37–0.77; P < 0.001).
These findings indicate that lower peripheral ALC is independently associated with an increased likelihood of HER2-positive breast cancer.
Feature Importance Ranking in Random Forest Models
To evaluate the relative importance of each variable in predicting HER2-positive status, we applied two feature importance metrics derived from the random forest model: Mean Decrease in Gini (MDI) and Mean Decrease in Accuracy (MDA).
As shown in Figure 2, ALC emerged as a consistently important predictor across both metrics. Specifically, ALC ranked second in importance based on MDI and sixth based on MDA, suggesting a meaningful but moderate contribution to HER2 status classification.
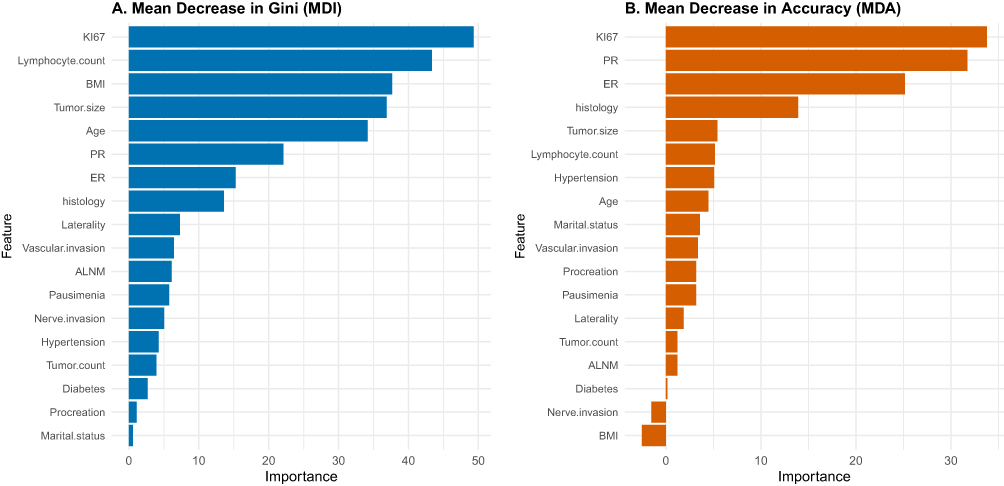 |
Figure 2 Variable importance rankings from the random forest model assessed using two metrics: (A) Mean Decrease in Gini (MDI) and (B) Mean Decrease in Accuracy (MDA). Absolute lymphocyte count (ALC) ranked second by MDI and sixth by MDA, suggesting a moderate and consistent contribution to the model in distinguishing HER2 status. |
Exploration of Nonlinear Relationships
To assess potential nonlinear associations between peripheral ALC and HER2-positive status, we incorporated restricted cubic spline (RCS) functions into fully adjusted logistic regression models.
As shown in Figure 3, no significant nonlinear association was detected (P for nonlinearity = 0.646). However, the overall association was statistically significant (P for overall trend = 0.003), indicating a significant linear inverse relationship: the risk of HER2 positivity progressively declined with increasing ALC levels.
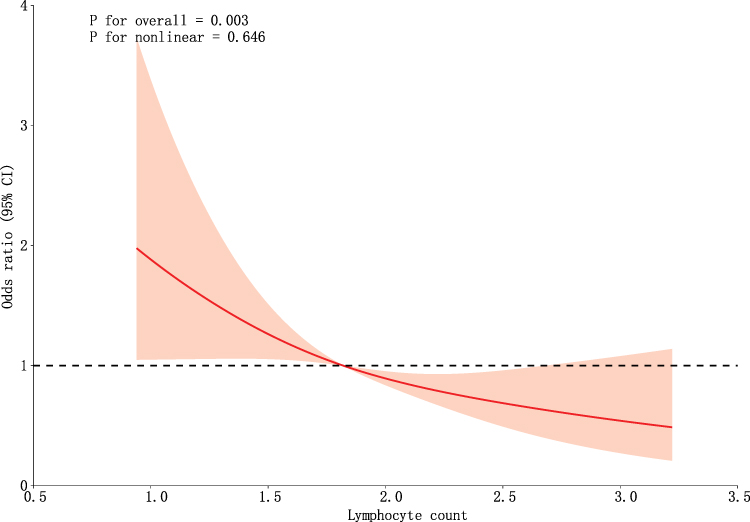 |
Figure 3 Association Between Peripheral Blood Lymphocyte Count and HER2-Positive Risk Modeled Using Restricted Cubic Splines. |
Subgroup Analysis Results
Subgroup analyses were conducted to further assess the robustness of the association between absolute lymphocyte count and HER2-positive status across different patient characteristics. Stratification variables included age, tumor laterality, histological grade, hypertension, diabetes, body mass index (BMI), menopausal status, and tumor size. As shown in Table 3, a significant inverse association between ALC and HER2 positivity was observed across most subgroups. No significant interactions were detected in any of the predefined subgroups (all P for interaction > 0.05), indicating that the inverse association between ALC and HER2-positive status remained consistent regardless of baseline clinical or tumor characteristics.
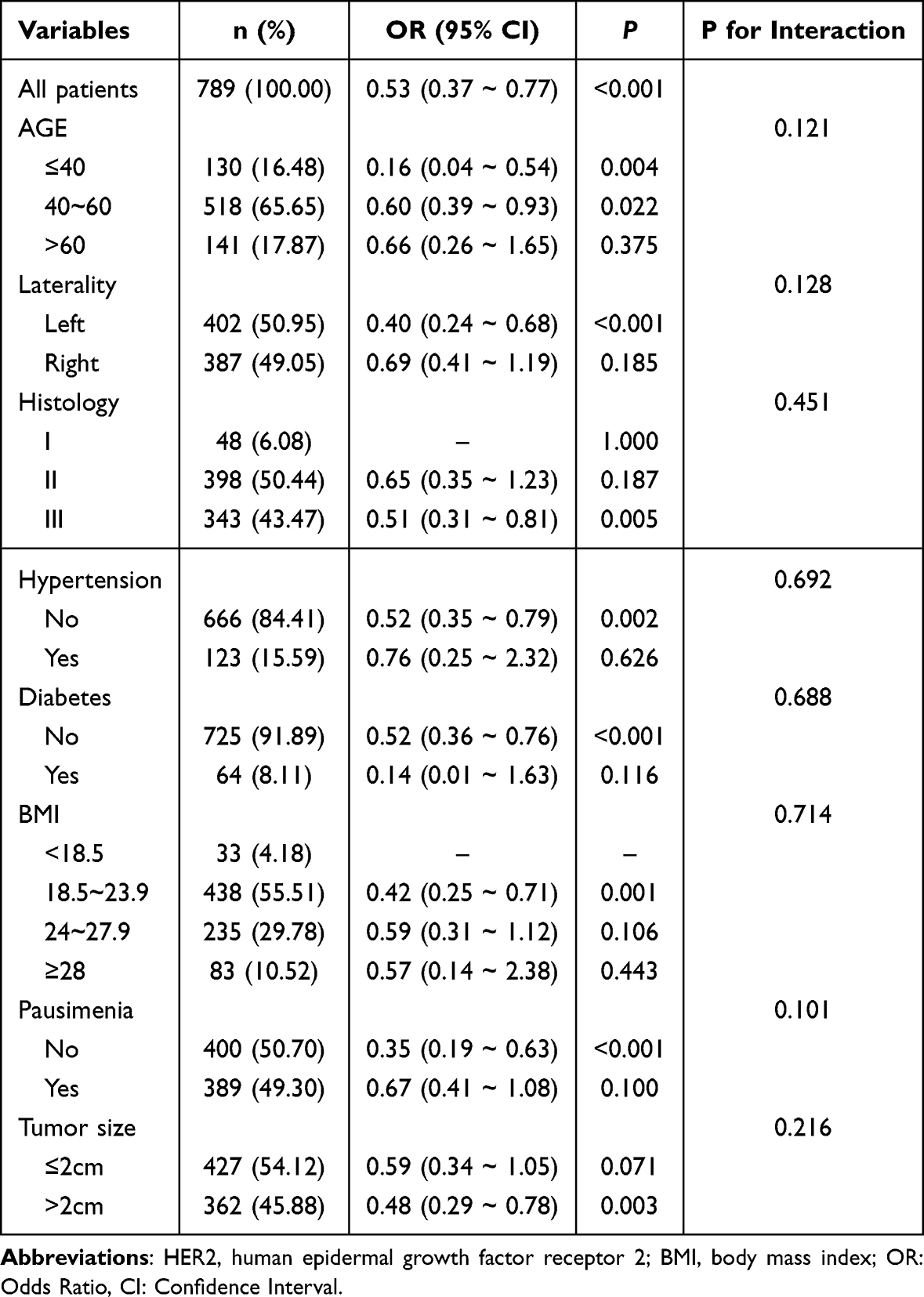 |
Table 3 Subgroup Analyses of the Association Between Peripheral Lymphocyte Count and HER2-Positive Status |
Association Between ERBB2 Expression and Immune Cell Infiltration in Breast Cancer Based on TIMER2.0
To further explore the relationship between ERBB2 (HER2) expression and the tumor immune microenvironment, we analyzed the infiltration levels of various immune cell subtypes in breast cancer tissues using the TIMER2.0 platform.
As detailed in Table 4, ERBB2 expression was negatively correlated with several immune cell subsets, including activated memory CD4⁺ T cells, Th1/Th2 helper T cells, and natural killer (NK) cells, suggesting that HER2 overexpression may be associated with suppression of adaptive immune responses. In contrast, significant positive correlations were observed with specific lymphocyte subsets, such as non-regulatory CD4⁺ T cells (ρ = 0.191, FDR = 5.1 × 10−8) and naive B cells (ρ = 0.141, FDR = 1.4 × 10−4), indicating potential selective recruitment or activation of these cell types in HER2-overexpressing tumors.
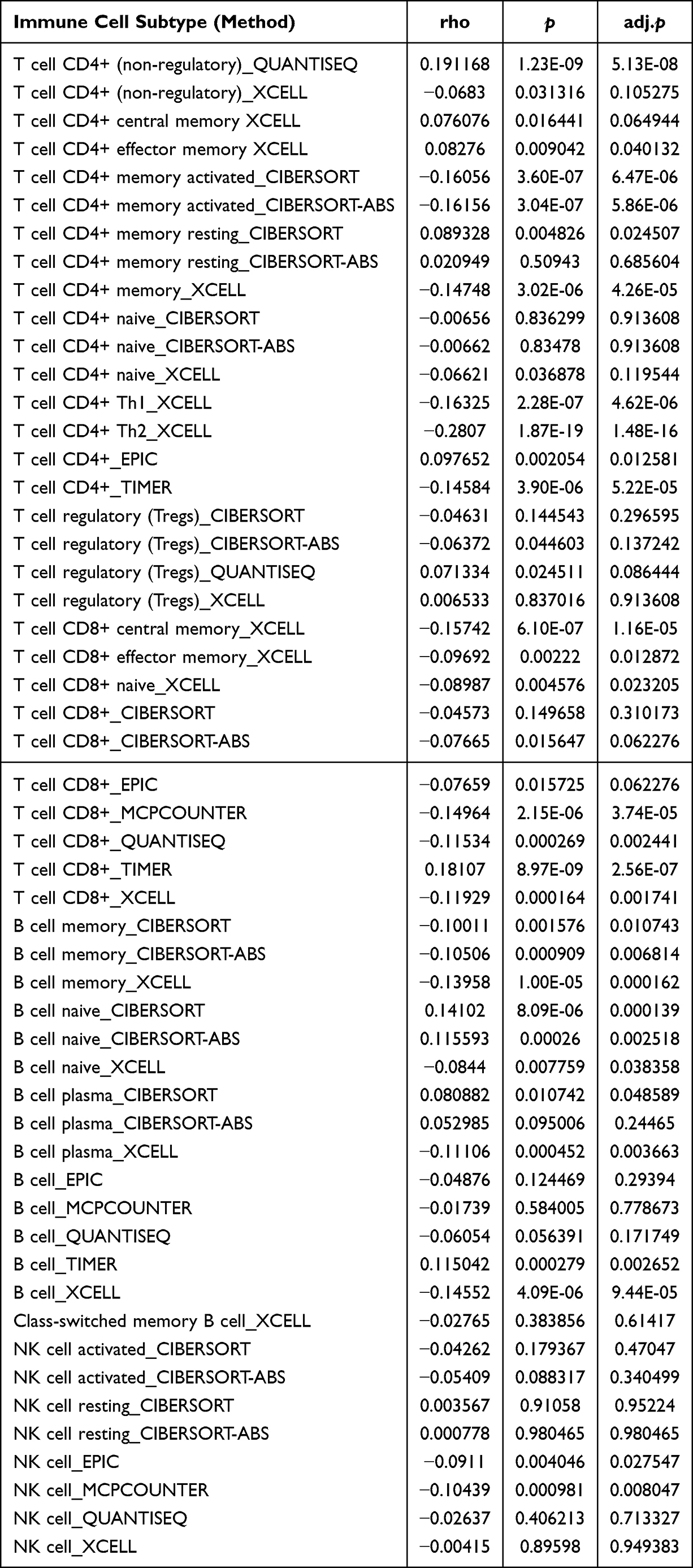 |
Table 4 Associations Between ERBB2 Expression and Immune Cell Infiltration (T Cells, B Cells, and NK Cells) in Breast Cancer from the TIMER2 Database |
Moreover, beyond the TIMER algorithm, most immune deconvolution methods consistently demonstrated a negative association between CD8⁺ T cell infiltration and ERBB2 expression, underscoring the robustness of this finding while also highlighting method-dependent variations in effect size.
In summary, HER2-overexpressing breast cancers display a complex immune infiltration landscape characterized by reduced helper and memory T cell populations alongside increased naive or non-effector lymphocytes. This dichotomous pattern may reflect ongoing immune remodeling and immune evasion mechanisms within the tumor microenvironment.
Discussion
This study revealed a robust and consistent inverse association between peripheral blood ALC and HER2-positive status in breast cancer patients. The relationship remained statistically significant across multiple analytical approaches, including multivariate logistic regression, random forest–based feature importance analysis, and restricted cubic spline (RCS) modeling. Furthermore, subgroup analyses demonstrated that this inverse association was consistently observed across various clinical and pathological subgroups, indicating that ALC may represent a reliable systemic immune indicator associated with HER2 expression. Importantly, this association reflects a population-level immunological trend rather than a discriminatory marker intended for individual-level clinical decision-making.
Analysis of the tumor immune microenvironment using the TIMER 2.0 platform further supported these findings. ERBB2 (HER2) expression was significantly negatively correlated with the infiltration of several key anti-tumor immune cell subsets, including CD8⁺ T cells, activated memory CD4⁺ T cells, Th1/Th2 cells, and natural killer (NK) cells. In contrast, HER2 expression showed a positive correlation with early-stage or non-effector lymphocytes, such as naive B cells and non-regulatory CD4⁺ T cells. These patterns suggest that HER2-overexpressing breast cancers may exist in a dual immunosuppressive state, characterized by both diminished systemic immune activity and reduced intratumoral immune infiltration.
ALC as a marker reflecting systemic immune status, is inherently non–tumor-specific. Previous studies have shown that ALC can be influenced by a variety of non-tumor–related factors, including acute infection or inflammatory responses, physiological or psychological stress (such as cortisol release), circadian rhythm variation, and other systemic conditions. Therefore, in tumor-related research, interpreting the relationship between ALC and molecular subtypes without adequate control for these confounding factors may result in biased conclusions. Accordingly, this study applied relatively stringent inclusion and exclusion criteria at the design stage to systematically minimize the influence of non-tumor–related factors that could substantially affect peripheral immune status. Specifically, patients with recent severe infection or inflammation, autoimmune diseases, immune system disorders, or major organ dysfunction were excluded. Under these controlled conditions, the observed association between ALC and HER2 status is more likely to reflect tumor-related immune characteristics rather than being predominantly driven by systemic inflammation or stress-related immune fluctuations.
At the mechanistic level, previous studies have shown that activation of the HER2 signaling pathway can stimulate STAT3, leading to the secretion of immunomodulatory cytokines such as interleukin-6 (IL-6) by tumor cells. This contributes to the establishment of an immunosuppressive tumor microenvironment (TME).15 In such an inflammation-driven TME, the effector functions of cytotoxic T cells and NK cells are impaired, while immunosuppressive populations such as regulatory T cells and myeloid-derived suppressor cells are enriched, ultimately resulting in depletion of tumor-infiltrating lymphocytes (TILs).16–18 Moreover, chronic inflammatory signaling may induce emergency myelopoiesis in the bone marrow, skewing hematopoiesis toward the myeloid lineage at the expense of lymphoid development, thereby reducing peripheral absolute lymphocyte count.19 In addition, HER2 signaling has been reported to suppress antiviral and antitumor immune responses through AKT1-mediated inhibition of the STING pathway.20 Supporting this, Fukai et al observed that HER2-high regions in HER2-positive gastric cancers were associated with reduced CD8⁺ TIL infiltration and downregulation of STING-related gene expression, suggesting a role for HER2 in dampening local immune activation via STING suppression.21 Similarly, Nadine et al reported that HER2-low breast tumors displayed lower TIL densities and limited immune responses compared to HER2-0 tumors, further corroborating the immunosuppressive landscape associated with HER2 expression.22
Several studies have reported that both ALC and TILs are associated with prognosis, pathological complete response (pCR), and treatment sensitivity in patients with HER2-positive breast cancer.23–25 However, whether ALC directly participates in the regulation of HER2 expression remains uncertain. Evidence from animal models suggests a potential link: NK cells and perforin have been shown to reduce the number of primary tumors in HER2/neu transgenic mice, indicating that immune surveillance may selectively suppress HER2-overexpressing tumor clones.26 Nonetheless, further research is required to clarify whether systemic immune status can actively influence HER2 expression levels in human cancers.
In summary, this study identifies a potential association between ALC and HER2 expression status, suggesting that HER2-positive breast cancer may be characterized by a dual immunosuppressive profile involving both systemic immune deficiency and a locally suppressed tumor immune microenvironment. These findings contribute to a more comprehensive understanding of the immunological landscape in HER2-driven tumors. Given its cost-effectiveness, accessibility, and widespread use in clinical practice, ALC holds promise as an adjunctive marker for assessing HER2 status and evaluating immune microenvironment activity at the population level.
However, this study has several limitations. First, as a single-center retrospective analysis, the findings reflect associations rather than causality, necessitating validation through prospective cohort studies and mechanistic investigations. Second, immune cell infiltration estimates derived from platforms such as TIMER 2.0 are based on bulk transcriptomic data and may not fully capture the spatial, functional, and phenotypic heterogeneity of the TME. Future research should incorporate advanced technologies such as single-cell RNA sequencing, spatial transcriptomics, and multiplex immunohistochemistry to more precisely delineate the relationship between peripheral ALC dynamics, HER2 pathway activation, and immunosuppressive mechanisms within the TME. Third, although this study employed relatively stringent inclusion and exclusion criteria to minimize the impact of non-tumor-related factors on peripheral blood absolute lymphocyte count, the retrospective study design inherently precludes complete control over perioperative short-term medication or individual stress-related immune fluctuations. Although all preoperative blood samples were collected in the morning, defining the blood collection time window as within two weeks prior to surgery may still permit some degree of preoperative stress-related variability. Accordingly, the clinical interpretation of ALC warrants caution, and future multicenter, prospective studies will be required to evaluate the reproducibility of these findings and to determine whether clinically actionable thresholds or risk stratification strategies can be defined.
Conclusion
This study demonstrated a consistent inverse association between peripheral blood absolute lymphocyte count (ALC) and HER2-positive status in breast cancer patients. This association remained statistically significant across multiple analytical approaches and was further supported by tumor immune microenvironment analyses using the TIMER 2.0 platform. Collectively, these findings indicate that HER2-positive breast cancer may be associated with a population-level immunological profile characterized by reduced systemic immune activity and suppressed intratumoral immune infiltration. Given its accessibility and routine clinical availability, peripheral ALC may serve as a complementary systemic immune indicator for contextual assessment of HER2-related immune characteristics at the population level.
Data Sharing Statement
The data are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This retrospective study was approved by the Clinical Research Ethics Committee, The Second Affiliated Hospital of Fujian Medical University (Approval No. 2025-106). All procedures were conducted in strict accordance with the principles of the Declaration of Helsinki. Due to the retrospective nature of the study and the complete removal of all patient-identifying information to ensure anonymity, the Ethics Committee granted a waiver of written informed consent. All data were analyzed in an anonymized manner. All operations in this study complied with relevant guidelines and regulatory requirements.
This study was conducted and reported in accordance with the RECORD (REporting of studies Conducted using Observational Routinely-collected health Data) guidelines.
Consent to Participate
Not applicable. Informed consent was waived by the Ethics Committee due to the retrospective design and full anonymization of data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no competing interests in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–12. doi:10.3322/caac.21834
2. Bartsch R, Cameron D, Ciruelos E, et al. Expert recommendations on treatment sequencing and challenging clinical scenarios in human epidermal growth factor receptor 2-positive (HER2-positive) metastatic breast cancer. Cancer Treat Rev. 2025;132:102853. doi:10.1016/j.ctrv.2024.102853
3. Li X, Zhang X, Yin S, Nie J. Challenges and prospects in HER2-positive breast cancer-targeted therapy. Crit Rev Oncol Hematol. 2025;207:104624. doi:10.1016/j.critrevonc.2025.104624
4. Randall M, Akers R, Rao R. A review of current and future antibody drug conjugates in breast cancer. Curr Treat Options Oncol. 2024;25(12):1506–1516. doi:10.1007/s11864-024-01276-3
5. Sun L, Jia X, Wang K, Li M. Unveiling the future of breast cancer therapy: cutting-edge antibody-drug conjugate strategies and clinical outcomes. Breast. 2024;78:103830. doi:10.1016/j.breast.2024.103830
6. Chaganty BKR, Qiu S, Gest A, et al. Trastuzumab upregulates PD-L1 as a potential mechanism of trastuzumab resistance through engagement of immune effector cells and stimulation of IFNγ secretion. Cancer Lett. 2018;430:47–56. doi:10.1016/j.canlet.2018.05.009
7. Salgado R, Denkert C, Campbell C, et al. Tumor-infiltrating lymphocytes and associations with pathological complete response and event-free survival in her2-positive early-stage breast cancer treated with lapatinib and trastuzumab: a secondary analysis of the neoALTTO trial. JAMA Oncol. 2015;1(4):448–454. doi:10.1001/jamaoncol.2015.0830
8. Luz P, Ramos S, Oliveira MJ, Costa JG, Saraiva N, Fernandes AS. Interaction between redox regulation, immune activation, and response to treatment in HER2+ breast cancer. Redox Biol. 2025;82:103609. doi:10.1016/j.redox.2025.103609
9. Finkelman BS, Zhang H, Hicks DG, Rimm DL, Turner BM. Tumor infiltrating lymphocytes in breast cancer: a narrative review with focus on analytic validity, clinical validity, and clinical utility. Hum Pathol. 2025;162:105866. doi:10.1016/j.humpath.2025.105866
10. Schlam I, Loi S, Salgado R, Swain SM. Tumor-infiltrating lymphocytes in HER2-positive breast cancer: potential impact and challenges. ESMO Open. 2025;10(2):104120. doi:10.1016/j.esmoop.2024.104120
11. Obeagu EI, Obeagu GU. Lymphocyte infiltration in breast cancer: a promising prognostic indicator. Medicine. 2024;103(49):e40845. doi:10.1097/MD.0000000000040845
12. Feng F, Zheng G, Wang Q, et al. Low lymphocyte count and high monocyte count predicts poor prognosis of gastric cancer. BMC Gastroenterol. 2018;18(1):148. doi:10.1186/s12876-018-0877-9
13. Jimbo H, Horimoto Y, Ishizuka Y, et al. Absolute lymphocyte count decreases with disease progression and is a potential prognostic marker for metastatic breast cancer. Breast Cancer Res Treat. 2022;196(2):291–298. doi:10.1007/s10549-022-06748-4
14. Li T, Fu J, Zeng Z, et al. TIMER2.0 for analysis of tumor-infiltrating immune cells. Nucleic Acids Res. 2020;48(W1):W509–w514. doi:10.1093/nar/gkaa407
15. Hartman ZC, Yang XY, Glass O, et al. HER2 overexpression elicits a proinflammatory IL-6 autocrine signaling loop that is critical for tumorigenesis. Cancer Res. 2011;71(13):4380–4391. doi:10.1158/0008-5472.CAN-11-0308
16. Chen C, Wang Z, Ding Y, Qin Y. Tumor microenvironment-mediated immune evasion in hepatocellular carcinoma. Front Immunol. 2023;14:1133308. doi:10.3389/fimmu.2023.1133308
17. Yu J, Fu L, Wu R, et al. Immunocytes in the tumor microenvironment: recent updates and interconnections. Front Immunol. 2025;16:1517959. doi:10.3389/fimmu.2025.1517959
18. Liu C, Yin Q, Wu Z, et al. Inflammation and immune escape in ovarian cancer: pathways and therapeutic opportunities. J Inflamm Res. 2025;18:895–909. doi:10.2147/JIR.S503479
19. Aliazis K, Yenyuwadee S, Phikulsod P, Boussiotis VA. Emergency myelopoiesis in solid cancers. Br J Haematol. 2024;205(3):798–811. doi:10.1111/bjh.19656
20. Wu S, Zhang Q, Zhang F, et al. HER2 recruits AKT1 to disrupt STING signalling and suppress antiviral defence and antitumour immunity. Nat Cell Biol. 2019;21(8):1027–1040. doi:10.1038/s41556-019-0352-z
21. Fukai S, Nakajima S, Saito M, et al. Down-regulation of stimulator of interferon genes (STING) expression and CD8(+) T-cell infiltration depending on HER2 heterogeneity in HER2-positive gastric cancer. Gastric Cancer. 2023;26(6):878–890. doi:10.1007/s10120-023-01417-x
22. van den Ende NS, Smid M, Timmermans A, et al. HER2-low breast cancer shows a lower immune response compared to HER2-negative cases. Sci Rep. 2022;12(1):12974. doi:10.1038/s41598-022-16898-6
23. Che YQ, Zhang Y, Wang D, Liu HY, Shen D, Luo Y. Baseline lymphopenia: a predictor of poor outcomes in her2 positive metastatic breast cancer treated with trastuzumab. Drug Des Devel Ther. 2019;13:3727–3734. doi:10.2147/DDDT.S212610
24. Sang B, Fan Y, Wang X, et al. The prognostic value of absolute lymphocyte count and neutrophil-to-lymphocyte ratio for patients with metastatic breast cancer: a systematic review and meta-analysis. Front Oncol. 2024;14:1360975. doi:10.3389/fonc.2024.1360975
25. Denkert C, von Minckwitz G, Darb-Esfahani S, et al. Tumour-infiltrating lymphocytes and prognosis in different subtypes of breast cancer: a pooled analysis of 3771 patients treated with neoadjuvant therapy. Lancet Oncol. 2018;19(1):40–50. doi:10.1016/S1470-2045(17)30904-X
26. Street SE, Zerafa N, Iezzi M, et al. Host perforin reduces tumor number but does not increase survival in oncogene-driven mammary adenocarcinoma. Cancer Res. 2007;67(11):5454–5460. doi:10.1158/0008-5472.CAN-06-4084
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.