Back to Journals » International Journal of Women's Health » Volume 18
Association Between MTHFR Gene Polymorphisms and Subclinical Hypothyroidism in Early Pregnancy: A Retrospective Case-Control Study
Authors Liu L, Wang C, Chen X, Zhu Y, Jiao J, Li L, Huang C
Received 22 April 2026
Accepted for publication 11 June 2026
Published 18 June 2026 Volume 2026:18 619071
DOI https://doi.org/10.2147/IJWH.S619071
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Liyang Liu, Cheng Wang, Xia Chen, Yulu Zhu, Jie Jiao, Lei Li, Chunyan Huang
Department of Obstetrics and Gynecology, Affiliated Hospital of Jiangnan University, Wuxi, 214000, People’s Republic of China
Correspondence: Chunyan Huang, Department of Obstetrics and Gynecology, Affiliated Hospital of Jiangnan University, No. 1000 Hefeng Road, Binhu District, Wuxi, Jiangsu, 214000, People’s Republic of China, Email [email protected]
Objective: To investigate the association between methylenetetrahydrofolate reductase (MTHFR) gene polymorphisms and subclinical hypothyroidism (SCH) in early pregnancy.
Methods: This retrospective case-control study included 100 pregnant women diagnosed with SCH and 300 pregnant women with normal thyroid function who attended the Affiliated Hospital of Jiangnan University between June 2021 and December 2024. MTHFR C677T and A1298C polymorphisms were detected using polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP). Thyroid function indicators, including thyroid-stimulating hormone (TSH), free triiodothyronine (FT3), and free thyroxine (FT4), were measured. Genotype and allele distributions were compared, and dominant, recessive, and additive genetic models were analyzed. Multivariate logistic regression analysis was performed to identify factors associated with SCH.
Results: The proportions of abnormal pre-pregnancy body mass index (BMI) and anemia history were significantly higher in the SCH group than in the control group (P< 0.05). Genotype distributions of both MTHFR loci conformed to Hardy–Weinberg equilibrium. Significant differences were observed in genotype and allele distributions of the C677T locus between the two groups (P< 0.05), whereas no significant differences were found for the A1298C locus (P> 0.05). Significant associations were observed under dominant, recessive, and additive models for the C677T polymorphism (P< 0.05). Pregnant women with the TT genotype showed higher TSH levels than those with the CC and CT genotypes (P< 0.05). Multivariate logistic regression analysis identified the C677T T allele, abnormal pre-pregnancy BMI, and anemia history as factors associated with SCH (P< 0.05).
Conclusion: The MTHFR C677T polymorphism is associated with SCH in early pregnancy, whereas no significant association was observed for the A1298C polymorphism. Abnormal pre-pregnancy BMI and anemia history may also be associated with increased SCH risk. Further prospective multicenter studies are required to validate these findings.
Keywords: methylenetetrahydrofolate reductase, gene polymorphism, early pregnancy, subclinical hypothyroidism, folate metabolism
Introduction
Thyroid functional status during pregnancy has an important impact on maternal health and fetal development, and with the development of perinatal medicine, thyroid dysfunction during pregnancy has gradually attracted increasing attention.1 Among these conditions, subclinical hypothyroidism (SCH) in early pregnancy is a relatively common type of thyroid dysfunction and is easily overlooked because of its insidious clinical manifestations.2 However, studies3,4 have shown that SCH may be associated with adverse pregnancy outcomes such as miscarriage, preterm birth, hypertensive disorders of pregnancy, and abnormal fetal neurodevelopment, making its early identification and intervention of important clinical significance. At present, the pathogenesis of SCH during pregnancy has not been fully clarified. In addition to insufficient or excessive iodine intake, autoimmune factors, and environmental factors, the role of individual genetic background in disease susceptibility has gradually received attention. In recent years, with the development of molecular genetics, the role of gene polymorphisms in various endocrine and metabolic diseases has been gradually revealed,5–7 providing a new direction for further understanding disease mechanisms.
As an important component of one-carbon metabolism, folate metabolism plays a key role in DNA synthesis, repair, and methylation regulation.8,9 The demand for folate increases significantly during pregnancy, and changes in folate metabolic status not only affect fetal development but may also participate in the occurrence of various pregnancy-related diseases.10,11 Methylenetetrahydrofolate reductase (MTHFR) is a key enzyme in the folate metabolic pathway, and its gene polymorphisms may lead to reduced enzyme activity, thereby affecting folate metabolic efficiency and increasing homocysteine (Hcy) levels.12 Previous studies13,14 have shown that polymorphisms at the C677T and A1298C loci of the MTHFR gene are closely associated with a variety of diseases such as cardiovascular diseases and pregnancy complications. However, studies on the relationship between MTHFR gene polymorphisms and SCH during pregnancy remain relatively limited, and the reported findings have been inconsistent. Some studies have suggested that the MTHFR C677T polymorphism, particularly the TT genotype, may be associated with elevated thyroid-stimulating hormone (TSH) levels and an increased risk of thyroid dysfunction, whereas other studies failed to identify significant associations between MTHFR polymorphisms and thyroid function abnormalities.15,16 In addition, evidence regarding the role of different polymorphic loci, particularly A1298C, remains limited and inconclusive. These discrepancies may be related to differences in study populations, sample sizes, ethnic backgrounds, thyroid function assessment criteria, and adjustment for potential confounding factors.
Furthermore, thyroid autoimmunity has been recognized as an important contributor to SCH during pregnancy. The interaction among autoimmune factors, genetic susceptibility, iodine nutrition, and environmental exposures may jointly influence thyroid function and pregnancy outcomes.17 Based on this, the present study took pregnant women in early pregnancy from our hospital as the study subjects to analyze the correlation between polymorphisms at the C677T and A1298C loci of the MTHFR gene and SCH, aiming to provide a reference for further clarifying its potential mechanisms and clinical risk assessment.
Materials and Methods
General Information
Pregnant women who attended the Department of Obstetrics and Gynecology of our hospital and completed relevant examinations from June 2021 to December 2024 were selected as the study subjects. The primary objective of this study was to evaluate the association between MTHFR C677T and A1298C polymorphisms and the occurrence of subclinical hypothyroidism (SCH) in early pregnancy. A retrospective case-control study design was adopted, and participants were divided into the SCH group and the control group according to thyroid function test results. The SCH group included 100 pregnant women diagnosed with SCH in early pregnancy; during the same period, 300 pregnant women with normal thyroid function in early pregnancy were selected in order of visit as the control group. All study subjects were in early pregnancy (gestational age ≤12 weeks) and underwent thyroid function testing and MTHFR gene polymorphism testing during early pregnancy.
The study period from June 2021 to December 2024 was chosen to ensure an adequate sample size and to include multiple annual cohorts for consistency in clinical and laboratory procedures. The control group was selected in order of visit due to the retrospective nature of the study; this approach may introduce selection bias, which is acknowledged as a study limitation. This study was a single-center retrospective study. All study subjects were derived from existing clinical data, and no additional interventions were performed. The study protocol was approved by the Medical Ethics Committee of the Affiliated Hospital of Jiangnan University, Wuxi, China (Ethics approval number: FCK23-JY06) and complied with the principles of the Declaration of Helsinki. All study procedures were conducted in accordance with relevant ethical standards. As this was a retrospective study using anonymized clinical data, informed consent was waived by the ethics committee. Participants with incomplete clinical records or missing genetic testing results were excluded according to the predefined exclusion criteria. This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement. The study flowchart is shown in Figure 1.
 |
Figure 1 Flowchart of patient selection and study design. |
Inclusion and Exclusion Criteria
Inclusion Criteria
(1) The SCH group met the diagnostic criteria of the 2017 American Thyroid Association (ATA) guidelines for the diagnosis of thyroid disease during pregnancy;18 (2) pregnant women who established medical records and underwent regular prenatal examinations in our hospital; (3) singleton pregnancy; (4) gestational age ≤12 weeks; (5) complete clinical data, including thyroid function indicators and MTHFR gene testing results; (6) normal thyroid function in the control group.
Exclusion Criteria
(1) Previous definite diagnosis of hypothyroidism, hyperthyroidism, thyroiditis, or other thyroid diseases; (2) presence of significant dysfunction of major organs such as liver, kidney, or cardiovascular and cerebrovascular systems; (3) comorbid diabetes mellitus, autoimmune diseases, malignant tumors, or other severe systemic diseases; (4) multiple pregnancy; (5) use of levothyroxine sodium, antithyroid drugs, folate metabolism-related interventions, or other medications that may affect thyroid function or folate metabolism before or during early pregnancy; (6) recent infection, trauma, or stress conditions; (7) incomplete clinical data or missing gene testing results.
Observation Indicators and Detection Methods
General Clinical Data
General clinical data of the two groups of pregnant women were collected and compared, including age, gestational age, pre-pregnancy body mass index (BMI), gravidity, parity, history of anemia, adverse pregnancy history, and family history. BMI was calculated as body weight (kg)/height2 (m2), and according to clinical research requirements, it was categorized as normal or abnormal, with BMI <18.5 kg/m2 or >24.0 kg/m2 defined as abnormal.
Thyroid Function Testing
All study subjects underwent venous blood collection from the elbow vein in the early morning under fasting conditions during early pregnancy, with fasting for 8–12 hours prior to blood sampling. After sample collection, serum was separated by routine centrifugation, and thyroid function indicators, including thyroid-stimulating hormone (TSH), free triiodothyronine (FT3), and free thyroxine (FT4), were measured using chemiluminescence immunoassay (CLIA). All tests were performed in strict accordance with the reagent instructions and instrument operating procedures, and internal quality control was implemented to ensure the accuracy and stability of the results.
Detection of MTHFR Gene Polymorphisms
Polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP) was used to detect polymorphisms at the C677T and A1298C loci of the MTHFR gene. Peripheral venous anticoagulated blood was collected, and genomic DNA was extracted from peripheral blood leukocytes. After PCR amplification, the products were digested with corresponding restriction enzymes and separated by agarose gel electrophoresis. Genotypes were determined based on band patterns. The C677T locus was classified into CC, CT, and TT genotypes, and the A1298C locus into AA, AC, and CC genotypes. Genotype frequencies and allele frequencies were also calculated. To ensure reliability, a portion of samples was randomly selected for repeated testing.
Genetic Model Analysis
The association between polymorphisms at the MTHFR C677T locus and the occurrence of SCH was analyzed under dominant (CT+TT vs CC), recessive (TT vs CC+CT), and additive (CC, CT, TT) models; corresponding genetic models were also applied to the A1298C locus.
Multivariate Analysis
Taking the occurrence of SCH as the dependent variable, variables with statistical significance in univariate analysis as well as clinically relevant factors were included in a multivariate Logistic regression model. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to identify independent influencing factors for SCH occurrence.
Quality Control
To reduce bias and improve the reliability of the results, the following measures were adopted: (1) unified inclusion and exclusion criteria were applied to strictly screen study subjects; (2) all subjects were derived from the same period and the same medical institution to reduce differences related to region and testing platforms; (3) thyroid function tests and gene detection were conducted by the hospital laboratory under unified standards; (4) two researchers independently performed data entry and verification, and missing or abnormal values were rechecked; (5) Hardy–Weinberg equilibrium testing was conducted before statistical analysis to assess sample representativeness; (6) relevant confounding factors were included in multivariate analysis for adjustment to minimize bias.
Statistical Methods
Statistical analysis was performed using SPSS 26.0 software. Measurement data were tested for normality; data with normal distribution were expressed as mean ± SD and compared between groups using independent sample t-tests, and among multiple groups using analysis of variance; non-normally distributed data were expressed as median and interquartile range and compared using rank-sum tests. Count data were expressed as number of cases and percentages, and compared using the χ2-test. Hardy–Weinberg equilibrium testing was used to assess whether the genotype distributions of MTHFR conformed to genetic equilibrium in both groups. As a retrospective case-control study, no formal a priori sample size calculation was performed. The final sample size was determined by the number of eligible participants who met the inclusion criteria during the study period, which is comparable to previous genetic association studies in SCH and pregnancy populations. Multivariate Logistic regression analysis was used to identify independent influencing factors for SCH occurrence, with adjustment for potential confounders including age, gestational age, gravidity, parity, pre-pregnancy BMI, and anemia history. Due to the retrospective design, serum folate, vitamin B12, homocysteine, and DNA methylation markers were not measured; therefore, the biological mechanism linking MTHFR polymorphisms and SCH remains speculative. A P value <0.05 was considered statistically significant.
Results
Comparison of General Clinical Characteristics Between the Two Groups of Pregnant Women
The distributions of basic demographic and reproductive indicators, including age, gestational age, gravidity, and parity, were generally comparable between the two groups, with no statistically significant differences (P>0.05), indicating good baseline comparability. Further analysis showed that the proportion of abnormal pre-pregnancy BMI was significantly higher in the SCH group than in the control group (38.00% vs 24.33%, χ2=6.986, P=0.008). In addition, the prevalence of a history of anemia was also significantly higher in the SCH group (29.00% vs 17.67%, χ2=5.910, P=0.015). Detailed results are shown in Table 1.
 |
Table 1 Comparison of General Clinical Characteristics Between the Two Groups of Pregnant Women |
Comparison of MTHFR Genotype and Allele Distribution Between the Two Groups
The Hardy–Weinberg equilibrium (HWE) test demonstrated that the genotype distributions of the MTHFR C677T and A1298C loci were consistent with genetic equilibrium in both the SCH and control groups (C677T: χ2=0.63, P=0.43 in the SCH group; χ2=1.79, P=0.18 in the control group; A1298C: χ2=2.04, P=0.15 in the SCH group; χ2=2.95, P=0.086 in the control group), indicating satisfactory population representativeness and genetic stability of the study samples.
At the C677T locus, significant differences in genotype and allele distributions were observed between the two groups. The proportion of the TT genotype was higher in the SCH group than in the control group (26.00% vs 16.00%), and the frequency of the T allele was also significantly higher in the SCH group (49.00% vs 37.67%) (both P<0.05). In contrast, no statistically significant differences were identified in genotype or allele distributions at the A1298C locus (P>0.05). Detailed results are shown in Tables 2 and 3.
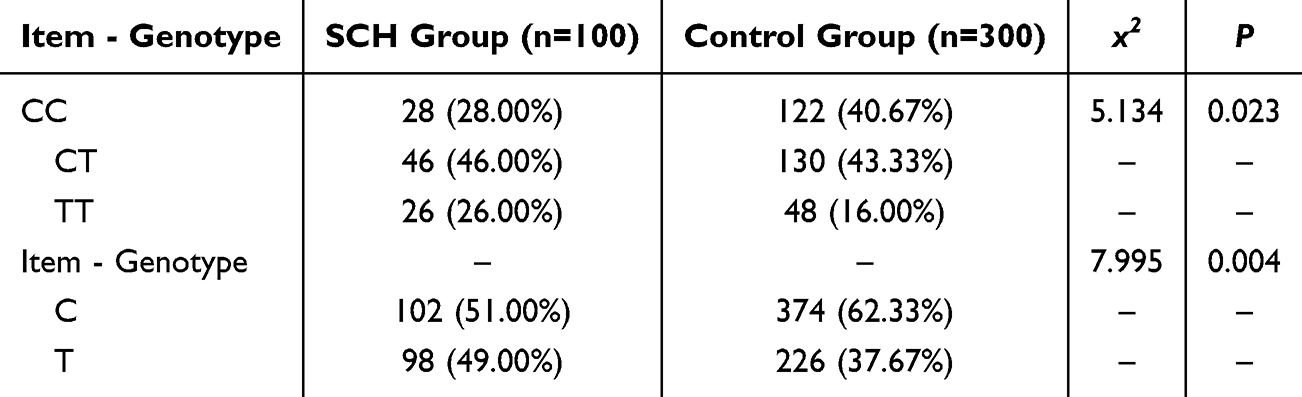 |
Table 2 Comparison of Genotype and Allele Distribution of MTHFR C677T Locus Between the Two Groups |
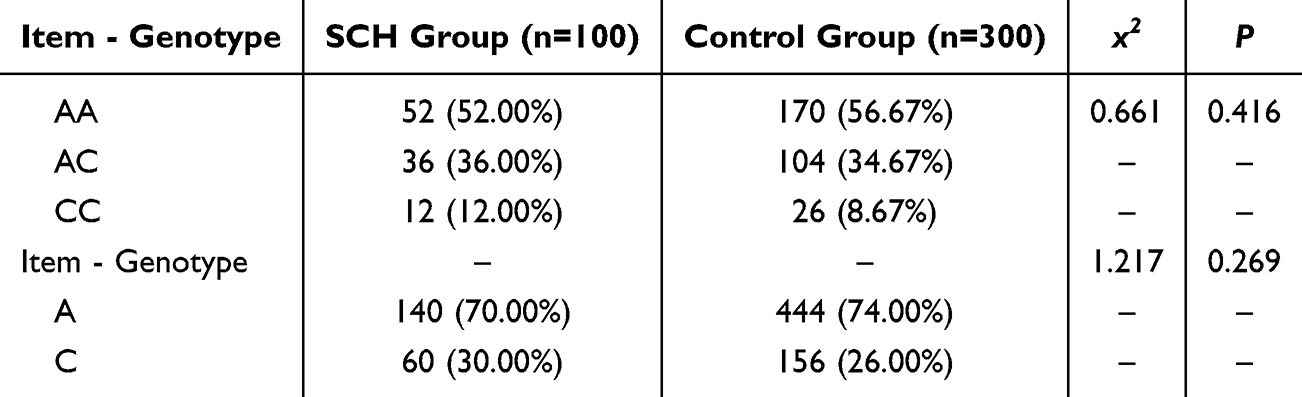 |
Table 3 Comparison of Genotype and Allele Distribution of MTHFR A1298C Locus Between the Two Groups |
Genetic Model Analysis
Further analysis under different genetic models demonstrated significant associations between the MTHFR C677T polymorphism and SCH. Compared with the CC genotype, the CT genotype was associated with an OR of 1.54 (95% CI: 0.91–2.62), whereas the TT genotype was associated with an OR of 2.36 (95% CI: 1.26–4.43). Under the dominant model (CT+TT vs CC), the OR was 1.76 (95% CI: 1.08–2.89), and under the recessive model (TT vs CC+CT), the OR was 1.84 (95% CI: 1.07–3.18). These findings suggest that the presence of the T allele was significantly associated with SCH in this study population. Detailed results are shown in Table 4.
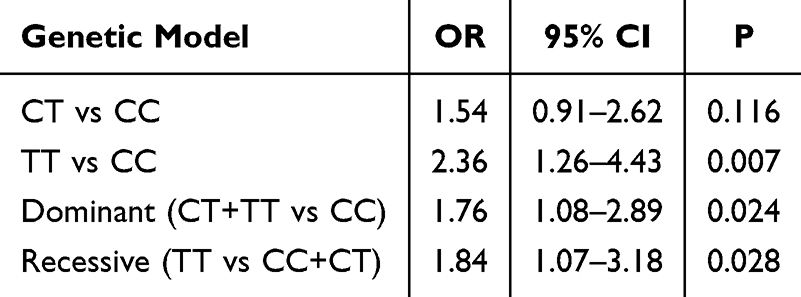 |
Table 4 Association Between MTHFR C677T Polymorphism and SCH Under Different Genetic Models |
Comparison of Thyroid Function Among Different Genotypes
Comparison of thyroid function indicators among different C677T genotypes showed significant differences in TSH levels (F=9.842, P<0.001). TSH levels were highest in individuals with the TT genotype, followed by those with the CT genotype and CC genotype. No significant differences were observed in FT3 or FT4 levels among the three genotype groups (P>0.05). Detailed results are shown in Table 5.
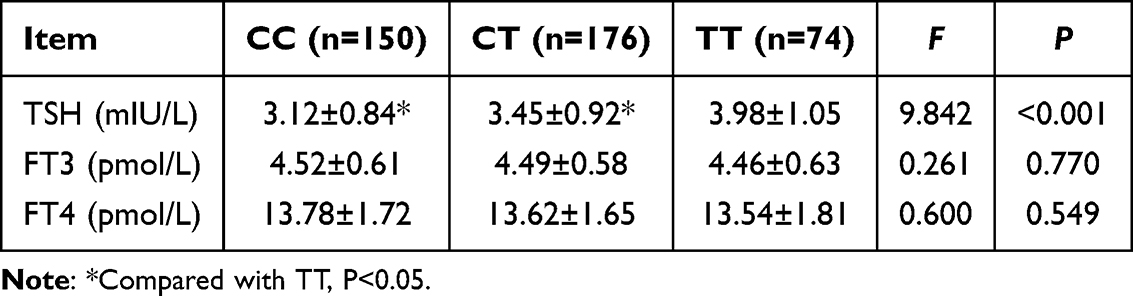 |
Table 5 Comparison of Thyroid Function Among Different C677T Genotypes |
Multivariate Logistic Regression Analysis of Factors Associated with SCH
Using the occurrence of SCH as the dependent variable, variables with statistical significance in univariate analysis were included in a multivariate Logistic regression model. The results showed that the T allele at the MTHFR C677T locus, abnormal pre-pregnancy BMI, and a history of anemia were independently associated with SCH (all P<0.05). Among these factors, carriage of the T allele was significantly associated with SCH (OR=2.277, 95% CI: 1.273–4.059, P=0.006). In addition, abnormal pre-pregnancy BMI (OR=1.902, 95% CI: 1.142–3.181, P=0.014) and a history of anemia (OR=1.798, 95% CI: 1.053–3.067, P=0.032) were also associated with SCH. Detailed results are shown in Table 6.
 |
Table 6 Multivariate Logistic Regression Analysis of Factors Associated with SCH |
Discussion
Early pregnancy is a critical period for embryonic organ formation and nervous system development. During this stage, fetal thyroid function is not yet fully established, and the fetus relies heavily on maternal thyroid hormone supply. Therefore, even mild abnormalities in maternal thyroid function may adversely affect pregnancy outcomes and fetal development.19 Due to its subtle clinical manifestations and mild laboratory changes, SCH is easily overlooked in clinical practice. However, previous studies20,21 have suggested that SCH during pregnancy is associated with adverse outcomes such as miscarriage, preterm birth, hypertensive disorders of pregnancy, and impaired fetal neurodevelopment. Therefore, clarifying its risk factors is clinically important. In this study, pregnant women in early pregnancy were selected to investigate the relationship between polymorphisms of the folate metabolism-related enzyme MTHFR and the occurrence of SCH. The results showed that the C677T polymorphism of the MTHFR gene was associated with the occurrence of SCH in early pregnancy, with the T allele potentially increasing the risk of SCH, whereas no significant association was observed for the A1298C locus. In addition, abnormal pre-pregnancy BMI and a history of anemia were identified as independent risk factors for SCH. These findings suggest that SCH in early pregnancy may be associated with genetic background, nutritional and metabolic status, and maternal physiological changes.
We first compared the general clinical characteristics of the two groups. No significant differences were observed in age, gestational age, gravidity, parity, adverse pregnancy history, or family history between the two groups, indicating good baseline comparability. The proportions of abnormal pre-pregnancy BMI and history of anemia were higher in the SCH group and remained significant in multivariate analysis, suggesting that maternal nutritional and metabolic status may be associated with SCH in early pregnancy. Pregnancy is a high-metabolic state that increases the requirements for energy, micronutrients, and endocrine homeostasis.22,23 Low pre-pregnancy BMI may indicate insufficient nutritional reserves, often accompanied by deficiencies in folate, iron, and vitamins; conversely, high BMI is often associated with insulin resistance, chronic low-grade inflammation, and lipid metabolism disorders. These changes may be associated with SCH through effects on the hypothalamic–pituitary–thyroid (HPT) axis, thyroid hormone metabolism, and stress responses.24,25 The association between anemia and SCH may also be biologically plausible. Anemia, particularly nutrition-related anemia, often reflects deficiencies in iron, folate, and B vitamins, which are closely involved not only in folate metabolism but also in the synthesis, transport, and metabolism of thyroid hormones.26 Therefore, anemia may reflect broader nutritional and metabolic insufficiency rather than only a hematological abnormality. Previous studies27,28 have also reported associations between abnormal body weight, malnutrition, anemia, and thyroid dysfunction during pregnancy, and the findings of this study are consistent with these observations.
In the genetic analysis, the genotype distributions of the MTHFR C677T and A1298C loci were consistent with Hardy–Weinberg equilibrium. The C677T genotype distribution differed significantly between the two groups, with a higher T allele frequency in the SCH group, suggesting that the C677T polymorphism may be associated with SCH susceptibility in early pregnancy. MTHFR is a key enzyme in the folate metabolism pathway, catalyzing the conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate, which serves as an important methyl donor in the remethylation of Hcy.29 The C677T locus is one of the most common and functionally significant polymorphic sites in the MTHFR gene. Studies30 have shown that the T allele can reduce enzyme activity, leading to decreased folate utilization efficiency and elevated Hcy levels. Abnormal folate metabolism may affect DNA synthesis, methylation, oxidative stress, and endothelial function. These changes may influence thyroid microenvironment and hormone regulation.31 In early pregnancy, increased requirements for folate and thyroid hormones may make thyroid regulation more susceptible to metabolic disturbances. Therefore, although causality cannot be inferred, the C677T polymorphism may be associated with thyroid dysfunction susceptibility during pregnancy. In contrast, no significant differences were observed in genotype or allele distributions at the A1298C locus between the two groups, suggesting a relatively limited association with SCH in early pregnancy. This finding is consistent with the variable functional effects of different MTHFR loci. Previous studies32,33 have indicated that although the A1298C polymorphism can affect MTHFR enzyme activity, its impact is generally weaker than that of C677T and has a relatively smaller effect on folate metabolism and Hcy levels. The role of A1298C may also vary across populations and disease contexts. The absence of a significant association for A1298C suggests that C677T may be more closely related to SCH in this population. Further studies with larger sample sizes and diverse populations are needed to clarify the role of the A1298C locus in thyroid dysfunction during pregnancy.
Genetic model analysis further showed that the C677T polymorphism was associated with SCH under dominant, recessive, and additive models. The dominant and recessive models suggest that both T allele carriage and the TT genotype may be associated with SCH. The additive model suggests a possible allele-dose association. These findings are consistent with the functional characteristics of the MTHFR C677T polymorphism. The CT genotype is generally associated with partial reduction of enzyme activity, whereas the TT genotype may lead to a more pronounced decrease in MTHFR activity.34 These findings provide additional statistical support for the association between C677T and SCH.
We further explored this association using thyroid function indicators. The results showed that TSH levels differed significantly among different C677T genotypes, with the TT genotype exhibiting higher TSH levels than the CC and CT genotypes, while no significant differences were observed in FT3 and FT4 levels. This finding is consistent with the pathophysiological characteristics of SCH. The TT genotype was associated with elevated TSH levels without corresponding decreases in FT3 or FT4, suggesting a possible relationship with early HPT-axis feedback changes while peripheral thyroid hormone levels remain relatively stable This suggests that C677T may serve as a potential risk indicator for SCH rather than a marker of disease severity. Previous studies35 have similarly reported an association between the MTHFR C677T polymorphism, particularly the TT genotype, and elevated TSH levels, and the findings of this study are generally consistent with these trends.
In the multivariate Logistic regression analysis, the T allele at the MTHFR C677T locus, abnormal pre-pregnancy BMI, and history of anemia were independently associated with SCH in early pregnancy. This suggests that the association between C677T and SCH persisted after adjustment for clinical factors such as abnormal BMI and anemia. The associations of abnormal BMI and anemia further support the potential combined influence of genetic, metabolic, and nutritional factors.36 From a clinical perspective, these findings provide important implications. Pregnant women with abnormal pre-pregnancy BMI, anemia history, or T allele carriage may require closer thyroid function monitoring. Enhanced thyroid monitoring and nutritional assessment may facilitate early identification and intervention.
From a mechanistic perspective, abnormal folate metabolism may partly explain the observed association between MTHFR polymorphisms and SCH. Reduced MTHFR activity leads to decreased production of methyl donors and elevated Hcy levels, which may affect thyroid function through multiple pathways. Elevated Hcy, endothelial dysfunction, oxidative stress, and altered DNA methylation may potentially affect thyroid tissue homeostasis and hormone regulation.37–39 However, because folate, vitamin B12, Hcy, and methylation markers were not measured in this study, these mechanisms remain speculative and require further validation.
This study has several limitations. (1) This was a single-center retrospective case-control study; although a single institution reduces variability in testing platforms and clinical management, the generalizability of the findings may be limited. (2) The sample size was moderate, and the statistical power may be insufficient to detect subtle associations for loci with weaker effects, such as A1298C. (3) Key biochemical indicators, including folate, vitamin B12, and Hcy, were not measured, limiting direct mechanistic interpretation. (4) Other factors, including thyroid autoantibody status, iodine nutrition, and dietary supplementation, were not analyzed in detail and should be considered in future studies.
Conclusion
The MTHFR C677T polymorphism is associated with the occurrence of SCH in early pregnancy, and the T allele may serve as an important genetic susceptibility factor, whereas no significant association was observed for the A1298C locus. These findings indicate that maternal genetic background, specifically the C677T variant, contributes to SCH risk in early pregnancy. Future studies with larger sample sizes, multicenter designs, and prospective approaches are warranted to further validate these associations and explore their potential utility in early screening and precision interventions for high-risk populations.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Toloza FJK, Derakhshan A, Männistö T, et al. Association between maternal thyroid function and risk of gestational hypertension and pre-eclampsia: a systematic review and individual-participant data meta-analysis. Lancet Diabetes Endocrinol. 2022;10(4):243–10. doi:10.1016/S2213-8587(22)00007-9
2. Aberle L, Nguyen CT. Subclinical hypothyroidism in pregnancy: an evolving and controversial landscape. Curr Opin Obstet Gynecol. 2025;37(2):60–65. doi:10.1097/GCO.0000000000001019
3. Xu H, Du Y-N, Yang S, et al. Relationship between BDNF content in cord blood and early neurobehavior in newborns with subclinical hypothyroidism during pregnancy: a preliminary study. Front Neurol. 2024;15:1465715. doi:10.3389/fneur.2024.1465715
4. Li MF, Ma L, Feng Q-M, et al. Effects of maternal subclinical hypothyroidism in early pregnancy diagnosed by different criteria on adverse perinatal outcomes in chinese women with negative TPOAb. Front Endocrinol. 2020;11:580380. doi:10.3389/fendo.2020.580380
5. Park S, Kim S, Kim B, et al. Multivariate genomic analysis of 5 million people elucidates the genetic architecture of shared components of the metabolic syndrome. Nat Genet. 2024;56(11):2380–2391. doi:10.1038/s41588-024-01933-1
6. Hong H, Fu Q, Gu P, et al. Investigating the common genetic architecture and causality of metabolic disorders with neurodegenerative diseases. Diabetes Obes Metab. 2025;27(3):1337–1349. doi:10.1111/dom.16130
7. Ellervik C, Boulakh L, Teumer A, et al. Thyroid function, diabetes, and common age-related eye diseases: a mendelian randomization study. Thyroid. 2024;34(11):1414–1423. doi:10.1089/thy.2024.0257
8. Hou H, Zhao H. Epigenetic factors in atherosclerosis: DNA methylation, folic acid metabolism, and intestinal microbiota. Clin Chim Acta. 2021;512:7–11. doi:10.1016/j.cca.2020.11.013
9. Kang W, Zhang Y, Cui W, et al. Folic acid promotes peripheral nerve injury repair via regulating DNM3-AKT pathway through mediating methionine cycle metabolism. Neuromolecular Med. 2025;27(1):23. doi:10.1007/s12017-025-08845-1
10. Seyoum Tola F. The concept of folic acid supplementation and its role in prevention of neural tube defect among pregnant women: PRISMA. Medicine. 2024;103(19):e38154. doi:10.1097/MD.0000000000038154
11. Li Y, Lian J, Yi L, et al. Folic acid supplementation in pregnant women with hepatitis B surface antigen improves infant hepatitis B surface antibody mediated by infant IL-4. Br J Nutr. 2023;129(10):1812–1819. doi:10.1017/S000711452200229X
12. Bošković A, Ćuk A, Mandrapa V, et al. Association of MTHFR polymorphism, folic acid and vitamin B12 with serum homocysteine levels in pregnant women. Biomol Biomed. 2024;24(1):138–143. doi:10.17305/bb.2023.9260
13. Jiang S, Liu Y, Lu C, et al. Associations of two common polymorphisms in MTHFR gene with blood lipids and therapeutic efficacy of simvastatin. Curr Pharm Des. 2022;28(26):2167–2176. doi:10.2174/1381612828666220623102537
14. Zhang L, Sun L, Wei T. Correlation between MTHFR gene polymorphism and homocysteine levels for prognosis in patients with pregnancy-induced hypertension. Am J Transl Res. 2021;13(7):8253–8261.
15. Li Y, Shan Z, Teng W, et al. Association between MTHFR C677T polymorphism and thyroid dysfunction: a systematic review and meta-analysis. Front Endocrinol. 2022;13:875682.
16. Wang X, Zhang H, Zhao L, et al. Relationship between MTHFR gene polymorphisms and thyroid function in women of reproductive age: a population-based study. BMC Endocr Disord. 2021;21(1):187. doi:10.1186/s12902-021-00851-1
17. Bogović Crnčić T, Brkljačić J, Granić R, et al. Autoimmune thyroid disease and pregnancy. J Clin Med. 2024;14(1):190. doi:10.3390/jcm14010190
18. Alexander EK, Pearce EN, Brent GA, et al. 2017 Guidelines of the American thyroid association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid. 2017;27(3):315–389.
19. Mladenovic V, Shah R, Medenica S, et al. Thyroid gland and pregnancy - clinical update. Horm Metab Res. 2025;57(5):303–314. doi:10.1055/a-2604-4177
20. Møllehave LT, Grand MK, Kriegbaum M, et al. Maternal thyroid function in early pregnancy and offspring school performance and neurodevelopmental disorders. J Clin Endocrinol Metab. 2025;110(4):e1000–e1008.
21. Björnholm L, Orell O, Kerkelä M, et al. Maternal thyroid function during pregnancy and offspring white matter microstructure in early adulthood: a prospective birth cohort study. Thyroid. 2023;33(10):1245–1254. doi:10.1089/thy.2022.0699
22. Hill DJ, Hill TG. Maternal diet during pregnancy and adaptive changes in the maternal and fetal pancreas have implications for future metabolic health. Front Endocrinol. 2024;15:1456629.
23. Muccini AM, Tran NT, de Guingand DL, et al. Creatine metabolism in female reproduction, pregnancy and newborn health. Nutrients. 2021;13(2):490. doi:10.3390/nu13020490
24. Sun Y, Shen Z, Zhan Y, et al. Effects of pre-pregnancy body mass index and gestational weight gain on maternal and infant complications. BMC Pregnancy Childbirth. 2020;20(1):390. doi:10.1186/s12884-020-03071-y
25. Derakhshan A, Peeters RP, Taylor PN, et al. Association of maternal thyroid function with birthweight: a systematic review and individual-participant data meta-analysis. Lancet Diabetes Endocrinol. 2020;8(6):501–510. doi:10.1016/S2213-8587(20)30061-9
26. Yang Y, Hou Y, Wang H, et al. Maternal thyroid dysfunction and gestational anemia risk: meta-analysis and new data. Front Endocrinol. 2020;11:201. doi:10.3389/fendo.2020.00201
27. Wang Y, Lu S, Xu X, et al. The interactive effects of pre-pregnancy body mass index, thyroid function, and blood lipid levels on the risk of gestational diabetes mellitus: a crossover analysis. BMC Pregnancy Childbirth. 2022;22(1):580. doi:10.1186/s12884-022-04908-4
28. Lu W, Wang Z, Sun Z, et al. The interactive effects of severe vitamin d deficiency and iodine nutrition status on the risk of thyroid disorder in pregnant women. Nutrients. 2022;14(21):4484.
29. Araszkiewicz AF, Jańczak K, Wójcik P, et al. MTHFR gene polymorphisms: a single gene with wide-ranging clinical implications-a review. Genes. 2025;16(4):441.
30. Li ZC, Huang M, Yao Q-Y, et al. Association between MTHFR C677T gene polymorphisms and the efficacy of vitamin therapy in lowering homocysteine levels among stroke patients with hyperhomocysteinemia. J Integr Neurosci. 2024;23(1):3. doi:10.31083/j.jin2301003
31. Gu YH, Zhang Q, Guo J, et al. Higher serum homocysteine and lower thyroid hormone levels in pregnant women are associated with neural tube defects. J Trace Elem Med Biol. 2021;68:126814. doi:10.1016/j.jtemb.2021.126814
32. Xu Y, Ban Y, Ran L, et al. Relationship between unexplained recurrent pregnancy loss and 5,10-methylenetetrahydrofolate reductase) polymorphisms. Fertil Steril. 2019;111(3):597–603. doi:10.1016/j.fertnstert.2018.11.011
33. Nguyen Ngoc N, Tran Ngoc Thao M, Trieu Tien S, et al. Evaluating the association between genetic polymorphisms related to homocysteine metabolism and unexplained recurrent pregnancy loss in women. Appl Clin Genet. 2022;15:55–62. doi:10.2147/TACG.S365281
34. Huang LL, Tong J-R, Huang Y, et al. Association of MTHFR gene C677T polymorphism with pregnancy outcome. Eur Rev Med Pharmacol Sci. 2023;27(1):166–171. doi:10.26355/eurrev_202301_30868
35. Kvaratskhelia T, Kvaratskhelia E, Kankava K, et al. Mthfr gene C677t Polymorphism and levels of dna methyltrasferases in subclinical hypothyroidism. Georgian Med News. 2017;(265):19–24.
36. Zhao T, Li C, Wang H, et al. Effects of maternal iodine deficiency in women with mild thyroid dysfunction during early pregnancy on mental and motor growth of their offspring during levothyroxine treatment. Biol Trace Elem Res. 2025;204:2186–2198. doi:10.1007/s12011-025-04810-y
37. Zou J, Wang Y. Association between serum thyroid measurements and hyperhomocysteinemia in euthyroid subjects: a retrospective cross-sectional study. Diabetes Metab Syndr Obes. 2023;16:3425–3433. doi:10.2147/DMSO.S436381
38. Zhu J, Liao X, Du L, et al. Associations of serum folate and vitamin B(12) levels with all-cause mortality among patients with metabolic dysfunction associated steatotic liver disease: a prospective cohort study. Front Endocrinol. 2024;15:1426103. doi:10.3389/fendo.2024.1426103
39. Ilhan C. Serum levels of thyroid hormone, Vitamin B12, Vitamin D3, folic acid, and ferritin in chalazion. Ocul Immunol Inflamm. 2022;30(4):776–780. doi:10.1080/09273948.2020.1828490
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.