Back to Journals » Clinical Ophthalmology » Volume 19
Association Between Maternal Pre-Pregnancy Body Mass Index and Astigmatism and Corneal Curvature in Offspring: A Cross-Sectional Study
Authors Han Y, Lv H, Cao Y, Wu J, Zeng X, Pazo EE ![]() , Zhao Y, Lv J, Lu W
, Zhao Y, Lv J, Lu W ![]() , Qian X, Wei N
, Qian X, Wei N
Received 2 April 2025
Accepted for publication 12 August 2025
Published 12 September 2025 Volume 2025:19 Pages 3371—3380
DOI https://doi.org/10.2147/OPTH.S532009
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yuanyuan Han,1,* Hongyu Lv,2,* Yidan Cao,3,* Jing Wu,1 Xiaoyu Zeng,1 Emmanuel Eric Pazo,1 Yaxin Zhao,1 Jia Lv,4 Wenli Lu,3 Xuehan Qian,1 Nan Wei1
1Tianjin Key Laboratory of Retinal Functions and Diseases, Tianjin Branch of National Clinical Research Center for Ocular Disease, Eye Institute and School of Optometry, Tianjin Medical University Eye Hospital, Tianjin, People’s Republic of China; 2Department of Pediatric Eye Care, Qinhuangdao Maternal and Child Health Care Hospital. Qinhuangdao, Hebei, People’s Republic of China; 3Department of Epidemiology and Statistics, School of Public Health, Tianjin Medical University, Tianjin, People’s Republic of China; 4Tianjin Aier Eye Hospital, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Nan Wei, Tianjin Key Laboratory of Retinal Functions and Diseases, Tianjin Branch of National Clinical Research Center for Ocular Disease, Eye Institute and School of Optometry, Tianjin Medical University Eye Hospital, Tianjin, 300384, People’s Republic of China, Email [email protected]
Purpose: To investigate the association between maternal pre-pregnancy body mass index (BMI) and astigmatism and corneal curvature in offspring.
Patients and Methods: Corneal topography and an optical biometer were used to measure ocular parameters, while cycloplegic autorefraction was performed to assess cylindrical diopter and axis. Demographic, pregnancy, and offspring-related information was collected through questionnaires. Multiple linear regression analyses were conducted to evaluate the association.
Results: A total of 213 mother-child pairs were included. Maternal pre-pregnancy BMI was categorized as underweight (11.3%), normal weight (66.7%), overweight (16.0%), and obese (6.1%). The mean age of the offspring was 6.80 ± 2.44 years (males 49.3%). Offspring born to mothers with overweight or obese pre-pregnancy BMI exhibited significantly higher steep corneal curvature, average corneal curvature, corneal astigmatism, and total astigmatism compared to those in the normal pre-pregnancy BMI group. In multiple linear regression analysis, after adjusting for relevant covariates, pre-pregnancy BMI was positively associated with steep corneal curvature (β=0.35, P=0.005), corneal astigmatism (β=0.21, P=0.001), and total astigmatism (β=0.22, P< 0.001). Compared to normal pre-pregnancy BMI, pre-pregnancy obesity was positively associated with offspring steep corneal curvature (β=1.52, P=0.002) and those born to mothers with overweight or obese pre-pregnancy BMI had a significantly higher prevalence of corneal astigmatism (overweight: β=0.56, P=0.001; obese: β=0.55, P=0.038) and total astigmatism (overweight: β=0.47, P=0.002; obese: β=0.59, P=0.010).
Conclusion: Offspring of mothers with overweight or obese pre-pregnancy BMI show higher prevalence of developing corneal and total astigmatism compared to the normal.
Keywords: pre-pregnancy BMI, astigmatism, corneal curvature, maternal health, offspring eye development
Introduction
A high pre-pregnancy body mass index (BMI) is associated with an increased risk of pregnancy-related complications, including gestational hypertension, preeclampsia, and gestational diabetes mellitus. Moreover, the likelihood of these complications rises proportionally with increasing pre-pregnancy BMI.1–3 Pre-pregnancy overweight and obesity are increasingly recognized as significant factors influencing both maternal and offspring health. Obesity has become a global public health concern, particularly in developed countries, where pre-pregnancy BMI is rising among women of reproductive age.4 Between 1998 and 2003, the number of women who were overweight or obese increased globally from 29.8% to 38%.5 In China, the rates of overweight and obesity among women are 30.6% and 12%, respectively, and are still on the rise.6 High pre-pregnancy BMI is also a key factor in poor outcomes for offspring, including obesity, cancer, cardiovascular disease, and type 2 diabetes mellitus.7 Maternal pre-pregnancy obesity may increase the risk of breast cancer in daughters.8 However, few studies examine the relationship between pre-pregnancy BMI and astigmatism and corneal curvature in offspring.
Astigmatism is a common refractive error that focuses on unequal or irregular curvature of the cornea or lens, causing blurred or distorted vision. Uncorrected astigmatism is a risk factor for amblyopia and requires timely diagnosis and proper refractive correction to avoid lasting effects on children’s vision.9 Astigmatism can be caused by a variety of factors, such as race, age, genetics, and eye structure.10 Previous studies have explored the relationship between child BMI and astigmatism. A study found that obesity was associated with a higher incidence of astigmatism in adolescents.11 It was also found that patients with high astigmatism or high corneal astigmatism tend to have with-the-rule astigmatism, and that children’s high BMI or weight is associated with with-the-rule astigmatism and corneal astigmatism.12 In addition, a study has explored the relationship between adult BMI and ocular parameters.13 The mechanical properties and behaviour of the cornea are referred to as corneal biomechanics, which play an important role in maintaining corneal morphology and clarity. These properties are influenced by hydration, collagen alignment, and central corneal thickness.14 Hormonal fluctuations during pregnancy can affect changes in central corneal thickness, which is an important factor affecting corneal biomechanics of the child.15
The relationship between pre-pregnancy BMI and offspring astigmatism and corneal curvature remains unclear. Given the rising trend in maternal pre-pregnancy BMI and the impact of astigmatism on children’s daily lives, it is crucial to investigate this association.
Materials and Methods
Participants
Three hundred and seven mother-child pairs took part in the study between October 2023 and January 2024 from the Pediatric Eye Care Department of Qinhuangdao Maternal and Child Health Care Hospital. Ninety-four mother-child pairs were excluded due to missing dates. A total of 213 mother-child pairs were included (Figure 1). The study was conducted in accordance with the guidelines of the Declaration of Helsinki, approved by the hospital ethics committee, and informed consent was obtained from the children’s guardians. Inclusion criteria were: (i) children aged 3 to 12 years, (ii) mothers who completed the pregnancy information questionnaire, (iii) and children able to cooperate with ophthalmologic examinations. Exclusion criteria were: (i) children with organic ocular pathology, such as congenital ptosis or congenital cataract. (ii) children with systemic organic diseases that may cause ocular complications, such as Down syndrome or albinism. (iii) children with neurological dysfunction, such as autism spectrum disorder. (iv) children with a history of ocular surgery or trauma, (v) and children with parents (both father and mother) diagnosed with astigmatism, with cylinder power absolute values ≥1.00 D as measured by autorefraction without cycloplegia.
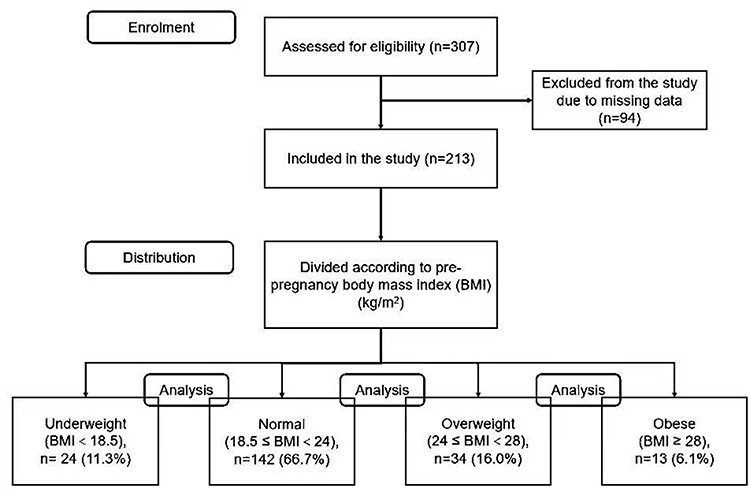 |
Figure 1 CONSORT flow diagram for cross-sectional study. |
Data Collection
Information on pre-pregnancy height and weight was collected through the mother’s self-report. Studies showed that self-reported height and weight data were highly correlated with hospital measurements.16,17 Pre-pregnancy BMI was calculated according to the formula: BMI (kg/m2) = weight (kg) / height (m)2. The pre-pregnancy BMI (kg/m2) was classified using the World Health Organization:18 underweight (BMI<18.5 kg/m2); normal weight (18.5≤BMI<24 kg/m2); overweight (24≤BMI<28 kg/m2); obesity (BMI≥28 kg/m2).
Detailed ocular examinations of the offspring were performed by an experienced ophthalmologist and an optometrist, and all participants received a uniform examination method. Cycloplegic autorefraction, anterior eye segment status, ocular motility, and ocular parameters were examined separately.
Cycloplegic autorefraction was performed using compound tropicamide eye drops, with one drop every 5 minutes for a total of 4 times. Autorefraction under cycloplegia was performed 40 minutes after the last drop. Cycloplegia was considered successful if the pupil was dilated to at least 6 mm and the light reflex was absent, as assessed by the examiner. The cylinder diopter (DC) was measured using an open-field autorefractor (WAM-5500, Grand Seiko, Japan) for eyes. Each eye was measured at least 3 times, with changes in cylindrical diopter < 0.50D between any two measurements, and then the average value was taken. The corneal topographer (TMS-4N, Tomey, Japan) was used to measure the corneal steep curvature (Ks), corneal flat curvature (Kf), average corneal curvature (AvgK), corneal astigmatism (CA), surface asymmetry index (SAI), and surface regularity index (SRI) of the offspring. CA was calculated based on the difference between Ks and Kf. The optical biometer (LS900, Switzerland) was employed to measure the anterior chamber depth (ACD), white-to-white corneal diameter (WTW), and pupil diameter (PD) of the offspring. All ocular measurements were performed by experienced optometrists using standardized protocols.
All results were analyzed using data from the right eye due to the high correlation between the two eyes. Total astigmatism was indicated by cylinder diopter (DC). According to the astigmatism axial classification: (i) With-the-rule (WTR) astigmatism: defined by a steep meridian at 90°±30°; (ii) Against-the-rule (ATR) astigmatism: defined by a steep meridian at 180°±30°; (iii) Oblique astigmatism (OBL): defined by a steep meridian between 30°–60°and 120°–150°.
A questionnaire was used to collect characteristics of the mother-child pairs, such as the maternal age at delivery and gestational diabetes. Birth history information, such as age, gender, birth weight, birth order and birth length, was also collected.
Statistical Analysis
All statistical analyses were performed in SPSS version 26.0 software. Continuous variables were expressed as mean ± SD or median (interquartile range), while categorical variables were presented as frequencies and percentages. The Kolmogorov–Smirnov test was employed to assess the normal distribution of continuous variables. If the data followed a normal distribution, one-way ANOVA was used for between-group comparisons; otherwise, the Kruskal–Wallis test was performed. For categorical variables, the χ2 test was used. Based on the results of the univariate analysis, the significance level α was set at 0.10 and statistically significant variables were screened for inclusion in the multiple linear regression model. Multiple linear regression model was applied to analyze the association between maternal pre-pregnancy BMI and ocular parameters of offspring. The dataset was analyzed for outliers and influential points using standardized residuals and Cook’s distance. P < 0.05 (two-sided) was considered statistically significant.
Results
Participants Characteristics
The study enrolled a total of 213 mother-child pairs. Among mothers, 24 (11.3%) were underweight, 142 (66.7%) were normal, 34 (16.0%) were overweight, and 13 (6.1%) were obese pre-pregnancy BMI. The average age of the offspring was 6.80±2.44 years, with male accounting for 49.3%. The P-values for age (P = 0.002), gestational week (P = 0.001), child BMI (P = 0.064), and birth weight (P = 0.063) were all <0.10 (Table 1).
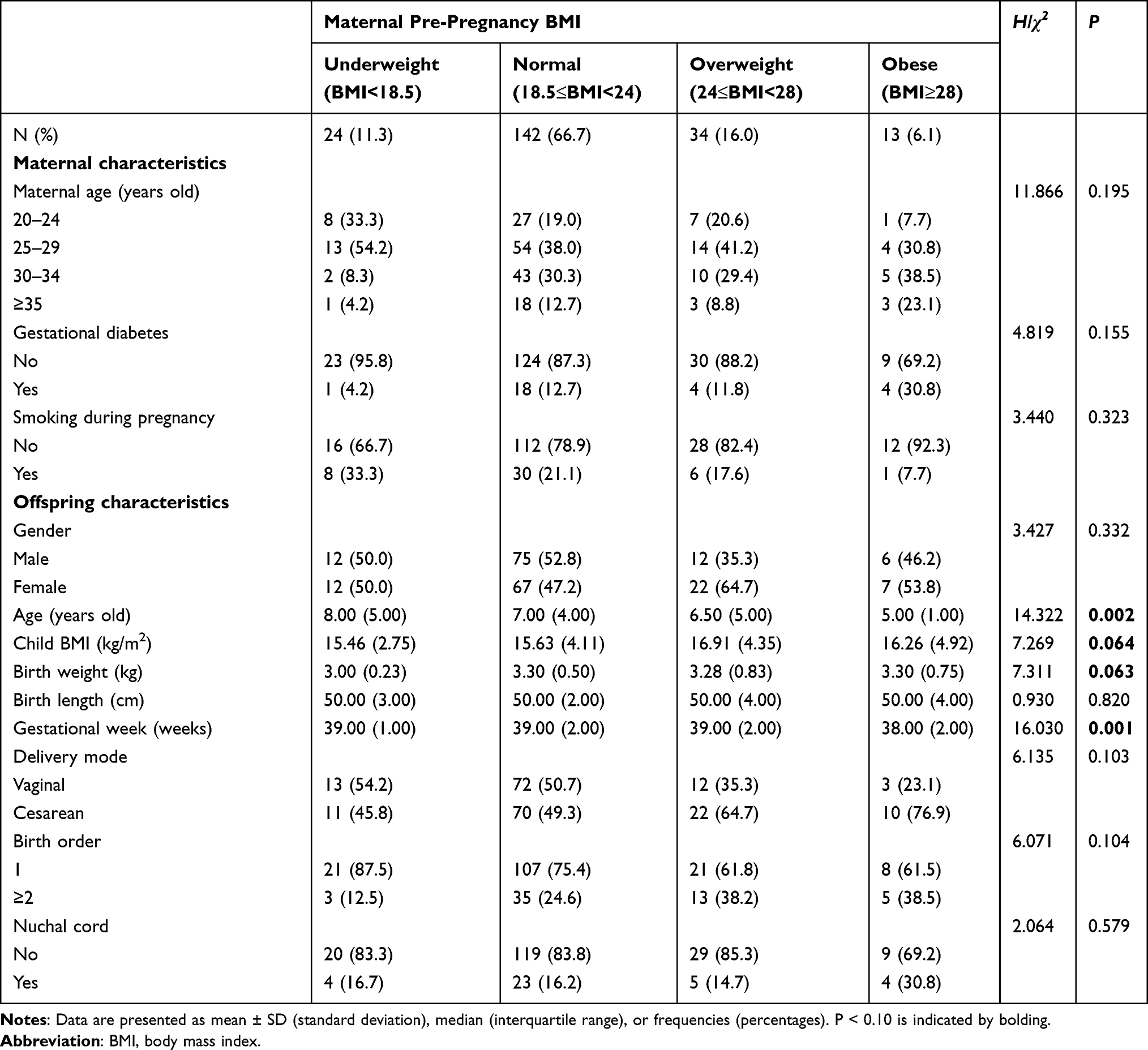 |
Table 1 Baseline Characteristics |
Comparison of Ocular Parameters in Offspring Between Groups
When comparing offspring ocular parameters across different pre-pregnancy BMI categories, it was found that the offspring of mothers with normal pre-pregnancy BMI had significantly lower Ks values than those in the other three groups, with the highest Ks observed in the obese group. The differences between the obese group and each of the other groups were statistically significant (all P < 0.05). Similarly, the AvgK was lowest in the normal pre-pregnancy BMI group and highest in the obese group. The differences between the obese group and both the normal (P = 0.005) and overweight (P = 0.021) groups were statistically significant. For CA, the lowest values were observed in offspring from the normal pre-pregnancy BMI group, with statistically significant differences between the normal and overweight groups (P = 0.015) as well as between the normal and obese groups (P = 0.038). Additionally, offspring of mothers with a normal pre-pregnancy BMI had the smallest DC values, with significant differences observed between the normal and overweight groups (P < 0.001) and between the normal and obese groups (P = 0.022). However, no statistically significant differences were found among the four groups for Kf, SAI, SRI, ACD, WTW, or PD (all P > 0.05) (Table 2).
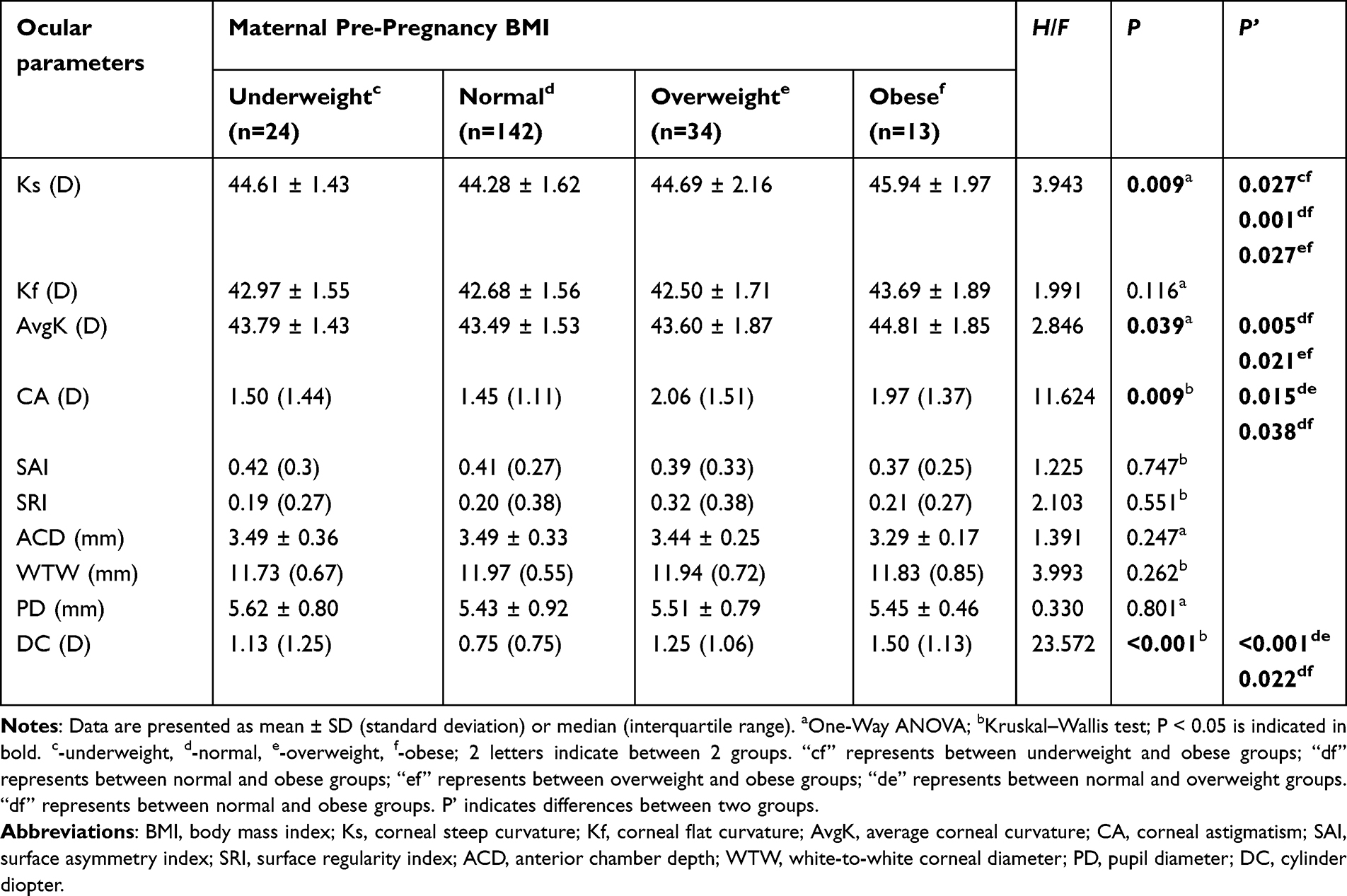 |
Table 2 Comparison of Ocular Parameters in Offspring Between 4 Groups |
Association Between Pre-Pregnancy BMI and Ocular Parameters in Offspring
In the multiple linear regression analysis, maternal pre-pregnancy BMI was significantly associated with offspring Ks (β = 0.34, 95% CI: 0.09–0.59, P = 0.009), CA (β = 0.19, 95% CI: 0.05–0.32, P = 0.007), and DC (β = 0.22, 95% CI: 0.10–0.33, P < 0.001) (Model 1). As pre-pregnancy BMI increased, offspring Ks, CA, and DC also increased (β > 0). After adjusting for relevant covariates, these associations remained significant: Ks (β = 0.35, 95% CI: 0.10–0.59, P = 0.005), CA (β = 0.21, 95% CI: 0.09–0.34, P = 0.001), and DC (β = 0.22, 95% CI: 0.11–0.34, P < 0.001) (Model 2) (Table 3). Sensitivity analysis demonstrated that after the removal of outliers, the coefficient variation rates of the primary predictors were as follows: DC (9.1%), Ks (11.7%), and CA (5.2%) (all below the 15% threshold), indicating robust results (Supplementary Table 1). Further analysis indicated that, compared to normal pre-pregnancy BMI, pre-pregnancy obesity was positively associated with offspring Ks (β = 1.52, 95% CI: 0.57–2.48, P = 0.002), whereas no significant associations were found between pre-pregnancy overweight or underweight and offspring Ks (P > 0.05). Both pre-pregnancy overweight and obesity were positively associated with offspring CA (overweight: β = 0.56, 95% CI: 0.22–0.90, P = 0.001; obese: β = 0.55, 95% CI: 0.03–1.07, P = 0.038) and DC (overweight: β = 0.47, 95% CI: 0.18–0.77, P = 0.002; obese: β = 0.59, 95% CI: 0.14–1.04, P = 0.010) compared to normal pre-pregnancy BMI. However, no significant associations were observed between underweight and offspring CA or DC (P > 0.05). When pre-pregnancy BMI was analyzed as a continuous variable, these associations remained significant (all P < 0.05) (Table 4 and Figure 2A–C).
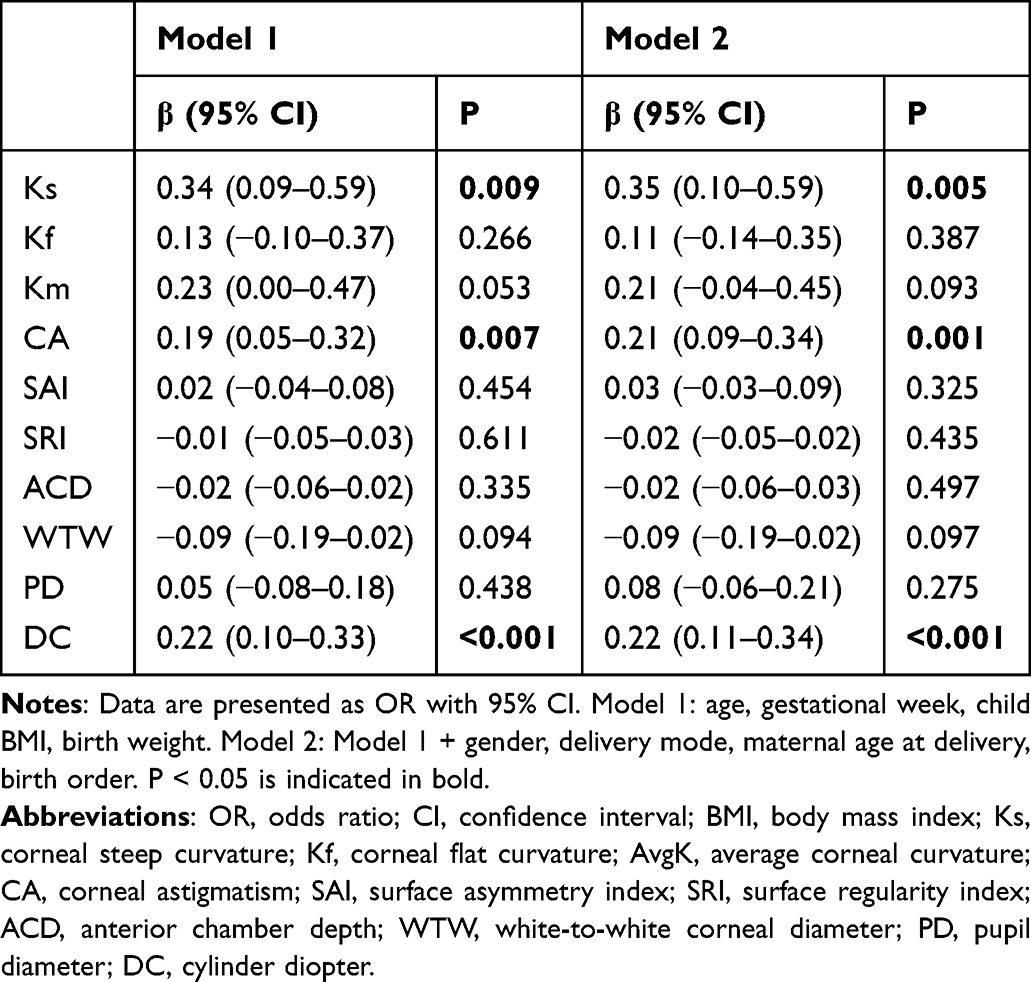 |
Table 3 The Relationship Between Pre-Pregnancy BMI and Offspring Ocular Parameters |
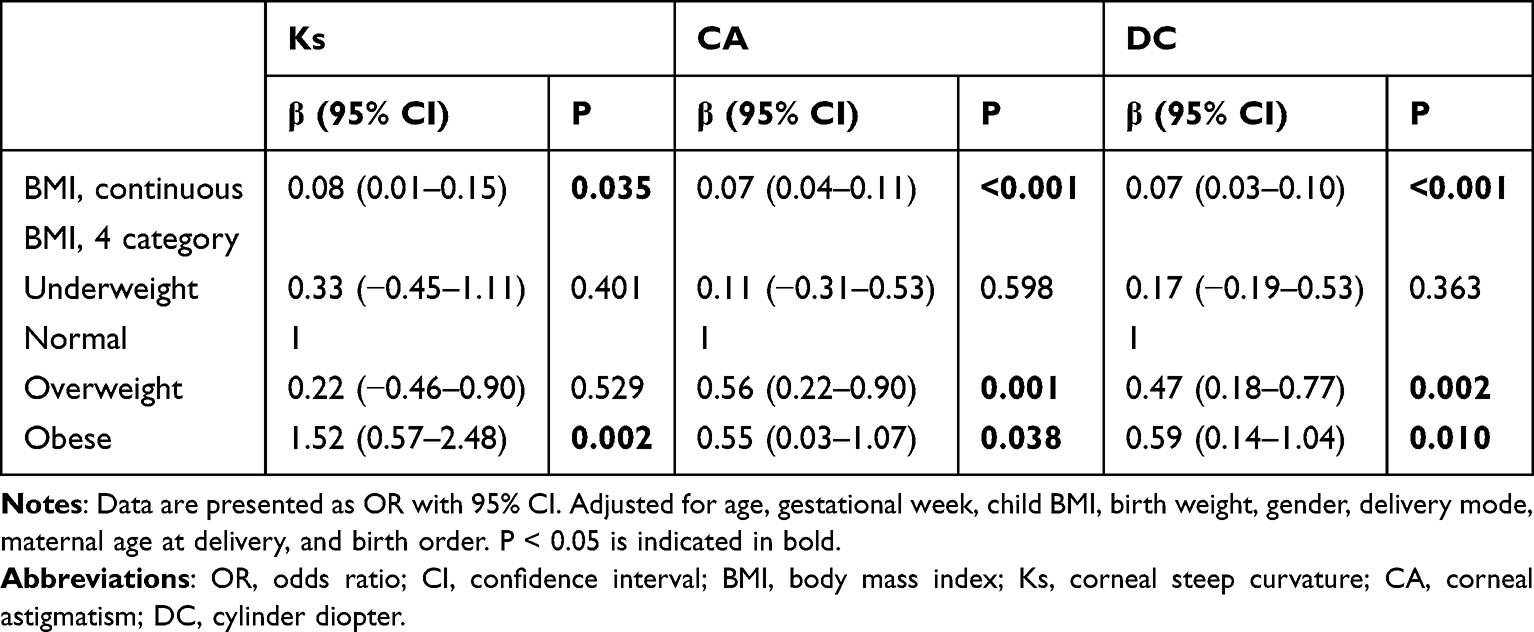 |
Table 4 The Relationship Between the Adjusted Pre-Pregnancy BMI and Ks, CA and DC in Offspring |
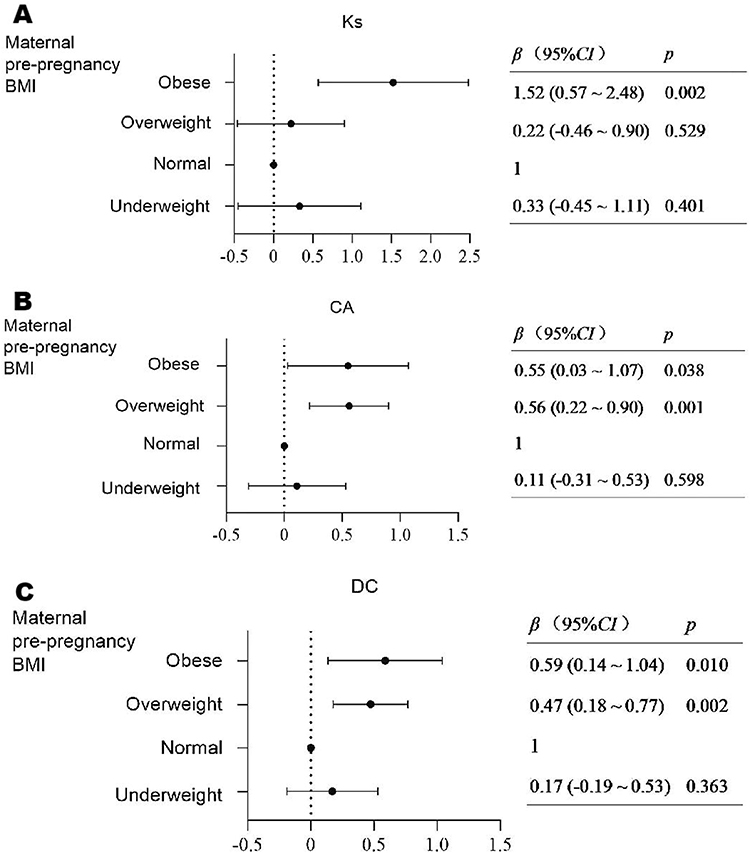 |
Figure 2 The association between maternal pre-pregnancy BMI and offspring Ks (A), CA (B), and DC (C). |
There was no significant difference between pre-pregnancy BMI and astigmatism classified by axis (P > 0.05) (Table 5).
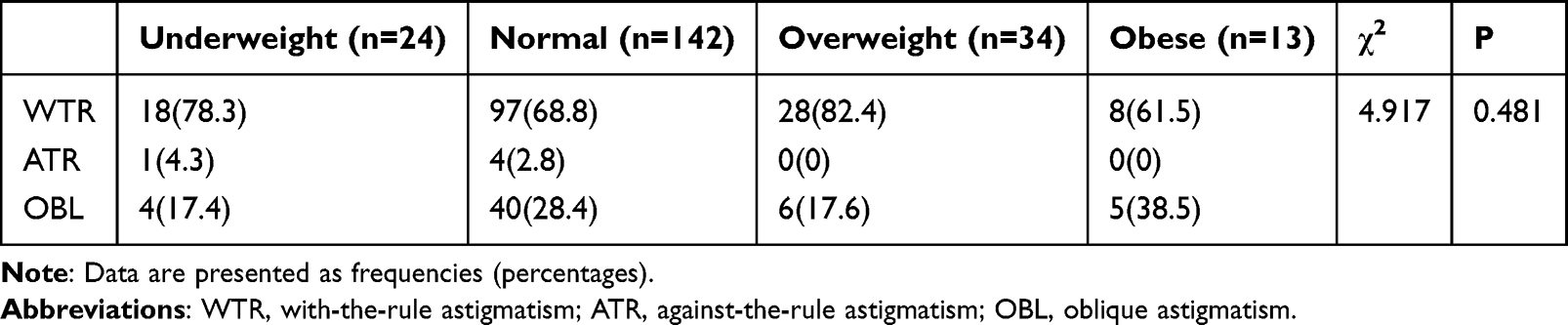 |
Table 5 Relationship Between Pre-Pregnancy BMI and Offspring Astigmatism According to the Axis |
Discussion
Approximately half of the global adult population and one-fifth of children are overweight or obese, with China having the highest number of overweight and obese individuals worldwide.19 Among pediatric patients with refractive errors, the prevalence of astigmatism reaches 14.9%.20 The astigmatism prevalence rates are 16.8% in Hispanic children and 12.7% in African American children.21 Additionally, the prevalence of astigmatism among Chinese preschool children is 21.1%.22 Asian children exhibit a higher prevalence of astigmatism, which may be attributed to distinct facial anatomical features, including tighter eyelids and narrower palpebral fissures commonly observed in Asian populations.10 Studies have demonstrated that astigmatism tends to follow an autosomal dominant inheritance pattern.23 However, conflicting findings have also been reported, indicating that compared to the high heritability of myopia and hyperopia, genetic factors exert the least influence on astigmatism.24 Both genetic and environmental factors contribute to the development of astigmatism. Nevertheless, the precise mechanisms underlying these effects remain incompletely understood.
This study demonstrates a significant association between maternal pre-pregnancy BMI and offspring astigmatism and corneal curvature. Our findings indicate a positive correlation between pre-pregnancy BMI and both corneal and total astigmatism in offspring. Notably, even after adjusting for potential confounding factors, astigmatism remained higher in the overweight and obese groups compared to the normal pre-pregnancy BMI group. In the short term, uncorrected astigmatism can exacerbate ocular fatigue and discomfort when reading.25 In the long term, uncorrected high astigmatism during early visual development in children may interfere with emmetropization, leading to permanent amblyopia.9 While numerous studies have highlighted the adverse health effects of elevated pre-pregnancy BMI, emerging evidence also suggests a link between obesity or high adult BMI and various ocular diseases, including glaucoma, diabetic retinopathy, cataracts, and age-related macular degeneration.26,27
Maternal pre-pregnancy BMI can affect maternal hormonal levels. Gaml-Sørensen et al found that pre-pregnancy obesity and overweight were associated with increased adipose tissue, which can lead to increased estradiol production.28 Meanwhile, McKay et al discovered that changes in estrogen and progesterone during embryonic development may affect the structure of the cornea. These hormones influence cellular activities through receptors expressed in corneal epithelial and stromal fibroblasts.29,30 However, the exact mechanism by which sex hormones affect corneal morphology and astigmatism is not fully understood and requires further exploration. In this cross-sectional study, offspring of pre-pregnancy overweight or obesity showed significantly steeper corneal curvature and higher average corneal curvature compared to offspring of normal pre-pregnancy BMI. This may be due to fluid retention in the corneal area caused by high levels of estrogen and progesterone, leading to increased corneal curvature.31,32 Additionally, obesity may lead to decreased growth hormone secretion, which can promote increased corneal curvature and decreased central corneal thickness.33
Total astigmatism is a combination of corneal astigmatism and intraocular astigmatism, and the most common is corneal astigmatism.34 Corneal astigmatism is defined as the difference between steep and flat curvature of cornea, and it is primarily caused by steep curvature of cornea.35 The study observed a positive association between maternal pre-pregnancy BMI and steep corneal curvature in offspring. In addition, Nitzan et al found that adolescents with higher BMI tend to have WTR astigmatism, while underweight adolescents are more likely to have ATR astigmatism, which may be attributed to reduced eyelid pressure.11 However, in our study, there was no significant difference in offspring axial astigmatism.
Maternal pre-pregnancy BMI is an important predictor of offspring obesity, and there is a positive correlation, indicating a genetic effect.36,37 The pressure exerted by the eyelids on the cornea is considered a potential factor in the development of corneal astigmatism. Obese patients may also experience greater corneal astigmatism due to increased eyelid pressure.
Shin et al found a negative correlation between pre-pregnancy BMI and diet quality during pregnancy and maternal nutritional biomarkers.38 Another study discovered that malnutrition may lead to decreased corneal stiffness, resulting in increased corneal astigmatism.39 Future research could further explore the relationship between the severity of pre-pregnancy BMI overweight or obesity and astigmatism and corneal curvature.
The study identified a positive association between maternal pre-pregnancy body mass index (BMI) and offspring corneal steep curvature, corneal astigmatism, and total astigmatism. For children born to mothers with elevated pre-pregnancy BMI, increased frequency of vision screening during routine pediatric health examinations is recommended. The cross-sectional findings suggest that maternal pre-pregnancy BMI may represent a potentially modifiable factor associated with offspring ocular development, warranting consideration for inclusion in maternal health education programs.
To our knowledge, this is the first study to evaluate the relationship between pre-pregnancy BMI and offspring astigmatism and corneal curvature while accounting for potential confounding factors related to pregnancy and birth history. However, this study has some limitations. First, the sample size was limited, and particular caution should be exercised in interpreting the results of the obese subgroup (n=13). It is recommended that future research employ formal sample size calculation methods to ensure adequate statistical power. Due to the study’s cross-sectional nature, we cannot determine the temporal order of exposures and outcomes or draw definitive conclusions about causality. Longitudinal research with a larger cohort is needed to validate these findings. Additionally, maternal pre-pregnancy BMI, pregnancy history, and birth history data were self-reported by mothers, which may introduce recall bias. Future studies incorporating objective medical records and longitudinal designs could strengthen the reliability of these associations. Thirdly, the study did not include parental history of refractive error (beyond astigmatism), environmental factors (outdoor time, near-work activity, screen use), socioeconomic status, or maternal nutritional. It is recommended that future research incorporate these key confounding factors.
Conclusion
In conclusion, our findings highlight a significant association between maternal pre-pregnancy BMI and offspring astigmatism and corneal curvature. Deviations from the normal pre-pregnancy BMI range, particularly overweight and obesity, are linked to increased corneal and total astigmatism in offspring, an association that persists even after adjusting for multiple confounding factors.
Abbreviations
OR, odds ratio; CI, confidence interval; BMI, body mass index; Ks, corneal steep curvature; Kf, corneal flat curvature; AvgK, average corneal curvature; CA, corneal astigmatism; SAI, surface asymmetry index; SRI, surface regularity index; ACD, anterior chamber depth; WTW, white-to-white corneal diameter; PD, pupil diameter; DC, cylinder diopter.
Ethics Approval and Informed Consent
This study passed the ethical review of the Qinhuangdao Maternal and Child Health Care Hospital (Ethics approval No QHDFY-2023031010).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funded by Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-037A).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Vinturache A, Moledina N, McDonald S, Slater D, Tough S. Pre-pregnancy Body Mass Index (BMI) and delivery outcomes in a Canadian population. BMC Pregnancy Childbirth. 2014;14:422. doi:10.1186/s12884-014-0422-y
2. Vézina-Im LA, Nicklas TA, Baranowski T. Intergenerational effects of health issues among women of childbearing age: a review of the recent literature. Curr Nutr Rep. 2018;7(4):274–285. doi:10.1007/s13668-018-0246-x
3. Wei YM, Yang HX, Zhu WW, et al. Risk of adverse pregnancy outcomes stratified for pre-pregnancy body mass index. J Matern Fetal Neonatal Med. 2016;29(13):2205–2209. doi:10.3109/14767058.2015.1081167
4. Kim SY, Dietz PM, England L, Morrow B, Callaghan WM. Trends in pre-pregnancy obesity in nine states, 1993-2003. Obesity. 2007;15(4):986–993. doi:10.1038/oby.2007.621
5. Mastroeni MF, Czarnobay SA, Kroll C, et al. The independent importance of pre-pregnancy weight and gestational weight gain for the prevention of large-for gestational age brazilian newborns. Matern Child Health J. 2017;21(4):705–714. doi:10.1007/s10995-016-2156-0
6. Zhang H, Xu H, Song F, Xu W, Pallard-Borg S, Qi X. Relation of socioeconomic status to overweight and obesity: a large population-based study of Chinese adults. Ann Hum Biol. 2017;44(6):495–501. doi:10.1080/03014460.2017.1328072
7. Eriksson JG, Sandboge S, Salonen MK, Kajantie E, Osmond C. Long-term consequences of maternal overweight in pregnancy on offspring later health: findings from the Helsinki birth cohort study. Ann Med. 2014;46(6):434–438. doi:10.3109/07853890.2014.919728
8. Zhang X, de Oliveira Andrade F, Zhang H, et al. Maternal obesity increases offspring’s mammary cancer recurrence and impairs tumor immune response. Endocr Relat Cancer. 2020;27(9):469–482. doi:10.1530/ERC-20-0065
9. Pascual M, Huang J, Maguire MG, et al. Risk factors for amblyopia in the vision in preschoolers study. Ophthalmology. 2014;121(3):622–629.e621. doi:10.1016/j.ophtha.2013.08.040
10. Read SA, Collins MJ, Carney LG. A review of astigmatism and its possible genesis. Clin Exp Optom. 2007;90(1):5–19. doi:10.1111/j.1444-0938.2007.00112.x
11. Nitzan I, Akavian I, Shmueli O, et al. Body mass index and astigmatism: a nationwide study. Clin Exp Ophthalmol. 2024;52(6):616–626. doi:10.1111/ceo.14406
12. Lai YH, Hsu HT, Wang HZ, Chang CH, Chang SJ. Astigmatism in preschool children in Taiwan. J Aapos. 2010;14(2):150–154. doi:10.1016/j.jaapos.2009.12.168
13. Panon N, Luangsawang K, Rugaber C, et al. Correlation between body mass index and ocular parameters. Clin Ophthalmol. 2019;13:763–769. doi:10.2147/OPTH.S196622
14. Hatami-Marbini H. Hydration dependent viscoelastic tensile behavior of cornea. Ann Biomed Eng. 2014;42(8):1740–1748. doi:10.1007/s10439-014-0996-6
15. Baptista PM, Ambrosio R, Oliveira L, Meneres P, Beirao JM. Corneal biomechanical assessment with ultra-high-speed scheimpflug imaging during non-contact tonometry: a prospective review. Clin Ophthalmol. 2021;15:1409–1423. doi:10.2147/OPTH.S301179
16. Hunt KJ, Ferguson PL, Neelon B, et al. The association between maternal pre-pregnancy BMI, gestational weight gain and child adiposity: a racial-ethnically diverse cohort of children. Pediatr Obes. 2022;17(8):e12911. doi:10.1111/ijpo.12911
17. Chin HB, Baird DD, McConnaughey DR, Weinberg CR, Wilcox AJ, Jukic AM. Long-term recall of pregnancy-related events. Epidemiology. 2017;28(4):575–579. doi:10.1097/EDE.0000000000000660
18. Madden D. BMI mobility and obesity transitions among children in Ireland. Econ Hum Biol. 2020;38:100896. doi:10.1016/j.ehb.2020.100896
19. Wang Y, Zhao L, Gao L, Pan A, Xue H. Health policy and public health implications of obesity in China. Lancet Diabetes Endocrinol. 2021;9(7):446–461. doi:10.1016/S2213-8587(21)00118-2
20. Hashemi H, Fotouhi A, Yekta A, Pakzad R, Ostadimoghaddam H, Khabazkhoob M. Global and regional estimates of prevalence of refractive errors: systematic review and meta-analysis. J Curr Ophthalmol. 2018;30(1):3–22. doi:10.1016/j.joco.2017.08.009
21. Fozailoff A, Tarczy-Hornoch K, Cotter S, et al. Prevalence of astigmatism in 6- to 72-month-old African American and hispanic children: the multi-ethnic pediatric eye disease study. Ophthalmology. 2011;118(2):284–293. doi:10.1016/j.ophtha.2010.06.038
22. Fan DS, Rao SK, Cheung EY, Islam M, Chew S, Lam DS. Astigmatism in Chinese preschool children: prevalence, change, and effect on refractive development. Br J Ophthalmol. 2004;88(7):938–941. doi:10.1136/bjo.2003.030338
23. Clementi M, Angi M, Forabosco P, Di Gianantonio E, Tenconi R. Inheritance of astigmatism: evidence for a major autosomal dominant locus. Am J Hum Genet. 1998;63(3):825–830. doi:10.1086/302014
24. Lee KE, Klein BE, Klein R, Fine JP. Aggregation of refractive error and 5-year changes in refractive error among families in the Beaver Dam eye study. Arch Ophthalmol. 2001;119(11):1679–1685. doi:10.1001/archopht.119.11.1679
25. Wiggins NP, Daum KM. Visual discomfort and astigmatic refractive errors in VDT use. J Am Optom Assoc. 1991;62(9):680–684.
26. Wang S, Ma W, Yuan Z, et al. Association between obesity indices and type 2 diabetes mellitus among middle-aged and elderly people in Jinan, China: a cross-sectional study. BMJ Open. 2016;6(11):e012742. doi:10.1136/bmjopen-2016-012742
27. Cheung N, Wong TY. Obesity and eye diseases. Surv Ophthalmol. 2007;52(2):180–195. doi:10.1016/j.survophthal.2006.12.003
28. Gaml-Sørensen A, Thomsen AH, Tøttenborg SS, et al. Maternal pre-pregnancy BMI and reproductive health in adult sons: a study in the Danish national birth cohort. Hum Reprod. 2024;39(1):219–231. doi:10.1093/humrep/dead230
29. McKay TB, Priyadarsini S, Karamichos D. Sex hormones, growth hormone, and the cornea. Cells. 2022;11(2):224. doi:10.3390/cells11020224
30. Karamichos D, Escandon P, Vasini B, et al. Anterior pituitary, sex hormones, and keratoconus: beyond traditional targets. Prog Retin Eye Res. 2022;88:101016. doi:10.1016/j.preteyeres.2021.101016
31. Diress M, Yeshaw Y, Bantihun M, et al. Refractive error and its associated factors among pregnant women attending antenatal care unit at the University of Gondar comprehensive specialized hospital, Northwest Ethiopia. PLoS One. 2021;16(2):e0246174. doi:10.1371/journal.pone.0246174
32. Kalogeropoulos D, Sung VC, Paschopoulos M, Moschos MM, Panidis P, Kalogeropoulos C. The physiologic and pathologic effects of pregnancy on the human visual system. J Obstet Gynaecol. 2019;39(8):1037–1048. doi:10.1080/01443615.2019.1584891
33. Faro ACN, Pereira-Gurgel VM, Salvatori R, et al. Ocular findings in adult subjects with an inactivating mutation in GH releasing hormone receptor gene. Growth Horm IGF Res. 2017;34:8–12. doi:10.1016/j.ghir.2017.04.002
34. Namba H, Sugano A, Murakami T, et al. Age-related changes in astigmatism and potential causes. Cornea. 2020;39(Suppl 1):S34–s38. doi:10.1097/ICO.0000000000002507
35. Friling R, Weinberger D, Kremer I, Avisar R, Sirota L, Snir M. Keratometry measurements in preterm and full term newborn infants. Br J Ophthalmol. 2004;88(1):8–10. doi:10.1136/bjo.88.1.8
36. Lee EY, Yoon KH. Epidemic obesity in children and adolescents: risk factors and prevention. Front Med. 2018;12(6):658–666. doi:10.1007/s11684-018-0640-1
37. Heslehurst N, Vieira R, Akhter Z, et al. The association between maternal body mass index and child obesity: a systematic review and meta-analysis. PLoS Med. 2019;16(6):e1002817. doi:10.1371/journal.pmed.1002817
38. Shin D, Lee KW, Song WO. Pre-pregnancy weight status is associated with diet quality and nutritional biomarkers during pregnancy. Nutrients. 2016;8(3):162. doi:10.3390/nu8030162
39. Lyle WM, Grosvenor T, Dean KC. Corneal astigmatism in Amerind children. Am J Optom Arch Am Acad Optom. 1972;49(6):517–524. doi:10.1097/00006324-197206000-00010
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.