Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 12
Association between heterozygote Val92Met MC1R gene polymorphisms with incidence of melasma: a study of Javanese women population in Yogyakarta
Authors Suryaningsih BE ![]() , Sadewa AH, Wirohadidjojo YW, Soebono H
, Sadewa AH, Wirohadidjojo YW, Soebono H ![]()
Received 20 February 2019
Accepted for publication 20 May 2019
Published 2 July 2019 Volume 2019:12 Pages 489—495
DOI https://doi.org/10.2147/CCID.S206115
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Betty Ekawati Suryaningsih1,2 Ahmad Hamim Sadewa,3 Yohanes Widodo Wirohadidjojo,2 Hardyanto Soebono2
1Department of Dermatovenereology, Faculty of Medicine Islamic Indonesia University, Yogyakarta, Indonesia; 2Department of Dermatovenereology, Faculty of Medicine Universitas Gadjah Mada, Yogyakarta, Indonesia; 3Department of Biochemistry, Faculty of Medicine, Universitas Gadjah Mada, Yogyakarta, Indonesia
Introduction: Melasma is an acquired hypermelanosis of the face. The pathogenesis of melasma is multifactorial and may be caused by interactions between genetics and the environment. Research has shown that skin pigmentation is regulated by the Melanocortin-1 Receptor gene (MC1R). In Japanese populations, Val92Met and Arg163Gln genotypes of MC1R gene polymorphisms are associated with freckles and lentigo solaris, because they have skin types II–III, but for Indonesians who are skin type IV, hyperpigmentation disorders are often melasma.
Purpose: This study aimed to identify the association between Val92Met and Arg163Gln genotypes of MC1R gene polymorphisms with the incidence of melasma in a Javanese women population.
Patients and methods: This study used unmatched case-control design, conducted by clinical examination and questionnaire. Data were analyzed with Chi-squared test and Odds Ratio (OR).
Results: This study evaluated 158 Javanese women from 18–60 years old with 79 case and 79 control subjects. The genotype of Val92Met was found more common in melasma subjects than in non-melasma (p=0.005) with (OR2.53; 95% CI:1.21–5.29). By using a bivariate test we showed sun exposure and family history of melasma were risk factors for melasma (OR:1.99; 95% CI:1.04–3.78) and (OR:35.32; 95% CI:10.25–121.70). However, genotype of Arg163Gln was not a risk factor for the incidence of melasma (OR: 0.86; 95% CI:0.39–1.89).
Conclusion: The findings showed Val92Met genotypes, sun exposure and family history were risk factors for melasma incidence. This is the first study on incidence of melasma in an Indonesian population and contributes to ongoing efforts to understand the mechanisms of melasma.
Keywords: Arg163Gln, MC1R, melasma, Val92Met, UV exposure
Introduction
Melasma is a hyperpigmentation disorder with a symmetrical distribution mostly over the face, which occurs in women of reproductive age and the darker-skin or in individuals who have the skin types III–V according to Fitzpatrick criteria, although it can also occur in men.1,2 The pathogenesis of melasma is not fully understood, because it is highly multifactorial. Genetics and ultraviolet (UV) exposure are the main factors in the development of melasma besides hormonal and cosmetic factors.3,4 Some studies such as one in Tunisia showed the role of genetics was found in 10–70% of the population who suffer from melasma and have a history of skin diseases in their families.5 Another study reported that 50% of individuals with darker skin also had a family member who suffers from melasma.6 Melasma often has a negative effect on the quality of life (QoL) of the sufferer’s social interaction and also causes stress on daily activities due to the lack of self-confidence because of their appearance. Degree of severity of melasma can be calculated using the melasma area severity index (MASI). Higher MASI score can measure how the condition affects the QoL of melasma sufferers.7–9
Human skin color is determined by eumelanin and pheomelanin pigment and there are two types of melanin in human epidermis, the brownish-black eumelanin and the reddish yellow pheomelanin and is also affected by the environment where an individual-lives. The pigmentation system is regulated by MC1R which controls the phenotype of human skin color by binding α MSH, or ACTH results in stimulation of cAMP and adenylate cyclase, which are triggers to activate tyrosinase in the melanin synthesis pathway. MC1R is a gene which has many polymorphisms.10,11 In Southeast Asia, the MC1R gene polymorphisms high frequencies are Val92Met and Arg163Gln, and this is the reason for choosing this gene in this study. Studies about pigment disorders in Asia are less frequently done compared to those in Europe.12,13
Several case control studies about melasma have been performed, but there is no study of genetic polymorphisms as a risk factor for the incidence and severity of melasma. This research is an unmatched case control study focused on the polymorphisms Val92Met and Arg163Gln of the MC1R gene to identify their association as a risk factor of melasma.
Materials and methods
This study was approved by the Medical and Health Research Ethics Committee of the Faculty of Medicine Universitas Gadjah Mada and Dr Sardjito Hospital with approval number (KE/FK/462/EC/2016). All participants provided written informed consent in this study. The study was performed in accordance with the 1964 Declaration of Helsinki and its successive updates and the recommendations on Good Clinical Practice ICH E6 (R1) 2015. An unmatched case control study was conducted between May 2016 and March 2017. Subjects were recruited from the Dermato-Venereology Clinic of Dr Sardjito Hospital and Be Queen Skin Care Clinic in Yogyakarta, Indonesia. Both groups were interviewed with a standardized questionnaire including the onset, UV exposure and family history of melasma. The subjects of this study were adult Javanese women aged 18–60 years old in Yogyakarta who had melasma for the case group and who were without melasma for the control group.
Melasma severity was estimated using the Melasma Area Severity Index (MASI) scores. MASI scoring assesses three factors: The involved area (A), Hyperpigmentation (D), and Homogeneity (H), based on inspection of facial skin. The face is divided into four areas: Forehead (F); Malar Right (MR); Malar Left (ML) and Chin (C) where each area represents: 30% forehead; 30% right cheek; 30% left cheek and 10% for chin. The four areas involved are rated from 0 to 6 (0= unaffected; 1=<10%; 2=10–29%; 3=30−49%; 4=50–69%; 5=70–89% and 6=90–100%). Hyperpigmentation and homogeneity are assigned a scale from 0 to 4 (0= absent; 1= slight; 2= mild; 3= marked and 4= maximum).14 The final result of MASI is the sum of hyperpigmentation and homogeneity multiplied by the involved facial area into a total score from 0 to 48.9,15
The exclusion criteria for this study were the use of hormonal contraceptives, pregnancy, having other pigmentation disorders beside melasma in the skin, and the use of whitening cream for the last two weeks prior to the study Kim et al.16 We examined the skin in both groups with Bombtech Skin Diagnosis A-ONE® (Korea) to identify the skin’s condition and the area of melasma in the case group, and a mexameter® MX18 courage-Khazaka (Germany) was used to measure skin pigmentation and calculate the MASI score.
As much as 3 mL of venous blood were taken from the subjects and stored in EDTA for DNA extraction with a Wizard® kit (Promega Corporation, Fitchburg, WI, USA). Polymerase chain reaction (PCR) was performed using a platinum® PCR Super Mix kit (Invitrogen, Thermo Fisher Scientific, Waltham, MA, USA) in the Biochemistry Laboratory Faculty of Medicine Universitas Gadjah Mada, Yogyakarta, Indonesia. Gene sequencing for MC1R was performed in the commercial laboratory of 1st BASE DNA in Malaysia.
We used the Sanger method for sequencing subject DNA with an Applied Biosystems (ABI, Thermo Fisher Scientific, Waltham, MA, USA) 3130 xl Genetic Analyzer to detect rs2228479 (Val92Met) and rs885479 (Arg163Gln) using the following primers. It is found from the finding through gene atlas: (F) 5′-GAA CCG GAA CCT GCA CTC A-3′ (R) 5′-GCC AGG AAG AAG ACC ACG AG-3′. A Molecular Evolutionary Genetic Analysis-7 (MEGA-7) software was used to analyze the sequencing data of Val92Met and Arg163Gln as detailed by Kumar et al.17
Data analysis
Data were analyzed by the chi-square test with p<0.05. To associate the genes and melasma, this study calculated Odds Ratio (OR) with 95% CIs. Estimated allele and genotype frequencies were calculated by counting expected value based on formula of p2 +2pq +q2=1. Hardy-Weinberg was performed and the results showed that the frequency distribution of both polymorphisms were in accordance with HWE (p>0.05). Since the two single nucleotide polymorphisms (SNPs) analyzed in this study were very closely located in the same locus, we did not analyze Linkage Disequilibrium and haplotype. We choose the chi-square test because the total number of subjects >40 and the expected observed in each cell is greater than five.
Results
A total of 158 women were recruited in this study and fulfilled the inclusion criteria, resulting in 79 melasma case subjects and 79 non-melasma subjects for the control group. The melasma and control groups had a mean age ± SD of 40.6±6.45 years and 38.5±7.48 years (p=0.146). They were all skin type IV. Historically, 53 (67.09%) of the melasma group had daily sun exposure for more than 60 minutes (81.51±21.94), compared to 40 (50.63%) in the control group (48.75±9.11; p=0.036). We found that 46 (62.03%) of the melasma group had a family history of melasma, compared to 33 (41.77%) of those without melasma (p=0.01).
The characteristics of the subjects are presented in Table 1.
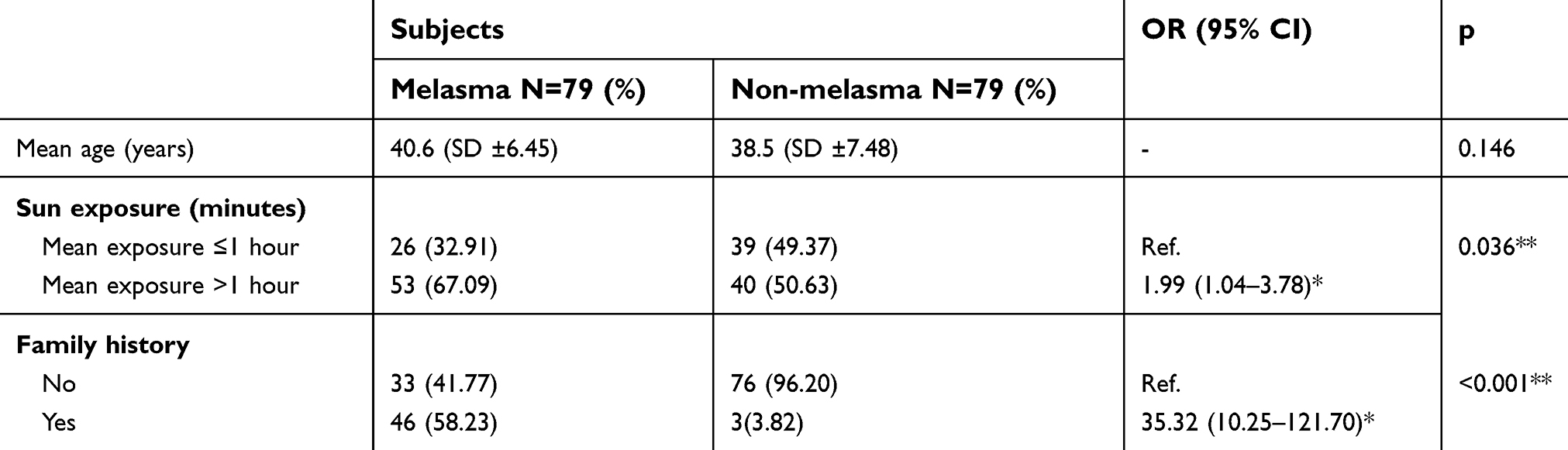 |
Table 1 Characteristics of age, sun exposures, and family history of the two groups: with melasma and without melasma (n=158) |
Sequencing result of genes MC1R Val92Met and Arg163Gln
The electropherogram showed substitution of Guanosine (G) to Adenosine (A) at codon 92 (Val92Met) and G to A at codon 163 (Arg163Gln). The sequencing results of the heterozygote Val92Met genotype of the MC1R gene polymorphisms and the sequencing results of the heterozygote Arg163Gln genotype of the MC1R gene polymorphisms are shown in Figures 1 and 2.
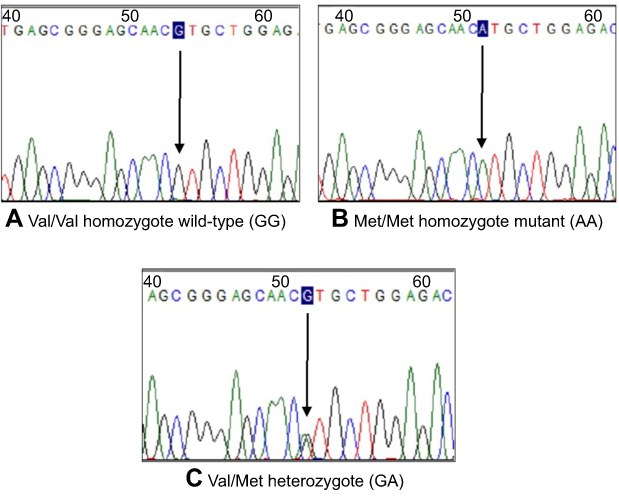 |
Figure 1 Sequencing results of the heterozygote Val92Met genotype of the MC1R gene polymorphisms. Notes: The MC1R Val92Met polymorphism involved amino acid substitution from Valine to Methonine at codon 92. (A) Wild-type (homozygote) for the Val/Val genotype (Valine/Valine-GG). (B) Homozygote mutant for Met/Met genotype (Methionine/Methionine-AA). (C) Heterozygote variant for the Val/Met genotype (Valine/methionine-GA). |
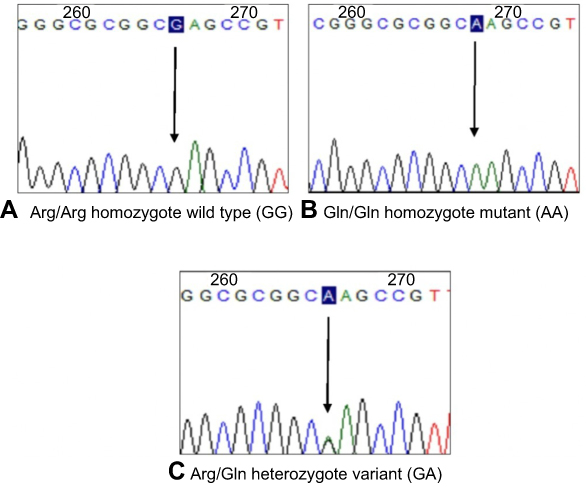 |
Figure 2 Sequencing results of the heterozygote Arg163Gln genotype of the MC1R gene polymorphisms. Notes: The MC1R Arg163 Gln polymorphism involved amino acid substitution from Arginine to Glutamine at codon 163. (A) Wild-type (homozygote) for the Arg/Arg genotype (Arginine/Arginine-GG). (B) Homozygote mutant for the Gln/Gln genotype (Glutamine/Glutamine-AA). (C) Heterozygote variant for the Arg/Gln genotype (Arginine/Glutamine-GA). |
The calculation of the polymorphisms MC1R genotype frequencies revealed the presence of the Val/Met genotype in 52 subjects of the melasma group and 35 of the non-melasma group, with the presence of the Val/Val in 17 and Met/Met in 10 of the melasma group and 29 and 15 of the non-melasma group, respectively. The frequency of the Arg/Gln genotype in the melasma group was 43 subjects and 40 in the non-melasma group, and the presence of Arg/Arg and Gln/Gln was 20 and 16 in the melasma group and 16 and 23 in the non melasma groups, respectively (Table 2).
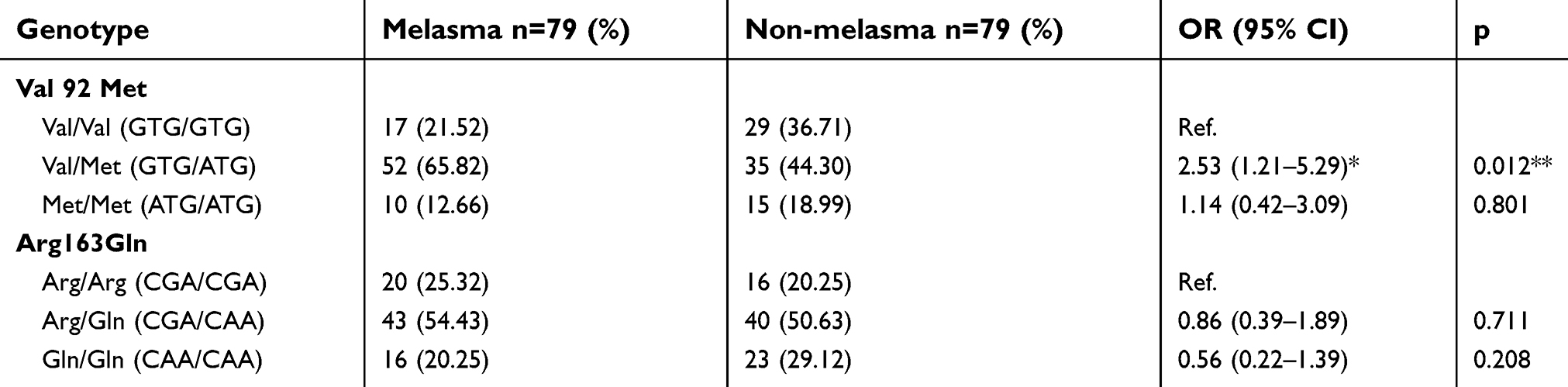 |
Table 2 Association between Val92Met and Arg163Gln genotypes of MC1R gene polymorphisms and melasma |
Data analysis showed the genotype of Val/Met was a risk factor for melasma with OR: 2.53; 95% CI:1.21–5.29. Meanwhile, the heterozygote of Arg163Gln was not associated with incidence of melasma with OR: 0.86; 95% CI: 0.39–1.89). These results show that the frequency of the heterozygote of Val/Met and Arg/Gln was greater in the melasma group than non-melasma group, whereas the homozygote was more common in the non-melasma group.
Discussion
Melasma pathogenesis is multifactorial; the two most important factors are UV exposure and genetics. One study in Iran showed a relationship between skin type and melasma, indicating that those who have skin type III–IV are more likely to suffer melasma.18,19 A study in nine countries showed that more than 80% of melasma cases occurred in skin type III–IV, consistent with the Fitzpatrick study of skin color type III–IV are more prone to have melasma, which showed that these skin types are more likely to have melasma than fair-skinned subjects.20 The melanosomes of fair-skinned individuals are predominantly located in melanocytes at phase II–III and in the keratinocyte at phase III, with faster degradation of melanosomes and larger quantities of pheomelanin. Conversely, in the darker skin types (IV–V), melanosomes are degraded more slowly and eumelanin becomes dominant because the melanosomes are predominantly located both in the melanocyte and keratinocyte at phase IV.21
A study on 324 women subjects with melasma found that 48% had a family history of melasma, and almost 90% had darker skin types.20 One study that related to the existence of family history with melasma was done in Brazil. As many as 56.3% from 302 patients have family history with melasma.6 In another study in the sub-Himalayan area, as many as 75% from 100 patients also had a family history with melasma.20 Some epidemiology studies about the effect of sun exposure on the incidence of melasma have been performed in a number of countries and in different populations such as in Singapore, India, Iran, Brazil, and France. From those studies results showed the negative effect due to UV exposure, and how the impact can be the trigger of melasma or even worsen the melasma itself. The effect varied depending on the duration of the exposure from the UV.4,14,18,21,22 The accumulation of sun exposure in individuals whose activity is outside home was calculated by the duration of sun exposure and was a risk factor for the incidence of melasma.23 A study in Basrah about the association of sun exposure to the incidence of melasma found that from 196 subjects there were 117 subjects exposed to the sun for 2–4 hours a day who had melasma.13 This result is similar to the study in the sub-Himalayan population that found that 68% of subjects who were exposed to the sun for 2–4 hours a day also had melasma.20
The 79 subjects who suffered from melasma had skin type IV, longer UV exposures, and they were more likely to have a family history of melasma than the non-melasma subjects. The hypothesized mechanism for this finding is that individuals with skin type IV produce abundant pigment along with high UV exposure, which is the main triggering factor of melasma. UV exposure stimulates melanocyte proliferation and melanogenesis, resulting in an increase of melanin synthesis inside the melanosome, which leads to hyperpigmentation or hyperactivity of epidermal melanin units in individuals with skin type IV. The current study found that sun exposure is a risk factor for melasma with OR: 1.99; 95% CI: 1.04–3.78) and showed that 62.03% of the case group had a positive family history for the same disease, suggesting that a positive family history is a risk factor for melasma with OR 35.32; 95% CI: 10.25–121.70). Family history results support the findings that in addition to environmental factors genetics contribute to the incidence of melasma in this study.
MC1R is a highly polymorphic gene that plays a role in the regulation of pigmentation, where the variants produced depend on the region the individual comes from. MC1R is located on chromosomal region 16q24.3 and it encodes a single exon of 954 bp and a protein of 317 amino acids.23 Among Asians, the most common polymorphisms are Val92Met and Arg163Gln. In Japan, MC1R was shown to be associated with freckles and lentigo solaris.13,23 MC1R regulates eumelanin and pheomelanin pigments in melanocytes, which are mediated by the α-MSH transduction signal to activate adenylyl cyclase, resulting in an increase of cyclic adenosine monophosphate (cAMP) and triggering tyrosinase activity cascades, which increase the ratio of eumelanin to pheomelanin products.24,25 In one in vitro study with a total of 134 subjects, heterozygous Val92Met was more prevalent in brown-skinned (50.75%) than in fair-skinned individuals (28.96%), while in 66 subjects, Arg163Gln was more prevalent in brown-skinned individuals (60.61%) than in fair-skinned individuals (24.24%).26,27 In this study we found that the frequencies of heterozygote Val92Met genotype was higher in melasma cases. This result supports the theory that heterozygote individuals with the MC1R gene tend to have dark melanin pigment which is a risk factor of melasma. This finding is supported by the fact that Indonesian populations have strong UV exposure, especially in Yogyakarta, and all of the subjects have skin type IV, which has a greater eumelanin-to-pheomelanin ratio, and this combination of pigment ratio with UV exposure may be the main cause of melasma.
The presence of the substitution of G to A at codon 92 causes a change from the amino acid valine (GTG) into methionine (ATG), further decreasing MC1R affinity for α-MSH up to two times more than that of the wild type.28 While the G-to-A base change at codon 163 causes the substitution of the amino acid arginine (CGA) for glutamine (CAA). MC1R gene polymorphisms may cause decreases in receptor function, either at the α-MSH binding level or cAMP signaling level, resulting in a quantitative shift of eumelanin synthesis to pheomelanin, which is potentially mutagenic.28,29 The results were possibly affected by the impaired function of the MC1R gene. The effect of amino acid substitutions on the resulting protein causes an excessive pheomelanin synthesis. In this study, all subjects had skin type IV where eumelanin is high, which can be a protection against sun exposure, although the decreasing function of MC1R did not affect the ratio of pheomelanin to eumelanin. These polymorphisms in the study population from Indonesia, especially in Javanese, appears to be a contributing cause of melasma, in addition to the photoaging mechanism due to the excessive sun exposure reported in this study.
Conclusion
This research is the first study on the incidence of melasma in Indonesia and contributes to ongoing efforts to understand the mechanisms of melasma. We found associations between the frequency of the Val92Met genotype and the incidence of melasma, with the heterozygote genotype Val/Met, sun exposures and family history as risk factors for melasma. Sun exposure and family history were aggravating factors associated with melasma. However, the mechanism of how the Val/Met genotype contributes to melasma is still unclear. Further studies should be conducted to provide a cellular signaling analysis to assess the MC1R genes response to melanocyte stimulating hormone in order to better understand the triggering mechanisms of melasma.
Acknowledgments
This study was supported by the Doctoral Research Funding of the Ministry of Research and Technology of the Republic of Indonesia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hexsel D, Lacerda DA, Cavalcante AS, et al. Epidemiology of melasma in Brazilian patients: a multicenter study. Int J Dermatol. 2013;53:440–444. doi:10.1111/j.1365-4632.2012.05748.x
2. Ritter CG, Fiss DVC, Borges da Costa JAT, de Carvalho RR, Bauermann G, Cestari TF. Extra-facial melasma: clinical, histopathological, and immunohistochemical case-control study. J Eur Acad Dermatol Venereol JEADV. 2013;27:1088–1094. doi:10.1111/j.1468-3083.2012.04655.x
3. Chatterjee M, Vasudevan B. Recent advances in melasma. Pigment Int. 2014;1:70–80. doi:10.4103/2349-5847.147044
4. Vázquez M, Maldonado H, Benmamán C, Sánchez JL. Melasma in men. A clinical and histologic study. Int J Dermatol. 1988;27:25–27. doi:10.1111/j.1365-4362.1988.tb02329.x
5. Guinot C, Cheffai S, Latreille J, et al. Aggravating factors for melasma: a prospective study in 197 Tunisian patients. J Eur Acad Dermatol Venereol. 2010;24:160–169.
6. Tamega ADA, Miot LDB, Bonfietti C, Gige TC, Marques MEA, Miot HA. Clinical patterns and epidemiological characteristics of facial melasma in Brazilian women: clinical patterns and epidemiology of melasma. J Eur Acad Dermatol Venereol. 2013;27:151–156. doi:10.1111/j.1468-3083.2011.04430.x
7. Ali R, Aman S, Nadeem M, Kazmi AH. Quality of life in patients of melasma. J Pak Assoc Dermatol. 2016;23:143–148.
8. Guarneri F. Etiopathogenesis of melasma. Pigment Disorder. 2014;1:2376–2427.
9. Tay EY, Gan EY, Tan VWD, et al. Pilot study of an automated method to determine melasma area and severity index. Br J Dermatol. 2015;172:1535–1540. doi:10.1111/bjd.13699
10. Abdel-Malek ZA, Knittel J, Kadekaro AL, Swope VB, Starner R. The melanocortin 1 receptor and the UV response of human melanocytes—a shift in paradigm. Photochem Photobiol. 2008;84:501–508. doi:10.1111/j.1751-1097.2008.00294.x
11. Videira IFDS, Moura DFL, Magina S. Mechanisms regulating melanogenesis. An Bras Dermatol. 2013;88:76–83. doi:10.1590/S0365-05962013000100009
12. Motokawa T, Kato T, Hashimoto Y, Katagiri T. Effect of Val92Met and Arg163Gln variants of the MC1R gene on freckles and solar lentigines in Japanese. Pigment Cell Res. 2007;20:140–143. doi:10.1111/pcr.2007.20.issue-2
13. Motokawa T, Kato T, Hashimoto Y, Takimoto H, Yamamoto H, Katagiri T. Polymorphism patterns in the promoter region of the MC1R gene are associated with development of freckles and solar lentigines. J Invest Dermatol. 2008;128:1588–1591. doi:10.1038/sj.jid.5701192
14. Pandya A, Berneburg M, Ortonne J-P, Picardo M. Guidelines for clinical trials in melasma. Pigmentation disorders academy. Br J Dermatol. 2006;156:21–28. doi:10.1111/bjd.2006.156.issue-s1
15. Majid I, Haq I, Imran S, Keen A, Aziz K, Arif T. Proposing melasma severity index: a new, more practical, office-based scoring system for assessing the severity of melasma. Indian J Dermatol. 2016;61:39–44. doi:10.4103/0019-5154.174024
16. Kim HE, Kim CY, Lee SE, Kang YH. The vascular characteristics of the melasma. J Dermatol Sci. 2007;46:111–116. doi:10.1016/j.jdermsci.2007.01.009
17. Kumar S, Stecher G, Tamura K. MEGA 7: molecular evolutionary genetics analysis version 7.0 for bigger datasets. Mol Biol Evol. 2016;33:1870–1874. doi:10.1093/molbev/msw005
18. Moin A, Jabery Z, Fallah N. Prevalence and awareness of melasma during pregnancy. Int J Dermatol. 2006;45:285–288. doi:10.1111/ijd.2006.45.issue-3
19. Sonthalia S, Sarkar R. Etiopathogenesis of melasma. Pigment Int. 2015;2:21–27. doi:10.4103/2349-5847.159389
20. Ortonne J, Arellano I, Berneburg M, et al. A global survey of the role of ultraviolet radiation and hormonal influences in the development of melasma. J Eur Acad Dermatol Venereol. 2009;23:1254–1262. doi:10.1111/j.1468-3083.2009.03295.x
21. Cichorek M, Wachulska M, Stasiewicz A, Tymińska A. Skin melanocytes: biology and development. Adv Dermatol Allergol Dermatol Alergol. 2013;30:30–41. doi:10.5114/pdia.2013.33376
22. Halder S, Halder A, Nag SC, Rajesh D, Sarkar P. Melasma in the people of Sub-Himalayan region of Eastern India. J Pak Assoc Dermatol. 2016;23:139–142.
23. Yamaguchi K, Watanabe C, Kawaguchi A, et al. Association of melanocortin 1 receptor gene (MC1R) polymorphisms with skin reflectance and freckles in Japanese. J Hum Genet. 2012;57:700–708. doi:10.1038/jhg.2012.96
24. Bastiaens M, Ter Huurne J, Gruis N, et al. The melanocortin-1-receptor gene is the major freckle gene. Hum Mol Genet. 2001;10:1701–1708. doi:10.1093/hmg/10.16.1701
25. Garcia-Borron JC, Sanchez-Laorden BL, Jimenez-Cervantes C. Melanocortin-1 receptor structure and functional regulation. Pigment Cell Res. 2005;18:393–410.
26. Beaumont KA, Shekar SL, Newton RA, et al. Receptor function, dominant negative activity and phenotype correlations for MC1R variant alleles. Hum Mol Genet. 2007;16:2249–2260. doi:10.1093/hmg/ddm177
27. Scott MC, Wakamatsu K, Ito S, et al. Human melanocortin 1 receptor variants, receptor function and melanocyte response to UV radiation. J Cell Sci. 2002;115:2349–2355.
28. Dessinioti C, Antoniou C, Katsambas A, Stratigos AJ. Melanocortin 1 receptor variants: functional role and pigmentary associations: photochemistry and photobiology. Photochem Photobiol. 2011;87:978–987. doi:10.1111/j.1751-1097.2011.00970.x
29. Rouzaud F, Kadekaro AL, Abdel-Malek ZA, Hearing VJ. MC1R and the response of melanocytes to ultraviolet radiation. Mutat Res Mol Mech Mutagen. 2005;571:133–152. doi:10.1016/j.mrfmmm.2004.09.014
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.