Back to Journals » Drug Design, Development and Therapy » Volume 20
Association Between Diclofenac Sodium Use and Reduced Cycle Cancellation from Premature Ovulation in Women with Diminished Ovarian Reserve Undergoing IVF: A Retrospective Cohort Study
Authors Song JY, Ma YJ ![]() , Cao XL, Sun ZG
, Cao XL, Sun ZG ![]()
Received 17 October 2025
Accepted for publication 11 January 2026
Published 14 January 2026 Volume 2026:20 575150
DOI https://doi.org/10.2147/DDDT.S575150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Solomon Tadesse Zeleke
Jing-Yan Song,1,* Ying-Jie Ma,2,* Xian-Ling Cao,2,3 Zhen-Gao Sun1,2
1The First Clinical College, Shandong University of Traditional Chinese Medicine, Jinan, Shandong, People’s Republic of China; 2Reproductive Center of Integrated Medicine, The Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Jinan, Shandong, People’s Republic of China; 3Section on Integrative Physiology and Metabolism, Joslin Diabetes Center, Harvard Medical School, Boston, MA, USA
*These authors contributed equally to this work
Correspondence: Xian-Ling Cao, Reproductive Center of Integrated Medicine, The Affiliated Hospital of Shandong University of Traditional Chinese Medicine, 42 Wenhua West Road, Lixia District, Jinan, Shandong, People’s Republic of China, Email [email protected] Zhen-Gao Sun, Reproductive Center of Integrated Medicine, The Affiliated Hospital of Shandong University of Traditional Chinese Medicine, 42 Wenhua West Road, Lixia District, Jinan, Shandong, People’s Republic of China, Email [email protected]
Purpose: To evaluate whether diclofenac sodium administration reduces premature ovulation and improves in vitro fertilization (IVF) outcomes in patients with diminished ovarian reserve (DOR).
Patients and Methods: Retrospective cohort study conducted at a single academic reproductive center from January 2022 to March 2025. We included women with DOR (anti-Müllerian hormone [AMH] < 1.1 ng/mL, antral follicle count [AFC] < 5) undergoing autologous IVF cycles with single dominant follicle development. A total of 1164 cycles from 616 patients were analyzed, comparing 382 cycles with diclofenac sodium 75mg daily from trigger day to oocyte retrieval versus 782 cycles without treatment. The primary endpoint was cycle cancellation due to premature ovulation. Secondary endpoints included oocyte retrieval success, fertilization rates, embryo outcomes, and clinical pregnancy rates. Generalized estimating equation (GEE) models with multivariable adjustment were used to account for correlation between multiple cycles from the same patient. A sensitivity analysis restricted to first cycles per patient (n=616) was performed using logistic regression to validate primary findings.
Results: Diclofenac sodium significantly reduced cycle cancellation due to premature ovulation (7.3% vs 19.8%, adjusted odds ratio [OR] 0.39, 95% confidence interval [CI] 0.21– 0.73, P=0.003) and decreased the proportion of cycles with no oocytes retrieved (21.8% vs 27.1%, adjusted OR 0.54, 95% CI 0.34– 0.84, P=0.007). Normal fertilization rates were higher in the diclofenac sodium group (77.5% vs 69.8%, P=0.041), though this lost significance after adjustment (P=0.184). The proportion of cycles without viable embryos was comparable between groups (42.3% vs 41.8%, P=0.727). Among limited fresh embryo transfers (n=124), clinical pregnancy (19.2% vs 11.2%, P=0.847) and live birth rates (15.4% vs 8.2%, P=0.948) were similar. The sensitivity analysis using first cycles per patient (n=616) confirmed these findings, showing a 47% reduction in premature ovulation odds with diclofenac sodium (adjusted OR 0.53, 95% CI 0.29– 0.94, P=0.031).
Conclusion: Diclofenac sodium is associated with reduced premature ovulation and improved oocyte retrieval success in DOR patients, though embryonic and pregnancy outcomes remain similar. These observational findings require validation through prospective randomized controlled trials with adequate power to assess cumulative reproductive outcomes.
Keywords: diclofenac sodium, premature ovulation, in vitro fertilization, diminished ovarian reserve, oocyte retrieval
Introduction
Premature ovulation is a major challenge in assisted reproductive technology (ART), especially for patients with DOR. This occurs when ovulation happens before the scheduled oocyte retrieval, leading to cycle cancellation and significant emotional and financial burden for patients.1,2 The incidence of premature ovulation varies widely across different patient populations and treatment protocols, with rates up to 20% in certain high-risk groups, significantly affecting ART success rates and causing treatment failure.3–5
The mechanism of ovulation involves multiple molecular steps, with prostaglandins playing a key role. Prostaglandin E2 (PGE2), produced by granulosa cells, stimulates the production of follicular matrix metalloproteases (MMPs), which break down the cumulus complex around the oocyte.6 This process causes the cumulus complex to separate from the follicular wall and leads to follicle rupture, releasing the follicular fluid and oocyte into the fallopian tube.7,8 Understanding this prostaglandin pathway has made cyclooxygenase (COX) inhibitors useful targets for preventing premature ovulation in ART.9
Non-steroidal anti-inflammatory drugs (NSAIDs), including diclofenac sodium, work by blocking cyclooxygenase enzymes, which reduces prostaglandin production.10,11 This mechanism has been used in reproductive medicine to delay ovulation, especially in natural cycle IVF and mild stimulation protocols where gonadotropin releasing hormone (GnRH) analogues are not commonly used. The idea of using NSAIDs as a “rescue strategy” was first reported by Nargund and Wei in 1996, who successfully used indomethacin to delay ovulation when an early luteinizing hormone (LH) surge occurred.12
A recent controlled study has provided strong evidence for the effects of NSAIDs in delaying ovulation. Von Wolff et al showed that ibuprofen (400 mg three times daily) significantly delayed ovulation in 84.6% of patients compared to 20.0% in controls (adjusted OR 22.72, 95% CI 5.77–115, P<0.001).13 Importantly, this intervention did not compromise oocyte or embryo quality, with 90.9% of aspirated follicles yielding mature metaphase II oocytes and maintaining high fertilization rates (95.2%). These findings showed the clinical value of NSAIDs in preventing premature ovulation without affecting reproductive outcomes.
However, there is debate about which NSAIDs are most effective for delaying ovulation and whether their effects are dose-dependent or timing-specific. While meloxicam has shown strong effects in delaying ovulation and has been suggested for emergency contraception,14 studies with other non-selective NSAIDs have shown variable results. Some large-scale studies based on questionnaires and daily diaries have not found clear effects of NSAIDs on fertility outcomes,15,16 while retrospective clinical studies in ART have shown benefits for different drugs including indomethacin and diclofenac.17,18
The clinical use of NSAIDs for ovulation control has mainly been reported in retrospective studies with heterogeneous patient populations, treatment protocols, and outcome measures. Kadoch et al reported lower spontaneous ovulation rates with indomethacin in modified natural cycle IVF,17 while Kawachiya et al demonstrated similar benefits with short-term, low-dose NSAID use in natural cycle IVF.18 Most existing evidence derives from natural cycle IVF or minimal stimulation protocols, with limited data on high-risk populations such as patients with DOR undergoing various stimulation protocols.19
Patients with DOR, typically defined by reduced AFC (< 5) and low AMH (< 1.1 ng/mL), represent a challenging subset of the ART population with significantly compromised reproductive outcomes.2,20 These patients often present with single dominant follicle development regardless of the stimulation protocol employed, making each treatment cycle critically important. DOR is becoming more common with delayed childbearing, affecting about 9–24% of women undergoing ART procedures.21 The limited number of retrievable oocytes in these patients amplifies the impact of premature ovulation, as the loss of even a single follicle can result in complete cycle cancellation. Despite this importance, specific treatments to prevent premature ovulation in DOR patients using different stimulation protocols have not been well studied.
Diclofenac sodium has several advantages as a drug to delay ovulation in this population. As a strong NSAID with known COX-blocking effects, diclofenac sodium has stronger anti-inflammatory effects than many other NSAIDs, with a long half-life allowing for once-daily dosing.22 Its favorable pharmacokinetic profile, with rapid absorption and predictable plasma concentrations, makes it suitable for standardized administration from trigger day through oocyte retrieval. The standard dose of 75 mg daily for three days is practical for clinical use while keeping patients compliant and reducing gastrointestinal side effects often seen with higher-dose NSAID treatments.23
There are several reasons to study diclofenac sodium in DOR patients using different stimulation protocols. First, DOR patients have a higher risk of premature ovulation, so effective prevention is clinically important. Second, these patients have limited eggs and few treatment chances, so each cycle must be optimized.24,25 Third, DOR patients usually develop only one follicle regardless of protocol, making them ideal for studying ovulation delay effects. Fourth, since our center has been using diclofenac sodium as prevention since 2024, we need evidence-based evaluation of its effectiveness and safety in different treatments.
Current evidence about NSAID use for ovulation control comes from different patient populations using various drugs, doses, and treatment protocols. The differences between studies make it difficult to establish clear clinical recommendations, particularly for specific high-risk groups undergoing different stimulation protocols. Furthermore, most prospective studies have been conducted in natural cycles with patients who have normal ovarian reserve, limiting the applicability of findings to DOR patients where different hormonal patterns and follicular characteristics may affect drug effectiveness.26
Therefore, we conducted this retrospective cohort study to evaluate the effectiveness of diclofenac sodium in preventing premature ovulation in patients with DOR. Our primary aim was to determine whether diclofenac sodium reduces cycle cancellation rates in this high-risk population.
Methods
Study Design
This was a retrospective cohort study conducted at a single academic-affiliated public reproductive center between January 2022 and March 2025. The study was authorized by the local institutional review board (Ethics Committee of the Affiliated Hospital of Shandong University of Traditional Chinese Medicine, Reference No. 2025055KY), with a waiver of informed consent due to its retrospective design. All patient data were anonymized and handled with strict confidentiality. The study was conducted in accordance with the Declaration of Helsinki.
Study Population
Patients aged 21–49 years with DOR defined by serum AMH < 1.1 ng/mL and AFC < 5, undergoing autologous IVF cycles with only one dominant follicle >15mm on trigger day were eligible. The following patients were not included in this study: (1) congenital or acquired uterine abnormalities; (2) preimplantation aneuploidy genetic testing (PGT-A); (3) in vitro maturation (IVM); (4) cryopreserved oocytes and/or donor oocytes; (5) unfollowed or incompletely documented data.
Study Protocol
In this study, five ovarian stimulation protocols were employed based on individual patient characteristics. Natural cycle involved no exogenous gonadotropin administration. The naturally developing dominant follicle was monitored, and final oocyte maturation was triggered with human chorionic gonadotropin (recombinant hCG 250 μg; Ovidrel, Merck Serono, Switzerland, or urinary hCG 8000 IU; Livzon Pharmaceutical, China) or GnRH agonist (0.2mg, triptorelin; Decapeptyl, Ipsen, France) when the follicle was greater than 15 mm in diameter, or occasionally no trigger was administered, followed by oocyte retrieval. Minimal stimulation protocol utilized low-dose gonadotropins (typically 75–150 IU daily) in combination with clomiphene citrate (Codal Synto Ltd, 50–100 mg daily for 5 days) or letrozole (Femara, Novartis, Switzerland, 2.5–5 mg daily for 5 days) to gently stimulate follicular development. GnRH-antagonist protocol, Progestin-Primed Ovarian Stimulation (PPOS) protocol, and GnRH-agonist long protocol: These three protocols shared a common gonadotropin stimulation approach, with ovarian stimulation initiated on cycle days 2–3. Recombinant follicle-stimulating hormone (rFSH; Gonal-F, Merck Serono, Switzerland, or Puregon, MSD, Netherlands) and/or human menopausal gonadotropin (hMG; Livzon Pharmaceutical, China) were administered daily, with dosing individualized based on patient age, body mass index (BMI), baseline AFC, and AMH levels. Follicular development was monitored through serial transvaginal ultrasonography and serum hormone measurements. The protocols differed in their approaches to prevent premature LH surge: the antagonist protocol employed GnRH antagonist (cetrorelix acetate; Cetrotide, Merck Serono, Germany, 0.25 mg daily) when the leading follicle reached 12–13 mm; the PPOS protocol utilized concurrent oral progestins (dydrogesterone, 20 mg daily, Duphaston, Abbott, Netherlands or medroxyprogesterone acetate, 10 mg daily, Xianju Pharmaceutical, Zhejiang, China) from stimulation onset with mandatory embryo cryopreservation; and the long protocol involved pituitary suppression with long-acting GnRH agonist (3.75 mg, triptorelin depot; Decapeptyl, Ipsen, France) administered on cycle days 2–3 prior to gonadotropin stimulation. Final oocyte maturation was triggered with hCG and/or GnRH agonist in the GnRH antagonist protocol, while the PPOS and GnRH-agonist long protocols predominantly employed hCG trigger.
Starting in 2024, diclofenac sodium enteric-coated tablets (Beijing Novartis Pharma Ltd., Beijing, China) have been introduced as a prophylactic intervention to prevent premature ovulation in women with DOR. Diclofenac sodium 75mg was administered orally once daily, starting on the evening of trigger day and continuing until the day of oocyte retrieval. The first dose was given 2–4 hours after hCG administration to ensure adequate drug levels during follicular maturation.
In routine practice at our center, diclofenac sodium was introduced as a prophylactic option in January 2024. From that time onward, clinicians were encouraged to prescribe diclofenac sodium for DOR patients with a single dominant follicle who were scheduled for oocyte retrieval, irrespective of the controlled ovarian stimulation protocol. However, use was not mandated, and the decision to administer diclofenac sodium could be influenced by physician preference, patient comorbidities (eg history of peptic ulcer or NSAID intolerance), and perceived risk of premature ovulation. As such, group allocation in this study reflects evolving real-world practice patterns over time rather than randomization.
Follicles that had not yet ovulated were aspirated. Follicle aspiration was scheduled 34–36 h after trigger. Briefly, the aspiration procedure was performed using an aspiration pressure of 135 mmHg and 17 G double-lumen needles (Zhejiang Horizon Medical Technology Co., Ltd., Shanghai, China), without the administration of anesthesia or analgesia. The follicles were flushed three to five times with a flushing medium containing heparin and gentamicin (ASPTM, Vitrolife Sweden AB, V. Frölunda, Sweden). Flushing volume was calculated based on the size of the follicle.
Following egg retrieval, fertilization was carried out using intracytoplasmic sperm injection (ICSI) or IVF depending on the quality of the male sperm. Under ultrasound guidance, a fresh embryo transfer was carried out, and any remaining viable embryos or blastocysts were vitrified. Alternatively, if clinically indicated, a freeze-all strategy was employed. A detailed description of the vitrification and thawing processes can be found elsewhere.27 The American Society for Reproductive Medicine committees’ opinions on guidance on the number of embryos to transfer were followed.28
Outcome Measures
The primary outcome measure was cycle cancellation rate resulting from premature ovulation, defined as the inability to proceed with oocyte retrieval due to spontaneous ovulation occurring prior to the scheduled retrieval procedure. This outcome was compared between patients who received diclofenac sodium on trigger day versus those who did not.
Secondary cycle-level outcomes included the proportion of cycles with no oocytes retrieved among those that proceeded to oocyte retrieval, defined as procedures yielding zero oocytes despite successful follicular aspiration; the proportion of cycles achieving normally fertilized oocytes among those with successful oocyte retrieval, calculated as cycles obtaining at least one two-pronuclei zygote; and cycles without viable embryos available for transfer or cryopreservation.
Clinical pregnancy and live birth outcomes were assessed among patients who underwent fresh embryo transfer. Clinical pregnancy rate was defined as the presence of at least one intrauterine gestational sac with fetal cardiac activity at 6–7 weeks of gestation. Live birth rate was defined as the delivery of at least one viable infant at 24 or more weeks of gestation.
Statistical Analysis
Descriptive statistics were used to summarize demographic and cycle characteristics. Continuous variables were compared with Student’s t-test, and categorical variables were analyzed with the chi-square test or Fisher’s exact test, as appropriate. For the multivariable analyses, we used generalized estimating equation (GEE) models with a logit link and binomial distribution to estimate odds ratios (ORs) and 95% confidence intervals (CIs), accounting for within-patient correlation arising from multiple cycles per woman by specifying an exchangeable working correlation structure. Unless otherwise specified, continuous covariates (antral follicle count, anti-Müllerian hormone level, duration of infertility, gravidity, serum estradiol on trigger day, and trigger-to-retrieval interval) were entered as continuous variables after assessment of linearity in the logit using fractional polynomials and visual inspection; categorical covariates (age ≥ 40 vs <40 years, BMI ≥ 24 vs <24 kg/m2, basic FSH ≥ 12 vs <12 IU/L, serum LH ≥ 20 vs <20 IU/L on trigger day, progesterone ≥ 1.0 vs <1.0 ng/mL on trigger day, etiology of infertility, controlled ovarian stimulation (COS) protocol, and trigger medication type) were coded as binary or multi-category indicator variables. Robust (sandwich) standard errors were used to obtain inference that is valid even if the working correlation structure is misspecified. A p-value of <0.05 was considered to indicate statistically significant difference.
To address potential methodological concerns about clustered data analysis and provide independent validation of our primary findings, we performed a comprehensive sensitivity analysis restricted to the first cycle per patient. This approach eliminated within-patient correlation, allowed for proper assessment of covariate relationships without clustering effects, and enabled standard logistic regression analysis rather than GEE modeling. We included all the same demographic, clinical, and treatment covariates as in the primary GEE analysis, using identical variable definitions and cut-points. For baseline comparisons, we used chi-square tests or Fisher’s exact tests for categorical variables and independent t-tests or Mann–Whitney U-tests for continuous variables, depending on data distribution. Multivariable logistic regression models were constructed using stepwise inclusion of all clinically relevant covariates, with separate models for different outcomes to account for varying sample sizes and relevant confounders. For the primary outcome of premature ovulation, we adjusted for female age, infertility etiology, BMI, ovarian reserve markers (AFC, AMH), baseline FSH, COS protocol, trigger medication, serum LH and progesterone levels on trigger day, and trigger-to-retrieval interval. For cycles with no oocytes retrieved, we additionally included the retrieving physician as a covariate. For embryological outcomes, we further included fertilization method in the adjustment. Clinical pregnancy and live birth analyses were adjusted for female age, number of embryos transferred, embryo quality, and endometrial thickness at transfer. This first-cycle analytical approach also enabled proper assessment of multicollinearity through standard correlation analysis and variance inflation factor calculations, since each patient contributed only one observation to the dataset. We assessed multicollinearity using Variance Inflation Factor (VIF) and Tolerance values to ensure no strong correlations existed between covariates (VIF < 5.0 and Tolerance > 0.1 are generally considered acceptable thresholds). Adjusted ORs and 95% CIs were calculated for all associations, with statistical significance set at p<0.05.
Results
Patient Characteristics
Between January 2022 and March 2025, 616 women underwent 1164 IVF cycles with oocyte retrieval at our Reproductive Center. Among these cycles, 382 (32.8%) received diclofenac sodium on trigger day while 782 (67.2%) did not receive this intervention. The cohort had a mean maternal age of 40.9 ± 5.6 years, with 60.5% of cycles performed in women aged 40 years or older. Combined factor infertility was the predominant diagnosis (57.6%), followed by tubal factor (19.4%) and male factor (15.1%) infertility. The median infertility duration was 3 years, and 32.1% of patients were nulliparous.
Baseline characteristics are presented in Table 1. Comparison between the diclofenac sodium and non-diclofenac sodium groups revealed similar maternal age (40.8 ± 3.2 vs 40.9 ± 5.8 years, P=0.685) and BMI (24.1 ± 3.2 vs 23.9 ± 3.5 kg/m2, P=0.312). However, infertility etiology distribution differed significantly (P<0.001), with the diclofenac sodium group showing higher rates of combined factor infertility (65.4% vs 53.7%) and male factor infertility (22.8% vs 11.4%), while tubal factor infertility was more prevalent in the non-diclofenac sodium group (26.6% vs 4.7%). The diclofenac sodium group had shorter infertility duration (P=0.009) and lower gravidity (P=0.001). Ovarian reserve parameters were comparable between groups, including AFC (median 2 vs 2, P=0.231), AMH levels (0.4 vs 0.6 ng/mL, P=0.185), and basal FSH levels (10.7 vs 10.9 mIU/mL, P=0.890). COS protocols varied significantly (P<0.001), with increased use of PPOS (20.9% vs 5.6%) and decreased use of GnRH-antagonist protocol (14.1% vs 24.8%) in the diclofenac sodium group. Serum estradiol levels on trigger day were significantly lower in the diclofenac sodium group (279.4 vs 314.5 pg/mL, P=0.001), while LH and progesterone levels remained similar. Significant differences were also observed in performing physician distribution (P<0.001) between the two groups.
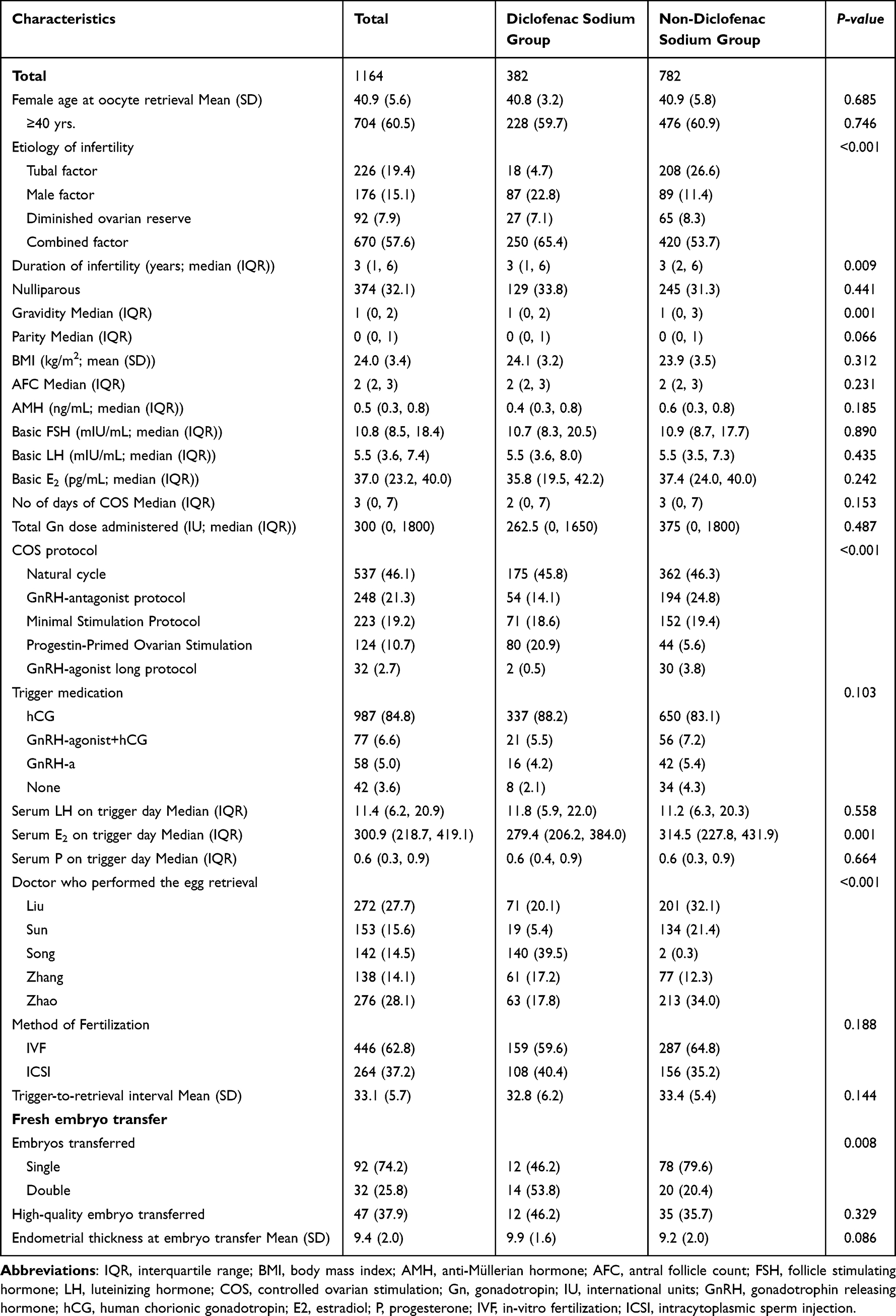 |
Table 1 Demographics of Patients Who Received or Did Not Receive Diclofenac Sodium on Trigger Day to Prevent Premature Ovulation Prior to Oocyte Retrieval. Data are Presented as Numbers (%) Unless Otherwise Noted |
Treatment Outcomes
Treatment outcomes are presented in Table 2. Among the 1164 IVF cycles analyzed, the primary outcome of cycle cancellation resulting from premature ovulation was significantly lower in the diclofenac sodium group compared to the non-diclofenac sodium group (7.3% vs 19.8%, unadjusted OR 0.47, 95% CI 0.27–0.83, P=0.009). After adjustment for potential confounders, this difference remained highly significant (adjusted OR 0.39, 95% CI 0.21–0.73, P=0.003), indicating a 61% reduction in the odds of cycle cancellation due to premature ovulation with diclofenac sodium administration.
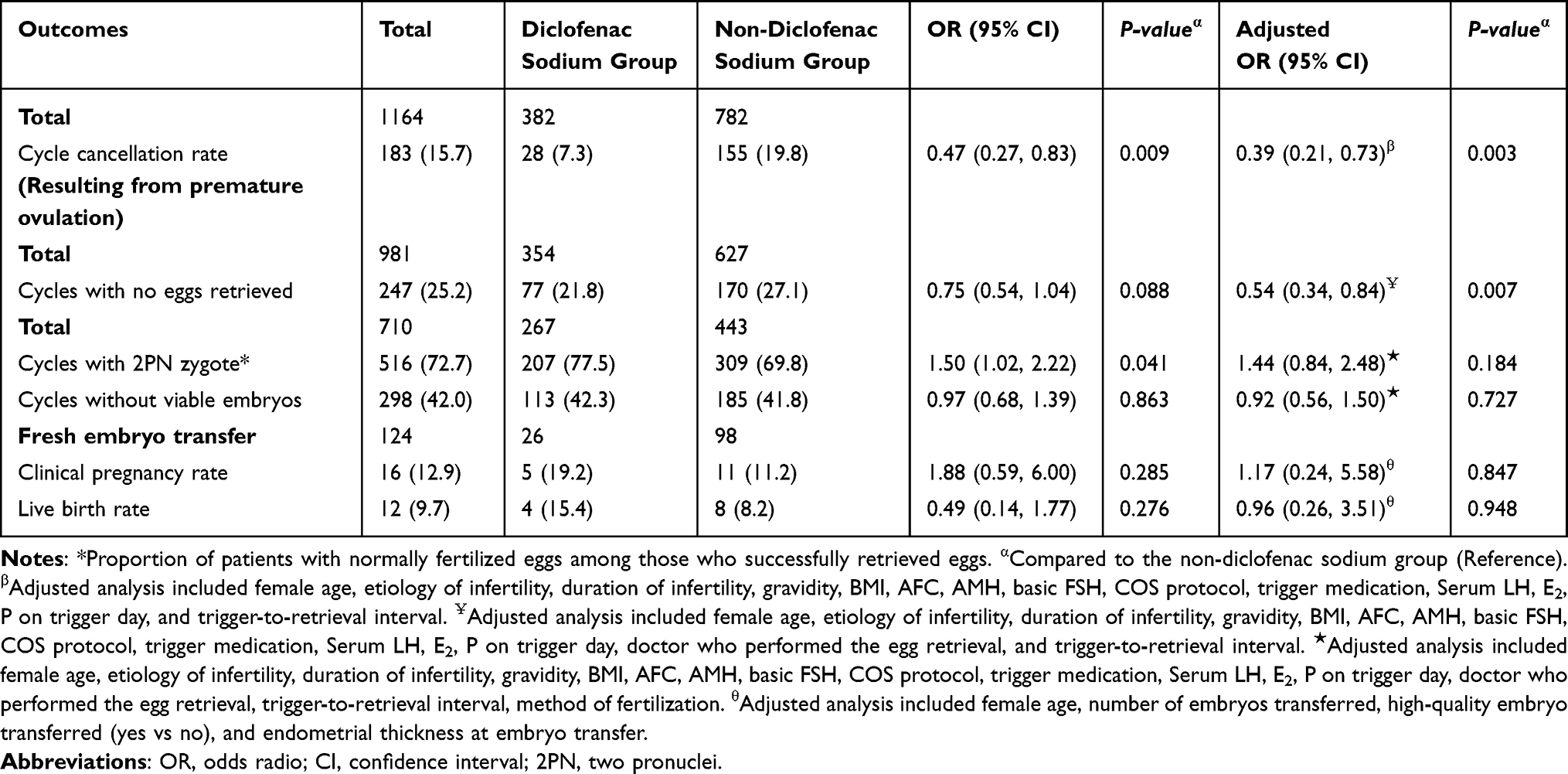 |
Table 2 Treatment Outcome of Patients Who Received or Did Not Receive Diclofenac Sodium on Trigger Day to Prevent Premature Ovulation Prior to Oocyte Retrieval. Data are Presented as Numbers (%) Unless Otherwise Noted |
Among cycles that proceeded to oocyte retrieval (n=981), the proportion of cycles with no eggs retrieved was lower in the diclofenac sodium group (21.8% vs 27.1%, P=0.088 for unadjusted analysis), achieving statistical significance after adjustment (adjusted OR 0.54, 95% CI 0.34–0.84, P=0.007). Among cycles with successful oocyte retrieval (n=710), the proportion achieving normally fertilized oocytes was higher in the diclofenac sodium group (77.5% vs 69.8%, unadjusted OR 1.50, 95% CI 1.02–2.22, P=0.041), though this difference was not significant after adjustment (adjusted OR 1.44, 95% CI 0.84–2.48, P=0.184). The proportion of cycles without viable embryos was similar between groups (42.3% vs 41.8%, P=0.863).
Pregnancy outcomes were evaluated among 124 cycles that underwent fresh embryo transfer. Clinical pregnancy rate showed a non-significant trend toward higher rates in the diclofenac sodium group (19.2% vs 11.2%, unadjusted OR 1.88, 95% CI 0.59–6.00, P=0.285), which remained non-significant after adjustment (adjusted OR 1.17, 95% CI 0.24–5.58, P=0.847). Similarly, live birth rates were comparable between groups (15.4% vs 8.2%, unadjusted OR 0.49, 95% CI 0.14–1.77, P=0.276; adjusted OR 0.96, 95% CI 0.26–3.51, P=0.948).
Multivariable Analysis for Premature Ovulation
GEE analysis was performed to identify factors independently associated with premature ovulation before oocyte retrieval, accounting for within-patient clustering effects (Table 3). After adjusting for multiple potential confounders including demographic, clinical, and treatment parameters, diclofenac sodium administration remained significantly associated with reduced odds of premature ovulation (OR 0.39, 95% CI 0.21–0.73, P=0.003) compared to the non-diclofenac sodium group.
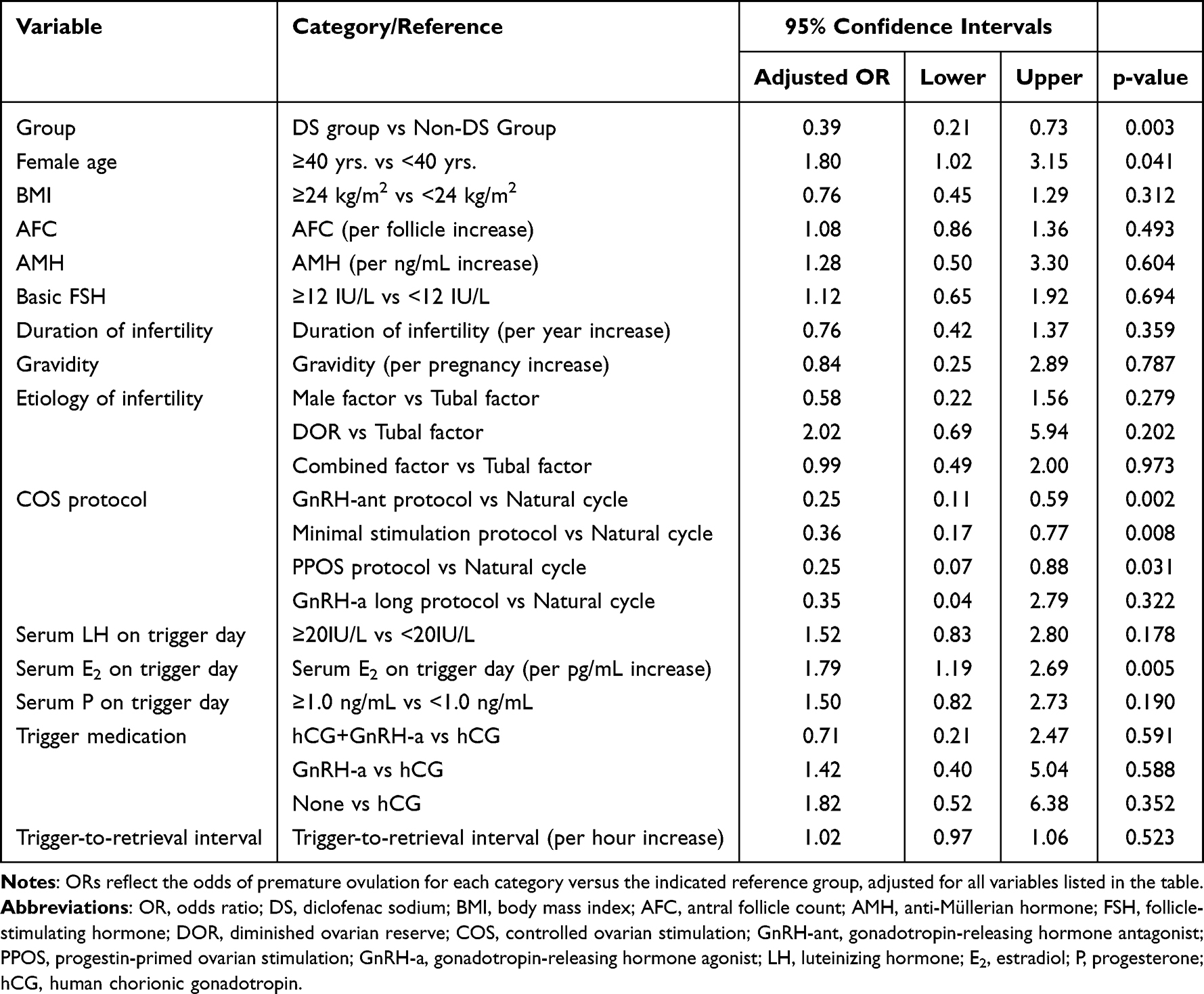 |
Table 3 Generalized Estimating Equation (GEE) Analysis for Factors Associated with Premature Ovulation Before Oocyte Retrieval |
Several other factors were identified as independent predictors of premature ovulation. Advanced maternal age (≥40 years) was associated with increased odds of premature ovulation (OR 1.80, 95% CI 1.02–3.15, P=0.041). The COS protocol significantly influenced premature ovulation risk, with all stimulation protocols showing protective effects compared to natural cycles: GnRH-antagonist protocol (OR 0.25, 95% CI 0.11–0.59, P=0.002), minimal stimulation protocol (OR 0.36, 95% CI 0.17–0.77, P=0.008), and progestin-primed ovarian stimulation protocol (OR 0.25, 95% CI 0.07–0.88, P=0.031). Higher serum estradiol levels on trigger day were associated with increased odds of premature ovulation (OR 1.79, 95% CI 1.19–2.69, P=0.005). Other analyzed factors, including body mass index, ovarian reserve markers (AFC, AMH, basal FSH), infertility duration, gravidity, infertility etiology, serum LH and progesterone levels on trigger day, trigger medication type, and trigger-to-retrieval interval, were not significantly associated with premature ovulation risk in the multivariable model.
Sensitivity Analysis Using First Cycles per Patient
We performed a sensitivity analysis using only the first cycle from each patient to validate our primary findings and address concerns about clustered data. This analysis included 616 patients: 170 in the diclofenac sodium group and 446 in the control group. Baseline characteristics were generally well-balanced between groups, though the diclofenac sodium group had more combined-factor infertility (61.2% vs 49.6%, P<0.001) and shorter trigger-to-retrieval intervals (33.0 vs 34.2 hours, P=0.033) (Supplementary Table S1).
The analysis confirmed our primary findings. Premature ovulation occurred in 11.8% of diclofenac sodium cycles compared to 21.1% of control cycles (crude OR 0.50, P=0.008). After multivariable adjustment for patient demographics, infertility factors, ovarian reserve, hormone levels, and treatment characteristics, diclofenac sodium reduced the odds of premature ovulation by 47% (adjusted OR 0.53, 95% CI 0.29–0.94, P=0.031). Among cycles proceeding to retrieval, diclofenac sodium also significantly reduced cycles with no oocytes retrieved (adjusted OR 0.52, 95% CI 0.29–0.93, P=0.027) (Supplementary Table S2).
The multivariable analysis identified consistent risk factors for premature ovulation. Female age ≥40 years increased risk by 82% (OR 1.82, P=0.015), while serum LH ≥20 IU/L on trigger day was the strongest predictor (OR 4.86, P<0.001). Elevated progesterone ≥1.0 ng/mL on trigger day (OR 1.82, P=0.020) and longer trigger-to-retrieval intervals (OR 1.12 per hour, P<0.001) were also significant risk factors (Supplementary Table S3).
Embryological outcomes showed similar patterns to the primary analysis. Normal fertilization rates were higher in the diclofenac sodium group (82.1% vs 66.8%) but marginally non-significant after adjustment (adjusted OR 2.12, P=0.068). Clinical pregnancy rates among the 114 fresh transfers showed numerical improvement with diclofenac sodium (21.7% vs 12.1%) but were not statistically significant due to small sample sizes (adjusted OR 1.07, P=0.923).
This sensitivity analysis provides strong validation of our primary findings. The effect sizes and risk factors were remarkably consistent with the GEE analysis, confirming that diclofenac sodium genuinely reduces premature ovulation in DOR patients rather than representing an artifact of the repeated-measures design.
Discussion
This retrospective cohort study demonstrates that diclofenac sodium administration on trigger day significantly reduces cycle cancellation due to premature ovulation in patients with DOR, with a 61% reduction in odds compared to controls (adjusted OR 0.39, 95% CI 0.21–0.73, P=0.003). These findings provide important clinical evidence for the use of NSAIDs as a preventive strategy in this high-risk population.
Our results are consistent with recent controlled studies showing that NSAIDs can delay ovulation. Von Wolff et al reported that ibuprofen significantly delayed ovulation in 84.6% of patients compared to 20.0% in controls, with an adjusted OR of 22.72 (95% CI 5.77–115, P<0.001) in natural cycles with hCG-triggered ovulation.13 Our findings expand on these results in DOR patients using different stimulation protocols, where premature ovulation occurred in only 7.3% of diclofenac sodium-treated cycles compared to 19.8% in controls. This protective effect works through cyclooxygenase inhibition, which reduces prostaglandin production needed for follicular rupture.9,29 Recent research has clarified the role of PGE2 and COX-2 pathways in ovulation, showing that NSAIDs disrupt the process that leads to matrix metalloprotease activation and cumulus complex breakdown.30,31 Our three-day diclofenac sodium protocol appears suitable for maintaining adequate COX inhibition throughout the critical period.
These findings are especially important for DOR patients, who are becoming more common and difficult to treat in reproductive medicine. Recent studies show that DOR affects about 9–24% of women having ART procedures, and this number is likely growing because more women are delaying pregnancy.2 For these patients, each treatment cycle is very important because they have limited ovarian reserve and fewer chances for treatment. Our study population, with a mean age of 40.9 years and 60.5% of cycles in women aged ≥40 years, shows the typical characteristics of DOR patients. The finding that older maternal age (≥40 years) independently increased premature ovulation risk (OR 1.80, 95% CI 1.02–3.15, P=0.041) shows the added difficulties that older patients with low ovarian reserve face.32,33 This is especially important because age-related factors seem to add to the existing risks of diminished ovarian reserve.
Our analysis showed that all stimulation protocols helped prevent premature ovulation compared to natural cycles. The GnRH-antagonist protocol had the strongest protective effect (OR 0.25, 95% CI 0.11–0.59, P=0.002), followed by minimal stimulation (OR 0.36, 95% CI 0.17–0.77, P=0.008) and progestin-primed ovarian stimulation (PPOS) protocols (OR 0.25, 95% CI 0.07–0.88, P=0.031). The good results with PPOS in our DOR patients match recent studies showing it works well in poor responders.34,35 Recent analyses have shown that PPOS protocols give similar egg and embryo results to standard protocols while being more flexible and requiring fewer injections.36,37 The higher use of PPOS in the diclofenac sodium group (20.9% vs 5.6%) may show changing treatment practices, since PPOS protocols have become more popular because they are convenient and use a freeze-all approach, which removes worries about luteal phase problems from NSAIDs.
Natural cycles made up 46.1% of all cycles in our study, showing that in real practice, many DOR patients respond poorly to hormone stimulation and are often treated with natural or minimal stimulation approaches. The strong protective effect seen across all protocol types suggests that diclofenac sodium works regardless of the hormone levels created by different treatment protocols.
An important finding was that diclofenac sodium treatment improved oocyte retrieval success, with fewer cycles getting no oocytes (21.8% vs 27.1%; adjusted OR 0.54, 95% CI 0.34–0.84, P=0.007). This better oocyte recovery rate is a meaningful benefit for DOR patients, where even one retrieved oocyte can be very important for treatment success. More cycles achieved normal fertilization in the diclofenac sodium group (77.5% vs 69.8%, P=0.041), but this difference was not significant after adjustment (adjusted OR 1.44, 95% CI 0.84–2.48, P=0.184). Recent research has shown the complex relationship between egg number and quality in women with diminished ovarian reserve.38,39 Our results suggest that while NSAIDs prevent follicular rupture and improve egg recovery, they may not fix the age- and reserve-related problems that affect egg and embryo quality.
The similar rates of cycles without viable embryos between groups (42.3% vs 41.8%, P=0.863) suggests that preventing premature ovulation alone may not solve the main challenges of diminished ovarian reserve.40,41 This matches studies showing that DOR patients have problems with both egg quantity and quality, with older maternal age being a main factor affecting embryo chromosome normality regardless of ovarian reserve levels.42,43
The clinical pregnancy and live birth outcomes warrant careful interpretation given the limited number of fresh embryo transfers (n=124). Clinical pregnancy rates showed a difference that was not statistically significant (19.2% vs 11.2%; adjusted OR 1.17, 95% CI 0.24–5.58, P=0.847), and the same was true for live birth rates (15.4% vs 8.2%; adjusted OR 0.96, 95% CI 0.26–3.51, P=0.948). The limited power to detect differences in pregnancy outcomes reflects the clinical reality of DOR management, where freeze-all strategies are commonly employed, particularly with PPOS protocols. Recent predictive studies have emphasized that live birth rates in ART are influenced by multiple factors beyond oocyte number, including maternal age, embryo quality, and endometrial receptivity.44,45 A 2023 systematic review demonstrated that cumulative live birth rates in DOR patients are more closely correlated with the number of euploid embryos obtained rather than the total number of oocytes retrieved.46
Our multivariable analysis revealed that higher serum estradiol levels on trigger day were associated with increased odds of premature ovulation (OR 1.79, 95% CI 1.19–2.69, P=0.005). This finding aligns with physiological understanding, as elevated estradiol levels may indicate more advanced follicular maturation and increased susceptibility to spontaneous luteinization. Interestingly, the diclofenac sodium group had significantly lower estradiol levels on trigger day (279.4 vs 314.5 pg/mL, P=0.001), which may partially explain the reduced premature ovulation rates observed. Other hormone levels, including LH and progesterone on trigger day, were not significantly linked to premature ovulation risk in our analysis, even though they are expected predictors of upcoming ovulation.
Although our retrospective design limited formal safety assessment, the short-term, low-dose NSAID regimen employed appears well-tolerated. Previous studies have reported minimal adverse effects with similar protocols, with the most common side effects being mild gastrointestinal symptoms in less than 5% of patients.47,48 The anti-inflammatory effects of NSAIDs may also help by reducing pain and swelling after the egg retrieval procedure.49 Recent safety studies have not found major concerns with short-term NSAID use around the time of ART procedures in reproductive-aged women.50 However, doctors should still be careful about potential stomach and heart-related risks, especially in older patients who may have other health conditions or take medications that could interact with NSAIDs.51
This study has several notable strengths. First, it represents one of the largest cohort studies examining NSAID use for preventing premature ovulation specifically in patients with diminished ovarian reserve, a high-risk population with limited treatment options and poor prognosis. The study included 1164 cycles from 616 unique patients across diverse stimulation protocols (natural cycle, minimal stimulation, GnRH-antagonist, PPOS, and GnRH-agonist long protocol), providing comprehensive evidence for the intervention’s effectiveness across different clinical approaches commonly used in DOR management. The use of generalized estimating equations appropriately accounted for within-patient correlation from multiple cycles, strengthening the statistical analysis beyond conventional approaches. Additionally, the comprehensive multivariable analysis controlled for numerous potential confounders including demographic factors, infertility etiology, ovarian reserve parameters, stimulation protocols, hormonal parameters, and treatment variables, substantially reducing the likelihood of residual confounding. The inclusion of a robust sensitivity analysis using only first cycles per patient (n=616) provided independent validation of our primary findings using standard logistic regression, demonstrating consistency across different analytical frameworks. Furthermore, this real-world study captures the complexity of actual clinical practice, enhancing the external validity and generalizability of our findings to routine clinical settings where treatment decisions involve multiple patient-specific considerations.
Several important limitations should be acknowledged. Several important limitations should be acknowledged. First, the retrospective, non-randomized design inherently introduces potential selection bias and precludes the establishment of definitive causality, limiting our conclusions to associational inferences. Second, the administration of diclofenac sodium was practice-driven rather than randomized, based on individual physician judgment; despite comprehensive multivariable adjustment for measured confounders and acceptable multicollinearity diagnostics (all VIF <1.2), residual confounding related to unmeasured physician preferences, patient characteristics, or practice variations cannot be completely excluded. Third, the heterogeneity of stimulation protocols, while reflecting real-world diversity, limits the assessment of protocol-specific effects and may introduce unmeasured variability in treatment responses. Fourth, the limited number of fresh embryo transfers (n=149 in primary analysis, n=114 in sensitivity analysis) reduced statistical power to detect differences in clinical pregnancy and live birth rates, precluding definitive conclusions about reproductive outcomes. Fifth, the common practice of embryo banking in this DOR population significantly complicates the analysis of frozen embryo transfer (FET) outcomes; as transferred embryos often originated from multiple retrieval cycles with disparate diclofenac exposure status (ie, pooling embryos from both treated and untreated cycles), the specific impact of the intervention on pregnancy outcomes in these “mixed” FET cycles could not be reliably isolated or attributed to the intervention. Sixth, our single-center design may limit generalizability to centers with different patient populations, practice patterns, or protocols. Seventh, the study span of several years may introduce temporal confounding from evolving clinical practices and laboratory techniques. Finally, we did not systematically collect safety data or assess potential adverse effects of diclofenac sodium administration, and the optimal dosing and timing regimen remains to be determined through dose-response studies.
Based on our findings, diclofenac sodium is a simple, low-cost treatment that can reduce cycle cancellation rates in DOR patients. The medication is taken once daily and works reliably, making it easy to use in regular clinical practice. Given the emotional and financial stress of cancelled cycles in these patients, the 61% reduction in premature ovulation risk provides real clinical benefit. The treatment works across different stimulation protocols, making it useful for the various approaches commonly used in DOR patients. However, Doctors and patients need to have realistic expectations about treatment outcomes and chances for a live birth. While preventing premature ovulation improves cycle completion rates and egg recovery, the basic challenges of DOR need broader management approaches that may include multiple cycles, considering donor eggs, or other methods such as in vitro maturation or dual stimulation protocols.
Conclusions
In this retrospective cohort study of women with DOR undergoing IVF with single dominant follicles, diclofenac sodium administration on trigger day was associated with significantly reduced rates of premature ovulation and cycle cancellation. These findings were consistent across multiple analytical approaches, including sensitivity analyses restricted to first cycles, demonstrating robust associations in this high-risk population. Although more oocytes were successfully retrieved with diclofenac sodium treatment, embryo and pregnancy outcomes remained similar between groups, suggesting that preventing premature ovulation alone cannot overcome the intrinsic challenges of DOR. While randomized controlled trials are needed to establish causality, our real-world data suggest that diclofenac sodium may represent a simple, safe, and cost-effective adjunctive strategy for improving cycle completion rates in this challenging patient population. These results support considering diclofenac sodium for high-risk DOR patients while underscoring the continued need for comprehensive treatment strategies and prospective randomized trials to definitively establish effects on live birth outcomes.
Data Sharing Statement
The de-identified data underlying this article are available from the corresponding author, Dr. Xian-Ling Cao, upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the Affiliated Hospital of Shandong University of Traditional Chinese Medicine (Reference No. 2025055KY), with informed consent waived due to the retrospective design.
Consent for Publication
Not applicable due to retrospective design with de-identified data.
Patient and Public Involvement
Patients and the public were not involved in the design, conduct, or reporting of this retrospective research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the grants from the National Key Research and Development Program of China (2024YFC3505800).
Disclosure
The authors report no conflicts of interest.
References
1. Practice Committee of American Society for Reproductive M. Diagnostic evaluation of the infertile female: a committee opinion. Fertil Steril. 2015;103(6):e44–14. doi:10.1016/j.fertnstert.2015.03.019
2. Ferraretti AP, La Marca A, Fauser BC, et al. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: the Bologna criteria. Hum Reprod. 2011;26(7):1616–1624. doi:10.1093/humrep/der092
3. Polyzos NP, Devroey P. A systematic review of randomized trials for the treatment of poor ovarian responders: is there any light at the end of the tunnel? Fertil Steril. 2011;96(5):1058–1061e1057. doi:10.1016/j.fertnstert.2011.09.048
4. Galatis D, Kalopita K, Grypiotis I, Flessas I, Kiriakopoulos N, Micha G. Researching the phenomenon of poor ovarian responders and management strategies in IVF: a narrative review. Acta Med Acad. 2022;51(2):108–122. doi:10.5644/ama2006-124.379
5. Ubaldi FM, Rienzi L, Ferrero S, et al. Management of poor ovarian responders in IVF. Reprod Biomed Online. 2005;10(2):235–246. doi:10.1016/S1472-6483(10)60946-7
6. Murdoch WJ, Hansen TR, McPherson LA. A review--role of eicosanoids in vertebrate ovulation. Prostaglandins. 1993;46(2):85–115. doi:10.1016/0090-6980(93)90037-8
7. Espey LL. Ovulation as an inflammatory reaction--a hypothesis. Biol Reprod. 1980;22(1):73–106. doi:10.1095/biolreprod22.1.73
8. O’Sullivan MJ, Stamouli A, Thomas EJ, Richardson MC. Gonadotrophin regulation of production of tissue inhibitor of metalloproteinases-1 by luteinized human granulosa cells: a potential mechanism for luteal rescue. Mol Hum Reprod. 1997;3(5):405–410. doi:10.1093/molehr/3.5.405
9. Duffy DM, Ko C, Jo M, Brannstrom M, Curry TE. Ovulation: parallels with inflammatory processes. Endocr Rev. 2019;40(2):369–416. doi:10.1210/er.2018-00075
10. Vane JR, Bakhle YS, Botting RM. Cyclooxygenases 1 and 2. Annu Rev Pharmacol Toxicol. 1998;38:97–120. doi:10.1146/annurev.pharmtox.38.1.97
11. Wallace JL. Prostaglandins, NSAIDs, and gastric mucosal protection: why doesn’t the stomach digest itself? Physiol Rev. 2008;88(4):1547–1565. doi:10.1152/physrev.00004.2008
12. Nargund G, Wei CC. Successful planned delay of ovulation for one week with indomethacin. J Assist Reprod Genet. 1996;13(8):683–684. doi:10.1007/BF02069650
13. von Wolff M, Reid G, Stute P, Schwartz ASK, Roumet M, Fink A. Ibuprofen delays ovulation by several hours: prospective controlled study in natural cycles with HCG-triggered ovulation. Reprod Biomed Online. 2024;49(3):103975. doi:10.1016/j.rbmo.2024.103975
14. Jesam C, Salvatierra AM, Schwartz JL, Croxatto HB. Suppression of follicular rupture with meloxicam, a cyclooxygenase-2 inhibitor: potential for emergency contraception. Hum Reprod. 2010;25(2):368–373. doi:10.1093/humrep/dep392
15. McInerney KA, Hatch EE, Wesselink AK, Rothman KJ, Mikkelsen EM, Wise LA. Preconception use of pain-relievers and time-to-pregnancy: a prospective cohort study. Hum Reprod. 2017;32(1):103–111. doi:10.1093/humrep/dew272
16. Jukic AMZ, Padiyara P, Bracken MB, McConnaughey DR, Steiner AZ. Analgesic use at ovulation and implantation and human fertility. Am J Clin Exp Obstet Gynecol. 2020;222(5):
17. Kadoch IJ, Al-Khaduri M, Phillips SJ, et al. Spontaneous ovulation rate before oocyte retrieval in modified natural cycle IVF with and without indomethacin. Reprod Biomed Online. 2008;16(2):245–249. doi:10.1016/S1472-6483(10)60581-0
18. Kawachiya S, Matsumoto T, Bodri D, Kato K, Takehara Y, Kato O. Short-term, low-dose, non-steroidal anti-inflammatory drug application diminishes premature ovulation in natural-cycle IVF. Reprod Biomed Online. 2012;24(3):308–313. doi:10.1016/j.rbmo.2011.12.002
19. Kohl Schwartz AS, Burkard S, Mitter VR, Leichtle AB, Fink A, Von Wolff M. Short-term application of ibuprofen before ovulation. Facts Views Vis Obgyn. 2020;12(3):179–184.
20. Younis JS, Ben-Ami M, Ben-Shlomo I. The Bologna criteria for poor ovarian response: a contemporary critical appraisal. J Ovarian Res. 2015;8:76.
21. Oudendijk JF, Yarde F, Eijkemans MJ, Broekmans FJ, Broer SL. The poor responder in IVF: is the prognosis always poor?: a systematic review. Hum Reprod Update. 2012;18(1):1–11. doi:10.1093/humupd/dmr037
22. Todd PA, Sorkin EM. Diclofenac sodium: a reappraisal of its pharmacodynamic and pharmacokinetic properties, and therapeutic efficacy. Drugs. 1988;35(3):244–285. doi:10.2165/00003495-198835030-00004
23. Gan TJ. Diclofenac: an update on its mechanism of action and safety profile. Curr Med Res Opin. 2010;26(7):1715–1731. doi:10.1185/03007995.2010.486301
24. Hu S, Xu B, Jin L. Perinatal outcome in young patients with diminished ovarian reserve undergoing assisted reproductive technology. Fertil Steril. 2020;114(1):118–124e111. doi:10.1016/j.fertnstert.2020.02.112
25. Levi AJ, Raynault MF, Bergh PA, Drews MR, Miller BT, Scott RT. Reproductive outcome in patients with diminished ovarian reserve. Fertil Steril. 2001;76(4):666–669. doi:10.1016/S0015-0282(01)02017-9
26. Pelinck MJ, Hoek A, Simons AH, Heineman MJ. Efficacy of natural cycle IVF: a review of the literature. Hum Reprod Update. 2002;8(2):129–139. doi:10.1093/humupd/8.2.129
27. Song J, Xiang S, Sun Z. Frozen embryo transfer at the cleavage stage can be performed within the first menstrual cycle following the freeze-all strategy without adversely affecting the live birth rate: a STROBE-compliant retrospective study. Medicine. 2019;98(38):e17329. doi:10.1097/MD.0000000000017329
28. Practice Committee of the American Society for Reproductive M. Guidance on the limits to the number of embryos to transfer: a committee opinion. Fertil Steril. 2021;116(3):651–654. doi:10.1016/j.fertnstert.2021.06.050
29. Sirois J, Sayasith K, Brown KA, Stock AE, Bouchard N, Dore M. Cyclooxygenase-2 and its role in ovulation: a 2004 account. Hum Reprod Update. 2004;10(5):373–385. doi:10.1093/humupd/dmh032
30. Niringiyumukiza JD, Cai H, Xiang W. Prostaglandin E2 involvement in mammalian female fertility: ovulation, fertilization, embryo development and early implantation. Reprod Biol Endocrinol. 2018;16(1):43. doi:10.1186/s12958-018-0359-5
31. Russell DL, Robker RL. Molecular mechanisms of ovulation: co-ordination through the cumulus complex. Hum Reprod Update. 2007;13(3):289–312. doi:10.1093/humupd/dml062
32. Practice Committee of the American Society for Reproductive M. Testing and interpreting measures of ovarian reserve: a committee opinion. Fertil Steril. 2020;114(6):1151–1157. doi:10.1016/j.fertnstert.2020.09.134
33. Aitken RJ. What is driving the global decline of human fertility? Need for a multidisciplinary approach to the underlying mechanisms. Front Reprod Health. 2024;6:1364352. doi:10.3389/frph.2024.1364352
34. Kuang Y, Chen Q, Fu Y, et al. Medroxyprogesterone acetate is an effective oral alternative for preventing premature luteinizing hormone surges in women undergoing controlled ovarian hyperstimulation for in vitro fertilization. Fertil Steril. 2015;104(1):62–70.e63. doi:10.1016/j.fertnstert.2015.03.022
35. Ata B, Capuzzo M, Turkgeldi E, Yildiz S, La Marca A. Progestins for pituitary suppression during ovarian stimulation for ART: a comprehensive and systematic review including meta-analyses. Hum Reprod Update. 2021;27(1):48–66. doi:10.1093/humupd/dmaa040
36. Wang Y, Chen Q, Wang N, Chen H, Lyu Q, Kuang Y. Controlled ovarian stimulation using medroxyprogesterone acetate and hMG in patients with polycystic ovary syndrome treated for IVF: a double-blind randomized crossover clinical trial. Medicine. 2016;95(9):e2939. doi:10.1097/MD.0000000000002939
37. Ata B, Kalafat E. Progestin-primed ovarian stimulation: for whom, when and how? Reprod Biomed Online. 2024;48(2):103639. doi:10.1016/j.rbmo.2023.103639
38. Coticchio G, Barrie A, Lagalla C, et al. Plasticity of the human preimplantation embryo: developmental dogmas, variations on themes and self-correction. Hum Reprod Update. 2021;27(5):848–865. doi:10.1093/humupd/dmab016
39. Cimadomo D, Fabozzi G, Vaiarelli A, Ubaldi N, Ubaldi FM, Rienzi L. Impact of maternal age on oocyte and embryo competence. Front Endocrinol. 2018;9:327. doi:10.3389/fendo.2018.00327
40. Ubaldi FM, Capalbo A, Vaiarelli A, et al. Follicular versus luteal phase ovarian stimulation during the same menstrual cycle (DuoStim) in a reduced ovarian reserve population results in a similar euploid blastocyst formation rate: new insight in ovarian reserve exploitation. Fertil Steril. 2016;105(6):1488–1495.e1481. doi:10.1016/j.fertnstert.2016.03.002
41. Vaiarelli A, Cimadomo D, Trabucco E, et al. Double stimulation in the same ovarian cycle (DuoStim) to maximize the number of oocytes retrieved from poor prognosis patients: a multicenter experience and SWOT analysis. Front Endocrinol. 2018;9:317. doi:10.3389/fendo.2018.00317
42. Franasiak JM, Forman EJ, Hong KH, et al. The nature of aneuploidy with increasing age of the female partner: a review of 15,169 consecutive trophectoderm biopsies evaluated with comprehensive chromosomal screening. Fertil Steril. 2014;101(3):656–663e651. doi:10.1016/j.fertnstert.2013.11.004
43. La Marca A, Sighinolfi G, Radi D, et al. Anti-Mullerian hormone (AMH) as a predictive marker in assisted reproductive technology (ART). Hum Reprod Update. 2010;16(2):113–130. doi:10.1093/humupd/dmp036
44. McLernon DJ, Steyerberg EW, Te Velde ER, Lee AJ, Bhattacharya S. Predicting the chances of a live birth after one or more complete cycles of in vitro fertilisation: population based study of linked cycle data from 113 873 women. BMJ. 2016;355:i5735. doi:10.1136/bmj.i5735
45. Ngwenya O, Lensen SF, Vail A, Mol BWJ, Broekmans FJ, Wilkinson J. Individualised gonadotropin dose selection using markers of ovarian reserve for women undergoing in vitro fertilisation plus intracytoplasmic sperm injection (IVF/ICSI). Cochrane Database Syst Rev. 2024;1(1):CD012693. doi:10.1002/14651858.CD012693.pub3
46. Li Y, Li X, Yang X, et al. Cumulative live birth rates in low prognosis patients according to the POSEIDON criteria: an analysis of 26,697 cycles of in vitro fertilization/intracytoplasmic sperm injection. Front Endocrinol. 2019;10:642. doi:10.3389/fendo.2019.00642
47. Bata MS, Al-Ramahi M, Salhab AS, Gharaibeh MN, Schwartz J. Delay of ovulation by meloxicam in healthy cycling volunteers: a placebo-controlled, double-blind, crossover study. J Clin Pharmacol. 2006;46(8):925–932. doi:10.1177/0091270006289483
48. Jesam C, Salvatierra AM, Schwartz JL, Fuentes A, Croxatto HB. Effect of oral administration of a continuous 18 day regimen of meloxicam on ovulation: experience of a randomized controlled trial. Contraception. 2014;90(2):168–173. doi:10.1016/j.contraception.2014.04.011
49. Gazvani R, Templeton A. Peritoneal environment, cytokines and angiogenesis in the pathophysiology of endometriosis. Reproduction. 2002;123(2):217–226. doi:10.1530/rep.0.1230217
50. Hamroun S, Couderc M, Flipo RM, et al. NSAID exposure delays time-to-pregnancy in patients with spondyloarthritis: an analysis of the GR2 prospective cohort. RMD Open. 2024;10(4):e004745. doi:10.1136/rmdopen-2024-004745
51. Schjerning AM, McGettigan P, Gislason G. Cardiovascular effects and safety of (non-aspirin) NSAIDs. Nat Rev Cardiol. 2020;17(9):574–584. doi:10.1038/s41569-020-0366-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.