Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Association Between Cutaneous Lupus Erythematosus and Atherosclerotic Cardiovascular Disease: A Systematic Review
Authors Althobaiti RF ![]() , Almansour TA, Altowairqi RK, Alzahrani NM, Samman LA, Almutairi NA
, Almansour TA, Altowairqi RK, Alzahrani NM, Samman LA, Almutairi NA ![]() , Aljoudi SB, Alharbi RH
, Aljoudi SB, Alharbi RH
Received 16 October 2025
Accepted for publication 6 January 2026
Published 17 January 2026 Volume 2026:19 574248
DOI https://doi.org/10.2147/CCID.S574248
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Renad F Althobaiti,1 Turki Ahmad Almansour,2 Raghad Khalid Altowairqi,3 Naif Mohammed Alzahrani,2 Lugain Ayman Samman,3 Naif Awwadh Almutairi,2 Sarah Bandar Aljoudi,4 Rehab Hamed Alharbi4
1College of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 2College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 3College of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 4Department of Dermatology, King Abdulaziz University Hospital, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Renad F Althobaiti, College of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia, Email [email protected]
Introduction: Cutaneous lupus erythematosus (CLE) is an autoimmune skin disorder increasingly recognized to have systemic effects, including possible links to atherosclerotic cardiovascular disease (ASCVD). However, the strength and pattern of this association remain uncertain.
Objective: To evaluate and assess available evidence on ASCVD risk in CLE, identify patterns across study designs and populations, and highlight research gaps requiring further study.
Methods: A systematic search of PubMed, Scopus, and Web of Science was conducted up to July 2025, following PRISMA 2020 guidelines (PROSPERO ID: CRD420251156382). Eligible studies included adult CLE populations reporting ASCVD outcomes. Data extraction and risk-of-bias assessment were independently performed using the Newcastle–Ottawa Scale and the AXIS tool.
Results: Six observational studies met the inclusion criteria, including population-based cohorts, hospital datasets, and case–control analyses. Across designs, CLE was consistently associated with elevated ASCVD risk, particularly stroke and thromboembolic events. Large registry-based studies showed significant associations even after adjustment for traditional risk factors, suggesting CLE-specific inflammatory mechanisms. Smaller cohorts highlighted high comorbidity burdens and subtype differences, particularly a stronger signal in discoid lupus.
Conclusion: Evidence indicates that CLE is linked to increased ASCVD risk, especially cerebrovascular and thromboembolic outcomes. Standardized definitions and longitudinal studies are needed to clarify subtype-specific risks and inform prevention strategies.
Keywords: cutaneous lupus erythematosus, discoid lupus, cardiovascular disease, atherosclerosis, stroke, thromboembolism
Introduction
Lupus erythematosus (LE), is an inflammatory autoimmune disease, manifestation can be classified to either systemic or cutaneous.1 Cutaneous lupus erythematosus (CLE) is defined by isolated skin lesions that lack prominent features of systemic lupus erythematosus (SLE) and occurs two to three times more frequently than SLE.2 There are three subtypes of dermatologic presentation: acute, subacute, and chronic. Acute CLE typically manifests as a malar rash, while subacute CLE features scaly, erythematous plaques. Disc-shaped plaques are the distinctive feature of chronic CLE, also known as discoid lupus, which most often involves the head and neck.3,4
To further understand the pathogenesis of CLE, it is essential to recognize that it involves T helper (Th) 1 and Th17 inflammatory reactions. These immune pathways release cytokines that drive endothelial dysfunction, vascular inflammation, and pro-thrombotic activity, providing a mechanistic link between CLE-related inflammation and cardiovascular complications.5
Given these mechanisms, CLE may have significant implications for cardiovascular health, contributing to an increased risk of atherosclerotic cardiovascular disease (ASCVD).5 In particular, chronic systemic inflammation promotes endothelial dysfunction and plaque formation,1 placing individuals with LE, including those with CLE, at increased risk for cardiovascular events such as myocardial infarction and stroke.4
Although increased risk and the involvement of both inflammatory and traditional risk factors have been observed, the mechanisms connecting CLE and cardiovascular disease remain unclear.6
Although SLE and other inflammatory autoimmune disorders have been shown to exhibit systemic inflammation, little is known regarding the systemic indicators of inflammation in CLE patients.6
This systematic review aims to evaluate the existing evidence on the relationship between CLE and ASCVD. The review emphasizes the exploration of possible shared pathophysiological mechanisms, evaluates the cardiovascular risk in individuals with CLE, and addresses key gaps in the current literature.
Methods and Materials
Registration and Reporting Guidelines
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines.7 The protocol was prospectively registered with PROSPERO ID: CRD420251156382.
Search Strategies
We systematically searched PubMed, Scopus, Web Of Science using a combination of Keywords (“cutaneous lupus” OR “cutaneous lupus erythematosus” OR “CLE” OR “discoid lupus” OR “subacute cutaneous lupus” OR “chronic cutaneous lupus”) AND (“atherosclerosis” OR “atherosclerotic cardiovascular disease” OR “ASCVD” OR “coronary artery disease” OR “myocardial infarction” OR “stroke” OR “vascular risk” OR “cardiovascular disease”) Database searches were performed until July 2025.
Study Design and Criteria
Both randomized and nonrandomized study types were included.
Inclusion Criteria
- Studies published up to July 2025.
- Observational studies: cohort (prospective or retrospective), cross-sectional, case reports and case-control studies.
- Studies involving adult patients with diagnosed CLE.
- Studies reporting cardiovascular outcomes related to atherosclerosis (either clinical or subclinical).
Exclusion Criteria
- Studies in languages other than English.
- Animal studies or in vitro research.
- Inappropriate study design (editorials, reviews, and meta-analysis).
- Studies focusing solely on SLE without subgroup analysis for CLE.
- Studies without cardiovascular outcomes.
- Incomplete or unclear CLE diagnostic criteria.
Screening and Selection of Studies
Search results were imported into Rayyan for systematic screening.8 After duplicate removal, three independent reviewers screened titles and abstracts in blinded mode. Full texts of potentially eligible studies were then retrieved and assessed by two independent reviewers. Any discrepancies were resolved by a third reviewer.
Data Extraction and Risk of Bias Assessment
Data extraction was conducted independently by two reviewers using a standardized form to capture study characteristics, patient demographics, CLE subtypes, diagnostic criteria, cardiovascular outcomes, measurement methods, and risk estimates. Any discrepancies were resolved through consensus. The risk of bias in the included studies was assessed using appropriate appraisal tools.9 The Newcastle–Ottawa Scale (NOS) was applied for cohort and case–control studies. The AXIS tool was used for the cross-sectional study.
Results
The Primary Results of the Search
The search strategy identified hundreds of records across the major biomedical databases. Searches of PubMed (61 records), Web of Science (92 records) and Scopus (176 records) yielded a total of 329 articles. After removing 102 duplicates, 227 unique records were screened. Title and abstract screening excluded 217 records, mainly because the articles were case reports or did not report ASCVD outcomes or did not involve CLE. Of the 10 reports identified as potentially relevant after the full text screening, we were unable to retrieve the full text for 4 of them. Six articles were assessed for eligibility, and ultimately all 6 were included in the study. The screening and selection process is summarized in Figure 1 using a PRISMA flow diagram.
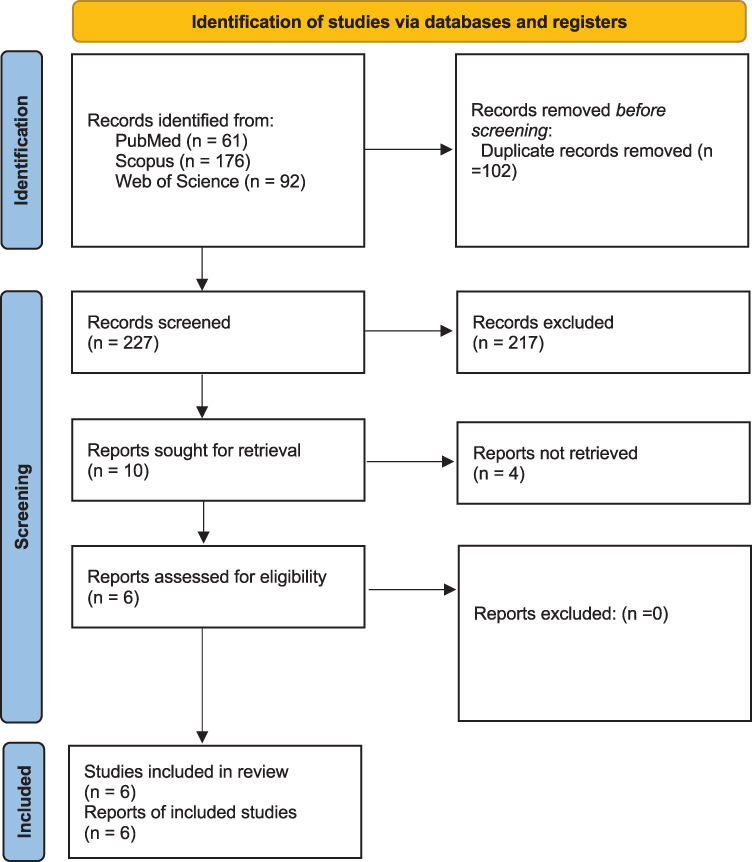 |
Figure 1 PRISMA flow diagram summarizing the study screening and selection process. |
Risk of Bias Assessment
The risk of bias assessments are summarized in Tables 1–3, using the NOS for cohort and case–control studies and the AXIS tool for the cross-sectional study.
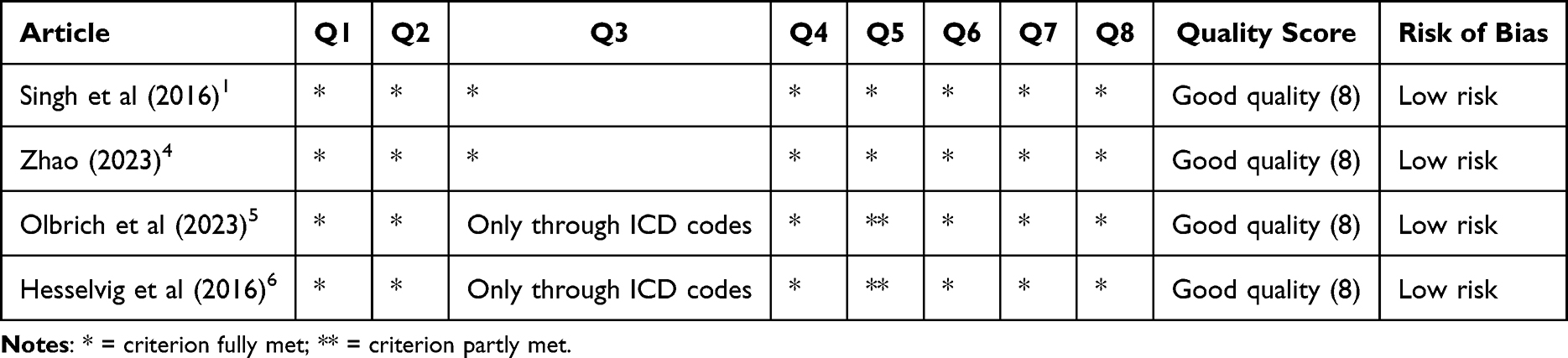 |
Table 1 Newcastle-Ottawa Scale Assessment for Included Cohort Studies |
 |
Table 2 Newcastle-Ottawa Scale Assessment for Included Case-Control Studies |
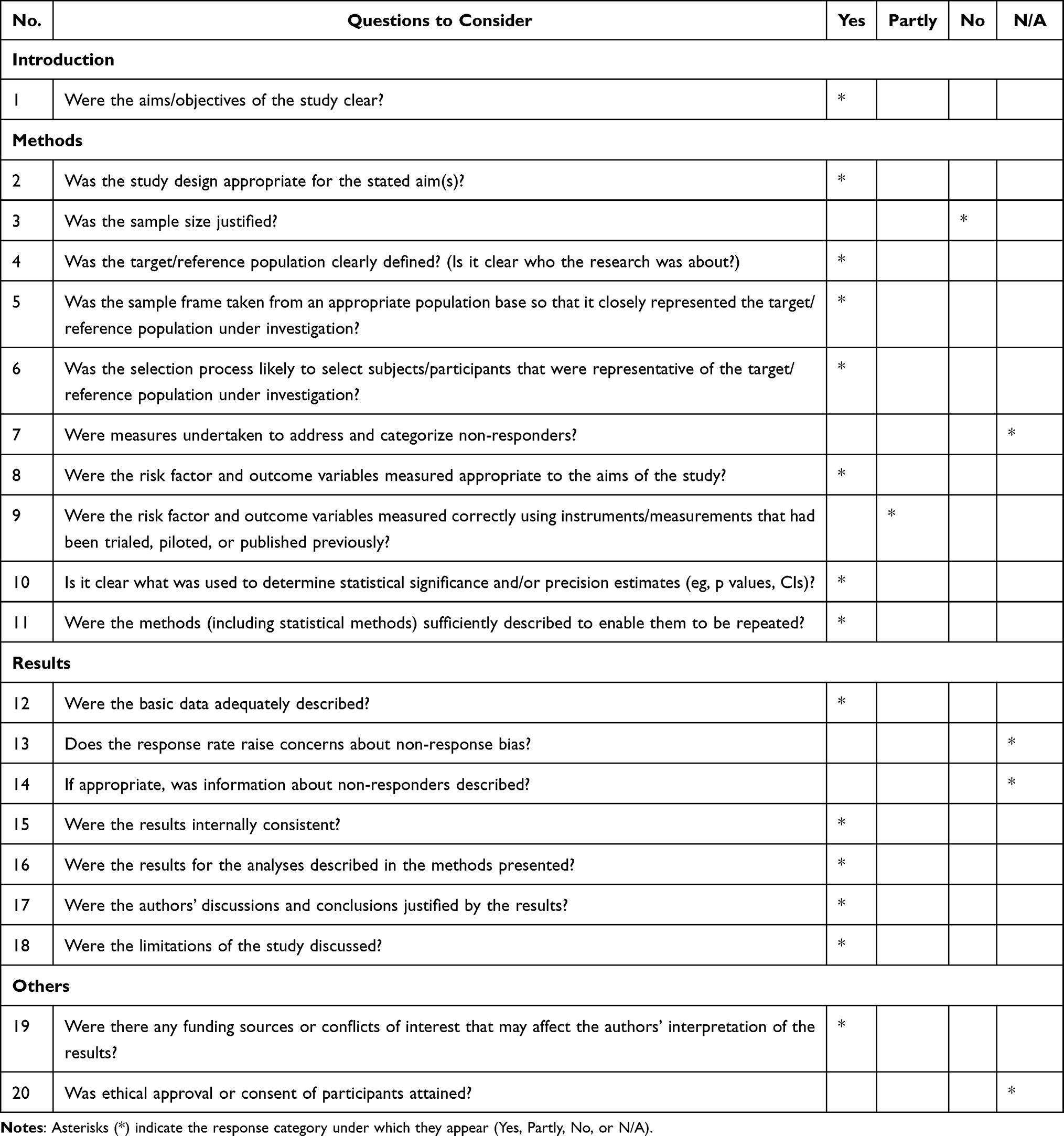 |
Table 3 Risk of Bias Assessment Using the AXIS Tool (He et al, 2023).3 |
An Overview of the Reviewed Studies’ Characteristics
The systematic review included studies published between 2016 and 2024. These studies originated from diverse geographical locations, including the United States, Denmark, and international cohorts (encompassing Europe and Asia). All included studies were observational in design. Specifically, the review comprised two population-based cohort studies by Singh et al and Hesselvig et al, two retrospective cohort studies by Zhao (2023) and Olbrich (2023), one study that analyzed a national hospitalization dataset by He et al, and one case-control study by Patil et al. Sample sizes across the studies varied significantly, ranging from 155 CLE patients in a population-based cohort described by Singh et al to over 62,000 hospitalizations in a nationwide study by He et al. All cohorts exclusively involved adult populations. The mean ages of participants across the studies ranged from approximately 42.3 years in Hesselvig et al to 58.5 years in He et al. Women consistently constituted a majority of participants, with representation ranging from 65% in Singh et al to 86% in Patil et al in studies that reported gender distribution. In studies that provided racial demographics, White participants generally formed the largest group, although Black/African American, Hispanic, and Asian participants were also well-represented.
Results of Individual Studies
The overview of the included studies and their reported cardiovascular outcomes is presented in Table 4. Across six observational studies, individuals with CLE consistently demonstrated an increased risk of ASCVD, though the strength and scope of associations varied. For clarity, hazard ratio (HR) and odds ratio (OR) are used to express relative risks across studies. Singh et al and Hesselvig et al reported increased risks of cerebrovascular accidents (HR 2.97) and peripheral arterial disease (HR 2.06), along with a 31% higher hazard of composite cardiovascular outcomes, even when ischemic heart disease was not elevated. He et al and Olbrich et al highlighted circulatory complications, with He et al reporting 5-year incidences of stroke (3.8%) and heart failure (3.6%), while Olbrich’s large global cohort found significantly higher hazards of myocardial infarction (HR 1.177), cerebral infarction/stroke (HR 1.428), arterial embolism and thrombosis (HR 1.399), pulmonary embolism (HR 1.195), angina pectoris (HR 1.173), heart failure (HR 1.242), and major adverse cardiovascular events (MACE composite, HR 1.208), along with elevated all-cause mortality (HR 1.304). Smaller cohorts reported similar patterns: Zhao (2023) described a 10-year ASCVD event rate of 13.5%, while Patil et al identified markedly higher odds of cardiometabolic disorders compared with controls (OR 4.61). Despite these converging patterns, marked heterogeneity in CLE subtypes, diagnostic approaches, and definitions of cardiovascular outcomes limited comparability across studies. Mortality was reported in three studies; however, only Singh et al specifically assessed cardiovascular mortality, while others provided all-cause mortality or did not report it, leaving uncertainty about mortality outcomes. Overall, the evidence indicates an elevated risk of cardiovascular morbidity in CLE, underscoring gaps in standardized outcome definitions, limited reporting on mortality, and underrepresentation of certain CLE subtypes.
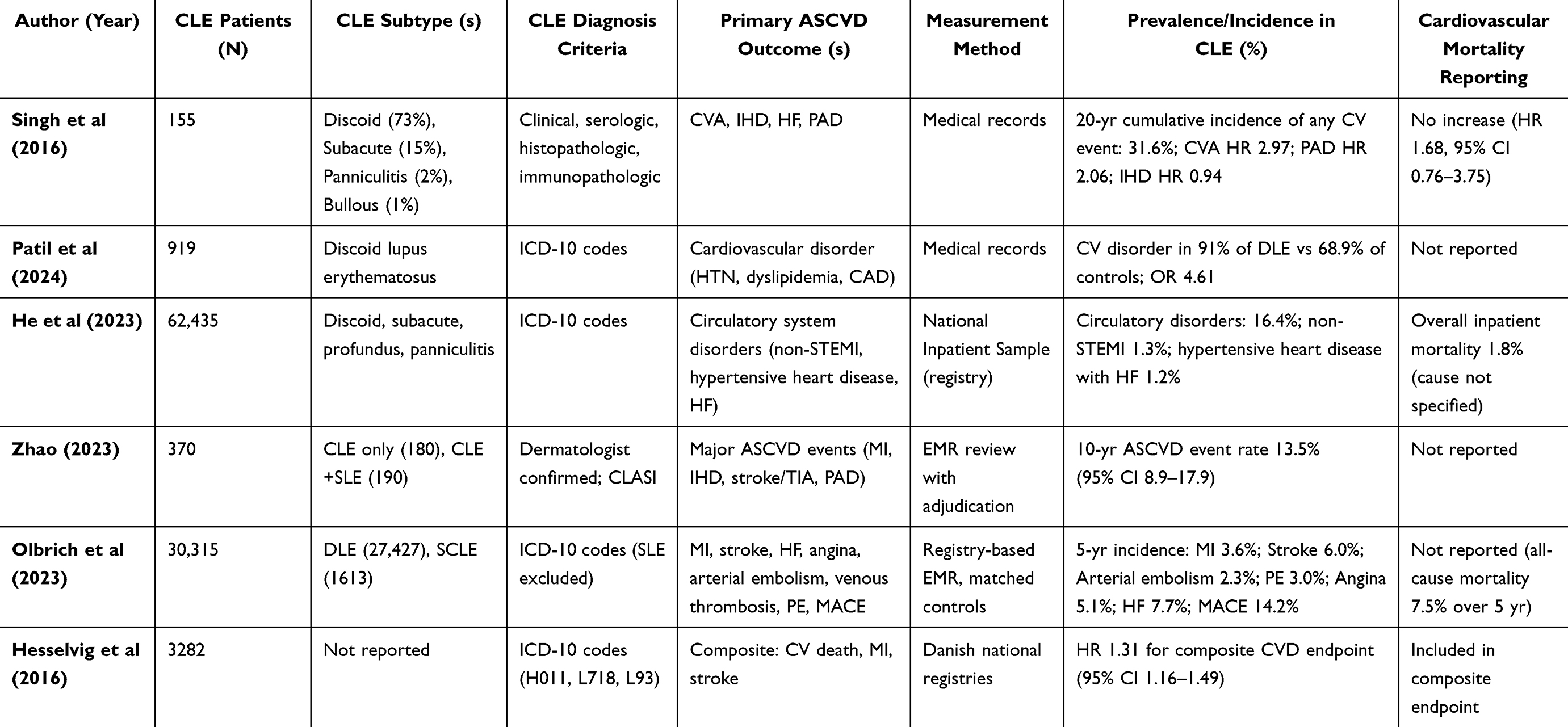 |
Table 4 Overview of Included Studies and Reported Cardiovascular Outcomes |
Discussion
Overview of Main Findings
This systematic review synthesizes evidence on the association between CLE and ASCVD. Our principal finding is that CLE is consistently associated with elevated risks of vascular and cardiac outcomes across multiple observational designs, though the magnitude and specificity of risk vary across studies.
Evidence from Large-Scale Studies
The study by Chen et al provides recent confirmation: in a large claims database, individuals with CLE had significantly higher incident and prevalent ASCVD compared with matched controls, with effect sizes modestly lower than those seen in systemic lupus but higher than in psoriasis. This positioning of CLE between systemic lupus and other inflammatory dermatoses suggests that, while CLE is clinically defined by cutaneous manifestations, systemic cardiovascular involvement may also be relevant. The authors further noted that risk estimates remained significant after adjusting for traditional cardiovascular risk factors, indicating that additional disease-related pathways could contribute.10 These findings align with the registry-based analysis of Olbrich et al, which examined multiple cardiovascular endpoints across global electronic medical records and provided subtype-specific insights, particularly a stronger association in discoid lupus erythematosus compared with subacute CLE.5 Together, such large-scale analyses underscore that CLE should not be regarded as exclusively skin-limited.
Patterns in Cardiovascular Outcomes
Registry studies have also reported that thromboembolic and cerebrovascular outcomes appeared more consistently elevated than coronary events.1,3 Differences in outcome patterns may reflect variability in definitions, coding, and follow-up across datasets rather than a single underlying mechanism. The heterogeneity also illustrates how study design and case definitions influence observed associations: small clinical cohorts with detailed characterization sometimes yielded different results than larger registry-based datasets. Across settings, however, the recurrence of stroke- and embolism-related signals supports the interpretation that these associations are reproducible. Similar patterns were observed in the Danish nationwide cohort by Hesselvig et al, which reported an increased risk for a composite of cardiovascular outcomes in CLE, though effect sizes were comparatively modest. Olbrich et al subsequently confirmed these associations on a larger scale, particularly for thromboembolic and cerebrovascular outcomes.5,6 Taken together, these studies suggest that risk elevations in CLE are consistent, but the strength of association varies according to the dataset, follow-up duration, and outcome definitions applied.
Findings from Smaller Cohorts
Beyond large registries, smaller population-based and clinical cohorts provide additional context. Singh et al observed elevated risks of cerebrovascular accidents and peripheral arterial disease in CLE, though ischemic heart disease was not clearly increased, suggesting vascular risk may differ by territory.1 Zhao reported a 10-year ASCVD event rate of 13.5% in a carefully adjudicated cohort,4 while Patil et al demonstrated higher odds of hypertension, dyslipidemia, and other cardiometabolic comorbidities in discoid lupus erythematosus.2 These findings highlight how comorbidity burden interacts with CLE-specific inflammation to magnify overall vascular susceptibility. Hospital-based data add another perspective. He et al, analyzing over 62,000 CLE hospitalizations, found notable circulatory complications including stroke, non–ST elevation myocardial infarction, and heart failure, with overall inpatient mortality approaching 2%.3 While such datasets likely overrepresent severe disease, they underscore the real-world clinical consequences of cardiovascular risk in CLE and emphasize that this burden extends beyond subclinical endpoints.
Clinical Implications
From a clinical standpoint, these observations indicate that dermatologists and rheumatologists should be attentive to cardiovascular risk in patients with CLE. While there are no disease-specific screening protocols, recognition that CLE patients often harbor both traditional cardiometabolic risk factors and potential disease-driven inflammatory pathways supports careful monitoring and preventive strategies. Standard assessment of hypertension, dyslipidemia, diabetes, and smoking status remains essential, and early referral for cardiovascular evaluation may be justified in select patients.11
Limitations of the Evidence
Despite this emerging evidence, several limitations temper interpretation. Most large-scale studies rely on ICD coding, which may misclassify CLE and does not capture disease severity or activity. Subtype-specific data remain sparse, with discoid lupus generally better represented than subacute or other variants. Adjustment for confounders such as smoking, obesity, and physical activity is inconsistent, and few prospective longitudinal cohorts exist to establish temporality or clarify dose–response relationships. Mortality outcomes are also inconsistently reported, limiting conclusions on long-term prognosis.11 These gaps highlight the need for standardized outcome definitions and prospective, subtype-stratified studies that can more precisely define the cardiovascular burden of CLE.
Summary of Overall Interpretation
In summary, while the association between CLE and ASCVD is increasingly well supported, the field still faces important evidence gaps, particularly regarding subtype-specific risks, mortality outcomes, and prospective longitudinal data. Addressing these gaps will be critical to translating epidemiologic signals into practical guidance for patient care.
Conclusion
This systematic review shows that CLE is associated with an increased risk of ASCVD, particularly thromboembolic and cerebrovascular outcomes. These findings highlight the importance of cardiovascular risk awareness in CLE care. Key evidence gaps remain regarding subtype-specific risks, long-term outcomes, and standardized definitions. Future prospective studies are needed to refine screening and prevention strategies.
Data Sharing Statement
All data supporting this review are contained within the published articles cited in the manuscript.
Ethics Approval and Informed Consent
Not applicable. This study is a systematic review and did not involve human participants, animals, or patient-level data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that they received no funding for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singh AG, Crowson CS, Singh S, et al. Risk of cerebrovascular accidents and ischemic heart disease in cutaneous lupus erythematosus: a population-based cohort study. Arthritis Care Res. 2016;68(11):1664–9. doi:10.1002/acr.22892
2. Patil MK, Salazar CE, Nayudu K, Rohan TZ, Nambudiri VE. Comorbidities associated with discoid lupus erythematosus: a case-control study in the all of us research program. Exp Dermatol. 2024;33(8):e15162. doi:10.1111/exd.15162
3. He E, Hino C, Aihie O, et al. Analysis of cutaneous lupus hospitalizations: a United States national population-based study. Cureus. 2023;15(5):e38982. doi:10.7759/cureus.38982
4. Zhao M, Feng R, Werth VP, Williams KJ. State of current management of the heightened risk for atherosclerotic cardiovascular events in an established cohort of patients with lupus erythematosus. Lupus Sci Med. 2023;10(2):e000908. doi:10.1136/lupus-2023-000908
5. Olbrich H, Kridin K, Zirpel H, et al. Cutaneous lupus erythematosus is associated with an increased risk of cardiac and vascular diseases: a large-scale, propensity-matched global retrospective cohort study. EBioMedicine. 2023;93:104639. doi:10.1016/j.ebiom.2023.104639
6. Hesselvig JH, Ahlehoff O, Dreyer L, Gislason G, Kofoed K. Cutaneous lupus erythematosus and systemic lupus erythematosus are associated with clinically significant cardiovascular risk: a Danish nationwide cohort study. Lupus. 2017;26(1):48–53. doi:10.1177/0961203316651739
7. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
8. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan-a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. doi:10.1186/s13643-016-0384-4
9. Munn Z, Moola S, Lisy K, Riitano D, Tufanaru C. Methodological guidance for systematic reviews of observational epidemiological studies reporting prevalence and cumulative incidence data. Int J Evid Based Healthc. 2015;13(3):147–153. doi:10.1097/XEB.0000000000000054
10. Chen HW, Liu J, Yang DM, et al. Incidence and prevalence of atherosclerotic cardiovascular disease in cutaneous lupus erythematosus. JAMA Dermatol. 2025;161(2):175–182. doi:10.1001/jamadermatol.2024.4991
11. Guo LN, Nambudiri VE. Cutaneous lupus erythematosus and cardiovascular disease: current knowledge and insights into pathogenesis. Clin Rheumatol. 2021;40(2):491–499. doi:10.1007/s10067-020-05257-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.