Back to Journals » International Journal of Women's Health » Volume 18
Association Between Body Fat Percentage and Endometriosis Severity Based on American Association of Gynecologic Laparoscopists 2021 Endometriosis Classification
Authors Milla H ![]() , Ritonga MA
, Ritonga MA ![]() , Bayuaji H
, Bayuaji H ![]() , Heriyanto A
, Heriyanto A ![]() , Direza FH
, Direza FH ![]()
Received 18 November 2025
Accepted for publication 9 February 2026
Published 17 February 2026 Volume 2026:18 582542
DOI https://doi.org/10.2147/IJWH.S582542
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Haidarotul Milla,1 Mulyanusa Amarullah Ritonga,2 Hartanto Bayuaji,2 Agus Heriyanto,1 Fikry Haerusulistio Direza3
1Department of Obstetrics and Gynecology, Hasan Sadikin General Teaching Hospital, Faculty of Medicine, Padjadjaran University, Bandung, West Java, Indonesia; 2Endocrinology Reproductive and Fertility Division, Department of Obstetrics and Gynecology, Hasan Sadikin General Teaching Hospital, Faculty of Medicine, Padjadjaran University, Bandung, West Java, Indonesia; 3Faculty of Medicine, Padjadjaran University, Bandung, West Java, Indonesia
Correspondence: Haidarotul Milla, Department of Obstetrics and Gynecology, Hasan Sadikin General Teaching Hospital, Faculty of Medicine, Padjadjaran University, Pasteur No. 38 Street, Pasteur, Bandung, West Java, 40161, Indonesia, Tel +6281388857911, Email [email protected]
Purpose: Endometriosis is one of the main reproductive issues that the modifiable risk factors is still the main research focus. It is still unclear how various adiposity affect the onset and spread of endometriosis because some studies have found that there was inverse correlation, while others showed different findings. This study aims to determine the association between body fat percentage (BFP) and the severity of endometriosis in women of reproductive age using American Association of Gynecologic Laparoscopists (AAGL) 2021 Endometriosis Classification.
Patients and Methods: This was a cross-sectional analytic design conducted at Hasan Sadikin Hospital from July to October 2025. Some inclusion (endometriosis woman who will undergo laparoscopic surgery with age of 20– 45 years) and exclusion (subject with suspected malignancy) criteria are applied in this study. Statistical analysis was performed to determine the significance of baseline characteristic, body mass index (BMI), waist–hip ratio (WHR), mid-upper arm circumference (MUAC), and BFP towards AAGL endometriosis stage.
Results: Our analysis indicates that the baseline characteristic showed no significant differences between the two groups (Mild-Moderate [Stage I–II] vs Severe [Stage III–IV]). Subsequently, this study revealed significant results WHR, MUAC, and BMI with p-values of 0.012, < 0.001, and 0.023, respectively, towards AAGL stage. The study found a significant association between BFP and AAGL stage, with p-values < 0.001. The negative association between WHR and MUAC with Body Fat Percentage towards AAGL was significant for WHR ≤ 0.80, WHR > 0.80, and MUAC ≤ 23 cm, but not for MUAC > 23 cm.
Conclusion: The study found a significant inverse relationship between BFP and endometriosis stage, with similar results for other measurements like BMI, WHR, and MUAC. In addition, shorter menstrual cycles due to high BFP were also associated with an increased risk of endometriosis.
Keywords: endometriosis, body fat percentage, American association of gynecologic laparoscopists, obesity
Introduction
Endometriosis, which is characterised by the development of endometriotic lesions from endometrial glands and stroma, is one of the main reproductive issues. According to World Health Organization, an estimated 10% of women globally who are of reproductive age have endometriosis (190 million).1 About 6–10% of women of reproductive age suffer endometriosis, which is also found in 40–60% of women who experience pelvic pain and 30–50% of infertile women.2 Furthermore, compared to women without endometriosis, those with the condition had a 20% lower quality of life.3 It is suggested that endometriosis is linked to other conditions that are marked by inflammation and oxidative stress, including atopic diseases, asthma, autoimmune, cardiovascular, and malignancies.4,5 Endometriosis remains a clinical enigma despite its very high incidence and impact because of its contentious origin and lack of diagnostic biomarkers.6 Patients with symptomatic endometriosis may be treated with hormonal medications that suppress menstruation and ovulation, surgery, or a combination of the two. Although they have not been thoroughly investigated, diet and lifestyle changes may possibly be beneficial.7
It is still unclear how various adiposity affect the onset and spread of endometriosis, even though some risk factors, such early age at menarche and short menstrual cycle length, have been regularly documented.5,6 Comprehensive epidemiological research has shown that those with endometriosis are more likely to be underweight and have a lower BMI than control subjects.8 Then, a number of studies have looked into the connection between endometriosis and body mass index (BMI). Some studies have found that there was inverse correlation between endometriosis and BMI. These findings were obtained by a case–control study conducted by Yun et al, a descriptive‑comparative study by Vaghar et al, and a meta-analysis study by Liu Y.9–11 Another risk factor for endometriosis is an increased distribution of fat in the body, especially the peripheral fat.12 The results of the waist-to-hip ratio (WHR), which is associated to fat distribution, also varied. Women’s reproductive status and health are associated with lower WHR.13 Additionally, according to Backonja et al, women who have a smaller mid-upper arm circumference (MUAC) are more likely to develop endometriosis than those who have a greater MUAC.14
While many studies have successfully demonstrated the inverse relationship between adipose tissue and endometriosis as measured by various methods, there are some other studies that show different findings. A cross-sectional study conducted by Saha et al showed that there was no correlation between BMI and endometriosis.15 Then, in a cross-sectional study conducted by Silva et al also found that no significant difference in both group (endometriosis vs no endometriosis) towards association with BFP.16 By looking at these data, this study aims to determine the correlation between BFP and the severity of endometriosis in women of reproductive age using American Association of Gynecologic Laparoscopists (AAGL) 2021 Endometriosis Classification.
Materials and Methods
Study Design and Settings
This was a cross-sectional analytic design conducted at Hasan Sadikin Hospital from July to October 2025.
Study Population
Primary data was collected through a screening process based on inclusion and exclusion criteria.
Subject included in this study was endometriosis woman who will undergo laparoscopic surgery with age of 20–45 years. Subjects with suspected malignancy were excluded from this study.
Sample Size Estimation
In this study, the author used a minimum sample size of 30 participants based on the rule of thumb (comparison groups should have 30 participants each).17 As the aim was to compare two different groups, with this number, each group had a minimum sample size of 30, with a total minimum of 60 participants.
Data Collection and Measurements
Baseline Characteristics
Participants completed questionnaires on sociodemographic factors, such as age (years), age of menarche (years), history of parity, and length of marriage (years). In addition, participants were also asked about their menstrual cycle history (normal [24–38 days]; abnormal [>38 days])18 and history of dysmenorrhea, dyspareunia, pelvic pain (outside the menstrual cycle), and dyschezia.
Body Fat Percentage (BFP)
BFP in this study was assessed with a specialized-digital body fat measurement scale (OneMed Body Fat Scan 825; SKU B000010695; Tangerang, Indonesia) using 8 electrodes. This device uses the principle of bioelectrical impedance analysis (BIA). For women, a BFP between 18% and 28% is considered healthy. Thus, BFP <18 was categorised as low, 18–28 as normal, and >28 as high in this study.19
Body Mass Index (BMI)
In this study, the BMI was also calculated by calculating the weight-to-height square ratio. BMI categories based on the Asia-Pacific classification are as follows: (1) underweight (<18.5), (2) normal weight (18.5–22.9), (3) overweight (23–24.9), and (4) obese (≥25).20
Waist–Hip Ratio (WHR)
WHR defined as the ratio of waist circumference to hip circumference. While the hip circumference was measured at the widest point of the buttock and at the conclusion of a typical expiration, the waist circumference was measured in the middle between the last ribs that could still be felt with crista illiaca. The WHR with >0.80 was taken as high for women.21
Mid-Upper Arm Circumference (MUAC)
The circumference of the middle portion of an inactive arm is measured by MUAC. The olecranon, or elbow portion, and the acromion, or protruding portion of the shoulder, are the midpoints of the upper arm’s circumference, which is measured by MUAC. Cut-off points for MUAC (≤23.0 cm) can be an indicator of low BMI (<18.5).22
American Association of Gynecologic Laparoscopists (AAGL) 2021 Endometriosis Classification
In November 2021, the American Association of Gynecologic Laparoscopists (AAGL) 2021 Endometriosis Classification was released, claiming to replace the revised American Society for Reproductive Medicine (rASRM) with a better staging system. Utilizing a schema of disease location, morphology, and size, the tool produces cumulative points that are subsequently applied to preset thresholds for stage allocation.23 The following are the staging categories of AAGL 2021: (1) Stage 1 (≤ 8), (2) Stage 2 (9 to 15), (3) Stage 3 (16 to 21), (4) Stage 4 (>21).24 In this study, we grouped the four stages of AAGL into two groups, which were Stage I–II (mild-moderate) and Stage III–IV (severe) and the staging assessment was assessed by the operating surgeon, while the patient is undergoing the laparoscopy procedure.
Statistical Analysis
Statistical calculations were performed analytically using SPSS Software 27th Edition (IBM Corp. Released 2020. IBM SPSS Statistics for Window, Version 27.0. Armonk, NY: IBM Corp). The variables in this study used univariate analysis with T-test and Mann–Whitney test if the data were not normally distributed. The chi-square test was then utilized in bivariate analysis. The significance of the test results was determined based on the p value <0.05.
Results
During the research period, we obtained 30 participants in the Stage I–II group and another 30 in the Stage III–IV group (a total of 60 participants). There were no significant differences between the baseline characteristics in both AAGL stage groups in this study, as shown in Table 1. However, in the history of menstrual cycle variable, it was found that in the stage I–II group, the majority was dominated by abnormal menstrual cycles (56.7%), while in stage III–IV, it was dominated by normal menstrual cycles (66.7%).
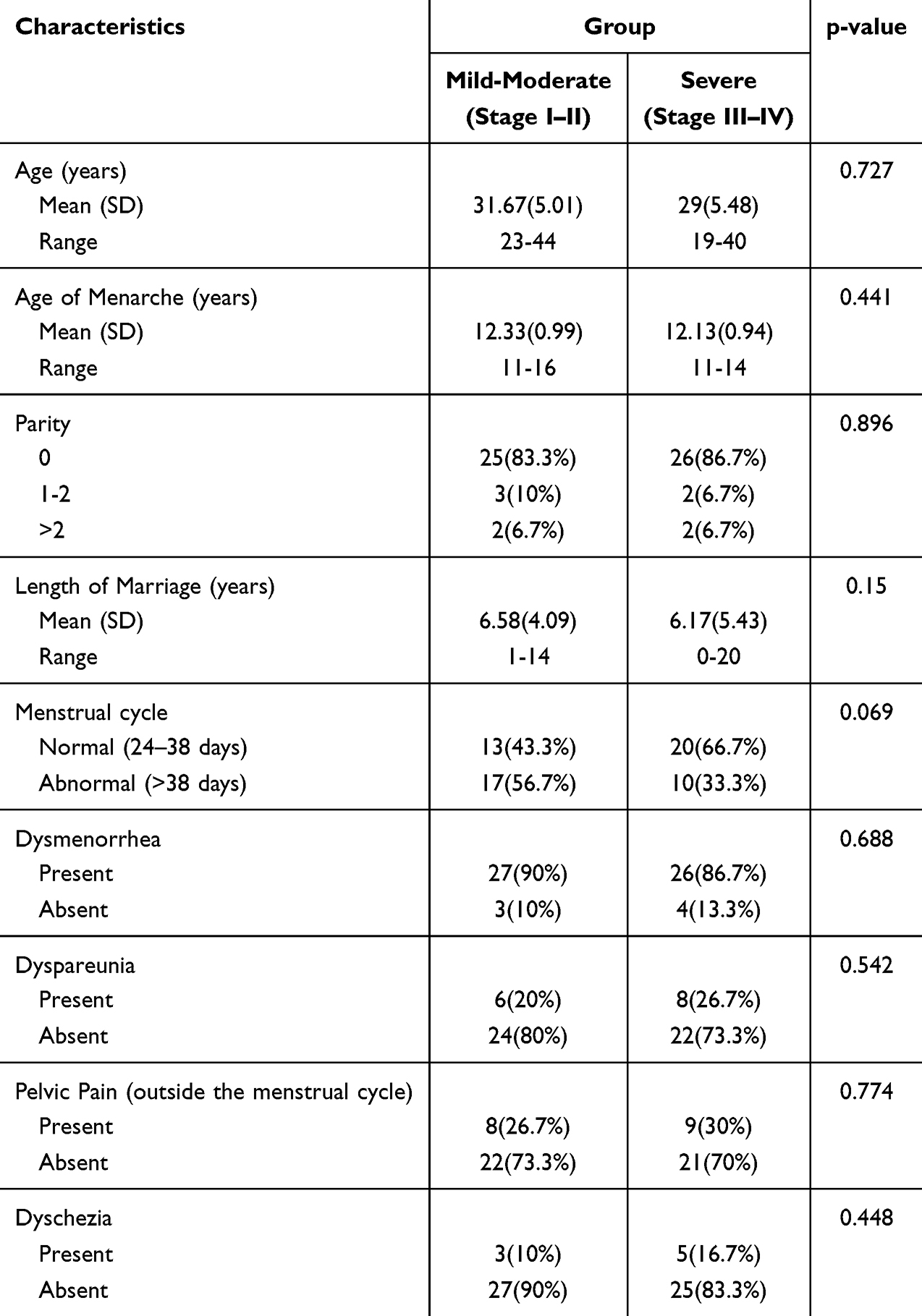 |
Table 1 Baseline Characteristics of Study Subject |
Table 2 demonstrates the results of the analysis of the correlation between WHR, MUAC, and BMI with AAGL stage. In the WHR variable, it was found that WHR >0.80 dominated in both groups (83.33% in the Stage I–II group; 53.33% in the Stage III–IV group). Then, a different finding was observed in the MUAC variable, where MUAC >23 cm was found to dominate in the Stage I–II group (86.7%), while MUAC ≤23 cm dominated in the Stage III–IV group (83.33%). Another interesting finding was discovered in the BMI category, where normal weight was the majority in both groups (46.67% in the Stage I–II group; 66.67% in the Stage III–IV group). This study revealed significant results for all three variables with p-values of 0.012, <0.001, and 0.023, respectively.
 |
Table 2 The Association of Waist-to-Hip Ratio, Mid-Upper Arm Circumference and Body Mass Index with Endometriosis |
Furthermore, an analysis was also conducted between the correlation of BFP and Stage AAGL, as shown in Table 3. Statistical analysis showed significant results with a p-value <0.001. Moreover, a correlation analysis was conducted between WHR and MUAC with BFP towards AAGL stage in Table 4. Statistical results showed significance in the variables WHR ≤0.80, WHR >0.80, and MUAC ≤23 cm with p-values of 0.005, 0.002, and 0.029, respectively. However, for the MUAC >23 cm variable, the results were not significant with a p-value of 0.893.
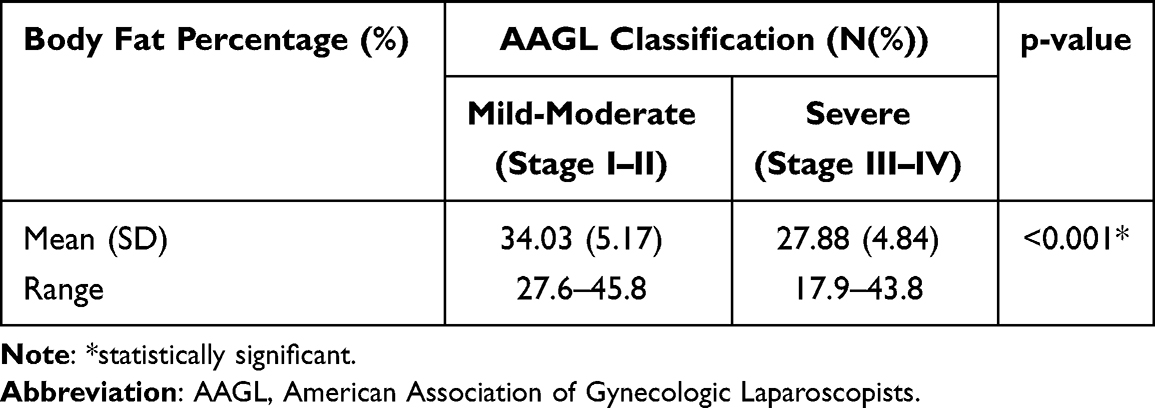 |
Table 3 Correlation of Body Fat Percentage with Endometriosis |
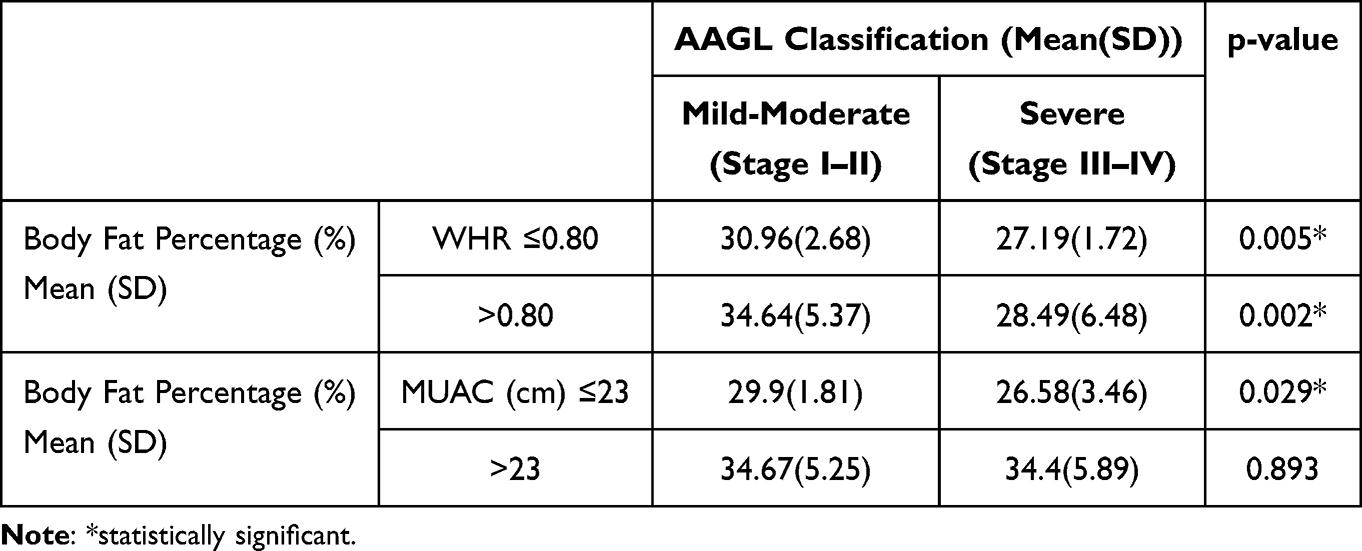 |
Table 4 Correlation of Waist-to-Hip Ratio and Mid-Upper Arm Circumference to Body Fat Percentage Towards Endometriosis |
Discussion
In this study, we examined the relationship between BFP measured using a validated and calibrated body fat scale. In addition, other body measurements were taken, including BMI, WHR, and MUAC. From the characteristic data, ranging from age, age at menarche, parity, length of marriage, and menstrual cycle, it was found that these variables did not differ between the two AAGL stage groups. This finding is consistent with the results of research by Byun et al, which showed that there were no clear associations between a woman’s characteristics and stage of endometriosis.6
In terms of menstrual cycle history, although no significant results were found between the two groups, it was found that the Stage I–II group was dominated by participants with abnormal menstrual cycles (56.7%), while in the Stage III–IV group, the opposite was observed, with normal menstrual cycles dominating (66.7%). Shorter menstrual cycle duration and endometriosis have been identified as risk factors for endometriosis,25 as happened in this case. Then, in a meta-analysis study conducted by Wei et al, it was found that menstrual cycle length shorter than or equal to 27 days increase the risk of endometriosis and cycle length longer than or equal to 29 days decrease the risk.26 The phenomenon observed in this study and several other studies can be explained by Sampson’s theory of retrograde menstruation. According to the basic theory, endometrial cells that are present in menstrual blood regurgitate into the peritoneal cavity through patent fallopian tubes, where they may be implanted.27 A short menstrual cycle often indicates a higher frequency of menstruation and a higher risk of exposure to it. This may lead to an increased risk of retrograde bleeding and, ultimately, a higher incidence of endometriosis.26
The association between short menstrual cycle duration and increased risk of endometriosis may also be related to BFP levels. Obesity are associated with greater menstrual cycle irregularity and the polycystic ovary syndrome (PCOS), which can result in infrequent or absent menstrual periods.28 The impact of obesity on irregular menstruation is complex. Obese people have a lot of adipose tissue, which is important for steroid metabolism and increases the synthesis of estrogen. The activity of aromatase, which changes androgens into estrogens in fat tissues, disturbs the hormonal balance and causes irregular menstruation. Adipokines such as leptin and adiponectin, which are essential for controlling menstrual cycles and reproductive hormones, are also impacted by obesity.29 In addition, obesity affects menstrual cycle disruption, eventually leading to endometriosis due to a chronic low-grade inflammation process characterised by elevated levels of inflammatory cytokines like TNF-α, IL-6, and CRP.30
In the incidence of dysmenorrhea, dyspareunia, pelvic pain (outside the menstrual cycle), and dyschezia, no significant differences were found between the two groups in this study. In a retrospective study, Piriyev et al used the ENZIAN classification to analyze the relationship between BMI and endometriosis. They found no significant differences in dysmenorrhea between patients with and without deep infiltrating endometriosis. However, different results were found for dyspareunia and dyschezia, which were found to be significant in the same study.31 In endometriosis, adipose-derived hormones and cytokines (such leptin) stimulate angiogenesis and systemic inflammation. Therefore, obesity may change sensory thresholds or lesion activity. Low BMI, on the other hand, may exacerbate neurogenic hyperalgesia. Overall, these BMI-specific symptom patterns seem to be shaped by the interaction of neurological, hormonal/metabolic, and inflammatory variables, as findings vary between this study and the study conducted by Piriyev et al.31,32
In terms of WHR, MUAC, and BMI measurements in relation to AAGL stage, it was found that all three variables differed statistically between the two groups. For all three variables, it was found that WHR ≤0.80, MUAC ≤23 cm, and low BMI were more prevalent in AAGL stages III–IV. Previous research has linked endometriosis to a lower BMI, a smaller WHR, or a smaller waist circumference, and smaller MUAC.14 Furthermore, correlations between decreased obesity characteristics and the severity of endometriosis have been documented.33 The inverse relationship between BMI and endometriosis diagnosis has been explained by a number of theories. It is commonly known that anovulation and/or oligomenorrhea are frequently linked to obesity or larger bodies. Therefore, obese women may have a lower risk of menstruation regurgitation in the pelvic cavity.12 However, by controlling for menstrual variables in their studies, epidemiological data have demonstrated that BMI is an independent risk related with the frequency of endometriosis. Another theory is that endometriosis-related chronic pain sensations cause gastrointestinal issues or emotional stress, which lowers appetite and food intake and causes endometriosis-affected women to have smaller bodies.8,34
In terms of BFP, this study found that BFP levels were higher in the AAGL Stage I–II group than in the Stage III–IV group, and this was statistically significant. This indicates a correlation between low body fat levels and the severity of endometriosis. In this regard, in a study of 45 women with endometriosis verified by laparoscopy and 46 controls, the WHR and waist-to-thigh ratios were found to be negatively associated with endometriosis risk in women under 30. More peripheral body fat was associated with greater estrogen levels in the case group, indicating that a particular somatotype with a preponderance of peripheral body fat was linked to the condition. Furthermore, lean body habits, specifically low levels of adipose tissue and adipose tissue below the waist, were linked to endometriosis, according to a recent systematic review that included 21 papers.3 This result was in line with the theory that estrogen affects the quantity and distribution of adipose tissue, given that endometriosis is an estrogen-dependent condition.12
A major strength of this study lies in its various measurements to assess the association between BFP and endometriosis. Measurements using standardised body fat scales, BMI, WHR, and MUAC were used in this study. In addition, we also sought associations between patient characteristics and BFP and endometriosis.
This study has several limitations. First, the study sample included women only from Indonesia, which limits generalizability. Second, this study utilised a body fat scale measuring device that uses BIA, which has limitations including potential inaccuracies due to factors like hydration levels, foot placement, and body weight fluctuations. This may affect the results of BFP measurements for each patient. Third, while this study used a small sample size, further research with larger samples could be performed to validate the findings. Finally, we did not include data on the reasons for surgery (fertility, pain management, diagnosis, etc). These limitations restrict the extrapolation and generalisation of the research results.
Conclusion
In summary, our study demonstrated a significant inverse relationship between BFP and endometriosis stage as assessed by AAGL. Other measurement variables, including BMI, WHR, and MUAC, showed similar results. In addition, shorter menstrual cycles due to high BFP are also associated with an increased risk of endometriosis.
Ethics Approval and Consent to Participate
This study complies with the Declaration of Helsinki and was approved by the Ethics Committee of Dr. Hasan Sadikin General Hospital, Bandung with number of DP.04.03/D.XIV.6.5/346/2025. Informed consent was obtained from all individual participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Endometriosis. World Health Organization. 2025 [Cited January 4, 2026]. Available from: https://www.who.int/news-room/fact-sheets/detail/endometriosis.
2. Saunders PTK, Horne AW. Endometriosis: etiology, pathobiology, and therapeutic prospects. Cell. 2021;184(11):2807–9. doi:10.1016/j.cell.2021.04.041
3. Backonja U, Buck Louis GM, Adiposity LDRO. Adipose tissue distribution, and endometriosis: a systematic review. Nurs Res. 2016;65(2):151–166. doi:10.1097/NNR.0000000000000146
4. Kvaskoff M, Mu F, Terry KL, et al. Endometriosis: a high-risk population for major chronic diseases? Hum Reprod Update. 2015;21(4):500–516. doi:10.1093/humupd/dmv013
5. Shafrir AL, V FL, Shah DK, et al. Risk for and consequences of endometriosis: a critical epidemiologic review. Best Pract Res Clin Obstet Gynaecol. 2018;51:1–15. doi:10.1016/j.bpobgyn.2018.06.001
6. Byun J, Peterson CM, Backonja U, et al. Adiposity and endometriosis severity and typology. J Minim Invasive Gynecol. 2020;27(7):1516–1523. doi:10.1016/j.jmig.2020.01.002
7. Allaire C, Bedaiwy MA, Yong PJ. Diagnosis and management of endometriosis. CMAJ. 2023;195(10):E363–E371. doi:10.1503/cmaj.220637
8. Holdsworth-Carson SJ, Dior UP, Colgrave EM. The association of body mass index with endometriosis and disease severity in women with pain. J Endometr Pelvic Pain Disord. 2018;10(2):79–87. doi:10.1177/2284026518773939
9. Yun KY, Hwang SY, Lee HJ, et al. The association of body mass index with incidence, stage and recurrence of endometriosis: case-control study in Korean women. CEOG. 2020;47(1):53–56.
10. Vaghar M. Evaluation of lifestyle and endometriosis in infertile women referring to the selected hospital of Tehran University medical sciences. J Family Med Prim Care. 2019;8(11):3574. doi:10.4103/jfmpc.jfmpc_496_19
11. Liu Y, Zhang W. Association between body mass index and endometriosis risk: a meta-analysis. Oncotarget. 2017;8(29):46928.
12. Hong J, Yi K. What is the link between endometriosis and adiposity? Obstet Gynecol Sci. 2022;65(3):227–233. doi:10.5468/ogs.21343
13. Butovskaya M, Sorokowska A, Karwowski M, et al. Waist-to-Hip ratio, body-mass index, age and number of children in seven traditional societies. Sci Rep. 2017;7(1):1622. doi:10.1038/s41598-017-01916-9
14. Backonja U, Hediger ML, Chen Z, et al. Beyond body mass index: using anthropometric measures and body composition indicators to assess odds of an endometriosis diagnosis. J Womens Health. 2017;26(9):941–950. doi:10.1089/jwh.2016.6128
15. Saha R, Kuja-Halkola R, Tornvall P, Marions L. Reproductive and lifestyle factors associated with endometriosis in a large cross-sectional population sample. J Womens Health. 2016;26(2):152–158. doi:10.1089/jwh.2016.5795
16. da SJB, Gurian MBF, Nonino CB, et al. Analysis of body composition and pain intensity inwomen with chronic pelvic pain secondary to endometriosis. Revista Brasileira de Ginecologia e Obstetrícia. 2020;42.
17. Praharaj S, Ameen S. Sample size estimation in research: necessity or compromise? Kerala J Psychiatry. 2024;37(1):66–71.
18. Munro MG, Critchley HOD, Fraser IS; Committee the FMD. The two FIGO systems for normal and abnormal uterine bleeding symptoms and classification of causes of abnormal uterine bleeding in the reproductive years: 2018 revisions. Int J Gynecol Obstet. 2018;143(3):393–408. doi:10.1002/ijgo.12666
19. Lebiedowska A, Hartman-Petrycka M, Błońska-Fajfrowska B. How reliable is BMI? Bioimpedance analysis of body composition in underweight, normal weight, overweight, and obese women. Irish J Med Sci. 2021;190(3):993–998. doi:10.1007/s11845-020-02403-3
20. Artime E, Zimner-Rapuch S, Chen R, et al. Clinical and humanistic burden of adult obesity in Asia–Pacific: a systematic literature review. Advanc Therap Adis. 2025;42(10):4741–4767. doi:10.1007/s12325-025-03324-2
21. Gadekar T, Dudeja P, Basu I, Vashisht S, Mukherji S. Correlation of visceral body fat with waist–hip ratio, waist circumference and body mass index in healthy adults: a cross sectional study. Med J Armed Forces India. 2020;76(1):41–46. doi:10.1016/j.mjafi.2017.12.001
22. Hanifah AV, Budihastuti UR, Balgis B. The association between body mass index, waist to hip ratio and mid-upper arm circumference with endometriosis. Unnes J Public Health. 2022;11(2):173–178. doi:10.15294/ujph.v11i2.46095
23. Mak JN, Uzuner C, Espada M, et al. Inter-observer reproducibility of the 2021 AAGL endometriosis classification. Aust N Z J Obstetrics Gynaecol. 2025;65(1):101–106. doi:10.1111/ajo.13851
24. Abrao MS, Andres MP, Miller CE, et al. AAGL 2021 endometriosis classification: an anatomy-based surgical complexity score. J Minim Invasive Gynecol. 2021;28(11):1941–1950.e1. doi:10.1016/j.jmig.2021.09.709
25. Harder C, Velho RV, Brandes I, Sehouli J, Mechsner S. Assessing the true prevalence of endometriosis: a narrative review of literature data. Int J Gynecol Obstet. 2024;167(3):883–900. doi:10.1002/ijgo.15756
26. Wei M, Cheng Y, Bu H, Zhao Y, Zhao W. Length of menstrual cycle and risk of endometriosis: a meta-analysis of 11 case–control studies. Medicine. 2016;95(9):e2922. doi:10.1097/MD.0000000000002922
27. Lamceva J, Uljanovs R, Strumfa I. The main theories on the pathogenesis of endometriosis. Int J Mol Sci. 2023;24(5):4254. doi:10.3390/ijms24054254
28. Itriyeva K. The effects of obesity on the menstrual cycle. Curr Probl Pediatr Adolesc Health Care. 2022;52(8):101241. doi:10.1016/j.cppeds.2022.101241
29. Zheng L, Yang L, Guo Z, Yao N, Zhang S, Pu P. Obesity and its impact on female reproductive health: unraveling the connections. Front Endocrinol. 2024;14:1326546.
30. Šišljagić D, Blažetić S, Heffer M, Vranješ Delać M, Muller A. The interplay of uterine health and obesity: a comprehensive review. Biomedicines. 2024;12(12):2801. doi:10.3390/biomedicines12122801
31. Piriyev E, Mennicken C, Schiermeier S, Römer T. Does BMI have an impact on endometriosis symptoms and endometriosis types according to the #ENZIAN classification? J Clin Med. 2025;14(12):4040. doi:10.3390/jcm14124040
32. Rahman MS, Park Y, Hosseinirad H, Shin JH, Jeong JW. The interplay between endometriosis and obesity. Trends Endocrinol Metab. 2025;36(12):1140–1153. doi:10.1016/j.tem.2025.03.011
33. Rahmioglu N, Macgregor S, Drong AW, et al. Genome-wide enrichment analysis between endometriosis and obesity-related traits reveals novel susceptibility loci. Hum Mol Genet. 2015;24(4):1185–1199. doi:10.1093/hmg/ddu516
34. Pantelis A, Machairiotis N, Lapatsanis DP. The formidable yet unresolved interplay between endometriosis and obesity. Sci World J. 2021;2021(1):6653677. doi:10.1155/2021/6653677
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.