Back to Journals » International Journal of Women's Health » Volume 18
Association Between Baseline Mammographic Breast Density and the Incidence of Natural Menopause in Korean Women: A Nationwide Population–Based Study Using National Health Screening Data
Authors Yoon H ![]() , Park JY, Kim C, Shin I, Park JY, Chung YJ, Han K
, Park JY, Kim C, Shin I, Park JY, Chung YJ, Han K
Received 13 April 2026
Accepted for publication 1 June 2026
Published 9 June 2026 Volume 2026:18 616569
DOI https://doi.org/10.2147/IJWH.S616569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Hyonjee Yoon,1 Ju-Yeong Park,2 Chaewon Kim,1 Inhye Shin,3 Jung Yoon Park,4 Youn-Jee Chung,4 Kyungdo Han2
1Department of Obstetrics and Gynecology, Eunpyeong St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea; 2Department of Statistics and Actuarial Science, Soongsil University, Seoul, Republic of Korea; 3Department of Obstetrics and Gynecology, Yeouido St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea; 4Department of Obstetrics and Gynecology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea
Correspondence: Youn-Jee Chung, Department of Obstetrics and Gynecology, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, 222 Banpo–Daero, Seocho–Gu, Seoul, 06591, Republic of Korea, Email [email protected] Kyungdo Han, Department of Statistics and Actuarial Science, Soongsil University, 369 Sangdo–ro, Dongjak–gu, Seoul, 06978, Republic of Korea, Email [email protected]
Background: High mammographic breast density (MBD) reflects cumulative exposure to sex hormones. While it is well established that breast density declines during the menopausal transition, the association between baseline MBD and the subsequent timing of natural menopause remains underexplored. We investigated the relationship between baseline MBD and incident natural menopause in Korean women.
Methods: We conducted a retrospective cohort study using the Korean National Health Insurance Service database. A total of 428,998 premenopausal women aged 40– 55 years who underwent breast cancer screening in 2009 were included. Baseline MBD was classified using the BI–RADS system. Incident natural menopause was defined by consistent self–reports across at least two subsequent screenings (2011– 2013). Multivariate logistic regression models were used to estimate odds ratios (ORs) for incident menopause, adjusting for confounders including age, BMI, and reproductive history.
Results: A total of 73,599 women (17.16%) experienced natural menopause. Higher MBD was associated with progressively lower odds of incident menopause. Women with extremely dense breasts exhibited the lowest likelihood of reaching menopause (adjusted OR 0.8, 95% CI 0.77– 0.83), indicating a delayed menopausal transition. Stratified analyses revealed that the inverse association was more pronounced in women age < 50 years and those with late menarche (≥ 13 years).
Conclusion: High premenopausal MBD was independently and inversely associated with the incidence of natural menopause, suggesting a potential link between dense fibroglandular tissue and variations in reproductive aging. Clinically, baseline MBD could potentially serve as a readily available indicator to evaluate reproductive aging patterns, aiding in more personalized health counseling regarding reproductive health and surveillance strategies.
Keywords: mammographic density, menopause, reproductive aging
Introduction
Mammographic breast density, which refers to the amount of radiologically dense, fibro–glandular and stromal tissue in the breast, is well–defined as one of the strongest risk factors for breast cancer.1–3 Women with high breast density are known to have four– to six–fold greater risk of breast cancer than women with low density, fatty breasts.1,2 The underlying mechanism behind this association of mammographic density with breast cancer risk is currently unclear, but is hypothesized to be closely related to cumulative lifetime exposure to sex hormones, particularly estrogen.4–7
Mammographic breast density is known to be influenced by various demographic and reproductive factors. Age and body mass index (BMI) are inversely associated with breast density,8,9 whereas nulliparity, late first birth, and hormone replacement therapy are typically associated with higher density.10–13 The most dramatic changes in breast density occur during the menopausal transition. As ovarian function ceases and circulating estrogen and progesterone levels decline, the glandular tissue in the breast regresses and is replaced by fat, leading to a decrease in mammographic density.14,15
However, while the effect of menopause on accelerating the decline of breast density is well documented, the reverse clinical question – whether baseline breast density can serve as an indicator of the subsequent timing of natural menopause – remains largely underexplored. Biologically, it is possible to hypothesize that the maintenance of high breast density might reflect sustained ovarian function and a more robust hormone profile.6,16 If validated, establishing this relationship could carry important clinical implications, as the timing of menopause has profound implications for long–term health outcomes, including cardiovascular disease and osteoporosis.17,18 While previous literature has hinted at shared hormonal pathways, large–scale longitudinal studies clarifying this association are lacking, especially in Asian populations where breast density is generally higher than in Western populations.19,20 Therefore, this study aims to evaluate the potential association between baseline mammographic breast density and the incidence of natural menopause in a large cohort of premenopausal Korean women.
Materials and Methods
Study Design and Data Source
This study is a large–scale, retrospective cohort study using data from the National Health Screening Program (NHSP) of the National Health Insurance Service (NHIS) in Korea. The NHIS provides mandatory universal health insurance coverage for about 97% of the total South Korean population. As part of this service, the NHSP offers biennial health examinations to all individuals aged 40 years or older. The database contains comprehensive health screening information, sociodemographic variables, medical claims, and questionnaire–based health and lifestyle information. The data is open for use for research through anonymization and deidentification of the subjects.
Study Population
A total of 3,109,491 women aged ≥ 40 years who participated in the national health and cancer screening programs between January and December 2009 were initially screened. From this cohort, we first included only women aged ≤ 55 years at baseline (n = 1,726,373) to focus on the perimenopausal period. We then excluded those with missing information on their menopausal status (n = 45,120) and those who were already postmenopausal at baseline (n = 622,066). To ascertain the menopause outcome, we included only participants who underwent at least two follow–up health screenings between 2011 and 2013 (n = 592,569). Finally, we excluded individuals with missing or implausible data for key covariates, such as age at menarche and other reproductive history variables. A final study population of 428,998 premenopausal women was included in the analysis (Figure 1).
 |
Figure 1 Study participant selection flowchart. |
Exposure Assessment: Breast Density
The primary exposure was mammographic breast density, assessed at the baseline health screening in 2009. Breast density was categorized by radiologists according to the American College of Radiology’s Breast Imaging–Reporting and Data System (BI–RADS) into four groups based on the percentage of fibroglandular tissue:21
- < 25% (Almost entirely fatty)
- 25–50% (Scattered areas of fibroglandular density)
- 51–75% (Heterogeneously dense)
- 76–100% (Extremely dense)
For our analysis, we used these four categories, with the < 25% group serving as the reference.
Outcome Ascertainment: Menopause
The primary outcome of the study was incident natural menopause. Menopause status was determined based on self–reported questionnaires administered during the follow–up health screenings from 2011 to 2013. To ensure the reliability of the outcome, menopause was strictly defined as participants who reported being “menopausal” on at least two separate occasions in the health screenings conducted between 2011 and 2013.
Other Baseline Characteristics
Data on a range of potential confounders was collected from the baseline health screening questionnaires and examinations in 2009. Demographic and socioeconomic factors included age and income level (25th percentile or medical aid beneficiary). Body mass index (BMI) was calculated with participants’ height and weight. Lifestyle factors included smoking status, alcohol consumption, and regular physical activity level (moderate exercise for >5 days or vigorous exercise for >3 days per week). Reproductive history included age at menarche, parity (number of live births), breastfeeding history, and history of oral contraceptive use. All baseline anthropometric and physiological parameters, including waist circumference, systolic blood pressure (SBP), and diastolic blood pressure (DBP), were acquired as single–time–point measurements on the specific day of the 2009 baseline health examination.
Statistical Analysis
For the baseline characteristics, we used the Chi–square test for categorical variables and one–way analysis of variance (ANOVA) for continuous variables to compare characteristics across the four breast density groups.
To investigate the association between breast density and incident menopause, we used multivariate logistic regression models to calculate odds ratios (ORs) with 95% confidence intervals (CIs). Logistic regression was selected over time–to–event analyses, because menopausal status was assessed at discrete intervals via biennial health screening questionnaires rather than continuous, exact–date tracking. We developed a series of nested models to adjust for potential confounders (Model 1: non–adjusted; Model 2: adjusted for age; Model 3: adjusted for age, income, smoking, regular exercise; Model 4: adjusted for variables in model 3 plus diabetes mellitus, hypertension, dyslipidemia, and chronic kidney disease; Model 5: adjusted for variables in mode 4 plus age at menarche, parity, breastfeeding, and oral contraceptive). Covariates for the nested multivariate models were selected based on known epidemiological associations with ovarian aging.
Finally, we conducted stratified analyses to assess whether the association between breast density and menopause was consistent across different subgroups, including age (<50 vs. ≥50 years), age at menarche (<13 vs. ≥13 years), parity, breastfeeding history, and oral contraceptive use duration (<1 vs. ≥1 year).
Statistical significance was defined as p < 0.05. Statistical analyses were performed using SAS, version 9.4 (SAS Institute In., Cary, NC, USA).
Statement of Ethics
This study was conducted using fully anonymized data provided by the NHIS (REQ2025110855–002). The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of the Catholic University of Korea (KC25ZASI0761). The requirement for informed consent was waived due to the retrospective nature of the study and the use of deidentified data.
Results
Baseline Characteristics of the Study Population
A total of 428,998 women were included in the final analysis. The baseline characteristics of the study subjects, categorized by mammographic breast density, are presented in Table 1. The mean age of the participants was 44.99 ± 3.85 years. Women with higher breast density were, on average, younger (mean age [SD], 44.37 [3.65] in the highest density group vs. 45.7 [4.03] in the lowest density group). Higher breast density was associated with an earlier age at menarche (menarche before age 14; 37.46% in the highest density group vs. 32.16% in the lowest density group), lower parity (percentage of no live birth; 4.83% vs. 1.98%), and a lower likelihood of having breastfed (no history of breastfeeding; 20.19% vs. 14.15%). There was a strong inverse relationship between breast density and measures of adiposity. As breast density increased, mean BMI, weight, and waist circumference decreased. Meanwhile, lifestyle factors showed varied patterns. Alcohol consumption was positively correlated with breast density, increasing from 26.75% in the lowest density group to 28.7% in the highest. The pattern for regular exercise was non–linear, peaking at 18.28% in the 25–50% density group and decreasing thereafter.
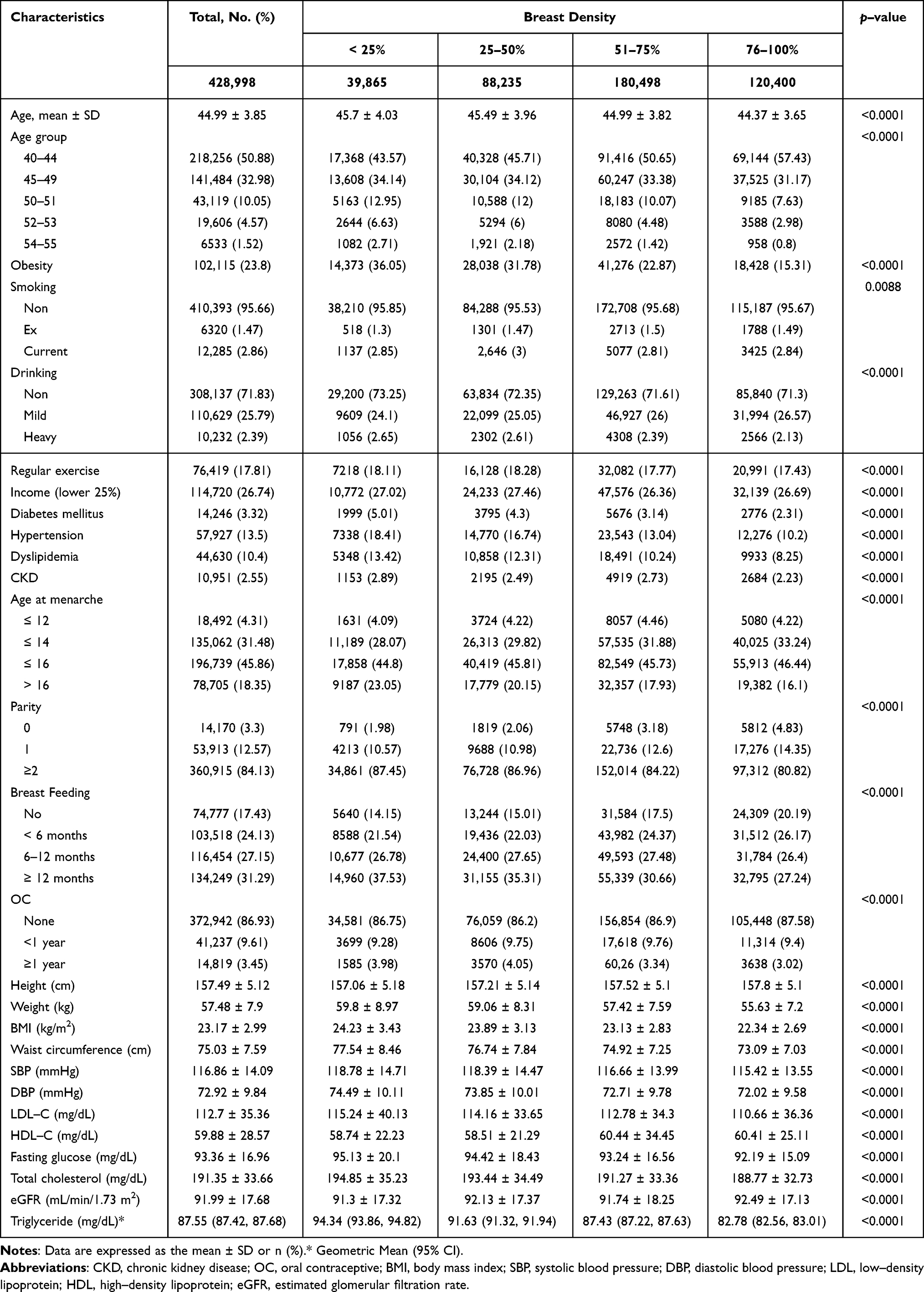 |
Table 1 Baseline Characteristics |
Association Between Breast Density and Incident Menopause
During the follow–up period, a total of 73,599 women (17.16%) experienced menopause. The incidence of menopause decreased as breast density increased, from 22.85% in the lowest density group (<25%) to 12.98% in the highest density group (76–100%) (Table 2). The inverse association between breast density and incident menopause remained statistically significant after adjusting for potential confounding factors in the adjusted models (Model 2–5). In the fully adjusted model (Model 5; adjusted for age, income, smoking, physical activity, DM, hypertension, dyslipidemia, CKD, age at menarche, parity, breastfeeding, and OC), the odds ratios (ORs) were 0.86 (95% CI, 0.83–0.89) for the 51–75% group and 0.8 (95% CI, 0.77–0.83) for the 76–100% group, compared to the reference group of density <25%. The trend was similar, but not statistically significant, for the 25–50% group (OR 0.97, 95% CI, 0.93–1).
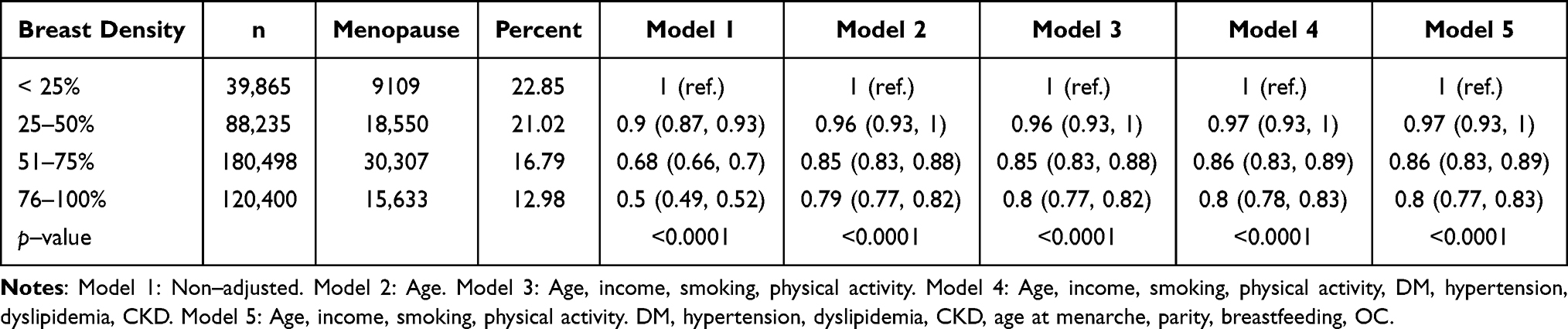 |
Table 2 Association Between Breast Density and Incident Menopause |
Subgroup Analyses
The results of the stratified analyses across various subgroups are presented in Table 3. The inverse association between higher breast density and lower risk of menopause was largely consistent across most subgroups. A statistically significant interaction was observed by age group, with the association appearing stronger in women younger than 50 years old. In this group, when compared to the lowest density group, women with the highest density had 24% lower menopausal rate (OR 0.76, 95% CI, 0.73–0.8). For women aged over 50 years, the trend was similar (OR 0.86, 95% CI, 0.81–0.91), but the magnitude of association was stronger in younger women (p for interaction = 0.0037).
 |
Table 3 Subgroup Analysis of the Association Between Breast Density and Incident Menopause |
A highly significant interaction was found between breast density and age at menarche (p for interaction = 0.0013). For women with menarche at age 13 or older, there was a strong protective relationship, with the highest density group showing a 21% lower menopausal rate (OR 0.79, 95% CI 0.77–0.82). Conversely, for women with early menarche (before age 13), this protective effect was reversed. The 25–50% density group showed a statistically significant 50% increase in menopausal rate (OR 1.5, 95% CI 1.19–1.88), and the 51–75% density group showed a 27% increased rate (OR 1.27, 95% CI 1.03–1.57).
Other subgroups related to reproductive factors also showed similar inverse relationship between breast density and menopausal risk. However, in contrast to age and age at menarche, they did not show statistically significant interactions. The association was consistent regardless of parity (p for interaction = 0.4572), and breastfeeding history (p for interaction = 0.1289).
Discussion
In this large–scale retrospective cohort study of 428,998 premenopausal Korean women, we found a significant inverse association between baseline mammographic breast density and the incidence of natural menopause. Women with higher breast density were less likely to experience menopause during the follow–up health screening period compared to those with lower density, suggesting that high mammographic breast density may serve as a clinical indicator of a later onset of menopause. In the fully adjusted model (adjusted for multiple confounders, including age, BMI, and reproductive history), women with extremely dense breasts (76–100%) had a 20% lower likelihood of experiencing menopause compared to those with fatty breasts (< 25%).
In Table 2, a notable shift in odds ratios was observed from the unadjusted Model 1 (OR 0.5 for the 76–100% group) to the age–adjusted Model 2 (OR 0.79). This substantial shift identifies chronological age as the predominant confounding factor; younger premenopausal women naturally maintain higher breast density and are concurrently less likely to transition into menopause within a short–term tracking window. Notably, following the initial control for age–confounding effect, the adjusted estimates remained highly stale through Model 5. This consistency demonstrates that baseline mammographic breast density holds a robust, independent inversed association with incident menopause.
The relationship between breast density and menopausal status has been investigated in previous studies, and there is a well–established consensus that mammographic breast density undergoes significant involution during the menopausal transition. Longitudinal studies have consistently demonstrated that the cessation of ovarian function leads to a decline in fibroglandular tissue of the breasts and a corresponding increase in adipose tissue.14,15,22–26 Boyd et al14 and Engmann et al23 showed that the rate of density decline accelerates specifically during the perimenopausal period due to the withdrawal of estrogen and progesterone. This phenomenon appears to be universal, as a pooled analysis involving data from 22 countries confirmed that the most rapid reduction in breast density occurs between the ages of 45 and 55, coinciding with the menopausal transition.27 A recent longitudinal study specifically targeting middle–aged Korean women confirmed that mammographic breast density significantly decreases in tandem with rising FSH and falling estradiol levels during the menopausal transition.28
However, the majority of such existing literature has focused primarily on the consequence of menopause on breast tissue. In contrast, the potential for baseline mammographic breast density to serve as a clinical indicator for the timing of natural menopause remains underexplored. Biologically, high mammographic breast density is closely related to cumulative lifetime exposure to sex hormones.6,16 Women with extensive fibroglandular tissue tend to have higher circulating estrogen6,29 and insulin–like growth factor–1 (IGF–1) levels,30 which are markers of robust ovarian function. Since menopause onset is driven by the depletion of ovarian follicles, women with dense breasts may possess a larger ovarian reserve, potentially experiencing a delayed menopausal transition. Our results align with the biological plausibility that the maintenance of dense fibroglandular tissue of the breasts might reflect sustained ovarian activity, ultimately correlating with a later onset of natural menopause.
Notably, this study provides unique evidence from an Asian population. It is well established that Asian women generally exhibit higher mammographic breast density compared to Western populations, despite a lower incidence of breast cancer,19,20 a paradox often attributed to smaller breast volume,31 genetic variants, and dietary differences.32,33 Our findings suggest that despite these baseline ethnic differences in breast tissue composition, the inverse association between fibroglandular tissue and ovarian aging appears to be preserved across ethnic groups. Given that dense breast tissue is highly prevalent in premenopausal Asian women, considering mammographic breast density as a potential clinical indicator for reproductive aging may be particularly relevant in this population.
In the subgroup analysis, we observed a significant interaction between breast density and age at screening (p for interaction = 0.0037), indicating that the magnitude of the association varies by age group. While high breast density was inversely associated with incident menopause in both groups, the inverse association was stronger in women younger than 50 years (OR 0.76; 95% CI, 0.73–0.8) compared to those age 50 years or older (OR 0.86; 95% CI, 0.81–0.91). This finding suggests that mammographic breast density may serve as a more sensitive clinical indicator of ovarian biological age in younger premenopausal women. For women under 50, retaining high breast density may reflect a more preserved ovarian reserve relative to their chronological age, which corresponds to a later onset of menopause. In contrast, for women aged 50 and older – who are already approaching or have surpassed the average age of menopause – the dominant driver of menopausal transition is chronological aging itself. Clinically, this implies that mammographic breast density could be a particularly informative parameter for assessing reproductive aging and health risk stratification in women under 50.
Another notable finding in our stratified analysis was the significant interaction between breast density and age at menarche (p for interaction = 0.0013). Among women with menarche at age 13 or older, high breast density was associated with a delayed onset of menopause, consistent with our main findings. However, in women with early menarche (age <13 years), this inverse association was reversed, and higher density was associated with an increased rate of menopause. Since early menarche is known to be associated with childhood obesity and insulin resistance,34,35 this phenomenon may be due to such metabolic factors, which can independently influence both breast density30 and menopausal timing.36 In this specific subgroup, metabolic dysregulation might alter the typical hormone–density relationship observed in the general population. Further research is needed to validate this hypothesis and fully understand how metabolic dysregulation specifically modifies the clinical relevance of breast density in this population.
The timing of menopause has profound implications for long–term health outcomes. While delayed menopause confers benefits for cardiovascular and bone health, it also increases the risk of hormone–dependent cancers due to prolonged estrogen exposure. Our findings imply that women with high baseline breast density may maintain this dense tissue for a longer duration. Recent evidence by Kulturoglu et al37 demonstrated that women with persistently high breast density who do not experience a decline over time are at a higher risk of breast cancer compared to those whose density decreases. Therefore, the delayed involution of breasts observed in our study population highlights the importance of prolonged vigilance and tailored screening strategies for women with dense breasts. Clinicians could consider high mammographic breast density not only as a risk factor for breast cancer, but also as an informative factor regarding reproductive aging to provide personalized health counseling.
The primary strength of our study is its large, population–based design, which provides robust findings that are broadly representative of women across Korea. A methodological strength lies in the strict ascertainment of menopausal status. By defining the outcome based on consistent self–reported responses across at least two subsequent health screenings (2011–2013), rather than a single time–point measurement, we significantly minimized the potential for misclassification and recall bias common in survey–based studies. Furthermore, the temporal separation between the exposure assessment (baseline breast density in 2009) and the outcome ascertainment ensures that breast density was measured prior to the final determination of menopausal status, thereby clarifying the directionality of the association. Finally, the comprehensive nature of the NHIS database enabled us to adjust for a wide array of potential confounding factors, particularly detailed reproductive history (eg, age at menarche, parity, oral contraceptive use) and metabolic comorbidities, which are critical in analyzing ovarian aging.
Several limitations should also be acknowledged. First, the ascertainment of menopause was based on self–reported questionnaires without biochemical confirmation (eg, FSH or estradiol levels). Although we strengthened the validity of the outcome by requiring consistent responses across serial examinations, the potential for recall bias or misclassification remains, compared to hormonal verification. Second, the follow–up period of 2 to 4 years from the 2009 baseline is relatively short, which restricts our ability to track long–term menopausal timing. Third, the possibility of reverse causation cannot be fully eliminated; because beast density naturally undergoes involution during early perimenopause, women who were chronologically closer to menopause at baseline might have already possessed lower breast density. Although we excluded women who reported being postmenopausal at baseline to minimize this effect, residual confounding may persist. Additionally, potential endocrine parameters that modulate reproductive cyclicity, such as thyroid function indicators, could not be evaluated because they are not included in the standard routine parameters of the National Health Screening Program, and were thus unavailable in the database. Also, the mammographic breast density was assessed using the clinical BI–RADS classification system, rather than a quantitative, software–based measurement. While this may introduce inter–observer variability, BI–RADS represents the standard screening tool in clinical practice, thereby enhancing the real–world applicability of our findings. Lastly, given the observational nature of the study design, it is difficult to establish a definitive causal link. While our findings demonstrate a strong association between breast density and incident menopause, the question of whether it is a direct cause–and–effect relationship or is mediated by common underlying factors remains to be elucidated.
Conclusion
Premenopausal high mammographic breast density is independently and inversely associated with the incidence of natural menopause in Korean women, suggesting that it may reflect the rate of ovarian aging. Future long–term longitudinal studies integrating hormonal assays are warranted to further elucidate the biological pathways linking breast tissue composition to reproductive lifespan.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Boyd NF, Guo H, Martin LJ, et al. Mammographic density and the risk and detection of breast cancer. N Engl J Med. 2007;356(3):227–11. doi:10.1056/NEJMoa062790
2. McCormack VA, Dos Santos Silva I. Breast density and parenchymal patterns as markers of breast cancer risk: a meta–analysis. Cancer Epidemiol Biomarkers Prev. 2006;15(6):1159–1169. doi:10.1158/1055-9965.EPI-06-0034
3. Bodewes FTH, van Asselt AA, Dorrius MD, et al. Mammographic breast density and the risk of breast cancer: a systematic review and meta–analysis. Breast. 2022;66:62–68. doi:10.1016/j.breast.2022.09.007
4. Missmer SA, Eliassen AH, Barbieri RL, et al. Endogenous estrogen, androgen, and progesterone concentrations and breast cancer risk among postmenopausal women. J Natl Cancer Inst. 2004;96(24):1856–1865. doi:10.1093/jnci/djh336
5. Key T. Endogenous sex hormones and breast cancer in postmenopausal women: reanalysis of nine prospective studies. J Natl Cancer Inst. 2002;94(8):606–616. doi:10.1093/jnci/94.8.606
6. Tamimi RM, Byrne C, Colditz GA, et al. Endogenous hormone levels, mammographic density, and subsequent risk of breast cancer in postmenopausal women. J Natl Cancer Inst. 2007;99(15):1178–1187. doi:10.1093/jnci/djm062
7. Clemons M, Goss P. Estrogen and the risk of breast cancer. N Engl J Med. 2001;344(4):276–285. doi:10.1056/NEJM200101253440407
8. Boyd NF, Martin LJ, Sun L, et al. Body size, mammographic density, and breast cancer risk. Cancer Epidemiol Biomarkers Prev. 2006;15(11):2086–2092. doi:10.1158/1055-9965.EPI-06-0345
9. Checka CM, Chun JE, Schnabel FR, et al. The relationship of mammographic density and age: implications for breast cancer screening. AJR Am J Roentgenol. 2012;198(3):W292–5. doi:10.2214/AJR.10.6049
10. Butler LM, Gold EB, Greendale GA, et al. Menstrual and reproductive factors in relation to mammographic density: the Study of Women’s Health Across the Nation (SWAN). Breast Cancer Res Treat. 2008;112(1):165–174. doi:10.1007/s10549-007-9840-0
11. El–Bastawissi AY, White E, Mandelson MT, et al. Reproductive and hormonal factors associated with mammographic breast density by age (United States). Cancer Causes Control. 2000;11(10):955–963. doi:10.1023/a:1026514032085
12. Greendale GA, Reboussin BA, Sie A, et al. Effects of estrogen and estrogen–progestin on mammographic parenchymal density. Postmenopausal Estrogen/Progestin Interventions (PEPI) investigators. Ann Intern Med. 1999;130(4 Pt 1):262–269. doi:10.7326/0003-4819-130-4_Part_1-199902160-00003
13. McTiernan A, Martin CF, Peck JD, et al. Estrogen–plus–progestin use and mammographic density in postmenopausal women: women’s health initiative randomized trial. J Natl Cancer Inst. 2005;97(18):1366–1376. doi:10.1093/jnci/dji279
14. Boyd N, Martin L, Stone J, et al. A longitudinal study of the effects of menopause on mammographic features. Cancer Epidemiol Biomarkers Prev. 2002;11(10 Pt 1):1048–1053.
15. Kerlikowske K, Ichikawa L, Miglioretti DL, et al. Longitudinal measurement of clinical mammographic breast density to improve estimation of breast cancer risk. J Natl Cancer Inst. 2007;99(5):386–395. doi:10.1093/jnci/djk066
16. Martin LJ, Boyd NF. Mammographic density. Potential mechanisms of breast cancer risk associated with mammographic density: hypotheses based on epidemiological evidence. Breast Cancer Res. 2008;10(1):201. doi:10.1186/bcr1831
17. Muka T, Oliver–Williams C, Kunutsor S, et al. Association of age at onset of menopause and time since onset of menopause with cardiovascular outcomes, intermediate vascular traits, and all–cause mortality: a systematic review and meta–analysis. JAMA Cardiol. 2016;1(7):767–776. doi:10.1001/jamacardio.2016.2415
18. Shuster LT, Rhodes DJ, Gostout BS, et al. Premature menopause or early menopause: long–term health consequences. Maturitas. 2010;65(2):161–166. doi:10.1016/j.maturitas.2009.08.003
19. Maskarinec G, Meng L, Ursin G. Ethnic differences in mammographic densities. Int J Epidemiol. 2001;30(5):959–965. doi:10.1093/ije/30.5.959
20. Rajaram N, Mariapun S, Eriksson M, et al. Differences in mammographic density between Asian and Caucasian populations: a comparative analysis. Breast Cancer Res Treat. 2017;161(2):353–362. doi:10.1007/s10549-016-4054-y
21. Magny SJ, Shikhman R, Keppke AL. Breast imaging reporting and data system. In: StatPearls. Treasure Island (FL) ineligible companies: StatPearls Publishing Copyright © 2025, StatPearls Publishing LLC; 2025.
22. Maskarinec G, Pagano I, Lurie G, et al. A longitudinal investigation of mammographic density: the multiethnic cohort. Cancer Epidemiol Biomarkers Prev. 2006;15(4):732–739. doi:10.1158/1055-9965.EPI-05-0798
23. Engmann NJ, Scott C, Jensen MR, et al. Longitudinal changes in volumetric breast density in healthy women across the menopausal transition. Cancer Epidemiol Biomarkers Prev. 2019;28(8):1324–1330. doi:10.1158/1055-9965.EPI-18-1375
24. Kelemen LE, Pankratz VS, Sellers TA, et al. Age–specific trends in mammographic density: the minnesota breast cancer family study. Am J Epidemiol. 2008;167(9):1027–1036. doi:10.1093/aje/kwn063
25. Lokate M, Stellato RK, Veldhuis WB, et al. Age–related changes in mammographic density and breast cancer risk. Am J Epidemiol. 2013;178(1):101–109. doi:10.1093/aje/kws446
26. McCormack VA, Perry NM, Vinnicombe SJ, et al. Changes and tracking of mammographic density in relation to Pike’s model of breast tissue aging: a UK longitudinal study. Int, J, Cancer. 2010;127(2):452–461. doi:10.1002/ijc.25053
27. Burton A, Maskarinec G, Perez–Gomez B, et al. Mammographic density and ageing: a collaborative pooled analysis of cross–sectional data from 22 countries worldwide. PLoS Med. 2017;14(6):e1002335. doi:10.1371/journal.pmed.1002335
28. Cho Y, Jang Y, Woo H–Y, et al. Longitudinal changes in mammographic density and reproductive hormones during the menopausal transition in middle–aged Korean women: effect modification by obesity. Breast Cancer Res. 2025;27(1):193. doi:10.1186/s13058-025-02122-6
29. Boyd NF, Stone J, Martin LJ, et al. The association of breast mitogens with mammographic densities. Br J Cancer. 2002;87(8):876–882. doi:10.1038/sj.bjc.6600537
30. Diorio C, Pollak M, Byrne C, et al. Insulin–like growth factor–I, IGF–binding protein–3, and mammographic breast density. Cancer Epidemiol Biomarkers Prev. 2005;14(5):1065–1073. doi:10.1158/1055-9965.EPI-04-0706
31. Ursin G, Ma H, Wu AH, et al. Mammographic density and breast cancer in three ethnic groups. Cancer Epidemiol Biomarkers Prev. 2003;12(4):332–338.
32. Takata Y, Maskarinec G, Park S–Y, et al. Mammographic density and dietary patterns: the multiethnic cohort. Eur J Cancer Prev. 2007;16(5):409–414. doi:10.1097/01.cej.0000243852.05104.02
33. Mariapun S, Li J, Yip CH, et al. Ethnic differences in mammographic densities: an Asian cross–sectional study. PLoS One. 2015;10(2):e0117568. doi:10.1371/journal.pone.0117568
34. Biro FM, Lucky AW, Simbartl LA, et al. Pubertal maturation in girls and the relationship to anthropometric changes: pathways through puberty. J Pediatr. 2003;142(6):643–646. doi:10.1067/mpd.2003.244
35. Ahmed ML, Ong KK, Dunger DB. Childhood obesity and the timing of puberty. Trends Endocrinol Metab. 2009;20(5):237–242. doi:10.1016/j.tem.2009.02.004
36. Mishra GD, Pandeya N, Dobson AJ, et al. Early menarche, nulliparity and the risk for premature and early natural menopause. Hum Reprod. 2017;32(3):679–686. doi:10.1093/humrep/dew350
37. Kulturoglu MO, Aydin F, Sagdic MF, et al. The impact of changes in breast density over time on breast cancer risk. Sci Rep. 2025;15(1):23900. doi:10.1038/s41598-025-09315-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.