Back to Journals » International Journal of Women's Health » Volume 17
Association Between Allometric Body Shape Indices and Osteoporosis in Postmenopausal Women: A Cross-Sectional Study from NHANES
Received 9 August 2024
Accepted for publication 20 December 2024
Published 22 January 2025 Volume 2025:17 Pages 109—118
DOI https://doi.org/10.2147/IJWH.S490741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Songfeng Zhao,1,2 Xin Pan1,2
1Department of Endocrinology, The First People’s Hospital of Xiaoshan District, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Endocrinology, Xiaoshan Affiliated Hospital of Wenzhou Medical University, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Xin Pan, Department of Endocrinology, The First People’s Hospital of Xiaoshan District, No. 199 South Shixin Road, Xiaoshan District, Hangzhou, Zhejiang, People’s Republic of China, Tel +86-0571-83807971, Email [email protected]
Background: Osteoporosis is a common health concern in postmenopausal women. Obesity, commonly assessed using body mass index (BMI), may have a protective effect on osteoporosis in postmenopausal women. As BMI is limited to the distinguishing fat accumulation, the study aimed to explore the association between allometric body shape indices [including a body shape index (ABSI), hip index, (HI), and waist–hip index (WHI)] and osteoporosis in postmenopausal women.
Methods: Postmenopausal women aged > 50 years in the National Health and Nutrition Examination Survey from 2017 through 2020 (revised to 01/2017 through 12/2020) were included. Potential covariates were selected using the univariate logistic regression models. The association between allometric body shape indices and osteoporosis was explored using weighted univariate and multivariate logistic regression models, with results presented as odds ratios (ORs) and 95% confidence intervals (CIs). The association was further explored in different age and BMI populations. Area under the curve (AUC) analysis was conducted to evaluate the predictive performance of WHI.
Results: In total, 810 postmenopausal women aged > 50 years were included. Among them, 597 (73.70%) women have osteoporosis. WHI ≥ 0.094 (OR = 2.07, 95% CI: 1.14– 3.78) was associated with higher odds of osteoporosis in postmenopausal women. BMI ≥ 30 kg/m2 (OR = 0.23, 95% CI: 0.11– 0.50) was also related to decreased odds of osteoporosis. ABSI ≥ 85.74 was related to a higher incidence of osteoporosis in women aged ≥ 70 years (OR = 4.18, 95% CI: 1.22– 14.35) and BMI ≥ 30 kg/m2 (OR = 4.25, 95% CI: 1.82– 9.95). The WHI has a better predictive performance with an AUC of 0.656 (95% CI: 0.613– 0.699) than the waist–hip ratio.
Conclusion: Higher WHI was associated with an increased incidence of osteoporosis in postmenopausal women. Higher ABSI was related to a higher incidence of osteoporosis in women aged ≥ 70 years and those with a BMI ≥ 30 kg/m2. WHI could predict the incidence of osteoporosis in postmenopausal women.
Keywords: osteoporosis, postmenopausal, a body shape index, hip index, waist–hip index
Introduction
Osteoporosis is a significant public health concern, characterized by reduced bone mass and micro-architectural deterioration of bone tissue, leading to increased bone fragility and susceptibility to fractures.1 Particularly among menopausal women, estrogen levels decline, precipitating dysregulation in bone remodeling processes, thereby accelerating bone loss and the deterioration of bone microarchitecture.1,2 According to the International Osteoporosis Foundation, one in three postmenopausal women is afflicted with osteoporosis, making a heavy burden on both families and society.3,4 The identification of reliable indicators for assessing osteoporosis risk is crucial for early detection and intervention to minimize its impact.
Most research has reported the protective effect of obesity on osteoporosis among postmenopausal women.5–7 Body mass index (BMI) has been commonly used to measure obesity in previous studies, but it fails to distinguish fat accumulation in different body compartments.8 An alternative approach involved creating new, BMI-independent allometric body shape indices, including a body shape index (ABSI),9 hip index (HI),10 and waist-to-hip index (WHI).11 These indices are mathematical conversions of waist circumference (WC), hip circumference (HC), and waist–hip ratio (WHR), respectively, normalized to height and weight; thus, they are uncorrelated with height and weight. ABSI is linked to spine bone mineral density (BMD), and a higher ABSI may increase the risk of osteoporosis.12,13 Kim et al14 also reported the relationship between ABSI, obesity, and a higher risk of osteoporosis.
No research has systematically explored the associations of ABSI, HI, and WHI with osteoporosis in postmenopausal women. Therefore, our study was conducted using the National Health and Nutrition Examination Survey (NHANES) database to provide a theoretical basis for enhancing the management of osteoporosis in postmenopausal women and identifying specific high-risk populations.
Methods
Study Design and Participants
The NHANES program, conducted by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention, comprises continuous, thorough, cross-sectional, population-based surveys to gather information on the health, nutritional status, and health behaviors of the non-institutionalized civilian resident population of the United States.15 The study protocol was approved by the NCHS Research Ethics Review Board and underwent an annual review, with all participants signing written informed consent.
Information on postmenopausal women was obtained from the database from 2017 to 2020 (Revised to 01/2017–12/2020). WC, HC, and BMD were assessed in 2017–2020 (Revised to 01/2017–12/2020) in NHANES, and we used data from these years. Meanwhile, BMD measurements were only performed for women aged >50 years old in the NHANES, so our study included women aged >50 years old. Women were excluded from those having chronic kidney disease (CKD), missing complete assessment information on WC, HC, and BMD. The requirement of ethical approval for the study was waived by the Institutional Review Board of The First People’s Hospital of Xiaoshan District because the data was assessed from a publicly available database.
ABSI, HI, and WHI Assessment
The allometric counterparts of waist and hip circumference, ABSI9 and HI,10 were calculated using published formulas derived for participants in the NHANES. The calculation of WHI was based on the previous study.16



Osteoporosis
BMD (g/cm2) at the femoral neck or total spine areas was assessed using a DXA scan (Hologic, Bedford, MA, USA), assessing the femoral neck on the left hip, unless there was a history of prior fracture or surgery, in which case the right hip was used. Osteoporosis was defined based on the BMD measurement of the total femur, femoral neck, and lumbar spine from previous studies.17 The mean BMD values of female participants 20–29 years were used as the reference values.18 Individuals with any BMD value <2.5 standard deviations below the reference value were classified as having osteoporosis. To determine osteoporosis history, participants were asked, “Has a doctor ever told you that you had osteoporosis, sometimes called thin or brittle bones?”, if the response was affirmative, the subjects were documented as having osteoporosis.
Covariates
Covariates selected in our study included age, educational level, marital status, poverty income ratio (PIR), cardiovascular disease (CVD), sleep duration, and previous fracture. Educational level was categorized into under high school, high school, and above high school. Marital status included single, married, and unknown. The section on medical conditions, identified by the prefix MCQ in the variable name, covers self- and proxy-reported interview data encompassing a wide range of health conditions and medical history for both children and adults. This section incorporates questions such as
Has a doctor or other health professional ever told you that you had angina, heart failure, heart attack, coronary heart disease, stroke, and congestive heart failure?
These questions were labeled MCQ160B-F in the household questionnaires conducted during home interviews.19 Participants responding “yes” to any of these questions were classified as having a history of CVD. Patients with CVD were also identified as those taking cardiovascular drugs. Sleep duration was classified according to tertiles (<6h, 6–8h, and >8h). Individuals who experienced a broken or fractured hip, wrist, or spine were considered as having a previous fracture.20
Statistical Analysis
All analyses in the study utilized sampling weights to address variations in selection probabilities, non-response, and non-coverage. The masked variance unit pseudo-stratum was SDMVSTRA, and the masked variance unit pseudo-primary sampling unit was SDMVPSU. The confidence interval (CI) was applied to assess the reliability of an estimate. The continuous data were described as means and standard errors (S.E) (Revised to S±E), and the comparison between osteoporosis and no osteoporosis groups was conducted using weighted t-tests. Categorical data were described as the number of cases and constituent ratio (n%), with the comparison between two groups using chi-square tests. Potential confounders were screened using weighted univariate logistic regression models. The relationship between allometric body shape indices and osteoporosis was investigated with weighted univariate and multivariate logistic regression models, with results reported by odds ratios (ORs) and 95% CIs. The relationship was further investigated in different age and BMI populations. Area under the curve (AUC) analysis was conducted to evaluate the predictive performance of WHI. All analyses were conducted using SAS 9.4, with P <0.05 considered statistical significance.
Results
Characteristics of Postmenopausal Women
In total, 810 postmenopausal women aged >50 years were included in the final analysis. Women were excluded from those having CKD (n = 201), as well as missing assessment information on WC, HC, and BMD (N = 235). Figure 1 depicts the screening process for included women. With a mean age of 63.96 (0.44) years, 597 (73.70%) women have osteoporosis. Compared to no osteoporosis group, there were statistical differences between the two groups in age, educational level, marital status, PIR, duration of sedentary activity, CVD, previous fracture, BMI, energy intake, WC, HC, ABSI, HI, and WHI (all P < 0.05). More baseline characteristics of postmenopausal women are presented in Table 1.
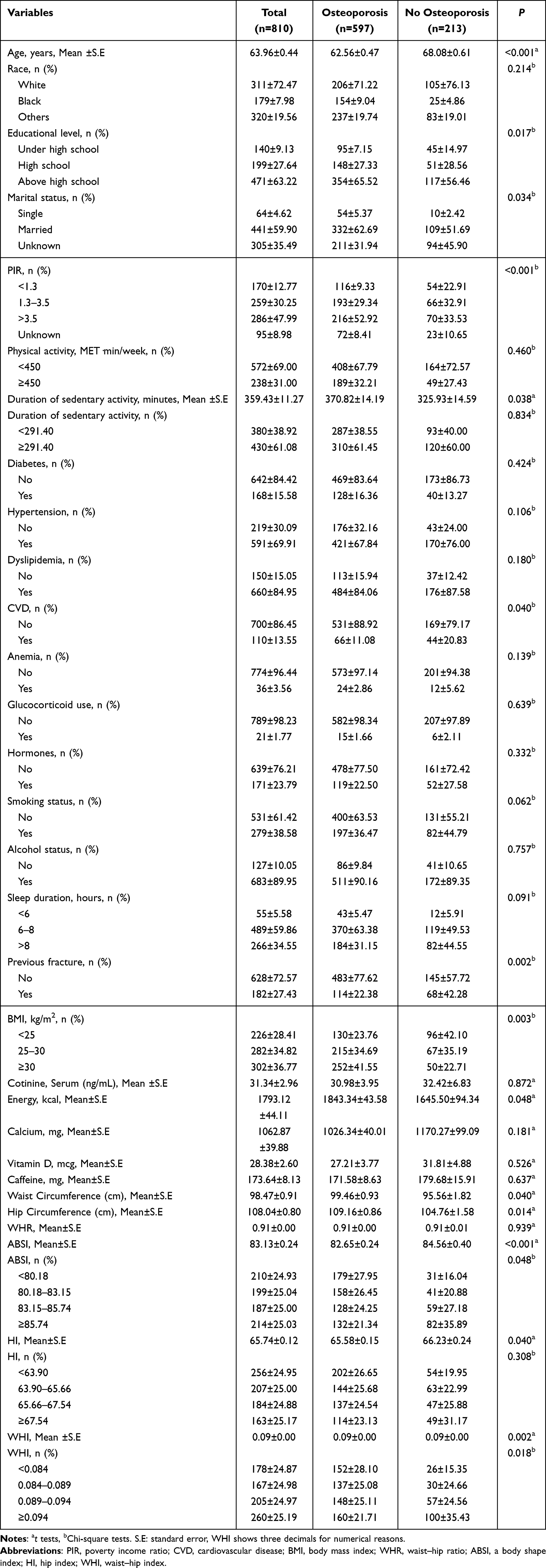 |
Table 1 Characteristics of Postmenopausal Women |
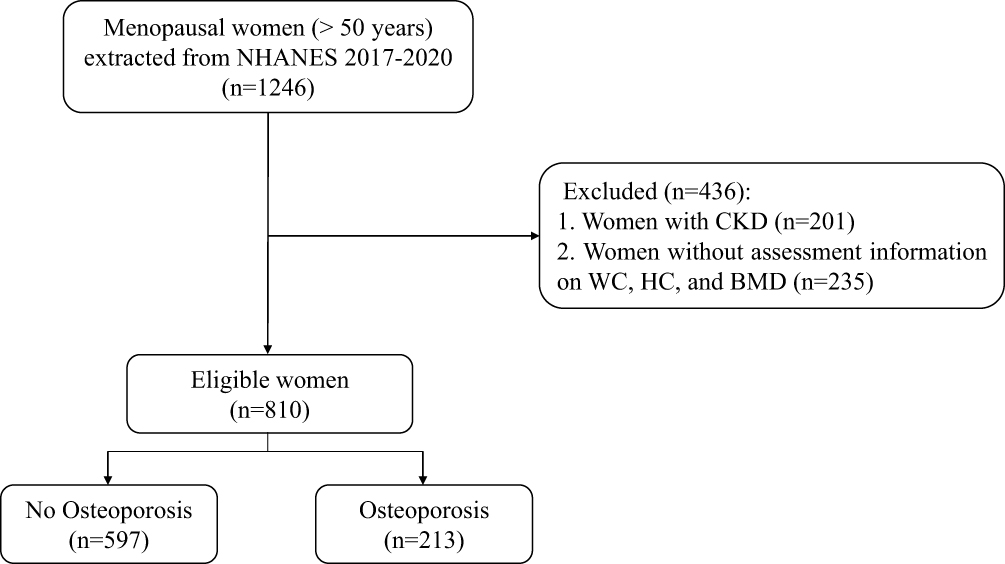 |
Figure 1 Screening process of the study sample. |
Associations of ABSI, HI, WHI, and BMI with Osteoporosis in Postmenopausal Women
Table 2 illustrates the relationships of ABSI, HI, WHI, and BMI with osteoporosis in postmenopausal women. After adjusting age, educational level, marital status, PIR, CVD, sleep duration, and previous fracture, the relationship between WHI ≥0.094 (OR = 2.07, 95% CI: 1.14–3.78) and higher odds of osteoporosis was reported. Higher BMI (≥30 kg/m2) (OR = 0.23, 95% CI: 0.11–0.50) was related to decreased odds of osteoporosis in postmenopausal women. No associations of higher ABSI (OR = 1.99, 95% CI: 0.92–4.33) or HI (OR = 1.66, 95% CI: 0.79–3.49) with osteoporosis were observed in postmenopausal women.
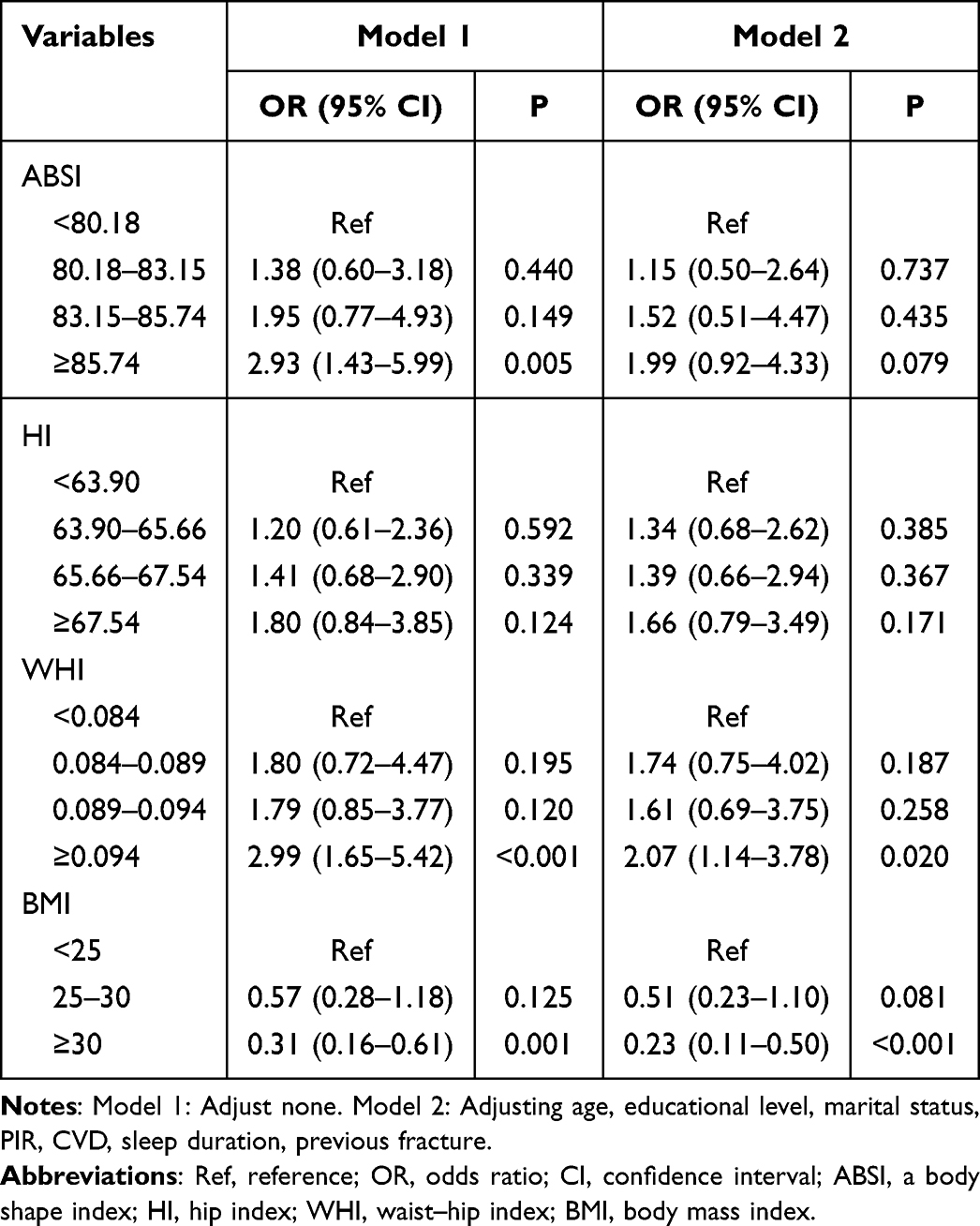 |
Table 2 Associations of ABSI, HI, WHI, BMI with Osteoporosis in Postmenopausal Women |
Associations of ABSI, HI, and WHI with Osteoporosis in Different Age and BMI Population
The association was further explored in different age and BMI populations (Table 3). The covariates were adjusted for age, educational level, marital status, PIR, CVD, sleep duration, and previous fracture. ABSI ≥85.74 (OR = 4.18, 95% CI: 1.22–14.35) was associated with higher odds of osteoporosis in women aged ≥70 years. Similarly, the relationship was also found in women with BMI ≥30 kg/m2 (OR = 4.25, 95% CI: 1.82–9.95). In women aged ≥70 years, HI of 63.90–65.66 (OR = 4.25, 95% CI: 1.82–9.95) was associated with a higher incidence of osteoporosis.
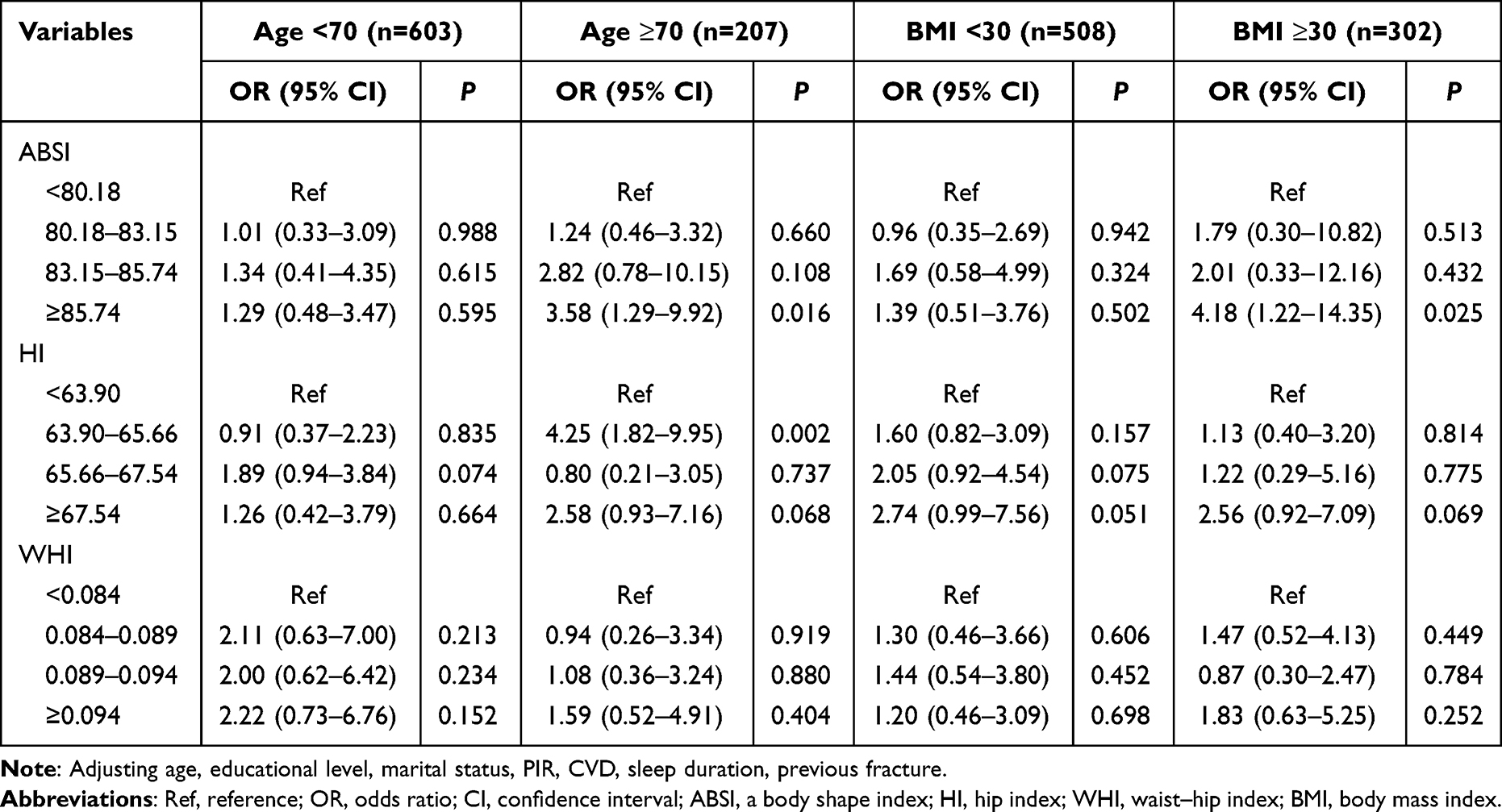 |
Table 3 Associations of ABSI, HI, and WHI with Osteoporosis in Different Age and BMI Subgroups |
The Predictive Value of WHI on Osteoporosis in Postmenopausal Women
The predictive performance of WHI and WHR for osteoporosis were compared using the receiver operating characteristic curves, as summarized in Table 4 and Figure 2. The results indicated that WHI achieved a better predictive performance with AUC of 0.656 (95% CI: 0.613–0.699) between the two anthropometric indicators. DeLong-test shows a significant difference between the two AUCs in predicting osteoporosis in postmenopausal women (P<0.0001).
 |
Table 4 The Predictive Value of WHI on Osteoporosis in Postmenopausal Women |
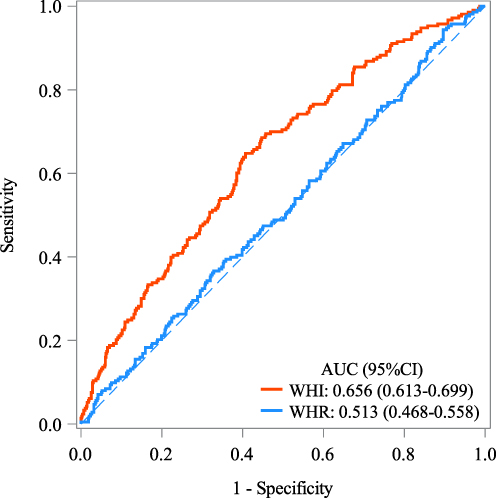 |
Figure 2 The predictive value of WHI on osteoporosis in postmenopausal women. |
Discussion
Our study investigated the associations of allometric body shape indices, including the ABSI, HI, and WHI, with osteoporosis in postmenopausal women. The prevalence of osteoporosis was 73.70% for postmenopausal women in our study. Women with higher WHI were related to a higher incidence of osteoporosis in postmenopausal women. Interestingly, in subgroups of women aged ≥70 years and those with a BMI ≥30 kg/m2, higher ABSI was associated with increased odds of osteoporosis. Additionally, a specific range of HI values (63.90–65.66) was also related to a higher incidence of osteoporosis. The findings contribute to our understanding of the relationship between body shape indices and osteoporosis risk in menopausal women.
Our results regarding the association between WHI and osteoporosis align with previous studies that have reported the link between central obesity and bone health.21,22 WHI has been recognized as a more comprehensive measure of body fat distribution than traditional WHR.16 Central obesity, indicated by a higher WHI, was a risk factor for osteoporosis.6 Meanwhile, Hassan et al reported overweight/obesity may be a protective factor for bone health.23 Differences in participant characteristics, such as age, ethnicity, and lifestyle factors, may contribute to divergent results. Additionally, variations in the definition and measurement of central obesity and osteoporosis across studies may lead to contrasting results. The finding suggests that the distribution of body fat, particularly around the waist and hip, may be influential in the development of osteoporosis in postmenopausal women. WHI may be considered as a valuable predictor of osteoporosis in menopausal women.
The association between higher ABSI and increased odds of osteoporosis was also found in women aged ≥70 years and those with a BMI ≥30 kg/m2. The results indicate that obesity, as measured by ABSI, may play a role in the pathogenesis of osteoporosis in the old and those with obesity.24,25 Increased abdominal fat, particularly visceral fat, has been linked to chronic low-grade inflammation and alterations in adipokine secretion, which may negatively impact BMD and remodeling.26 Furthermore, older age and obesity are known risk factors for hormonal imbalances, such as decreased estrogen levels and insulin resistance, which can contribute to bone loss.27 Additionally, sarcopenia is common in the elderly, and sarcopenia and osteoporosis share common risk factors, including hormonal changes, inflammatory processes, and physical inactivity.28,29 Therefore, sarcopenic may partly mediate the relationship between ABSI and osteoporosis. Our study also showed that an HI value of 63.90–65.66 was associated with a higher incidence of osteoporosis in postmenopausal women. While limited to the small sample size of subgroups, further investigation is warranted to understand the mechanisms through this association.
WHI may serve as a predictor of osteoporosis in postmenopausal women. By recognizing the significance of body shape indices, clinicians can assess individuals at risk more effectively during routine clinical assessment. Incorporating WHI into osteoporosis screening protocols may enhance risk stratification and targeted interventions for individuals at higher risk. Additionally, our findings suggest that older women and those with obesity should be closely monitored for osteoporosis.
For this study, the cross-sectional design restricts our ability to establish causality between allometric body shape indices and osteoporosis in postmenopausal women. Longitudinal and random controlled trials are necessary to validate the association and explore the temporal relationships. Furthermore, we did not account for potential confounding variables which unmeasured in the database, which may impact both body shape indices and osteoporosis risk.
Conclusion
Postmenopausal women with higher WHI were associated with higher odds of osteoporosis. Higher ABSI was related to increased odds of osteoporosis in subgroups of women aged ≥70 years and those with a BMI ≥30 kg/m2. Comparing the predictive value of WHI with traditional WHR, WHI is a superior indicator of osteoporosis risk in menopausal women. Further research is needed to elucidate the underlying mechanisms and validate the clinical utility of these body shape indices in osteoporosis risk assessment.
Data Sharing Statement
All data generated or analyzed during this study are available from the NHANES.
Acknowledgments
We would like to thank the NHANES (National Health and Nutrition Examination Survey) for the offering the related data regarding the paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; Songfeng Zhao took part in drafting, revising or critically reviewing the article; Xin Pan gave final approval of the version to be published; all authors have agreed on the journal to which the article has been submitted and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declared that Songfeng Zhao and Xin Pan have no competing interests.
References
1. de Villiers TJ. Bone health and menopause: osteoporosis prevention and treatment. Best Pract Res Clin Endocrinol Metab. 2024;38(1):101782. doi:10.1016/j.beem.2023.101782
2. Watts NB, Manson JE. Osteoporosis and fracture risk evaluation and management: shared decision making in clinical practice. JAMA. 2017;317(3):253–254. doi:10.1001/jama.2016.19087
3. Gregson CL, Armstrong DJ, Bowden J, et al. UK clinical guideline for the prevention and treatment of osteoporosis. Arch Osteoporos. 2022;17(1):58. doi:10.1007/s11657-022-01061-5
4. Pinto D, Alshahrani M, Chapurlat R, et al. The global approach to rehabilitation following an osteoporotic fragility fracture: a review of the rehabilitation working group of the International Osteoporosis Foundation (IOF) committee of scientific advisors. Osteoporos Int. 2022;33(3):527–540. doi:10.1007/s00198-021-06240-7
5. Lloyd JT, Alley DE, Hawkes WG, Hochberg MC, Waldstein SR, Orwig DL. Body mass index is positively associated with bone mineral density in US older adults. Arch Osteoporos. 2014;9:175. doi:10.1007/s11657-014-0175-2
6. Zheng R, Byberg L, Larsson SC, Höijer J, Baron JA, Michaëlsson K. Prior loss of body mass index, low body mass index, and central obesity independently contribute to higher rates of fractures in elderly women and men. J Bone Miner Res. 2021;36(7):1288–1299. doi:10.1002/jbmr.4298
7. Cao JJ. Effects of obesity on bone metabolism. J Orthop Surg Res. 2011;6:30. doi:10.1186/1749-799X-6-30
8. Nevill AM, Stewart AD, Olds T, Holder R. Relationship between adiposity and body size reveals limitations of BMI. Am J Phys Anthropol. 2006;129(1):151–156. doi:10.1002/ajpa.20262
9. Krakauer NY, Krakauer JC. A new body shape index predicts mortality hazard independently of body mass index. PLoS One. 2012;7(7):e39504. doi:10.1371/journal.pone.0039504
10. Krakauer NY, Krakauer JC. An anthropometric risk index based on combining height, weight, waist, and hip measurements. J Obes. 2016;2016:8094275. doi:10.1155/2016/8094275
11. Christakoudi S, Evangelou E, Riboli E, Tsilidis KK. GWAS of allometric body-shape indices in UK Biobank identifies loci suggesting associations with morphogenesis, organogenesis, adrenal cell renewal and cancer. Sci Rep. 2021;11(1):10688. doi:10.1038/s41598-021-89176-6
12. Xiong MF, He P, Chen YH, Cao RR, Lei SF. The effect of a body shape index (ABSI) and its interaction with low estimated glomerular filtration rate (eGFR) on osteoporosis in elderly Chinese. J Orthop Sci. 2024;29(1):262–267.
13. Deng G, Yin L, Li K, et al. Relationships between anthropometric adiposity indexes and bone mineral density in a cross-sectional Chinese study. Spine J. 2021;21(2):332–342. doi:10.1016/j.spinee.2020.10.019
14. Kim B, Kim GM, Kim E, et al. The anthropometric measure ‘A body shape index’ may predict the risk of osteoporosis in middle-aged and older Korean people. Int J Environ Res Public Health. 2022;19(8):4926.
15. Ahluwalia N, Dwyer J, Terry A, Moshfegh A, Johnson C. Update on NHANES dietary data: focus on collection, release, analytical considerations, and uses to inform public policy. Adv Nutr. 2016;7(1):121–134. doi:10.3945/an.115.009258
16. Kjaergaard AD, Krakauer J, Krakauer N, Teumer A, Winkler TW, Ellervik C. Allometric body shape indices, type 2 diabetes and kidney function: a two-sample Mendelian randomization study. Diabetes Obes Metab. 2023;25(7):1803–1812. doi:10.1111/dom.15037
17. Tang Y, Peng B, Liu J, Liu Z, Xia Y, Geng B. Systemic immune-inflammation index and bone mineral density in postmenopausal women: a cross-sectional study of the national health and nutrition examination survey (NHANES) 2007–2018. Front Immunol. 2022;13:975400. doi:10.3389/fimmu.2022.975400
18. Looker AC, Orwoll ES, Johnston CC, et al. Prevalence of low femoral bone density in older U.S. adults from NHANES III. J Bone Miner Res. 1997;12(11):1761–1768. doi:10.1359/jbmr.1997.12.11.1761
19. Liu C, Liang D. The association between the triglyceride-glucose index and the risk of cardiovascular disease in US population aged ≤ 65 years with prediabetes or diabetes: a population-based study. Cardiovasc Diabetol. 2024;23(1):168. doi:10.1186/s12933-024-02261-8
20. Xu Y, Wu Q. Decreasing trend of bone mineral density in US multiethnic population: analysis of continuous NHANES 2005–2014. Osteoporos Int. 2018;29(11):2437–2446. doi:10.1007/s00198-018-4648-9
21. Lee J, Jung JH, Kim J, et al. Associations between body composition and the risk of fracture according to bone mineral density in postmenopausal women: a population-based database cohort study. Eur J Endocrinol. 2023;189(5):527–536. doi:10.1093/ejendo/lvad156
22. Liu Y, Liu Y, Huang Y, et al. The effect of overweight or obesity on osteoporosis: a systematic review and meta-analysis. Clin Nutr. 2023;42(12):2457–2467. doi:10.1016/j.clnu.2023.10.013
23. Al-Tohamy M, El-Lebedy D, Adel Abdelhalim D, Amin D, Megahed S, Khalil A. Bone health and its relation to energy intake, fat mass and its distribution. Pak J Biol Sci. 2020;23(8):1075–1085. doi:10.3923/pjbs.2020.1075.1085
24. Qin K, He M, Cao XT, et al. [Obesity and osteoporosis in men aged above 50]. Sichuan Da Xue Xue Bao Yi Xue Ban. 2017;48(1):17–22. Danish
25. An K, Qin K, Li SY, et al. [Obesity and bone mineral density in menopausal women]. Sichuan Da Xue Xue Bao Yi Xue Ban. 2017;48(1):23–27. Danish
26. Gkastaris K, Goulis DG, Potoupnis M, Anastasilakis AD, Kapetanos G. Obesity, osteoporosis and bone metabolism. J Musculoskelet Neuronal Interact. 2020;20(3):372–381.
27. Suda M, Paul KH, Tripathi U, Minamino T, Tchkonia T, Kirkland JL. Targeting cell senescence and senolytics: novel interventions for age-related endocrine dysfunction. Endocr Rev. 2024;45:655–675. doi:10.1210/endrev/bnae010
28. Anagnostis P, Dimopoulou C, Karras S, Lambrinoudaki I, Goulis DG. Sarcopenia in post-menopausal women: is there any role for vitamin D? Maturitas. 2015;82(1):56–64. doi:10.1016/j.maturitas.2015.03.014
29. Greco EA, Pietschmann P, Migliaccio S. Osteoporosis and sarcopenia increase frailty syndrome in the elderly. Front Endocrinol. 2019;10:255. doi:10.3389/fendo.2019.00255
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.