Back to Journals » Clinical Ophthalmology » Volume 20
Assessment of Peripheral Anterior Synechiae Using Linear Gonio-Images Following Trabeculotomy with Trabectome
Authors Takagi Y ![]() , Asano R, Yamashita K, Sakai Y, Ichikawa K, Ichikawa K
, Asano R, Yamashita K, Sakai Y, Ichikawa K, Ichikawa K ![]()
Received 31 October 2025
Accepted for publication 6 January 2026
Published 12 January 2026 Volume 2026:20 578215
DOI https://doi.org/10.2147/OPTH.S578215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yuki Takagi,1,2 Ryo Asano,3 Kanna Yamashita,2 Yukihiro Sakai,2 Kei Ichikawa,2 Kazuo Ichikawa2
1Department of Ophthalmology, Japan Community Healthcare Organization Kanitounou Hospital, Kani, Gifu, Japan; 2Chukyo Eye Clinic, Nagoya, Aichi, Japan; 3Asano Eye Clinic, Nagoya, Aichi, Japan
Correspondence: Yuki Takagi, Department of Ophthalmology, Japan Community Healthcare Organization Kanitounou Hospital, Kani, Gifu, Japan, Tel +81-574-25-3113, Fax +81-574-28-6382, Email [email protected]
Purpose: To quantify peripheral anterior synechiae (PAS) extent after Trabectome surgery using automated gonioscopy (GS-1) and its effects on intraocular pressure (IOP) reduction.
Patients and Methods: This retrospective, single-center study included patients who underwent Trabectome surgery and were followed for ≥ 6 months. GS-1 was performed at 6 and 12 months postoperatively to quantify PAS as the proportion of the angle circumference. Analysis of covariance (ANCOVA; linear regression) was performed at 6 and 12 months postoperatively, with IOP reduction rate, PAS extent, and preoperative IOP as the dependent variable, independent variable, and covariate, respectively. The 6- and 12-month PAS extents were compared using the Wilcoxon signed-rank test. The correlations of 6- and 12-month IOP reduction rates with age, preoperative IOP, preoperative score, and PAS extent were determined using Spearman’s rank coefficients.
Results: The data of 33 eyes (33 patients; 20 males; mean age, 68.5 ± 14.2 years) were analyzed. Trabectome surgery was performed as a standalone procedure for 28 patients and combined with cataract surgery for five. GS-1 revealed PAS in all eyes at 6 and 12 months. The mean PAS extents at 6 and 12 months were not significantly different at 40.16 ± 21.42% and 43.92 ± 20.68%, respectively (P = 0.286). Only preoperative IOP showed significant correlations with the 6- and 12-month IOP reduction rates (r = 0.641, 0.776; P = 0.002, < 0.001, respectively). ANCOVA revealed partial regression coefficients of 0.41 (P = 0.002) and 0.019 (P = 0.952) at 6 months and 0.37 (P = 0.014) and − 0.180 (P = 0.623) at 12 months for preoperative IOP and PAS extent, respectively.
Conclusion: Widespread PAS was detected by GS-1 at 6 and 12 months postoperatively. However, its effect on postoperative IOP reduction and prognosis appears limited. Moreover, the long-term effects remain unclear; therefore, further studies are warranted.
Keywords: automated gonioscopy, peripheral anterior synechia, glaucoma
Introduction
Reduction of intraocular pressure (IOP) is the only proven treatment strategy for glaucoma.1 The efficacies of trabeculectomy and trabeculotomy have been established. However, they are relatively invasive and require conjunctival incisions. Minimally invasive glaucoma surgery (MIGS) has advanced in recent years, and studies have reported the efficacy and safety of outflow-reconstructive procedures using the Trabectome (Alcon, formerly NeoMedix, CA, USA)2–6 as well as devices that insert an implant into the trabecular meshwork, such as the iStent series (Glaukos, CA, USA)7–10 and the Hydrus Microstent (Alcon, CA, USA).11,12 Trabectome surgery, an early MIGS procedure, received US FDA clearance in 2004 and approval in Japan in 2010 and has been used for ab interno trabeculotomy; its utility has been documented in several studies.2–6
Peripheral anterior synechiae (PAS) can develop after trabeculotomy performed with the Trabectome or Tanito microhook trabeculotomy (μLOT).13 Conventional gonioscopy can confirm the presence or absence of postoperative PAS. However, using it for longitudinal and quantitative evaluations is challenging. The GS-1 automated gonioscope (hereafter GS-1; NIDEK, Gamagori, Japan) enables the acquisition of 360° gonio-photographs with minimal invasiveness and within a short time.14–16 Therefore, it is useful for the longitudinal assessment of angle structures. The extent of PAS formation after Trabectome surgery and its effect on IOP have not been established, although an association between PAS formation after μLOT and postoperative outcomes has been reported based on GS-1 imaging findings.13 We evaluated PAS after trabeculotomy using the Trabectome based on GS-1 linear-stitched images (Figures 1–3) and investigated its impact on treatment efficacy.
 |
Figure 1 A GS-1 linear-stitched gonioscopic image obtained after Trabectome surgery in an eye with a 360° trabeculotomy. Widespread PAS is observed, extending from the temporal to the nasal region, with the most marked involvement in the inferior region. |
 |
Figure 2 A GS-1 linear-stitched gonioscopic image obtained after Trabectome surgery in another eye with a 360° trabeculotomy. In contrast to Figure 1, PAS is only mildly present in the superior and inferior regions. |
 |
Figure 3 A GS-1 linear-stitched gonioscopic image obtained after Trabectome surgery in an eye with a 240° trabeculotomy. PAS formation is also observed in the superior quadrant, which was not included in the surgical incision. |
Materials and Methods
Participants
We enrolled the eyes of patients treated at JCHO Chukyo Hospital and Chukyo Eye Clinic between July 2020 and July 2022. The included eyes underwent Trabectome surgery via a 240–360° incision performed by a single surgeon, had interpretable GS-1 gonio-photographs available, and were followed for ≥ 6 months. For patients in whom both eyes met the inclusion criteria, only one eye per patient was included to avoid intereye correlation, and the eye with the higher preoperative IOP was selected to better evaluate the IOP-lowering effect of the surgery.
The IOP and antiglaucoma medication scores were evaluated preoperatively and at 1, 3, 6, 9, and 12 months postoperatively (±1 month). The medication score was defined as 1 point per topical antiglaucoma medication (2 points for a fixed-combination preparation). The number of oral acetazolamide tablets taken per day was added to the score. The GS-1 imaging data acquired at 6 and 12 months postoperatively (±1 month) were retrospectively extracted for analysis. The IOP was measured using Goldmann applanation tonometry.
This study was based on a retrospective analysis of the examination data extracted from the electronic medical records. The study protocol was approved by the Institutional Review Board of Chukyo Eye Clinic (approval number: 20240620081). Informed consent was obtained via the opt-out method, and the study was conducted in accordance with the Declaration of Helsinki.
Surgery
The eyes treated with 360° trabeculotomy had 7–0 silk traction sutures placed on the lateral and medial rectus muscles. Three 1.7-mm corneal incisions (superotemporal, superonasal, and inferior) were created. The Trabectome handpiece was introduced through each incision, and the trabecular meshwork opposite the corneal entry site at approximately 120° was ablated. The globe was rotated by pulling the traction sutures to position the intended corneal entry site temporally for the inferior approach. The intraoperative bleeding was cleared using Trabectome irrigation after completion of the trabecular incision at each site. The handpiece was withdrawn, and the corneal wounds were sutured using 10–0 Vicryl. Finally, intraoperative IOP was measured using a Barraquer applanation tonometer (Ocular Instruments, Bellevue, WA, USA), and the procedure was completed after adjusting the IOP to ≥ 21 mmHg.
The eyes treated with 240° trabeculotomy did not have traction sutures placed. Two 1.7-mm corneal incisions (superotemporal and superonasal) were created. Trabecular meshwork ablation was performed over 120° at each incision site.
The postoperative topical regimen included levofloxacin hydrate, bromfenac sodium hydrate, and pilocarpine hydrochloride (2%). Fluorometholone (0.02%) was administered after Trabectome surgery alone, whereas betamethasone sodium phosphate was administered after combination with cataract surgery. All eye drops were continued for approximately 1 month.
Automated Gonioscopy
The orthoptist acquired the images under bright illumination after topical anesthesia (oxybuprocaine hydrochloride). The GS-1 outputs (16 directional views) were reconstructed into linear-stitched angle images. The extent of PAS was determined from the reconstructed images using ImageJ and expressed as the ratio of the cumulative PAS length to the total length of the stitched image (percentage of angle circumference). PAS was defined as iris adhesion extending beyond the scleral spur to the posterior trabecular meshwork. The measurements for some cases were repeated on a different day to assess reproducibility. All ImageJ measurements were performed by the same examiner.
Statistical Analysis
Analysis of covariance (ANCOVA) was performed for the primary outcome. The IOP reduction rate at 12 months was the dependent variable, the 12-month PAS extent was the independent variable, and the preoperative IOP was the covariate. The same ANCOVA was performed for the 6-month outcome using the 6-month IOP reduction rate (dependent variable), the 6-month PAS extent (independent variable), and preoperative IOP (covariate).
The secondary outcomes of preoperative and postoperative IOPs and medication scores were compared using the Wilcoxon signed-rank test. The PAS extents for the eyes with available GS-1 images were also compared at 6 and 12 months using the Wilcoxon signed-rank test.
Spearman’s rank correlation coefficients were used to determine the relationships between the 6- and 12-month IOP reduction rates and preoperative IOP, medication score, age, and PAS extent. The 6- and 12-month PAS extents were stratified by incision range (360° vs 240°) and compared using the Mann–Whitney U-test.
The intraclass correlation coefficient (ICC) was used to assess the reproducibility of the PAS measurements obtained from GS-1 images based on the results of the two measurements.
Cases with missing data were excluded from each analysis (complete-case analysis). Only eyes with all relevant variables available at each time point were included. Statistical analyses were performed using SPSS (version 29.0; IBM Corp., Armonk, NY, USA). Statistical significance was set at P < 0.05.
Results
Thirty-three eyes of 33 patients were included. The participants included 20 males (20 eyes) and 13 females (13 eyes). Their mean age was 68.5 ± 14.2 years. Fifteen and 18 eyes were phakic and pseudophakic, respectively. Nineteen had primary open-angle glaucoma, seven had exfoliation glaucoma, and seven had secondary glaucoma. Trabectome surgery was performed as a standalone procedure for 28 eyes and combined with cataract surgery for 5 (Table 1). The trabecular meshwork was incised over 360° and 240° in 18 and 15 eyes, respectively.
 |
Table 1 Clinical Characteristics of the Patients in This Study |
The mean IOPs obtained preoperatively and at 1, 3, 6, 9, and 12 months postoperatively (±1 month) were 19.55 ± 5.57, 14.09 ± 3.85, 15.33 ± 4.03, 14.91 ± 3.99, 15.24 ± 3.32, and 14.10 ± 4.95 mmHg, respectively (Table 2). The corresponding medication scores were 4.76 ± 1.46, 2.55 ± 2.05, 2.21 ± 1.87, 2.30 ± 1.75, 2.56 ± 1.76, and 2.45 ± 1.74. The IOPs and medication scores were significantly lower postoperatively than preoperatively (P < 0.05). The mean IOP reduction rates at 1, 3, 6, 9, and 12 months postoperatively were 22.33 ± 30.82, 16.27 ± 30.18, 16.87 ± 36.76, 16.17 ± 26.29, and 18.79 ± 34.04%, respectively.
 |
Table 2 Changes in Intraocular Pressure and Medication Score |
PAS was detected in all eyes on the GS-1 images obtained at 6 and 12 months. The mean extents of PAS at 6 and 12 months were 40.16 ± 21.42% and 43.92 ± 20.68%, respectively, and the difference was not significant (P = 0.286). This analysis included 12 eyes for which GS-1 images were available at 6 and 12 months. The mean extents of PAS for the 360° and 240° groups were 40.67 ± 21.94% and 39.09 ± 21.73% at 6 months, respectively, with no significant difference (P = 0.176). The corresponding values for the two groups were 45.40 ± 17.05% and 42.59 ± 24.35%, with no significant difference (P = 0.842).
PAS was present in the inferior quadrant in all eyes, the temporal and nasal quadrants in 30 eyes, and the superior quadrant in 19 eyes. Five of the 15 eyes that had a 240° incision (no superior trabeculotomy) had PAS in the superior quadrant.
Only the preoperative IOP was significantly correlated with the 12-month IOP reduction rate (ρ = 0.641, P = 0.002; Table 3). The extent of PAS was not significantly correlated with the 12-month IOP reduction rate (P = 0.593). The preoperative IOP was also significantly correlated with the 6-month IOP reduction rate (ρ = 0.776, P < 0.001; Table 4). However, the PAS extent was not significantly correlated with the 6-month IOP reduction rate (P = 0.200). The relationships between the IOP reduction and the extent of PAS at 6 and 12 months are shown in Figure 4A and B, respectively.
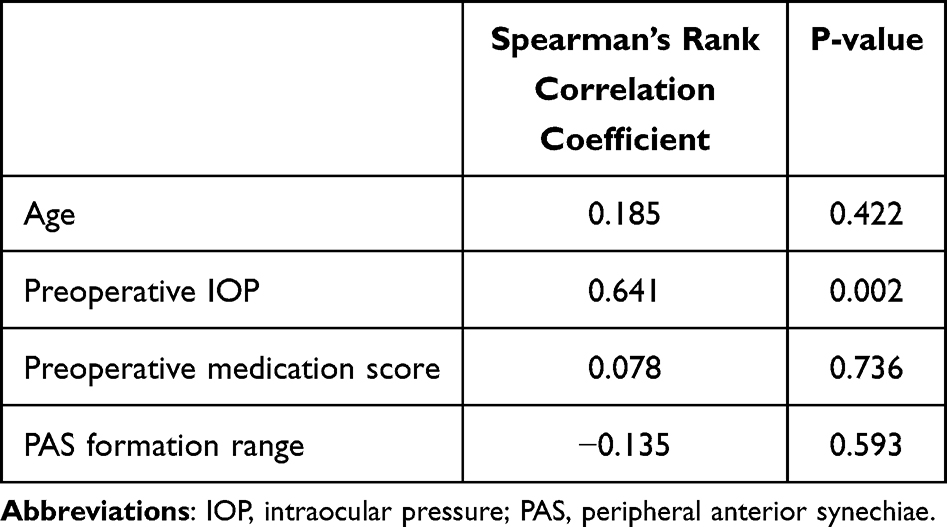 |
Table 3 Correlation with Intraocular Pressure Reduction Rate at 12 Months Postoperatively |
 |
Table 4 Correlation with Intraocular Pressure Reduction Rate at 6 Months Postoperatively |
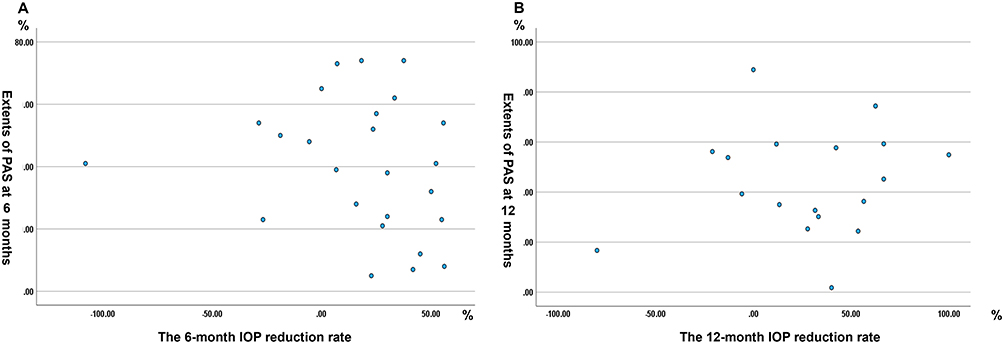 |
Figure 4 Scatter plot showing the relationship between the extent of PAS and IOP reduction rate at 6 (A) and 12 months (B). No significant correlations were found in either relationship ((A) r = –0.135, P = 0.593; (B) r = −0.265, P = 0.20). |
The preoperative IOP was significantly associated with the 6-month outcome (B = 0.41, P = 0.002), but the PAS extent was not (B = 0.019, P = 0.952). The regression coefficients (B) for the preoperative IOP and PAS extent at 12 months were 0.37 (P = 0.014) and −0.180 (P = 0.623), respectively. The reproducibility was evaluated using GS-1 images of 17 eyes. The ICC was 0.923 (95% confidence interval, 0.805–0.971; P < 0.001).
Discussion
We quantitatively evaluated PAS formation after ab interno trabeculotomy (240–360°) using GS-1 linear-stitched images and examined its impact on postoperative outcomes. PAS developed in all eyes, and its mean extent was approximately 40%. However, it did not significantly affect the IOP reduction rates at 6 and 12 months postoperatively. The reported prevalence of postoperative PAS after μLOT ranges from 56 to 86%.4,13 The prevalence of PAS in the present study was higher than that reported previously. This discrepancy may be attributable to the differences in the incision extent (120–240° for the previous μLOT studies vs 240–360° for our Trabectome series) and the device used. These factors may influence PAS formation. However, preoperative GS-1 imaging was not performed in this study; therefore, the preoperative baseline status of the angle was unknown, and the PAS observed postoperatively cannot be definitively attributed to the surgical procedure. Future prospective studies evaluating the preoperative angle status are required to clarify this issue.
A previous study using GS-1 to evaluate the extent of PAS after μLOT reported PAS in 4.1 of the 16 GS-1 sectors, corresponding to 25.63% of the angle.13 This is less than the extent of PAS observed in our subgroup that had 240° incisions. Trabectome may induce greater collateral tissue effects and inflammation owing to ablation of the trabecular meshwork via electrocautery, which may increase the risk of extensive PAS. The extent of PAS was slightly greater at 12 months than at 6 months, but the difference was not significant. This trend may be attributable to the small number of eyes with measurements at both time points (n = 12). This limited sample size substantially reduces the statistical power of the analysis and raises the possibility of a type II error, potentially obscuring a true difference in PAS extent between 6 and 12 months (P = 0.286). Furthermore, the analysis was limited by the inclusion of only two postoperative assessment points (6 and 12 months). Future studies with larger sample sizes and more frequent follow-up are warranted to better characterize longitudinal changes in PAS. No significant difference in the extent of PAS was detected between the 240° and 360° incision groups. This may reflect PAS formation outside the incised sectors. Superior quadrant PAS (in a non-incised region) was observed in 5 (33%) of the 15 eyes with a 240° incision. PAS formation in non-incised areas has also been reported.13 However, the findings cannot be attributed solely to the incision extent because the concomitant procedures (standalone vs combined surgery) and lens status were not uniform in our cohort. Further studies with standardized surgical conditions are warranted.
Only the preoperative IOP was significantly correlated with the IOP reduction rate at 6 and 12 months. This finding is consistent with those of previous studies that reported greater percentage reductions in IOP in patients with higher baseline IOP.6 Previous reports have documented increased IOP when the extent of PAS exceeds 50%.17,18 Several eyes in the present study had a PAS extent of ≥ 50%. However, the extent and distribution of PAS were not significantly associated with the IOP reduction rate. The previous studies involved phakic eyes without surgery, whereas our cohort comprised eyes that had undergone outflow reconstruction. The aqueous outflow from the non-PAS sectors may have been better than that from the nonsurgical eyes, potentially preventing IOP elevation. However, extensive PAS may still adversely affect postoperative outcomes following trabeculotomy. Further investigations involving larger samples and longer follow-up are warranted.
This study had some limitations. Previous reports have evaluated μLOT, but we used the Trabectome. Device-related differences may influence the degree of PAS formation, highlighting the need for direct inter-device comparisons. In patients for whom both eyes met the inclusion criteria, the eye with the higher preoperative IOP was selected for analysis to avoid intereye correlation. However, this selection strategy may have introduced a bias toward eyes with higher baseline IOP. Because the magnitude of postoperative IOP reduction is partly dependent on baseline IOP, this approach may have influenced the observed treatment effect. Therefore, this limitation should be considered when interpreting the postoperative IOP outcomes. The sample was small, and the duration of observation was short. Larger studies with longer follow-up are warranted. Although intraobserver agreement for PAS grading based on GS-1 images was good, interobserver agreement was not assessed, representing an important methodological limitation that may affect the generalizability and reproducibility of the ImageJ-based PAS measurements. Adverse events such as postoperative hyphema and transient IOP spikes were not analyzed. Future studies should re-examine the safety outcomes. Furthermore, this study included eyes undergoing standalone Trabectome surgery as well as combined Trabectome and cataract surgery. The degree of postoperative inflammation may differ between standalone and combined procedures and could influence PAS formation. However, because of the limited sample size, we did not perform a subgroup analysis comparing standalone and combined surgeries. Further studies with larger sample sizes are warranted to enable such comparisons. Despite several limitations, this study is novel in its quantitative assessment of PAS formation following Trabectome surgery. It also indicates that a wider incision range may result in a more extensive development of PAS and supports previous findings that PAS can occur even in non-incised areas.
Conclusion
Widespread PAS was detected by GS-1 at 6 and 12 months postoperatively. However, its impact on postoperative IOP reduction and overall prognosis appears to be limited. The long-term effects remain unclear; therefore, further studies are needed to determine whether trabeculotomy using the Trabectome is effective.
Abbreviations
ICC, Intraclass correlation coefficient; IOP, Its effects on intraocular pressure; MIGS, Minimally invasive glaucoma surgery; PAS, Peripheral anterior synechiae; μLOT, microhook trabeculotomy.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol was approved by the Institutional Review Board of Chukyo Eye Clinic (approval number: 20240620081). Informed consent was obtained via the opt-out method, and the study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made significant contributions to the work reported, including its conception, study design, execution, data acquisition, analysis, and interpretation. They also participated in drafting, revising, or critically reviewing the article, approved the final version for publication, agreed on the journal to which the article was submitted, and agreed to be accountable for all its aspects.
Funding
This research received no specific grants from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Kazuo Ichikawa reports grants, personal fees, from STAAR Surgical, non-financial support from Rxsight, personal fees, non-financial support from Alcon, personal fees from Kowa Company, Ltd., personal fees from WAKAMOTO PHARMACEUTICAL CO., LTD., personal fees from Lumenis Japan Co. Ltd., outside the submitted work. The author(s) report no conflicts of interest in this work.
References
1. Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311(18):1901–8. doi:10.1001/jama.2014.3192
2. Maeda M, Watanabe M, Ichikawa K. Evaluation of Trabectome in open-angle glaucoma. J Glaucoma. 2013;22(3):205–208. doi:10.1097/IJG.0b013e3182311b92
3. Kitamura K, Fukuda Y, Hasebe Y, Matsubara M, Kashiwagi K. Mid-term results of ab interno trabeculectomy among Japanese glaucoma patients. J Clin Med. 2023;12(6):2332. doi:10.3390/jcm12062332
4. Kono Y, Kasahara M, Hirasawa K, et al. Long-term clinical results of Trabectome surgery in patients with open-angle glaucoma. Graefes Arch Clin Exp Ophthalmol. 2020;258(11):2467–2476. doi:10.1007/s00417-020-04897-0
5. Weber C, Ludwig E, Hundertmark S, et al. Five-year clinical outcomes of inferior quadrant trabectome surgery for open angle glaucoma. J Glaucoma. 2023;32(6):480–488. doi:10.1097/IJG.0000000000002164
6. Tojo N, Hayashi A. The outcomes of Trabectome surgery in patients with low, middle, and high preoperative intraocular pressure. Clin Ophthalmol. 2020;14:4099–4108. doi:10.2147/OPTH.S285883
7. Bahler CK, Smedley GT, Zhou J, Johnson DH. Trabecular bypass stents decrease intraocular pressure in cultured human anterior segments. Am J Ophthalmol. 2004;138(6):988–994. doi:10.1016/j.ajo.2004.07.035
8. Bahler CK, Hann CR, Fjield T, Haffner D, Heitzmann H, Fautsch MP. Second-generation trabecular meshwork bypass stent (iStent inject) increases outflow facility in cultured human anterior segments. Am J Ophthalmol. 2012;153(6):1206–1213. doi:10.1016/j.ajo.2011.12.017
9. Nitta K, Yamada Y, Morokado S, Sugiyama K. iStent trabecular micro-bypass stent implantation with cataract surgery in a Japanese glaucoma population. Clin Ophthalmol. 2020;14:3381–3391. doi:10.2147/OPTH.S274281
10. Samuelson TW, Sarkisian SR, Lubeck DM, et al. Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results. Ophthalmology. 2019;126(6):811–821. doi:10.1016/j.ophtha.2019.03.006
11. Samuelson TW, Chang DF, Marquis R, et al. A Schlemm canal microstent for intraocular pressure reduction in primary open-angle glaucoma and cataract: the HORIZON study. Ophthalmology. 2019;126(1):29–37. doi:10.1016/j.ophtha.2018.05.012
12. Zebardast N, Zheng C, Jampel HD. Effect of a Schlemm’s canal microstent on early postoperative intraocular pressure after cataract surgery: an analysis of the HORIZON randomized controlled trial. Ophthalmology. 2020;127(10):1303–1310. doi:10.1016/j.ophtha.2020.01.025
13. Matsuo M, Inomata Y, Kozuki N, Tanito M. Characterization of peripheral anterior synechiae formation after microhook Ab-interno trabeculotomy using a 360-degree gonio-camera. Clin Ophthalmol. 2021;15:1629–1638. doi:10.2147/OPTH.S306834
14. Teixeira F, Sousa DC, Leal I, Barata A, Neves CM, Pinto LA. Automated gonioscopy photography for iridocorneal angle. Eur J Ophthalmol. 2020;30(1):112–118. doi:10.1177/1120672118806436
15. Shi Y, Yang X, Marion KM, Francis BA, Sadda SR, Chopra V. Novel and semiautomated 360-degree gonioscopic anterior chamber angle imaging in under 60 seconds. Ophthalmol Glaucoma. 2019;2(4):215–223. doi:10.1016/j.ogla.2019.04.002
16. Takagi Y, Watanabe M, Kojima T, Sakai Y, Asano R, Ichikawa K. Comparison of the efficacy and invasiveness of manual and automated gonioscopy. PLoS One. 2023;18(4):e0284098. doi:10.1371/journal.pone.0284098
17. Zhang M, Mao GY, Ye C, Fan SJ, Liang YB, Wang NL. Association of peripheral anterior synechia, intraocular pressure, and glaucomatous optic neuropathy in primary angle-closure diseases. Int J Opthalmol. 2021;14(10):1533–1538. doi:10.18240/ijo.2021.10.09
18. Foster PJ, Machin D, Wong TY, et al. Determinants of intraocular pressure and its association with glaucomatous optic neuropathy in Chinese Singaporeans: the Tanjong Pagar study. Invest Ophthalmol Vis Sci. 2003;44(9):3885–3891. doi:10.1167/iovs.03-0012
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.