Back to Journals » Patient Preference and Adherence » Volume 12
Assessment of patients’ warfarin knowledge and anticoagulation control at a joint physician- and pharmacist-managed clinic in China
Authors Li X ![]() , Sun S, Wang Q, Chen B, Zhao Z, Xu X
, Sun S, Wang Q, Chen B, Zhao Z, Xu X
Received 10 November 2017
Accepted for publication 1 March 2018
Published 9 May 2018 Volume 2018:12 Pages 783—791
DOI https://doi.org/10.2147/PPA.S156734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Xingang Li,1,2 Shusen Sun,3 Qiaoyu Wang,1 Buxing Chen,4 Zhigang Zhao,1,2 Xiaowei Xu4
1Department of Pharmacy, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Precision Medicine Research Center for Neurological Disorders, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 3College of Pharmacy and Health Sciences, Western New England University, Springfield, MA, USA; 4Department of Cardiology, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China
Purpose: Warfarin is a widely used anticoagulant with a narrow therapeutic index, and it requires close monitoring and adequate patient education. We aimed to assess the knowledge level regarding warfarin therapy among its users and to identify the factors that significantly influence anticoagulation control.
Patients and methods: Patients attending the Warfarin Clinic at the Beijing Tiantan Hospital were enrolled in this study. Patients’ knowledge on warfarin was assessed using a validated Anticoagulation Knowledge Assessment (AKA) questionnaire. Patients’ responses to each question were analyzed to identify areas of improvement in current warfarin education. International normalized ratio (INR) control was defined by the time in therapeutic range (TTR) calculated using the Rosendaal method. Spearman correlation analysis was used to investigate the association between TTR and the independent variables.
Results: A total of 65 patients were enrolled in this study. Eleven questions were answered correctly by <50% of the patients. A total of 858 INR results were recorded; 432 INR values (50.3%) reached the predefined goals, and the mean TTR was 49.8%±24.8%. There were significant associations between TTR and patients’ AKA scores (R=0.356, P=0.004) and between TTR and patients’ educational levels (R=0.339, P=0.006). No significant association was observed between other factors (age and duration of anticoagulation) and TTR. The INR outcome measure was positively associated with patients’ knowledge on warfarin and their educational levels.
Conclusion: Areas for improvement in patient education have been identified, and processes for educational modification are currently in development.
Keywords: International normalized ratio, educational level, People’s Republic of China
Plain language summary
We aimed to identify the factors that significantly influence anticoagulation control. Patients’ knowledge on warfarin was assessed using a validated Anticoagulation Knowledge Assessment (AKA) questionnaire, and analysis of the AKA responses was used to identify the areas for improvement in patient education. We found that the INR outcome measure “time in therapeutic range” is positively associated with patients’ warfarin knowledge and educational levels among the patients of our clinic, and pharmacists should spend more time to educate patients with low levels of education and warfarin knowledge.
Introduction
Warfarin remains widely used by patients with cardiovascular and/or cerebrovascular diseases in mainland China.1,2 Due to high interindividual variability, the anticoagulant activity of warfarin has to be monitored using the international normalized ratio (INR) to ensure that an adequate yet safe dose is taken.3–5 The therapeutic and adverse effects of warfarin depend largely on the percentage of time during which the INR is within the therapeutic range.6 Anticoagulation clinics can help patients to manage their warfarin therapy and to achieve better clinical outcomes.7
To effectively manage patients on warfarin therapy, an anticoagulation clinic jointly managed by a physician and a pharmacist has been established at the Beijing Tiantan Hospital since May 2013. The role of the pharmacist is to provide patients with individualized anticoagulant education, management, and follow-up to ensure that their INR values are within the therapeutic goals. However, in our practice, we found that some patients’ INR values were always suboptimal, with large variations. It has been shown that patients’ knowledge of warfarin can improve anticoagulation control, with a decrease in adverse drug reaction and other associated complications.8 To date, there have been no studies that have either assessed the knowledge level among warfarin users in mainland China or examined the relationship between patients’ warfarin knowledge and anticoagulant control. There is an urgent need to identify the factors related to patients’ INR variations through assessment of patients’ warfarin knowledge.
Aims of the study
The aims of this study were 1) to assess the knowledge level of patients receiving warfarin therapy in an anticoagulant clinic by using the validated Anticoagulation Knowledge Assessment (AKA) questionnaire and 2) to examine the relationship between patients’ warfarin knowledge and anticoagulant control as measured by the INR.
Methods
Study setting
Beijing Tiantan Hospital is a 1,150-bed tertiary-care, teaching institution. The anticoagulation clinic accepts all patients requiring warfarin therapy discharged from the hospital. Prior to the initiation of warfarin therapy, each patient is educated by the clinic’s pharmacist about warfarin therapy, the session generally lasting about 30 minutes on average. The content of the verbal education includes the following: 1) warfarin therapy (treatment rationale, benefits, and length); 2) medication administration (dosing, when to take a dose, how to store the medication, and what to do in case of a missed dose); 3) drug–drug or drug–food interactions; 4) activity or procedure precautions (fall, contact sports, shaving or brushing, surgery, or dental procedures); 5) dietary considerations and consistency; 6) side effects (signs of overanticoagulation or disease recurrence, and what to do in case of bleeding); 7) when to contact clinicians; and 8) laboratory monitoring (INR and frequency). Written education materials are also provided to each patient, including a list of warfarin-interacting medications or foods. For illiterate patients, drawings are used to highlight the main teaching points during verbal education. Patients are asked to read the written information carefully at home and contact the clinic’s pharmacist if they have any questions following the reading of the written material. This study was approved by the institution review board of Beijing Tiantan Hospital, Capital Medical University, Beijing, PRC. Written informed consent was obtained from patients after the nature and purpose of the study were explained.
Study population and the questionnaire
The study population was composed of patients undergoing warfarin therapy who visited the clinic from September 2015 to June 2017. Inclusion criteria were as follows: 1) patient had received a verbal anticoagulation education and received written educational material before participating in the study; 2) patient had taken warfarin continuously for >3 months to ensure that warfarin had reached the steady state; and 3) patients were able to visit the clinic for each of the 1-month follow-ups and had at least five INR measurements during the 1-year study period.
The AKA questionnaire was selected to assess patients’ warfarin knowledge.8–10 The AKA questionnaire comprises 29 multiple-choice questions related to different aspects of warfarin therapy. The English questionnaire was translated into a Chinese version according to the standard translation procedures.11 The following information was obtained from patients’ medical records: gender, age, educational level, duration of therapy, and diagnosis. Patients who met the inclusion criteria were invited to the study, and those who consented to the study self-completed the questionnaire at the clinic.
INR monitoring
Patients were required to visit the clinic at regular intervals (every month), and their INR values were measured during each visit. INR testing was performed using a Roche CoaguChek XS handheld coagulation analyzer or ACL9000 coagulation analyzer (Instrumentation Laboratory).12 The two methods were prevalidated to ensure that the INR results were comparable. The target range of INR was 2.5–3.5 for heart valve replacement and 2.0–3.0 for other indications, according to the hospital anticoagulation protocol. INR control, the secondary study outcome, was defined by both the number of INR values within the therapeutic range as well as the time in therapeutic range (TTR), calculated using the Rosendaal method.13 This method adds each patient’s TTR and divides it by the total times of observations. In addition to recording the results in terms of each INR value, patients’ adverse reactions to warfarin were also recorded.
Data extraction and statistical analysis
The level of anticoagulation knowledge was determined based on the total score on the AKA questionnaire and the number of questions answered correctly. Each question was graded and was given one point for a correct answer or zero for a wrong answer. To avoid grading errors, each questionnaire was graded by two study investigators. Patients who answered at least 21 questions correctly (72.4% correct) were considered to have obtained a passing score, as suggested in a previous study using the AKA questionnaire.10
Statistical analyses were conducted using SPSS (version 19.0; IBM Corporation, Armonk, NY, USA). Continuous variables were expressed as mean ± SD, and categorical data were presented as numbers and percentages. Spearman correlation analysis was used to investigate the association between TTR and the independent variables (gender, age, duration of warfarin therapy, education level, and AKA questionnaire score). Significance was defined as P-value <0.05.
Results
Baseline characteristics
Totally, 125 patients met the inclusion criteria and were invited for the study; 71 patients consented, and 70 completed the questionnaire (98.6% completion rate). A total of 65 valid questionnaires were included for the final analysis (four patients failed to come to the clinic for follow-ups, and one patient had less-than-five INR measurements). The demographic and clinical data of the patients are presented in Table 1.
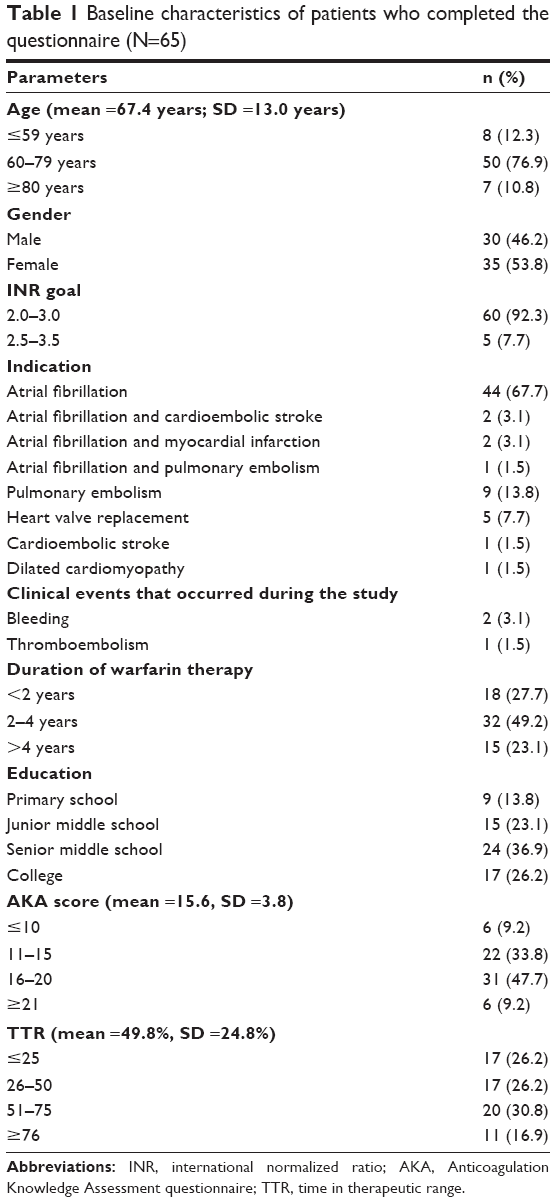 | Table 1 Baseline characteristics of patients who completed the questionnaire (N=65) |
The mean age of the patients was 67.4±13.0 years, and the sample included 35 female patients (53.8%). Nine patients (13.8%) had only completed primary school education, a total of 6 years’ schooling. The majority of patients were being treated for atrial fibrillation (n=44, 67.7%). Other indications included pulmonary embolism (n=9, 13.8%) and valve replacement (n=5, 7.7%). Indication categories are not mutually exclusive, and patients with multiple indications were included in all applicable categories. Most patients had been treated for at least 1 year, except that two patients (3.1%) were treated for <1 year. For the assessment of individual INR goal values preset by the clinic, 60 patients (92.3%) had a goal range of 2–3, and five patients (7.7%) with heart valve replacement had a goal range of 2.5–3.5. A total of 858 INR values were recorded, 432 INR values (50.3%) reached the predefined goals, and the mean TTR was 49.8%±24.8%. Among the 65 patients, two patients had minor bleeding and one patient experienced a thromboembolic event during the study period.
Analysis of answers to the questionnaire
Of the 65 patients, only 9.2% (n=6) achieved a passing score or were able to answer at least 21 questions correctly on the 29-item AKA questionnaire, and none of the patients were able to score 100%. The mean AKA questionnaire score was 15.6±3.8, with the being range 5–23 points. Patients scored the highest on Question 8 (what to do when patient runs out of warfarin) and Question 14 (the best time to take warfarin), with scores of 96.9% and 89.2%, respectively. Out of the 29 questions, 11 questions were answered correctly by <50% of the patients (Table 2).
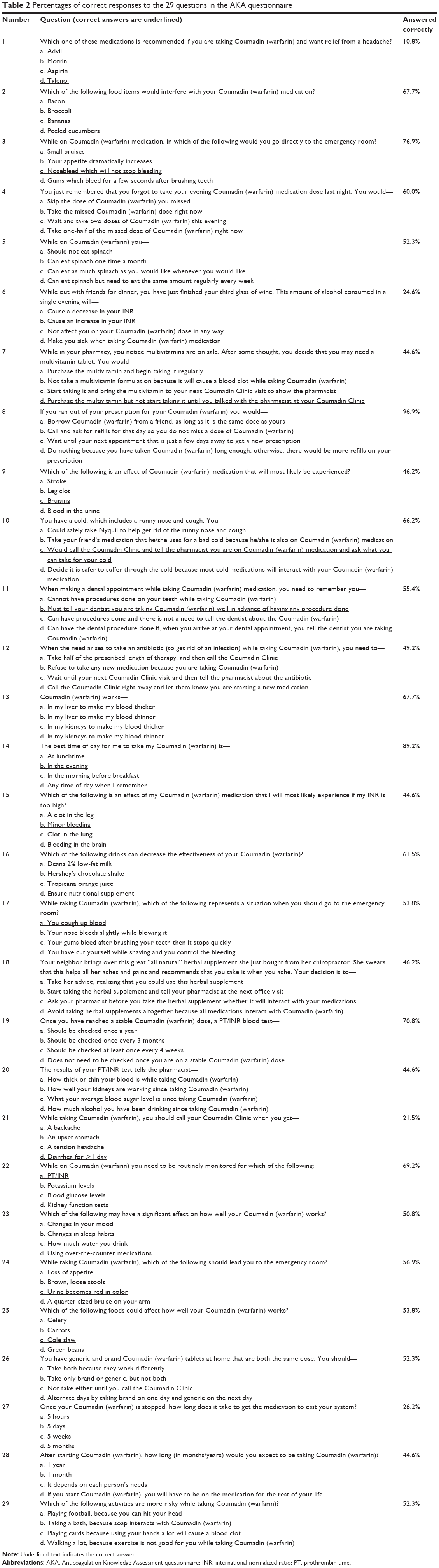 | Table 2 Percentages of correct responses to the 29 questions in the AKA questionnaire |
Association analysis
No significant association was found between age or the duration of warfarin therapy on the one hand and the TTR on the other (Table 3). As shown in Table 3 and Figure 1, there were significant associations between TTR and patients’ AKA scores (R=0.356, P=0.004) as well as between TTR and patients’ educational levels (R=0.339, P=0.006).
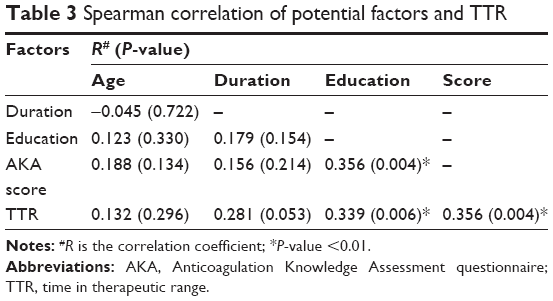 | Table 3 Spearman correlation of potential factors and TTR |
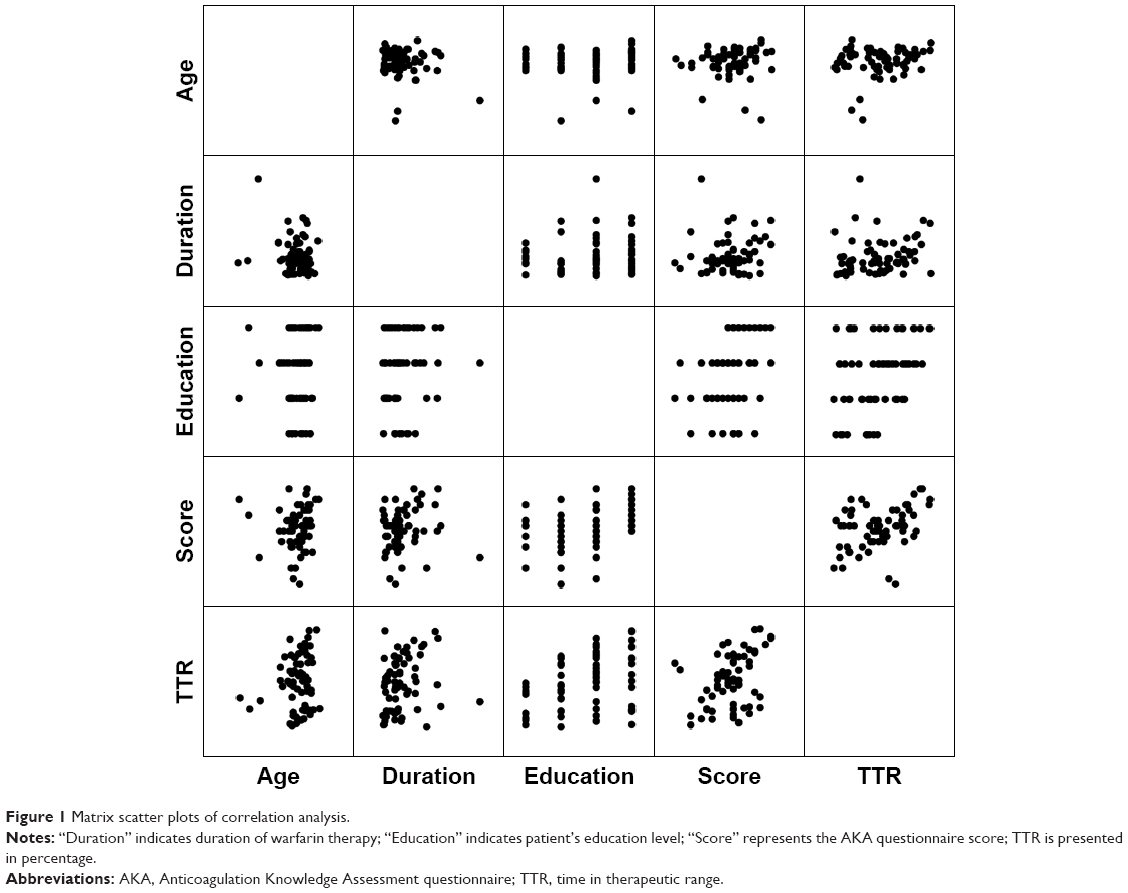 | Figure 1 Matrix scatter plots of correlation analysis. |
Discussion
This study was the first to assess warfarin knowledge level among clinical patients in mainland China. In the study population, 90.8% patients were found to have inadequate knowledge about their warfarin therapy. This number was higher compared to the result in studies conducted in Canada (61%)14 and the US (74.1%)10 but was lower than the study conducted in Nepal (94.1%).8 Although direct comparison of study results is difficult because patient education methods and study methodology varied among warfarin clinics and study samples, our findings indicated poor knowledge level in our study population.
Eleven questions were answered correctly by <50% of the patients. Five questions covered drug or diet interactions with warfarin: alcohol (Question 6), multivitamins (Question 7), pain medications (Question 1), antibiotics (Question 12), and herbals (Question 18). Question 1 addressed pain medications that can be safely used to relieve headache. Most patients indicated that they did not experience headache while on warfarin therapy, and they were not educated about this topic. Two more questions with the most-often-incorrect responses covered bleeding (Question 9) and nonbleeding (Question 21) adverse reactions from warfarin therapy. Questions 15 and 20 assessed patients’ understanding of the value of laboratory monitoring of INR. The question on the duration of warfarin effects, namely, the elimination time, had a correct response of only 26.2% (Question 27). Question 28 assessed patients’ understanding of the duration of their warfarin therapy. Since most patients in our study required either long-term or lifelong warfarin therapy, 35.4% patients chose the answer “taking the medication on a lifelong basis”.
These frequently incorrect-response-yielding questions indicate potential areas for improvement in patient education, in addition to representing potential starting points for reeducation of current warfarin patients and future targeted education for new patients seen in the clinic aimed at the clinic’s pharmacist. For example, the meaning of INR should be explained in plain, easy-to-understand language: “the INR provides some information about a person’s blood’s tendency to clot (which is often described as how “thin” or “thick” your blood is), and warfarin is used to raise the INR and dilute (“thin”) the blood to reduce the risk of blood clot. When your INR is too high, you will most likely experience minor bleeding”. Patients should be educated about how single excessive drinking causes an increase in INR and the risk of bleeding. Prior to taking over-the-counter multivitamins and “all natural” herbal supplements (agents with the perception of being safe due to their over-the-counter availability), patients should consult with their physicians and/or pharmacists whether these supplements may interact with warfarin. The most common prescription drugs that may have significant drug interactions with warfarin, such as certain antibiotics, should be reviewed with patients. Before taking these interacting medications, patients should seek advice from clinicians. Both common bleeding signs/symptoms and nonbleeding adverse effects of warfarin should be communicated to patients, along with the proper course of action to take should these events occur. It is also very important to tell patients that the duration of their warfarin therapy depends on their disease states and is individualized and that they should not stop the therapy on their own. Currently, we are conducting the reevaluation of our current standard patient education methods and instructional materials based on this analysis, and more-targeted individualized patient education will be offered to the clinic’s patients by the clinic’s pharmacist.
TTR is important for the safety and effectiveness of warfarin anticoagulation, and it is a way of summarizing the INR control over time. Among the 65 study patients, the mean TTR was 49.8%±24.8%, which was inadequate according to the recommended level of anticoagulant control (>60.0%).15 This result was worse than the TTR presented by other authors.7,15–17 The reasons explaining our low TTR require further investigations.
The existing literature indicates mixed results when assessing the relationship between patient warfarin knowledge and INR control. A study conducted in Hong Kong found that knowledge was a determinant of anticoagulation control, and more attention should be given to the education of elderly and illiterate patients. However, only nine questions were used to test patients’ knowledge of warfarin therapy, and another limitation was that only four INR results were reviewed per patient in that study.6 A study conducted in the US reported that there was no significant relationship between patient warfarin knowledge and INR control.10 Another study carried out in Malaysia reported that there was a negative correlation between patients’ knowledge and age, as well as a positive correlation between patients’ knowledge and education level.18 Our study found that TTR was positively related to both the patients’ anticoagulation knowledge level and the patients’ educational level, whereas other factors, such as age and duration of warfarin therapy, had no effect on the TTR. Based on our findings, pharmacists should spend more time or find innovative teaching techniques to educate patients with low educational levels and use the AKA as a tool to provide reeducation to current warfarin patients based on the knowledge deficits identified herein.
Our study has the following limitations: 1) the small sample size drawn from a single clinic; a large-scale and multicenter study would be necessary to generalize the study findings; and 2) aspects that could lead to INR variations, such as diets and use of herbal and/or dietary supplements, were not assessed.
Conclusion
Majority of the patients of our clinic had poor level of knowledge on warfarin. There was a significant association between the INR outcome measure and both the patients’ educational level and warfarin knowledge. The frequently few correct-response-generating AKA questions represent potential areas for improvement in patient education. Pharmacists should reevaluate current educational materials and techniques to provide individualized and targeted warfarin patient education.
Acknowledgment
The authors would like to acknowledge and thank the physicians, pharmacists, and patients who participated in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
Zhao SJ, Zhao HW, Wang XP, et al. [Current status of warfarin therapy in Chinese patients with nonvalvular atrial fibrillation: a single center analysis]. Zhonghua Xin Xue Guan Bing Za Zhi. 2016;44(11):940–944. | ||
Zhang J, Yang XA, Zhang Y, et al. Oral anticoagulant use in atrial fibrillation-associated ischemic stroke: a retrospective, multicenter survey in northwestern China. J Stroke Cerebrovasc Dis. 2017;26(1):125–131. | ||
Ansell J, Hirsh J, Hylek E, et al. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians evidence-based clinical practice guidelines (8th edition). Chest. 2008;133(6 suppl):160S–198S. | ||
Riley RS, Rowe D, Fisher LM. Clinical utilization of the international normalized ratio (INR). J Clin Lab Anal. 2000;14(3):101–114. | ||
Michaels K, Regan EN. Teaching patients INR self-management. Nursing. 2013;43(5):67–69. | ||
Tang EO, Lai CS, Lee KK, Wong RS, Cheng G, Chan TY. Relationship between patients’ warfarin knowledge and anticoagulation control. Ann Pharmacother. 2003;37(1):34–39. | ||
van Walraven C, Jennings A, Oake N, Fergusson D, Forster AJ. Effect of study setting on anticoagulation control: a systematic review and metaregression. Chest. 2006;129(5):1155–1166. | ||
Shrestha S, Sapkota B, Kumpakha A, Acharya U, Sharma R. Evaluation of patients’ knowledge on warfarin in outpatient pharmacy of a tertiary care cardiac center. BMC Res Notes. 2015;8:429. | ||
Briggs AL, Jackson TR, Bruce S, Shapiro NL. The development and performance validation of a tool to assess patient anticoagulation knowledge. Res Social Adm Pharm. 2005;1(1):40–59. | ||
Baker JW, Pierce KL, Ryals CA. INR goal attainment and oral anticoagulation knowledge of patients enrolled in an anticoagulation clinic in a Veterans Affairs medical center. J Manag Care Pharm. 2011;17(2):133–142. | ||
World Health Organization [webpage on the Internet]. Process of Translation and Adaptation of Instruments. 2017. Available from: http://www.who.int/substance_abuse/research_tools/translation/en/. Accessed November 10, 2017. | ||
Nam MH, Roh KH, Pak HN, et al. Evaluation of the Roche CoaguChek XS handheld coagulation analyzer in a cardiac outpatient clinic. Ann Clin Lab Sci. 2008;38(1):37–40. | ||
Rosendaal FR, Cannegieter SC, van der Meer FJ, Briet E. A method to determine the optimal intensity of oral anticoagulant therapy. Thromb Haemost. 1993;69(3):236–239. | ||
Hu A, Chow CM, Dao D, Errett L, Keith M. Factors influencing patient knowledge of warfarin therapy after mechanical heart valve replacement. J Cardiovasc Nurs. 2006;21(3):169–175; quiz 176–167. | ||
Connolly SJ, Pogue J, Eikelboom J, et al; ACTIVE W Investigators. Benefit of oral anticoagulant over antiplatelet therapy in atrial fibrillation depends on the quality of international normalized ratio control achieved by centers and countries as measured by time in therapeutic range. Circulation. 2008;118(20):2029–2037. | ||
de Lima Silva RG, Bertollo CM, Ferreira IG, Brant LC, Martins MAP. Assessment of oral anticoagulation control at two pharmacist-managed clinics in Brazil. Int J Clin Pharm. 2017;39(6):1157–1161. | ||
Dlott JS, George RA, Huang X, et al. National assessment of warfarin anticoagulation therapy for stroke prevention in atrial fibrillation. Circulation. 2014;129(13):1407–1414. | ||
Hasan SS, Shamala R, Syed IA, et al. Factors affecting warfarin-related knowledge and INR control of patients attending physician- and pharmacist-managed anticoagulation clinics. J Pharm Pract. 2011;24(5):485–493. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.