Back to Journals » Local and Regional Anesthesia » Volume 14
Assessment of Morphological and Morphometrical Variations of Sacral Hiatus in Dry Human Sacrum in Ethiopia
Authors Abera Z, Girma A ![]() , Bekele A, Oumer M
, Bekele A, Oumer M ![]()
Received 2 November 2020
Accepted for publication 12 February 2021
Published 24 February 2021 Volume 2021:14 Pages 25—32
DOI https://doi.org/10.2147/LRA.S277556
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Zerihun Abera,1 Amanuel Girma,2 Assegedech Bekele,2 Mohammed Oumer2,3
1Department of Biomedical Sciences, School of Medicine, College of Medicine and Health Sciences, Arsi University, Arsi, Oromia, Ethiopia; 2Department of Human Anatomy, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Amhara, Ethiopia; 3Department of Epidemiology, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Amhara, Ethiopia
Correspondence: Amanuel Girma Tel +251 913554235
Email [email protected]
Background: The sacral hiatus is an opening present at the lower end of the sacral canal. The anatomy of the sacral hiatus and its variations are clinically important during administration of caudal epidural block (CEB) in obstetrics and gynecology, orthopedic, urology and general surgical practices. The success and reliability of CEB depends upon the sound knowledge of anatomical variations of the sacral hiatus.
Objective: The aim of this study was to assess the morphological and morphometric variation of the sacral hiatus in dry human sacrum.
Methods: An institution-based observational cross-sectional study design was conducted to assess morphological and morphometric variations of the sacral hiatus in 61 dry human sacrum specimens at the anatomy departments of Gondar, Addis Ababa, Hawassa and Jimma universities and Hayat and Korea Medical Colleges in Addis Ababa. Descriptive analysis was applied to analyze the data.
Results: The most commonly recorded shape of the sacral hiatus is inverted-V (41%) followed by inverted-U (37.7%). The least common was complete bifida (1.6%). The apex of the sacral hiatus is mostly seen at the level of the 4th sacral vertebra (60.7%), while the base is commonly located at the level of the 5th sacral vertebra (78.7%). The mean length of the sacral hiatus is 22.67 ± 11.84 mm. The mean transverse width and mean anteroposterior diameter of the sacral hiatus at the apex are 13.14 mm ± 2.85 mm and 5.57 mm ± 1.53 mm, respectively.
Conclusion: The sacral hiatus has anatomical variations. These variations should be kept in mind during administration of caudal epidural anesthesia and analgesia.
Keywords: assessment, sacrum, sacral hiatus, variations, Ethiopia
Background
The sacrum is a large triangular bone formed by the fusion of five sacral vertebrae in adults.1–6 The sacrum forms the postero-superior wall of the pelvic cavity, wedged between the two innominate bones.7–9 It has a blunted caudal apex which articulates with the coccyx and a superior wide base which articulates with the fifth lumbar vertebra at the lumbosacral angle. In addition the sacrum presents pelvic, dorsal and lateral surfaces and a sacral canal. The opening at the caudal end of the sacral canal is known as the sacral hiatus (SH).10,11 It is formed due to the failure of fusion of laminae of the fifth (occasionally fourth) sacral vertebra. It is located inferior to the fourth (or third) fused sacral spines or the lower end of the median sacral crest.10–12
The sacral hiatus (SH), which is roughly triangular in shape, contains the fifth sacral nerve, coccygeal nerve roots, filum terminale externum and fibro-fatty tissue. For a successful caudal epidural block (CEB), knowledge of the anatomy of the sacral hiatus and its variations is important.13
Anatomical variations occur frequently, making the sacrum the most variable portion of the spine. Developmental malformations occur ranging from variations in the sacral hiatus to caudal agenesis.14 The sacral hiatus shows variations during development. Non-fusion of laminae of the 4th or the upper vertebrae results in an elongated sacral hiatus. Non-fusion of all the sacral vertebrae results in sacral spina bifida. This leads to decreased surface area for the attachment of extensor muscle at the back, which may be a cause of backache.7
Considerable variability is seen in the anatomy of the sacral hiatus, which may be closed, asymmetrically open or wide open. As age advances, the overlying ligaments and the cornua thicken. Consequently, identification of hiatus margins becomes challenging. In addition to this, anatomic variations in size, shape and orientation of the sacral hiatus increase the problems in caudal anesthesia.15,16
For a successful CEB intervention, a fundamental knowledge of the anatomy of the sacral hiatus is a prerequisite.13 However, the considerable anatomical variations of the SH may make its identification difficult.17 A sacral approach to the epidural space is used for giving analgesia and anaesthesia for a variety of operations. Caudal epidural block (CEB) has been widely used for the treatment of lumbar spinal disorders and also for the management of chronic back pain.18 Caudal epidural block involves injection of a drug into the epidural space through the sacral hiatus to provide analgesia and anesthesia in various clinical settings.19 Caudal analgesia is used during surgical procedures in urology, proctology, general surgery, obstetrics and gynecology and orthopedics. Anesthetic agents are injected through the sacral hiatus in caudal epidural anesthesia to act on the sacral and coccygeal nerves and are often employed to relax the perineal musculature for painless childbirth.17
The reliability and success of caudal epidural anesthesia depends upon anatomical variations of the sacral hiatus as observed by various authors. Therefore, the aim of this study is to discover the anatomical variations of the sacral hiatus, investigating the morphometry and morphology of the sacrum in Ethiopia.
Methods and Materials
An institution-based descriptive cross-sectional study design was applied. A total of 61 dry human sacral bones held at the Department of Anatomy in Gondar, Jimma, Addis Ababa, Hawassa Universities, Hayat and Korea Medical Colleges in Addis Ababa were used within this study. The bones, which were of undetermined age and gender, were subjected to morphometric study. The analysis was carried out in two parts:
Part I: Non-Metric Analysis
- The shape of the sacral hiatus was classified as inverted-V shape, inverted-U shape, dumb-bell shape, irregular shape, bifida shape and complete bifida shape.
- Level of the apex of the sacral hiatus was evaluated in relation to the vertebra level as S1, S3, S4 and S5.
- Level of the base of the sacral hiatus was evaluated in relation to the sacral and the coccygeal vertebra as S5, Co1.
Part II: Metric Analysis
- Length of sacral hiatus: The distance from the apex to the midpoint of the base of the SH.
- Transverse width of sacral hiatus (intercornual distance): The distance between the inner surface of the inferior limit of the sacral cornua.
- Antero-posterior diameter of sacral hiatus: Antero-posterior depth at the apex of the SH.
The parameters were measured twice by the same author using caliper, divider and steel measuring tape. Observations were substantiated with photographs. Damaged, mutilated and deformed sacra were excluded. Descriptive analysis was applied to analyze the data.
Ethical Approval and Consent
The study protocol was approved by the ethical review committee of College of Medicine and Health Sciences, University of Gondar.
Results
Part I: Non-Metric Analysis
- The sacral hiatus of each specimen was classified according to shape. The shape was mainly inverted-V (41%) or inverted-U (37.7%), which is normal type. Dumb-bell shape (11.5%) with a nodular bony growth projecting medially from both margins, irregular shape (4.9%) and bifid shape (3.3%) were also observed. The dorsal wall of sacral canal was entirely incomplete in 1.6% of cases (Table 1) (Figure 1–6).
- The level of the apex of the sacral hiatus varied from S1 to S5. It was as high as S1 in 3.3%, as low as S5 in 9.8% and was most commonly located against S4 in 60.7% cases. In the remaining 26.2% of cases the apex was found at the S3 level (Table 2) (Figures 1, Figures 2, Figures 3Figures 4, Figures 5, Figures 6, Figures 7 and 8).
- The level of the base of the sacral hiatus was commonly located at S5 (78.7%). In 21.3% of cases, the base was found at the first coccygeal level (Table 3) (Figures 9 and 10).
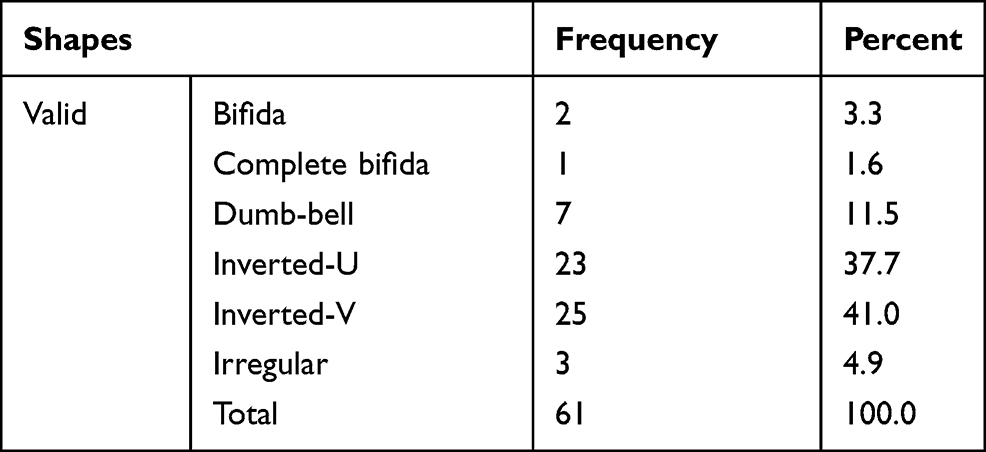 |
Table 1 Shape of the Sacral Hiatus |
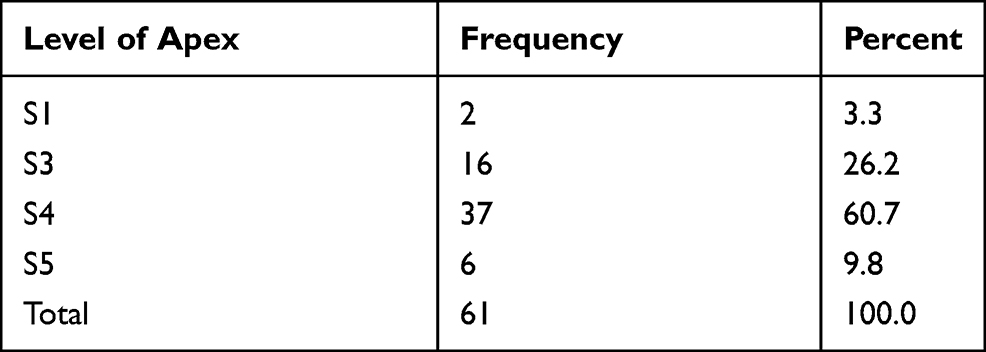 |
Table 2 Level of Apex of SH with Respect to Level of Sacral Vertebra |
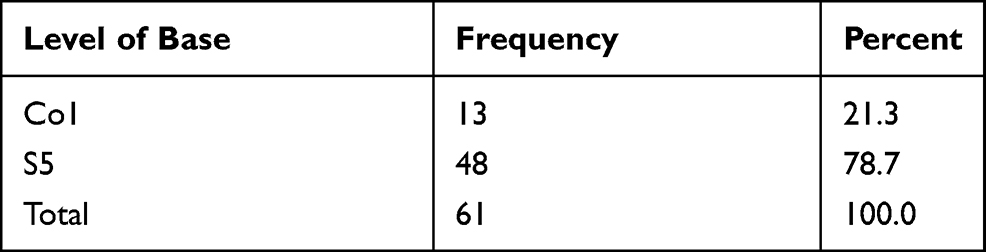 |
Table 3 Level of Base of Sacral Hiatus with Respect to Level of Sacral Vertebra |
 |
Figure 1 Schematic representation of dumb-bell shape of SH. |
 |
Figure 2 Schematic representation of bifida shape of SH. |
 |
Figure 3 Schematic representation of irregular shape of SH. |
 |
Figure 4 Schematic representation of inverted-V shape of SH. |
 |
Figure 5 Schematic representation of inverted-U shape of SH. |
 |
Figure 6 Schematic representation of complete bifida. |
 |
Figure 7 Schematic representation of level of apex at S4. |
 |
Figure 8 Schematic representation of level of apex at S5. |
 |
Figure 9 Schematic representation of level of base at S5. |
 |
Figure 10 Schematic representation of level of base at Co1. |
Part II: Metric Analysis
- Length of the sacral hiatus varied from 6 mm to 80 mm, with the arithmetic mean 22.67 mm and standard deviation 11.84 mm. The proportion of sacrum specimens having a sacral hiatus length of 0–10 mm was 4.9%, while 45.9% had a length of 11–20 mm and 34.4% of human sacra had a sacral hiatus length of 21–30 mm; 14.7% of specimens had a sacral hiatus longer than 31 mm (Tables 4 and 5) (Figure 11).
- Transverse width of the sacral hiatus (intercornual distance) varied from 9mm to 21mm, with the arithmetic mean 13.14mm and standard deviation 2.85mm. The majority of human sacra (63.9%) had the transverse width in the range 11–15mm, 19.7% had transverse width of 6–10 mm, 14.8% of the human sacra had 16–20 mm and only 1.6% had the transverse width >21 mm (Tables 4 and 5).
- Antero-posterior diameter of sacral hiatus varied from 3 mm to 9 mm, with the arithmetic mean 5.57 mm and standard deviation 1.53 mm. The largest proportion (60.7%) of human sacra had the AP diameter between 4 and 6 mm, followed by 31.1% with AP diameter of 7–9 mm and only 8.2% associated with the AP diameter 0–3 mm (Tables 4 and 5).
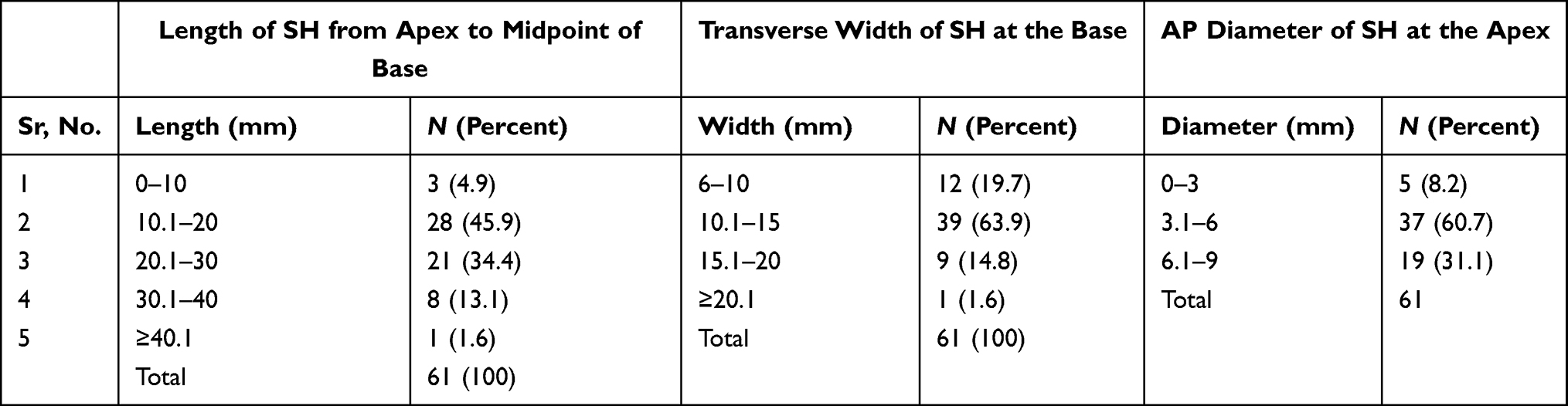 |
Table 4 Length, Transverse Width and AP Depth of Sacral Hiatus |
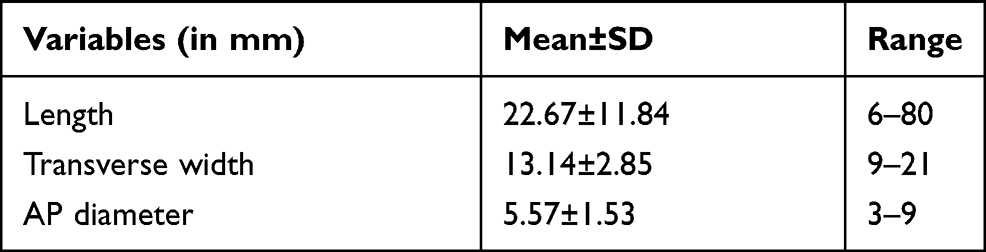 |
Table 5 Length, Transverse Width and AP Depth of Sacral Hiatus (Expressed in Terms of Mean, Standard Deviation and Range) |
 |
Figure 11 Schematic representation length of SH from apex to base. |
Discussion
Caudal epidural block and caudal epidural anesthesia, which are accessed through the SH, have a wide range of clinical applications. Successful CEB is possible with determining the anatomical structure of the SH.20 The apex of SH location is also required for procedures such as colposcopy and trans-sacral endoscopy.21–23 However, because of anatomical variation of the SH, a problem can be encountered during insertion of a needle in the sacral canal through the SH.20 Locating the apex of the SH is also difficult because of its variation.14 Hence knowledge on anatomical structure of the SH is essential for successful clinical procedures.
The shape of the SH is one of the most important landmarks.15,16 Inverted-V (41%) and inverted-U (37.7%) were the most common types, somewhat similar to the results of the study by Ukoha et al24 who reported inverted-V (33.1%) and inverted-U (24%). This was contradictory to the observations by Bhattacharya et al25 who reported inverted-U (65%) and inverted-V (23%), and Doshi et al26 who reported inverted-V (14%) and inverted-U (56%). Inverted-V and inverted-U shapes provide enough space for inserting the needle into the sacral canal without obstacle and are considered as normal.
Thus, difficulties encountered in the SH may possibly be due to other SH types which accounted for 21.3%. In our study, we found that 11.5% of SH were dumb-bell shaped, which is high compared with previous investigators who reported only 3%27 and 9.3%.24 Bifid sacral hiatus was seen in 3.3%, which was similar to the report by Malarvani et al27 (3%). Complete spina bifida was observed in 1.6%, which is low when compared with observation by Malarvani et al27 (3%). Irregular shape was found in 4.9%, with Malarvani et al27 and Desai et al26 reporting 14% and 16%, respectively.
Knowledge of the apex of the SH is important to ensure safety of dura. The apex of SH location was most frequently reported at level of S4. Bhattacharya et al25 and Ukoha et al24 reported 74% and 66.6%, respectively. In our study it was 60.7%. Apex of the SH located at S3 and above, accounting for 29.5% in our study, is not safe since it is close to the dura mater.
Base of the SH location is frequently reported at the level of the S5 vertebra. In the works of Malarvani et al,27 Desai et al26 and Ukoha et al,24 the prevalence was 54%, 62% and 59.3%, respectively. In this study, a base of the SH at coccyx level was found in 21.3% of specimens. In the works of Malarvani et al27 and Ukoha et al24 the figures were 1% and 14%, respectively. In this study, the base was defined as S5 segment in 78.7% of specimens.
Length of SH varied widely in our study. The lower level was 6 mm which was close to the report by Ukoha et al24 (6.1 mm). But the upper level in our study was much higher compared to that of the Ukoha et al24 report (80 mm and 57 mm, respectively). The arithmetic mean was 22.67 mm, which was higher compared to the Ukoha et al24 (20 mm), and lower compared to the Desai et al26 (25.2 mm) reports. A longer hiatus facilitates needle entry into the sacral canal; at the same time, it indicates reduced distance between the apex of the SH and termination of the dural sac, thus increasing the possibility of the needle puncturing the dural sac. A shorter hiatus, especially in obese individuals because of the overlying fat, may prove difficult when locating the SH. In our study, 45.9% had a length of the SH in the range 11–20 mm, similar to the study conducted by Clarista et al10 (45%) and higher compared to the report by Desai et al26 (15%). A length of SH below 10 mm was found in 4.9%, which is close to the report by Desai et al26 (4%) but lower when compared to the report by Clarista et al10 (11.9%). A length of SH in the range 31–40mm was found in 13.1%, similar to the study conducted by Ukoha et al24 (13%).
Transverse width (intercornual distance) measurement has been found to range from 9 mm to 21 mm, with mean 13.14 mm ± 2.84 mm. The range was narrower when compared with the report by Desai et al26 (3–25 mm, mean 19.5 mm), Clarista et al10 (6.5–29.2 mm, mean 16.87 ± 3.66 mm) and Ukoha et al24 (5–20.5 mm, mean 12.35 ± 3.12 mm). Intercornual distance wider than a centimeter is sufficient for needle insertion. In our study intercornual distance up to 10 mm accounted for 19.7%, which was higher compared to reports by Ukoha et al24 (11.1%) and Clarista et al10 (2.1%).
Anteroposterior diameter of the SH at apex needs to be sufficient to admit the needle into the sacral canal. In our study it ranged from 3 to 9 mm, with mean 5.57 ± 1.53 mm. Ukoha et al24 reported 0.4–11.1 mm, with mean 5.52 ± 1.89 mm. Another report by Clarista et al10 found the range 1.98–9.92 mm, with mean 5.58 ± 1.66 mm. Clarista et al10 reported that the diameter of the SH at apex was less than 2 mm in 1% of sacral bones, hence impeding the use of 22G needles for CEB. In our study no case was reported below 2 mm anteroposterior diameter.
Conclusion
The sacral hiatus has anatomical variations, and understanding of these variations may improve the success rate for administration of caudal epidural anesthesia. In this study, shapes of sacral hiatus that may present hindrance to needle insertion, higher level of apex of SH close to the dura and narrow transverse width of SH were found in significant percentage. This should be kept in mind while giving caudal anesthesia in the Ethiopian population.
Abbreviations
AP, anteroposterior; SH, sacral hiatus; Co, coccyx; S, sacral; CEB, caudal epidural block; CEA, caudal epidural anesthesia.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Acknowledgments
Authors sincerely acknowledge University of Gondar for funding the research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding was covered by University of Gondar (www.edu.uog.et).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Patel ZK, Thummar B, Patel S, Zalawadia A. Multicentric morphometric study of dry human sacrum of Indian population in Gujarat Region. NJIRM. 2011;2(2):2–6.
2. Aggarwal A, Harjeet SD. Morphometry of sacral hiatus and its clinical relevance in caudal epidural block. Surg Radiol Anat. 2009;31(10):793–800. doi:10.1007/s00276-009-0529-4
3. Saha D, Bhattacharya S, Uzzaman A, Mazumdar S, Mazumdar A. Morphometric study of variations of sacral hiatus among West Bengal population and clinical implications. Ital J Anat Embryol. 2016;165–171.
4. Shewale SN, Laeeque M, Kulkarni PR, Diwan CV, Government H, College M. Morphological and morphometrical study of sacral hiatus. Int J Recent Trends Sci Tech. 2013;6(1):48–52.
5. The sacrum the holy bone; 2003. Available from: http://www.MedicineNet.com.
6. Frazer EJ. Anatomy of the Human Skeleton. London: J and A Churchill ltd; 1914:37–42.
7. Brailsford JF. Deformities of lumbosacral region of spine. Br J Surg. 1929;16(64):562–570. doi:10.1002/bjs.1800166405
8. Basaloglu H, Turgut M, Taser FA, Ceylan T, Basaloglu HK, Ceylan AA. Morphometry of the sacrum for clinical use. Surg Radiol Anat. 2005;27(6):467–471. doi:10.1007/s00276-005-0036-1
9. Ergur J, Akcalio O, Kiray A, Kosay C, Tayefi H. Neurovascular risk of sacral screws with bicortical purchase: an anatomical study. Eur Spine J. 2007;16(9):1529. doi:10.1007/s00586-007-0326-x
10. Clarista MQ, Gautham K. Morphometrical study of sacral hiatus in dry human. CIBTech J Surg. 2013;2(2):56–63.
11. Williams. PL, Bannister LH, Berry. MM, et al. Gray’s Anatomy.
12. McLeod G. Spinal anaesthesia: intradural and extradural. In: Davis NJH, Cashman JN, editors. Lee’s Synopsis of Anaesthesia.
13. Parashuram R. Morphometrical study of sacral hiatus in dry human sacra. J Res Med Sci. 2015;3(7):1726–1733. doi:10.18203/2320-6012.ijrms20150260
14. Sekiguchi M, Yakuki S, Kikuchi S. An anatomic study of sacral hiatus: a basis for successful caudal epidural block. Clin J Pain. 2004;20(1):51–54. doi:10.1097/00002508-200401000-00010
15. Mrudula C, Naveena S. Morphometry of sacral hiatus and its clinical relevance. Int J Adv Res. 2013;1(7):29–34.
16. Mohamed SM, Omayma MM, El Raouf HHA, Hosam MA. Morphometric study Of Sacral hiatus in adult human Egyptian sacra: their significance in caudal epidural anesthesia. Saudi J Anaesth. 2012;6(4):350–357. doi:10.4103/1658-354X.105862
17. Edwards WB, Hingson RA. Continuous caudal anaesthesia in obstetrics. Am J Surg. 1942;57(3):459–464. doi:10.1016/S0002-9610(42)90599-3
18. Anjali A, Aditya A, Daisy S. Morphometry of sacral hiatus and its clinical relevance in caudal epidural block. Surg Radiol Anat. 2009;31:793800.
19. Chen PC, Tang STF, Hsu T-C, et al. Ultrasound guidance in caudal epidural need placement. Anaesthesiol. 2004;101(1):181–184. doi:10.1097/00000542-200407000-00028
20. Senoglu N, Senoglu M, Oksuz H, et al. Landmarks of the sacral hiatus for caudal epidural block: an anatomical study. Br J Anaesth. 2005;95(5):692–695. doi:10.1093/bja/aei236
21. Nagar SK. A study on sacral hiatus in dry human sacra. J Anat Soc India. 2004;53:18–21.
22. Suma HY, Kulkarni R, Kulkarni RN. A study of sacral hiatus among sacra in South Indian population. Anat Karnataka. 2011;5:40–44.
23. Phalgunan V, Baskaran S. Morphometric analysis of sacral hiatus and its Clinical Significance. Health Agenda. 2013;1:10–15.
24. Ukoha UU, Okafor JI, Anyabolu AE, Ndukwe GU, Eteudo AN, Okwudiba NJ. Morphometric study of the sacral hiatus in Nigerian dry human sacral bones. Int J Med Res Heal Sci. 2014;3(1):115.
25. Bhattacharya S, Majumdar S, Chakraborty P, Mazumdar S, Mazumdar A. Original article: a morphometric study of sacral hiatus for caudal epidural block among the population of West Bengal. Int J Basic Appl Med Res. 2013;Vol.-2(Issue–7):660–667.
26. Desai RR, Jadhav SD, Doshi MA, Ambali MP, Desai AR. Variations in anatomical features of the sacral hiatus in Indian dry sacra. Int J Med Res Heal Sci. 2014;3(3):634.
27. Malarvani T, Ganesh E, Nirmala P. Study of sacral hiatus in dry human sacra in Nepal, Parsa Region. Int J Anat Res. 2015;3(1):848–855. doi:10.16965/ijar.2014.527
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.