Back to Archived Journals » Chronic Wound Care Management and Research » Volume 7
Assessment of Acceptability and Ease of Use of Haemoglobin Spray (Granulox®) in the Management of Chronic Wounds
Authors Kröger K, Gäbel G, Juntermanns B
Received 20 September 2019
Accepted for publication 4 February 2020
Published 13 March 2020 Volume 2020:7 Pages 1—10
DOI https://doi.org/10.2147/CWCMR.S212108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Marco Romanelli
Knut Kröger, Gabor Gäbel, Benjamin Juntermanns
Department of Vascular Medicine, HELIOS Clinic Krefeld, Krefeld, Germany
Correspondence: Knut Kröger
Department of Vascular Medicine, HELIOS Clinic Krefeld, Lutherplatz 40, Krefeld 47805, Germany
Tel/Fax +49 2151 321669
Email [email protected]
Abstract: Wound healing is a complex and orchestrated process. Oxygen is one of the molecules that is required throughout the wound healing continuum for various underlying processes from innate immune response at the inflammatory phase to building of collagen type III at the remodelling phase. Therefore, it is not surprising that, due to primary diseases like venous insufficiency and diabetes mellitus, hypoxia caused by sustained lack of oxygen is common in chronic wounds. Adjunct to systemic therapies of the primary disease aimed at revascularizing the tissue, recently developed technologies are now available that provide topical oxygen-enhanced wound healing. Several devices are designed to provide pure oxygen directly to the wound either with or without pressure. Another approach to the provision of additional topical oxygen is to use haemoglobin to facilitate oxygen diffusion. This phenomenon was first shown more than 50 years ago, but it has only recently been discovered as a means of improving wound healing. In vitro and in vivo studies have shown that haemoglobin is capable of transporting oxygen outside of erythrocytes. Furthermore, several clinical studies have shown a beneficial effect on wound healing in different wound types. In this review, we summarise publicly available in vitro and in vivo clinical data and discuss the acceptability and ease of use of haemoglobin spray (Granulox®) in the management of chronic wounds. In conclusion, currently available data are promising, demonstrating that purified haemoglobin in an aqueous solution is able to serve as an oxygen shuttle by facilitating diffusion. No severe side effects have been reported in the literature, implying that it is a safe product. In clinical studies, it has been observed to improve the speed of healing of different types of chronic wounds. As a simple spray, it can be used as adjunct treatment in many standard-of-care settings with only a few limitations.
Keywords: oxygen, hypoxia, facilitated diffusion, topical oxygen therapy, wound healing, oxygen carrier
Introduction
Chronic Wounds
Chronic wounds are characterised by not healing in an orderly and timely manner within a time frame of 4 weeks to 3 months.1,2 Prevalence of chronic non-healing wounds is estimated at 1 to 2% of the population in the industrialised world and it is speculated that these numbers will increase due to an increase in elderly population and patients with diabetes or other causative conditions.2–4
The main types of chronic wounds diagnosed are vascular ulcers (eg venous and arterial ulcers), diabetic ulcers, and pressure ulcers (PUs).1 Due to the various underlying primary diseases or conditions like diabetes mellitus, venous insufficiency, arterial occlusive disorder or other comorbidities, the proper diagnosis and treatment of such wounds need to be a multidisciplinary teamplay to enable best care for the patients.1,2,5,6
Consequently, chronic wounds are an increasing burden for the health care systems worldwide. In Europe, wound management costs are estimated to account for 2–4% of health-care budgets.2 As the number of elderly people and people with diabetes is increasing in developed countries, the costs of managing chronic wounds therapies are likely to increase too.7,8 Although the underlying aetiologies may differ, several characteristics are commonly identified among the various types of chronic wounds including infections, biofilm, high level of inflammation, or macro- or microvascular disturbances and hypoxia.1,9,10
Oxygen in Wound Healing
It is well known that an interplay of various biochemical processes needs to be coordinated in a well-controlled fashion during all phases of healing to enable a fast and persistent closure of a wound.11–14 Oxygen is one utmost important molecular player required during the entire wound healing process. As well as being required for energy production in mitochondria (ATP), oxygen plays an important role in many other processes like antimicrobial defence, cell proliferation, generation and maintenance of extracellular matrix, angiogenesis and cell movement.12,13,15,16
In an acute wound, the disruption of capillaries leads to a transient local decrease of oxygen within the wound resulting in inadequate oxygenation of the tissue (hypoxia). It is well known that hypoxia serves as one of the initial stimuli to accelerate wound healing mainly via the transcription factor hypoxia-inducible factor-1 (HIF-1). This factor is involved in the regulation of many molecular repair processes in damaged tissue during hypoxia. As a transcription factor, HIF-1 upregulates the expression of various proteins like cell adhesion integrins, growth factors (TGF-β, VEGF), extracellular matrix type I collagen and fibronectin; it also serves as a positive regulator of various processes during the initial transient hypoxic phase and entire wound healing as adaptive response to hypoxia.17–20 In contrast to the acute wound situation where there is transient and mild-to-moderate hypoxia, one of the commonly observed factors in non-healing or chronic wounds is sustained extreme deprivation of oxygen.13,17,20 Cells that are exposed to prolonged hypoxia convert to a survival mode mechanism. The consequences of this are the uncoupling of anaerobic glycolysis from the tricarboxylic acid (TCA) cycle and oxidative phosphorylation. This response might be regarded as a part of the resistance strategy of cells to hypoxia to maintain energy (in the form of ATP) supply for minimal cellular functions and survival impairing processes like angiogenesis, collagen synthesis, and re-epithelisation.11,21,22 A prolonged disturbance of oxygen supply may ultimately cause cell death and tissue necrosis.
Topical Oxygen and Skin Transmission
The concept of topical oxygen application has been investigated for many years. There are several ways oxygen may penetrate through the skin, which has porous and nonporous regions. Oxygen is a small molecule and can easily pass through skin pores, which span the full thickness of skin layers. An earlier study contrasting oxygen passage across sheets of viable and nonviable epidermis showed similar rates, suggesting that the major route of oxygen transmission is mediated by physiochemical structure rather than active cellular function.23 Distribution of oxygen through human dermal tissue is dependent upon oxygen partial pressure gradients and the solubility of oxygen in the tissue. Allocation of oxygen involves internal transport by cutaneous circulation via dermal papillae and externally by transcutaneous diffusion of atmospheric oxygen. Therefore, in terms of the respiratory needs of the individual, the contribution by the skin is negligible, providing only ~2% of total respiration needs.27 The degree to which cutaneous respiration can contribute to dermal metabolic needs is dependent upon the depth to which topical oxygen penetrates human skin. Penney et al in 1968 showed that sheets of isolated human stratum corneum allow diffusion of oxygen from a chamber of water equilibrated with air to a chamber that contained water deoxygenated by nitrogen.24 It was shown that oxygen diffused through the stratum corneum, raising the oxygen partial pressure of the de-oxygenated water. The thickness of the stratum corneum was estimated to average 12 µm. Piantadosi described in 1999 that topically delivered oxygen was only able to diffuse 50–100 µm.25 Roe and colleagues showed in in vitro experiments that topically applied dissolved oxygen penetrates through >700 µm of human skin slices. Furthermore they found that topically applied oxygen penetrates better though dermis than epidermis and that topical dissolved oxygen devices deliver oxygen more effectively than topical gaseous oxygen devices (see below).26
The goal of appropriate oxygen therapies for wound care is to transfer sufficient oxygen to interstitial tissues to maintain processes required for wound healing throughout all phases of the healing process.
As the concept of topical oxygen application is still under discussion, we provide a findings and limitations of topical oxygen therapy with a focus on the haemoglobin spray.
Topical Oxygen Wound Therapies
As discussed above, a proper diagnosis and identification of underlying causes of chronicity is an important part of wound treatment. If insufficient oxygen supply is identified as one of the factors involved, then addressing the underlying primary diseases is one of the central elements in the treatment of patients with chronic wounds, with the aim of re-vascularising the affected tissue.
Local wound treatment can be considered as the second tier of appropriate therapy. Phase-adapted, moist wound healing according to M.O.I.S.T5 or TIME28 is considered to be the gold standard for the treatment of the majority of chronic wounds. In the newer M.O.I.S.T. concept, oxygen is recognised as an important factor for wound healing. Meanwhile, several approaches are described in the literature, which are aimed at specifically improving the oxygen availability in order to promote the oxygen-dependent processes of wound healing in a targeted manner.2,9,29–31 In 2017, the European Wound Management Association published an evaluation of the current oxygen therapies to guide clinicians on the existing oxygen delivery devices and products (Figure 1).2
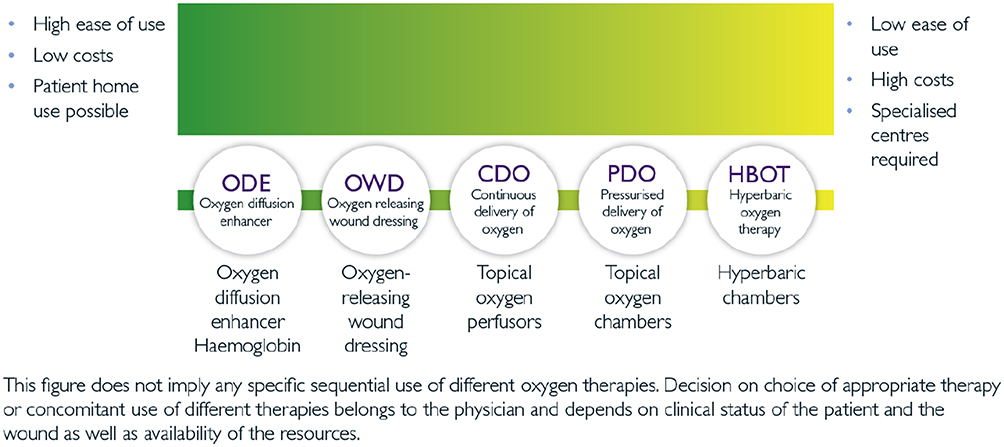 |
Figure 1 General considerations on oxygen therapies. Note: Copyright © 2017. Reproduced with permission from EWMA. Gottrup et al, Use of Oxygen Therapies in Wound Healing. J Wound Care. 2017;26(Sup5):S1–S43.2 |
One approach is a systemic delivery of additional oxygen by hyperbaric oxygen therapy (HBOT). This therapy has been in use for a long time and is suggested to have a beneficial impact on wound healing at least in diabetic foot ulcers.2,30 It requires pressure chambers which are mainly available at dedicated centres.
More recently developed topically acting devices can be divided into three classes. One class of device is based on the local supply of pure humidified oxygen (O2) either by local pressure chambers or small devices continuously delivering oxygen to the wound without pressure. A second class is topical oxygen-releasing dressings which incorporate or release oxygen by a biochemical reaction. The third class of device focuses on the enhancement of oxygen diffusion in the wound bed to the hypoxic area via purified haemoglobin molecules.
In this article, we focus on the acceptability and ease of use of the haemoglobin-based oxygen diffusion-enhancing approach to the management of chronic wounds. Although there are different oxygen-binding molecules described in the literature, only one haemoglobin-based product is currently available. The information obtained for this article was identified by literature searches using publicly accessible databases, namely Pubmed, and Embase, as well as NICE database and Cochrane database for systemic reviews. In addition, articles from other online publishing journals were obtained by searching Google and Google Scholar. The following keywords and meaningful combinations of such were used: “oxygen”, “wound, healing”, “chronic wound”, “haemoglobin”, “topical”, “facilitated diffusion” “spray”, “solution”, “oxygen therapy”, and “oxygen carrier”.
Currently, the only commercially available device is a spray solution comprising 10% of purified porcine haemoglobin stabilised by carbon monoxide. Some additional information (Instructions for Use, IFU) were obtained from the homepage of the manufacturer.
In vitro and in vivo Mode of Action
The approach of using haemoglobin spray is based on the assumption that the wound exudate or even a moist layer on the wound bed acts as a diffusion barrier due to the limited solubility of oxygen in aqueous solutions. The concept to open up this diffusion barrier by using haemoglobin as adjunct wound therapy was originally described by Barnikol and colleagues in 2005.9,32
The principle is called facilitated diffusion, a process which was described as early as the 1960s when it was demonstrated that the addition of purified haemoglobin to a solution augments the transport of oxygen along an oxygen gradient from high to low concentration significantly.33,34
Recent in vitro research published by Petri et al35,36 involved the exposure of a thin layer of haemoglobin spray repetitively to either ambient air or nitrogen to simulate high or low oxygen concentration resulting in a de- and reoxygenation of haemoglobin. The results showed that the haemoglobin spray is capable of binding and releasing oxygen in a fast and repetitive manner, confirming the proposed reversible binding capacity of the haemoglobin.
A second wave of research involved the application of the spray onto chronic venous leg ulcers in a clinical study. The aim of this study was to bridge the in vitro and in vivo situation showing the ability of the applied haemoglobin to provide oxygen. By using a photo-optoacoustic tomography approach, the researchers were able to visualise the conversion of carboxy-haemoglobin to oxyhaemoglobin within less than 20 mins after application. Furthermore, they observed an increase of oxygenation of haemoglobin in the tissue, suggesting an increased diffusion of oxygen facilitated by the haemoglobin spray.35,36
Clinical Evidence
Database searches revealed several clinical studies and case reports published for different wound types. Initial case reports and an open-label study from as early as 2005 suggest a positive impact on wound healing across a comprehensive range of chronic wound types.32,37,38
Venous Leg Ulcers
A prospective, randomised, controlled, single-blinded clinical study published in 2013 compared the adjunct haemoglobin spray therapy on wound size reduction in “hard to heal” patients to a standard-of-care comparator group (moist wound treatment, compression therapy).39 Significant and continuous healing with a reduction of the average wound size by 53% after 13 weeks of treatment was reported for the group receiving haemoglobin spray. In contrast, the comparator group showed no reduction in mean wound size. In addition, the positive healing outcome was independent of the wound surface size when starting treatment. Subsequently case reports and cohort studies involving venous leg ulcer patients support the positive trend of accelerating wound healing.40–42
Diabetic Foot Ulcers
One retrospective, controlled, prospective cohort study evaluated the use of the haemoglobin spray-on diabetic foot ulcers (DFU).7,37 These patients have a greater than two-fold increase in mortality compared with non-DFU patients, highlighting the importance of this work.43 Twenty patients were treated with the haemoglobin spray for 6 months unless wound closure was obtained earlier. A cohort of 20 patients treated over the same period during the year before the introduction of the haemoglobin spray in the clinic served as a retrospective control group. To obtain comparable data, the same inclusion and exclusion criteria were applied. All 20 (100%) haemoglobin spray-treated patients and 15 (75%) control patients experienced some wound healing by week 4, with a mean wound size reduction of 63% in the haemoglobin spray group versus 26% in the control group. The more rapid reduction in overall wound size in the haemoglobin spray group compared to the control group was observed until the end of the study, increasing to 95% reduction at week 28 in the haemoglobin spray group versus 63% for controls (p<0.05 at all timepoints).
Further observations were a) a substantially faster lowering of pain scores (VAS, (100% haemoglobin group pain-free from week 12 onwards vs 33% control), b) an elimination of slough after 4 weeks in the haemoglobin group versus 10% mean reduction in the control group (p<0.001, similar baseline slough levels) and c) an improved impact on exudate level reduction within 4 weeks.
Other explorative case reports37 indicate that the adjunctive haemoglobin spray might be a valid tool to facilitate wound healing in DFUs.
Pressure Ulcers
A first published evaluation reported the use of the topical haemoglobin spray adjunct to standard care in 18 patients with pressure ulcers. Following a 4 weeks treatment period, a clear wound size reduction was observed in 17 wounds.44 For 11 patients who continued to be treated for 3 months, 9 wounds healed and 2 showed a wound-size reduction. In all cases, fast prevention of slough recurrence was achieved while 9 out of 10 patients with pain at baseline were pain-free by week 8.45
Chronic Wounds
Arenberger and colleagues summarised the results of an open labelled prospective clinical study from Mexico (42 patients) as well as several case series of wounds with different aetiologies in Germany (6 patients), the Czech Republic (5 patients) and Mexico (9 patients).37 They stated that the application of the haemoglobin spray promoted wound healing in most of the analysed cases.
In a retrospectively controlled cohort study conducted in the United Kingdom, 50 patients with different types of chronic healing wounds were treated with the haemoglobin spray as adjunctive treatment for an evaluation period of 26 weeks.42 and compared to a similar retrospective control group. Wound closure was obtained in 90% of the patients with the adjunct treatment in a mean time to closure of 6.6 weeks while 38% (p<0.01) wound closure was achieved in the control group within a mean time of 11.4 weeks (p<0.01). According to the authors, a Cox proportional hazards analysis model adjusting for baseline wound size and wound age showed significant treatment effects. Similar to the DFU study mentioned earlier, pain and exudate levels, as well as slough recurrence, were all reduced to a greater extent versus the control group.42
Unfortunately, the authors stated that there was a difference between the groups in wound management which might have a significant bias on the outcome as dressing changes in the control group were conducted by a health-care professional, while haemoglobin spray patients generally self-treated or were treated by their carer due to a change in the departmental practices over time. However, it has to be acknowledged that all results obtained by the published cohort studies may not be as robust as they could be in a formal randomised, fully blinded clinical study. As such, it is obvious that future well-designed, prospective, randomised studies may reduce any potential bias changes in clinical practice tested.
In view of these promising findings for various chronic wound types, further higher-level studies like an RCT would be of benefit in helping to fully elucidate the efficacy of the haemoglobin spray.
Haemoglobin Wound Therapy Modalities and Compatibilities
Appropriate management of chronic wounds requires as prerequisite an initial thorough assessment of the wound and patient to understand the underlying factors responsible for delaying or inhibiting the healing process. The first step of wound treatment is appropriate wound bed preparation which is important for all wound therapies to ensure the effectiveness of all applied treatments such as local oxygen therapies.46,47
As the haemoglobin topical oxygen treatment is described in the literature as an adjunct therapy, it is intended to be aligned with most of the moist wound therapies without changing the established treatment modalities.2,9 As mentioned earlier, wound debridement or at least cleansing is required before haemoglobin spray application to optimise conditions for oxygen delivery. Dependent on the wound status and the need to apply further additional therapies, treatment intervals may vary from once daily to twice a week as outlined in several publications.9,37,39,42
Haemoglobin spray is reported to be easy to apply onto the wound as an even layer (Figure 2).
 |
Figure 2 Application of haemoglobin spray as thin layer onto a diabetic foot ulcer after wound cleansing. Note: Photo courtesy of K Kröger 2019. |
Compared to other technical devices, this approach is very simple. As it is a protein-containing product, the product should be stored in a refrigerator according to the manufacturer.
Regarding dressings and other treatment modalities used in combination with the haemoglobin spray, different product combinations have been used in the reports mentioned in this article, but the spray has mainly been used with a simple foam as a secondary dressing. Dependent on the exudate level, superabsorbent dressings were also used.
It is emphasised by various authors that the secondary dressing used should be air-permeable to enable sufficient oxygen to penetrate to the wound bed.9,39,41,48
Expert consensus recommendations guide that topical haemoglobin should be considered for wounds which are considered as being, or at risk of becoming, chronic that have failed to respond substantially to best practice standard care treatment after 2–4 weeks. An improvement in wound healing should be observed at least after 4 weeks of the adjunct haemoglobin application.49,50
Oxygen is required during all wound healing phases implying that this type of adjunctive therapy should be beneficial throughout all phases. The starting point of first application reported in clinical settings varies from the inflammatory phase to the epithelisation phase,42,48,51,52 while several authors describe the usage of haemoglobin until full wound closure.41,42,45,48,51,52
Hunt et al explicitly strengthened the necessity to treat until wound closure and not to premature treatment discontinuation before wound closure as they have observed a stagnation of healing and re-emergence of slough and pain in patients who stopped the adjunctive treatment too soon.52
As described above, the haemoglobin spray has been used in combination with various different dressings. Beyond administration of the spray, the haemoglobin spray is not expected to impact upon the standard wound care procedure. As haemoglobin is a protein which is vulnerable to degradation, limitations in compatibility with other therapies may arise by using products with proteolytic properties, low pH (<pH4) or other chemicals which denature or precipitate proteins.
Safety
None of the published clinical case reports or cohort studies using the haemoglobin spray reported spray-related severe adverse events. Within the study by Arenbergerova et al,39 safety was assessed as a secondary endpoint. One subject treated with the haemoglobin spray was admitted to hospital with liver disease. However, this was reported to be unrelated to treatment. Similarly, Arenberger et al37 reported that there were no undesirable treatment-related events within the study and the described case reports in different countries. A recent publication by Harnoss and colleagues evaluated the irritation potential of the product utilising the established hen’s egg model.53 The authors reported that the haemoglobin spray showed no irritation in the performed test, thus supporting the safety of the spray as suggested by the clinical testing.
As the haemoglobin is from porcine origin, there might be the potential for an allergic response in rare cases. So far, no such reports have been found in the literature. As the spray is applied topically, the risk of systemic absorption of large amounts of the protein is very minor.
In addition, one has to note, that the haemoglobin spray should not be used by patients who are pregnant as no data are available to assess the impact of the product within this group according to the Instruction for Use supplied with the product.
Health Economic Impact
A published economic evaluation of the clinical data suggested that Granulox® is likely to be effective and produce resource savings within NHS Scotland.54 The main evidence was based on the VLU RCT and three different cohort studies performed in the United Kingdom. The report noted that the strength of the cohort studies was in the number of patients in the adjunct treatment cohorts with an equal number of controls providing statistical power to detect clinically significant differences in outcomes. A significant medico-economic impact of adding haemoglobin spray to the standard wound care protocols in different settings was recognised, estimating a cost-saving to the UK healthcare system of an average of £2,330 for every diabetic foot ulcer patient and £1,469 for every chronic wound patient after six months.
However, the report noted several weaknesses of the VLU RCT and commented on the general limitations of the three cohort studies due to its observational design and the retrospective recruitment of controls. The promising results on the acceleration of wound healing and reduction of treatment costs are recognized but further data collection should provide more accurate and unbiased estimates of the relative effectiveness of the haemoglobin spray in a variety of healthcare settings.
A second health economic analysis was performed by a German group.55 The aim of this analysis was to explore the impact of the topical haemoglobin spray-on treatment costs from the perspective of the German statutory health insurance. The group applied a Markov model to the existing clinical data and performed sensitivity analyses to obtain robust data on the cost impact in patients with DFU. The group calculated approximately 40% lower costs for the treatment of DFUs by adding the haemoglobin spray to the treatment regimen. The authors concluded that, with the adjunctive treatment, a substantial cost reduction could be achieved from the perspective of the German statutory health insurance.
Discussion
In the recent literature, various reviews emphasise the adjunctive administration of oxygen as an important component of the modern management of chronic wounds.2,5,13
Additional systemic supply of oxygen by HBOT increases the amount of dissolved oxygen in the body, by which an improvement of wound healing can be achieved. As HBOT is not accessible to the majority of patients and has certain limitations due to diffusion and wound exudate/slough penetration constraints, local topical oxygen therapies may provide more accessible oxygen delivery systems.15,56
Currently, several local oxygen therapies are described. One class is the oxygen-releasing dressings. This approach utilizes the direct release of oxygen incorporated in the dressing after being in contact with the wound or indirect release via biochemical reactions. Only limited clinical data are available demonstrating a beneficial impact on wound healing.2,9
A second class is devices that deliver purified oxygen to the wound either by continuous perfusion without additional pressure or as small chambers with mild pressurized conditions.2,9
Clinical results from recently published RCTs for continuously57,58 as well as pressurised oxygen delivery devices59 indicate promising outcomes, especially in the treatment of diabetic foot ulcers. While the outcome of studies with continuous oxygen delivery devices suggest a major benefit to only older patients with chronic wounds,58 the results of the recently published study by Frykberg and colleagues using a pressurized oxygen delivery system demonstrated the beneficial impact on treating diabetic foot ulcers in a larger number of patients compared to a sham-treated control group.60 In both cases, the major focus was on treating healing refractory wounds.
Although it is known that oxygen penetrates the skin and contributes by diffusion to the overall oxygen delivery, the thickness of the skin is a barrier to oxygen diffusion to deeper layers in comparison to the situation in the lung.61 As wound exudate may increase the diffusion barrier, it makes it a significant challenge to ensure that additional atmospheric oxygen reaches deep into a wound.
Another approach to improve the oxygen status within the wound is to facilitate oxygen diffusion by using the properties of haemoglobin for oxygen uptake and offloading. It is proposed to apply the haemoglobin solution as adjunctive treatment to standard wound care of hypoxic chronic wounds to assist in adjusting oxygen levels and help to enhance wound healing. Currently, only one product is commercially available as a medical device, which provides the haemoglobin as a spray onto the wound.
The extensive literature search revealed one RCT describing the successful treatment of “hard to heal” venous leg ulcers with the adjunctive haemoglobin spray compared to a standard of care (SoC) group which failed. Several clinical case reports and observational studies describe improved healing for different wound types like diabetic foot ulcers, pressure ulcers or arterial ulcers as well as surgical wounds with healing disturbances and burns. These data may serve as the first guide to evaluating the potential of this treatment. Described to be useful in all healing phases, a consensus paper published by Chadwick et al might pilot the implementation of this treatment option in existing therapy concepts of chronic wounds when starting to explore the therapy49 (see Box 1).
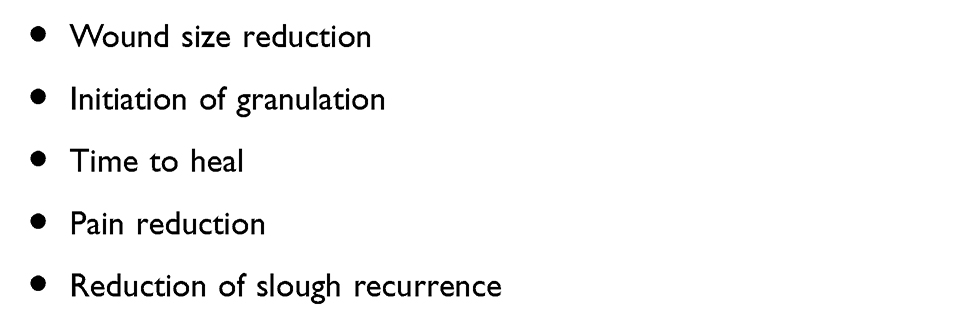 |
Box 1 Most Valuable Parameter to Explore in an Evaluation of Haemoglobin Spray Oxygen Therapy |
As mentioned by several authors the spray is easy to apply without the need of specific training or technical services like for pumps of devices delivering purified oxygen. One drawback might be that the product should be stored in a refrigerator to avoid damaging effects at high temperatures, which might not be available in all places.
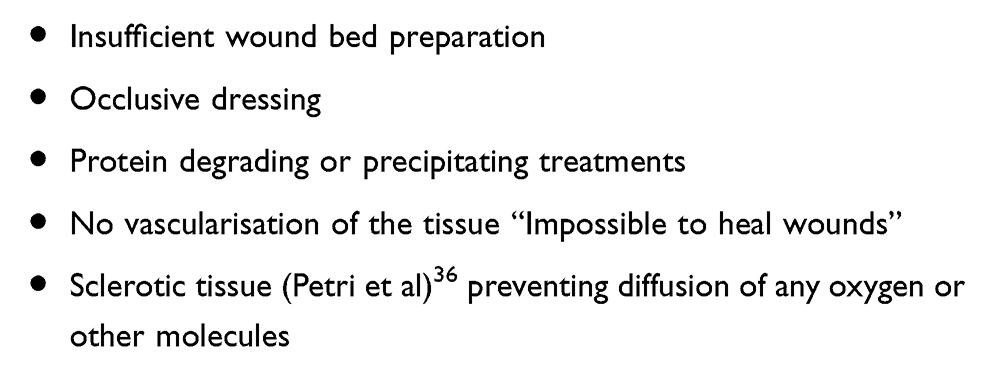 |
Box 2 Factors Which Might Negatively Influence the Outcome of Haemoglobin Spray Oxygen Therapy |
Available data on clinical studies and case reports raises the promise of being very useful to improve wound healing but highest level, distinct evidence for the usage of the haemoglobin spray in different wound types or healing phase remains to be published. However, some further well designed and controlled studies and further reports of clinical experiences in particular on wounds at risk may increase the level of evidence of the usefulness of the approach to facilitate oxygen diffusion in the wound (see Box 2).
During the last decade, an increasing number of controlled clinical studies and case reports showed that topical oxygen therapies as an adjunctive treatment option have the potential to improve wound healing of chronic wounds. The major focus of most of the studies was on DFUs. Historically, the HBO therapy was used for the treatment of DFUs, but the results were inconsistent.30 Local oxygen therapies on DFU seems to attract more attention as the results are promising. This applies to different approaches like the multimodality cyclical pressure oxygen delivery device, haemoglobin mediated oxygen delivery or continuous oxygen delivery devices.58,60,62 A benefit is the increasing accessibility of such mobile devices compared to the stationary HBO chambers.
As with all topical local oxygen therapies, an appropriate wound bed preparation is a prerequisite for the best results also with the haemoglobin mediated facilitated oxygen diffusion approach. Secondly, oxygen is required during the entire healing cascade at an increased demand.
The clinical results available for the different approaches are primarily obtained for DFU, leading to the question of which approach can be used for alternative types of wounds. Haemoglobin shows promising results from a VLU RCT,39 but for other types of wounds, the majority of results are based on cohort studies and case reports. At this stage, the different approaches require further exploration on pressure ulcers and other wounds to achieve a more comprehensive insight into the potential for oxygen therapies.
Considering the potential of facilitated oxygen diffusion via the applied haemoglobin and the other oxygen approaches it might be a reliable option to explore synergistic effects either by a combined treatment or sequential therapy eg after HBOT, to promote a beneficial impact on wound healing until wound closure.
Moreover, the broad clinical variation of wounds observed may direct the exploration of further new combinations as it might prove interesting to explore synergistic effects or combinations with products like growth factors or other biological molecules.
Conclusion
Purified haemoglobin applied on chronic wounds to facilitate oxygen diffusion is a recently introduced adjunct treatment option to accelerate wound healing. As there is only one product currently available, the clinical evidence is based solely on the results obtained from this product (Granulox®).
Current literature on the haemoglobin spray used as an adjunct in different wound types and clinical treatment regimens facilitates the usefulness of this therapy to improve wound healing and quality of life. This is applicable in treating venous leg ulcers and diabetic foot ulcers, and also in a broad spectrum of chronic wounds with similar levels of hypoxia such as pressure ulcers, surgical wounds with healing by secondary intention or burns.
The product is reported as “easy to use” as it can be applied as a thin liquid layer onto the wound bed before covering the wound with a “breathable” non-occlusive dressing.
Nevertheless, the use of this adjunctive topical oxygen treatment should be guided by factors like wound type, the experience of the clinician, cost-effectiveness and acceptability by the patient.
Disclosure
Knut Kröger reports they have been a member of the European Wound Management Association (EWMA) working group on Oxygen till 2017. The authors report no other conflicts of interest in this work.
References
1. Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv Wound Care (New Rochelle). 2015;4(9):560–582. doi:10.1089/wound.2015.0635
2. Gottrup F, Dissemond J, Baines C, et al. Use of oxygen therapies in wound healing. J Wound Care. 2017;26(Sup5):S1–s43. doi:10.12968/jowc.2017.26.Sup5.S1
3. Heyer K, Herberger K, Protz K, Glaeske G, Augustin M. Epidemiology of chronic wounds in Germany: analysis of statutory health insurance data. Wound Repair Regen. 2016;24(2):434–442. doi:10.1111/wrr.12387
4. Guest JF, Ayoub N, McIlwraith T, et al. Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open. 2015;5(12):e009283–e009283. doi:10.1136/bmjopen-2015-009283
5. Dissemond J, Assenheimer B, Engels P, et al. M.O.I.S.T. - a concept for the topical treatment of chronic wounds. J Dtsch Dermatol Ges. 2017;15(4):443–445.
6. Lazarus GS, Cooper DM, Knighton DR, et al. Definitions and guidelines for assessment of wounds and evaluation of healing. Arch Dermatol. 1994;130(4):489–493. doi:10.1001/archderm.1994.01690040093015
7. Hjort A, Gottrup F. Cost of wound treatment to increase significantly in Denmark over the next decade. J Wound Care. 2010;19(5):173–174, 176, 178, 180, 182, 184. doi:10.12968/jowc.2010.19.5.48046
8. Posnett J, Gottrup F, Lundgren H, Saal G. The resource impact of wounds on health-care providers in Europe. J Wound Care. 2009;18(4):154–161. doi:10.12968/jowc.2009.18.4.41607
9. Dissemond J, Kroger K, Storck M, Risse A, Engels P. Topical oxygen wound therapies for chronic wounds: a review. J Wound Care. 2015;24(2):
10. Guo S, Dipietro LA. Factors affecting wound healing. J Dent Res. 2010;89(3):219–229. doi:10.1177/0022034509359125
11. Hunt TK, Hopf H, Hussain Z. Physiology of wound healing. Adv Skin Wound Care. 2000;13(2 Suppl):6–11.
12. Schreml S, Szeimies RM, Prantl L, Karrer S, Landthaler M, Babilas P. Oxygen in acute and chronic wound healing. Br J Dermatol. 2010;163(2):257–268. doi:10.1111/bjd.2010.163.issue-2
13. Sen CK. Wound healing essentials: let there be oxygen. Wound Repair Regen. 2009;17(1):1–18. doi:10.1111/wrr.2009.17.issue-1
14. Rodriguez PG, Felix FN, Woodley DT, Shim EK. The role of oxygen in wound healing: a review of the literature. Dermatol Surg. 2008;34(9):1159–1169. doi:10.1111/j.1524-4725.2008.34254.x
15. Gottrup F. Oxygen in wound healing and infection. World J Surg. 2004;28(3):312–315. doi:10.1007/s00268-003-7398-5
16. Eisenbud DE. Oxygen in wound healing: nutrient, antibiotic, signaling molecule, and therapeutic agent. Clin Plast Surg. 2012;39(3):293–310. doi:10.1016/j.cps.2012.05.001
17. Ruthenborg RJ, Ban JJ, Wazir A, Takeda N, Kim JW. Regulation of wound healing and fibrosis by hypoxia and hypoxia-inducible factor-1. Mol Cells. 2014;37(9):637–643. doi:10.14348/molcells.2014.0150
18. Lokmic Z, Musyoka J, Hewitson TD, Darby IA. Hypoxia and hypoxia signaling in tissue repair and fibrosis. Int Rev Cell Mol Biol. 2012;296:139–185.
19. Nauta TD, van Hinsbergh VW, Koolwijk P. Hypoxic signaling during tissue repair and regenerative medicine. Int J Mol Sci. 2014;15(11):19791–19815. doi:10.3390/ijms151119791
20. Hong WX, Hu MS, Esquivel M, et al. The role of hypoxia-inducible factor in wound healing. Adv Wound Care. 2014;3(5):390–399. doi:10.1089/wound.2013.0520
21. LaVan FB, Hunt TK. Oxygen and wound healing. Clin Plast Surg. 1990;17(3):463–472.
22. Payen VL, Brisson L, Dewhirst MW, Sonveaux P. Common responses of tumors and wounds to hypoxia. Cancer J. 2015;21(2):75–87. doi:10.1097/PPO.0000000000000098
23. Flynn G. Cutaneous and trandermal delivery processes. In: Banker GS, Rhodes CT, editors. Modern Pharmaceutics.
24. Penneys R, Felder W, Christophers E. The passage of oxygen through isolated sheets of human stratum corneum. Proc Soc Exp Biol Med. 1968;127(4):1020–1022. doi:10.3181/00379727-127-32860
25. Piantadosi CA. Physiology of hyperbaric hyperoxia. Respir Care Clin N Am. 1999;5(1):7–19, v.
26. Roe DF, Gibbins BL, Ladizinsky DA. Topical dissolved oxygen penetrates skin: model and method. J Surg Res. 2010;159(1):e29–e36. doi:10.1016/j.jss.2009.10.039
27. Fitzgerald LR. Cutaneous respiration in man. Physiol Rev. 1957;37(3):325–336. doi:10.1152/physrev.1957.37.3.325
28. Ayello EA, Dowsett C, Schultz GS, et al. TIME heals all wounds. Nursing. 2004;34(4):
29. Gordillo GM, Schlanger R, Wallace WA, Bergdall V, Bartlett R, Sen CK. Protocols for topical and systemic oxygen treatments in wound healing. Methods Enzymol. 2004;381:575–585.
30. Kranke P, Bennett MH, Martyn-St James M, Schnabel A, Debus SE, Weibel S. Hyperbaric oxygen therapy for chronic wounds. Cochrane Database Syst Rev. 2015;(6):CD004123.
31. Gordillo GM, Sen CK. Evidence-based recommendations for the use of topical oxygen therapy in the treatment of lower extremity wounds. Int J Low Extrem Wounds. 2009;8(2):105–111. doi:10.1177/1534734609335149
32. Barnikol WKR, Teslenko A, Pötzschke H. Eine neue topische Behandlung chronischer Wunden mit Hämoglobin und Sauerstoff: verfahren und erste Ergebnisse. ZfW. 2005;13(3):98–108.
33. Scholander PF. Oxygen transport through hemoglobin solutions. Science. 1960;131(3400):585–590. doi:10.1126/science.131.3400.585
34. Wittenberg JB. The molecular mechanism of hemoglobin-facilitated oxygen diffusion. J Biol Chem. 1966;241(1):104–114.
35. Petri M, Stoffels I, Jose J, et al. Photoacoustic imaging of real-time oxygen changes in chronic leg ulcers after topical application of a haemoglobin spray: a pilot study. J Wound Care. 2016;25(2):87,89–91. doi:10.12968/jowc.2016.25.2.87
36. Petri M, Stoffels I, Griewank K, et al. Oxygenation status in chronic leg ulcer after topical hemoglobin application may act as a surrogate marker to find the best treatment strategy and to avoid ineffective conservative long-term therapy. Mol Imaging Biol. 2018;20(1):124–130. doi:10.1007/s11307-017-1103-9
37. Arenberger P, Engels P, Arenbergerova M, et al. Clinical results of the application of a hemoglobin spray to promote healing of chronic wounds. GMS Krankenhhyg Interdiszip. 2011;6(1):Doc05.
38. Barnikol WK, Potzschke H. Complete healing of chronic wounds of a lower leg with haemoglobin spray and regeneration of an accompanying severe dermatoliposclerosis with intermittent normobaric oxygen inhalation (INBOI): a case report. Ger Med Scie. 2011;9.
39. Arenbergerova M, Engels P, Gkalpakiotis S, Dubska Z, Arenberger P. [Topical hemoglobin promotes wound healing of patients with venous leg ulcers]. Hautarzt. 2013;64(3):180–186. doi:10.1007/s00105-012-2528-3
40. Norris R. A topical haemoglobin spray for oxygenating chronic venous leg ulcers: a pilot study. Br J Nurs. 2014;23(Suppl 20):S48–S53. doi:10.12968/bjon.2014.23.Sup20.S48
41. Babadagi-Hardt Z, Engels P, Kanya S. Wound management with compression therapy and topical hemoglobin solution in a patient with Budd-Chiari Syndrome. J Dermatol Case Rep. 2014;8(1):20–23. doi:10.3315/jdcr.2014.1165
42. Hunt S, Elg F. The clinical effectiveness of haemoglobin spray as adjunctive therapy in the treatment of chronic wounds. J Wound Care. 2017;26(9):558–568. doi:10.12968/jowc.2017.26.9.558
43. Chammas NK, Hill RL, Edmonds ME. Increased mortality in diabetic foot ulcer patients: the significance of ulcer type. J Diabetes Res. 2016;2016:2879809. doi:10.1155/2016/2879809
44. Tickle J. A topical haemoglobin spray for oxygenating pressure ulcers: a pilot study. Br J Community Nurs. 2015;Suppl Wound Care:S12,S14–18.
45. Tickle J, Bateman SD. Use of a topical haemoglobin spray for oxygenating pressure ulcers: healing outcomes. Br J Community Nurs. 2015;20(Suppl 12):S14–S21. doi:10.12968/bjcn.2015.20.Sup12.S14
46. Sibbald RG, Williamson D, Orsted HL, et al. Preparing the wound bed–debridement, bacterial balance, and moisture balance. Ostomy Wound Manage. 2000;46(11):
47. Sibbald RG, Woo KY, Queen D. Wound bed preparation and oxygen balance–a new component? Int Wound J. 2007;4(Suppl 3):9–17. doi:10.1111/j.1742-481X.2007.00388.x
48. Mustafi N, Engels P. Post-surgical wound management of pilonidal cysts with a haemoglobin spray: a case series. J Wound Care. 2016;25(4):
49. Chadwick PM, Mccardle J, Mohamud L, Tickle J, Vowden K, Vowden P. Appropriate use of topical haemoglobin in chronic wound management: consensus recommendations. Wounds UK. 2015;EWMA Special:30–35.
50. Strohal RGV, Kröger K, Kurz P, et al. Expert consensus to practical aspects of wound therapy with hemoglobin spray. Wund Manag. 2016;5(10):276–284.
51. Hunt SD, Elg F. Clinical effectiveness of hemoglobin spray (Granulox(®)) as adjunctive therapy in the treatment of chronic diabetic foot ulcers. Diabet Foot Ankle. 2016;7. doi:10.3402/dfa.v3407.33101.
52. Hunt S, Elg F. Assessment of clinical effectiveness of haemoglobin spray as adjunctive therapy in the treatment of sloughy wounds. J Wound Care. 2018;27:210–219. doi:10.12968/jowc.2018.27.4.210
53. Harnoss JC, Elrub QMA, Jung JO, et al. Irritative potency of selected wound antiseptics in the hen’s egg test on chorioallantoic membrane to predict their compatibility to wounds. Wound Repair Regen. 2019;27(2):183–189. doi:10.1111/wrr.12689
54. 006/2016 IMTON. Granulox® haemoglobin spray; 2016. Available from: http://www.healthcareimprovementscotland.org/our_work/technologies_and_medicines/shtg_imto/imto_006-2016aspx.
55. Brüggenjürgen B, Hunt SD, Eberlein T. Wundversorgung des diabetischen Fuß-Ulkus (DFU) – inkrementelle Kostenanalyse der mit einem Hämoglobinspray erweiterten Therapie der diabetisch-neuropathischen Fußläsion in Deutschland. Gesundh Ökon Qual Manag. 2018;23(06):320–327. doi:10.1055/s-0043-120204
56. Thom SR. Hyperbaric oxygen: its mechanisms and efficacy. Plast Reconstr Surg. 2011;127 Suppl 1:131s–141s. doi:10.1097/PRS.0b013e3181fbe2bf
57. Yu J, Lu S, McLaren AM, Perry JA, Cross KM. Topical oxygen therapy results in complete wound healing in diabetic foot ulcers. Wound Repair Regen. 2016;24(6):1066–1072. doi:10.1111/wrr.12490
58. Driver VR, Reyzelman A, Kawalec J, French M, Prospective A, Randomized B. Controlled trial comparing transdermal continuous oxygen delivery to moist wound therapy for the treatment of diabetic foot ulcers. Ostomy Wound Manage. 2017;63(4):12–28.
59. Blackman E, Moore C, Hyatt J, Railton R, Frye C. Topical wound oxygen therapy in the treatment of severe diabetic foot ulcers: a prospective controlled study. Ostomy Wound Manage. 2010;56(6):24–31.
60. Frykberg RG, Franks PJ, Edmonds M, et al. A multinational, multicenter, randomized, double-blinded, placebo-controlled trial to evaluate the efficacy of cyclical topical wound oxygen therapy (TWO2) in the treatment of chronic diabetic foot ulcers: the TWO2 Study. Diabetes Care. 2019.
61. Ladizinsky D, Roe D. New insights into oxygen therapy for wound healing. Wounds. 2010;22(12):294–300.
62. Hayes PD, Alzuhir N, Curran G, Loftus IM. Topical oxygen therapy promotes the healing of chronic diabetic foot ulcers: a pilot study. J Wound Care. 2017;26(11):652–660. doi:10.12968/jowc.2017.26.11.652
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.