Back to Journals » Patient Preference and Adherence » Volume 14
Assessing Knowledge and Perceptions of Alzheimer’s Disease Among Employees of a Pharmaceutical Company in Spain: A Comparison Between Caregivers and Non-Caregivers
Authors Garcia-Ribas G, García-Arcelay E, Montoya A, Maurino J ![]()
Received 18 September 2020
Accepted for publication 12 November 2020
Published 1 December 2020 Volume 2020:14 Pages 2357—2364
DOI https://doi.org/10.2147/PPA.S282147
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Guillermo Garcia-Ribas,1 Elena García-Arcelay,2 Alonso Montoya,3 Jorge Maurino2
1Department of Neurology, Hospital Universitario Ramón y Cajal, Madrid, Spain; 2Medical Department, Roche Farma, Madrid, Spain; 3Medical Affairs, Neuroscience, Hoffmann-La Roche Limited, Mississauga, ON, Canada
Correspondence: Elena García-Arcelay
Roche Farma, Ribera del Loira, 50, Madrid 28042, Spain
Tel +34 91 324 81 00
Email [email protected]
Background: Raising knowledge about Alzheimer’s disease (AD) may help in identifying the disorder, seeking earlier appropriate healthcare, and decreasing its stigma. The aim of this study was to determine the knowledge and perceptions towards people with AD among employees of a pharmaceutical company in Spain.
Methods: A non-interventional, cross-sectional study was conducted among 447 employees. Participants answered demographic questions and completed the Alzheimer’s Disease Knowledge Scale (ADKS). Caregivers also answered questions related to their personal experience with patients with AD and completed the Satisfaction with Life Scale (SWLS), the Revised Memory and Behavior Problems Checklist (RMBPC), and the Beck Depression Inventory-Fast Screen (BDI-FS).
Results: Participants were mostly between 30 and 50 years old (63%), female (65.3%), and had bachelor or master degrees (82.7%). Forty-two (9.4%) of participants were caregivers, mainly of moderate to severe dementia subjects. Overall knowledge about AD was moderate (mean ADKS score = 21.2 ± 2.8 [70.6% of correct answers]). Risk factors and caregiving were the domains with lowest scores (correct answers: 58.58% and 63%, respectively). Mean total ADKS score was significantly higher in participants caring for people with AD compared with non-caregivers (22.1 ± 2.9 and 21.0 ± 2.8; p=0.02, respectively). There was no statistically significant association between total ADKS score and age, sex, educational level, or relative’s AD severity. Most caregivers were satisfied with life (mean SWLS score = 26.8 ± 5.6) showing a low impact from behavioral problems (mean RMBPC reaction score = 26.81 ± 20.2). Six of them (14.3%) were scored as depressed.
Conclusion: There is a continuing need to improve understanding of AD to fill the gaps in knowledge of the disease, even in a population working in healthcare sector with a high educational level.
Keywords: Alzheimer’s disease, dementia, knowledge, pharmaceutical company, caregivers
Introduction
Global population growth leads to a progressive increase in the number of older people. One in four persons living in Europe and Northern America could be aged 65 or over in 2050.1 The number of persons aged 80 years or over is projected to triple, from 143 million in 2019 to 426 million in 2050.1 In this context, it is expected that the burden of chronic neurodegenerative disorders, particularly dementia, will grow exponentially becoming a major public health concern.2,3
Alzheimer’s disease (AD) is the most prevalent type of dementia and is characterized by a progressive decline in cognitive function and an overall deterioration in function leading to a considerable burden on the individual and society.4 An adequate public knowledge of AD may help in identifying the disorder, seeking earlier appropriate healthcare and decreasing its stigma, while also opening a better informed debate about the needs of affected individuals.5,6 Unfortunately, although information about AD has been widely disseminated through numerous awareness campaigns and education programs, previous studies measuring the public’s knowledge about dementia and AD have revealed several gaps in this regard.7–10 The most common misconception is that dementia is a normal part of aging and there is a lack of clarity about the point at which normal age-related memory loss problems become severe enough to indicate dementia.7
The negative perceptions and attitudes toward AD are also harmful for their family and caregivers. Employees who simultaneously serve as an informal caregiver of disabled or elderly relatives have higher levels of home-to-work difficulties, depression, emotional exhaustion, and lower levels of job engagement compared with non-caregiver-employees.11 Over 75% of caregivers of people with AD show stress or anxiety and are more likely to develop psychological and physical disorders, social isolation, and poorer self-perceived health more frequently than the general population or age-matched controls.12,13 The latest Alzheimer’s Disease International report on stigma found that 35% of caregivers across the world had hidden the diagnosis of dementia of a family member and over 50% reported their health suffering as a result of their caring responsibilities even while expressing positive sentiments about their role.14
Limited studies have assessed the knowledge and perceptions towards people affected by AD in the workforce where many employees are balancing their careers with caregiving responsibilities.7,15 The main aim of this study was to assess levels of knowledge and perceptions about AD among employees of a pharmaceutical company. Life satisfaction, impact of memory and behavioral problems, and mood were evaluated in those participants caring for relatives with AD. In addition, comparison of AD knowledge between caregivers and non-caregivers was analyzed.
Methods
A non-interventional, cross-sectional web-based study was conducted (CONOCE study). The study was approved by the investigational review board of the Hospital Universitario Ramón y Cajal of Madrid (reference code: 372) and conformed with the Helsinki Declaration of 1964, as revised in 2013, concerning human and animal rights.
Population
All employees (2376) of a pharmaceutical company in Spain (Roche Diagnostics, Roche Diabetes Care Spain SL, Roche Farma S.A. and Global Infrastructure & Solutions Madrid) were invited to participate in this study in the context of the 2019 World Alzheimer’s Day. This company has been involved in the clinical development of several molecules for the treatment of AD for the last decade. Recruitment was opened between December 2, 2019 and February 3, 2020. Informed consent was obtained from all subjects.
Procedure and Measurements
Participants answered questions regarding demographic data and completed the 30-item Alzheimer’s Disease Knowledge Scale (ADKS).16 Those participants with a first-degree relative affected with AD also answered six questions about caregiving (type of relationship, time to diagnosis, healthcare professional who made diagnosis, severity, impact, and time devoted to care) and completed the Satisfaction with Life Scale (SWLS),17 the Revised Memory and Behavior Problems Checklist (RMBPC),18 and the Beck Depression Inventory-Fast Screen (BDI-FS).19
The ADKS belongs to a group of psychometric scales aiming to assess knowledge about AD to help to develop psychoeducational curricula and interventions for dementia care.16,20 It consists of 30 true or false items to assess what people know about AD covering risk factors, symptoms, assessment and diagnosis, life impact, treatment and management, caregiving, and disease course.16 The total score ranges from 0 (worst) to 30 (best). Despite some criticisms linked to dichotomous item assessment, reverse scored items, and a likely ceiling effect for some items, the ADKS is currently one of the few questionnaires with adequate psychometric properties for assessing AD knowledge among laypeople, patients, caregivers, and professionals.20,21 The SWLS is a five-item scale designed to measure global cognitive judgments of one’s life satisfaction.17 Participants indicate how much they agree or disagree with each item using a seven-point scale that ranges from strongly agree to strongly disagree. Scores between 5 and 9 indicate the respondent is extremely dissatisfied with life, whereas scores between 31 and 35 indicate the respondent is extremely satisfied. The RMBPC is a 24-item caregiver-report measure to assess behavioral problems in patients with dementia including memory-related problems, affective distress, and disruptive behaviors.18 Scores are computed for the presence or absence of each problem first, and then for caregiver “reaction” or the extent to which caregivers were “distressed” by each behavior. Frequency of behaviors is assessed based on a Likert-scale of 0 to 4 (never occurs to occurs daily or more often). The caregivers’ reactions to each behavior are also scored on a four-point scale (not at all to extremely). Higher scores indicate higher levels of perceived caregiver burden. The BDI-FS is a seven-item questionnaire assessing the level of depressive symptoms.19 Responses to the items are provided on a four-point scale (no symptoms to severe symptoms). Total score ranges from 0 to 21, with higher scores indicating greater severity of depressive symptoms. Cut-off scores ≥4 and ≥9 are used to define the presence of depression and moderate-to-severe depression, respectively. All questionnaires were administered in Spanish and English.
Statistical Analyses
Sociodemographic characteristics and total scores on the scales (i.e., ADKS, SWLS, RMBPC and BDI-FS) are expressed as mean and standard deviation. Descriptive analyses were performed using frequencies and percentages for qualitative variables. Student’s t-test was used to compare the ADKS score between two groups or ANOVA in the case of three or more groups. Missing data were not considered in the analyses and a significance level of 0.05 was used for statistical testing. The SPSS statistical package version 22 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis.
Results
Study Participants
Four hundred forty-seven subjects participated in the study. Most participants were between 30 and 50 years old (63.3%), female (65.3%), and had a bachelor’s or master’s degree (82.7%). Sociodemographic characteristics of the sample are shown in Table 1.
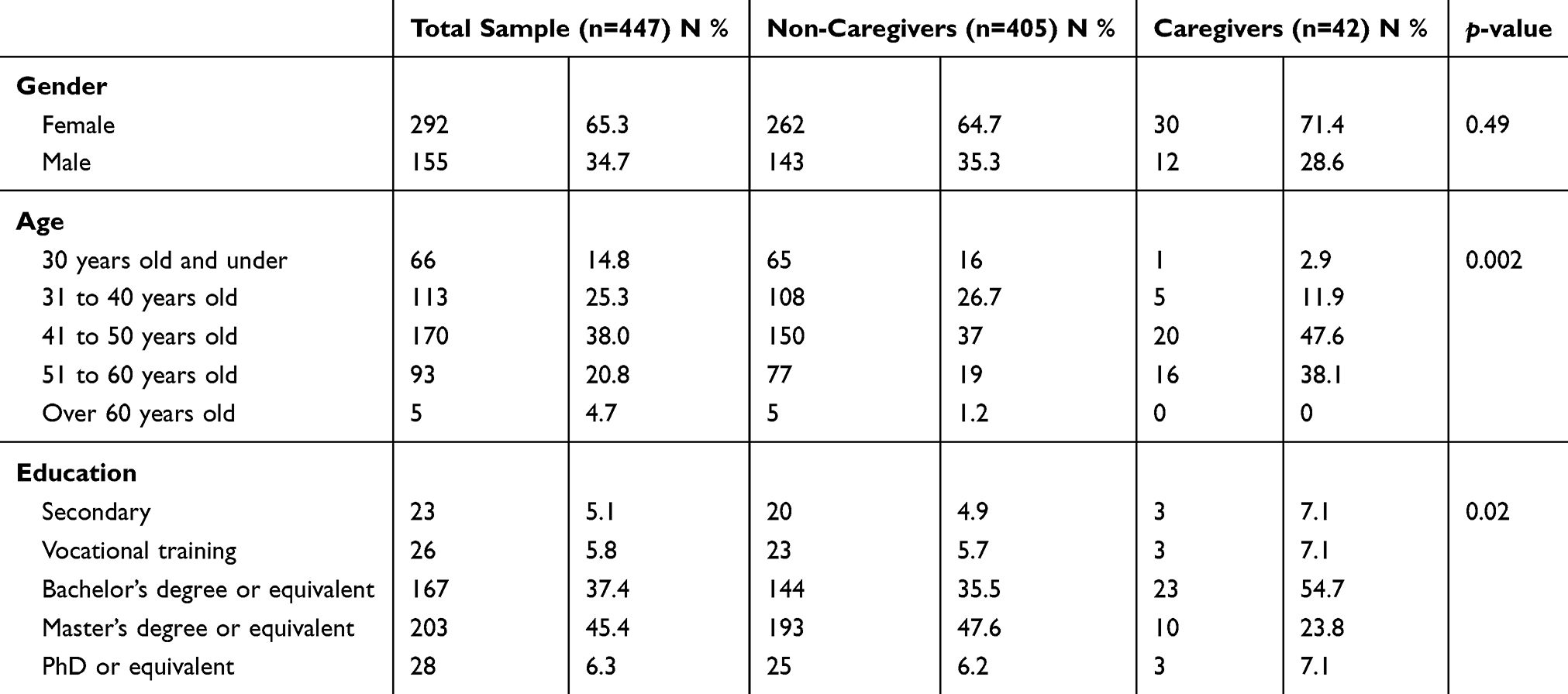 |
Table 1 Sociodemographic Characteristics of the Sample |
Forty-two (9.4%) participants reported having a first-degree relative with AD, with the mother being the most frequent relative affected (40%). Most of them (66.7%) reported that informal caregiving activities did not or partially affected their social life or work with less than 10 hours per week providing assistance. Background and experience with people with AD are shown in Table 2.
 |
Table 2 Background and Impact of Caregivers (N=42) |
Knowledge About AD
The overall mean score of dementia knowledge as measured by the ADKS was 21.2 ± 2.8 out of 30 (70.5% correct). Participants scored particularly high in the ADKS domains of treatment management and life impact (Table 3). Knowledge about risk factors and caregiving were the domains with the lowest scores (58.6 and 63% of correct answers, respectively).
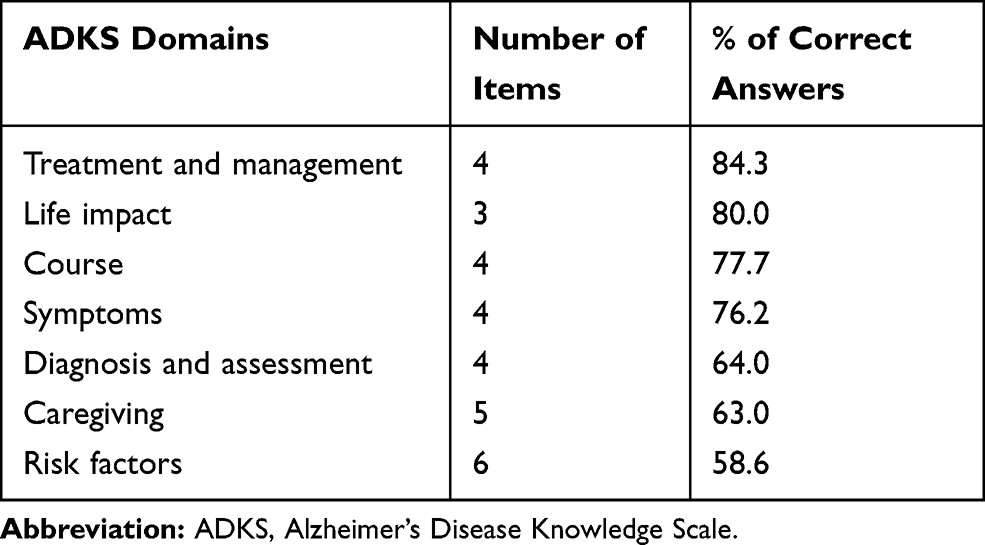 |
Table 3 Content Domains of the Alzheimer’s Disease Knowledge Scale (n=447) |
Mean total ADKS score was significantly higher in participants caring for people with AD compared with non-caregivers (22.1 ± 2.9 and 21.0 ± 2.8; p=0.02, respectively). Caregivers showed a better AD knowledge in 20 of the 30 items of the ADKS than non-caregivers, mainly in symptoms, assessment and diagnosis, and course domains (Table 4). There was no statistically significant association between total ADKS score and age, sex, educational level, or relative’s AD severity.
 |
Table 4 Alzheimer’s Disease Knowledge Scale: Comparison of Correct Answers Between AD Caregivers and Non-Caregivers |
Most of the caregivers (73.8%) reported a high level of satisfaction with their current life. The mean SWLS score was 26.8 ± 5.6. Memory impairment was the most common behavioral problem. However, depression-related problem was the most distressful behavior among caregivers (Table 5). The mean BDI-FS score was low (1.6 ± 2.6). However, six caregivers (14%) were scored as depressed. Most were aged between 30 and 50, female and had a relative with severe AD. No correlation was found between the presence of depressive symptoms and relative’s AD severity (ANOVA p=0.83).
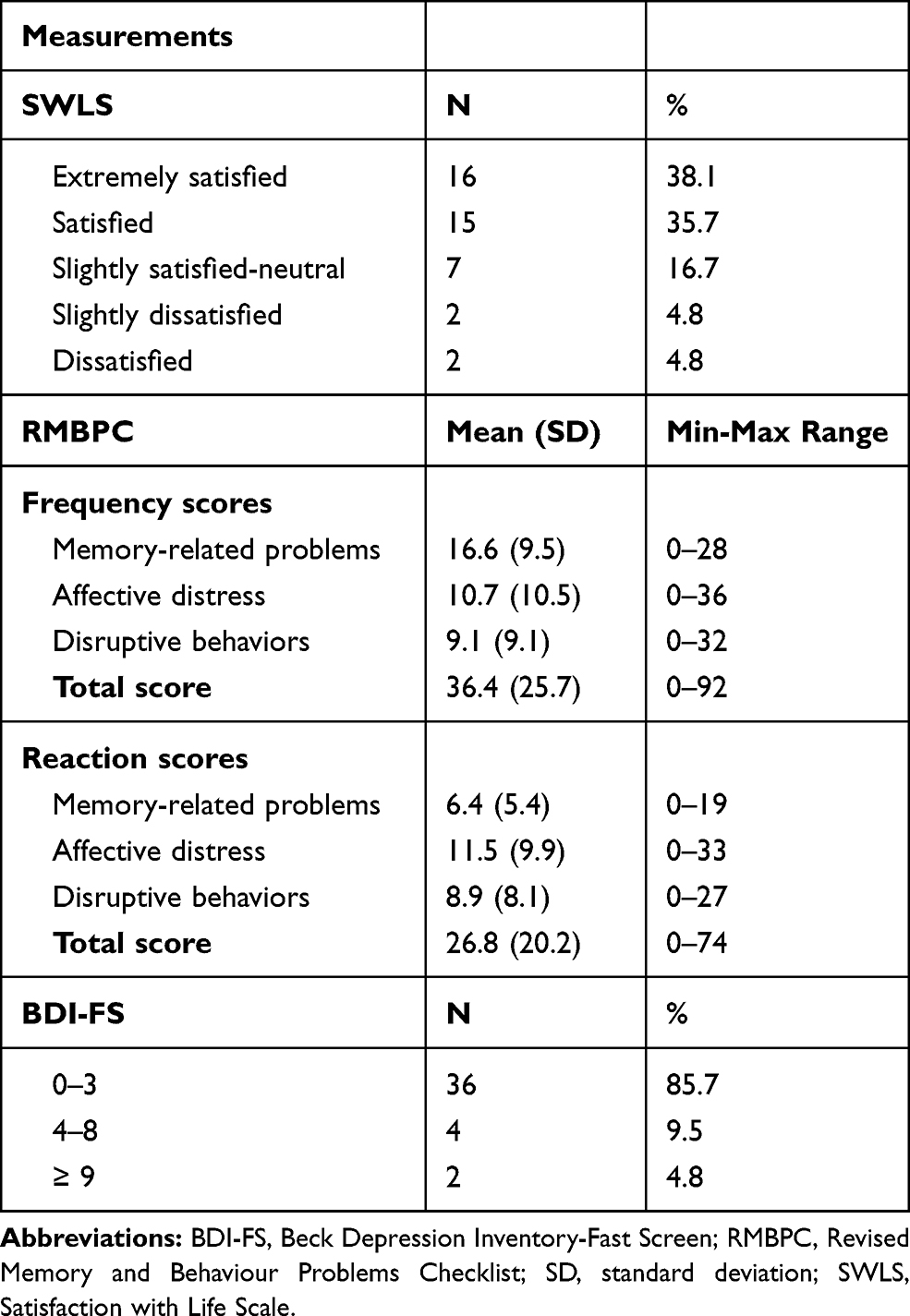 |
Table 5 Satisfaction with Life, Impact of Memory and Behavioral Problems, and Mood in Participants Caring for People with Alzheimer’s Disease |
Discussion
This study assessed knowledge of AD in a sample of people with a predominately high educational level working in a pharmaceutical company in Spain. Despite generally good knowledge, risk factors and prevention of AD were noteworthy gaps. Our results are consistent with previous studies7,22–24 In a systematic review of 40 studies addressing the public’s knowledge of AD, Cahill et al found a poor to very limited level of AD literacy.7 The most common correlates of knowledge investigated were age, sex, and education. Higher levels of knowledge were found among younger persons, women, and better educated people. Risk factors and prevention were the knowledge domains with the most common identified gaps.7 Jorge et al found a poor knowledge of AD in a sample of 215 informal caregivers and 204 individuals from the general population in Spain.22 Questions related to risk factors and caregiving had the highest rate of errors. Krempel-Amado et al found a moderate knowledge of AD in a survey including 1414 people in Brazil (mean ADKS score = 21.6).23 The scores were positively influenced by educational level, professional skills (better for health professionals, mainly physicians) and by age (younger than 65 years). Healthcare professionals also show knowledge gaps about AD, with risk factors and disease course being the most frequent identified gaps.23
Caring for someone with dementia is a complex, multi-disciplinary task requiring the involvement of families, healthcare professionals, and social services and generates higher levels of stress and anxiety than caring for patients with other chronic disabling diseases.25,26 In our study, a total of 42 (9.4%) participants reported being informal caregivers of first-degree relatives with AD. They showed a better knowledge of AD compared with non-caregivers as measured by the ADKS. Interestingly, different findings were reported in the literature. Jorge et al did not find significant differences between caregivers and non-caregivers for overall mean ADKS score (19.2 vs. 18.9, respectively; p=0.97).22 Being a caregiver or family member also did not influence knowledge about the disease in a study conducted in Brazil.23 Older adults and caregivers knew less than healthcare professionals but were more knowledgeable than senior center staff and undergraduate students in a study involving 794 people in the UK.24
While research has not yet discovered disease-modifying agents in AD, there is a robust evidence about the potential to prevent cases of dementia with early management of risk factors such as hypertension, hypercholesterolemia, high body mass index, or diabetes.27–29 However, knowledge about the potential for dementia prevention and treatment is poor.30,31 Nearly half of respondents agreed that dementia is a normal part of aging and is not preventable in a recent systematic review of 34 studies conducted predominantly in Europe and the US.31 The role of cardiovascular risk factors was poorly understood overall.
Because the risk of getting dementia increases with age, people living with dementia are likely to experience a “double stigma”.14 Information and knowledge about AD are needed because the ignorance around dementia results in discrimination, loss of rights and perpetuates negative beliefs towards those affected by the disease.14,31
This study has several limitations. First, there is self-selection bias in participants and it is possible that the most motivated or more knowledgeable respondents about AD may have completed the survey. Second, no questionnaires on dementia knowledge have been developed or culturally adapted into Spanish-speaking countries. Therefore, we had to use a non-validated Spanish version of the ADKS. In addition, this scale lacks a cut-off for the minimum acceptable level of knowledge. Third, it is also likely that many people mixed the terms AD and dementia. Finally, carrying out the study in only one pharmaceutical company may limit the generalizability of the findings to other healthcare communities or even the general population. Despite these limitations, our study shows a valuable sample of participants with a wide spectrum of age, level of education, and experience in caregiving people with AD.
Conclusion
Misconceptions about AD in the general population have been present for many years. This study assessed the knowledge and perceptions about AD from the caregiver and non-caregiver perspectives in the workplace. Understanding the modifiable risk factors for AD may encourage early preventative health behaviors and ultimately reduce late-life incidence and its associated costs. Therefore, there is a critical need for more public health campaigns to fill knowledge gaps even in young populations with a high educational level.
Data Sharing Statement
Qualified researchers may request access to individual patient level data through the clinical study data request platform (https://vivli.org/). Further details on Roche’s criteria for eligible studies are available here (https://vivli.org/members/ourmembers/). For further details on Roche’s Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see here (https://www.roche.com/research_and_development/who_we_are_how_we_work/clinical_trials/our_commitment_to_data_sharing.htm).
Acknowledgments
This study was funded by Roche Farma Spain Medical Department. The authors would like to acknowledge all Roche employees that took their time to complete the survey. We also thank Mónica Palomanes, Beatriz Pérez, Luis Manuel González, Beatriz Lozano, and Stefanos Tsamousis (Roche Spain ConnecTeam) for their support and commitment to the success of this project. The abstract of this paper was presented at the 30th Virtual Alzheimer Europe Conference as a poster presentation with interim findings (PO 3.8; October 20, 2020).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
EG-A and JM are employees of Roche Farma Spain. AM is an employee of Hoffmann-La Roche Limited, Canada. The authors report no other conflicts of interest in this work.
References
1. United Nations. 2019 revision of world population prospects. Available from: https://population.un.org/wpp/.
2. Wimo A, Guerchet M, Ali GC, et al. The worldwide costs of dementia 2015 and comparisons with 2010. Alzheimers Dement. 2017;13(1):1–7. doi:10.1016/j.jalz.2016.07.150
3. Nichols E, Szoeke CEI, Vollset SE, GBD. Global, regional, and national burden of alzheimer’s disease and other dementias, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(1):88–106. doi:10.1016/S1474-4422(18)30403-4
4. Kumfor F, Halliday GM, Piguet O. Clinical aspects of alzheimer’s disease. Adv Neurobiol. 2017;15:31–53. doi:10.1007/978-3-319-57193-5_2
5. Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet. 2017;390(10113):2673–2734. doi:10.1016/S0140-6736(17)31363-6
6. Werner P, AboJabel H, Maxfield M. Conceptualization, measurement and correlates of dementia worry: a scoping review. Arch Gerontol Geriatr. 2021;92:104246. doi:10.1016/j.archger.2020.104246
7. Cahill S, Pierce M, Werner P, Darley A, Bobersky A. A systematic review of the public’s knowledge and understanding of alzheimer’s disease and dementia. Alzheimer Dis Assoc Disord. 2015;29(3):255–275. doi:10.1097/WAD.0000000000000102
8. Farina N, Suemoto CK, Burton JK, Oliveira D, Frost R. Perceptions of dementia amongst the general public across Latin America: a systematic review. Aging Ment Health. 2020;1–10. doi:10.1080/13607863.2020.1725738
9. Smith BJ, Ali S, Quach H. Public knowledge and beliefs about dementia risk reduction: a national survey of Australians. BMC Public Health. 2014;14:661. doi:10.1186/1471-2458-14-661
10. Shinan-Altman S, Werner P. Illness representations of dementia: a scoping review. Clin Interv Aging. 2019;14:179–193. doi:10.2147/CIA.S193316
11. Converso D, Sottimano I, Viotti S, Guidetti G. I’ll be a caregiver-employee: aging of the workforce and family-to-work conflicts. Front Psychol. 2020;11:246. doi:10.3389/fpsyg.2020.00246
12. Blendon RJ, Benson JM, Wikler EM, et al. The impact of experience with a family member with Alzheimer’s disease on views about the disease across five countries. Int J Alzheimers Dis. 2012;903645. doi:10.1155/2012/903645
13. Macdonald M, Martin-Misener R, Weeks L, Helwig M, Moody E, MacLean H. Experiences and perceptions of spousal/partner caregivers providing care for community-dwelling adults with dementia: a qualitative systematic review. JBI Database System Rev Implement Rep. 2019. doi:10.11124/JBISRIR-2017-003774
14. Alzheimer’s Disease International. World Alzheimer Report 2019: Attitudes to Dementia. London; 2019. Available from: https://www.alz.co.uk/research/WorldAlzheimerReport2019.pdf.
15. Allen TD, Martin A. The work-family interface: a retrospective look at 20 years of research in JOHP. J Occup Health Psychol. 2017;22(3):259–272. doi:10.1037/ocp0000065
16. Carpenter BD, Balsis S, Otilingam PG, Hanson PK, Gatz M. The alzheimer’s disease knowledge scale: development and psychometric properties. Gerontologist. 2009;49(2):236–247. doi:10.1093/geront/gnp023
17. Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale and the emerging construct of life satisfaction. J Posit Psychol. 2008;3(2):137–152. doi:10.1080/17439760701756946
18. Teri L, Truax P, Logsdon R, Uomoto J, Zarit S, Vitaliano PP. Assessment of behavioral problems in dementia: the revised memory and behavior problems checklist. Psychol Aging. 1992;7(4):622–631. doi:10.1037//0882-7974.7.4.622
19. Beck AT, Steer RA, Brown GK. BDI-II Fast Screen for Medical Patients, Manual. San Antonio, Texas: The Psychological Corporation, A Harcourt Assessment Company; 2000.
20. Spector A, Orrell M, Schepers A, Shanahan N. A systematic review of ‘knowledge of dementia’ outcome measures. Ageing Res Rev. 2012;11(1):67–77. doi:10.1016/j.arr.2011.09.002
21. Sullivan KA, Mullan MA. Comparison of the psychometric properties of four dementia knowledge measures: which test should be used with dementia care staff? Australas J Ageing. 2017;36(1):38–45. doi:10.1111/ajag.12299
22. Jorge C, Cetó M, Arias A, et al. Level of understanding of alzheimer disease among caregivers and the general population. Neurologia. 2018;11:S0213–S4853. doi:10.1016/j.nrl.2018.03.004
23. Krempel-Amado D, Brucki SMD. Knowledge about alzheimer’s disease in the Brazilian population. Arq Neuropsiquiatr. 2018;76(11):775–782. doi:10.1590/0004-282X20180106
24. Carpenter BD, Zoller SM, Balsis S, Otilingam PG, Gatz M. Demographic and contextual factors related to knowledge about alzheimer’s disease. Am J Alzheimers Dis Other Dem. 2011;26(2):121–126. doi:10.1177/1533317510394157
25. Queluz FNFR, Kervin E, Wozney L, Fancey P, McGrath PJ, Keefe J. Understanding the needs of caregivers of persons with dementia: a scoping review. Int Psychogeriatr. 2020;32(1):35–52. doi:10.1017/S1041610219000243
26. Kokorelias KM, Gignac MAM, Naglie G, et al. A grounded theory study to identify caregiving phases and support needs across the alzheimer’s disease trajectory [published online ahead of print, 2020 Jul 20]. Disabil Rehabil. 2020;1–10. doi:10.1080/09638288.2020.1788655
27. Yu JT, Xu W, Tan CC, et al. Evidence-based prevention of alzheimer’s disease: systematic review and meta-analysis of 243 observational prospective studies and 153 randomised controlled trials. J Neurol Neurosurg Psychiatry. 2020. doi:10.1136/jnnp-2019-321913
28. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet. 2020;396(10248):413–446. doi:10.1016/S0140-6736(20)30367-6
29. Alacreu M, Pardo J, Azorín M, Climent MT, Gasull V, Moreno L. Importance of increasing modifiable risk factors knowledge on alzheimer’s disease among community pharmacists and general practitioners in Spain. Front Pharmacol. 2019;10:860. doi:10.3389/fphar.2019.00860
30. Rosenberg A, Coley N, Soulier A, et al., MIND-AD and HATICE groups. Experiences of dementia and attitude towards prevention: a qualitative study among older adults participating in a prevention trial. BMC Geriatr. 2020;20(1):99. doi:10.1186/s12877-020-1493-4
31. Cations M, Radisic G, Crotty M, Laver KE, Werner P. What does the general public understand about prevention and treatment of dementia? A systematic review of population-based surveys. PLoS One. 2018;13(4):e0196085. doi:10.1371/journal.pone.0196085
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.