Back to Journals » Risk Management and Healthcare Policy » Volume 14
Assessing Drug Consumption Rooms and Longer Term (5 Year) Impacts on Community and Clients
Authors Tran V ![]() , Reid SE, Roxburgh A
, Reid SE, Roxburgh A ![]() , Day CA
, Day CA ![]()
Received 26 July 2021
Accepted for publication 30 October 2021
Published 15 November 2021 Volume 2021:14 Pages 4639—4647
DOI https://doi.org/10.2147/RMHP.S244720
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Vincent Tran,1 Sharon E Reid,2,3 Amanda Roxburgh,1,4– 6 Carolyn A Day1,2
1Sydney Medical School, Faculty of Medicine and Health, The University of Sydney, Camperdown, New South Wales, Australia; 2Edith Collins Centre (Translational Research in Alcohol, Drugs and Toxicology), Sydney Local Health District, Sydney, New South Wales, Australia; 3Sydney School of Public Health, Faculty of Medicine and Health, The University of Sydney, Camperdown, New South Wales, Australia; 4Health Risks Program, Burnet Institute, Melbourne, Victoria, Australia; 5National Drug and Alcohol Research Centre, UNSW, Randwick, New South Wales, Australia; 6Monash Addiction Research Centre, Monash University, Clayton, Victoria, Australia
Correspondence: Carolyn A Day Tel +61 2 95191446
Email [email protected]
Background: Drug consumption rooms (DCRs) and supervised injecting facilities (SIFs) provide a safe environment in which people who inject drugs (PWIDs) can inject under hygienic and supervised conditions. Numerous reviews have documented the benefits of these facilities; however, there is a lack of clarity surrounding their long-term effects.
Purpose: To conduct, with a systematic approach, a literature review, of published peer-reviewed literature assessing the long-term impacts of DCRs/SIFs.
Methods: A systematic search of the PubMed and Embase database was performed using the keywords: (“SUPERVISED” OR “SAFE*”) AND (“CONSUMPTION” OR “INJECT*” OR “SHOOTING”) AND (“FACILITY*” OR “ROOM*” OR “GALLERY*” OR “CENTRE*” OR “CENTER*” OR “SITE*”). Included studies were original articles reporting outcomes for five or more years and addressed at least one of the following client or community outcomes; (i) drug-related harms; (ii) access to substance use treatment and other health services; (iii) impact on local PWID population; (iv) impact on public drug use, drug-related crime and violence; and (v) local community attitudes to DCRs.
Results: Four publications met our inclusion criteria, addressing four of the five outcomes. Long-term data suggested that while the health of PWID naturally declined over time, DCRs/SIFs helped reduce injecting-related harms. The studies showed that DCRs/SIFs facilitate drug treatment, access to health services and cessation of drug injecting. Local residents and business owners reported less public drug use and public syringe disposal following the opening of a DCR/SIF.
Conclusion: Long-term evidence on DCRs/SIFs is consistent with established short-term research demonstrating the benefits of these facilities. A relative paucity of studies was identified, with most evidence originating from Sydney and Vancouver. The overall body of evidence would be improved by future studies following outcomes over longer periods and being undertaken in a variety of jurisdictions and models of DCRs/SIFs.
Keywords: safe injecting facilities, intravenous, Injecting, harm reduction
Introduction
Drug consumption rooms (DCRs) and supervised injecting facilities (SIFs) provide a place where people who inject drugs (PWIDs) can self-administer substances, procured elsewhere, in hygienic conditions under the supervision of qualified staff.1 The first SIF was established in Switzerland in the 1980s, and facilities have since expanded, with some European countries, such as Germany operating multiple services.2 There is a wide range of service models upon which SIFs are based,3 including government sanctioned and unsanctioned SIFs, as well as similar facilities such as Overdose Prevention Sites (OPSs) found in Canada.4,5
SIFs can operate as fixed, stand-alone services, or as co-located services operating within broader facilities such as hospitals and community health centres, or they can operate as mobile outreach services.6 Staff providing these services also range from social workers, harm reduction workers and people with lived experience to nurses and other medical professionals.7
Although these services respond to overdose, and administer naloxone where necessary, for opioid overdose management, most tend to do so with limited or no medical support. Medically supervised SIFs, however, are a relatively newer model, with the first Medically Supervised Injecting Centre opening in Sydney in 2001,8 followed by another in Vancouver, Canada, in 2003.9 More recently, European countries such as Denmark and France have since followed, opening SIFs under similar models.10 In 2017, Ireland passed legislation for a similar service largely based on the Sydney MSIC model.10 In Canada, an epidemic of opioid-related deaths and more than 10-years of successful operation of the Vancouver SIF, has led to a national expansion of SIF and DCR type services.11 In Australia, a second SIF was established in Melbourne in 2018.12
SIFs aim to attract people who engage in high risk injecting behaviours13,14 and work to improve their injecting practices,15,16 therefore minimising their exposure to overdose risks and injecting related harms. Further benefits include referring clients to addiction treatment and other health and social services.3 Previously, Potier et al17 summarised SIFs as having seven key objectives: i) to support marginalised populations of PWID to access health and social services; ii) to reduce overdose-induced morbidity and mortality; iii) to enhance health behaviours amongst PWID; iv) to improve injecting practices; v) to improve the health of PWID; vi) to increase access to substance abuse treatment programs; and vii) to decrease public drug use and related crime.
To date, the research published in SIFs is extensive and their benefits have been well summarised in numerous reviews.9,17–24 The evidence supports positive impacts on both public health and order15,25,26 and improvements in individual health outcomes.27,28 Despite the growing evidence demonstrating the benefits of SIFs, the movement to establish and operate these facilities has often faced significant challenges. Notably, in 2016, the UK Advisory Committee on the Misuse of Drugs gave a recommendation to implement SIFs but was rejected by the UK government in 2017. Lloyd et al29 suggests that this is likely due to fear of political backlash and media portrayal of establishing “drug dens”. Similarly, despite the success of Vancouver’s first SIF, concerted opposition from the government and law enforcement agencies in 2006 changed legislation to halt further funding and SIF trials from being established in Canada.30 This long-standing obstacle was only recently amended in 2016 to allow the expansion of these services throughout the country.9 The supervised injecting facility in Melbourne faced similar resistance from the Victorian state government before eventually opening in 2018.31
Despite some vocal opposition to the opening and operation of SIFs, largely due to the stigma attached to drug use, support for harm reduction strategies has also been well documented. Using a population-level survey, Strike et al32 found a trend of increasing support for SIFs over the period of 2003 to 2009. Recently in 2019, the National Drug Strategy Household Survey found that 54% of respondents supported regulated injecting rooms, with this increasing to 79% in people who had recently injected drugs.33
Though there are more than one hundred facilities operating in numerous countries worldwide, the bulk of literature is from the Sydney MSIC and Vancouver’s Insite,3 which may limit the applicability of evidence to other environments and populations. Most of the SIF research report outcomes over a short (1–2 year) period or report on cross-sectional data only. Although several services have been operating for more than a decade, the lack of clarity surrounding the long-term impacts for periods up to and beyond five years remains. Therefore, we aimed to examine the long-term impacts of SIFs, given that they are a cost-effective intervention34–36 with potential to reduce overdose-related mortality.
We reviewed and consolidated the objectives outlined by Potier et al,17 and determined that a review of the long-term impacts on five key objectives would be beneficial: i) drug-related harms; ii) access to substance use treatment and other health services; iii) impact on the local PWID population, ie, whether numbers of PWID have increased or decreased over time in jurisdictions with SIFs; iv) impact on public drug use, drug-related crime and violence; v) local community attitudes to SIFs. The aims of this review were therefore to determine client and community-related outcomes, if any, for five or more years.
Methods
A systematic search in the literature was performed, with the search carried out in the Medline and Embase databases. Our search strategy was adapted from Potier et al,17 using the keywords: (“SUPERVISED” OR “SAFE*”) AND (“CONSUMPTION” OR “INJECT*” OR “SHOOTING”) AND (“FACILITY*” OR “ROOM*” OR “GALLERY*” OR “CENTRE*” OR “CENTER*” OR “SITE*”). The search results were then further refined using the following MESH terms: “SUBSTANCE ABUSE” AND “INTRAVENOUS/”.
The article selection process is outlined in Figure 1. Studies were limited to human studies and those reported in the English language, and articles published from 1946 to June 2020 were included in the selection process. Duplicate studies were removed using the Ovid deduplicate function, and any further duplicates found were removed manually.
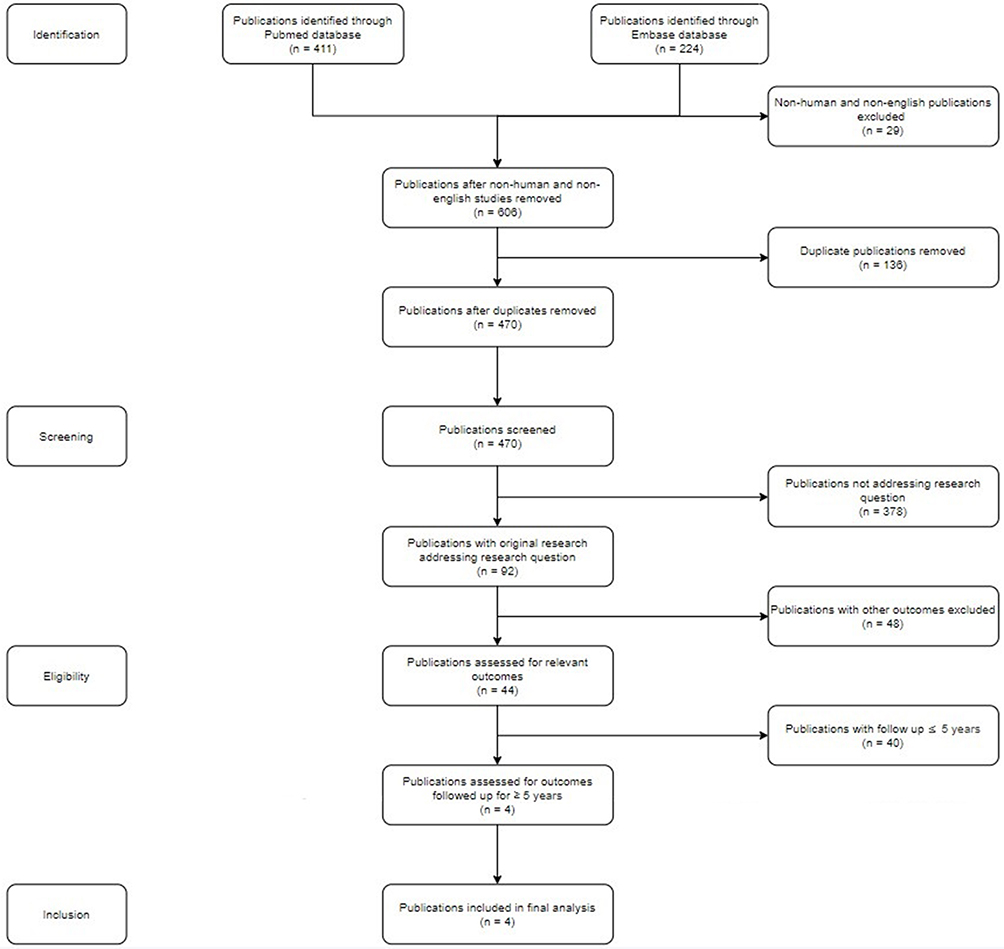 |
Figure 1 Article selection process. Abbreviations: DCR, drug consumption rooms; SIF, safe injecting facility; PWID, people who inject drugs. |
The studies were screened by title by one author (VT) for original research that addressed our research topic. The abstracts of the remaining studies were then assessed to determine whether they addressed any of the five objectives derived by Potier et al:17 (i) drug-related harms, (ii) access to substance use treatment and other health services, (iii) impact on local PWID population, (iv) impact on public drug use, drug-related crime and violence, (v) local community attitudes to DCRs. The remaining studies were separately read in detail by both VT and a second author (CD) to determine whether they included longer-term outcomes, defined as five or more years. Any discrepancies were discussed until a consensus was reached to include or exclude studies from the final count. If both authors were unable to unanimously agree, a third author would have been consulted, however this was not required.
Results
The initial search found 470 publications. Only four publications met the selection criteria (Table 1). Thirteen of the studies excluded in the final screening step were cross-sectional and largely consisted of qualitative or survey-style studies. Most studies were excluded as they examined periods of less than five years, with seven studies having a follow-up period of less than one year and sixteen with 1–4-year period. One study assessed community attitudes and drug-related harms over four years, falling short of our criteria and was thus not included.
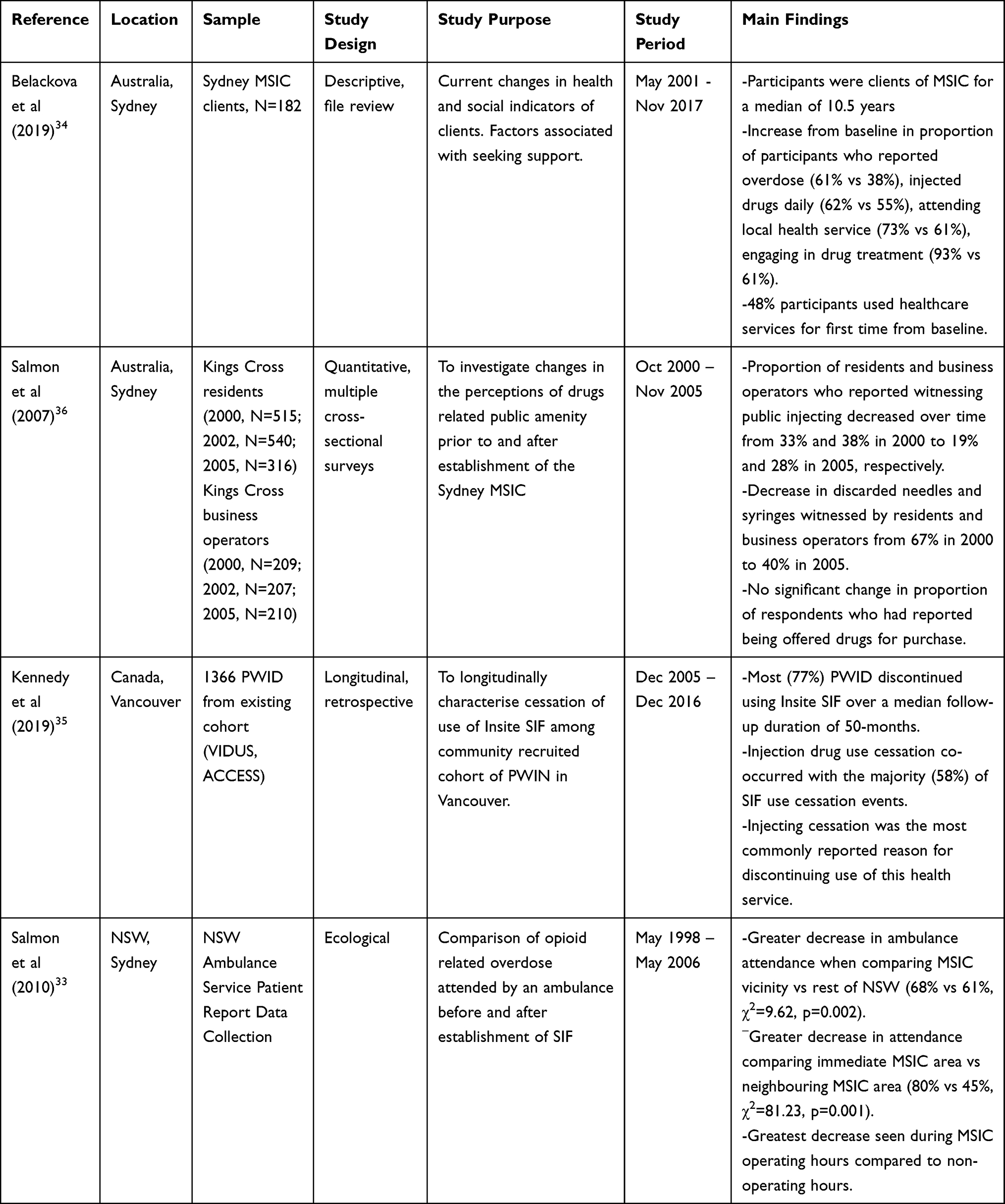 |
Table 1 Summary of Included Studies |
Of the five outcomes assessed, we found that only four had been assessed with longer term data, three client-related and one community-related: (i) drug-related harms, (ii) access to substance use treatment and other health services, (iii) impact on the local PWID population, (iv) impact on public drug use, drug-related crime and violence.
Client Outcomes
Drug Related Harms
Of the four studies included in the final analysis, two investigated the effects of DCRs on harms related to injecting drug use experienced by clients.
In Sydney, Salmon et al27 used data from NSW State Ambulance Service to evaluate patterns of ambulance attendance at suspected opioid overdoses. Over 60 months following the opening of the Sydney MSIC, there was an 80% decrease in ambulance attendances in the immediate vicinity compared to a 45% decrease in neighbouring areas (45%).27 Although ambulance attendance patterns in the rest of NSW also decreased by 61%, the area where the MSIC was located still showed a net benefit, with a greater reduction of 68%. The differences in decline seen in both comparisons were statistically significant.27
Also investigating the Sydney MSIC, Belackova et al37 collected health and social information from clients using interviewer-administered questions similar to those collected from clients at registration. This data was then compared to data collected at the client’s initial registration. The study found that clients who participated had been using the service for an average of nine years, with a mean of 800 visits. A significantly higher proportion of clients had experienced overdose at the follow-up interview (61%) when compared to baseline (38%). Furthermore, there was a seven percent increase in the proportion of clients who reported injecting drugs daily at the time of follow-up.37
Access to Substance Use Treatment and Other Health Services
The data collected by Belackova et al37 also revealed that long-term SIF clients were also more likely to engage with health services. When compared to their initial visit, there was an increase in the proportion of clients currently engaged in drug treatment (93% vs 61%) and use of local primary health care services had similarly increased (73% vs 33%). Almost half (48%) of the survey participants also reported utilising nearby healthcare services for the first time since their initial visit to the Sydney MSIC.37
Impact on the Local PWID Population
Kennedy et al38 investigated patterns of use of Vancouver’s SIF. They found that a significant proportion of PWID (77%) had at least one episode of discontinuing SIF attendance, and that the majority of these episodes (58%) occurred in conjunction with drug use cessation.38 This was reinforced by client responses stating that injection cessation was the most common reason for ceasing attendance at the facility.38
Community Outcomes
Impact on Public Drug Use, Drug Related Crime and Violence
Salmon et al39 surveyed residents and business operators to investigate whether local perception of public amenity had changed since the opening of the Sydney MSIC. They found that the proportion of residents and business owners who reported witnessing public injecting decreased over time from 33% and 38% in 2000 to 19% and 28% in 2005, respectively.39 Similarly, there was a significant decrease in discarded needles and syringes witnessed by both residents and business operators over the five-year period.39 However, there was no significant change in the proportion of respondents who had reported being offered drugs for purchase.39
Discussion
Of the five SIF objectives we investigated, long-term outcomes were identified for only four of these objectives. There is substantial literature on SIFs; however, only a small number of these studies report on outcomes over a period of five or more years.
Importantly, overdose reduction, a key aim of SIFs, was found to have an enduring impact, with data reported by Salmon et al27 showing a decrease in opioid suspected overdoses requiring ambulance attendance. This benefit was most notable during the opening hours of the service, further implicating the service’s role in the reductions. However, the authors noted that the benefit of freeing-up ambulance services to attend to other medical emergencies may not be applicable to SIFs that do not administer naloxone in overdoses, or have protocols that mandate ambulance attendance.27 These findings are similar to shorter term evidence from Vancouver’s Insite, which managed 336 overdoses without a fatality over an 18-month period.40,41 While it remains unclear whether SIFs reduce the total number of overdoses experienced by PWIDs who use SIFs, it is clear that the mortality rate of overdoses is reduced in areas with SIFs.
One important finding from Belackova et al37 was that the overall health of clients at the Sydney MSIC declined over time, defined as an increase in the proportion of clients who reported a physical or mental health issue, unemployment, previous incarceration or recent overdose, from their initial visit. This finding likely reflects the increasing needs of clients who attend SIFs, given the complexities and challenges faced by many clients attending, which often include long-term substance use disorders and increased overdose risk.42–44 Therefore, SIFs are well-placed to provide both acute overdose intervention as well as ongoing support and referral to other health services as part of longer-term care. Groups opposed to SIFs have suggested that the worsening health of clients could also be interpreted as SIFs enabling continued drug use and thus increasing the risk of harms45 However, given the expansive literature on poor outcomes for people who inject drugs generally, deteriorating health cannot reasonably be attributed to SIFs.43,44,46
The significant increase in the proportion of Sydney MSIC clients engaged in drug treatment and local health services indicates that SIFs play an important role in facilitating engagement with health services among clients.37 This is consistent with studies that have shown, over shorter durations, a positive relationship between SIF utilisation and likelihood of referral to health and social services.47–50 Shorter term studies from Vancouver’s Insite have reported a large volume of referrals made in a 12-month period, with a substantial proportion (40%) for addiction treatment51 and a concurrent 30% increase in the uptake of detoxification services.52
Kennedy et al38 found that SIFs can play a role in the cessation of injecting drug use through referrals into treatment. Their results noted that a significant number of SIF clients reported discontinuation of SIF use and injecting cessation.38 This is consistent with other studies, which have described increased engagement with addiction treatment amongst SIF clients, leading to subsequent decreases in drug and SIF use.47,48,50,52,53 Whether SIFs enable long-term abstinence is still unclear as Kerr et al found that there was no significant change in the number of clients who continued injecting drugs in a one-year period prior to and following the opening of a SIF.54 Kennedy et al38 observed that many of the clients had multiple periods of cessation of SIF use, which is consistent with the remission/relapsing nature of substance use disorders and the difficulty that users experience even when engaged in addiction treatment.55–57 Additionally, the broader literature shows there is no evidence to suggest that SIFs increase the rate of initiation into injecting drug use in the community, with research at the Vancouver SIF showing clients were already engaged in injecting practices prior to their use of the service.58 Furthermore, prior injecting history is a requirement at many SIFs such as the Sydney MSIC.8
Salmon et al39 demonstrated that SIFs improve public amenity by decreasing public drug use and unsafe syringe disposal. These results corroborate the findings of other short-term community surveys, which found local residents reported seeing less public injecting shortly following the opening of the Sydney MSIC.59,60 This result is also supported by short-term studies from Vancouver and Rotterdam, which found that 71%25 and 83%61 of SIF clients, respectively, reported using drugs less often in public. A one-year study by Stoltz et al26 also found that clients who consistently use Vancouver’s SIF were more likely to report safe syringe disposal. This is likely explained by clients, prior to SIF opening, often lacking a safe, alternative place to inject, frequently caused by the absence of stable housing.62 Salmon et al’s39 findings of a lack of change in the proportion of residents being offered drugs, supports earlier work conducted in Sydney and Vancouver where data on drug crime before and after SIF opening suggested that there was no increase associated with the facility opening.63,64
Several studies have also found that local community opinion has generally been favourable. Specifically, a survey in 2000 by Thein et al,60 of the community around Sydney MSIC showed most respondents (68%) supported the facility prior to its opening, with this increasing to 78% in 2002 once opened. Similar attitudes were found even when surveying communities without SIFs, with up to 74% of respondents saying they support the harm reduction measure.65,66 As shown above, support following the opening of SIFs has been attributed to the improved public amenity, with decreases in public injection reported by both clients25,61 and community members.39,59 However, public support for these services may not be as strong in certain areas, as a survey by McGinty et al67 showed that only 29% of surveyed US adults supported the legalisation of SIFs. This may reflect how cultural stigmas surrounding opioid and injecting drug use may negatively affect attitudes to these facilities.
The findings from this review have important public health and research implications. SIFs play an important public health role in reducing the harms associated with injecting, by providing a safer space for people to inject, without judgement regarding their drug use or their level of engagement in drug treatment or other health services. SIFs also play an important role in advocating for equitable health service access for their clients. The model for the MSIR in Melbourne is unique and promising in that it is co-located with a range of other services including alcohol and drug treatments, basic dental care, general practice and mental health services, blood-borne virus testing and treatment as well as housing and legal resources.68 The availability of these resources on site may enhance opportunities for clients to engage with these services, thus improving their health and social wellbeing. Research investigating the impact of integrating these services within SIFs is crucial in informing the design and establishment of future facilities. Future research should also consider linking client data to external health services to better understand the needs and accessibility of services amongst SIF clients. This will also allow evaluation of SIF impact on local health services and at a public health scale.
This review has several limitations. First, we define long-term effects as outcomes followed for five years or more, which may have contributed to the relative paucity of studies included. As discussed, most studies identified reported on outcomes measured following less than five years of operation/follow-up and were therefore excluded. The breadth of our search may also have been limited as we considered only peer-reviewed papers indexed on either Medline or Embase. However, the bulk of research identified in other reviews was drawn from the medical literature,3,9,17,19–24 making these two databases the most relevant. Further, we were interested in only considering the most robust research findings, and therefore peer-reviewed literature was the most appropriate. We included only studies published in English, therefore our findings may have been restricted to research originating from countries in which English is the primary language. As has been previously identified,17 most of the research has been centred on the medical SIFs with an Australian and Canadian research bias. Therefore, information surrounding client and community outcomes of non-medical SIFs is lacking. These results are also likely to suffer from publication bias, whereby null or negative findings have not been reported in the scientific literature. This may limit the ability to generalise these findings when considering the feasibility of SIFs in other settings or with different service models.
Nevertheless, we have identified a lack of research investigating the long-term (≥ 5 years) effects of SIFs and that currently available research addresses four of the five SIF objectives we sought to investigate. Encouraging future studies to focus on longer follow-up periods would, therefore, improve our understanding of the long-term effects of SIFs. Such research should, however, be undertaken in a variety of jurisdictions and with a range of DCR/SIFs models. Despite this, the available evidence supports a substantial base of short-term research that shows SIFs reduce drug-related harms, improve access to drug treatment and health services, facilitate a reduction or cessation of injecting drug use, improve public amenity, and that there is a small but burgeoning body of working looking at longer-term outcomes.
Disclosure
Amanda Roxburgh is funded by a National Health and Medical Research Council (NHMRC) Investigator Grant (APP1173505). Amanda Roxburgh and Carolyn A Day are both research affiliates with the Uniting Medically Supervised Injecting Centre in Sydney. The authors report no other conflicts of interest in this work.
References
1. EMCDDA. Drug Consumption Rooms: An Overview of Provision and Evidence. Lisbon: European Monitoring Centre for Drugs and Drug Addiction; 2016.
2. Broadhead R, Kerr T, Grund J-P. Safer injection facilities in North America: their place in public policy and health initiatives. J Drug Issues. 2002;32:329–355. doi:10.1177/002204260203200113
3. Belackova V, Salmon A. Overview of International Literature - Supervised Injecting Facilities & Drug Consumption Rooms. Sydney: Uniting Medically Supervised Injecting Centre. 2017.
4. Kral AH, Lambdin BH, Wenger LD, Davidson PJ. Evaluation of an unsanctioned safe consumption site in the United States. N Engl J Med. 2020;383(6):589–590. doi:10.1056/NEJMc2015435
5. Pauly B, Wallace B, Pagan F, et al. Impact of overdose prevention sites during a public health emergency in Victoria, Canada. PLoS One. 2020;15(5):e0229208. doi:10.1371/journal.pone.0229208
6. Dietze P, Winter R, Pedrana A, Leicht A, Majó IRX, Brugal MT. Mobile safe injecting facilities in Barcelona and Berlin. Int J Drug Policy. 2012;23(4):257–260. doi:10.1016/j.drugpo.2012.02.006
7. Kimber J, Dolan K, Wodak A. Survey of drug consumption rooms: service delivery and perceived public health and amenity impact. Drug Alcohol Rev. 2005;24(1):21–24. doi:10.1080/09595230500125047
8. MSIC Evaluation Committee. Final report of the evaluation of the Sydney medically supervised injecting centre; 2003.
9. Kerr T, Mitra S, Kennedy MC, McNeil R. Supervised injection facilities in Canada: past, present, and future. Harm Reduct J. 2017;14(1):28. doi:10.1186/s12954-017-0154-1
10. Gostin LO, Hodge JG
11. Young S, Fairbairn N. Expanding supervised injection facilities across Canada: lessons from the Vancouver experience. Can J Public Health. 2018;109(2):227–230. doi:10.17269/s41997-018-0089-7
12. Van Den Boom W, del Mar Quiroga M, Fetene DM, et al. The Melbourne safe injecting room attracted people most in need of its service. Am J Prev Med. 2021;61:217–224. doi:10.1016/j.amepre.2021.02.018
13. Stoltz J-A, Wood E, Miller C, et al. Characteristics of young illicit drug injectors who use North America’s first medically supervised safer injecting facility. Addict Res Theory. 2009;15:63–69. doi:10.1080/16066350601081090
14. Reddon H, Wood E, Tyndall M, et al. Use of North America’s first medically supervised safer injecting facility among HIV-positive injection drug users. AIDS Educ Prev. 2011;23(5):412–422. doi:10.1521/aeap.2011.23.5.412
15. Zurhold H, Degkwitz P, Verthein U, Haasen C. Drug consumption rooms in Hamburg, Germany: evaluation of the effects on harm reduction and the reduction of public nuisance. J Drug Issues. 2003;33(3):663–688. doi:10.1177/002204260303300308
16. Kinnard EN, Howe CJ, Kerr T, Skjødt Hass V, Marshall BDL. Self-reported changes in drug use behaviors and syringe disposal methods following the opening of a supervised injecting facility in Copenhagen, Denmark. Harm Reduct J. 2014;11(1):29. doi:10.1186/1477-7517-11-29
17. Potier C, Laprévote V, Dubois-Arber F, Cottencin O, Rolland B. Supervised injection services: what has been demonstrated? A systematic literature review. Drug Alcohol Depend. 2014;145:48–68. doi:10.1016/j.drugalcdep.2014.10.012
18. Hedrich D, Hartnoll R. Harm Reduction Interventions. Milano: Springer Milan; 2014:1291–1313.
19. Hedrich D, Kerr T, Dubois-Arber F. Drug consumption facilities in Europe and beyond. Harm Reduct Evidence, Impacts Challenges. 2010;3:305–332.
20. Kerr T, Kimber J, DeBeck K, Wood E. The role of safer injection facilities in the response to HIV/AIDS among injection drug users. Curr HIV/AIDS Rep. 2007;4(4):158–164. doi:10.1007/s11904-007-0023-8
21. Kimber J, Dolan K, Beek IV, Hedrich D, Zurhold H. Drug consumption facilities: an update since 2000. Drug Alcohol Rev. 2003;22(2):227–233. doi:10.1080/095952301000116951
22. Kimber J, Palmateer N, Hutchinson SJ, Hickman M, Goldberg DJ, Rhodes T. Harm reduction among injecting drug users - evidence of effectiveness; 2010.
23. Milloy MJ, Wood E. Emerging role of supervised injecting facilities in human immunodeficiency virus prevention. Addiction. 2009;104(4):620–621.
24. Semaan S, Fleming P, Worrell C, Stolp H, Baack B, Miller M. Potential role of safer injection facilities in reducing HIV and hepatitis C infections and overdose mortality in the United States. Drug Alcohol Depend. 2011;118(2–3):100–110. doi:10.1016/j.drugalcdep.2011.03.006
25. Petrar S, Kerr T, Tyndall MW, Zhang R, Montaner JS, Wood E. Injection drug users’ perceptions regarding use of a medically supervised safer injecting facility. Addict Behav. 2007;32(5):1088–1093. doi:10.1016/j.addbeh.2006.07.013
26. Stoltz J-A, Wood E, Small W, et al. Changes in injecting practices associated with the use of a medically supervised safer injection facility. J Public Health. 2007;29(1):35–39.
27. Salmon AM, van Beek I, Amin J, Kaldor J, Maher L. The impact of a supervised injecting facility on ambulance call-outs in Sydney, Australia. Addiction. 2010;105(4):676–683.
28. Marshall BD, Milloy MJ, Wood E, Montaner JS, Kerr T. Reduction in overdose mortality after the opening of North America’s first medically supervised safer injecting facility: a retrospective population-based study. Lancet. 2011;377(9775):1429–1437. doi:10.1016/S0140-6736(10)62353-7
29. Lloyd C, Stöver H, Zurhold H, Hunt N. Similar problems, divergent responses: drug consumption room policies in the UK and Germany. J Subst Use. 2017;22(1):66–70. doi:10.3109/14659891.2016.1143049
30. Wood E, Kerr T, Tyndall MW, Montaner JSG. The Canadian government’s treatment of scientific process and evidence: inside the evaluation of North America’s first supervised injecting facility. Int J Drug Policy. 2008;19(3):220–225. doi:10.1016/j.drugpo.2007.11.001
31. Munckton S. Labor ignores push for safe injecting room. In: Green Left Weekly. Informit; 2017:8.
32. Strike C, Jairam JA, Kolla G, et al. Increasing public support for supervised injection facilities in Ontario, Canada. Addiction. 2014;109(6):946–953. doi:10.1111/add.12506
33. Australian Institute of Health and Welfare. National drug strategy household survey 2019; 2020.
34. Bayoumi AM, Zaric GS. The cost-effectiveness of Vancouver’s supervised injection facility. Can Med Assoc J. 2008;179(11):1143–1151. doi:10.1503/cmaj.080808
35. Pinkerton SD. Is Vancouver Canada’s supervised injection facility cost-saving? Addiction. 2010;105(8):1429–1436. doi:10.1111/j.1360-0443.2010.02977.x
36. Andresen MA, Boyd N. A cost-benefit and cost-effectiveness analysis of Vancouver’s supervised injection facility. Int J Drug Policy. 2009;21(1):70–76. doi:10.1016/j.drugpo.2009.03.004
37. Belackova V, Silins E, Salmon AM, Jauncey M, Day CA. “Beyond safer injecting” - Health and social needs and acceptance of support among clients of a supervised injecting facility. J Environ Res. 2019;16(11):2032.
38. Kennedy MC, Klassen DC, Dong H, Milloy MJS, Hayashi K, Kerr TH. Supervised injection facility utilization patterns: a prospective cohort study in Vancouver, Canada. J Preventive Med. 2019;57(3):330–337.
39. Salmon AM, Thein HH, Kimber J, Kaldor JM, Maher L. Five years on: what are the community perceptions of drug-related public amenity following the establishment of the Sydney Medically Supervised Injecting Centre? Int J Drug Policy. 2007;18(1):46–53. doi:10.1016/j.drugpo.2006.11.010
40. Kerr T, Tyndall M, Lai C, Wood E. Drug-related overdoses within a medically supervised safer injection facility. Int J Drug Policy. 2006;17:436–441. doi:10.1016/j.drugpo.2006.05.008
41. Kerr T, Small W, Moore D, Wood E. A micro-environmental intervention to reduce the harms associated with drug-related overdose: evidence from the evaluation of Vancouver’s safer injection facility. Int J Drug Policy. 2007;18(1):37–45. doi:10.1016/j.drugpo.2006.12.008
42. Darke S. Heroin overdose. Addiction. 2016;111(11):2060–2063. doi:10.1111/add.13516
43. Hser YI, Hoffman V, Grella CE, Anglin MD. A 33-year follow-up of narcotics addicts. Arch Gen Psychiatry. 2001;58(5):503–508. doi:10.1001/archpsyc.58.5.503
44. Darke S. Pathways to heroin dependence: time to re-appraise self-medication. Addiction. 2013;108(4):659–667. doi:10.1111/j.1360-0443.2012.04001.x
45. Dolan K, Kimber J, Fry C, Fitzgerald J, McDonald D, Trautmann F. Drug consumption facilities in Europe and the establishment of supervised injecting centres in Australia. Drug and Alcohol Rev. 2000;19(3):337–346. doi:10.1080/713659379
46. Kimber J, Copeland L, Hickman M, et al. Survival and cessation in injecting drug users: prospective observational study of outcomes and effect of opiate substitution treatment. BMJ. 2010;341:c3172. doi:10.1136/bmj.c3172
47. DeBeck K, Kerr T, Bird L, et al. Injection drug use cessation and use of North America’s first medically supervised safer injecting facility. Drug Alcohol Depend. 2011;113(2–3):172–176. doi:10.1016/j.drugalcdep.2010.07.023
48. Kimber J, Mattick RP, Kaldor J, van Beek I, Gilmour S, Rance JA. Process and predictors of drug treatment referral and referral uptake at the Sydney Medically Supervised Injecting Centre. Drug Alcohol Rev. 2008;27(6):602–612. doi:10.1080/09595230801995668
49. Salmon A, Belackova V, Schwanz R, Jauncey M, Hiley S, Demirkol A. Homelessness among clients of Sydney’s supervised injecting facility. Drugs Alcohol Today. 2017;17. doi:10.1108/DAT-06-2017-0026
50. Wood E, Tyndall MW, Zhang R, et al. Attendance at supervised injecting facilities and use of detoxification services. N Engl J Med. 2006;354(23):2512–2514. doi:10.1056/NEJMc052939
51. Tyndall MW, Kerr T, Zhang R, King E, Montaner JG, Wood E. Attendance, drug use patterns, and referrals made from North America’s first supervised injection facility. Drug Alcohol Depend. 2006;83(3):193–198. doi:10.1016/j.drugalcdep.2005.11.011
52. Wood E, Tyndall MW, Zhang R, Montaner JSG, Kerr T. Rate of detoxification service use and its impact among a cohort of supervised injecting facility users. Addiction. 2007;102(6):916–919. doi:10.1111/j.1360-0443.2007.01818.x
53. Gaddis A, Kennedy MC, Nosova E, et al. Use of on-site detoxification services co-located with a supervised injection facility. J Subst Abuse Treat. 2017;82:1–6. doi:10.1016/j.jsat.2017.08.003
54. Kerr T, Stoltz JA, Tyndall M, et al. Impact of a medically supervised safer injection facility on community drug use patterns: a before and after study. BMJ. 2006;332(7535):220–222. doi:10.1136/bmj.332.7535.220
55. Xia Y, Seaman S, Hickman M, et al. Factors affecting repeated cessations of injecting drug use and relapses during the entire injecting career among the Edinburgh Addiction Cohort. Drug Alcohol Depend. 2015;151:76–83. doi:10.1016/j.drugalcdep.2015.03.005
56. Galai N, Safaeian M, Vlahov D, Bolotin A, Celentano DD. Longitudinal patterns of drug injection behavior in the ALIVE Study cohort, 1988–2000: description and determinants. Am J Epidemiol. 2003;158(7):695–704. doi:10.1093/aje/kwg209
57. Genberg BL, Gange SJ, Go VF, Celentano DD, Kirk GD, Mehta SH. Trajectories of injection drug use over 20 years (1988–2008) in Baltimore, Maryland. Am J Epidemiol. 2011;173(7):829–836.
58. Kerr T, Tyndall MW, Zhang R, Lai C, Montaner JS, Wood E. Circumstances of first injection among illicit drug users accessing a medically supervised safer injection facility. Am J Public Health (N Y). 2007;97(7):1228–1230. doi:10.2105/AJPH.2006.086256
59. Wood E, Kerr T, Small W, et al. Changes in public order after the opening of a medically supervised safer injecting facility for illicit injection drug users. CMAJ. 2004;171(7):731–734. doi:10.1503/cmaj.1040774
60. Thein -H-H, Kimber J, Maher L, MacDonald M, Kaldor JM. Public opinion towards supervised injecting centres and the Sydney Medically Supervised Injecting Centre. Int J Drug Policy. 2005;16(4):275–280. doi:10.1016/j.drugpo.2005.03.003
61. van der Poel A, Barendregt C, van de Mheen D. Drug consumption rooms in Rotterdam: an explorative description. Eur Addict Res. 2003;9(2):94–100. doi:10.1159/000068807
62. Fry C, Fox S, Rumbold G. Establishing safe injecting rooms in Australia: attitudes of injecting drug users. Aust N Z J Public Health. 1999;23(5):501–504. doi:10.1111/j.1467-842X.1999.tb01306.x
63. Freeman K, Jones CG, Weatherburn DJ, Rutter S, Spooner CJ, Donnelly N. The impact of the Sydney medically supervised injecting centre (MSIC) on crime. Drug Alcohol Rev. 2005;24(2):173–184. doi:10.1080/09595230500167460
64. Wood E, Tyndall MW, Lai C, Montaner JS, Kerr T. Impact of a medically supervised safer injecting facility on drug dealing and other drug-related crime. Subst Abuse Treat Prev Policy. 2006;1(1):1–4. doi:10.1186/1747-597X-1-13
65. White B, Haber PS, Day CA. Community attitudes towards harm reduction services and a newly established needle and syringe automatic dispensing machine in an inner-city area of Sydney, Australia. Int J Drug Policy. 2016;27:121–126. doi:10.1016/j.drugpo.2015.05.010
66. Cruz MF, Patra J, Fischer B, Rehm J, Kalousek K. Public opinion towards supervised injection facilities and heroin-assisted treatment in Ontario, Canada. Int J Drug Policy. 2007;18(1):54–61. doi:10.1016/j.drugpo.2006.12.001
67. McGinty EE, Barry CL, Stone EM, et al. Public support for safe consumption sites and syringe services programs to combat the opioid epidemic. Prev Med. 2018;111:73–77. doi:10.1016/j.ypmed.2018.02.026
68. Roxburgh A, Jauncey M, Day C, et al. Adapting harm reduction services during COVID-19: lessons from the supervised injecting facilities in Australia. Harm Reduct J. 2021;18(1):20. doi:10.1186/s12954-021-00471-x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.