Back to Journals » Clinical Optometry » Volume 17
Assessing Access to and Utilization of the Advanced Diagnostic and Management Equipment for Early Keratoconus in Public and Private Healthcare Facilities Across Nyanza and Western Kenya
Authors Njeru MM ![]() , Maina SN, Signes-Soler I, Golicha HA
, Maina SN, Signes-Soler I, Golicha HA
Received 5 February 2025
Accepted for publication 28 July 2025
Published 20 August 2025 Volume 2025:17 Pages 269—279
DOI https://doi.org/10.2147/OPTO.S520763
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor John Girkin
Millicent Muthoni Njeru,1 Sheilah Nangena Maina,1,* Isabel Signes-Soler,1,2,* Hussein Adams Golicha3,*
1Department of Optometry and Vision Sciences, Masinde Muliro University of Science and Technology, Kakamega, Kenya; 2Department of Optics and Optometry and Vision Sciences, Research Group in Preventive Optometry and Visual Treatments (OPTV), Universitat de València, Valencia, Spain; 3Department of Physics, Masinde Muliro University of Science and Technology, Kakamega, Kenya
*These authors contributed equally to this work
Correspondence: Millicent Muthoni Njeru, Masinde Muliro University of Science and Technology, Department of Optometry and Vision Sciences, P.O. BOX 190 – 50100, Kakamega, Kenya, Tel +254715867693, Email [email protected]
Purpose: To evaluate the availability and utilization of the advanced equipment for the diagnosis and management of early keratoconus in the public and private healthcare facilities in Nyanza and Western Kenya.
Methods: A cross-sectional study design was applied. An online questionnaire was sent to the eyecare practitioners. Data on socio-demographics, equipment availability, and utilization for early keratoconus diagnosis and management were obtained and analyzed using SPSS V 29.
Results: A total of 134 eyecare practitioners (out of 143), with the majority 80 (59.7%) being males, responded to the questionnaire. The study found that advanced equipment were scarcely available, such as Tomographer 14 (10.4%), Topographer 17 (12.7%) and Pachymeter 21 (15.7%) as compared to basic equipment: distance VA chart 134 (100%), trial lens/phoropter 129 (96.3%), retinoscope 128 (95.5%) and slit-lamp 111 (82.8%), with level 6 having the highest availability. Additionally, the available advanced equipment had working conditions far below standards and below standards: topographer 6 (35.2%) and contact lens fitting set 12 (46.1%). The utilization rates of the advanced equipment were low as follows: contact lens fitting set 8 (31.0%), pachymeter 11 (52.4%) and topographer 9 (52.9%). A chi-square test found a significant association between equipment availability and their utilization, VA chart (p=0.03333), trial lens/phoropter (p=0.00292), slit-lamp (p=0.00283) and keratometer (p=0.00001).
Conclusion: The study revealed a lack of advanced diagnostic equipment, with some existing tools falling below standard and underutilized. It recommends that healthcare institutions prioritize the acquisition and maintenance of essential equipment. Additionally, the Ministry of Health should collaborate with stakeholders to incorporate early keratoconus detection into national eyecare guidelines.
Keywords: eyecare practitioners, advanced equipment, equipment utilization, early keratoconus diagnosis and management, Kenya
Introduction
Keratoconus (KC) is a progressive corneal disease that leads to irregular astigmatism, reduced visual acuity, and cornea thinning.1,2 Keratoconus primarily affects young individuals in their second and third decades of life,3 often leading to significant visual impairment if not diagnosed and managed early.4 Timely diagnosis of KC requires competent eye care professionals and advanced diagnostic tools, as early signs of the disease may be missed with basic diagnostic tools.5 Advanced diagnostic tools such as corneal topographers, tomographers and pachymeters are a higher sensitivity and specificity equipment that are able to detect and diagnose KC at the sub-clinical stages, even before the clinical signs manifest. Advanced equipment is essential for the early detection of KC,6–8 allowing for timely intervention and improved patient outcomes.9
Regarding KC prevalence, a study by Hashemi et al, reported the global KC prevalence of 0.14%.10 It is now a growing health concern, with increasing KC prevalences across the globe, whereby regional studies in Asia have had higher rates in the recent times as opposed to earlier ones (0.04%) done in South Korea in 201411 and (2.39%) in Turkey in 2021.12 Moreover, an increasing trend has been observed in Saudi Arabia with year 2015 data depicting a KC prevalence of 8.59%13 and recent files in 2017 showing rates of 18.70%.14 Furthermore, similar increasing trends have been noted in the USA with 0.01% in 2009,15 and 0.15% in 2021.16 The increasing rates could be as a result of rising numbers of KC patients, improved diagnostic technology or both. In Africa, a meta-analysis that included different countries showed prevalence of 7.91%,17 with some differing prevalences across the countries. South Africa (24.21%), Egypt (17.50%) and Kenya (30.89%), showing higher rates compared to other countries.18–20
In Kenya, research on KC remains limited, with existing studies showing inconsistent prevalence rates. Rashid et al reported a low prevalence of 1.67% among high school students,21 while Mugho et al found a much higher prevalence of 30.89%,20 which could be due to the allergic conjunctivitis population used, as it is associated with KC.22 Another study on contact lens use revealed that most patients presented with moderate to severe KC, highlighting a lack of early detection in clinical practice.23 In terms of management, a study showed that a number of moderate and severe KC patients were managed using spectacles.24 In a different study, some Ophthalmic Clinical Officers (OCOs) performed corneal cross-linking (CXL), while optometrists were more involved in contact lens fitting. Referrals to and co-management with ophthalmologists were also reported.25 However, these findings may not reflect the full picture, as other key eye care cadres were excluded from the study. Additionally, regarding referrals in Africa, most of the practitioners in Ghana and Nigeria refer KC patients to the ophthalmologists in case of progression, but most reported no co-management with them.26
Most existing studies have focused on generalized KC, with minimal attention to early-stage disease, where timely intervention could yield better outcomes. Although some studies mentioned the presence of diagnostic equipment, none assessed its functionality or utilization which are critical factors in effective early diagnosis. Additionally, research has largely been confined to metropolitan areas like Nairobi, overlooking rural and low-income regions where variations in socioeconomic status and climatic conditions may influence KC prevalence and access to care. These gaps underscore the need for more comprehensive, inclusive research on early KC detection and management across diverse settings in Kenya such as Western and Nyanza region.
In Kenya, the healthcare system is structured into six hierarchical levels, ranging from community-based care to national referral services. Levels 1 to 3 comprise community health services, dispensaries, and health centers, respectively. They generally do not offer eye care services which are predominantly provided at Levels 4 to 6 including keratoconus care, which consist of sub-county, county, and national referral hospitals. Level 4 facilities provide primary and some, secondary eye care services, including basic ocular examinations and minor surgical procedures. At Level 5, services expand to include specialized eye care, encompassing advanced diagnostic and therapeutic interventions such as medical and surgical treatment of ocular diseases, refractive care, low vision services, laser treatments, and visual rehabilitation. Level 6 facilities, which include teaching and referral hospitals, provide the most advanced and subspecialized ophthalmic services in the country.27–29
Early detection and appropriate management of keratoconus are essential for preventing significant visual impairment.9 The ability of ECPs to diagnose and manage keratoconus varies significantly based on their level of training and professional cadre in Kenya. The eye care workforce comprises five main professional categories: ophthalmologists, optometrists, optometry technologists, ophthalmic clinical officers (OCOs), and comprehensive ophthalmology and cataract surgeons (COCs). Ophthalmologists, who are medical doctors with an additional three-year Master’s degree in ophthalmology, are typically the final referral point for advanced keratoconus cases that require surgical intervention. However, their numbers remain critically low, with only about 160 ophthalmologists to serve a population of approximately 60 million Kenyans. They are disproportionately concentrated in urban area, leaving rural and marginalized communities significantly underserved.27
Optometrists are trained either through a five-year Bachelor of Optometry (optometry officers) or a three-year diploma program (optometry technologists). Optometry officers typically perform refractions, prescribe contact lenses and refer patients to ophthalmologists when surgical intervention is necessary.27 On the other hand, OCOs and COCs undergo a three-year diploma in clinical medicine and receive additional training focused on ophthalmology and cataract surgical for 1.5 years or 3 years to become OCO and COCS, respectively.27,30 While these cadres can diagnose keratoconus, they are not licensed to perform keratoconus-related surgeries. Although ECPs across these cadres are generally capable of diagnosing and initiating management for keratoconus, there is limited data on the availability and effective utilization of advanced diagnostic equipment in Kenya. It is therefore necessary to determine the availability and utilization of advanced equipment in the different levels of health facilities, with this being the first study on early keratoconus in Kenya and Africa. There is no denying that the gaps in infrastructure and equipment distribution in many low-resource settings, such as Kenya, often contribute to underdiagnosis and delays in appropriate treatment for keratoconus.31–33
Materials and Methods
Study Design and Setting
The study adopted a cross-sectional design. Data was collected from eye health facilities located in the Western and Nyanza regions of Kenya, from August to September 2024. These regions collectively comprise ten counties: Nyanza (Migori, Nyamira, Kisii, Siaya, Homa Bay, and Kisumu) and Western (Kakamega, Busia, Vihiga, and Bungoma). The health facilities included in the study consisted of both public and private hospitals offering eye care services. These facilities were classified based on the Kenyan health system classification, as Level 4 (sub-county hospitals), Level 5 (county/regional referral hospitals), or Level 6 (national referral hospitals/teaching and research institutions).
Population and Sampling
The study population consisted of eye care practitioners (ECPs) working in eye health facilities across the Western and Nyanza regions of Kenya. For the purpose of this study, ECPs were defined as ophthalmologists, optometrists, ophthalmic clinical officers, and comprehensive ophthalmology and cataract surgeons. The number of ECPs practicing in the study area was determined using data obtained from relevant professional bodies, including the Optometrists Association of Kenya (OAK), the Clinical Officers Council of Kenya (COC-K), and the Kenya Medical Practitioners, Pharmacists and Dentists Union (KMPDU). Based on these records, a total of 143 ECPs were identified to be actively working in the Western and Nyanza regions. Due to the small population size, a census approach was used to minimize sampling bias and ensure complete representation. The study only included participants who were actively in practice and willingly gave their consent to participate in the study. Participants who did not consent to the study were excluded.
Data Collection Methods
Data were collected using a structured online questionnaire on Google forms. The questionnaire was developed and designed for this study. The questionnaire gathered information on the socio-demographic characteristics of the eye care practitioners (ECPs), including age, gender, academic qualifications, institution of training, highest level of education attained, years of professional experience, county of practice, the level of the health facility (Level 4, 5, or 6) and the type of facility (public or private). Additional data were collected on the availability and utilization of diagnostic equipment for keratoconus, and the working condition of the available equipment. The working condition was basically considered as the state of the equipment in terms of optimal maintenance, tear and wear, structural and functional quality.
To ensure the validity and reliability of the data collection tool, a pilot study was conducted in Kiminini Constituency, Trans-Nzoia County, Kenya. Ten ECPs participated in the pilot. Feedback from the pilot study was used to refine the questionnaire, while face and content validity was done to improve on its accuracy and relevance to the research objectives. Several modifications were made following the pilot. All scaled questions were standardized to a 5-point Likert scale, replacing the initial mixture of 3-point and 5-point scales. Open-ended questions were revised to include multiple-choice options, minimizing ambiguity and simplifying response analysis. Yes/No questions were reformulated into Likert-scale format to capture a broader range of responses. Ambiguous or unclear questions were reworded to enhance clarity and respondent understanding. The final version of the questionnaire was then disseminated online, to all eligible participants across the ten counties using email, WhatsApp and professional networks.
Ethical Considerations
Ethical approval for the study was obtained from the Institutional Scientific and Ethics Review Committee of Masinde Muliro University of Science and Technology (MMUST-ISERC) (MMUST/ISERC/074/2024). A research permit (NACOSTI/P/24/39382) was granted by the National Commission for Science, Technology and Innovation (NACOSTI). In addition, permission to conduct the study was obtained from the respective health facilities where the eye care practitioners were employed.
All participants received detailed information about the purpose, procedures, and voluntary nature of the study. Informed consent was obtained electronically through a consent form that participants were required to sign before proceeding with filling the anonymous questionnaire. The research was conducted in accordance with the principles outlined in the Declaration of Helsinki.
Statistical Analysis
After completion of the questionnaire, data was saved in an Excel sheet, after which, it was cleaned and analyzed using the Statistical Package for the Social Sciences (SPSS) version 29. Descriptive statistics, including frequencies and percentages, were used to summarize the ECPS socio-demographic and professional characteristics, availability of equipment and their utilization. Inferential statistics were applied using the chi-square test to assess associations between availability of diagnostic equipment and their utilization. All statistical tests were conducted at a significance level of 0.05, with a 95% confidence interval.
Results
A total of 134 out of 143 ECPs completed the questionnaire, yielding a high response rate of 93.7%. However, the possibility of response bias cannot be entirely excluded, as practitioners from facilities with limited diagnostic equipment may have been underrepresented. The majority of respondents were male, accounting for 80 (59.7%), while females comprised 54 (40.3%). A majority of the ECPs, 71 (53.3%), reported working in private hospitals. Additionally, most respondents, 86 (64.2%), were affiliated with Level 4 hospitals, followed by 40 (29.9%) from Level 5 hospitals, and 6 (4.5%) from Level 6 hospitals. In terms of age distribution, the largest proportion of ECPs 62 (48.4%) was between 30 and 39 years of age with mean age of participants being 33.54 years, a range of 37 years and a standard deviation of ±7.97.
The study assessed the availability of essential ophthalmic equipment and consumables necessary to diagnose and manage early Keratoconus across Level 4, 5, and 6 hospitals in Western and Nyanza region. The findings reveal significant disparities in resource distribution, with basic diagnostic tools widely accessible while advanced equipment and consumables were disparagingly limited as shown in Figure 1, particularly in level 4 and 5 hospitals. Basic diagnostic equipment was consistently available possibly because they are required for routine eye examination, though it varied depending on the hospital level. Slit lamps were present in 75.0% of Level 4, 97.5% of Level 5, and all Level 6 hospitals, while direct ophthalmoscopes followed a similar trend, ie 84.1% in Level 4, 95.0% in Level 5, and 100% in Level 6. Retinoscopes were nearly equally distributed (97.7%) in Level 4, (90.0%) in Level 5, and (100%) in Level 6, which depicted high availability, possibly due to relatively lower cost. While Trial lens sets/phoropters showed greater availability in Levels 4 (96.6%) and 5 (97.5%), there was a slight decline in Level 6 (83.3%). Keratometers demonstrated an increase with the level of hospitals, with 44.3% availability in level 4 as compared to level 5 (72.5%) and (83.3%) in level 6. Advanced diagnostic tools were scarcely available across all hospital Levels, possibly due to their high procurement costs, tomographers with the lowest availability. Equally, pachymeters and topographers demonstrated low availability with slightly better availability in level 6 hospitals (50%) and (16.7%) respectively as shown in Table 1. Generally, levels 6 were more equipped as compared to the other levels, which could be due to their national referral level and teaching status.
 |
Table 1 Equipment/Consumable Available per Hospital Level, Frequency (n) and Percentages % |
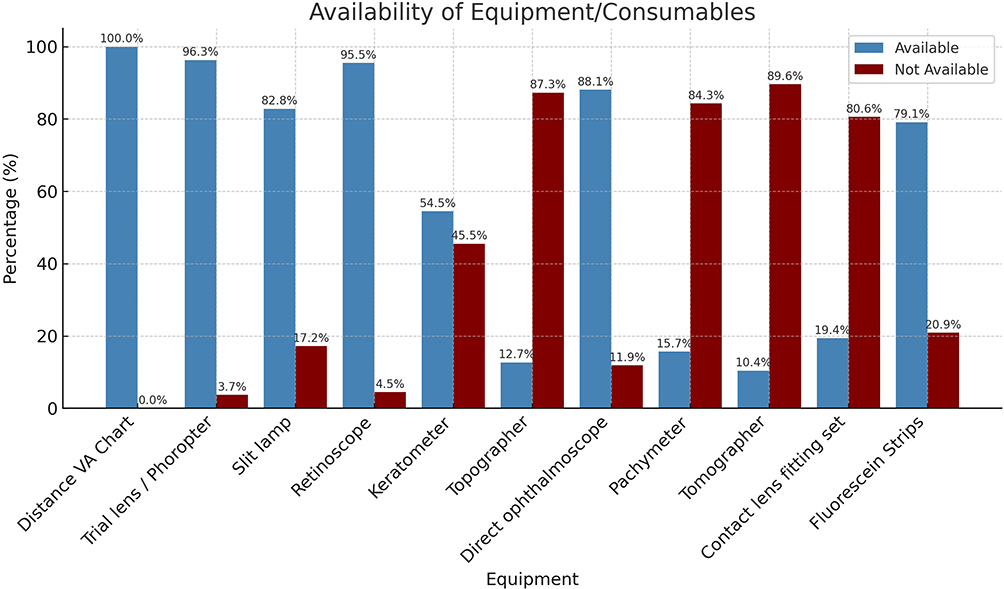 |
Figure 1 Availability/accessibility of ophthalmic equipment and consumables in place of practice, expressed as a percentage. |
In addition, this study also evaluated the quality and standards of equipment used to diagnose and manage early keratoconus. The study findings highlight that Advanced Diagnostic Equipment such as the Topographer, only 11.8% of devices exceeded standards, while 35.2% were rated as overall poor. Tomographers, while 42.3% exceeded standards, a mere 1.4% were rated as overall poor, indicating relatively better performance in this category, Pachymeters: 28.6% exceeded standards, but 19.1% were classified as overall poor. Majority of the other essential basic diagnostic equipment, Keratometers, Slit Lamps and Retinoscopes met standards with 56.2%, 59.5% and 56.3%, respectively, but a notable proportion (19.2, 13.5% and 16.4%) was rated as poor. Despite contact lens fitting sets being essential in the management of early keratoconus, it was noted that 46.1% of Contact Lens Fitting Sets were rated as overall poor, reflecting a significant deficiency in tools necessary for managing keratoconus with specialty contact lenses. As for Trial Lens Sets/Phoropters, while 57.4% met standards, 16.3% were of poor standards, potentially affecting refractive management in early cases (Table 2).
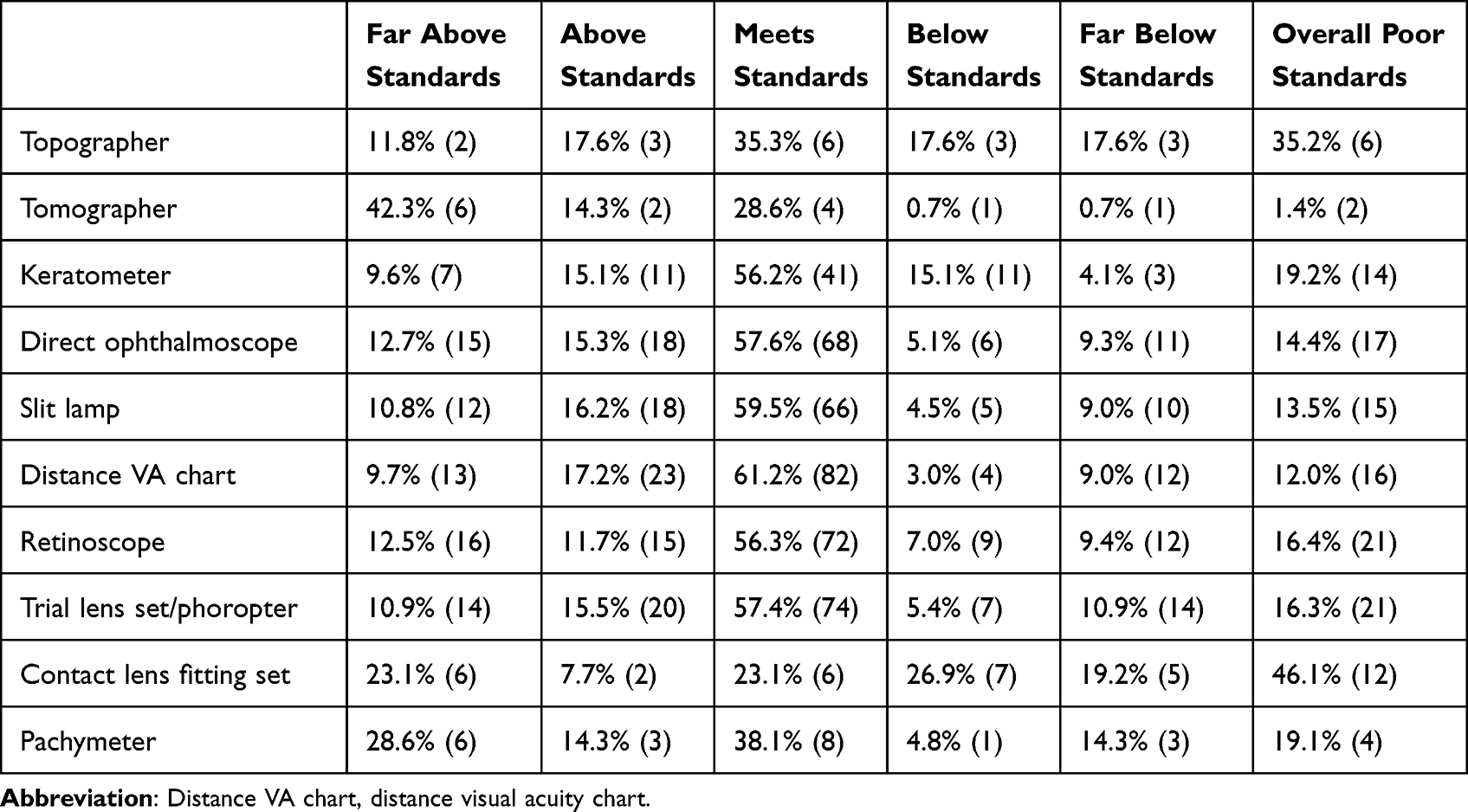 |
Table 2 Working Conditions of the Available Equipment in Percentages (%) and Frequencies (n) |
The study utilization rates of the available equipment were high especially for basic equipment such as distance VA chart (91.8%), trial lens/phoropter (89.9%), slit-lamp (78.4%) and retinoscope (75.0%), which despite it being basic, it is also able to detect early KC. The advanced equipment had lower utilization rates including the contact lens fitting set (31.0%), pachymeter (52.4%) and topographer (52.9%) as shown in Figure 2. A Chi-square determined if there was an association between equipment availability and utilization. The test showed a statistical significance between availability and utilization of distance VA chart (p=0.03333), trial lens/phoropter (p=0.00292), slit-lamp (p=0.00283) and keratometer (p=0.00001) (p-value ≤ 0.05) CI 95% as shown in (Table 3). The study found that equipment with higher availability tends to be utilized more often as seen with Distance VA chart, trial lens/phoropter, slit-lamp and keratometer.
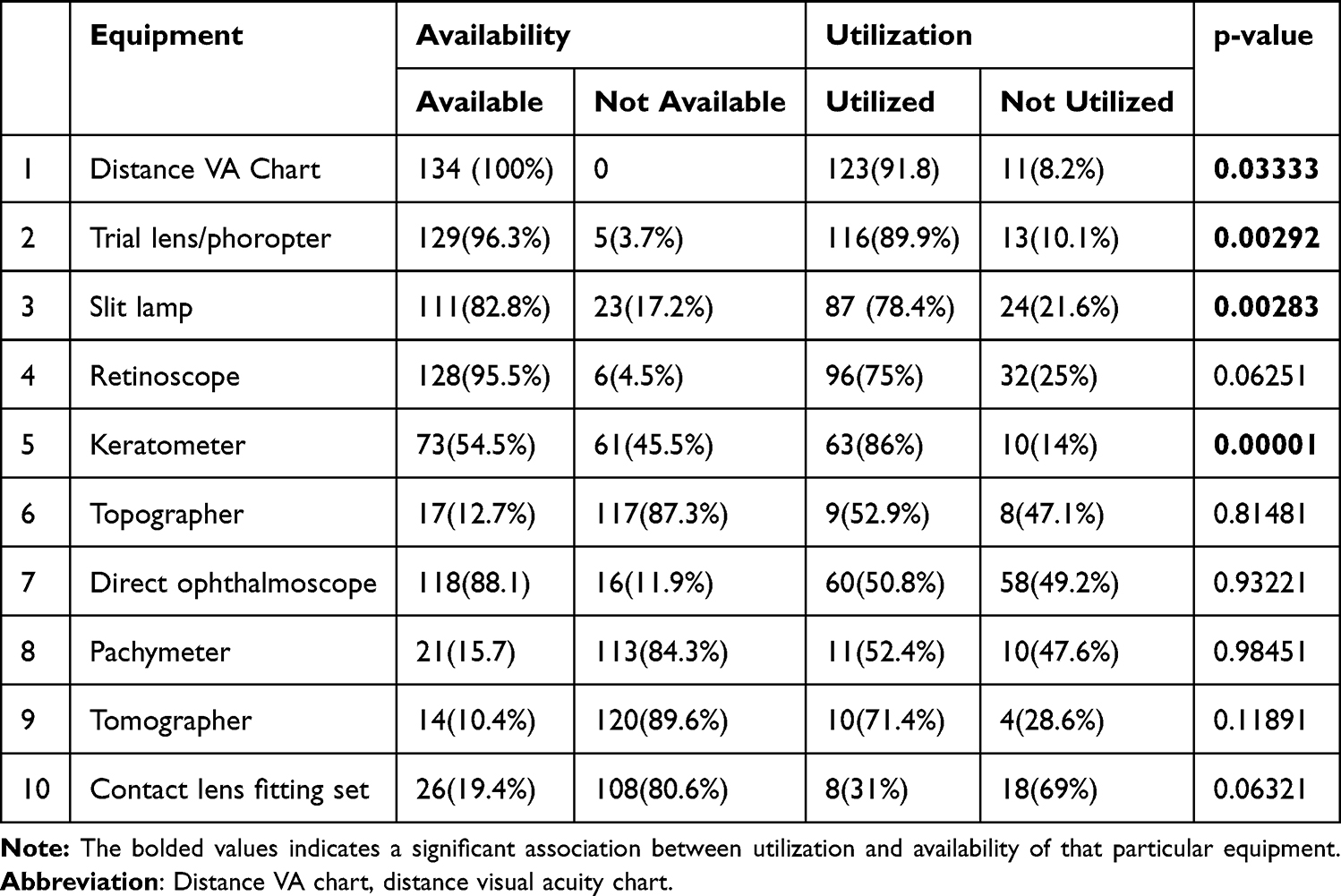 |
Table 3 Equipment Availability and Their Utilization, Chi-Square at 0.05 Significance Level and CI 95% |
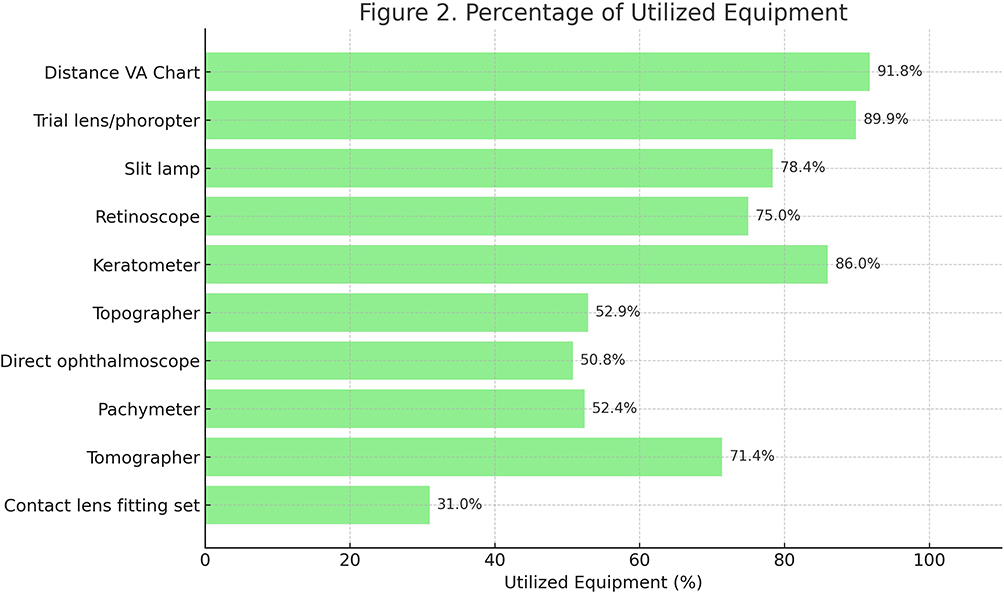 |
Figure 2 Percentage of utilization for each available ophthalmic equipment item in clinical practice, based on survey responses. |
Discussion
The availability of advanced diagnostic equipment for early keratoconus (KC) detection remains a significant challenge in many settings, as demonstrated by our findings. Similar to studies in the United Kingdom and Latin America,34–36 we found that advanced diagnostic equipment such as topographers, pachymeters, and tomographers, were scarce. The limited availability is likely due to financial constraints, a lack of prioritization for early KC screening, and knowledge gaps in equipment utilization, as identified in our study. This was, however, different from studies done in India and Saudi Arabia where the advanced equipment was available.37,38
On the other hand, the basic equipment were more readily available, possibly because of the wider range and their diverse application. The findings were consistent to a study done in Kwa Zulu, South Africa.39 This was, however, contrary to another study in South Africa where some basic equipment like the slit-lamp was not available.40 Similar to a study in South Africa,41 the tertiary hospitals, L6s had the highest availability of equipment for both the basic and the advanced equipment, with slit-lamp (100%), direct ophthalmoscope (100%), retinoscope (100%), trial lens/phoropter (83.3%) and keratometer (83.3%).
The scarcity of advanced equipment and abundance of basic equipment which are less sensitive in detecting early KC suggests that many clinicians must rely on less sensitive methods, potentially delaying detection until symptomatic stages. This leads to diagnosis of KC at late stages,18,19 as it progresses to severe state,4 which is normally expensive and risky to manage in addition to leading to visual impairment and blindness.9,42,43 It is therefore crucial to ensure that KC is diagnosed and managed at the early stages. At the early stages, KC can be managed using optical options, such as spectacles and corneal RGP contact lenses, and minor surgical intervention (cross-linking) for the progressive KC, which have less complications and are fairly less costly as compared to other surgical interventions.44,45 This would therefore present with more advantages to the KC patients as opposed to management at the late severe stages which mostly employs surgical options such as penetrating keratoplasty (PK) and deep anterior lamellar keratoplasty (DALK). Often, these are coupled with numerous disadvantages including high costs and post-surgical complications such as graft rejection.46–49 To avoid these, KC needs to be diagnosed and managed early, which is possible only if the advanced equipment is available.
This study highlights significant shortfalls on the quality of equipment used for early KC diagnosis and management. Moreover, it raises concerns about its impact on clinical outcomes. While basic diagnostic tools like Keratometers and slit lamps generally met minimum standards, advanced devices particularly topographer showed alarming variability, with only (11.8%) exceeding quality standards and (35.2%) rated as poor. Given the critical role of topography in detecting early corneal irregularities, substandard equipment risks delayed or missed diagnoses. Tomographers performed relatively better, suggesting they may offer a more reliable alternative where available. However, the prevalence of poor-quality contact lens fitting sets (46.1%) and trial lenses (16.3%) further complicates effective management, underscoring systemic challenges in keratoconus care.
These findings reveal complicated situation of limited availability and erratic equipment standard, which more often than not affects resource-limited settings, as characterised by poor working conditions such as inadequate maintenance, irregular calibration, and variable procurement standards, which likely contribute to these deficiencies, potentially compromising early detection, disease monitoring, and treatment efficacy. Addressing these issues requires standardized quality assurance programs, improved clinician training, and investment in robust technologies. Interestingly, some of the equipment was still being utilized despite their poor working condition. This would likely lead to errors in diagnosis, a possibility of overestimation or underestimation or both altogether.
Our study revealed a critical gap between equipment availability and actual utilization. Even when diagnostic tools were present, they were not fully utilized, consistent with findings by Motowa and Morjaria.37 This underutilization may stem from a lack of training and confidence among practitioners, further contributing to missed early KC. This draws on the need to research on knowledge levels. This was, however, different from a study in Trinidad and Tobago, which reported that the available equipment was put in use.50 When the equipment is available, the ECPs will be able to use them as depicted in this study. Ensuring availability and utilization of the advanced equipment would highly benefit the KC patient, as it would enhance the diagnosis and management of early KC, thus promoting sustainable development goal (SDG) 3 on good health thus better eye health. With good eye health, the school going KC patients would perform better in class as promoted by better eye sight. With KC patients having an opportunity to be fully and comfortably involved in class work, this promotes good performance academically, thus promoting SDG 4 on education. Consequently, they become employable and being able to qualify for decent jobs, consequently promoting economic growth, thus achieving SDG 8. Equally, universal health coverage (UHC) is achieved as early KC would be accessed anywhere, anytime and at fair diagnosis and management costs.
The failure to use the equipment may consequently lead to missing out on the diagnosis of the early KC. To bridge this gap, it is imperative that practitioners fully utilize the equipment already available, ensuring timely and accurate diagnosis and better patient outcomes.
Conclusion
Accurate and timely diagnosis of early keratoconus (KC) depends on the availability and proper utilization of advanced diagnostic equipment. However, our study found that such equipment is both scarce and underutilized, with some having sub-standard quality, thus increasing the risk of missed diagnoses. Additionally, healthcare institutions and policymakers should prioritize the procurement and maintenance of essential diagnostic equipment to bridge this gap. The Ministry of Health should collaborate with other stakeholders to develop and integrate early KC detection into national eye care guidelines. Policy strengthening of early KC diagnosis will not only enhance patient outcomes but also improve the overall quality of eye care services.
Abbreviations
KC, keratoconus; VA, visual acuity; MMUST, Masinde Muliro University of Science and Technology; ECPs, Eye care practitioners; L4, level four; L5, level five; L6, level six; USA, United States of America; SDG, sustainable development goals; UHC, universal health coverage; COCs, comprehensive ophthalmology and cataract surgeons; OCOs, ophthalmic clinical officers; SPSS, statistical package for social sciences; ISREC, institutional scientific and ethics review committee; NACOSTI, national commission for science, technology and innovation; ICRS, intracorneal ring segments, PK, penetrating keratoplasty; DALK, deep anterior lamellar keratoplasty.
Data Sharing Statement
Data generated during this study is included in this article. Further data can be accessed on request from the corresponding author.
Ethical Approval and Informed Consent
The ethical approval for this study was obtained from NACOSTI (NACOSTI/P/24/39382) and the biomedical research approval from MMUST-ISERC (MMUST/ISERC/074/2024). The research was carried out in accordance with the tenets of the Helsinki Declaration. On the online questionnaire, information regarding the study was given on the preamble and a question on whether they consented to the study was asked. One could only proceed on with the study if they indicated a “YES” to the consent; otherwise, one could not proceed to the questionnaire. These consenting cues were approved by the biomedical research committee of MMUST-ISERC and NACOSTI.
Acknowledgments
The authors would like to thank the ophthalmologists, the optometrists, the OCOs, the academicians and the researchers that helped review the questionnaire. Additionally, thank you to the OCOs, the COCs, the ophthalmologists and the optometrists who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Martínez-Abad A, Piñero DP. New perspectives on the detection and progression of keratoconus. J Cataract Refract Surg. 2017;43(9):1213–1227. doi:10.1016/j.jcrs.2017.07.021
2. Zhou W, Yu H, Feng Y. Decrease in tear film lipid layer thickness in patients with keratoconus. J Clin Med. 2022;11(18):5252. doi:10.3390/jcm11185252
3. Cruz-Becerril A, Valdivia A, Peralta R, Dominguez-Fernandez RN, Castro-Reyes MA. Prevalence of refractive errors in Mexican patients with keratoconus. OPTO. 2015;39. doi:10.2147/OPTO.S80654
4. Pinheiro-Costa J, Correia PJ, Pinto JV, et al. Increased choroidal thickness is not a disease progression marker in keratoconus. Sci Rep. 2020;10(1):19938. doi:10.1038/s41598-020-77122-x
5. Gomes JAP, Tan D, Rapuano CJ, et al. Global consensus on keratoconus and ectatic diseases. Cornea. 2015;34(4):359. doi:10.1097/ICO.0000000000000408
6. Santodomingo-Rubido J, Carracedo G, Suzaki A, Villa-Collar C, Vincent SJ, Wolffsohn JS. Keratoconus: an updated review. Contact Lens Anterior Eye. 2022;45(3):101559. doi:10.1016/j.clae.2021.101559
7. Belin MW, Duncan JK. Keratoconus: the ABCD grading system. Klin Monbl Augenheilkd. 2016;233(6):701–707. doi:10.1055/s-0042-100626
8. Bevara A, Vaddavalli PK. The evolution of diagnostics for keratoconus: from ophthalmometry to biomechanics. Seminars Ophthalmol. 2023;38(3):265–274. doi:10.1080/08820538.2022.2152716
9. Espandar L, Meyer J. Keratoconus: overview and update on treatment. Middle East Afr J Ophthalmol. 2010;17(1):15–20. doi:10.4103/0974-9233.61212
10. Hashemi H, Heydarian S, Hooshmand E, et al. The prevalence and risk factors for keratoconus: a systematic review and meta-analysis. Cornea. 2020;39(2):263. doi:10.1097/ICO.0000000000002150
11. Hwang S, Lim DH, Chung TY. Prevalence and incidence of keratoconus in South Korea: a nationwide population-based study. Am J Ophthalmol. 2018;192:56–64. doi:10.1016/j.ajo.2018.04.027
12. Özalp O, Atalay E, Yıldırım N. Prevalence and risk factors for keratoconus in a university-based population in Turkey. J Cataract Refract Surg. 2021;47(12):1524. doi:10.1097/j.jcrs.0000000000000669
13. Althomali TA, Al-Qurashi IM, Al-Thagafi SM, Mohammed A, Almalki M. Prevalence of keratoconus among patients seeking laser vision correction in Taif area of Saudi Arabia. Saudi J Ophthalmol. 2018;32(2):114–118. doi:10.1016/j.sjopt.2017.11.003
14. Al-Amri AM. Prevalence of keratoconus in a refractive surgery population. J Ophthalmol. 2018;2018(1):5983530. doi:10.1155/2018/5983530
15. Ljubic AD. Keratoconus and its prevalence in Macedonia. Macedonian J Med Sci. 2009;2(1):58–62. doi:10.3889/MJMS.1857-5773.2009.0034
16. Munir SZ, Munir WM, Albrecht J. Estimated prevalence of keratoconus in the United States from a large vision insurance database. Eye & Contact Lens. 2021;47(9):505. doi:10.1097/ICL.0000000000000812
17. Akowuah PK, Kobia-Acquah E, Donkor R, Adjei-Anang J, Ankamah-Lomotey S. Keratoconus in Africa: a systematic review and meta-analysis. Ophthalmic Physiol Opt. 2021;41(4):736–747. doi:10.1111/opo.12825
18. Saro AS, Radwan GA, Mohammed UA, Abozaid MA. Screening for keratoconus in a refractive surgery population of upper Egypt. Delta J Ophthalmol. 2018;19(1):19. doi:10.4103/DJO.DJO_39_17
19. Rupnarain S, Madlala N, Memela N, et al. Clinical characteristics of keratoconus patients at the University of KwaZulu-Natal eye clinic. Afr Vision Eye Health. 2020;79(1):7. doi:10.4102/aveh.v79i1.528
20. Mugho SN. Prsevalence of keratoconus in patients with allergic conjunctivitis attending Kenyatta national hospital eye clinic. 2016. Available from: http://erepository.uonbi.ac.ke/handle/11295/99080.
21. Rashid ZA, Moodley VR, Mashige KP. Prevalence and demographic profile of keratoconus among high school students in Kenya. Int Ophthalmol. 2023;19. doi:10.21203/rs.3.rs-3697729/v1
22. Lee HK, Jung EH, Cho BJ. Epidemiological association between systemic diseases and Keratoconus in a Korean population: a 10-year nationwide cohort study. Cornea. 2020;39(3):348. doi:10.1097/ICO.0000000000002206
23. Yego WK, Chemjor H. Profile and performance of rigid gas permeable and scleral lenses on Keratoconic patients in the developing contact lens practice settings. Open J Ophthalmol. 2020;10(03):201. doi:10.4236/ojoph.2020.103021
24. Kibet Yego W, Moodley VR. Visual acuity and refractive error improvement in Keratoconic patients: a low-income context management perspective. Clin Optom. 2020;12:113–122. doi:10.2147/OPTO.S258905
25. Rashid ZA, Moodley VR, Mashige KP. Diagnosis and management of keratoconus by eye care practitioners in Kenya. BMC Ophthalmol. 2023;23(1):37. doi:10.1186/s12886-023-02792-w
26. Junior Obinwanne C, Barrah S, Kobia-Acquah E, Titiati PE, Karikari LAA, Akowuah P. Referral pattern and comanagement of patients with Keratoconus in West Africa: a survey-based study of optometrists in Ghana and Nigeria. Eye Contact Lens. 2025;51(2):70. doi:10.1097/ICL.0000000000001139
27. MOH-Kenya. 2020. Available from: http://guidelines.health.go.ke:8000/media/National_Eye_Health_Strategic_Plan-_2020-2025.pdf.
28. Nyawira L, Tsofa B, Musiega A, et al. Management of human resources for health: implications for health systems efficiency in Kenya. BMC Health Serv Res. 2022;22(1):1046. doi:10.1186/s12913-022-08432-1
29. Mbindyo R, Kioko J, Siyoi F, et al. Legal and institutional foundations for universal health coverage, Kenya. Bull World Health Organ. 2020;98(10):706–718. doi:10.2471/BLT.19.237297
30. JKUAT. BSc. comprehensive ophthalmology and cataract surgery. Jomo Kenyatta University of Agriculture and Technology. 2025. Available from: https://www.jkuat.ac.ke/bsc-comprehensive-ophthalmology-and-cataract-surgery/.
31. Singh P, Jain N, Verma S, Sharma B. Commentary: ophthalmology training programs: optimization of human resource to supplement clinical expertise and strengthen eye care delivery systems. Indian J Ophthalmol. 2023;71(1):274. doi:10.4103/ijo.IJO_2222_22
32. Thulasiraj R. Primary eye care – key to universal eye health. Indian J Ophthalmol. 2022;70(5):1448. doi:10.4103/ijo.IJO_740_22
33. Krishnaveni G, Joseph S, Thulasiraj R. Uptake pattern of training programs over two decades at an international ophthalmic training institute in India. Indian J Ophthalmol. 2023;71(1):268. doi:10.4103/ijo.IJO_1196_22
34. Hodge C, Chan C, Zantos S, Kokkinakis J, Stapleton F, Sutton G. Therapeutic treatment of keratoconus: a survey of local optometric practice criteria. Clin Exp Optometry. 2015;98(4):312–318. doi:10.1111/cxo.12233
35. Alatawi SK. Quality of life of a sample of people with keratoconus in KSA. J Taibah Univ Sci. 2023;18(5):1157–1169. doi:10.1016/j.jtumed.2023.03.008
36. Ortiz-Toquero S, Martin R. Current optometric practices and attitudes in keratoconus patient management. Contact Lens Anterior Eye. 2017;40(4):253–259. doi:10.1016/j.clae.2017.03.005
37. Al Motowa S, Khandekar R, Al-Towerki A. Resources for eye care at secondary and tertiary level government institutions in Saudi Arabia. Middle East Afr J Ophthalmol. 2014;21(2):142–146. doi:10.4103/0974-9233.129761
38. Naidoo K, Arvind A, Abesamos-Dichoso C, Tan KO, Govender-Poonsamy P. Optometry in South-East Asia. In: Das T, Nayar PD editors. South-East Asia Eye Health: Systems, Practices, and Challenges. Springer; 2021:303–311. doi:10.1007/978-981-16-3787-2_18
39. Maake ME, Moodley VR. An evaluation of the public sector optometric service provided within the health districts in KwaZulu-Natal, South Africa. Afr Vision Eye Health. 2018;77(1):1–9. doi:10.4102/aveh.v77i1.407
40. Nkoana PMW, Mashige KP, Moodley VR. Strengthening keratoconus management systems in South African public sector facilities. Afr Vision Eye Health. 2024;83(1):1–11. doi:10.4102/aveh.v83i1.832
41. Buthelezi LM, van Staden D. Integrating eye health into policy: evidence for health systems strengthening in KwaZulu-Natal. Afr Vision Eye Health. 2020;79(1):10. doi:10.4102/aveh.v79i1.549
42. Prabhu SS, Kaakeh R, Sugar A, Smith DG, Shtein RM. Comparative cost-effectiveness analysis of descemet stripping automated endothelial keratoplasty versus penetrating keratoplasty in the United States. Am J Ophthalmol. 2013;155(1):45–53.e1. doi:10.1016/j.ajo.2012.06.014
43. Roe RH, Lass JH, Brown GC, Brown MM. The value-based medicine comparative effectiveness and cost-effectiveness of penetrating keratoplasty for keratoconus. Cornea. 2008;27(9):1001. doi:10.1097/ICO.0b013e31817bb062
44. Godefrooij DA, et al. What are the costs of corneal cross-linking for the. - google scholar. 2016. Available from: https://scholar.google.com/scholar?hl=en&as_sdt=0%2C5&q=What+Are+the+Costs+of+Corneal+Cross-linking+for+the+Treatment+of+Progressive+Keratoconus%3F+Daniel+A.+Godefrooij%2C+MD%2C+Pepijn+van+Geuns%2C+BSc%2C+G.+Ardine+de+Wit%2C+PhD%2C+and+Robert+P.+L.+Wisse%2C+MD%2C+PhD&btnG=.
45. Salmon HA, Chalk D, Stein K, Frost NA. Cost effectiveness of collagen crosslinking for progressive keratoconus in the UK NHS. Eye. 2015;29(11):1504–1511. doi:10.1038/eye.2015.151
46. Edelstein SL, DeMatteo J, Stoeger CG, Macsai MS, Wang CH. Report of the eye bank association of America medical review subcommittee on adverse reactions reported from 2007 to 2014. Cornea. 2016;35(7):917–926. doi:10.1097/ICO.0000000000000869
47. Musa FU, Patil S, Rafiq O, Galloway P, Ball J, Morrell A. Long-term risk of intraocular pressure elevation and glaucoma escalation after deep anterior lamellar keratoplasty. Clin Exp Ophthalmol. 2012;40(8):780–785. doi:10.1111/j.1442-9071.2012.02796.x
48. Zhang YM, Wu SQ, Yao YF. Long-term comparison of full-bed deep anterior lamellar keratoplasty and penetrating keratoplasty in treating keratoconus. J Zhejiang Univ Sci B. 2013;14(5):438–450. doi:10.1631/jzus.B1200272
49. Cursiefen C, Schaub F, Bachmann B. Update: tiefe anteriore lamelläre Keratoplastik (DALK) bei Keratokonus. Ophthalmologe. 2016;113(3):204–212. doi:10.1007/s00347-015-0204-6
50. Braithwaite T, Winford B, Bailey H, et al. Health system dynamics analysis of eyecare services in Trinidad and Tobago and progress towards vision 2020 goals. Health Policy Plann. 2018;33(1):70–84. doi:10.1093/heapol/czx143
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.