Back to Journals » Patient Preference and Adherence » Volume 20
Artificial Intelligence in Medication Adherence: A National Assessment of Knowledge, Attitudes, and Perceptions Among Chronic Disease Patients in Jordan
Authors Merdas ZJ, Abed A ![]() , Zakaria ZZ
, Zakaria ZZ ![]() , Abu Assab M
, Abu Assab M ![]() , Abu Dayyih W, Almbaideen WA
, Abu Dayyih W, Almbaideen WA ![]() , Zakaraya Z, Bustami M
, Zakaraya Z, Bustami M ![]()
Received 31 December 2025
Accepted for publication 24 March 2026
Published 31 March 2026 Volume 2026:20 592602
DOI https://doi.org/10.2147/PPA.S592602
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Zekrayat JH Merdas,1 Anas Abed,2 Zain Z Zakaria,3 Mohammad Abu Assab,4 Wael Abu Dayyih,5 Wasan A Almbaideen,5 Zainab Zakaraya,2 Mona Bustami6
1Pharmacy Department, College of Pharmacy, Amman Arab University, Amman, Jordan; 2Department of Biopharmaceutics and Clinical Pharmacy, Faculty of Pharmacy, Al-Ahliyya Amman University, Amman, Jordan; 3Clinical Affairs Department, Qatar University, Doha, Qatar; 4Clinical Pharmacy Department, Faculty of Pharmacy, Zarqa University, Zarqa, Jordan; 5Faculty of Pharmacy, Mutah University, Alkarak, Jordan; 6Faculty of Pharmacy, University of Petra, Amman, Jordan
Correspondence: Anas Abed, Department of Biopharmaceutics and Clinical Pharmacy, Faculty of Pharmacy, Al-Ahliyya Amman University, Amman, Jordan, Email [email protected]
Purpose: To assess knowledge, attitudes, and perceptions toward AI-based medication adherence tools in a national cross-sectional survey among Jordanian adults with chronic diseases and to identify factors associated with favorable acceptance.
Patients and Methods: A national cross-sectional online survey was conducted between January and July 2025 using convenience and snowball sampling and a self-developed, pilot-tested, and content-validated Arabic questionnaire. The questionnaire captured sociodemographic characteristics, digital literacy, chronic disease information, and KAP toward AI-based medication adherence tools. Knowledge was assessed using eight statements describing AI capabilities and rated on a five-point Likert scale, which were recoded dichotomously for scoring (score range 0– 8; ≥ 5 indicating good knowledge). Attitudes and perceptions were measured using five-point Likert scales (mean scores ≥ 3.5 indicating positive or high levels). Descriptive statistics, chi-square tests, multivariable logistic regression, sensitivity analyses, and polypharmacy subgroup analyses were performed to identify factors associated with favorable acceptance.
Results: Among 552 participants (mean age 52.7 ± 12.6 years; 56.3% female), the most prevalent chronic diseases were hypertension (213, 38.6%) and diabetes mellitus (179, 32.4%), with 154 (27.9%) reporting polypharmacy (≥ 5 medications). 59.2% demonstrated good knowledge (mean score 5.3 ± 1.8). Moderately positive attitudes were observed in 48.6% (mean 3.6 ± 0.9), while 52.7% reported high perceptions (mean 3.7 ± 0.9). Strong support was reported for AI-based reminders (80%) and educational functions (76%), whereas endorsement of predictive features was lower (49– 58%). Major concerns included privacy (71%), technical reliability, and reduced human interaction. Chi-square tests showed significant associations with age and digital literacy (p < 0.001). Multivariable logistic regression confirmed that younger age, higher education, advanced digital literacy, and smartphone ownership independently predicted favorable KAP (p < 0.001). Polypharmacy was associated with greater receptivity in unadjusted analyses but was not an independent predictor after adjustment. Findings remained robust in sensitivity analyses.
Conclusion: Jordanian patients with chronic diseases show moderate-to-good knowledge and cautiously positive attitudes toward AI-enabled medication adherence tools. Acceptance is shaped mainly by digital literacy and trust, underscoring the need for governance frameworks, clinician oversight, Arabic-language design, and targeted digital literacy initiatives to support equitable integration into national platforms such as Hakeem.
Keywords: digital public health, medication adherence, digital health literacy, patient acceptance, health equity, chronic disease management
Introduction
Chronic diseases represent a major public health challenge in Jordan, where conditions such as hypertension, diabetes mellitus, cardiovascular diseases, and asthma account for a substantial proportion of morbidity and healthcare utilization.1 The increasing life expectancy and the shift toward a more urbanized lifestyle have contributed to a rising burden of chronic medication use.2 However, despite the availability of effective therapies, medication non-adherence remains a critical barrier to achieving optimal health outcomes.3
Recent national data from Jordan indicate that medication non-adherence affects approximately 45.7% of patients with multimorbidity (defined as high adherence rate of only 54.3% using the validated General Medication Adherence Scale). Condition-specific adherence rates in this population were 53.9% for hypertension, 54.0% for diabetes mellitus, 54.8% for cardiovascular/heart disease, and 53.7% for asthma.4 Also, studies conducted in Jordan have consistently shown that non-adherence is influenced by multiple factors, including complex medication regimens, limited follow-up, high out-of-pocket costs, drug shortages, inadequate patient counselling, and cultural beliefs surrounding medications.4–7 These adherence gaps contribute to disease progression, increased hospitalizations, and higher healthcare costs, placing considerable strain on an already pressured healthcare system.
Globally, artificial intelligence (AI) is emerging as a transformative tool in healthcare, offering advanced capabilities in clinical decision support, patient monitoring, predictive analytics, and personalized treatment optimization.8,9 AI-enabled applications have demonstrated value in improving medication adherence through automated reminders, refill notifications, educational support, risk prediction, and remote monitoring.10 Unlike conventional digital health interventions that rely primarily on basic reminders (such as SMS alerts or standard mobile applications), AI-enabled adherence tools incorporate advanced capabilities including predictive analytics to forecast non-adherence risk, machine learning-driven personalization of interventions, real-time pattern recognition in adherence behavior, and adaptive patient education tailored to individual needs and contexts.11 Although several countries have integrated AI into routine care pathways, its adoption varies significantly based on health infrastructure, digital literacy, and regulatory readiness.12–15
In the Middle East, AI-driven healthcare is rapidly evolving, yet its application in medication adherence remains limited. Most available evidence comes from Gulf countries with highly digitized health systems, such as Saudi Arabia, where patients demonstrate relatively high awareness of AI tools and electronic health applications .16 In contrast, Jordan is at an earlier stage of digital health integration. While initiatives such as the Hakeem electronic health record system and national digital transformation strategies have improved data accessibility, AI applications specifically targeting patient behaviour and adherence support remain underdeveloped. Moreover, disparities in healthcare access between urban and rural areas, variations in digital literacy across age groups, and the absence of unified AI governance frameworks may influence public acceptance and perceptions of AI in healthcare.
Understanding how Jordanian patients perceive AI tools, and whether they trust them, has become increasingly important. As healthcare providers explore digital solutions to improve self-management and reduce clinic burden, patient-centered insights are essential for designing effective AI-based interventions. Yet, to date, there is a notable gap in local research exploring Jordanian patients’ knowledge, attitudes, and perceptions (KAP) regarding the use of AI to enhance medication adherence. Without such evidence, policymakers and digital health developers cannot accurately design or implement AI-supported adherence programs that meet patient needs and align with cultural and technological readiness.
Given Jordan’s escalating prevalence of chronic diseases, the growing complexity of long-term pharmacotherapy, and the country’s strategic movement toward digital health transformation, examining public readiness for AI-enabled adherence support is both timely and policy-relevant. Based on patterns reported in similar regional and international surveys of patient attitudes toward clinical AI, we anticipated moderate levels of knowledge and cautiously positive attitudes toward AI-supported medication adherence tools overall, with higher receptivity expected among younger patients, those with higher educational attainment, and individuals with advanced digital literacy, while concerns related to data privacy, technical reliability, and potential reduction in human interaction were expected to remain prominent. This study provides the first national assessment of Jordanian chronic disease patients’ knowledge, attitudes, and perceptions regarding AI-supported medication adherence. By characterizing patient acceptance and identifying determinants of AI readiness, this work offers critical evidence to inform the design, implementation, and ethical governance of future digital health interventions within the Jordanian health system.
Materials and Methods
Study Design
A cross-sectional analytical design was used to evaluate knowledge, attitudes, and perceptions (KAP) toward AI-based medication adherence tools among Jordanian adults with chronic diseases. This study adhered to the STROBE guidelines for reporting observational studies to ensure methodological rigor, transparency, and reproducibility.
Study Setting and Population
The study was conducted nationally in Jordan, targeting adults aged 18 years and older who self-reported at least one chronic disease requiring long-term medication (eg., hypertension, diabetes, asthma, dyslipidemia, cardiovascular diseases, thyroid disorders, or autoimmune conditions). Participants needed to reside in Jordan, read Arabic, and provide electronic informed consent. Exclusions included pregnant individuals or those unable to consent. To achieve broad representation, an online community-based approach was employed, allowing recruitment from diverse urban and rural areas without reliance on specific healthcare facilities.
Sample Size Calculation
The required sample size was estimated using OpenEpi version 3.01. Assuming a large national population and an expected prevalence of adequate AI-related knowledge of 50% (a conservative estimate used when no local data are available), a 95% confidence level and 5% margin of error yielded a minimum sample size of 384 participants.
Sampling Strategy
A non-probability convenience sampling method was applied, combined with snowballing to enhance reach. This approach is commonly used in nationwide online health surveys where the target population is community-based and not accessible through centralized registries. All eligible individuals accessing the survey link and completing it were included, aiming for national coverage across demographics. Although this non-probability convenience and snowball sampling approach enabled national reach, it carries a risk of selection bias toward more digitally literate and urban participants; this limitation is discussed further in the Limitations section.
Recruitment and Data Collection Procedures
Data were collected entirely online between January and July 2025. An electronic questionnaire was created using Google Forms and distributed through commonly used social media platforms in Jordan, including Facebook, WhatsApp, X, and Telegram. The link was also shared through chronic disease patient support groups, pharmacy community pages, university networks, and local online community groups. No direct contact occurred between the researchers and participants; all data were collected anonymously and electronically. Before accessing the questionnaire, participants viewed an information page detailing the study’s purpose, eligibility criteria, and voluntary participation. They were required to provide digital informed consent before proceeding. To prevent duplicate responses, Google Forms’ “limit to one response” function was applied for users logged into Google accounts, and IP screening was used to detect probable duplicates. Duplicate responses were further prevented by manual review of IP addresses and completion timestamps for identical patterns, and exclusion of any suspected duplicates (n = 12) prior to analysis.
Questionnaire Development and Validation
The questionnaire was originally developed based on a comprehensive literature review of AI applications in healthcare, medication adherence barriers, and existing KAP studies on digital health technologies.9,10,13,17–19 The WHO Multidimensional Medication Adherence Framework (WHO, 2003) also informed item construction by highlighting key patient-related and system-related factors relevant to adherence and their alignment with AI-enabled support tools. The final instrument included items covering sociodemographic characteristics, health-related information, knowledge of AI-supported medication adherence, and attitudes and perceptions toward AI-enabled interventions. The questionnaire was developed in Arabic to ensure linguistic accuracy, cultural appropriateness, and contextual relevance for Jordanian respondents.
A panel of seven experts in clinical pharmacy, artificial intelligence, public health, and behavioral sciences reviewed the instrument for content validity, clarity, relevance, and contextual fit. Minor revisions were made to based on the experts feedback, primarily involving clarification of terminology (eg., replacing “machine learning” with “artificial intelligence applications”), simplification of two knowledge items for readability, and addition of one example in the attitude section to improve cultural relevance for Jordanian respondents.
The final KAP section of the questionnaire consisted of 21 closed-ended items: 8 knowledge items, 7 attitude items, and 6 perception items. All items were presented as statements rated on a five-point Likert scale (strongly disagree to strongly agree). For analytical purposes, responses to the knowledge items were recoded dichotomously (agreement = correct; neutral or disagreement = incorrect/uncertain) to generate the knowledge score used in the analysis. No open-ended questions were included in the KAP domains (Supplementary Figure S1).
A pilot study involving 30 Jordanian patients with chronic diseases was conducted to assess comprehension, response consistency, and technical functionality of the online survey. These participants were excluded from the final dataset. Reliability analyses demonstrated strong internal consistency across domains, with Cronbach’s alpha values of 0.82 for knowledge items, 0.87 for attitudes, and 0.89 for perceptions. Content validity was quantified using the Item-Content Validity Index (I-CVI) and Scale-Content Validity Index (S-CVI). All items achieved I-CVI ≥ 0.86 and the overall S-CVI/Ave was 0.93, exceeding the recommended threshold of 0.80.
Questionnaire Structure and Scoring
The questionnaire consisted of four sections: (1) sociodemographics characteristics (age, gender, education level, monthly household income, governorate of residence, employment status, and smartphone ownership); (2) health-related information (type and duration of chronic disease and medication use); (3) knowledge of AI applications in medication adherence; and (4) attitudes and perceptions toward AI-supported adherence tools.
Knowledge was assessed using eight statements describing potential AI capabilities related to medication adherence. Participants rated each statement using a five-point Likert scale (1 = strongly disagree to 5 = strongly agree). For analytical purposes, responses were recoded dichotomously, where agreement with correct statements (agree or strongly agree) was coded as 1 (correct) and neutral or disagreement responses were coded as 0 (incorrect or uncertain). The summed score ranged from 0 to 8, with ≥5 indicating good knowledge and <5 indicating poor knowledge.
Attitudes and perceptions used a five-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree); mean scores ≥3.5 denoted positive/high, 3.0–3.49 neutral/moderate, and <3.0 negative/low. These thresholds were applied to generate the summary categories used in the analysis.
Digital literacy was assessed via a single self-reported item (limited/moderate/high or advanced ability) rather than a validated multi-item scale because the survey was already lengthy and the item has been shown to correlate strongly with objective digital skills in previous Jordanian health surveys, allowing efficient capture of this key predictor.
Data Management
Responses were stored on an encrypted drive accessible only to the principal investigator. Daily reviews ensured completeness, with no personal identifiers collected. After cleaning, data were exported to SPSS format.
Statistical Analysis
Data analysis was performed using IBM SPSS Statistics version 26. Descriptive statistics were used to summarize participant characteristics and responses. Categorical variables were presented as frequencies and percentages, while continuous variables were expressed as means and standard deviations after verifying normality.
Associations between demographic variables and KAP levels were examined using chi-square tests; Fisher’s exact test was applied where expected cell counts were low. Independent t-tests and Mann–Whitney U-tests were applied for continuous variables as appropriate. To identify factors associated with favorable acceptance (good knowledge, positive attitudes, and high perceptions), chi-square tests were first used for bivariate associations, followed by multivariable logistic regression models with good knowledge (≥5/8), positive attitude (mean ≥3.5), and high perception (mean ≥3.5) as dependent variables. Candidate predictors included age, sex, educational level, income, digital literacy, employment status, and number of chronic medications. All statistical tests were two-tailed, and a p-value of <0.05 was considered statistically significant. A subgroup analysis focused on polypharmacy patients (≥5 medications), and sensitivity analyses tested alternative categorization thresholds (mean ≥4.0 for positive/high attitudes/perceptions; ≥6 for good knowledge) to assess robustness of predictors.
Ethical Considerations
Ethical approval was obtained from Al-Ahliyya Amman University’s Institutional Review Board (IRB number AAU/2/5/2024 2025). Procedures followed the Declaration of Helsinki, with voluntary participation, electronic consent, withdrawal options, and strict anonymity/confidentiality.
Results
Participants Characteristics
A total of 552 participants completed the survey and met the eligibility criteria for inclusion in the final analysis. Table 1 summarizes the sociodemographic and clinical characteristics of the study population. The mean age of participants was 52.7 ± 12.6 years, with the largest group falling between 40–59 years (45.8%). Women represented 56.3% of the sample. Most participants held either a secondary school certificate (34.4%) or a university degree (49.1%), reflecting typical educational patterns in urban Jordan.
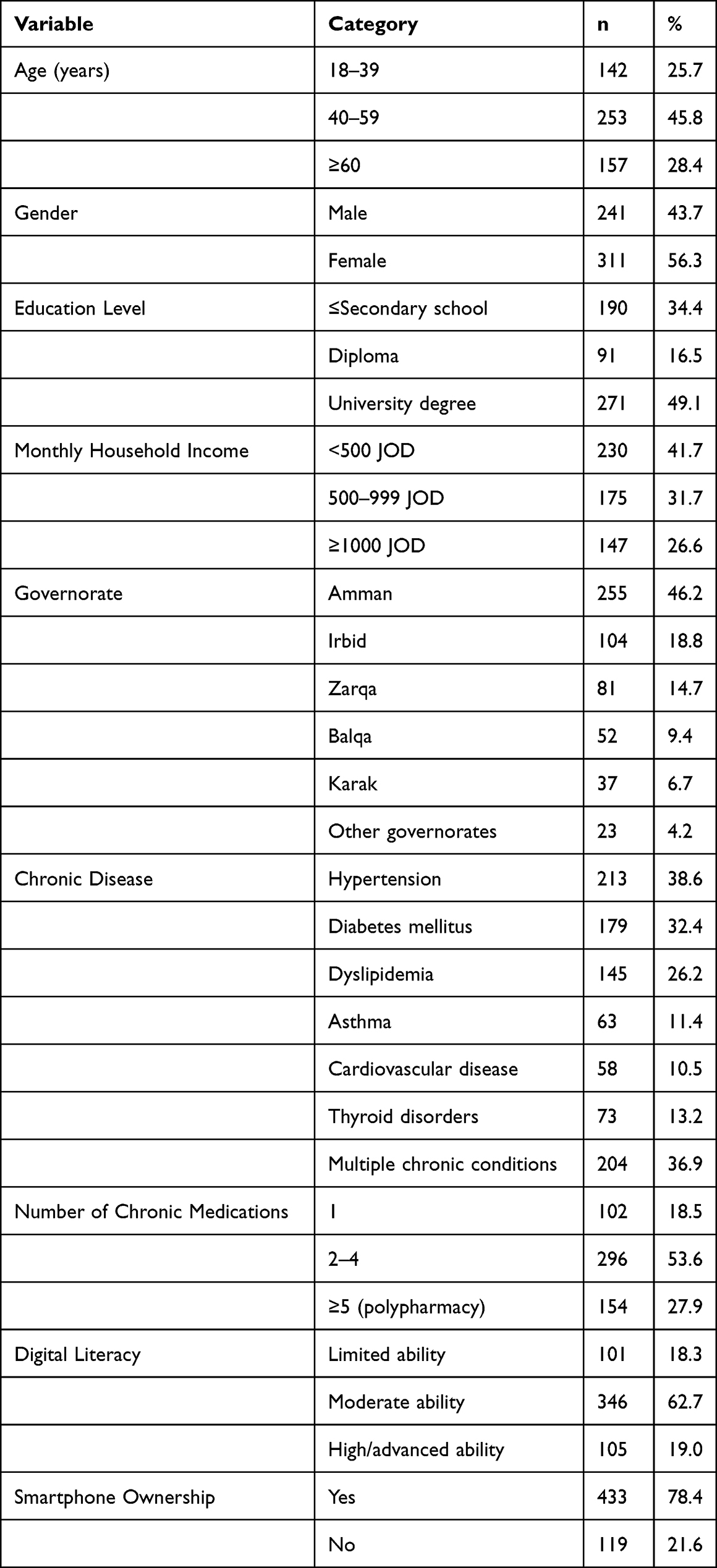 |
Table 1 Sociodemographic and Clinical Characteristics of the Study Participants (N = 552) |
Regarding income, 41.7% reported monthly household incomes below 500 JOD, consistent with national income distributions. Hypertension was the most prevalent condition (213 participants, 38.6%), followed by diabetes mellitus (179, 32.4%) dyslipidemia (145, 26.2%), asthma (63, 11.4%), cardiovascular disease (58, 10.5%), and thyroid disorders (73, 13.2%). Multiple chronic conditions were reported by 204 participants (36.9%). polypharmacy (≥5 medications) was reported by 27.9%, while 18.7% used only a single chronic medication.
Digital literacy varied with 62.7% rated themselves as “moderately able” to use digital tools, while 19.0% reported advanced digital proficiency. A majority (78.4%) owned smartphones capable of installing health-related applications.
Overall Knowledge, Attitude, and Perception Levels
Overall, 59.2% of participants demonstrated good knowledge about the potential role of AI in improving medication adherence, while 40.8% had poor knowledge (Table 2). The mean knowledge score was 5.3 ± 1.8 out of 8, suggesting moderate-to-good awareness at the population level.
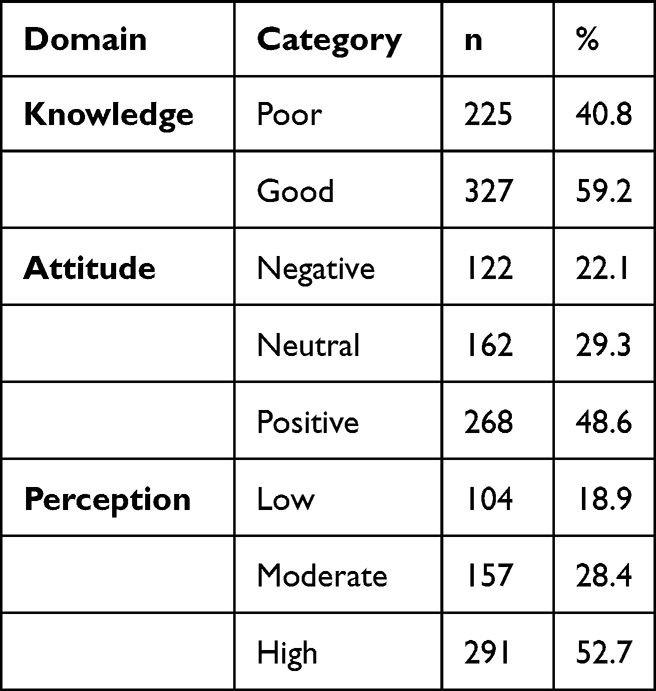 |
Table 2 Overall Knowledge, Attitude, and Perception (KAP) Levels Toward AI in Medication Adherence (N = 552) |
Attitudes toward AI were moderately positive, with 48.6% of participants exhibiting a positive attitude toward the use of AI in supporting medication adherence (mean attitude score 3.6 ± 0.9), 29.3% neutral, and 22.1% negative. Perception levels were similarly favorable, with 52.7% reporting high perception of AI’s usefulness in this context (mean perception score 3.7 ± 0.9), 28.4% moderate, and 18.9% low.
Item-Level Analysis of Knowledge, Attitude, and Perception
Item-level analysis revealed greater nuance due to the expanded five-point response options (Table 3). In the knowledge domain, participants showed strong endorsement of basic, patient-facing AI functionalities. For instance, 80% agreed or strongly agreed that AI applications can provide timely medication reminders (mean 4.0 ± 0.8), and 76% endorsed AI’s ability to deliver educational information about medications (mean 3.9 ± 0.8). Agreement remained substantial for monitoring adherence (70%; mean 3.8 ± 0.9) and managing refills (68%; mean 3.7 ± 0.9). However, support was more moderate for advanced capabilities, such as personalized treatment recommendations (61%; mean 3.6 ± 1.0), predicting adverse reactions (58%; mean 3.5 ± 1.0), and forecasting future non-adherence (49%; mean 3.4 ± 1.0), with higher neutrality on these items.
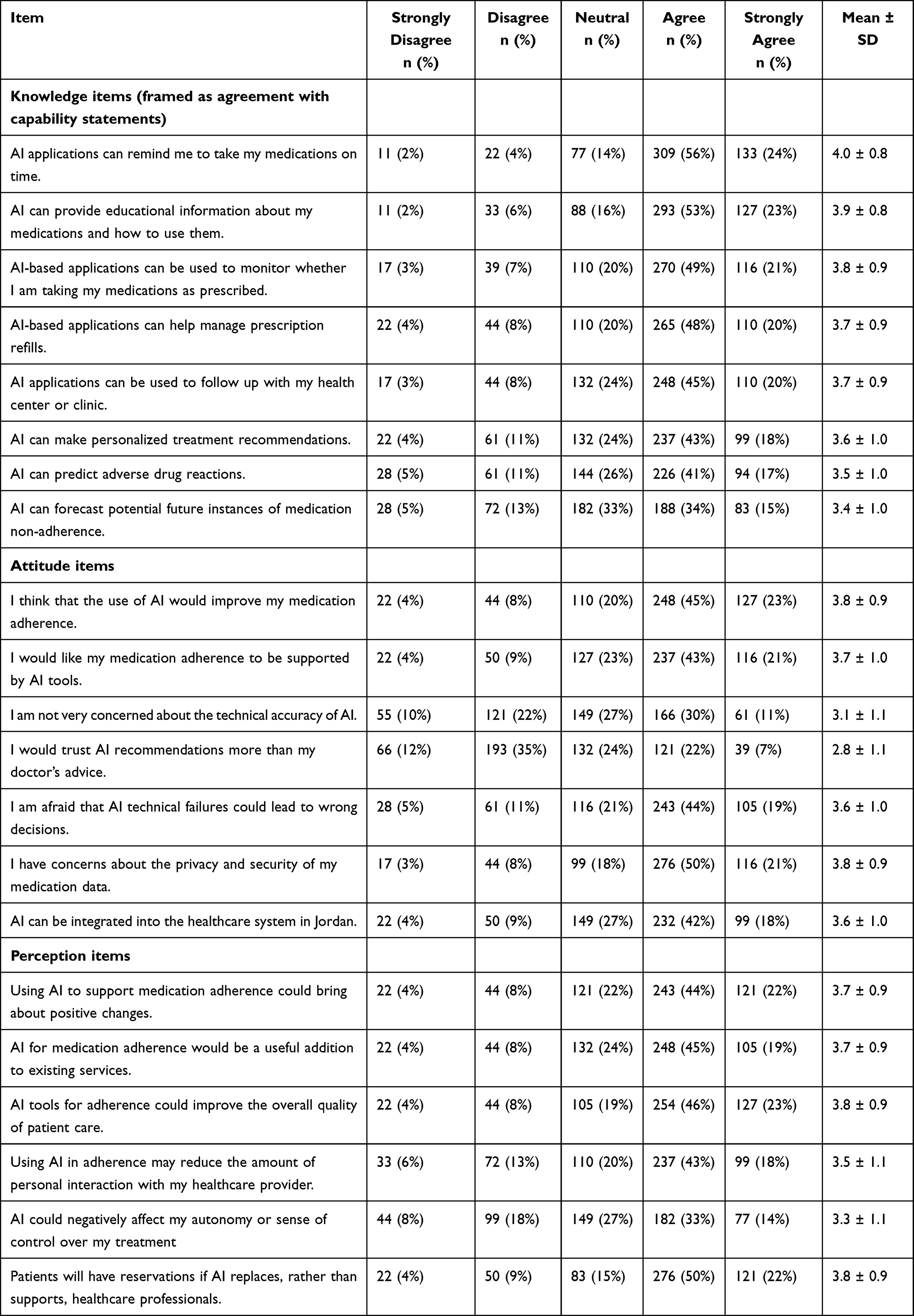 |
Table 3 Item-Level Responses for Knowledge, Attitude, and Perception Toward AI in Medication Adherence (N = 552) |
Attitudinal items reflected moderate-to-positive views overall. A majority agreed or strongly agreed that AI could improve their personal medication adherence (68%; mean 3.8 ± 0.9) and that they would welcome AI support alongside traditional care (64%; mean 3.7 ± 1.0). Integration of AI into the Jordanian healthcare system was also viewed favorably (60%; mean 3.6 ± 1.0). Concerns were evident but not overwhelming: 63% expressed worry about technical failures (mean 3.6 ± 1.0) and 71% about privacy and security of medication data (mean 3.8 ± 0.9). Notably, trust in AI recommendations over physician advice remained low (only 29% agreed or strongly agreed; mean 2.8 ± 1.1), and lack of concern about technical accuracy was limited (41%; mean 3.1 ± 1.1).
Perception items showed similar patterns of cautious optimism. Strong agreement was observed for AI improving quality of care (69%; mean 3.8 ± 0.9), bringing positive changes (66%; mean 3.7 ± 0.9), and serving as a useful addition to services (64%; mean 3.7 ± 0.9). Reservations persisted around reduced personal interaction with providers (61% agreed or strongly agreed; mean 3.5 ± 1.1), potential loss of autonomy (47%; mean 3.3 ± 1.1), and patient concerns if AI were to replace human professionals (72%; mean 3.8 ± 0.9).
Association Between Participant Characteristics and KAP Levels
We next examined how key demographic and digital characteristics were associated with KAP levels (Table 4). Age was significantly associated with all three domains. Participants aged 18–39 years were more likely to have good knowledge (69.0%) compared to those of older age (p = 0.002). A similar pattern was observed for attitudes and perceptions where positive attitudes were most common in the youngest group (57.7%) and least common in the oldest (39.5%; p = <0.001), while high perception levels declined from 59.9% in the youngest group to 44.6% in the oldest group (p = <0.001).
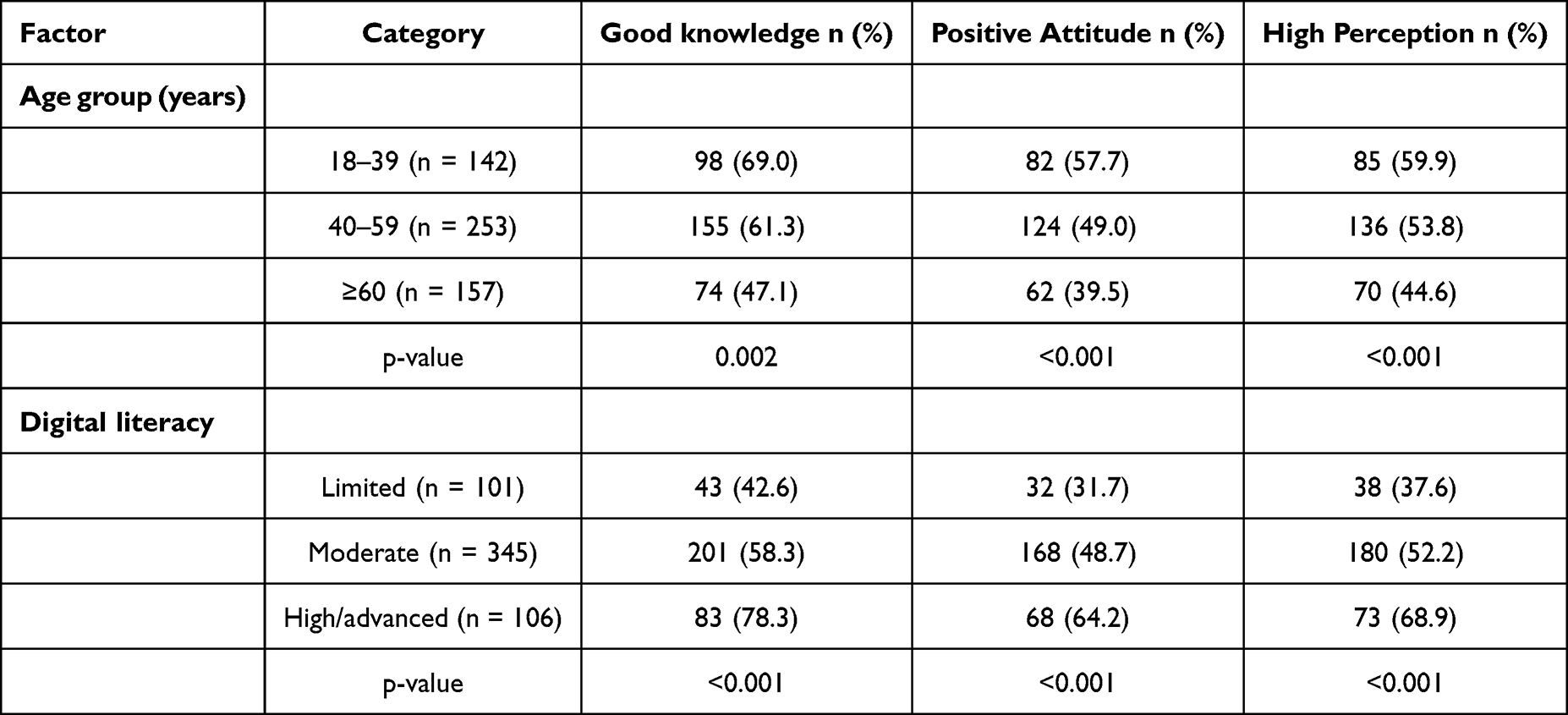 |
Table 4 Associations Between Age and Digital Literacy with Knowledge, Attitude, and Perception Levels (N = 552) |
Digital literacy showed similar association patterns. Among participants reporting high or advanced digital ability, 78.3% had good knowledge compared with 42.6% among those with limited ability (p < 0.001). Positive attitudes were also more prevalent in the high-literacy group (64.2% vs. 31.7%), and high perception levels followed the same gradient (68.9% vs. 37.6%; both p < 0.001).
Multivariable Logistic Regression Analysis
To identify independent predictors of favorable KAP, three multivariable logistic regression models were fitted with good knowledge, positive attitude (mean ≥3.5), and high perception (mean ≥3.5) as dependent variables, respectively (Table 5). After adjustment for age, sex, education, income, digital literacy, smartphone ownership, and number of chronic medications, several factors remained significantly associated.
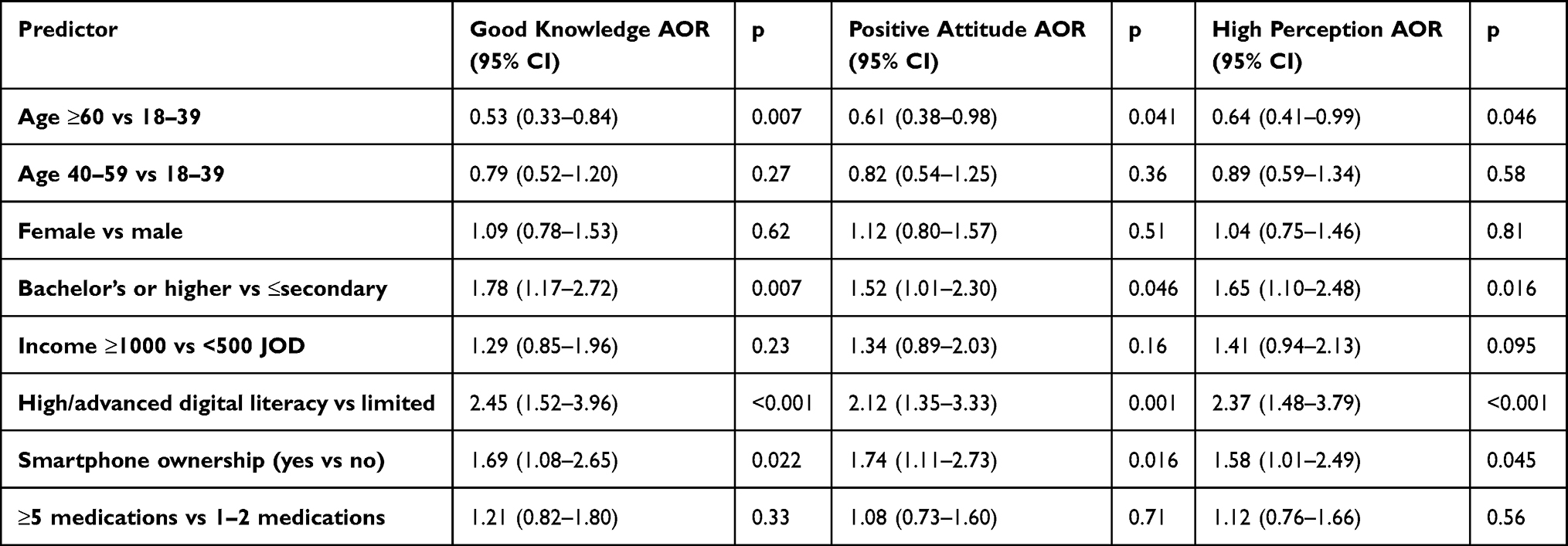 |
Table 5 Multivariable Logistic Regression Analysis of Factors Associated with Good Knowledge, Positive Attitudes, and High Perception Toward AI in Medication Adherence (N = 552) |
Younger age and higher digital literacy were the most consistent predictors across models. Compared with participants aged 18–39 years, those aged ≥60 years had significantly lower odds of good knowledge (AOR = 0.53, 95% CI 0.33–0.84; p = 0.007), positive attitudes (AOR = 0.61, 95% CI 0.38–0.98; p = 0.041), and high perceptions (AOR = 0.64, 95% CI 0.41–0.99; p = 0.046). Participants with high/advanced digital literacy had more than twice the odds of favorable outcomes in all domains compared with those with limited ability (knowledge: AOR = 2.45, 95% CI 1.52–3.96; p < 0.001; attitude: AOR = 2.12, 95% CI 1.35–3.33; p = 0.001; perception: AOR = 2.37, 95% CI 1.48–3.79; p < 0.001).
Higher education (bachelor’s or above) and smartphone ownership also independently associated with improved outcomes, including good knowledge (AOR = 1.78, 95% CI 1.17–2.72; p = 0.007), positive attitudes (AOR = 1.52, 95% CI 1.01–2.30; p = 0.046), and high perceptions (AOR = 1.65, 95% CI 1.10–2.48; p = 0.016). Smartphone ownership similarly predicted better KAP outcomes (knowledge: p = 0.022; attitude: p = 0.016; perception: p = 0.045). In contrast, income level, sex, and polypharmacy were not independently associated with any of the KAP domains.
Sensitivity Analysis
To evaluate the robustness of the categorization thresholds, sensitivity analyses were performed using stricter cutoffs (mean ≥4.0 for positive attitudes and high perceptions; ≥6 correct responses for good knowledge). The pattern of independent predictors remained consistent across all models: younger age, higher education, advanced digital literacy, and smartphone ownership were significantly associated with favorable KAP outcomes. These results confirm that the main findings are not sensitive to the choice of thresholds.
Relationships Between Knowledge, Attitudes, and Perception
Finally, we explored associations between knowledge levels and attitudes/perceptions (Table 6). Participants with good knowledge were substantially more likely to express positive attitudes and high perceptions toward AI.
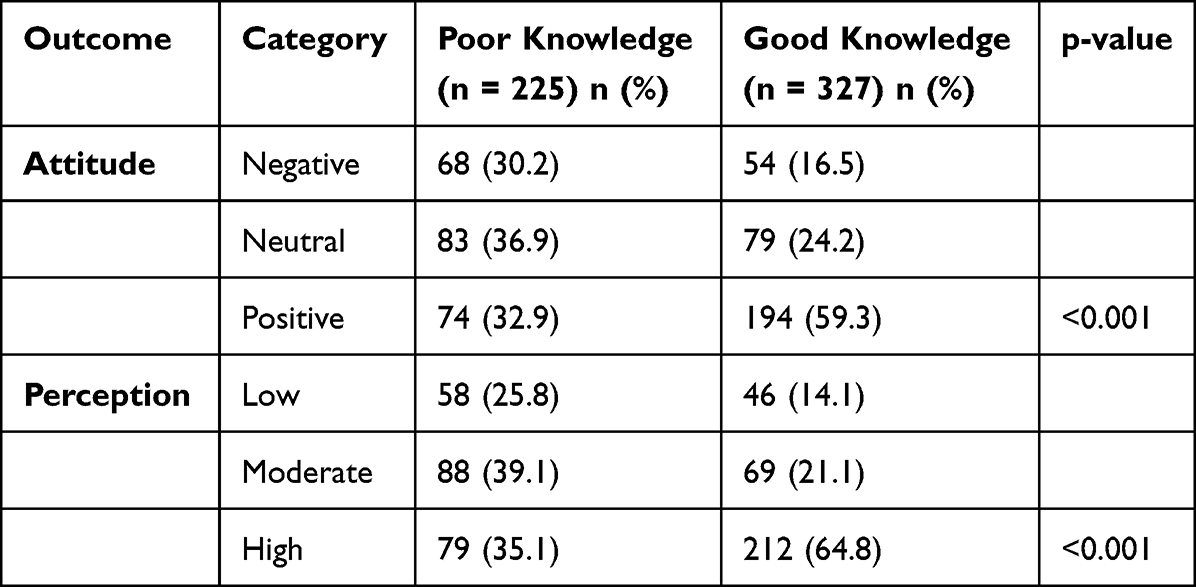 |
Table 6 Cross-Tabulation of Knowledge Level with Attitude and Perception Toward AI in Medication Adherence (N = 552) |
Among those with good knowledge, 58.4% had positive attitudes compared with 32.9% among those with poor knowledge (p < 0.001). Similarly, high perception levels were reported by 64.5% of participants with good knowledge versus 35.1% of those with poor knowledge (p < 0.001).
These stronger associations, consistent with the greater granularity offered by the five-point scale, suggest that enhancing knowledge about AI’s role, benefits, and limitations may be a key mechanism for fostering greater acceptance and more favorable perceptions among Jordanian patients with chronic diseases.
Discussion
The present study examined Jordanian patients’ knowledge, attitudes, and perceptions toward AI in supporting medication adherence. Overall, participants demonstrated moderate-to-good knowledge and moderately positive attitudes, a pattern consistent with international evidence showing that most patients possess general familiarity with AI but limited understanding of its clinical applications.20 Importantly, it is necessary to distinguish between acceptance—defined as willingness to consider or try AI tools, as captured in this cross-sectional KAP survey—and actual adoption or sustained use in routine care. The present study reflects the former, whereas future longitudinal and implementation studies will be needed to evaluate real-world utilization and adherence outcomes.
Consistent with the finding from previous global studies, younger adults, individuals with higher education, and those who frequently use digital technologies were more receptive to AI tools.20–22 Our sample showed similar demographic gradients, and patients with polypharmacy, who typically have greater caregiving demands and digital engagement, also displayed higher acceptance of AI-assisted adherence support. Good knowledge was strongly linked to more favorable attitudes and perceptions, highlighting education as a key lever. Such associations align with research demonstrating that higher AI literacy directly predicts better perceptions. Overall, this national study demonstrates moderate knowledge and cautiously positive attitudes toward AI-enabled medication adherence tools among Jordanian patients with chronic diseases, with acceptance shaped primarily by digital literacy, education, and trust-related factors. From a digital public health perspective, these findings emphasize that AI adoption is not solely a technological challenge but a behavioral, educational, and governance issue.
Regionally, our findings contribute to a consistent Middle Eastern picture in which receptivity to AI coexists with targeted reservations. Studies from the Gulf show variation: UAE citizens have expressed skepticism, especially among individuals with lower education or unstable employment,23 whereas surveys in Saudi Arabia report widespread awareness of AI and moderate-to-positive optimism regarding its role in improving care.16,24 our results align closely with these patterns, showing comparable receptivity with similar targeted reservations where Jordanian patients recognize AI’s potential but remain cautious about privacy, accuracy, and overreliance on automated systems.
Globally, patient attitudes toward AI follow similar patterns of informed optimism tempered by concern. In a 43-country multicenter survey of 13,806 hospital patients, 57.6% expressed generally positive attitudes toward clinical AI, but a strong preference remained for physician-supervised, explainable systems.25 More than 70% of respondents favored “explainable AI,” and nearly three-quarters insisted that healthcare professionals maintain final decision-making authority even if this reduced algorithmic accuracy. Parallel findings in public surveys, such as a recent Pew Research poll indicating that 60% of Americans feel uncomfortable with AI-driven medical decisions (Pew Research Center, 2023), reinforce that trust and transparency remain central determinants of AI acceptance. Our respondents expressed the same reservations in which AI was welcomed as a supportive tool but not as a replacement for clinicians.
Importantly, moderate patient knowledge and mixed attitudes do not imply resistance; instead, they highlight the need for structured education and digitally inclusive implementation. Global digital health research shows that effectiveness of AI-enabled interventions depends not only on the technology itself but on patients’ ability to understand and use it.26–28 Jordan, despite high internet penetration, still faces digital literacy gaps, particularly among older adults, rural populations, and individuals with lower socioeconomic status. Without tailored educational efforts, AI solutions risk widening rather than narrowing inequality. Our findings therefore highlight that scaling AI-supported adherence tools must be accompanied by accessible, Arabic-language, culturally appropriate patient education.
Evidence from international trials demonstrates that digital and AI-enhanced adherence tools, including reminder systems, predictive adherence algorithms, conversational agents, and real-time monitoring solutions, can meaningfully improve adherence across chronic diseases.29–32 However, effectiveness varies, and long-term success requires seamless integration into health systems rather than standalone app use. Human-centered AI remains essential where healthcare professionals must interpret AI outputs, engage patients, and contextualize recommendations. Our participants’ emphasis on human oversight directly reflects this literature and reinforces the need to maintain the primacy of such relationships.
These findings also have direct implications for clinical pharmacists, who play a central role in medication adherence management. As medication experts and highly accessible healthcare professionals, clinical pharmacists are well positioned to introduce AI-enabled adherence tools during medication counseling and chronic disease management visits. Pharmacists could use AI-supported systems to identify patients at risk of non-adherence, deliver personalized medication education, and monitor adherence patterns through digital platforms integrated with electronic health records. Importantly, pharmacists may also serve as trusted intermediaries who interpret AI-generated insights for patients, ensuring that recommendations are clinically appropriate and understandable. By combining AI-driven adherence monitoring with pharmacist-led patient education and medication review, healthcare systems may achieve more effective and patient-centered adherence support. Therefore, integrating clinical pharmacists into the implementation and governance of AI-assisted adherence tools will be essential to maximize both patient trust and clinical impact.
These insights have significant implications for Jordan’s digital health and AI policy landscape. Jordan’s National HIS Strategic Plan and AI Policy Framework already emphasize interoperability, data governance, and public trust-building (Ministry of Digital Economy & Entrepreneurship, 2020; WHO Jordan Office, 2023). The ongoing USTDA-supported expansion of the Hakeem electronic health record, which is preparing the platform for AI integration, provides a timely opportunity to embed adherence-support systems into national care pathways. Such integration could enable AI-generated reminders, predictive risk alerts, and personalized educational messaging linked directly to patient records, allowing healthcare professionals to monitor adherence support in real time and intervene promptly. Yet this must be accompanied by robust privacy protections, transparency rules, and explainability requirements to reflect patient concerns and align with WHO ethical guidance.
For successful implementation, several priorities emerge. First, AI-enabled adherence tools must be designed in Arabic, optimized for local cultural context, and accessible to individuals with varying literacy levels. Second, investments in digital health literacy programs are essential, community-based workshops and clinic-based training can support older and lower-literacy patients in using AI-enabled tools effectively. Third, trust-building measures are crucial where healthcare professionals should be central introducers of AI tools, emphasizing their supportive, and not replacement, role in care. Fourth, integration into Hakeem ensures that AI becomes part of a coordinated clinical ecosystem rather than an isolated intervention. Finally, prioritizing high-need groups, such as patients with polypharmacy or complex regimens, may yield early success and demonstrate usefulness, encouraging broader adoption.
Limitations
Several limitations should be considered when interpreting these findings. First, the cross-sectional design precludes causal inference; observed associations between demographic factors, digital literacy, and AI acceptance cannot establish directionality. Longitudinal studies are needed to assess how patient attitudes evolve with real-world exposure to AI-enabled adherence tools.
Second, the study relied on self-reported data, which may be subject to recall bias or social desirability bias, particularly regarding digital literacy and attitudes toward emerging technologies. Additionally, medication adherence behavior itself was not objectively measured, and perceptions of AI utility may not fully translate into actual usage or sustained engagement.
Third, the online, convenience-based sampling approach may have led to underrepresentation of individuals with limited internet access, lower digital literacy, or advanced age. Although this approach enabled broad national reach, it likely biased the sample toward more digitally engaged participants, potentially inflating overall knowledge and acceptance estimates.
Fourth, the study assessed hypothetical acceptance of AI-based adherence tools rather than user experiences with deployed systems. Patient perceptions may differ once AI tools are implemented in clinical practice, particularly in response to usability challenges, data governance concerns, or clinician endorsement.
Finally, while this study focused on patient perspectives, it did not capture the views of healthcare professionals, policymakers, or system administrators, whose acceptance and readiness are equally critical for successful implementation. Future mixed-methods research integrating patient, provider, and system-level perspectives will be essential to inform comprehensive AI adoption strategies.
Despite these limitations, the study offers robust, policy-relevant insights into patient readiness for AI-supported medication adherence in Jordan and provides a strong empirical foundation for future implementation and evaluation studies.
Conclusion
This study provides the first national evidence on Jordanian chronic disease patients’ readiness to engage with artificial intelligence-supported medication adherence interventions. Participants exhibited moderate-to-good knowledge and moderately positive attitudes toward AI-driven adherence solutions, with acceptance particularly pronounced among younger, more educated, and digitally literate patients, while polypharmacy showed greater receptivity in unadjusted analyses but was not an independent predictor after adjustment.
Importantly, acceptance was conditional rather than absolute. While AI-enabled reminders, educational support, monitoring, and system integration received strong endorsement, participants expressed persistent concerns, often with notable intensity, regarding data privacy, technical reliability, loss of human interaction, and over-reliance on automation. Trust in AI recommendations surpassing physician advice remained low. These findings underscore that AI in medication adherence should be positioned as a clinician-supervised supportive technology, augmenting rather than replacing professional judgment and patient–provider relationships.
From a public health perspective, the results affirm the feasibility of integrating AI-based adherence tools into Jordan’s evolving digital health infrastructure. Embedding such solutions within the national Hakeem electronic health record system presents a strategic opportunity to deliver scalable reminders, predictive alerts, and personalized education while leveraging existing data flows for real-time clinician oversight. Success, however, hinges on robust ethical governance, including stringent privacy protections, transparency, and explainability measures aligned with international standards.
Equitable implementation will require Arabic-language, culturally tailored design, accessibility across literacy levels, and targeted digital health literacy initiatives—especially for older adults and socioeconomically disadvantaged groups. Prioritizing high-need populations, such as those with polypharmacy or complex regimens, could yield early demonstrable benefits and build broader trust.
By addressing these priorities, Jordan can responsibly harness AI to strengthen medication adherence, enhance chronic disease outcomes, and advance health system efficiency while upholding patient-centered values and reducing disparities.
Future research should move beyond perception studies toward longitudinal and interventional evaluations of AI-enabled adherence tools in real clinical settings, assessing their impact on medication adherence, patient outcomes, and healthcare system efficiency.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Khamaiseh AM, Habashneh SS. Prevalence and associated factors of non-communicable chronic diseases among university academics in Jordan. PLoS One. 2024;19:e0304829. doi:10.1371/journal.pone.0304829
2. Fermini B, Bell DC. On the perspective of an aging population and its potential impact on drug attrition and pre-clinical cardiovascular safety assessment. J Pharmacol Toxicol Methods. 2022;117:107184. doi:10.1016/j.vascn.2022.107184
3. Religioni U, Barrios-Rodríguez R, Requena P, Borowska M, Ostrowski J. Enhancing therapy adherence: impact on clinical outcomes, healthcare costs, and patient quality of life. Medicina. 2025;61:153. doi:10.3390/medicina61010153
4. Abed A, Abu Assab M, Abu Dayyih W, Alotaibi BS, Alsubaie N. Medication adherence in Jordanian patients with multimorbidity: a cross-sectional mixed-methods study in outpatient clinics. Front Pharmacol. 2025;Volume 16. doi:10.3389/fphar.2025.1619023
5. Basheti IA, Hait SSE, Qunaibi EA, Aburuz S, Bulatova N. Associations between patient factors and medication adherence: a Jordanian experience. Pharm Pract. 2016;14:639.
6. Al-Qerem W, Jarab A, Eberhardt J, et al. Medication adherence among Jordanian adults with chronic conditions: a combined analysis using regression and machine learning. Ann Med. 2025;57:2548979. doi:10.1080/07853890.2025.2548979
7. Al-Sutari MM, Abdelkader RH, Ababneh NH. Determinants of medication adherence among jordanian patients with end-stage kidney disease. The Open Nurs J. 17;2023.
8. Khare PS, Shaikh SA, Havelikar U. Artificial Intelligence and precision medicine for optimizing patient care: a comprehensive review. Intell Hosp. 2025;100042. doi:10.1016/j.inhs.2025.100042.
9. Bajwa J, Munir U, Nori A, Williams B. Artificial intelligence in healthcare: transforming the practice of medicine. Futur Healthc J. 2021;8:e188–14. doi:10.7861/fhj.2021-0095
10. Babel A, Taneja R, Mondello Malvestiti F, Monaco A, Donde S. Artificial intelligence solutions to increase medication adherence in patients with non-communicable diseases. Front Digit Heal. 2021;3:669869. doi:10.3389/fdgth.2021.669869
11. Moon Z, Walsh J. Digital interventions in medication adherence: a narrative review of current evidence and challenges. Front Pharmacol. 2025;16:1632474. doi:10.3389/fphar.2025.1632474
12. Wang Z. Artificial intelligence in Chinese healthcare: a review of applications and future prospects. Biomed Eng Lett. 2025;15:1065–1072. doi:10.1007/s13534-025-00515-2
13. Cresswell K, Williams R, Dungey S, et al. A mixed methods formative evaluation of the United Kingdom National health service artificial intelligence lab. NPJ Digit Med. 2025;8:448. doi:10.1038/s41746-025-01805-w
14. Nawabi J, Eminovic S, Weissflog JS, et al. Artificial intelligence in radiology: a comparative analysis of reimbursement and regulatory developments in the US and EU. Eur J Radiol Artif Intell. 2026;5:100056. doi:10.1016/j.ejrai.2025.100056
15. Nong P, Adler-Milstein J, Apathy NC, Holmgren AJ, Everson J. Current use and evaluation of artificial intelligence and predictive models in us hospitals. Health Aff. 2025;44:90–98. doi:10.1377/hlthaff.2024.00842
16. Alsanosi SM, Aldajani A, Gheliwi H, et al. Knowledge, attitudes, and perceptions of chronic patients in saudi arabia regarding the use of artificial intelligence to improve medication adherence. Patient Prefer Adherence. 2025;19:1781–1792. doi:10.2147/PPA.S519427
17. Hasan HE, Jaber D, Al Tabbah S, et al. Knowledge, attitude and practice among pharmacy students and faculty members towards artificial intelligence in pharmacy practice: a multinational cross-sectional study. PLoS One. 2024;19:e0296884. doi:10.1371/journal.pone.0296884
18. Sharma MK. Attitude, and practice survey in health care – how does it matter? J Adv Lung Heal. 2023;4:2–3. doi:10.4103/jalh.jalh_52_23
19. Zarei F, Dehghani A, Ratansiri A, et al. ChecKAP: a checklist for reporting a knowledge, attitude, and practice (KAP) Study. Asian Pac J Cancer Prev. 2024;25:2573–2577. doi:10.31557/APJCP.2024.25.7.2573
20. Fritsch SJ, et al. Attitudes and perception of artificial intelligence in healthcare: a cross-sectional survey among patients. Digit Heal. 2022;8:20552076221116772.
21. Longoni C, Bonezzi A, Morewedge CK. Resistance to medical artificial intelligence. J Consum Res. 2019;46:629–650. doi:10.1093/jcr/ucz013
22. Doraiswamy PM, Blease C, Bodner K. Artificial intelligence and the future of psychiatry: insights from a global physician survey. Artif Intell Med. 2020;102:101753. doi:10.1016/j.artmed.2019.101753
23. Jarab AS, Al-Qerem W, Al-Hajjeh DM, et al. Artificial intelligence utilization in the healthcare setting: perceptions of the public in the UAE. Int J Environ Health Res. 2025;35:585–593. doi:10.1080/09603123.2024.2363472
24. Syed W, Babelghaith SD, Al-Arifi MN. Assessment of Saudi public perceptions and opinions towards artificial intelligence in health care. Medicina. 2024;60:938. doi:10.3390/medicina60060938
25. Busch F, Hoffmann L, Xu L, et al. Multinational attitudes toward ai in health care and diagnostics among hospital patients. JAMA Netw Open. 2025;8:e2514452. doi:10.1001/jamanetworkopen.2025.14452
26. Hogg HDJ, Martindale APL, Liu X, Denniston AK. Clinical evaluation of artificial intelligence-enabled interventions. Invest Ophthalmol Vis Sci. 2024;65:10. doi:10.1167/iovs.65.10.10
27. Arbelaez Ossa L, Rost M, Bont N, et al. Exploring patient participation in ai-supported health care: qualitative study. JMIR AI. 2025;4:e50781. doi:10.2196/50781
28. Kumar P, Sharma S, Dutot V. Artificial intelligence (AI)-enabled CRM capability in healthcare: the impact on service innovation. Int J Inf Manage. 2023;69:102598. doi:10.1016/j.ijinfomgt.2022.102596
29. Bain EE, Shafner L, Walling DP, et al. Use of a novel artificial intelligence platform on mobile devices to assess dosing compliance in a phase 2 clinical trial in subjects with schizophrenia. JMIR mHealth uHealth. 2017;5:e18. doi:10.2196/mhealth.7030
30. Gracey B, Jones CA, Cho D, et al. Improving medication adherence by better targeting interventions using artificial intelligence-a randomized control study. Value Heal. 2018;21:S76. doi:10.1016/j.jval.2018.04.532
31. da Silva VJ, et al. Commercial devices-based system designed to improve the treatment adherence of hypertensive patients. Sensors. 2019;19.
32. Nayak A, Vakili S, Nayak K, et al. Use of voice-based conversational artificial intelligence for basal insulin prescription management among patients with type 2 diabetes: a randomized clinical trial. JAMA Network Open. 2023;6:e2340232. doi:10.1001/jamanetworkopen.2023.40232
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Experiences and Perspectives of Medication Information and Use Among Arabic-Speaking Migrant Women in Sweden: A Multistage Focus Group Study
Al Musawi A, Axelsson M, Eriksson T, Rämgård M
Patient Preference and Adherence 2025, 19:305-318
Published Date: 8 February 2025