Back to Journals » Clinical and Experimental Gastroenterology » Volume 19
Artificial Intelligence in Gastrointestinal Endoscopy: Current Advances, Clinical Integration, and Future Directions: A Narrative Review
Authors Yagnik VD ![]() , Choudhary PR
, Choudhary PR ![]() , Garg P
, Garg P ![]()
Received 13 October 2025
Accepted for publication 15 March 2026
Published 24 March 2026 Volume 2026:19 573930
DOI https://doi.org/10.2147/CEG.S573930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Andreas M. Kaiser
Vipul D Yagnik,1 Prema Ram Choudhary,2 Pankaj Garg3
1Department of Surgery, Banas Medical College and Research Institute, Palanpur, Gujarat, India; 2Department of Physiology, Banas Medical College and Research Institute, Palanpur, Gujarat, India; 3Garg Fistula Research Institute, Panchkula, Haryana, India
Correspondence: Vipul D Yagnik, Department of Surgery, Banas Medical College and Research Institute, Palanpur, Gujarat, India, Email [email protected]
Background: Artificial intelligence (AI) has emerged as a transformative force in gastrointestinal (GI) endoscopy, aiming to enhance diagnostic accuracy, detection rates, and workflow efficiency. With multiple AI-assisted systems now reaching clinical use, there is a growing need to consolidate evidence regarding their performance, applications, and limitations.
Objective: To synthesize contemporary evidence from randomized trials, meta-analyses, and real-world studies to provide a clinically oriented overview of the effectiveness, limitations, and implementation challenges of artificial intelligence in gastrointestinal endoscopy, and to identify key translational gaps that justify the need for this updated review.
Methods: A structured narrative synthesis of literature from PubMed, Scopus, Web of Science, and manual reference screening (2005– 2025) was performed. Evidence was thematically analyzed across major domains including CADe, CADx, upper gastrointestinal neoplasia, capsule endoscopy, quality monitoring, implementation challenges, and real-world performance. Key lessons, translational barriers, and future research priorities were extracted. Quantitative performance estimates were derived from representative randomized controlled trials and meta-analyses and are presented as reported ranges rather than pooled analyses.
Results: CADe systems have demonstrated a consistent 15– 20% relative increase in adenoma detection rate (ADR) compared to conventional colonoscopy. CADx algorithms achieve > 90% accuracy in differentiating neoplastic from non-neoplastic polyps, supporting “resect-and-discard” strategies. AI tools in upper GI endoscopy achieve diagnostic accuracies of 88– 96% for early esophageal and gastric neoplasia, outperforming non-expert endoscopists. Despite these benefits, barriers persist—dataset bias, lack of generalizability, medicolegal ambiguity, and regulatory inconsistency.
Conclusion: AI has proven efficacy in improving detection and diagnostic precision in GI endoscopy. Future progress requires multicenter validation, standardized datasets, ethical frameworks, and clinician training to enable equitable, safe, and evidence-based integration into routine clinical practice.
Keywords: artificial intelligence, gastrointestinal endoscopy, computer-aided detection, computer-aided diagnosis, adenoma detection rate, colonoscopy, Barrett’s esophagus
Introduction
Artificial intelligence (AI) is increasingly shaping a new era in gastroenterology, revolutionizing how gastrointestinal (GI) diseases are detected, diagnosed, and managed. Its influence is now evident across several areas of GI care—enhancing lesion recognition and diagnostic precision in endoscopy, refining perioperative planning and postoperative monitoring in GI surgery, and improving the accuracy of real-time diagnostic modalities such as capsule endoscopy. In this technique, the patient swallows a tiny wireless capsule equipped with a camera that captures tens of thousands of high-resolution images throughout the gastrointestinal tract. This innovation exemplifies the technological shift currently transforming diagnostic gastroenterology. When artificial-intelligence algorithms are applied to interpret these images instantaneously, clinicians gain the ability to recognize minute mucosal changes and early disease manifestations with a level of precision and timeliness that previously was not possible.1,2
Gastrointestinal cancers—particularly those of the colon, stomach, and esophagus—remain among the leading global contributors to cancer-related illness and death. Early neoplastic transformation is notoriously difficult to recognize, as such lesions are frequently subtle and can be missed even during standard endoscopic examinations.3–5 For example, while esophagogastroduodenoscopy (EGD) is regarded as a highly sensitive procedure for detecting gastric cancer (GC), evidence shows that approximately one in ten cases may still escape diagnosis.4 Similarly, colonoscopy, despite being the established reference standard for detecting and removing colorectal neoplasms, is associated with a notable miss rate. Up to one-quarter of neoplastic polyps may go undetected in routine practice, particularly when the lesions are flat, sessile, or very small (≤5 mm in diameter). The likelihood of missing lesions also increases in patients who present with multiple or synchronous polyps. Moreover, the diagnostic performance of upper GI endoscopy varies considerably among operators and institutions, underscoring the importance of robust quality indicators and standardized examination techniques.6 These limitations highlight the urgent need for tools that can augment human performance while ensuring consistently high diagnostic accuracy.
Although endoscopy is the cornerstone of modern GI practice, its success is constrained by inter-operator variability, visual fatigue, and time pressure during demanding procedures—all of which may contribute to missed pathology.7–11 Even skilled endoscopists are susceptible to cognitive bias and perceptual lapses, especially in lengthy or complex cases. Improving adenoma detection rate (ADR)—a core quality metric that reflects the proportion of patients in whom at least one adenoma is identified—and refining lesion characterization are therefore essential goals in ensuring endoscopic quality and patient safety.
Rapid advances in computational capability, cloud processing, and access to large, well-curated image datasets have enabled the swift adoption of AI, particularly through machine learning (ML) and deep learning (DL) approaches.12,13 Convolutional neural networks (CNNs), a specialized form of deep learning (DL) architecture, have demonstrated exceptional capability in real-time endoscopic interpretation. They can accurately detect diminutive polyps, differentiate between neoplastic and non-neoplastic lesions, and identify blind spots that may escape human observation. Trained on millions of annotated images, these models recognize subtle visual features that even skilled endoscopists may fail to notice6.
Over recent years, artificial intelligence (AI) has transitioned from an experimental concept to a practical component of clinical endoscopy. One of the earliest and most notable innovations is the GI Genius system, the first AI-driven colonoscopy platform authorized by the US Food and Drug Administration as a Class II device through the de novo pathway. This software has since gained widespread clinical adoption across North America, Europe, and parts of Asia. Multiple controlled studies consistently demonstrate that GI Genius significantly improves adenoma detection rates (ADR), thereby strengthening early colorectal screening and diagnosis. Comparable progress has also been achieved with AI-assisted surveillance systems for Barrett’s esophagus and early gastric neoplasia, where diagnostic performance parallels that of experienced endoscopists.
Furthermore, next-generation systems now integrate automated quality-assurance features—for instance, algorithms that continuously assess colonoscope withdrawal time—to promote standardized reporting and enhance procedural efficiency across institutions.
Despite these advances, the incorporation of AI into daily endoscopic workflows presents several challenges. Issues surrounding regulatory oversight, medico-legal accountability, user training, and adaptation of clinical routines must be addressed to ensure safe implementation.9,10 Ongoing debates also concern the opacity of algorithmic decision-making, bias within training datasets, and ethical data governance, emphasizing the urgent need for structured clinician-training programs that foster confident, transparent, and responsible collaboration between human operators and AI systems.
Despite the rapid expansion of literature, several important gaps remain. Many existing reviews focus primarily on technical performance without integrating real-world effectiveness, implementation challenges, regulatory considerations, and health-system impact. Furthermore, recent developments such as large language models (LLMs), generative AI, foundation models, and multimodal learning have not been adequately contextualized within gastrointestinal workflows.
The scope of this review is to provide a clinically focused synthesis of evidence across major endoscopic domains while highlighting translational barriers and implementation pathways. The manuscript is organized into sections covering current advances, clinical implications, challenges, implementation strategies, and future directions.
Methodology
This review was conducted as a narrative synthesis of published evidence on artificial intelligence (AI) applications in gastroenterology, with emphasis on endoscopic imaging, lesion detection, bowel preparation assessment, and diagnostic decision support. A comprehensive literature search was performed in PubMed, Scopus, and Google Scholar databases for English-language studies published between January 2005 and April 2025 using combinations of the keywords: “artificial intelligence”, “machine learning”, “deep learning”, “endoscopy”, “CADe”, “CADx”, “colonoscopy”, “bowel preparation”, “Helicobacter pylori”, and “irritable bowel syndrome”. Although databases such as IEEE (Institute of Electrical and Electronics Engineers) Xplore, Springer, Wiley, and Elsevier host relevant content, most biomedical studies indexed in these platforms are captured through PubMed, Scopus and google Scholar. Additional references were identified by manual screening of bibliographies from relevant reviews and clinical trials. Eligible publications included original research, randomized controlled trials, meta-analyses, systematic reviews, and significant cohort studies addressing AI in gastrointestinal diagnostics, therapeutic decision-making, or workflow optimization. Following study selection, the evidence was organized using a thematic framework covering major domains of clinical application (CADe, CADx, upper gastrointestinal neoplasia, capsule endoscopy, quality assessment, and implementation). Emerging technological domains, including transformer-based architectures, large language models (LLMs), generative AI, federated learning, explainable AI (XAI), and multimodal systems, were also reviewed where relevant to clinical translation. Key outcomes, study design characteristics, and reported performance metrics were extracted and synthesized narratively. Representative ranges of diagnostic performance and clinical impact were summarized from high-quality randomized trials and meta-analyses to highlight practical clinical implications rather than to perform quantitative pooling.
Because of the wide variability in study design, endpoints, and data sources, a formal risk-of-bias or quality assessment was not undertaken. Instead, methodological rigor was inferred from study design and reporting quality. The goal of this narrative review was to integrate technological, clinical, and operational perspectives to illustrate how AI contributes to disease detection (including H. pylori infection and irritable bowel syndrome), bowel preparation assessment, and future endoscopic innovation. This structured thematic approach enabled identification of key lessons, translational challenges, and evidence gaps across domains, which informed the synthesis presented in the subsequent sections. Both the potential benefits and the limitations of AI, including variability in real-world performance, implementation challenges, and evidence gaps, were critically evaluated to provide a balanced clinical perspective. Given this heterogeneity, a meta-analytic approach was not considered appropriate.
Current Advances in Artificial Intelligence for Endoscopic Gastroenterology
Current developments in AI for endoscopic gastroenterology focus primarily on two areas: computer-aided detection (CADe) and computer-aided diagnosis (CADx). CADe systems—most commonly based on CNNs—have proven especially useful in colonoscopy, where they enhance polyp detection and recognition of early neoplastic changes, thereby consistently improving diagnostic yield.
Recent meta-analyses and randomized controlled trials have confirmed that CADe increases adenoma detection rates (ADR) by approximately 15– 20% compared with standard colonoscopy, translating into meaningful improvements in colorectal cancer prevention, even in community and diverse clinical settings.14,15 Importantly, these gains appear to be robust across clinicians with varying experience levels, underscoring the broad generalizability and real-world applicability of CADe.
Applications of artificial intelligence (AI) have yielded remarkable outcomes in upper gastrointestinal (GI) endoscopy. In the surveillance of Barrett’s esophagus, convolutional neural network (CNN)–based algorithms have demonstrated sensitivities and specificities approaching 90%, frequently matching or even surpassing the performance of experienced endoscopists in both still-image and video-based analyses.16,17 For instance, De Groof et al created a computer-aided detection (CAD) model trained on more than 1700 white-light endoscopic images that achieved an overall accuracy of 89%, exceeding that of general endoscopists (88% vs 73%) and correctly identifying biopsy targets in over 90% of cases—results comparable to those of expert evaluators.18 Likewise, CNN-driven systems for detecting early esophageal neoplasia have achieved sensitivities up to 96.4% and specificities exceeding 94%, confirming their capacity to improve lesion recognition and reduce inter-observer variation.19 Meta-analyses also indicate excellent diagnostic performance for Artificial intelligence (AI) has demonstrated strong diagnostic capability in the assessment of early gastric cancer (EGC), achieving pooled sensitivity and specificity estimates of 0.87 and 0.88, respectively.16,17 In another study, a convolutional neural network (CNN) model exceeded the performance of human endoscopists in evaluating the depth of tumor invasion, offering 17.25% greater overall accuracy together with superior specificity—information that could be invaluable for guiding optimal treatment selection.20
Growing clinical evidence continues to reinforce the role of computer-aided detection (CADe) in identifying colorectal neoplasia. Several randomized controlled trials and meta-analyses have consistently demonstrated that CADe integration enhances the adenoma detection rate (ADR) by approximately 20%(Relative increase), a key quality metric closely linked to a reduced incidence of interval colorectal cancer and corresponding decreases in mortality.21–23 Long-term follow-up studies have further verified that higher ADRs translate into improved survival outcomes.24
Despite encouraging outcomes in controlled studies, findings from real-world observational cohorts have been less consistent; in certain clinical environments, the adoption of CADe has not led to significant improvements in neoplasia detection or measurable reductions in procedural workload.25 This divergence between the strong results reported in randomized trials and the variability seen in daily clinical use highlights the need for pragmatic, well-structured investigations that accurately represent routine endoscopic practice to establish the true clinical value of CADe.25
While most randomized trials and meta-analyses indicate that CADe improves adenoma detection rates (ADR) when compared with conventional colonoscopy, the magnitude of this advantage is not uniform across users. The benefit appears to be influenced by operator experience—gains are most pronounced among fellows and early-career endoscopists, whereas the incremental improvements for highly seasoned practitioners are smaller and often fail to reach statistical significance.26 Similarly, computer-aided diagnosis (CADx) technologies designed for optical biopsy and real-time histologic assessment have demonstrated promising potential, though their performance varies considerably among different systems. For instance, when CAD-EYE was applied as an independent diagnostic tool, it did not satisfy the Preservation and Incorporation of Valuable Endoscopic Innovations (PIVI)-1 benchmark (negative predictive value < 90%) in some study populations. In contrast, when AI-assisted interpretations were performed by endoscopists, PIVI-1 was achieved, and PIVI-2 criteria were met under the European Society of Gastrointestinal Endoscopy (ESGE) guidelines, although consistent fulfillment of the US Multi-Society Task Force (USMSTF) threshold was not observed; while some studies have reported high NPVs and >95% surveillance concordance, others found no consistent superiority over expert assessment.27
The applications of AI extend beyond colonoscopy. In esophageal squamous cell carcinoma (ESCC), CNN-based systems exhibit sensitivities between 85% and 100% for image- and video-based detection, clearly surpassing or augmenting human observers.28–30 In Barrett’s esophagus, CNN models have reached sensitivities of up to 96.4% and specificities near 94%, equaling expert interpretations.17 These developments reduce reliance on random biopsies, improve dysplasia recognition, and minimize missed lesions—enabling earlier, potentially curative intervention.
For early gastric cancer, CNN-based algorithms have achieved diagnostic accuracies exceeding 90% across modalities such as white-light endoscopy (WLE), magnifying endoscopy with narrow-band imaging (ME-NBI), and other image-enhanced endoscopy (IEE) techniques. Sensitivities up to 91.06–97.59% and specificities above 89.01% have been reported, frequently outperforming human experts.31,32 Such evidence suggests that AI can lessen inter-observer variability and help standardize global practice in upper GI cancer diagnosis.
Beyond colorectal neoplasia detection, AI demonstrates broad utility in multiple endoscopic domains. In the esophagus, deep-learning systems designed for Barrett’s surveillance can accurately detect and localize early neoplastic change with external validation accuracies around 88–90%. Benchmarking trials confirm that these models outperform non-expert endoscopists, and successful real-time clinical deployment has already been demonstrated.18,33
In the stomach, AI applications in gastric endoscopy extend beyond neoplasia detection. Deep learning–based systems have shown high performance in detecting gastric ulcers and early gastric cancer, with some models achieving sensitivity exceeding 90% for early lesions.34 Similarly, convolutional neural networks trained on endoscopic images can accurately diagnose Helicobacter pylori infection, with diagnostic accuracy surpassing that of expert endoscopists (83.1–87.7%%).35 AI has shown promise in improving the diagnosis of celiac disease, which traditionally relies on duodenal biopsy interpretation with notable interobserver variability. Recent machine learning models trained on thousands of whole-slide images have achieved >95% accuracy and AUC >0.99, matching or exceeding pathologist performance. These systems not only enhance diagnostic reliability but also hold potential to reduce reporting time and variability across centers.36,37 Artificial intelligence is increasingly applied in IBD, particularly Crohn’s disease and ulcerative colitis. AI tools have shown promise in improving the accuracy and reproducibility of endoscopic and histological scoring, reducing interobserver variability, and providing objective assessments of disease severity.38 Deep learning models have achieved high accuracy in predicting histological remission, postoperative recurrence, and even treatment response.38,39 Moreover, AI-assisted capsule endoscopy and ultrasound are being explored for small bowel Crohn’s disease, offering sensitive, non-invasive diagnostic support. AI applications in bowel preparation not only optimize the adequacy of cleansing but also reduce variability between patients, directly improving the diagnostic yield of colonoscopy. By providing real-time feedback and personalized reminders, AI-based tools hold promises for becoming an integral part of pre-procedure preparation protocol.40 These expanding domains underscore that AI extends far beyond polyp detection, with broad relevance to gastroenterology practice.
In capsule endoscopy (CE), AI has enhanced diagnostic efficiency by reducing review times and improving lesion detection. Commercially available AI-powered CE systems have demonstrated high sensitivity, particularly in small bowel evaluations.41 However, challenges remain: incomplete lesion detection, lack of standardization, and limited clinical validation currently prevent full reliance on AI. Ongoing improvements must focus on algorithm refinement, standardized performance metrics, and patient-centered outcome validation.41
Computer-aided diagnosis (CADx) systems further consolidate the expanding role of artificial intelligence (AI) in histologic prediction. For diminutive colorectal polyps (≤5 mm), pooled sensitivity and specificity values of 93% and 87%, respectively, with an area under the curve (AUC) of 0.961, have been reported.42,43 Using enhanced imaging techniques such as narrow-band imaging (NBI), CADx consistently differentiates between neoplastic and non-neoplastic lesions, achieving negative predictive values (NPVs) exceeding 90% in the rectosigmoid colon. These outcomes meet the “Preservation and Incorporation of Valuable Endoscopic Innovations” (PIVI) performance thresholds and support practical strategies such as the “diagnose-and-leave” approach for non-neoplastic lesions and the “resect-and-discard” policy for low-risk adenomas.44 Implementing these AI-supported workflows can substantially reduce unnecessary resections, pathology expenses, and overall procedure times while preserving diagnostic reliability and patient safety.42,43,45
Finally, real-world registry data and prospective trials have confirmed that AI-assisted workflows can safely improve efficiency. In randomized controlled trials, platforms such as WISENSE and ENDOANGEL have demonstrated their ability to reduce blindspots and improve gastroscopy & colonoscopy quality in randomized controlled trials respectively.46,47 Beyond lesion detection and diagnosis, these systems also track key quality indicators, including withdrawal time and bowel preparation scores, while flagging unexamined mucosal areas.48–50 Furthermore, standardization of documentation through automation and integration with electronic medical records (EMR) enhances standardization and procedural effectiveness.47,50,51 The regulatory approval for such endoscopic AI tools as ENDOANGEL and GI Genius is already in place in Asia, Europe, and North America, which guarantees their large-scale applicability readiness and is the beginning of a novel endoscopy era.47,50,51
Evidence for commercially available platforms such as GI Genius, EndoScreener, and Skout remains mixed. While some trials report modest but significant ADR gains, others show limited benefit, particularly in expert hands.52 Variations in trial design, patient selection, and comparator methodologies create substantial heterogeneity, making it difficult to generalize efficacy outcomes across different practice environments.
Clinical Implications of Artificial Intelligence in Endoscopy
While the preceding section summarizes technological developments and diagnostic performance of AI systems, this section focuses on their real-world clinical impact, including effects on patient outcomes, workflow efficiency, training, and quality standardization. The clinical impact of artificial intelligence (AI) in endoscopic gastroenterology is most evident in its ability to enhance lesion detection, improve diagnostic precision, and streamline procedural workflow. Multiple meta-analyses have consistently shown that the integration of computer-aided detection (CADe) technologies raises adenoma detection rates (ADR) by approximately 20% while simultaneously reducing missed lesions. In practical terms, even a seemingly modest 1% increase in ADR corresponds to a 3% reduction in the risk of interval colorectal cancer and nearly a 5% decrease in mortality from colorectal cancer.21,48,53,54 Observations from high-volume centers further confirm that these benefits are sustainable across a broad range of patient populations and among endoscopists with differing experience levels.21 In this way, AI meaningfully narrows the performance gap between expert and non-expert practitioners, elevating the overall standard of care in colonoscopy. However, the incremental improvement achieved with AI may be smaller among highly experienced endoscopists with already high baseline detection rates, where AI is likely to serve primarily as a quality assurance and standardization tool rather than substantially enhancing individual performance.
Beyond detection, AI demonstrates remarkable strength in lesion characterization. Computer-aided diagnosis (CADx) systems are now capable of reliably differentiating adenomatous from hyperplastic polyps in real time, supporting the cost-effective “resect-and-discard” strategy while enabling endoscopists with limited experience to achieve diagnostic accuracies comparable to those of specialists.43,55 This strategy reduces reliance on histopathologic assessment for diminutive lesions and may improve cost-efficiency and workflow, although current evidence shows no significant benefit of CADx in improving diagnostic accuracy or clinical outcomes.55 Furthermore, CADx platforms have shown promise in accelerating the learning process for trainees, fostering the development of advanced visual recognition and classification skills that traditionally required years of clinical experience to master.56 A multicenter randomized trial in trainee colonoscopists found that an AI-aided system (CAD EYE) did not increase adenoma detection rate (ADR) but significantly reduced adenoma miss rate (AMR) and missed adenomas per patient, while improving ACE tool scores for pathology identification and localization. These results suggest AI can enhance detection reliability and cognitive performance during training even when overall ADR remains unchanged. Such tools may therefore strengthen colonoscopy quality and educational outcomes, supporting safer, more consistent examinations in early operators.57
In upper GI endoscopy, AI has improved diagnostic confidence by consistently identifying subtle neoplastic changes that might be missed by the human eye, especially in regions where gastric and esophageal cancers are highly prevalent.18 Real-time AI support for detecting early lesions in Barrett’s esophagus or gastric mucosa can lead to earlier therapeutic interventions and better survival outcomes.58 By reducing inter-observer variability, AI systems ensure greater consistency in diagnostic accuracy across different practice settings.
These advantages extend to workflow and resource optimization as well. Automated documentation and AI-driven quality monitoring not only reduce the administrative burden but also reinforce adherence to best practice guidelines and highlight procedural variability for targeted improvement.59 Tools that measure withdrawal time, monitor the completeness of mucosal inspection, and track polyp detection provide objective, actionable feedback and foster continuous quality improvement. Seamless integration with electronic medical record (EMR) systems further supports reporting, billing, and follow-up, which are particularly valuable in resource-limited or high throughput environments. However, several challenges remain. False positive scan distracts endoscopists, prolong procedures, and create “alarm fatigue”, in which frequent alerts reduce attentiveness.60,61 Early implementation studies have also revealed mixed acceptance, with clinicians citing concerns about workflow disruption, and uncertainty over delegating decision-making to AI systems.62 Questions regarding patient and provider trust, cost-effectiveness beyond controlled trials, and applicability across different healthcare systems continue to be actively debated.63 Together, these issues underscore the importance of ongoing real-world validation, comprehensive cost-effectiveness studies, and ethically grounded strategies to ensure equitable and sustainable deployment of AI in endoscopic gastroenterology.
A concise summary of the major clinical domains and validated applications of AI in gastrointestinal endoscopy—including CADe, CADx, capsule endoscopy, and upper GI neoplasia—is presented in Table 1.
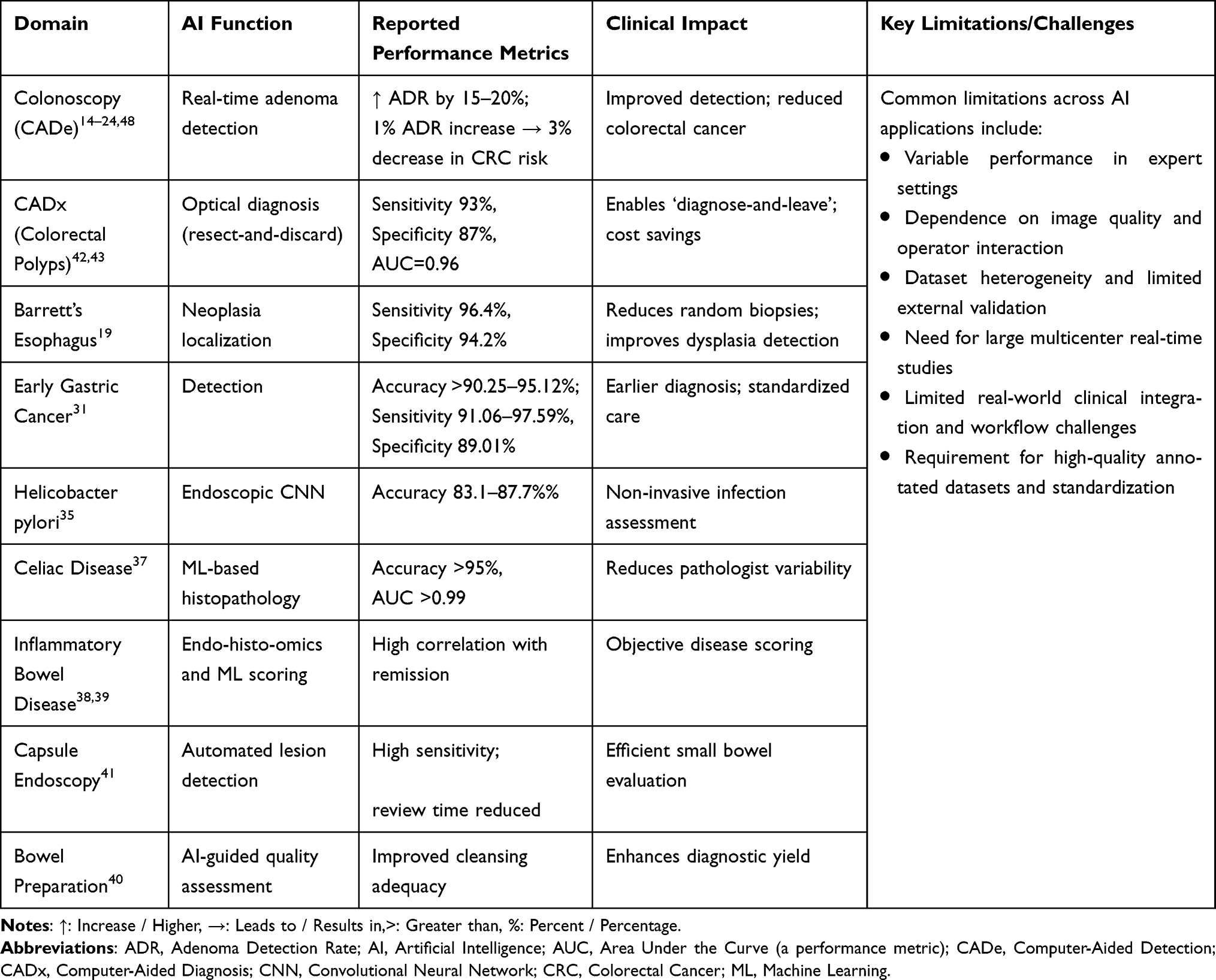 |
Table 1 Key Clinical Applications of Artificial Intelligence in Gastrointestinal Endoscopy |
Challenges and Barriers to Widespread Adoption
Despite the rapid progress of artificial intelligence (AI)in gastroenterology, several hurdles limit its widespread use. From a technical perspective, the development of robust algorithms depends heavily on access to large, annotated datasets. Interoperability between AI platforms and existing hospital IT systems remains limited, while variability in image quality arising from hardware differences or patient-related factors can undermine performance.64,65 The diversity and quality of training data are especially critical, as algorithms often perform well in the environments in which they are developed but degrade significantly when applied to new populations or clinical settings. The absence of standardized protocols for data acquisition, labeling, and sharing makes it difficult to create universally applicable models and complicates comparisons across studies.64 Moreover, embedding AI into real-time clinical workflows demands advanced computing infrastructure and seamless integration with reporting systems, which are frequently lacking in resource-limited settings, risking greater global disparities in access.64,65
Regulatory challenges are equally significant, including issues related to data privacy, algorithm transparency, validation standards, medico-legal accountability, and the lack of uniform regulatory frameworks for clinical deployment of AI systems. While agencies such as the US The Food and Drug Administration (FDA), European Medicines Agency (EMA), and Japanese regulators have already approved several AI-based solutions; however, regulatory harmonization worldwide is still incomplete. Existing frameworks have been largely designed for static medical devices rather than adaptive algorithms that evolve with continuous learning.66,67 This raises the practical question of how often algorithms should be revalidated. How should updates be communicated to clinicians? What mechanisms should be used to ensure safety monitoring after implementation66? Clinical validation of AI, including multicenter trials across racially and geographically diverse populations, is still evolving and remains a topic of ongoing debate.68 Without such robust evidence, there is a real risk that AI tools may show promise in controlled environments but fail to provide consistent benefits in routine practice.
Legal and ethical concerns further complicate its adoption in clinical practice. Issues such as accountability for AI-assisted decisions, safeguarding of patient data, and potential algorithmic bias are especially pressing as AI assumes more autonomous clinical roles.66,67 In cases of diagnostic errors, liability remains unclear, whether it lies with developers, institutions, or end users. Using patient data for training raises privacy concerns, particularly under regulations such as the European Union’s General Data Protection Regulation (GDPR).68
Another challenge is the potential overreliance on AI. As systems assume greater decision- making responsibilities, clinicians may risk losing their essential interpretive and problem- solving skills. Conversely, centers without access to AI may fall behind, creating new inequalities in patient care. Inconsistent validation across populations and poor interoperability can further erode trust, particularly in real-world practices.66
Finally, organizational and educational barriers should not be underestimated in this context. Successful adoption requires more than technical integration; it demands that clinicians be trained not only in how to use AI tools but also in understanding their limitations, biases, and the appropriate contexts for application. Sustained institutional support, structured change management, and continuous feedback loops are vital for ensuring that AI is a reliable and trusted component of gastroenterology practice.67
Prior reviews by Mennella et al (2024) and Karalis et al (2024) have have highlighted key challenges of AI adoption, including regulatory frameworks, integration into hospital IT systems, and medico-legal implications.69,70 Our review builds on these by linking technical performance with translational considerations and real-world registry data.
Beyond technical hurdles, widespread implementation raises complex questions regarding algorithmic bias, accountability in adverse events, validation across diverse practice settings, and reimbursement models. Integration into existing electronic health records and hospital IT systems remains a significant bottleneck. Addressing these challenges will require collaboration between clinicians, regulators, payers, and industry to ensure safe, equitable, and sustainable AI deployment.
Pathways to Widespread Adoption and Future Directions
The widespread adoption of artificial intelligence (AI) in endoscopic gastroenterology depends on coordinated progress across several domains. Robust evidence from multicenter prospective validation studies is essential to confirm the safety, effectiveness, and generalizability across different patient populations, varying levels of endoscopist expertise, and diverse practice environments.71,72 Encouragingly, recent multicenter trials, such as those evaluating AI- assisted capsule endoscopy and gastric neoplasm detection, have demonstrated significant diagnostic improvements and underscored the importance of validating AI in heterogeneous, real-world settings.71,73 Long-term follow-up may be important to establish whether these benefits are sustained over time and to mitigate risks, such as overdiagnosis.74 Shared open-access datasets are another cornerstone of this progress.
Initiatives such as GastroHUN, GastroEndoNet, and Polyp-Size provide rigorously curated and annotated repositories that promote reproducibility, enable fair comparisons, and accelerate innovation.75–77 By standardizing formats and ensuring transparency in curation, such collaborative databases can play a pivotal role in AI from a promising research tool into a reliable partner in daily clinical practice.75,76
Regulatory harmonization is equally important. Clear and consistent approval pathways, effective post-marketing surveillance, and transparency in algorithm updates are necessary to build trust and ensure safe usage. Regulatory bodies, including the FDA, European regulators under the EU AI Act, and international harmonization groups, should prioritize frameworks for adaptive AI algorithms, such as predetermined change-control plans that allow safeguarding patient safety.68 Similar to pharmacovigilance in drug safety, post-market surveillance for AI must be strengthened to track its performance in real-world practice and to quickly identify emerging issues.78 Transparent policies on data ownership, privacy, and cross-border data sharing, such as those embedded in the EU AI Act, further support clinician and patient confidence.79 Similarly, harmonized liability frameworks must clearly define the responsibilities of developers, clinicians, and institutions to minimize legal uncertainty and foster responsible adoption.
At the practical level, implementation science and structured change management are critical for ensuring successful integration of AI in healthcare. Pilot programs can demonstrate early success and help build trust among clinicians. These should be coupled with robust user training, including structured onboarding and real-time support, to ease workflow transitions.80,81 Early adopters of AI in endoscopy have benefited from structured onboarding and seamless integration with existing systems and approaches that improve usability and acceptance.80 Continuous feedback loops, in which clinicians actively evaluate and refine AI performance, are necessary to ensure that the systems remain responsive to clinical needs.82,83 Interdisciplinary collaboration is central; clinicians, data scientists, regulators, and industry leaders must work together through cross-disciplinary groups and professional societies to set best practice standards, create governance frameworks, and establish clear decision-making pathways.84
Finally, future research must extend beyond the technical performance. Economic evaluations are essential for determining whether AI tools deliver meaningful value, especially in resource- limited settings. Evidence suggests that CADe-assisted colonoscopy is cost-effective and improves outcomes while lowering overall costs.85 AI-based CADx tools also appear promising, with incremental cost-effectiveness ratios (ICERs) of approximately USD11, 093per QALY gained.86 Microsimulation models further suggest that AI-assisted screening colonoscopy could reduce colorectal cancer incidence and mortality while generating substantial healthcare savings, estimated at USD 290 million annually in the US85 Patient-centered outcomes are equally important: understanding trust in AI diagnoses, multicentre trials, inclusion of diverse populations, and real-world validation are essential to ensure generalisable and unbiased AI systems.87 However, without deliberate attention to equity and algorithmic fairness, AI risks reinforcing existing healthcare disparities, particularly if minority populations are underrepresented in training datasets.
The principal technical, regulatory, ethical, and organizational limitations impeding broad clinical deployment are summarized in Table 2. Commercially available AI platforms and their clinical evidence are summarized in Table 3. A practical framework outlining the technical, regulatory, and organizational requirements for safe clinical integration is presented in Table 4.
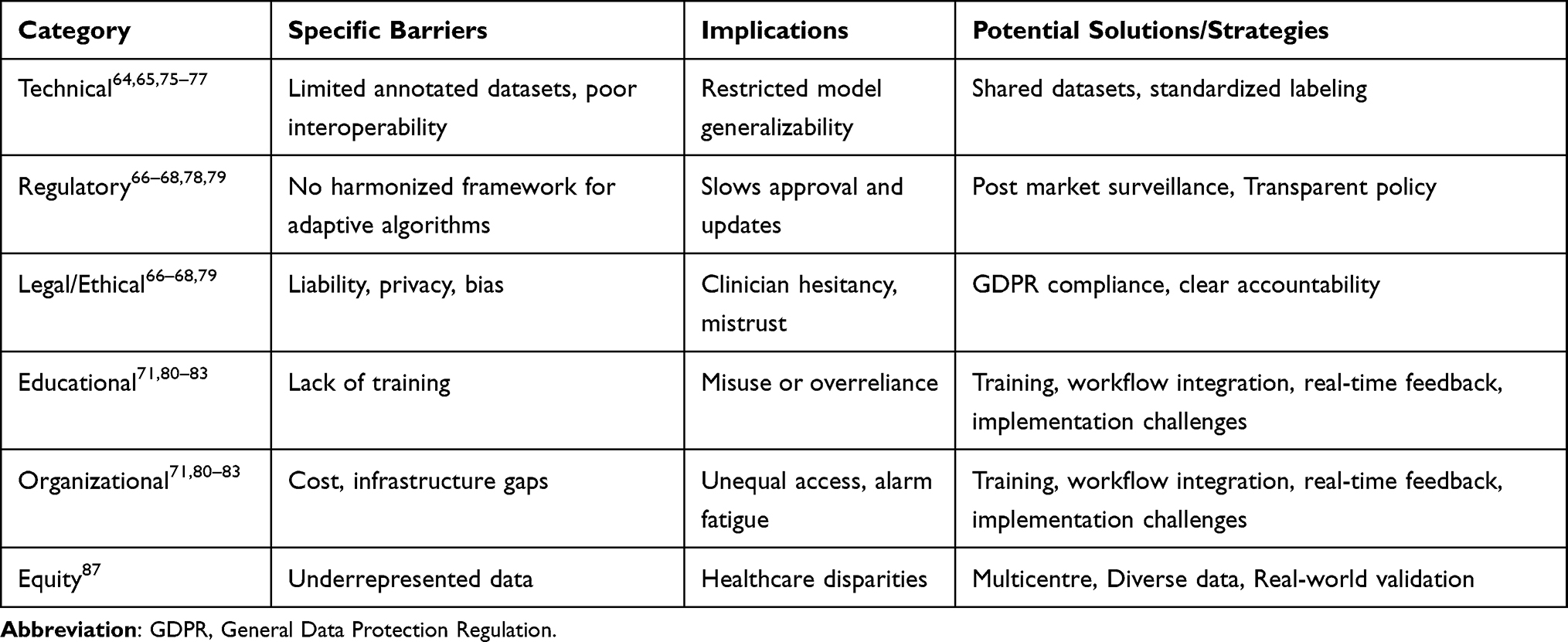 |
Table 2 Challenges and Barriers to Widespread AI Adoption in Endoscopic Gastroenterology |
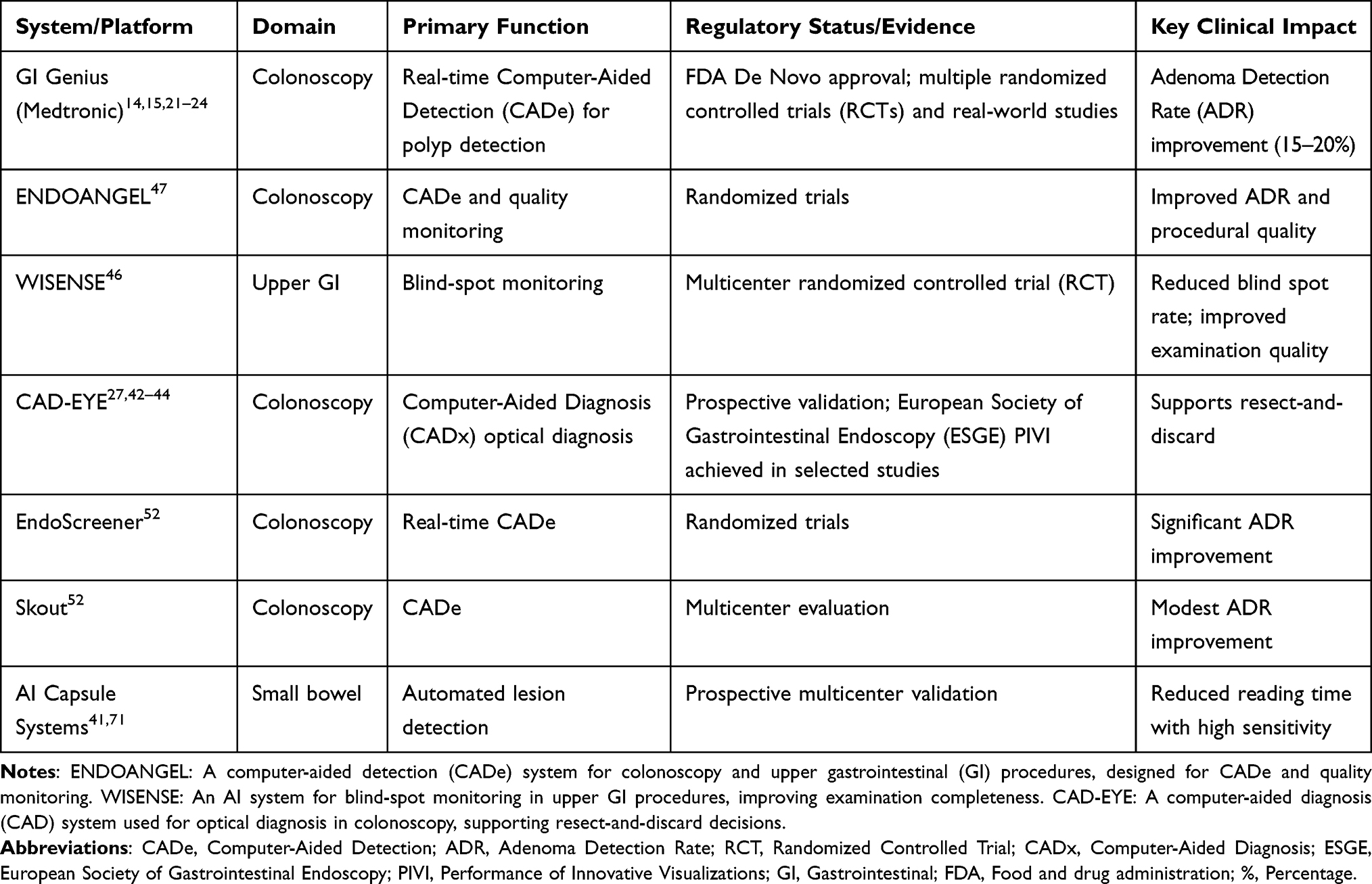 |
Table 3 Major AI Systems in Gastrointestinal Endoscopy |
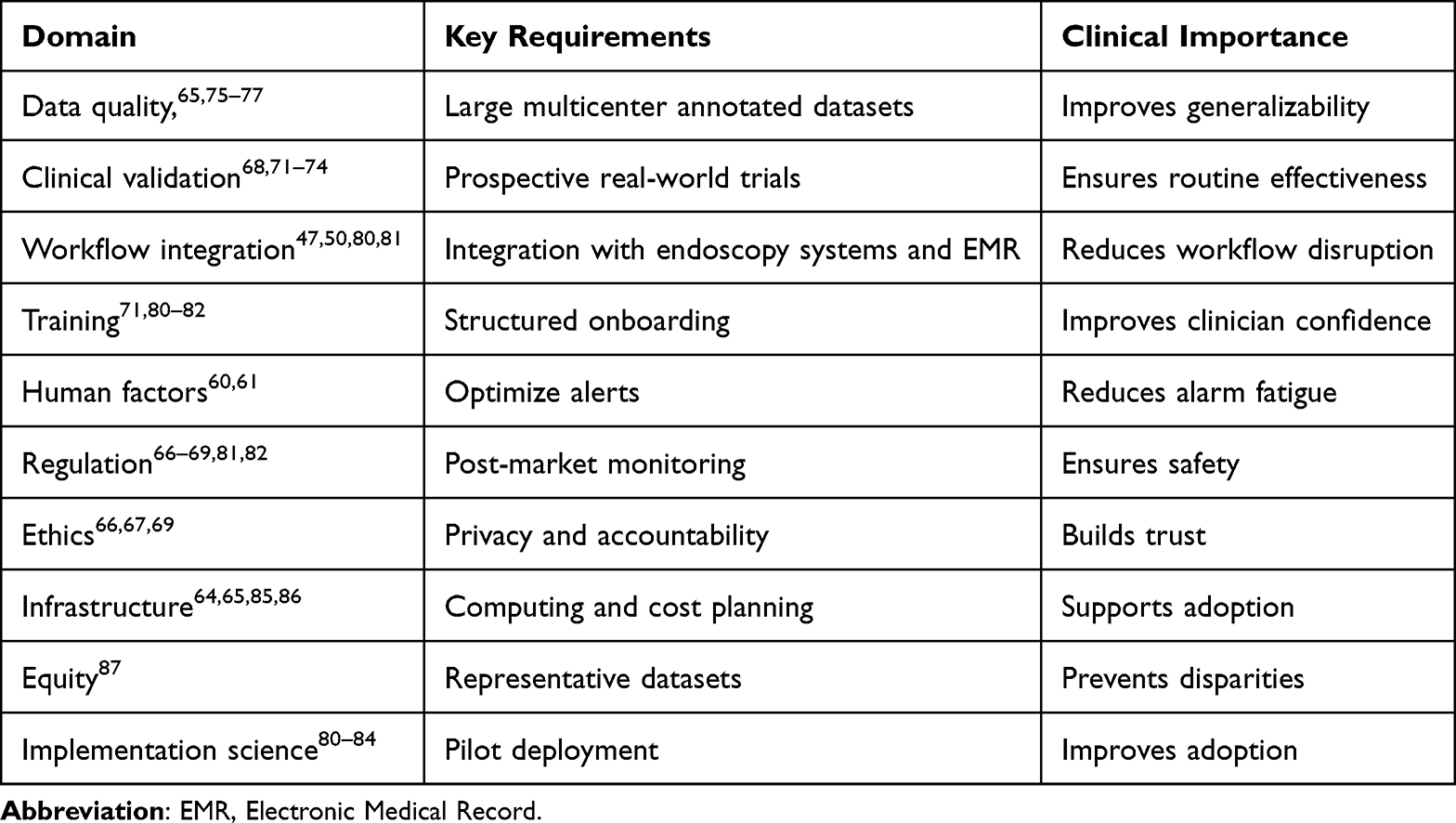 |
Table 4 Implementation Framework for Clinical Integration of AI |
A conceptual roadmap for stepwise clinical implementation is illustrated in Figure 1.
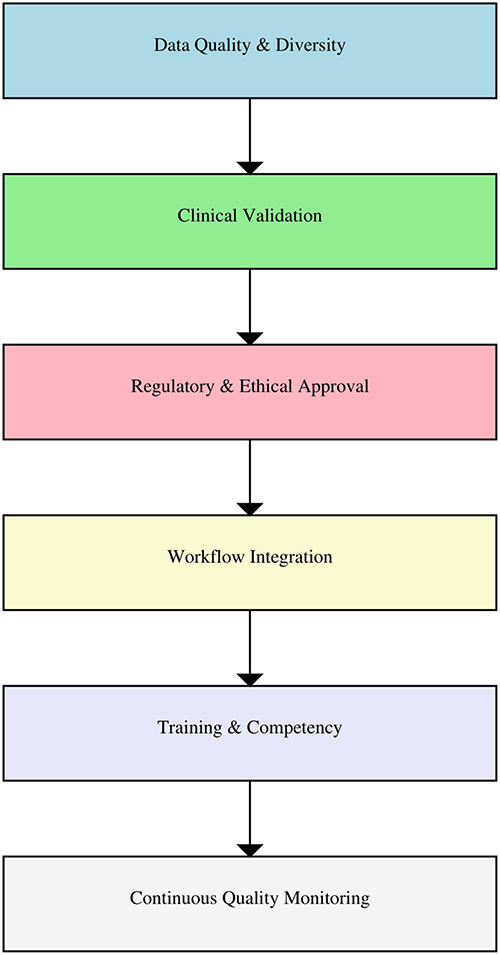 |
Figure 1 A conceptual roadmap for stepwise clinical implementation of AI. |
This Review Provides Unique Value by
Synthesizing evidence across all domains of AI in gastroenterology, including CADe, CADx, capsule endoscopy, and upper GI neoplasia into a unified perspective.
Linking diagnostic improvements to operational efficiency and population-level outcomes places AI’s clinical impact of AI in the broader healthcare context.
A balanced assessment was provided by contrasting trial efficacy with real-world challenges such as alarm fatigue, medicolegal uncertainty, and integration barriers.
An implementation roadmap that highlights regulatory harmonization, ethical safeguards, clinician training, and equitable access is outlined.
Establishing research priorities for the future, including patient-reported outcomes, cost-effectiveness, and health equity, will enable its meaningful worldwide adoption.
Technically, AI is not only a technical augmentation but also an impetus for updating endoscopy quality standards. At the clinical, technical, and policy levels, collaborative AI action can facilitate accelerated early detection of gastrointestinal cancer, eradicate diagnostic care inequalities, and dramatically control cancer morbidity and mortality worldwide.
Novelty
Unlike prior reviews that primarily focus on technical performance, our manuscript integrates evidence from RCTs, meta-analyses, and real-world data to provide a comprehensive roadmap for clinical adoption. We uniquely contrast trial efficacy with real-world challenges such as alarm fatigue, regulatory hurdles, and workflow integration barriers, and we link ADR gains to population-level outcomes and cost-effectiveness data. This holistic perspective provides clinicians, researchers, and policymakers with actionable insights to guide sustainable implementation of AI in gastroenterology.
Conclusion
Artificial intelligence is rapidly transforming gastrointestinal endoscopy from an operator-dependent practice to a data-driven precision discipline. Evidence from randomized and real-world studies demonstrates meaningful improvements in adenoma detection, diagnostic accuracy, and consistency across the GI tract. This review highlights the transition of AI from experimental models to clinically validated and regulatory-approved systems, while outlining the practical requirements for safe implementation, including multicenter validation, diverse datasets, workflow integration, clinician training, and continuous performance monitoring. Despite these advances, challenges related to generalizability, algorithm bias, medico-legal accountability, ethical governance, and resource disparities must be addressed to ensure responsible adoption. With structured validation and implementation frameworks, AI is poised to evolve from a supportive tool to an integral component of precision endoscopy, improving quality, efficiency, and equity in gastrointestinal care.
Disclosure
The authors report no conflicts of interest, including financial conflicts, in this work.
References
1. Kröner PT, Engels MM, Glicksberg BS, et al. Artificial intelligence in gastroenterology: a state-of-the-art review. World J Gastroenterol. 2021;27(40):6794–15. PMID: 34790008; PMCID: PMC8567482. doi:10.3748/wjg.v27.i40.6794
2. Patel V, Khan MN, Shrivastava A, et al. Artificial intelligence applied to gastrointestinal diagnostics: a review. J Pediatr Gastroenterol Nutr. 2020;70(1):4–11. PMID: 31567886; PMCID: PMC6934912. doi:10.1097/MPG.0000000000002507
3. Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. GastrointestEndosc. 2015;81(1):31–53. PMID: 25480100. doi:10.1016/j.gie.2014.07.058
4. Pimenta-Melo AR, Monteiro-Soares M, Libânio D, Dinis-Ribeiro M. Missing rate for gastric cancer during upper gastrointestinal endoscopy: a systematic review and meta-analysis. Eur J Gastroenterol Hepatol. 2016;28(9):1041–1049. doi:10.1097/MEG.0000000000000657
5. Rodríguez de Santiago E, Hernanz N, Marcos-Prieto HM, et al. Rate of missed esophageal cancer at routine endoscopy and survival outcomes: a multicentric cohort study. United Eur Gastroenterol J. 2019;7(2):189–198. PMID: 31080603; PMCID: PMC6498796. doi:10.1177/2050640618811477
6. Kim NH, Jung YS, Jeong WS, et al. Miss rate of colorectal neoplastic polyps and risk factors for missed polyps in consecutive colonoscopies. Intest Res. 2017;15(3):411–418. doi:10.5217/ir.2017.15.3.411
7. Harewood GC, Chrysostomou K, Himy N, Leong WL. Impact of operator fatigue on endoscopy performance: implications for procedure scheduling. Dig Dis Sci. 2009;54(8):1656–1661. PMID: 19034661. doi:10.1007/s10620-008-0549-7
8. Lee A, Iskander JM, Gupta N, et al. Queue position in the endoscopic schedule impacts effectiveness of colonoscopy. Am J Gastroenterol. 2011;106(8):1457–1465. PMID: 21448145; PMCID: PMC4098876. doi:10.1038/ajg.2011.87
9. Stasinos I, Voulgaris TA, Alexopoulos T, Karamanolis GP. Combining techniques and technologies increases adenoma detection rates in colonoscopy: more is more. World J Gastrointest Endosc. 2025;17(8):107734. PMID: 40838157; PMCID: PMC12362565. doi:10.4253/wjge.v17.i8.107734
10. Jover R, Zapater P, Polanía E, et al. COLONPREV study investigators. Modifiable endoscopic factors that influence the adenoma detection rate in colorectal cancer screening colonoscopies. GastrointestEndosc. 2013;77(3):381–389.e1. PMID: 23218945. doi:10.1016/j.gie.2012.09.027
11. Shaukat A, Mongin S, Church T, Kim A, Rank J, Allen J. Variability in adenoma detection rate and withdrawal time, and effect of performance improvement interventions over time. Am J Gastroenterol. 2013;108(Suppl):S179. doi:10.14309/00000434-201310001-00610
12. Min JK, Kwak MS, Cha JM. Overview of deep learning in gastrointestinal endoscopy. Gut Liver. 2019;13(4):388–393. PMID: 30630221; PMCID: PMC6622562. doi:10.5009/gnl18384
13. Nie Z, Xu M, Wang Z, Lu X, Song W. A review of application of deep learning in endoscopic image processing. J Imag. 2024;10(11):275. doi:10.3390/jimaging10110275
14. Makar J, Abdelmalak J, Con D, Hafeez B, Garg M. Use of artificial intelligence improves colonoscopy performance in adenoma detection: a systematic review and meta-analysis. GastrointestEndosc. 2025;101(1):68–81.e8. PMID: 39216648. doi:10.1016/j.gie.2024.08.033
15. Soleymanjahi S, Huebner J, Elmansy L, et al. Artificial intelligence-assisted colonoscopy for polyp detection: a systematic review and meta-analysis. Ann Intern Med. 2024;177(12):1652–1663. PMID: 39531400. doi:10.7326/ANNALS-24-00981
16. Luo D, Kuang F, Du J, et al. Artificial intelligence-assisted endoscopic diagnosis of early upper gastrointestinal cancer: a systematic review and meta-analysis. Front Oncol. 2022;12:855175. PMID: 35756602; PMCID: PMC9229174. doi:10.3389/fonc.2022.855175
17. de Groof AJ, Struyvenberg MR, Fockens KN, et al. Deep learning algorithm detection of Barrett’s neoplasia with high accuracy during live endoscopic procedures: a pilot study. GastrointestEndosc. 2020;91(6):1242–1250. PMID: 31926965. doi:10.1016/j.gie.2019.12.048
18. de Groof AJ, Struyvenberg MR, van der Putten J, et al. Deep-learning system detects neoplasia in patients with Barrett’s esophagus with higher accuracy than endoscopists. Gastroenterology. 2020;158(4):915–929.e4. PMID: 31759929. doi:10.1053/j.gastro.2019.11.030
19. Hashimoto R, Requa J, Dao T, et al. Artificial intelligence using convolutional neural networks for real-time detection of early esophageal neoplasia in Barrett’s esophagus. GastrointestEndosc. 2020;91(6):1264–1271.e1. PMID: 31930967. doi:10.1016/j.gie.2019.12.049
20. Zhu Y, Wang QC, Xu MD, et al. Application of convolutional neural network in the diagnosis of the invasion depth of gastric cancer based on conventional endoscopy. GastrointestEndosc. 2019;89(4):806–815.e1. PMID: 30452913. doi:10.1016/j.gie.2018.11.011
21. Aleissa MA, Luca M, Singh JP, et al. Current status of artificial intelligence colonoscopy on improving adenoma detection rate based on systematic review of multiple meta-analyses. ArtifIntell Gastroenterol. 2025;6(1):106149. doi:10.35712/aig.v6.i1.106149
22. Lee MCM, Parker CH, Liu LWC, Farahvash A, Jeyalingam T. Impact of study design on adenoma detection in the evaluation of artificial intelligence-aided colonoscopy: a systematic review and meta-analysis. GastrointestEndosc. 2024;99(5):676–687.e16. PMID: 38272274. doi:10.1016/j.gie.2024.01.021
23. Shao L, Yan X, Liu C, Guo C, Cai B. Effects of AI-assisted colonoscopy on adenoma miss rate/adenoma detection rate: a protocol for systematic review and meta-analysis. Medicine. 2022;101(46):e31945. PMID: 36401456; PMCID: PMC9678521. doi:10.1097/MD.0000000000031945
24. Leung FW, Hsieh YH. Artificial intelligence (computer-assisted detection) is the most recent novel approach to increase adenoma detection. GastrointestEndosc. 2021;93(1):86–88. PMID: 33353642. doi:10.1016/j.gie.2020.07.059
25. Patel HK, Mori Y, Hassan C, et al. Lack of effectiveness of computer-aided detection for colorectal neoplasia: a systematic review and meta-analysis of nonrandomized studies. Clin Gastroenterol Hepatol. 2024;22(5):971–980.e15. PMID: 38056803. doi:10.1016/j.cgh.2023.11.029
26. Bernhofer S, Prosenz J, Venturi D, et al. The impact of artificial intelligence on the adenoma detection rate. Wien Klin Wochenschr; 2025. doi:10.1007/s00508-025-02561-3
27. El Zoghbi M, Shaukat A, Hassan C, Anderson JC, Repici A, Gross SA. Artificial intelligence-assisted optical diagnosis: a comprehensive review of its role in leave-in-situ and resect-and-discard strategies in colonoscopy. Clin Transl Gastroenterol. 2023;14(10):e00640. PMID: 37747097; PMCID: PMC10584286. doi:10.14309/ctg.0000000000000640
28. Horie Y, Yoshio T, Aoyama K, et al. Diagnostic outcomes of esophageal cancer by artificial intelligence using convolutional neural networks. GastrointestEndosc. 2019;89(1):25–32. PMID: 30120958. doi:10.1016/j.gie.2018.07.037
29. Guo L, Xiao X, Wu C, et al. Real-time automated diagnosis of precancerous lesions and early esophageal squamous cell carcinoma using a deep learning model (with videos). GastrointestEndosc. 2020;91(1):41–51. PMID: 31445040. doi:10.1016/j.gie.2019.08.018
30. Fukuda H, Ishihara R, Kato Y, et al. Comparison of performances of artificial intelligence versus expert endoscopists for real-time assisted diagnosis of esophageal squamous cell carcinoma (with video). GastrointestEndosc. 2020;92(4):848–855. PMID: 32505685. doi:10.1016/j.gie.2020.05.043
31. Jin J, Zhang Q, Dong B, et al. Automatic detection of early gastric cancer in endoscopy based on Mask region-based convolutional neural networks (Mask R-CNN) (with video). Front Oncol. 2022;12:927868. PMID: 36338757; PMCID: PMC9630732. doi:10.3389/fonc.2022.927868
32. Lei C, Sun W, Wang K, Weng R, Kan X, Li R. Artificial intelligence-assisted diagnosis of early gastric cancer: present practice and future prospects. Ann Med. 2025;57(1):2461679. PMID: 39928093; PMCID: PMC11812113. doi:10.1080/07853890.2025.2461679
33. Ebigbo A, Mendel R, Probst A, et al. Real-time use of artificial intelligence in the evaluation of cancer in Barrett’s oesophagus. Gut. 2020;69(4):615–616. PMID: 31541004; PMCID: PMC7063447. doi:10.1136/gutjnl-2019-319460
34. Hirasawa T, Aoyama K, Tanimoto T, et al. Application of artificial intelligence using a convolutional neural network for detecting gastric cancer in endoscopic images. Gastric Cancer. 2018;21(4):653–660. PMID: 29335825. doi:10.1007/s10120-018-0793-2
35. Shichijo S, Nomura S, Aoyama K, et al. Application of convolutional neural networks in the diagnosis of Helicobacter pylori infection based on endoscopic images. EBioMedicine. 2017;25:106–111. PMID: 29056541; PMCID: PMC5704071. doi:10.1016/j.ebiom.2017.10.014
36. Carreras J. Artificial intelligence analysis of celiac disease using an autoimmune discovery transcriptomic panel highlighted pathogenic genes including BTLA. Healthcare. 2022;10(8):1550. PMID: 36011206; PMCID: PMC9408070. doi:10.3390/healthcare10081550
37. Jaeckle F, Denholm J, Schreiber B, et al. Machine learning achieves pathologist-level coeliac disease diagnosis. NEJM AI. 2025;2(4):aioa2400738. PMID: 40438269; PMCID: PMC7617718. doi:10.1056/AIoa2400738
38. Ahmad HA, East JE, Panaccione R, et al. Artificial intelligence in inflammatory bowel disease: implications for clinical practice and future directions. Intest Res. 2023;21(3):283–294. PMID: 37075809; PMCID: PMC10397545. doi:10.5217/ir.2023.00020
39. Iacucci M, Santacroce G, Zammarchi I, et al. Artificial intelligence and endo-histo-omics: new dimensions of precision endoscopy and histology in inflammatory bowel disease. Lancet Gastroenterol Hepatol. 2024;9(8):758–772. PMID: 38759661. doi:10.1016/S2468-1253(24)00053-0
40. Zhu Y, Zhang DF, Wu HL, et al. Improving bowel preparation for colonoscopy with a smartphone application driven by artificial intelligence. NPJ Digit Med. 2023;6(1):41. doi:10.1038/s41746-023-00786-y
41. Giordano A, Romero-Mascarell C, González-Suárez B, et al. Integration of artificial intelligence-enhanced capsule endoscopy in clinical practice: a review of market-available tools for clinical practice. Dig Dis Sci. 2025;70(9):2966–2976. doi:10.1007/s10620-025-09099-4
42. Bang C, Lee J, Baik G. Computer-aided diagnosis of diminutive colorectal polyps in endoscopic images: systematic review and meta-analysis of diagnostic test accuracy. J Med Internet Res. 2021;23(8):e29682. doi:10.2196/29682
43. Byrne MF, Chapados N, Soudan F, et al. Real-time differentiation of adenomatous and hyperplastic diminutive colorectal polyps during analysis of unaltered videos of standard colonoscopy using a deep learning model. Gut. 2019;68(1):94–100. PMID: 29066576; PMCID: PMC6839831. doi:10.1136/gutjnl-2017-314547
44. Rex DK, Kahi C, O’Brien M, et al. The American society for gastrointestinal endoscopy pivi (Preservation and incorporation of valuable endoscopic innovations) on real-time endoscopic assessment of the histology of diminutive colorectal polyps. GastrointestEndosc. 2011;73(3):419–422. PMID: 21353837. doi:10.1016/j.gie.2011.01.023
45. Kudo SE, Misawa M, Mori Y, et al. Artificial intelligence-assisted system improves endoscopic identification of colorectal neoplasms. Clin Gastroenterol Hepatol. 2020;18(8):1874–1881.e2. PMID: 31525512. doi:10.1016/j.cgh.2019.09.009
46. Wu L, Zhang J, Zhou W, et al. Randomized controlled trial of WISENSE, a real-time quality improving system for monitoring blind spots during esophagogastroduodenoscopy. Gut. 2019;68(11):2161–2169. doi:10.1136/gutjnl-2018-317366
47. Gong D, Wu L, Zhang J, et al. Detection of colorectal adenomas with a real-time computer-aided system (ENDOANGEL): a randomized controlled study. Lancet Gastroenterol Hepatol. 2020;5(4):352–361. doi:10.1016/S2468-1253(19)30413-3
48. Corley DA, Jensen CD, Marks AR, et al. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med. 2014;370(14):1298–1306. doi:10.1056/NEJMoa1309086
49. Zhou J, Wu L, Wan X, et al. A novel artificial intelligence system for the assessment of bowel preparation (with video). GastrointestEndosc. 2020;91(2):428–435.e2. doi:10.1016/j.gie.2019.11.026
50. Repici A, Badalamenti M, Maselli R, et al. Efficacy of real-time computer-aided detection of colorectal neoplasia in a randomized trial. Gastroenterology. 2020;159(2):512–520.e7. doi:10.1053/j.gastro.2020.04.062
51. Vulpoi RA, Luca M, Ciobanu A, et al. Artificial intelligence in digestive endoscopy—Where are we and where are we going? Diagnostics. 2022;12(4):927. doi:10.3390/diagnostics12040927
52. Wei MT, Fay S, Yung D, Ladabaum U, Kopylov U. Artificial intelligence-assisted colonoscopy in real-world clinical practice: a systematic review and meta-analysis. Clin Transl Gastroenterol. 2024;15(3):e00671. PMID: 38146871; PMCID: PMC10962886. doi:10.14309/ctg.0000000000000671
53. Lou S, Du F, Song W, et al. Artificial intelligence for colorectal neoplasia detection during colonoscopy: a systematic review and meta-analysis of randomized clinical trials. EClinicalMedicine. 2023;66:102341. doi:10.1016/j.eclinm.2023.102341
54. Tang CP, Shao PP, Hsieh YH, Leung FW. A review of water exchange and artificial intelligence in improving adenoma detection. Tzu Chi Med J. 2020;33(2):108–114. doi:10.4103/tcmj.tcmj_88_2
55. Hassan C, Rizkala T, Mori Y, et al. CADx analysis study group. Computer-aided diagnosis for the resect-and-discard strategy for colorectal polyps: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2024;9(11):1010–1019. PMID: 39303733. doi:10.1016/S2468-1253(24)00222-X
56. Hassan C, Balsamo G, Lorenzetti R, Zullo A, Antonelli G. Artificial intelligence allows leaving-in-situ colorectal polyps. Clin Gastroenterol Hepatol. 2022;20(11):2505–2513.e4. PMID: 35835342. doi:10.1016/j.cgh.2022.04.045
57. Yamaguchi D, Shimoda R, Miyahara K, et al. Impact of an artificial intelligence-aided endoscopic diagnosis system on improving endoscopy quality for trainees in colonoscopy: prospective, randomized, multicenter study. Dig Endosc. 2024;36(1):40–48. PMID: 37079002; PMCID: PMC12136242. doi:10.1111/den.14573
58. Zhou R, Liu J, Zhang C, et al. Efficacy of a real-time intelligent quality-control system for the detection of early upper gastrointestinal neoplasms: a multicenter, single-blinded, randomized controlled trial. EClinicalMedicine. 2024;75:102803. PMID: 39281103; PMCID: PMC11402435. doi:10.1016/j.eclinm.2024.102803
59. Lux TJ, Saßmannshausen Z, Kafetzis I, et al. Assisted documentation as a new focus for artificial intelligence in endoscopy: the precedent of reliable withdrawal time and image reporting. Endoscopy. 2023;55(12):1118–1123. PMID: 37399844; PMCID: PMC11321719. doi:10.1055/a-2122-1671
60. Chung GE, Lee J, Lim SH, et al. A prospective comparison of two computer-aided detection systems with different false positive rates in colonoscopy. NPJ Digit Med. 2024;7(1):366. PMID: 39702474; PMCID: PMC11659580. doi:10.1038/s41746-024-01334-y
61. Campion JR, O’Connor DB, Lahiff C. Human-artificial intelligence interaction in gastrointestinal endoscopy. World J Gastrointest Endosc. 2024;16(3):126–135. PMID: 38577646; PMCID: PMC10989254. doi:10.4253/wjge.v16.i3.126
62. Tiankanon K, Karuehardsuwan J, Aniwan S, et al. Performance comparison between two computer-aided detection colonoscopy models by trainees using different false positive thresholds: a cross-sectional study in Thailand. Clin Endosc. 2024;57(2):217–225. PMID: 38556473; PMCID: PMC10984740. doi:10.5946/ce.2023.145
63. Fernandes C, Miles S, Lucena C, Cowan D. Artificial intelligence technologies for coping with alarm fatigue in hospital environments because of sensory overload: algorithm development and validation. J Med Internet Res. 2019;21(11):e15406. PMID: 31738168; PMCID: PMC6905471. doi:10.2196/15406
64. David-Olawade AC, Aderinto N, Egbon E, Olatunji GD, Kokori E, Olawade DB. Enhancing endoscopic precision: the role of artificial intelligence in modern gastroenterology. J Gastrointest Surg. 2025;29(10):102195. PMID: 40840824. doi:10.1016/j.gassur.2025.102195
65. Ali S. Where do we stand in AI for endoscopic image analysis? Deciphering gaps and future directions. NPJ Digit Med. 2022;5(1):184. PMID: 36539473; PMCID: PMC9767933. doi:10.1038/s41746-022-00733-3
66. Santra S, Kukreja P, Saxena K, Gandhi S, Singh OV. Navigating regulatory and policy challenges for AI-enabled combination devices. Front Med Technol. 2024;6:1473350. PMID: 39669903; PMCID: PMC11634576. doi:10.3389/fmedt.2024.1473350
67. Zhang S, Li Y, Liu W, et al. A decade of review in global regulation and research of artificial intelligence medical devices (2015–2025). Front Med Lausanne. 2025;12:1630408. PMID: 40747091; PMCID: PMC12310608. doi:10.3389/fmed.2025.1630408
68. U.S. Food and Drug Administration (FDA). Artificial intelligence and machine learning (AI/ML)-enabled medical devices. Available from: https://www.fda.gov/medical-devices/software-medical-device-samd/artificial-intelligence-enabled-medical-devices.
69. Mennella C, Maniscalco U, De Pietro G, Esposito M. Ethical and regulatory challenges of AI technologies in healthcare: a narrative review. Heliyon. 2024;10(4):e26297. PMID: 38384518; PMCID: PMC10879008. doi:10.1016/j.heliyon.2024.e26297
70. Karalis VD. The integration of artificial intelligence into clinical practice. Appl Biosci. 2024;3(1):14–44. doi:10.3390/applbiosci3010002
71. Spada C, Piccirelli S, Hassan C, et al. AI-assisted capsule endoscopy reading in suspected small bowel bleeding: a multicenter prospective study. Lancet Digit Health. 2024;6(5):e345–e353. PMID: 38670743. doi:10.1016/S2589-7500(24)00048-7
72. ClinicalTrials.gov. AI-assisted endoscopy in colorectal cancer screening (NCT04232462). Available from: https://clinicaltrials.gov/study/NCT04232462.
73. Lee H, Chung J-W, Yun S-C, et al. Validation of artificial intelligence computer-aided detection on gastric neoplasm in upper gastrointestinal endoscopy. Diagnostics. 2024;14(23):2706. PMID: 39670745. doi:10.3390/diagnostics14232706
74. Chaudhary R, Dhangar P, Chaudhary A. Artificial intelligence in gastrointestinal endoscopy: a comprehensive systematic review. medRxiv. 2025. doi:10.1101/2025.07.02.25330317
75. Bravo D, Frias J, Vera F, et al. GastroHUN: an endoscopy dataset of complete systematic screening protocol for the stomach. Sci Data. 2025;12(1):102. PMID: 39824869; PMCID: PMC11742658. doi:10.1038/s41597-025-04401-5
76. Bitto AK, Bijoy MHI, Shakil KH, et al. GastroEndoNet: comprehensive endoscopy image dataset for GERD and polyp detection. Data Brief. 2025;60:111572. PMID: 40470347; PMCID: PMC12136698. doi:10.1016/j.dib.2025.111572
77. Song Y, Du S, Wang R, et al. Polyp-size: a precise endoscopic dataset for AI-driven polyp sizing. Sci Data. 2025;12(1):918. PMID: 40450075; PMCID: PMC12126491. doi:10.1038/s41597-025-05251-x
78. Babic B, Glenn Cohen I, Stern AD, Li Y, Ouellet M. A general framework for governing marketed AI/ML medical devices. Npj Digit Med. 2025;8(1):328. PMID: 40450160; PMCID: PMC12126487. doi:10.1038/s41746-025-00011-x
79. Team Consulting. Regulation of AI in Healthcare: navigating the EU AI Act and FDA. Available from: https://www.team-consulting.com/us/insights/regulation-of-ai-in-healthcare-navigating-the-eu-ai-act-and-fda/.
80. El-Sayed A, Salman S, Alrubaiy L. The adoption of artificial intelligence assisted endoscopy in the Middle East: challenges and future potential. Transl Gastroenterol Hepatol. 2023;8:42. PMID: 38021356; PMCID: PMC10643188. doi:10.21037/tgh-23-37
81. MedBridge. Implementation Strategies for AI Integration in Gastroenterology. 2025. Available from: https://www.medbridge.com/resources/ai-integration-strategies.
82. Leenhardt R, Koulaouzidis A, Histace A, et al. Key research questions for implementation of artificial intelligence in capsule endoscopy. Ther Adv Gastroenterol. 2022;15:17562848221132683. PMID: 36338789; PMCID: PMC9629556. doi:10.1177/17562848221132683
83. Chen HT, Zhang Y, Carneiro G, Singh R. Toward a human-centered AI-assisted colonoscopy system in Australia. In:
84. Kim JY, Boag W, Gulamali F, et al. Organizational governance of emerging technologies: AI adoption in healthcare. In:
85. Barkun AN, von Renteln D, Sadri H. Cost-effectiveness of artificial intelligence-aided colonoscopy for adenoma detection in colon cancer screening. J Can Assoc Gastroenterol. 2023;6(3):97–105. PMID: 37273970; PMCID: PMC10235593. doi:10.1093/jcag/gwad014
86. Yonazu S, Ozawa T, Nakanishi T, et al. Cost-effectiveness analysis of the artificial intelligence diagnosis support system for early gastric cancers. DEN Open. 2024;4(1):e289. :PMID: 37644958; PMCID: PMC10461711. doi:10.1002/deo2.289
87. Han R, Acosta JN, Shakeri Z, Ioannidis JPA, Topol EJ, Rajpurkar P. Randomized controlled trials evaluating artificial intelligence in clinical practice: a scoping review. Lancet Digit Health. 2024;6(5):e367–e373. PMID: 38670745; PMCID: PMC11068159. doi:10.1016/S2589-7500(24)00047-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.