Back to Journals » Patient Preference and Adherence » Volume 18
Patient, Care Partner, and Physician Voices in Treatment Decision-Making for Multiple Myeloma
Authors Dwyer Orr L, Lin D, Wu B ![]() , LeBlanc TW, Faiman B, Ahlstrom J, Yung M
, LeBlanc TW, Faiman B, Ahlstrom J, Yung M ![]() , Deering KL, Kulbokas V, Feldman JL, Kline E, Biran N
, Deering KL, Kulbokas V, Feldman JL, Kline E, Biran N
Received 11 May 2024
Accepted for publication 5 October 2024
Published 19 October 2024 Volume 2024:18 Pages 2147—2158
DOI https://doi.org/10.2147/PPA.S474722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Lisa Dwyer Orr,1 Dee Lin,1 Bingcao Wu,1 Thomas W LeBlanc,2 Beth Faiman,3 Jenny Ahlstrom,4 Margaret Yung,5 Kathleen L Deering,5 Victoria Kulbokas,5 Joshua L Feldman,6 Erika Kline,6 Noa Biran7
1Janssen Scientific Affairs LLC, Titusville, NJ, USA; 2Duke Cancer Institute, Duke University School of Medicine, Durham, NC, USA; 3Cleveland Clinic, Taussig Cancer Institute, Cleveland, OH, USA; 4HealthTree Foundation, Draper, UT, USA; 5EPI-Q Inc, Chicago, IL, USA; 6Inspire Insights, Arlington, VA, USA; 7Hackensack Meridian Health, John Theurer Cancer Center, Hackensack, NJ, USA
Correspondence: Lisa Dwyer Orr, Janssen Scientific Affairs LLC, Titusville, NJ, USA, Tel +1 561 290-9901, Email [email protected]
Introduction: Treatment decision-making for multiple myeloma (MM) is complex. Individuals involved in decision-making may value treatment attributes differently based on their role as a patient, care partner, or physician. This study describes those attributes, and what is most important by role.
Methods: We conducted a cross-sectional online survey with consenting adult patients with MM, MM care partners, and physicians treating MM. Respondents were recruited from US panels (Inspire and M3 Global Research) between September and December 2022. Survey items were informed by a targeted literature review, qualitative interviews, and a steering committee comprising clinical experts, a patient advocate, patient, and care partner. Descriptive statistics were generated and reported in aggregate.
Results: Email invitations were sent to 8071 Inspire members interested in or posting about MM. Of these, 4427 viewed the invitation, 941 responded, and 156 patients and care partners completed the survey (17% of respondents). For physicians, 5588 were invited via Email by M3 Global Research, with 761 viewing the invitation, 214 accessing the survey link, and 137 completing the survey (64% of respondents). Duration of response, side effects, and patients’ quality-of-life (QoL) were the top three treatment attributes selected across the three cohorts; alignment of these attributes was consistent among patients regardless of disease severity. Separately, patients rated QoL and the amount of caregiving needed during/after treatment as the most important factors for future treatment decisions. If more effective MM treatments were offered, care partners were more willing to assume greater family burden (77%) compared to patients (49%), and patients were more accepting of potential serious side effects (50%) than were care partners (34%).
Conclusion: Patients with MM, care partners, and physicians consider and value various treatment decision-making factors. Recognizing and addressing these differences is critical to meeting patients’ preferences, needs, and optimizing patient outcomes.
Keywords: Decision-making, treatment choice, cross-sectional survey, multiple myeloma
Introduction
Multiple myeloma (MM) is a rare hematologic cancer, with an estimated incidence of 35,730 in 2023; it accounts for approximately 1.8% of all new cancer cases in 2023.1 Despite its relatively low incidence, it ranks as the 15th leading cause of cancer-related deaths in the United States (US).1 Treatment for MM has improved significantly over the years, leading to improved survival rates and quality of life (QoL) for patients. However, there are still several challenges due to the disease’s heterogeneity and evolving treatment landscape, making it difficult to establish a definitive standard of care for all patients.2–4 Several factors need to be considered when choosing an appropriate therapy, including age, disease severity, potential toxicities, responses to previous therapies, and number of previous therapy lines.5 Despite high initial treatment response rates in patients with newly diagnosed MM, acquired drug resistance remains a significant challenge, resulting in shorter duration of response for subsequent lines of treatment.5
Considering the many therapies available, varying patient characteristics, and potential side effects, choosing the most appropriate treatment plan can be challenging. In addition, involving patients and their care partners in the decision-making process is crucial to achieving and maintaining the desired QoL for the patient. Many therapies can also be burdensome to patients and care partners; patients must carefully consider their options and balance the potential benefits of therapy with the possible side effects and impact on their QoL.6–8 Research demonstrates that patients’ treatment decisions are significantly influenced by personal circumstances, preferences, and the guidance provided by their physicians when presented with various treatment options.9 However, one investigation showed that, at baseline, only 24% of clinicians would consider patients’ preferences as part of the decision-making process, but after participating in an educational program covering shared decision-making (SDM) concepts, 69% stated they would.10
SDM is a communication process in which the interaction between a clinician and their patient includes both perspectives, and individual values are elicited and considered thoughtfully and respectfully before arriving at a treatment choice.11 When patients and care partners are included in the decision-making process, they can provide valuable insights about their experiences, concerns, and treatment expectations, which can help physicians tailor treatment plans accordingly. Additionally, published literature demonstrates that alignment between patients and those involved in their care yields improved treatment adherence and outcomes.12 Thus, it is essential to provide patients and care partners with information to improve their knowledge of treatment options available, and to learn about the various perspectives in MM decision-making to help patients achieve their treatment goals, optimize treatment outcomes, and maintain a desired QoL. This study sought to identify and describe how patients, care partners, and physicians prioritize treatment attributes in MM decision-making, and how these attributes may change over the treatment journey.
Materials and Methods
This was a cross-sectional survey of patients, care partners, and physicians in the US. Data were collected using online survey platforms from Inspire Insights (Inspire) and M3 Global Research between September 16 and December 26, 2022.
Selection of Participants
Patients and care partners were recruited via Inspire, the world’s largest online health community.13 Inspire has supported research in various health communities14–18 and their communities includes patients, care partners, patient advocates, and individuals interested in learning or sharing health information. Physicians were identified from M3 Global Research’s database, which represents a nationally diverse sample of physicians who agree to participate in survey research.19–25
All potential respondents were invited via Email to participate in the research and completed a screening questionnaire to ensure they were eligible to participate in the study. As part of the screening, respondents were asked to give electronic consent, and those who agreed were immediately directed to the main survey.
Patient eligibility included being at least 18 years old, having a self-reported diagnosis of MM for a minimum of 6 months, and currently receiving medical care for MM by a physician. Care partners were required to be 18 years or older and self-identify as a family member or friend who provided routine caregiving to a patient with MM (eg, medication management, scheduling doctor appointments, gathering medical information). Care partners employed as healthcare professionals by the patient or the patient’s family were excluded. Physicians who were recruited for the survey were required to be board certified in Hematology and/or Oncology, be licensed to practice medicine in the US, have at least 2 years of experience, and treat at least 5 patients with MM annually. The investigators were blinded to the identity of the patients, care partners, and physicians; thus, while linked dyads or triads could be possible, they could not be identified.
Main Survey
Survey questions were developed based on a targeted literature review of treatment attributes in MM treatment decision-making, in addition to insights gathered from qualitative interviews conducted with 20 patients and 5 care partners. The surveys were reviewed and modified based on input from a steering committee comprising of 3 clinical experts, 2 patients, and 1 care partner. Before rolling out the full launch to all eligible participants, a preliminary soft launch was conducted to verify data quality.
The surveys were tailored for each group (patient, care partner, physician) and included 35–39 questions of various multiple-choice, ranking, and Likert scale questions, including some questions that were adapted from previously validated scales. For example, the patient and care partner surveys included the Time and Outcomes Preference Scale26 to assess the baseline preferences of quality versus quantity of life (subscale 1) and present health versus future health (subscale 2). This study was approved by the Western Institutional Review Board-Copernicus Group Institutional Review Board.
Analysis
Aggregated descriptive statistics were used to report participant demographics, patient clinical characteristics, and responses to the survey questions. Means and standard deviations (SDs) were reported for continuous variables while frequencies and percentages were reported for categorical variables. Items with Likert scale responses were reported as frequencies and means ± SD. For ranking exercises, the average ranking values were calculated for each option and then sorted from least to greatest to determine the most preferred answer choice. The answer choice with the lowest average ranking indicated the most preferred selection. The Time and Outcomes Preference subscale scores were calculated for each patient and care partner by adding up the item scores per subscale and dividing by the number of items in each subscale. The median and interquartile range (IQR) of the respondents’ Time and Outcomes Preference subscale 1 and 2 scores were used to summarize their preferences.
Results
Email invitations were sent to 8071 Inspire health community members who were interested in or posted about MM. Among these, 4427 members viewed the invitation (55%) and 941 members responded to the Email (12%). A total of 156 patients and care partners were eligible to participate and completed the survey (17% of respondents). For physicians, 5588 were invited via Email by M3 Global Research, 761 viewed the invitation, 214 physicians accessed the survey link, and 137 physicians were eligible and completed the survey (64% of respondents).
The final survey groups consisted of 126 self-identified patients with MM, 30 self-identified MM care partners, and 137 physicians treating MM from various geographic regions in the US (Table 1). Patients living with MM reported having the disease for an average of 6.4 years (SD 4.2). Thirty-one (25%) of the 126 patient respondents had not experienced an MM relapse at the time of the survey, 62 (49%) patients had experienced 1 to 3 relapses, and 30 (24%) patients had experienced 4 or more relapses. Forty-seven percent (47%) of the care partners surveyed were a spouse or partner of a person living with MM. One-half (50%) of all the care partners had been providing care for 1 to 5 years. Additional patient and care partner characteristics are presented in Table S1. The majority of physicians practiced for more than 10 years (69%), practiced in the community setting (64%), and self-identified as an MM specialist (64%).
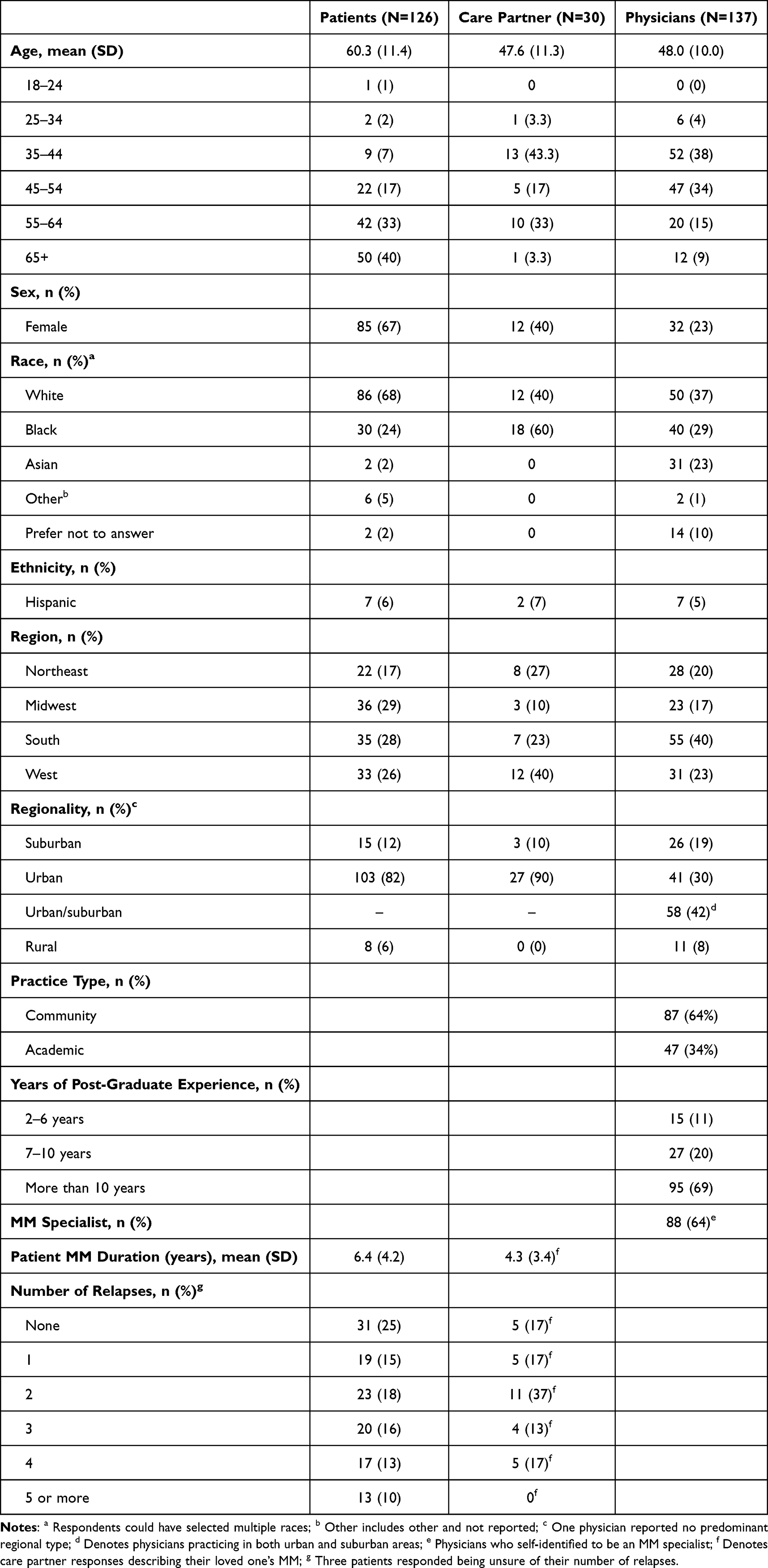 |
Table 1 Respondent Population and Characteristics |
Treatment Attributes
Multiple factors were important to patients, care partners, and physicians when making MM treatment decisions. All three respondent groups were asked to rank a list of 10 treatment attributes in order of importance from 1 (most important attribute) to 10 (least important attribute). Across all respondent groups, QoL, duration of response, and side effects were ranked in the top three (Table 2). Following these factors, preferences for the other treatment attributes varied among the respondents. For example, treatment breaks were more important to care partners (ranked #4) compared to patients (ranked #10) or physicians (ranked #8). Additionally, patients valued care partner support and cost (ranked #5 and #6, respectively) more highly than care partners themselves (ranked #7 and #8) and physicians (ranked #9 and #10). Other important attributes for physicians were logistics, such as monitoring (ranked #4) and treatment location (ranked #5); however, patients and care partners ranked those as least important.
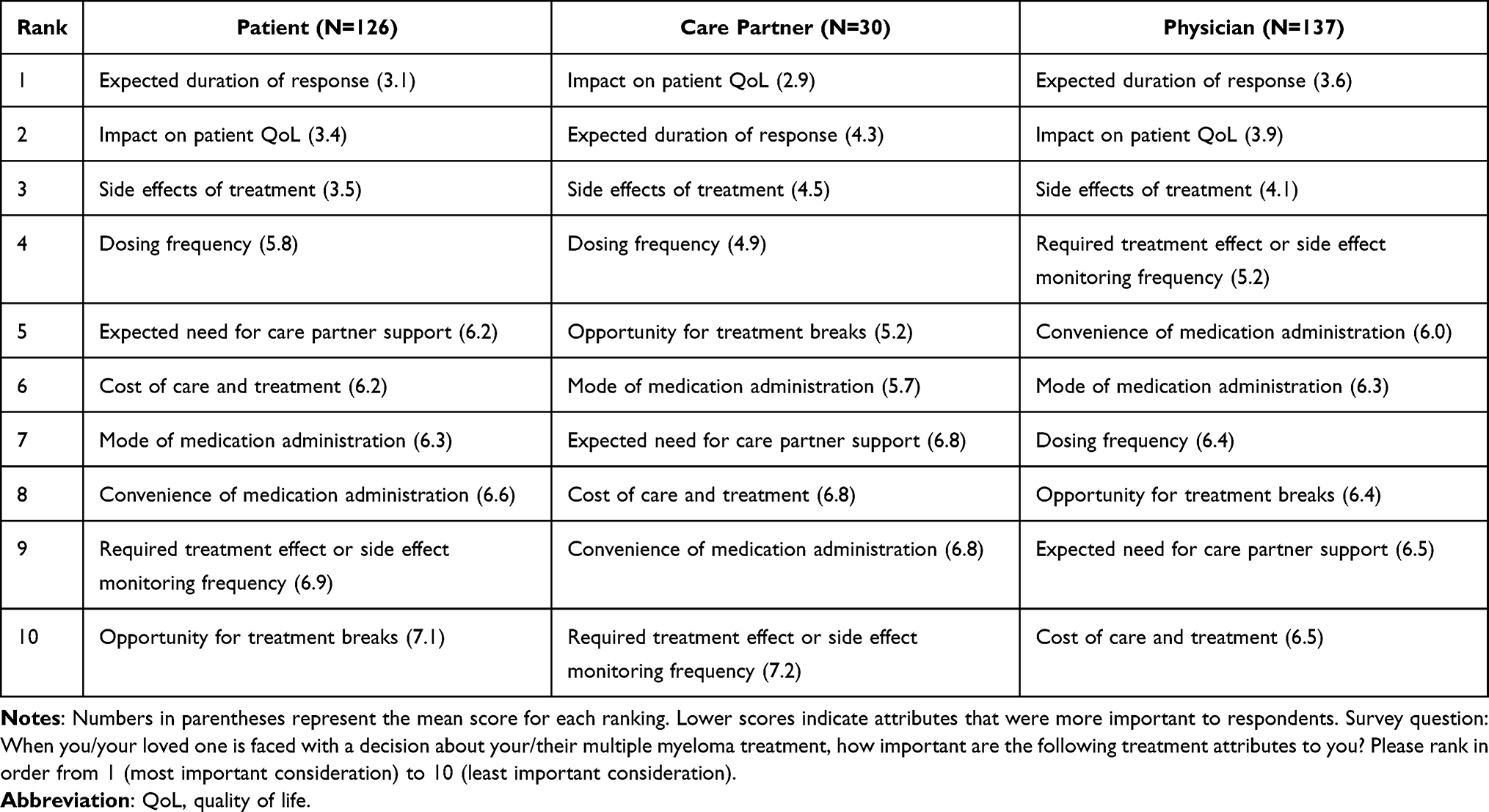 |
Table 2 Ranking of Treatment Attributes, by Respondent Type |
When evaluating treatment attributes reported by patients according to their place in therapy (defined by the number of relapses they have experienced), QoL, duration of response, and side effects were still selected as the top three treatment attributes overall (Table 3). Patients with no history of relapses ranked cost fourth; however, patients with a history of relapses ranked cost at seventh (1 to 3 relapses) and ninth (4 or more relapses). For patients who experienced 4 or more relapses, having treatment breaks (ranked #5) was prioritized more than patients who experienced fewer or no relapses (ranked #10).
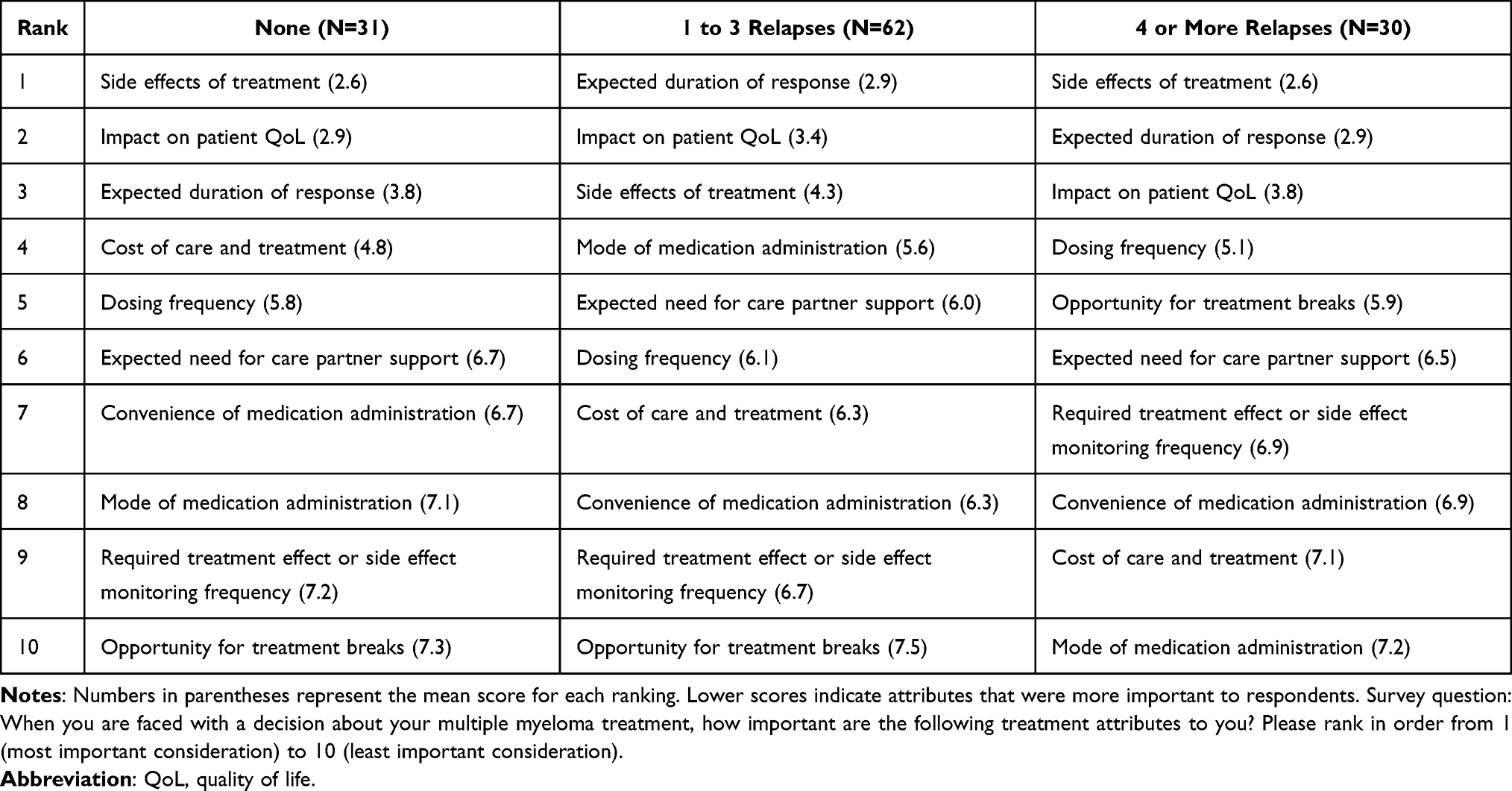 |
Table 3 Patient Ranking of Treatment Attributes by Number of Relapses Reported |
When physicians ranked treatment attributes based on the patient’s disease severity, cost was less of a concern when treating patients with relapsed or refractory MM, while convenience and the opportunity for treatment breaks became more important (Table 4).
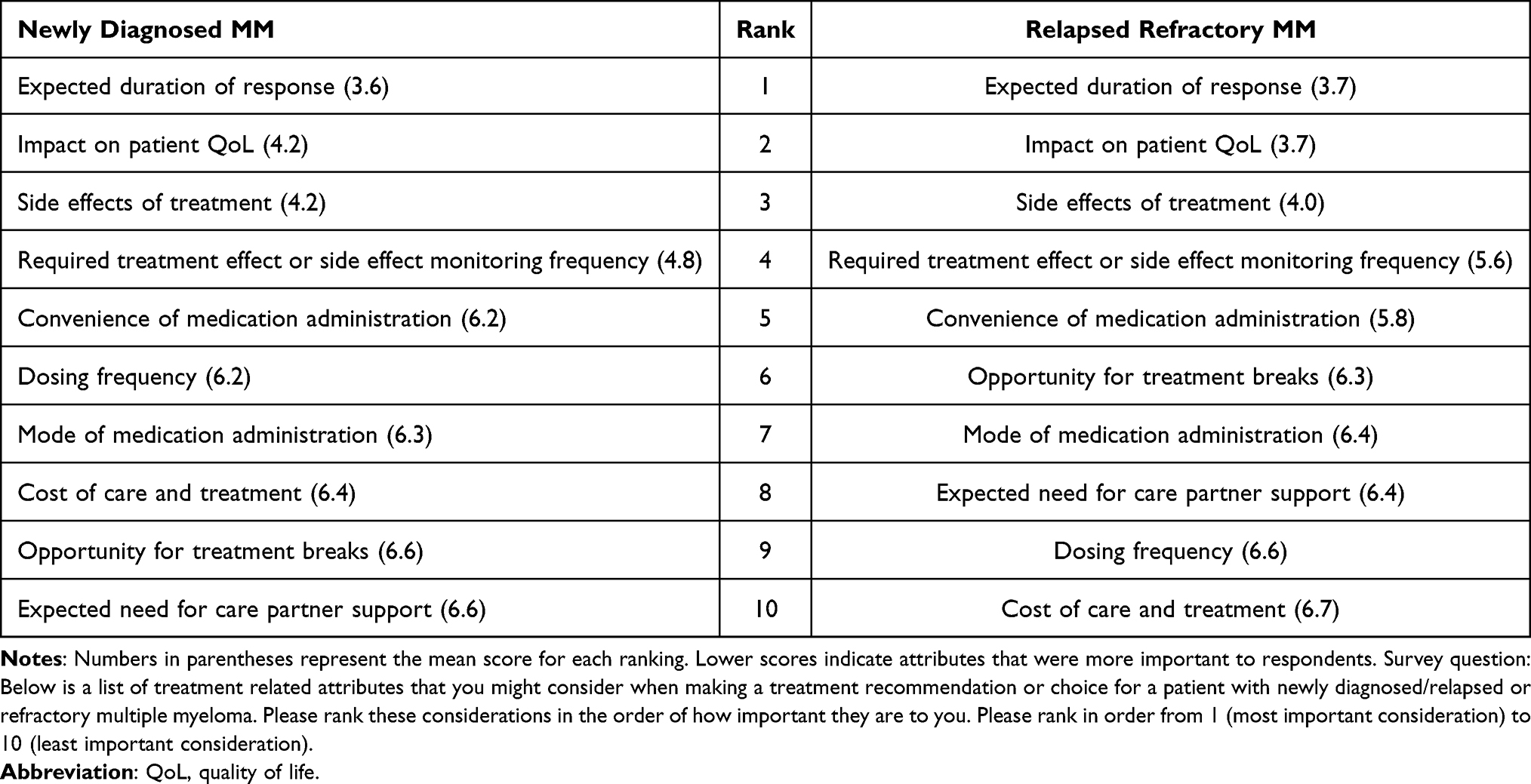 |
Table 4 Physician Ranking of Treatment Attributes by Patient Disease Severity |
In a separate exercise, patients and care partners were asked to rank factors (beyond treatment attributes) that were important to them when making a decision about their/their loved one’s next possible MM treatment (1-Not important at all; 4-Very important). The leading factors ranked as “more or very important” for both patients and care partners included the patient’s current QoL, how much caregiving was needed during or after treatment, experiences with prior medications, how well they can get around/to travel, and financial issues. Overall, a larger proportion of care partners attributed higher importance to most factors compared to patients when it came to the next treatment decision (Figure 1). Only the amount of caregiving needed (85% of patients vs 83% of care partners) and other family members’ opinion (67% of patients vs 53% of care partners) were ranked as “more or very important” by a slightly larger percentage of patients compared to care partners.
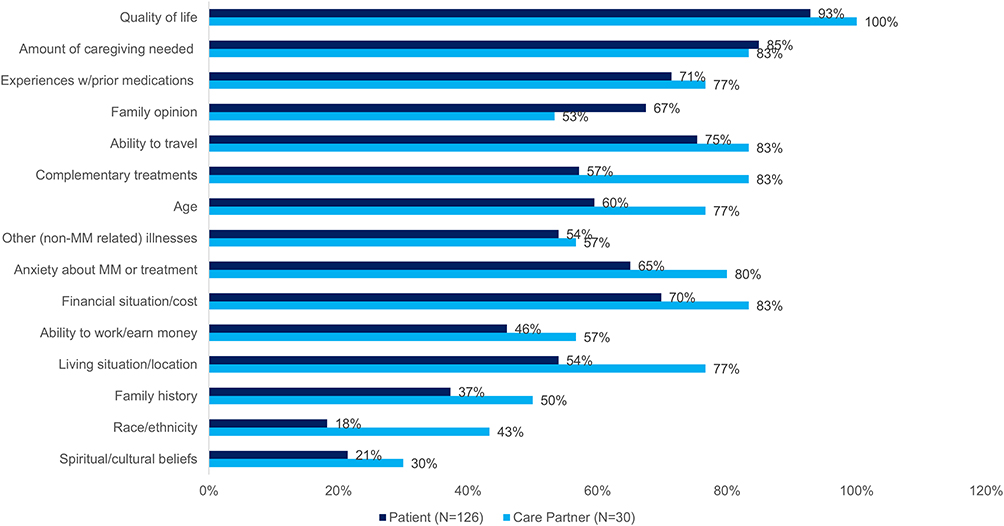 |
Figure 1 Factors ranked as more or very important when making a decision about next possible treatment for MM. Notes: Survey question: How important to you are the following factors when making decisions about a next possible multiple myeloma treatment for you/your loved one? |
Trade-Offs for Better Treatment Response
Respondents were asked how likely they would be to accept certain trade-offs of a newer MM treatment with potentially a more favorable response. Figure 2 shows the ranking of the trade-offs among patients and care partners (1-Highly Unlikely; 4-Highly Likely). Most patients and care partners were likely or highly likely to tolerate some inconveniences for a better treatment response; this included increasing the frequency of clinic visits to monitor for side effects (88% patients, 80% care partners), taking medications more frequently (84% patients, 74% care partners), adding treatment to control side effects (79% patients, 83% care partners), and being in the hospital to start treatment (80% patients, 83% care partners). Care partners were more willing to assume greater family burden (77%) compared to patients (49%), and patients were more accepting of potential serious side effects (50%) than were care partners (34%).
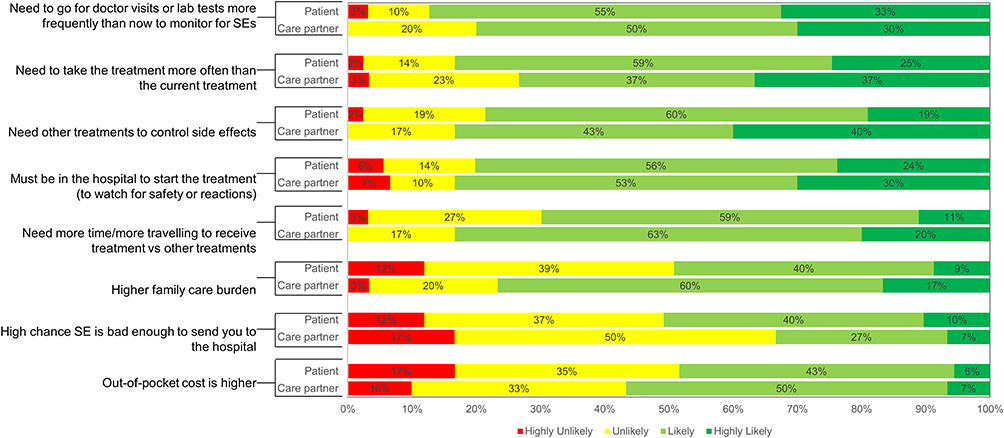 |
Figure 2 Acceptance of trade-offs for patients and care partners. Notes: Sample: All Patients (N=126) and care partners (N=30). Survey question: Imagine a new treatment for multiple myeloma was offered which would provide a very favorable response. How likely would you be to accept any of the following “trade-offs”? |
Patients and care partners were also asked to consider specific side effects as a trade-off for a new hypothetical treatment (Figure 3). Approximately 83% of patients and care partners were likely or highly likely to accept non-life-threatening cosmetic side effects. More than 70% of patients and care partners were likely or highly likely to accept a one-time side effect that may require hospitalization when starting treatment. A rare side effect that would be life threatening or cause a serious problem had the least acceptance, with 76% of both patients and care partners selecting “unlikely or highly unlikely” when presented with this statement.
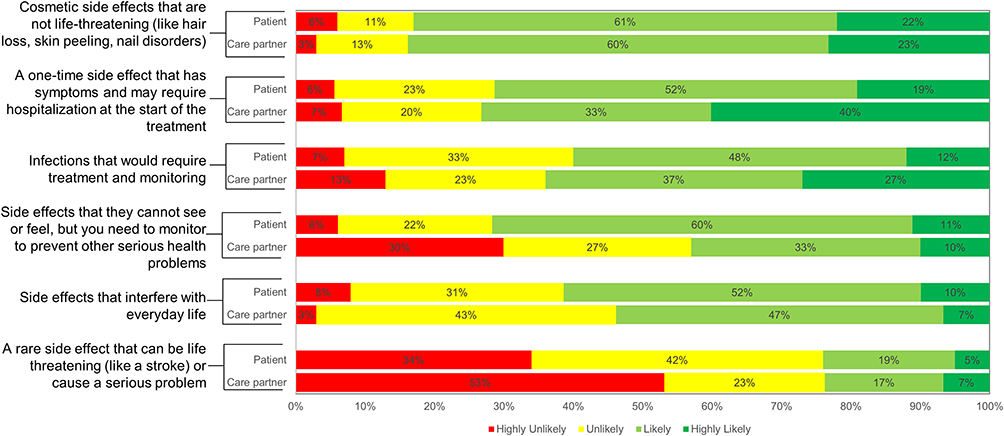 |
Figure 3 Acceptance of treatment side effects for patients and care partners. Notes: Sample: All Patients (N=126) and care partners (N=30). Survey question: Imagine a new treatment was offered to you for multiple myeloma which would provide a very favorable response. How likely would you be to accept the following types of side effects if they were known to occur with this treatment? |
Global Health Preferences
Although the trade-off exercises in this study were hypothetical, patients, care partners, and physicians often need to prioritize competing adverse side effects and desired outcomes when making treatment decisions. One way to clarify trade-offs in decision-making is to prioritize universal health outcomes. These outcomes include extension of life, reducing symptoms, and maintaining independence, which directly impact patients with various chronic conditions.27 The Time and Outcomes Preference Scale26 uses a 5-point scale to assess patient views on universal health outcomes and addresses two common trade-offs among these outcomes in treatment decisions: Subscale 1: quality versus quantity of life, and Subscale 2: present versus future health. The median score for the Subscale 1 was 3.5 for patients (interquartile range [IQR] 1.0) and 3.75 (IQR 1.5) for care partners, indicating more agreement with statements prioritizing quality over quantity of life. For Subscale 2, the median score was 2.17 (IQR 0.67) for patients and 2.33 (IQR 1.33) for care partners, suggesting more agreement with statements prioritizing future over present health.
Discussion
This study describes the treatment attributes and other factors valued by patients, care partners, and physicians during decision-making for MM treatment. Our findings show that the most important attributes among all groups were duration of response, QoL, and side effects. These attributes also did not change based on a patients’ number of relapses. Alignment on these top treatment attributes among individuals living with MM and their care team is consistent with previous preference research.6,28
Our study is unique in that few quantitative preference studies include QoL as a treatment attribute;29,30 most quantitative preference studies have focused on efficacy, safety, treatment frequency and mode, and cost attributes.6,28,31,32 The burden of MM has been shown to negatively impact patients’ QoL and their physical, emotional, and social wellbeing.33,34 While advances in MM treatment have extended life expectancy, treatment burden is substantial and patients need to balance the risk of disease complications and cumulative side effects from prolonged treatment.35 Our research highlights the significance of not concentrating solely on prolonging patients’ lifespan but also on effectively addressing the symptoms and adverse effects that impact their QoL.
Misalignment in understanding what is most important to patients and their care partners can lead to misconceptions about their needs and preferences, ultimately impacting the patient’s treatment journey. While there was agreement on the top treatment attributes, some heterogeneity among patients, care partners, and physicians was observed in factors that impacted QoL and trade-offs. For example, patients and care partners valued treatment factors related to QoL (eg, dosing frequency, care partner support requirements, treatment breaks) while physicians focused more on convenience factors (eg, monitoring frequency, medication administration). Additionally, when asked about trade-offs, patients and care partners showed a greater willingness to exchange convenience for the potential of achieving a better treatment response.
When evaluating patients by their experience with treatment relapses, a notable difference was found in the ranking of treatment breaks. For patients who experienced 4 or more relapses, treatment breaks were prioritized as the fifth most important attribute whereas those with 0–3 relapses ranked it last. Patients with relapsed or refractory MM are faced with complex trade-offs between benefits and risks across several treatment options, while enduring increased time burden, more frequent hospital visits, and longer treatment duration as their disease progresses.36 The fear of relapse and the uncertainty surrounding this clinical event have been highlighted as key contributors to emotional burden among patients;37 therefore, our findings may reflect patients who experienced side effects from prolonged treatment and who had increased care needs as their disease progressed. Understandably, treatment fatigue and burden are likely barriers to health and may impact outcomes.
As primary support systems, family members and care partners can be intimately involved in treatment decision-making. Although care partners’ and patients’ treatment preferences were mostly aligned, care partners were more willing to assume a greater family burden and placed lower importance on care partner support. Conversely, patients were more accepting of side effects compared to care partners. Improved and open communication between care partners and patients could enhance alignment in MM decision-making. According to a study by Pritlove et al, care partners typically assume the majority of the responsibilities related to illness care at home; however, this often came at the expense of the care partner’s own health needs.38 These findings may reflect that most care partners had a close relationship with their patient (eg, spouse or another relative) and may value long-term outcomes and improved QoL for their loved one. Another aspect to this is that care partners often neglect their own personal mental, social, and emotional well-being and, therefore, could benefit from receiving additional support for themselves.
Strengths and Limitations
There are several strengths in this study, which include the diverse representation of racial/ethnic groups in the three respondent groups; this is often a limitation in current literature. The important role of care partners in treatment decision-making and the patient journey is also highlighted in this study. The analysis includes a comparison of attributes across all disease stages (ie, newly diagnosed, early relapse, and late relapse), identifying how treatment decisions may change over a patient’s treatment journey.
Limitations to this study include the lack of generalizability of the results because the data from this descriptive study may not be representative of all people with MM, all care partners of people with MM, and all physicians treating people with MM. Due to the potentially non-representative data, descriptive statistics were chosen to prevent generating misleading or unreliable conclusions that might have been drawn from statistical comparisons and/or modeling. Patient respondents were from the US, and younger than the average age at which individuals are typically diagnosed with MM (median age 69). Also, given the online platform used for recruitment and survey administration, patients who are not engaged in social media or those who lack access to the internet or to electronic devices may be under-represented, resulting in selection and response bias. Additionally, recall bias may be relevant because participants may not remember previous events or experiences accurately or may omit important details. Furthermore, it is important to note that patients and care partners were not required to specify their roles when registering as members in the Inspire online health community. As a result, survey invitations were sent all potential and eligible members to participate, including those who had not previously identified as a patient or care partner. The low patient and care partner response rates may be partly due to individuals who received the survey invitation despite not being patients with MM or care partners. Finally, this study did not explore roles of other trusted healthcare team members, such as nurses and advanced practice clinicians, who may influence the treatment decision-making process with patients and care partners.
Conclusions
Given the complexity of MM treatment decisions and the impact on patients’ lives, understanding patients’ preferences and values is valuable to collaborative decision-making, which can reduce decisional conflict in treatment decisions. Our study emphasizes the importance of not only having a holistic treatment approach to targeting the disease, but also prioritizing the mitigation of treatment-related burden, while preserving patients’ daily functioning and emotional well-being. The differing perspectives among the groups in our study supports the need for clinicians to use SDM in their practice to ensure patients’ values and preferences are being elicited and incorporated into the treatment decision-making process. Additionally, considering care partners’ preferences and providing tailored support for them may alleviate care partners’ burden. Finally, individual treatment paths for MM may impact patients’ QoL differently; therefore, the practice of SDM through patient decision aids can be a vital tool in optimizing treatment outcomes while honoring patients’ personal values and preferences.
Acknowledgments
The study was previously presented at the European Hematology Association 2023 Annual Congress, held in Frankfurt, Germany, June 8-11, 2023. Dwyer L, Lin D, Wu B et al Shared decision-making in multiple myeloma: Do patients, caregivers, and physicians share the same goals and preferences? [P1690]. HemaSphere. 2023; 7(53). https://onlinelibrary.wiley.com/toc/25729241/2023/7/S3. Accessed October 1, 2024. The authors would like to acknowledge Peter Herout, PharmD for his contributions to the study design and management. TWL is a Scholar in Clinical Research of the Leukemia & Lymphoma Society.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Janssen Scientific Affairs, LLC.
Disclosure
LDO, DL, BW are current employees of Janssen Scientific Affairs, LLC. KLD, MY, and VK are employees of EPI-Q Inc., which received funding from Janssen Scientific Affairs, LLC associated with the development and execution of this study. JF and EK are current or former employees of Inspire Insights, which received funding associated with the development and execution of this study. TWL has received honoraria for consulting/advisory boards from AbbVie, Agilix, Agios/Servier, Apellis, Astellas, AstraZeneca, Beigene, BlueNote, BMS/Celgene, CareVive, Flatiron, Genentech, GSK, Lilly, Meter Health, Novartis, and Pfizer; speaking-related honoraria from AbbVie, Agios, Astellas, BMS/Celgene, and Incyte; equity interest in Dosentrx (stock options in a privately-held company); royalties from UpToDate; research funding from the AbbVie, American Cancer Society, AstraZeneca, BMS, Deverra Therapeutics, Duke University, GSK, Jazz Pharmaceuticals, Rigel, the Leukemia and Lymphoma Society, the National Institute of Nursing Research/ National Institutes of Health, and Seattle Genetics. JA has served on advisory boards for BMS, J&J, Pfizer, Regeneron, Sanofi, and Takeda Oncology. BF is a consultant to GSK, Janssen, Sanofi, and Pfizer. NB has served consulting/advisory roles for AbbVie, BMS, Janssen, Pfizer, and Sanofi; and, received research funding from Amgen, BMS, Karyopharm Therapeutics, and Merck. The authors report no other conflicts of interest in this work.
References
1. Surveillance Epidemiology, and End Results (SEER). Cancer stat facts: myeloma. Available from: https://seer.cancer.gov/statfacts/html/mulmy.html.
2. Mikhael J, Ismaila N, Cheung MC, et al. Treatment of multiple myeloma: ASCO and CCO joint clinical practice guideline. J Clin Oncol. 2019;37(14):1228–1263. doi:10.1200/JCO.18.02096
3. Rajkumar SV. Multiple myeloma: 2022 update on diagnosis, risk stratification, and management. Am J Hematol. 2022;97(8):1086–1107. doi:10.1002/ajh.26590
4. Cowan AJ, Green DJ, Kwok M, et al. Diagnosis and Management of Multiple Myeloma: a Review. JAMA. 2022;327(5):464. doi:10.1001/jama.2022.0003
5. Bazarbachi AH, Al Hamed R, Malard F, Harousseau J-L, Mohty M. Relapsed refractory multiple myeloma: a comprehensive overview. Leukemia. 2019;33(10):2343–2357. doi:10.1038/s41375-019-0561-2
6. Fifer SJ, Ho K-A, Lybrand S, Axford LJ, Roach S. Alignment of preferences in the treatment of multiple myeloma - a discrete choice experiment of patient, carer, physician, and nurse preferences. BMC Cancer. 2020;20(1):546. doi:10.1186/s12885-020-07018-6
7. Gupta S, Abouzaid S, Liebert R, Parikh K, Ung B, Rosenberg AS. Assessing the effect of adherence on patient-reported outcomes and out of pocket costs among patients with multiple myeloma. Clin Lymphoma Myeloma Leuk. 2018;18(3):210–218. doi:10.1016/j.clml.2018.01.006
8. Sonneveld P, De Wit E, Moreau P. How have evolutions in strategies for the treatment of relapsed/refractory multiple myeloma translated into improved outcomes for patients? Crit Rev Oncol/Hematol. 2017;112:153–170. doi:10.1016/j.critrevonc.2017.02.007
9. Tariman JD, Doorenbos A, Schepp KG, Becker PS, Berry DL. Patient, physician and contextual factors are influential in the treatment decision making of older adults newly diagnosed with symptomatic myeloma. Cancer Treat Commun. 2014;2(2–3):34–47. doi:10.1016/j.ctrc.2014.08.003
10. Tariman JD, Vahey-Marcello K, Huff CA, et al. Using continuing medical education to promote shared decision-making in patients diagnosed with multiple myeloma. Blood. 2016;128(22):2388. doi:10.1182/blood.V128.22.2388.2388
11. Joseph-Williams N, Newcombe R, Politi M, et al. Toward minimum standards for certifying patient decision aids: a modified delphi consensus process. Med Decis Mak. 2014;34(6):699–710. doi:10.1177/0272989X13501721
12. Krist AH, Tong ST, Aycock RA, Longo DR. Engaging Patients in Decision-Making and Behavior Change to Promote Prevention. Stud Health Technol Inform. 2017;2017:240. doi:10.3233/978-1-61499-790-0-284
13. Inspire Insights. 2023.
14. Kline E, Garrett AL, Brownstein C, et al. Using social media listening to understand barriers to genomic medicine for those living with Ehlers–Danlos syndromes and hypermobility spectrum disorders. Health Expectations. 2023;26(4):1524–1535. doi:10.1111/hex.13755
15. Robbins R, Jean-Louis G, Chanko N, Combs P, Byrne N, Loeb S. Using data from an online health community to examine the impact of prostate cancer on sleep. BJU Int. 2020;125(5):634–635. doi:10.1111/bju.14986
16. Tsai R, Hervey J, Hoffman K, et al. COVID-19 Vaccine Hesitancy and Acceptance among Individuals with Cancer, Autoimmune Diseases, or Other Serious Comorbid Conditions: cross-sectional, Internet-Based Survey. JMIR Public Health Surveill. 2022;8(1):e29872. doi:10.2196/29872
17. Timimi F, Ray S, Jones E, Aase L, Hoffman K. Patient-reported outcomes in online communications on statins, memory, and cognition: qualitative analysis using online communities. J Med Internet Res. 2019;21(11):e14809. doi:10.2196/14809
18. Ransohoff JD, Nikfarjam A, Jones E, et al. Detecting chemotherapeutic skin adverse reactions in social health networks using deep learning. JAMA Oncol. 2018;4(4):581. doi:10.1001/jamaoncol.2017.5688
19. M3 Global Research. Available from: https://m3globalresearch.blog/about-m3.
20. Samimi G, Heckman-Stoddard BM, Holmberg C, et al. Assessment of and interventions for women at high risk for breast or ovarian cancer: a survey of primary care physicians. Cancer Prev Res. 2021;14(2):205–214. doi:10.1158/1940-6207.CAPR-20-0407
21. Zetts RM, Stoesz A, Garcia AM, et al. Primary care physicians’ attitudes and perceptions towards antibiotic resistance and outpatient antibiotic stewardship in the USA: a qualitative study. BMJ Open. 2020;10(7):e034983. doi:10.1136/bmjopen-2019-034983
22. Edwards ML, Yin PT, Kuehn M, et al. Physician perceptions of drug utilization management: results of a national survey. PLoS One. 2022;17(9 September):e0274772. doi:10.1371/journal.pone.0274772
23. Wempe MM, Stewart MD, Glass D, et al. A national assessment of diagnostic test use for patients with advanced NSCLC and factors influencing physician decision-making. Am Health Drug Benef. 2020;13(3):110–119.
24. Bylund CL, Eggly S, LeBlanc TW, et al. Survey of patients and physicians on shared decision-making in treatment selection in relapsed/refractory multiple myeloma. Transl Behav Med. 2023;13(4):255–267. doi:10.1093/tbm/ibac099
25. Shields AM, Brown H, Phillips N, Drayson MT, Richter AA, Richter AG. Health Care Professionals’ Confidence and Preferences for Diagnostic Assays for SARS-CoV-2: a Global Study. Front Public Health. 2021;9:569315. doi:10.3389/fpubh.2021.569315
26. Case SM, Towle VR, Fried TR. Considering the Balance: development of a scale to assess patient views on trade-offs in competing health outcomes. J Am Geriatr Soc. 2013;61:1331–1336. doi:10.1111/jgs.12358
27. Fried TR, Tinetti M, Agostini J, et al. Health outcome prioritization to elicit preferences of older persons with multiple health conditions. Patient Educ Couns. 2011;83(2):278–282. doi:10.1016/j.pec.2010.04.032
28. Auclair D, Mansfield C, Fiala MA, et al. Preferences and Priorities for Relapsed Multiple Myeloma Treatments Among Patients and Caregivers in the United States. Patient Prefer Adherence. 2022;16:573–585. doi:10.2147/PPA.S345906
29. Mühlbacher AC, Nübling M. Analysis of physicians’ perspectives versus patients’ preferences: direct assessment and discrete choice experiments in the therapy of multiple myeloma. Eur J Health Econ. 2011;12(3):193–203. doi:10.1007/s10198-010-0218-6
30. Mühlbacher AC, Lincke HJ, Nübling M. Evaluating patients’ preferences for multiple myeloma therapy, a Discrete-Choice-Experiment. Psychosoc Med. 2008;2008:5.
31. Batchelder L, Philpott S, Divino V, et al. Physician treatment preferences for relapsed/refractory multiple myeloma: a discrete choice experiment. Future Oncol. 2022;18(25):2843–2856. doi:10.2217/fon-2022-0378
32. Tervonen T, Duenas A, Collacott H, et al. Current Health State Affected Patient Preferences More Than Disease Status: a Discrete Choice Experiment in Multiple Myeloma. Value Health. 2023;26(6):909–917. doi:10.1016/j.jval.2023.01.016
33. Gatopoulou X, Iraqi W, Morgan K, et al. The Burden of a Multiple Myeloma Diagnosis on Patients and Caregivers in the First Year: western European Findings. Clinicoecon Outcomes Res. 2022;14:731–753. doi:10.2147/CEOR.S367458
34. Lyall M, Crawford R, Bell T, et al. Characterizing the Patient Journey in Multiple Myeloma: qualitative Review. JMIR Cancer. 2022;8(3):e39068. doi:10.2196/39068
35. Zaleta AK, Miller MF, Olson JS, et al. Symptom burden, perceived control, and quality of life among patients living with multiple myeloma. J Natl Compr Canc Netw. 2020;18(8):1087–1095. doi:10.6004/jnccn.2020.7561
36. Chari A, Romanus D, DasMahapatra P, et al. Patient-Reported Factors in Treatment Satisfaction in Patients with Relapsed/Refractory Multiple Myeloma (RRMM). Oncologist. 2019;24(11):1479–1487. doi:10.1634/theoncologist.2018-0724
37. Hulin C, Hansen T, Heron L, et al. Living with the burden of relapse in multiple myeloma from the patient and physician perspective. Leukemia Res. 2017;59:75–84. doi:10.1016/j.leukres.2017.05.019
38. Pritlove C, Jassi M, Burns B, McCurdy A. The work of managing multiple myeloma and its implications for treatment-related decision making: a qualitative study of patient and caregiver experiences. BMC Cancer. 2021;21(1):793. doi:10.1186/s12885-021-08527-8
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.