Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
Treatment-Refractory Central Centrifugal Cicatricial Alopecia Responsive to a Novel Botanical Treatment
Authors Umar S ![]() , Kan P
, Kan P ![]() , Carter MJ
, Carter MJ ![]() , Shitabata P
, Shitabata P ![]()
Received 15 January 2022
Accepted for publication 31 March 2022
Published 8 April 2022 Volume 2022:15 Pages 609—619
DOI https://doi.org/10.2147/CCID.S358618
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Sanusi Umar,1– 3 Petrina Kan,4 Marissa J Carter,5 Paul Shitabata1,2,6
1Department of Medicine, University of California at Los Angeles, Los Angeles, CA, USA; 2Division of Dermatology, Department of Medicine, Harbor-UCLA Medical Center, Torrance, CA, USA; 3Dr. U Hair and Skin Clinic, Manhattan Beach, CA, USA; 4Department of Molecular Biology, University of California at Los Angeles, Los Angeles, CA, USA; 5Strategic Solutions, Inc, Bozeman, MT, USA; 6Dermatopathology Institute, Torrance, CA, USA
Correspondence: Sanusi Umar, Dr. U Hair and Skin Clinic, 2121 N. Sepulveda Avenue, Suite 200, Manhattan Beach, CA, 90266, USA, Tel +1 (310) 318-1500, Fax +1 (310) 318-1590, Email [email protected]
Purpose: Central centrifugal cicatricial alopecia (CCCA) is the most common cause of scarring alopecia in women of African descent. However, current treatments for CCCA, such as immunosuppressants and immunomodulatory pharmaceutical agents, have suboptimal efficacy and undesirable side effects. This case series reports the therapeutic effect of a new botanical formulation (Dr. UGro Gashee) in four patients with histologically supported diagnoses of CCCA. The formulations contain at least three phytoactive ingredients that affect multiple targets in the cascade of pathophysiologic events contributing to CCCA. Possible mechanisms of action include anti-inflammatory effects, inhibiting proinflammatory cytokines, and the net antifibrotic effect of inhibiting transforming growth factor-beta while upregulating AMP-activated protein kinase and peroxisome proliferator-associated receptor-gamma activity.
Patients and Methods: Four African American women with treatment-refractory CCCA were treated with a new topical botanical formula (cosmeceutical) alone or in combination with its oral formulation (nutraceutical) for 8 weeks to 1 year. The cosmeceutical and nutraceutical treatments contain similar phytoactive ingredient profiles. Treatment outcomes were collected using documented patient reports and images and by direct observation.
Results: In all patients, scalp pruritus cessation occurred within 2 weeks of treatment, and significant hair regrowth was observed within 2 months. All patients reported a high satisfaction level without adverse effects.
Conclusion: Patients with treatment-refractory CCCA responded to the novel botanical treatment reported in this study. Further evaluations in a controlled trial with more patients are warranted.
Keywords: scarring alopecia, follicular degeneration syndrome, hot comb alopecia, African American women, hair loss, cosmeceutical, nutraceutical, phytoactive
Plain Language Summary
Central centrifugal cicatricial alopecia (CCCA) is a chronic and severe condition that causes permanent hair loss and scarring. It is most common in women of African descent. Current pharmaceutical treatments are inadequate, with the potential for side effects that limit long-term use. We report four patients successfully treated for a period between 8 weeks and 1 year with the botanical formulations of Dr. UGro Gashee. The treatments were administered topically or in combination with its oral formulation. Significant hair regrowth was observed in all the patients. All patients reported cessation of scalp itch and no adverse effects.
Introduction
Central centrifugal cicatricial alopecia (CCCA), previously called follicular degeneration syndrome and hot comb alopecia, is a form of scarring alopecia characterized by permanent hair loss mainly in the vertex/crown region, of the scalp that spreads centrifugally with symptoms of inflammation, pain, or tenderness. The disease primarily occurs in middle-aged women of African descent. It is the most common form of scarring hair loss in African American women, affecting approximately 15% of the aforementioned population.1,2 CCCA rarely affects men or individuals belonging to other ethnic groups.1 At its onset, it is characterized by thinning hair at the central zones of the vertex, eventually resulting in permanent scarring alopecia that expands centrifugally to the entire scalp.2 Histologically, CCCA is characterized by varying degrees of fibrosis, lymphocytic inflammation, and follicular degeneration.3
Although genetic factors and hair grooming practices are significant contributors to CCCA, the exact mechanism by which CCCA occurs is unknown. Studies have implicated the role of pro-inflammatory factors, including tumor necrosis factor (TNF) and interleukin 6 (IL-6),4 increased fibrosis through the upregulation of the profibrotic factor transforming growth factor-beta (TGF-β),4,5 and the downregulation of fibrosis-mitigating factors, including peroxisome proliferator-activated receptor gamma (PPAR-γ)5 and AMP-activated protein kinase (AMPK).4,6 Additionally, a genetic predisposition to a lymphocytic immune response and loss of follicular immune privilege has been proposed.5 Other studies have suggested that CCCA is a variant of lichen planopilaris (LPP), whereby repeated trauma from heat, chemicals, and traction induces a Koebner-type reaction that manifests as CCCA, as the increased activity of the lymphocytes of the same immunophenotypes and smoldering fibrosis are observed in both conditions.7
Immunosuppressants and topical and intralesional steroids are used to stop inflammation and fibrotic activity in patients with CCCA, though these drugs are not specific.8–10 The chronic use of these drugs is often not feasible due to their side effects. Other treatments include tetracyclines, hydroxychloroquine, oral and topical minoxidil, calcineurin inhibitors, mycophenolate, cyclosporine, thalidomide, and topical metformin.5,6,10,11 However, these treatments often have suboptimal efficacy and are frequently associated with complications.
Literature Review and Case Series
Although there appears to be heightened interest in the role of botanicals and phytochemicals in the treatment of CCCA,12 we are only aware, from a literature search of the National Library of Medicine (PubMed) and SCOPUS databases in December 2021, of one patient in a publication13 we authored where we evaluated CCCA treatment using botanicals/non-pharmaceuticals. In the aforementioned paper, the effectiveness of a topical phytochemical formulation (Dr. UGro Gashee®, FineTouch Laboratories, Manhattan Beach, CA) designed to treat hair loss using a multimodal approach was evaluated in five patients with varying forms of alopecia. The paper described the key components and principles used in its formulation,13 and we reported a 50-year-old African American woman with a clinical diagnosis of traction alopecia and a histological diagnosis of CCCA, who had failed prior treatments with minoxidil and topical and intralesional steroid injections (Figure 1).13 Based on this observation, we reviewed our records of patients with histologically proven diagnoses of CCCA who were treated primarily with Gashee botanicals formulations. All patients had received either the topical Gashee formulation alone or in combination with Gashee oral hair supplements. Both oral and topical formulations of Gashee contain at least three botanical ingredients that favorably modulate several CCCA mechanistic processes.14–41 We herein report a case series of four treatment-refractory patients treated with either topical Gashee (cosmeceutical) alone or in combination with an oral Gashee formulation (nutraceutical).
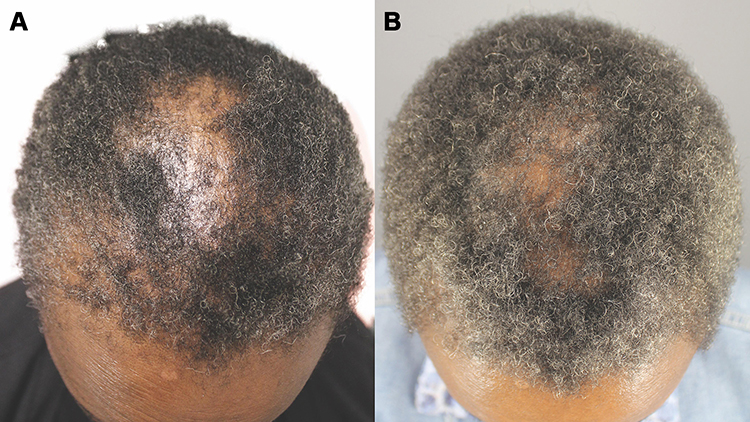 |
Figure 1 Vertex of the head of the patient from a previously authored study Images of the top of the head of a patient diagnosed with central centrifugal cicatricial alopecia obtained before (A) and after (B) 3 months of using Gashee lotion alone are shown. These images are used with permission from Case Reports in Dermatological Medicine (Umar S, Carter MJ. A multimodal hair-loss treatment strategy using a new topical phytoactive formulation: a report of five cases. Case Rep Dermatol Med. 2021;2021:6659943. Published online February 4, 2021. doi: 0.1155/2021/6659943; Figure 9). |
Ethics Statement
All patients provided written consent to publish the data and images in this report. This study was conducted in accordance with the 2013 Declaration of Helsinki. Approval from an Institutional Review Board was not sought or required given the retrospective description of the clinical findings in the routine care of the patients.
Patient 1
A 58-year-old African American woman with a long history of wearing tight ponytails and sister locks had a 6-year history of hair loss with scalp pruritus and significant thinning of the hair in the vertex zones (Figure 2A). A biopsy obtained from the anterior vertex showed histological features of perifollicular fibrosis, lymphocytic infiltrates, and desquamation of the outer root sheath supporting a diagnosis of CCCA. The patient had received prior treatments of other natural oral hair supplements and topical 5% minoxidil foam with suboptimal results and an adverse reaction of scalp irritation. After discontinuing her previous treatments, she started using Gashee lotion twice daily, that is, 1 mL per a palm-sized treatment area, combined with four daily capsules of Gashee oral supplements. Her scalp pruritus ceased within 2 weeks of treatment. New hair growth and improved coverage in the CCCA-affected vertex area were observed after 8 weeks of treatment (Figure 2B). The patient reported no adverse effects.
 |
Figure 2 Vertex and back of the head of patient 1 Images of the vertex and back of the head of a patient diagnosed with central centrifugal cicatricial alopecia before (A) and after (B) treatment with Gashee lotion and oral supplements. |
Patient 2
A 51-year-old African American woman reported a 3-year history of hair loss and the chronic use of chemical hair relaxers. She had mild scalp pruritus and irritation with marked thinning extending from the central zone of the vertex to the frontal area (Figure 3A). CCCA was confirmed histologically. Prior treatment with topical 5% minoxidil solution was unsuccessful. After discontinuing minoxidil, the patient started using topical Gashee lotion twice daily, that is, 1 mL per a palm-sized treatment area, and four daily capsules of Gashee oral supplements. At approximately 2 weeks of treatment, she noted a significant reduction of scalp pruritus and irritation, and at 5 months of treatment, hair coverage in the affected areas improved (Figure 3B). After 1 year of treatment, the improved hair coverage remained (Figures 4A and B), and the patient reported no adverse effects.
 |
Figure 3 Top of the head of patient 2 Images of the top of the head of a patient diagnosed with central centrifugal cicatricial alopecia obtained before (A) and after (B) 5 months of treatment with Gashee lotion and oral supplements. |
 |
Figure 4 Posterior vertex and back of the head of patient 2 Images of the posterior vertex and back of the head of a patient diagnosed with central centrifugal cicatricial alopecia obtained before (A) and after (B) 1 year of treatment with Gashee lotion and oral supplements. |
Patient 3
A 56-year-old African American woman reported a 1-year history of hair loss, inability to attain hair length, scalp pruritus, and chronic flat iron use to straighten her hair (Figure 5A). A biopsy confirmed a diagnosis of CCCA. Moreover, the patient reported suboptimal results after previous treatments of clobetasol 0.05% ointment and 50 mg daily of oral spironolactone. After discontinuing all other treatments, the patient started applying topical Gashee lotion once daily, that is, 1 mL per a palm-sized treatment area. Moreover, she began Gashee oral hair supplements with four capsules a day and underwent two sessions of platelet-rich plasma (PRP) scalp injections. Minimal improvement was noted 5 months later, although her scalp pruritus had resolved, and CCCA did not progress any further (Figure 5B). Subsequently, the patient was started on oral minoxidil at 0.625 mg daily. A session of scalp injections of micronized fat was performed. However, 13 months later, the patient showed minimal improvement. Due to supply issues that affected the availability of the oral Gashee supplement, the patient was advised to increase the frequency of her topical Gashee application from once daily to twice daily. Three months later, rapid hair regrowth with considerable coverage in all areas that had been refractory to the previous treatments and regimens was observed (Figures 6–8). Then, oral minoxidil was discontinued, and topical therapy was maintained as a sole treatment. A follow-up at three months and again at four months showed continuing hair growth with new areas of coverage and no hair shedding noted. She also noted significant improvement in hair length (Figure 9). Furthermore, histological analysis of biopsies taken from the left side of the vertex before and at four months after using topical gashee as a sole treatment showed interval changes of marked reduction in inflammatory cells, increased number of vellus hairs coinciding with a significant increase in adipocytes (Figures 10 and 11).
 |
Figure 5 Left parietal area and vertex of patient 3 Images of the left parietal area and vertex of a patient diagnosed with central centrifugal cicatricial alopecia obtained before (A) and after (B) 5 months of treatment with topical Gashee (applied once daily) and two sessions of platelet-rich plasma scalp injections are shown. |
 |
Figure 6 Left parietal area and vertex of patient 3 Images of the left parietal area and vertex of a patient diagnosed with central centrifugal cicatricial alopecia obtained 13 months after micronized fat injection, oral minoxidil, topical Gashee applications (once daily), and oral Gashee supplements (A). Images of the same area 3 months after treatment changed to topical Gashee treatments (twice daily) and oral minoxidil are shown (B). |
 |
Figure 7 Right parietal area and vertex of patient 3 Images of the right parietal area and vertex of a patient diagnosed with central centrifugal cicatricial alopecia obtained 13 months after micronized fat injection, oral minoxidil, topical Gashee applications (once daily), and oral Gashee supplements (A). Images of the same area 3 months after the treatment changed to topical Gashee treatments (twice daily) and oral minoxidil are shown (B). |
 |
Figure 8 Right parietal area and vertex of patient 3 Images of the vertex and posterior scalp of a patient with central centrifugal cicatricial alopecia obtained 13 months after micronized fat injection, oral minoxidil, topical Gashee applications (once daily), and oral Gashee supplements (A). Images of the same area 3 months after the treatment changed to topical Gashee treatments (twice daily) and oral minoxidil are shown (B). |
 |
Figure 9 Vertex and left parietal area of patient 3. Images of the vertex and posterior scalp (A) and left parietal area (B) of a patient with central centrifugal cicatricial alopecia obtained at 3 months and 4 months, respectively, after cessation of oral minoxidil and using topical Gashee twice a day as sole therapy. |
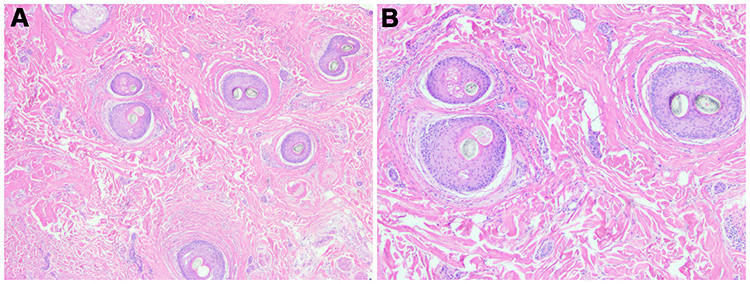 |
Figure 10 Hematoxylin and eosin stain of the vertex zone of Patient 3 at the time of stopping oral minoxidil The transverse section magnification X2 (A) and magnification X4 (B) show all follicles in catagen phase with a mild perifollicular lymphocytic infiltrate. One follicle shows premature desquamation of the inner root sheath. Scarring with diminished adipocytes is noted. |
 |
Figure 11 Hematoxylin and eosin stain of the vertex zone of Patient 3 at fourteen weeks after stopping oral minoxidil and using twice-daily topical Gashee as sole therapy. The transverse section magnification X2 (A) and magnification X4 (B) show follicles with mixed anagen and catagen phase as well as several vellus hair follicles, with increased adipocytes and absence of inflammation. |
Patient 4
A 55-year-old African American woman with a family history of hair loss reported the chronic use of a flat iron and hot comb for hair straightening and a 5-year history of hair loss. The patient exhibited significant thinning of hair extending from the central zone of the vertex, and a diagnosis of CCCA was confirmed histologically (Figure 12A). Prior treatments with a different oral nutraceutical, topical minoxidil 5% foam and clobetasol 0.05% ointment, were unsuccessful. After the discontinuation of previous treatments, she started using Gashee lotion twice daily, that is, 1 mL per a palm-sized treatment area, with four daily capsules of Gashee oral supplements. New hair growth and improved coverage in the CCCA-affected areas of the vertex were observed after 13 weeks of treatment (Figure 12B). The patient reported no adverse effects.
 |
Figure 12 Central vertex of Patient 4 Images of the central vertex of a patient with central centrifugal cicatricial alopecia obtained before (A) and after (B) 13 months of treatment with Gashee lotion and oral supplements are shown. |
Discussion
CCCA is a condition of scarring alopecia in women of African descent. The natural history of this disease is a chronic unremitting course that is poorly responsive to pharmaceutical treatments, with a high potential for adverse effects. Thus, there is a high unmet need for therapeutics that are effective and safe for chronic use. All four patients in this report and a fifth patient we described in a previous publication13 responded favorably to treatment using Gashee formulations. Of the five patients in the combined reports, three were on a regimen that combined topical and oral formulations. In contrast, two patients responded to topical Gashee alone. Although one of the latter in this group was initially on a combination of oral and topical treatments, her positive response was associated with a change in the application of topical Gashee alone from once daily to twice daily. Furthermore, she continued to show progressive improvement after discontinuing all other treatments. This suggests the need to further evaluate the optimal dosing of the topical regimen in larger controlled trials. Our findings here and those related to the patient previously reported13 may be explained by at least three ingredients found in both the topical and oral formulations of Gashee and discussed in more detail below. These ingredients may favorably impact hair loss, fibrosis, and inflammation that characterizes CCCA through the inhibition of TGF-β, upregulation of fibrosis-mitigating AMPK and PPAR-γ, and anti-inflammatory properties.
TGF-β1 Inhibition
TGF-β1 derived from dermal papillae cells inhibits hair growth and initiates catagen.14–16 It promotes fibrosis by the Smad pathway17–19 and is upregulated under various fibroproliferative conditions.4,20 The genes encoding TGF-β were upregulated in CCCA tissue compared with non-involved tissues of the same patient.4 Therefore, TGF-β1 is considered a significant factor in the pathogenesis of CCCA.20 Turmeric (curcumin), which is in both the topical and oral Gashee formulas, has been found to inhibit TGF-β (Table 1).
 |
Table 1 CCCA-Relevant Properties of Various Gashee Components |
AMPK and PPAR-γ Upregulation
AMPK and PPAR-γ play significant roles in the pathogenesis of several fibroproliferative diseases.4,32,33 In CCCA, protein kinase AMP-activated catalytic subunit alpha 2 (PRKAA2), the gene encoding the nuclear receptor AMPK, is downregulated.4 In a recent report, 10% topical metformin, an AMPK activator, regrew hair in two patients with advanced CCCA.5 PPAR-γ plays a vital role in lipid metabolism. It is anti-inflammatory and exerts antifibrotic activity both directly and indirectly by mitigating the fibrotic effects of TGF-β. The downregulation of PPAR-γ has been implicated in LPP, a similar primary cicatricial alopecia.34–37 Furthermore, it has been proposed that autoimmune attacks lead to the loss of follicular immune privileges and that TGF-β causes hair loss and fibrosis, which is unopposed by the downregulation of PPAR-γ.5 Several ingredients of the topical and oral forms of Gashee (including turmeric (curcumin),34,38–40 fenugreek oil (Trigonella foenum-graecum),22–24 and Fo-ti (Polygonum multiflorum)17,30,31) may exert anti-fibrotic effects in patients with CCCA (Table 1). These ingredients have been shown to upregulate the activity of both AMPK and PPAR-γ.
Anti-Inflammatory Activity
A study comparing CCCA-affected scalp tissue to non-affected scalps showed upregulated genes encoding pro-inflammatory cytokines IL-6 and members of the TNF superfamily.4 Topical and intralesional steroids, the current CCCA treatment of choice, suppress inflammation. Several ingredients in both the oral and topical formulations of Gashee have anti-inflammatory properties that are beneficial for patients with CCCA (Table 1), including turmeric (curcumin)25–27 and fenugreek oil (Trigonella foenum-graecum).28,29,41
Limitations
This study had some limitations, with its small sample size and retrospective nature as the main limitations. A prospective and well-controlled study that evaluates the use and optimal dosing of topical Gashee, oral Gashee, and combination treatment will better clarify its safety and efficacy in patients with CCCA.
Conclusion
The use of botanical and natural ingredients for the treatment of CCCA is gaining interest due to the refractory nature of the disease and suboptimal nature of current therapies.12 Although this case series is limited by its small sample size, our results suggest that the role of Gashee in the treatment of CCCA, including optimal dosing, warrants further investigation in larger controlled trials.
Abbreviations
CCCA, central centrifugal cicatricial alopecia; TNF, tumor necrosis factor; IL-6, interleukin 6; TGF-β, transforming growth factor-beta; PPAR-γ, peroxisome proliferator-activated receptor-gamma; AMPK, AMP-activated protein kinase; LPP, lichen planopilaris; PRP, platelet-rich plasma.
Ethics Approval and Informed Consent
All patients provided written consent to publish the data and images in this report. The study was conducted in accordance with the Declaration of Helsinki (revised 2013). Approval from an Institutional Review Board was not sought or required given the retrospective description of clinical findings in routine care of the patients.
Acknowledgments
The authors are particularly grateful to the patients.
Funding
This study received no funding.
Disclosure
Dr. Sanusi Umar has a patent application for Gashee and has equity in its parent company, FineTouch Laboratories Inc. Petrina Kan, Dr. Marissa J Carter, and Dr. Paul Shitabata declare no conflicts of interest in this work.
References
1. Bin Saif GA, McMichael A, Kwatra SG, et al. Central centrifugal cicatricial alopecia severity is associated with cowhage-induced itch. Br J Dermatol. 2013;168(2):253–256. doi:10.1111/bjd.12043
2. Aguh C, McMichael A. Central centrifugal cicatricial alopecia. JAMA Dermatol. 2020;156(9):1036. doi:10.1001/jamadermatol.2020.1859
3. Malki L, Sarig O, Romano MT, et al. Variant PADI3 in central centrifugal cicatricial alopecia. N Engl J Med. 2019;380(9):833–841. doi:10.1056/NEJMoa1816614
4. Aguh C, Dina Y, Talbot CC Jr, Garza L. Fibroproliferative genes are preferentially expressed in central centrifugal cicatricial alopecia. J Am Acad Dermatol. 2018;79(5):904–912. doi:10.1016/j.jaad.2018.05.1257
5. Araoye EF, Thomas JAL, Aguh CU. Hair regrowth in 2 patients with recalcitrant central centrifugal cicatricial alopecia after use of topical metformin. JAAD Case Rep. 2020;6(2):106–108. doi:10.1016/j.jdcr.2019.12.008
6. Olsen EA, Whiting D, Bergfeld W, Olsen EA, Whiting D, Bergfeld W, et al. A multicenter, randomized, placebo-controlled, double-blind clinical trial of a novel formulation of 5% minoxidil topical foam versus placebo in the treatment of androgenetic alopecia in men. J Am Acad Dermatol. 2007;57(5):767–774. doi:10.1016/j.jaad.2007.04.012
7. Alahmari L, Almesned R, Alhumidi A, Alkhalifah A. Lichen planopilaris with koebner phenomenon. JAAD Case Rep. 2018;4(8):848–850. doi:10.1016/j.jdcr.2018.05.009
8. Gathers RC, Lim HW. Central centrifugal cicatricial alopecia: past, present, and future. J Am Acad Dermatol. 2009;60(4):660–668. doi:10.1016/j.jaad.2008.09.066
9. Callender VD, Kazemi A, Young CM, et al. Safety and efficacy of clobetasol propionate 0.05% emollient foam for the treatment of central centrifugal cicatricial alopecia. J Drugs Dermatol. 2020;19(7):719–724. doi:10.36849/JDD.2020.5201
10. Okereke UR, Simmons A, Callender VD. Current and emerging treatment strategies for hair loss in women of color. Int J Womens Dermatol. 2019;5(1):37–45. doi:10.1016/j.ijwd.2018.10.021
11. Herskovitz I, Miteva M. Central centrifugal cicatricial alopecia: challenges and solutions. Clin Cosmet Investig Dermatol. 2016;9:175–181. doi:10.2147/CCID.S100816
12. Ezekwe N, King M, Hollinger JC. The use of natural ingredients in the treatment of alopecias with an emphasis on central centrifugal cicatricial alopecia: a systematic review. J Clin Aesthet Dermatol. 2020;13(8):23–27.
13. Umar S, Carter MJ. A multimodal hair-loss treatment strategy using a new topical phytoactive formulation: a report of five cases. Case Rep Dermatol Med. 2021;2021:6659943. doi:10.1155/2021/6659943
14. Hu Y, Liang H, Du Y, et al. Curcumin inhibits transforming growth factor-beta activity via inhibition of smad signaling in HK-2 cells. Am J Nephrol. 2010;31(4):332–341. doi:10.1159/000287230
15. Shishodia S. Molecular mechanisms of curcumin action: gene expression. Biofactors. 2013;39(1):37–55. doi:10.1002/biof.1041
16. Gupta SC, Patchva S, Aggarwal BB. Therapeutic roles of curcumin: lessons learned from clinical trials. AAPS J. 2013;15(1):195–218. doi:10.1208/s12248-012-9432-8
17. Gu W, Yang M, Bi Q, et al. Water extract from processed polygonum multiflorum modulate gut microbiota and glucose metabolism on insulin resistant rats. BMC Complement Med Ther. 2020;20(1):107.
18. Conic RRZ, Piliang M, Bergfeld W, Atanaskova-Mesinkovska N. Vitamin D status in scarring and nonscarring alopecia. J Am Acad Dermatol. 2021;85(2):478–480. doi:10.1016/j.jaad.2018.04.032
19. Jung D-H, Park H-J, Byun H-E, et al. Diosgenin inhibits macrophage-derived inflammatory mediators through downregulation of CK2, JNK, Nf-κb AND AP-1 activation. Int Immunopharmacol. 2010;10(9):1047–1054. doi:10.1016/j.intimp.2010.06.004
20. Subash J, Alexander T, Beamer V, McMichael A. A proposed mechanism for central centrifugal cicatricial alopecia. Exp Dermatol. 2020;29(2):190–195. doi:10.1111/exd.13664
21. Rinwa P, Kaur B, Jaggi AS, Singh N. Involvement of PPAR-gamma in curcumin-mediated beneficial effects in experimental dementia. Naunyn Schmiedebergs Arch Pharmacol. 2010;381(6):529–539. doi:10.1007/s00210-010-0511-z
22. Gautam S, Ishrat N, Yadav P, et al. 4-Hydroxyisoleucine attenuates the inflammation-mediated insulin resistance by the activation of AMPK and suppression of SOCS-3 coimmunoprecipitation with both the IR-β subunit as well as IRS-1. Mol Cell Biochem. 2016;414(1–2):95–104. doi:10.1007/s11010-016-2662-9
23. Zayed EA, AinShoka AA, El Shazly KA, et al. Fenugreek oil and metformin improve insulin resistance via increase of GLUT4 and PPARγ in metabolic syndrome‐induced rats. Asian J Res Rep Endocrinol. 2021;4:29–39.
24. Muraki E, Hayashi Y, Chiba H, et al. Dose-dependent effects, safety and tolerability of fenugreek in diet-induced metabolic disorders in rats. Lipids Health Dis. 2011;10:240. doi:10.1186/1476-511X-10-240
25. Panahi Y, Hosseini MS, Khalili N, et al. Effects of curcumin on serum cytokine concentrations in subjects with metabolic syndrome: a post-hoc analysis of a randomized controlled trial. Biomed Pharmacother. 2016;82:578–582. doi:10.1016/j.biopha.2016.05.037
26. Jurenka JS. Anti-inflammatory properties of curcumin, a major constituent of curcuma longa: a review of preclinical and clinical research. Altern Med Rev. 2009;14(2):141–153.
27. Abe Y, Hashimoto S, Horie T. Curcumin inhibition of inflammatory cytokine production by human peripheral blood monocytes and alveolar macrophages. Pharmacol Res. 1999;39(1):41–47. doi:10.1006/phrs.1998.0404
28. Chowdhury AA, Gawali NB, Munshi R, Juvekar AR. Trigonelline insulates against oxidative stress, proinflammatory cytokines and restores BDNF levels in lipopolysaccharide induced cognitive impairment in adult mice. Metab Brain Dis. 2018;33(3):681–691. doi:10.1007/s11011-017-0147-5
29. Moers-Carpi M. Influence of nutritive factors on hair growth. Aktuelle Derm. 2011;37:171–175. doi:10.1055/s-0030-1256369
30. Park SY, Jin ML, Chae SY, et al. Novel compound from polygonum multiflorum inhibits inflammatory response in LPS-stimulated microglia by upregulating AMPK/Nrf2 pathways. Neurochem Int. 2016;100:21–29. doi:10.1016/j.neuint.2016.08.006
31. Sun YN, Li W, Song SB, et al. Nuclear factor kappa B activation and peroxisome proliferator-activated receptor transactivational effects of chemical components of the roots of polygonum multiflorum. Pharmacogn Mag. 2016;12(45):31–35. doi:10.4103/0973-1296.176019
32. Rangarajan S, Bone NB, Zmijewska AA, et al. Metformin reverses established lung fibrosis in a bleomycin model. Nat Med. 2018;24(8):1121–1127. doi:10.1038/s41591-018-0087-6
33. da Silva Morais A, Abarca-Quinones J, Guigas B, et al. Development of hepatic fibrosis occurs normally in AMPK-deficient mice. Clin Sci (Lond). 2009;118(3):411–420. doi:10.1042/CS20090293
34. Islam N, Garza LA. Adipose and hair function: an aPPARent connection. J Invest Dermatol. 2018;138(3):480–482. doi:10.1016/j.jid.2017.10.019
35. Sardella C, Winkler C, Quignodon L, et al. Delayed hair follicle morphogenesis and hair follicle dystrophy in a lipoatrophy mouse model of Pparg total deletion. J Invest Dermatol. 2018;138(3):500–510. doi:10.1016/j.jid.2017.09.024
36. Karnik P, Tekeste Z, McCormick TS, et al. Hair follicle stem cell-specific PPARgamma deletion causes scarring alopecia. J Invest Dermatol. 2009;129(5):1243–1257. doi:10.1038/jid.2008.369
37. Mirmirani P, Karnik P. Lichen planopilaris treated with a peroxisome proliferator-activated receptor gamma agonist. Arch Dermatol. 2009;145(12):1363–1366. doi:10.1001/archdermatol.2009.283
38. Kim T, Davis J, Zhang AJ, et al. Curcumin activates AMPK and suppresses gluconeogenic gene expression in hepatoma cells. Biochem Biophys Res Commun. 2009;388(2):377–382. doi:10.1016/j.bbrc.2009.08.018
39. Siddiqui AM, Cui X, Wu R, et al. The anti-inflammatory effect of curcumin in an experimental model of sepsis is mediated by up-regulation of peroxisome proliferator-activated receptor-gamma. Crit Care Med. 2006;34(7):1874–1882. doi:10.1097/01.CCM.0000221921.71300.BF
40. Wang HM, Zhao YX, Zhang S, et al. PPAR gamma agonist curcumin reduces the amyloid-beta-stimulated inflammatory responses in primary astrocytes. J Alzheimers Dis. 2010;20(4):1189–1199. doi:10.3233/JAD-2010-091336
41. Wani SA, Kumar P. Fenugreek: a review on its nutraceutical properties and utilization in various food products. J Saudi Soc Agric Sci. 2018;17(2):97–106. doi:10.1016/j.jssas.2016.01.007
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.