Back to Journals » International Journal of Women's Health » Volume 18
A Crowdsourced Topic Map and Future Research Agenda for Women’s Health
Authors Verhulst S, Singh R, Dell'Aquila M, Kunze L, Lenz C ![]()
Received 19 December 2025
Accepted for publication 15 April 2026
Published 13 May 2026 Volume 2026:18 589408
DOI https://doi.org/10.2147/IJWH.S589408
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Everett Magann
Stefaan Verhulst,1,2 Roshni Singh,1 Marta Dell’Aquila,3 Leonie Kunze,3 Cosima Lenz3
1The Governance Laboratory, New York, NY, USA; 2The Datatank, Tandon School of Engineering, New York, NY, USA; 3Global Governance, Regulation, Innovation and Digital Economy Unit, Centre for European Policy Studies, Brussels, Belgium
Correspondence: Stefaan Verhulst, The Governance Laboratory, CUSP, 370 Jay Street, Floor 13, Brooklyn, NY, 11201, USA, Email [email protected]
Purpose: Women’s health research remains under-resourced, underprioritized, and narrowly defined. Across the life course, women experience distinct health needs with significant implications for health and wellbeing, yet persistent gaps in evidence and data continue to reinforce inequities. In the absence of a universally accepted definition of women’s health, this study aimed to develop a topic map to capture its breadth and to identify an evidence-informed set of the top ten priority questions to guide future women’s health research and innovation.
Methods: We used a participatory, iterative methodology inspired by the 100 Questions Initiative, combining structured stakeholder engagement, rapid evidence synthesis, and iterative validation. An initial topic map was developed through an in-person workshop and refined through ongoing engagement with 77 global experts in women’s health and data science. Guided by the topic map, experts submitted research questions via a virtual survey, which were refined, clustered, prioritized, and ranked.
Results: The topic map served as a shared framework to guide the submission of actionable research questions and comprised four branches: (1) key domains of women’s health; (2) determinants and barriers; (3) technology and innovation; and (4) research and evidence gaps. A total of 113 questions were submitted, clustered into 56 themes, and narrowed to a top ten through expert prioritization, followed by public ranking via a virtual survey that yielded 115 responses. The highest-ranked questions focused on reframing and prioritizing women’s health, strengthening investment and innovation ecosystems, and addressing evidence gaps, research participation, data quality, and equity.
Conclusion: This study presents a comprehensive topic map that captures the complexity and cross-sectoral nature of women’s health and provides a unifying framework for the field. The prioritized questions offer a strategic foundation to guide future global research, policy, and investment to advance women’s health innovation.
Keywords: women’s health, question science, research framework, topic map
Introduction
Women comprise more than half of the world’s population and live longer than men, yet they spend a quarter more of their lives in poor health.1,2 Despite this, women’s health remains underfunded, underrepresented, and narrowly conceptualized, often confined to sexual and reproductive health.3–5 This narrow focus limits the global capacity to recognize and respond to the full spectrum of women’s health challenges across all stages of life.6
Women experience unique physiological and psychological transitions, including menstruation, pregnancy, childbirth, and menopause, each carrying distinct implications for health and wellbeing. Yet research into these experiences, and their links to disease, prevention, and treatment, remains insufficient.7 This includes menstruation, gynecological conditions such as endometriosis, and pregnancy-related health matters that remain underfunded and under-researched, contributing to inadequate understanding and insufficient and limited treatment options.3,8 Persistent gender bias in biomedical research and innovation continues to reinforce these gaps: women of reproductive age or pregnant women are often excluded from clinical trials, and medical knowledge still relies heavily on male physiology as the default.3,5,9,10 These inequities extend beyond research to the implementation of innovations, where gender norms, unequal digital access, and the gendered division of labor shape both participation and benefit.11,12
The growing pressures of global challenges such as climate change, antimicrobial resistance, and digital transformation further heighten the urgency for a renewed and more comprehensive understanding of women’s health.13,14 Women are often disproportionately exposed to these threats, making the integration of sex and gender perspectives across medicine, research, and public health essential. However, the absence of robust, sex-disaggregated data continues to impede evidence-informed policymaking and the design of interventions responsive to women’s lived realities.15
Advancing women’s health requires acknowledging that wellbeing is determined by intersecting social, economic, environmental, and biological factors that affect men and women differently.16,17 Improving women’s health is therefore not only a matter of equity; it is a cornerstone of stronger, more resilient health systems and a catalyst for sustainable development.5,18
There is still no universally accepted definition of women’s health or women’s health research. Definitions focus on conditions that occur only, mostly, or differently in women.4 A broader, more inclusive understanding is needed, one that reflects the diversity and complexity of women’s health across all stages of life.
To move toward this vision, a broader, more inclusive understanding of women’s health is needed, one that recognizes conditions that occur only, mostly, or differently in women while also accounting for how gender dynamics shape access to care, research priorities, and innovation. As part of the 100 Questions Initiative, this study presents the development of a topic map that characterizes the breadth and structure of women’s health as a global research and innovation domain, along with an evidence informed set of the top ten priority questions to guide a future agenda for advancing women’s health innovation.19
This study offers added value through the application of an innovative, crowdsourced methodology that leverages the expertise of individuals across the women’s health research field to collaboratively contribute on a more equal footing. This approach contrasts with traditional models that rely on consensus panels or top-down priority-setting processes. By incorporating a crowdsourced strategy, the study introduces a novel lens for data collection and prioritization, enabling more diverse input and broader engagement of relevant stakeholders.
Methods
The development of the women’s health research agenda followed a participatory, iterative methodology inspired by the 100 Questions Initiative (100Qs) developed by the Governance Laboratory (The GovLab). The 100Qs methodology is a participatory approach that engages experts of a certain domain along with the public to identify and prioritizes the top actionable questions that can spur progress towards addressing complex societal challenges. The methodology is designed to identify priority research questions through structured stakeholder engagement, rapid evidence synthesis, and iterative validation, ensuring that the resulting agenda is evidence-informed and responsive to the needs of practitioners, policymakers, and researchers. This approach has been successfully applied across diverse global health domains to generate actionable, consensus-driven priorities including adolescent mental health.20 For women’s health, the 100Qs methodology was implemented in partnership with the Centre for European Policy Studies.
Our process comprised three sequential components: (1) development of a visual topic map of women’s health; (2) expert consultation and question development; and (3) final prioritization and ranking of questions. Ethical approval was not required as the study utilized anonymous, voluntarily submitted crowdsourced data with no personal identifiers.
Development of the Women’s Health Topic Map
The initial topic map was created through an in-person workshop held in March 2025, convening 18 global experts in women’s health. Discussions were structured around the central question: “What falls under the spectrum of women’s health?” Participants identified and organized key elements into three overarching categories:
- Domains: Core thematic areas encompassed within women’s health.
- Challenges: Existing and emerging issues that hinder or could adversely affect women’s health.
- Innovations: Fields with potential to generate new discoveries, technologies, or transformative advances shaping the future of women’s health.
Using Miro, the project team visually mapped participant insights using these categories, capturing relationships between subtopics and identifying areas requiring further exploration. The topic map served as the first iteration of a comprehensive framework representing the scope and complexity of women’s health.
The map organizes topics in four categories: (1) key domains, (2) technology and innovation, (3) determinants and barriers, and (4) research and evidence gaps. These clusters were derived through thematic assessment of workshop discussions designed to capture the multidimensional nature of women’s health. Each main branch unfolds into a series of cascading sub-branches, reflecting the relative priorities identified across areas.
Iterative Expert Consultation
The initial iteration of the topic map was presented in June 2025 to a broader group of 77 global experts in women’s health and data science during a virtual consultation. These experts represented 30 countries, with approximately half from high-income settings and half from low- and middle-income settings and included 66 women and 11 men. Experts represented diverse areas of expertise, including researchers, clinicians, practitioners, and advocates specializing in women’s health domains such as infectious disease, cardiology, mental health, femtech, fertility, and aging, among others. Participants were invited to review the map, identify omissions, recommend refinements, and comment on the relationships among domains, challenges, and areas of innovation. Their feedback informed the development of a revised second iteration of the map.
This iterative process aligned with the participatory principles of the 100Qs methodology, ensuring that the emerging agenda was crowd sourced, grounded in the perspectives of domain experts, and informed by current evidence and practice. The criteria guiding prioritization within the 100 Questions approach included:
- Desirability: Would investment in the topic transform understanding or generate high-impact interventions?
- Novelty: Is the topic poised to produce new insights or extend existing knowledge?
- Feasibility: Could meaningful progress be achieved in the near term if resources are allocated?
- Scalability: Can findings or interventions be applied across diverse contexts or populations?
Results
Women’s Health Innovation Topic Map
The central themes in women’s health innovation were distilled into a visual topic map structured around four primary branches (Figure 1). Finalized in June 2025, this map served as the foundation shared with experts to guide the submission of actionable questions aimed at advancing women’s health innovation globally. The four main branches (key domains, determinants and barriers, technology and innovation, and research and evidence gaps) each encompass multiple subtopics, which are described in greater detail below.
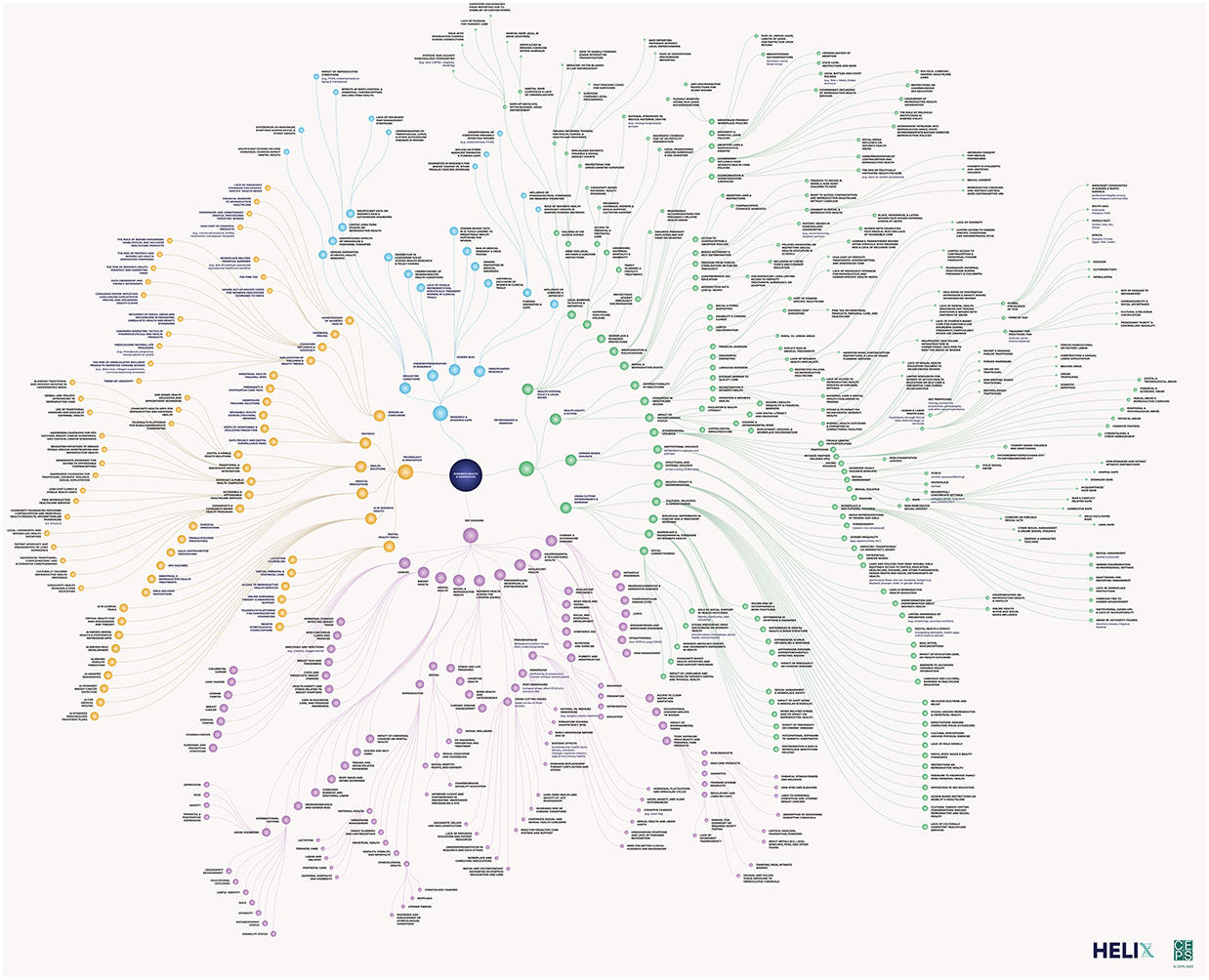 |
Figure 1 Women’s Health Topic Map. Color Key: Purple: key domains branch; green: determinants and barriers branch; yellow: technology and innovation branch; blue: research and evidence gaps branch. |
Key Domains
Key domains identified include sexual and reproductive health, mental health, women’s health across the lifespan and again, cancer, chronic and autoimmune diseases, breast health, and environmental and occupational health. Together, these domains capture the biological, social, and structural factors influencing women’s health across the lifespan from adolescents under geriatrics.
Determinants and Barriers
This section maps the social, cultural, and systemic barriers that impact women’s health and women’s health innovation. It considers factors including gender norms, cultural expectations, and inequities that shape women’s ability to make informed health decisions and receive adequate care. The main branches include health equity and access, health systems policies and legal issues, gender-based violence, patriarchal gender norms, social connectedness, workplace and environmental stressors, biological differences in disease risk and treatment response, cultural gender and religious norms, and biases myths and misconceptions.
Technology and Innovation
The branch highlights the innovations and technologies transforming and posing barriers for women’s healthcare. It discusses advancements in digital health, AI, and FemTech, as well as challenges related to commercialisation, gendered pricing, and access to essential health services. The main sub-branches in this section include AI in women’s health, medical innovations, digital health tools, women as consumers, and health solutions.
Research and Evidence Gaps
This section maps women’s health research and depicts underrepresentation of women in clinical trials, the lack of gender-specific research, and the need for more targeted funding to address overlooked health conditions. The main subbranches in this section include underrepresentation in research, neglected conditions, gender bias, and underfunded research.
Question Development and Prioritization
Using the topic map as a guiding framework, the 77 global experts were invited to submit at least one research question through an online survey, focusing on areas where further research and innovation are needed. For each question, experts were also asked to provide a brief rationale and to share any relevant published or grey literature supporting the proposed inquiry.
A total of 113 questions were submitted. Of these, of the 113 questions submitted, 30% (34 questions) were descriptive (what is), 38% (43 questions) were prescriptive (how), 16% (18 questions) were predictive (what will), and 16% (18 questions) were predictive (what will). Following submission, the project team reviewed all submitted questions to assess quality, identify overlaps, and consolidate similar entries to ensure that the resulting set was coherent, non-duplicative, and actionable. Questions with overlapping subject matter and focus were aggregated and combined as possible.
This process resulted in 56 refined and clustered questions organized across 15 thematic clusters. These clustered questions were then circulated to the expert group for review and prioritization. Table 1 presents the subtopics and the proportion of submitted questions associated with each thematic area.
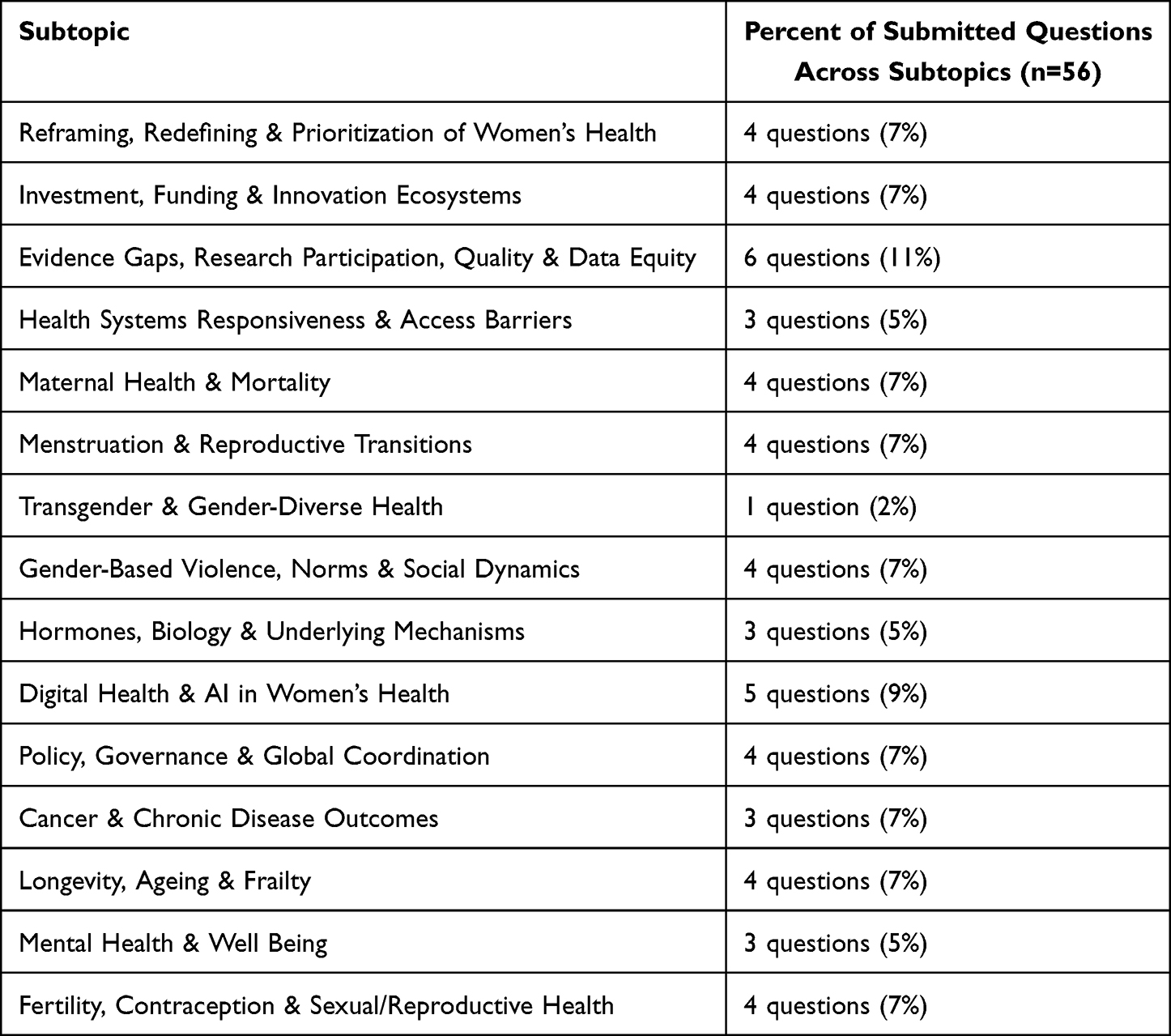 |
Table 1 Thematic Subtopics |
Common themes that cut across these subdomains included equity and inclusion, evidence and data gaps, regulatory frameworks and equitable governance, emerging health technologies, stage specific and life course needs, including transitions, health system barriers, social cultural norms and gender power dynamics, economic and investment models, sustainable financing, and psychosocial aspects of women’s health.
Expert Review and Prioritization
Following their review of the 56 clustered questions, experts provided detailed feedback on clarity, scope, and relevance. The questions were then iteratively refined to incorporate this input. Experts were subsequently invited to identify their top ten priorities from the updated set using an online form following the aforementioned prioritization criteria including desirability, novelty, feasibility, and scalability. Their responses were aggregated to generate the prioritized list of expert selected priority questions.
Public Voting
To broaden participation and extend the crowd sourced methodology, the project team launched a public voting phase based on the expert derived top ten questions. An electronic survey was disseminated through social media, women’s health events including the Innovation Equity Forum, and targeted outreach to women’s health organizations and networks via email, Facebook, WhatsApp, and LinkedIn. Public voting yielded 115 responses from individuals across more than thirty countries, including thirteen European countries, eight African countries, one Asian country, four Middle Eastern countries, two North American countries, and one country each from Oceania and South America. The resulting output produced the final ranked list of the top ten priority questions, presented in Table 2, with the highest ranked questions originating from the subtopics reframing, redefining and prioritizing women’s health, investment and innovation ecosystems, and evidence gaps, research participation, quality and data equity.
 |
Table 2 Top Ten Questions |
Discussion
This study demonstrates the value of a participatory approach that remains underused in the field of women’s health research and innovation. By leveraging a collaborative process informed by expert input and international engagement, we generated a demand-driven set of priorities for future research with substantial potential to guide both action and strategic investment. The final list of priority questions was derived through a two-step process. First, a topic map was developed to synthesize expert insights regarding key domains, challenges, and areas of innovation in women’s health. Second, international experts contributed via online discussions, Email exchanges, and virtual surveys to refine, validate, and prioritize these questions.
Our methodology contributes to advancing women’s health innovation in multiple ways. Beyond producing a structured and ranked set of research questions that can inform the decisions of policymakers, funders, and other stakeholders, the topic map offers an updated conceptualization of the women’s health landscape. It provides a holistic perspective that extends beyond the traditional focus on reproductive and sex-specific conditions, emphasizing the complex interactions between biological, social, and systemic factors. As such, the topic map serves as a practical tool for advocates, policymakers, donors, and researchers seeking to reassess prevailing assumptions and identify strategic areas for action. When used alongside complementary resources, such as the Women’s Health Opportunity Map, it can illuminate persistent gaps and emerging opportunities, supporting better alignment of research, policy, and investment. Involvement of global experts not only strengthened the accuracy and legitimacy of our findings but also facilitated the identification of shared priorities that can underpin future cross-sectoral collaborations. However, these findings should be interpreted as strategic guidance rather than definitive or exhaustive priorities, given that they are derived from a defined group of participants and reflect a time-bound, participatory consensus process.
Several limitations warrant consideration. Although this work aimed for broad international representation, the number of participating experts was relatively small and disproportionately drawn from Europe and North America. This composition may have influenced both the feedback shaping the topic map and the outcomes of the prioritization process. Future iterations should seek to ensure voices that were underrepresented in this initial phase are meaningfully engaged, particularly from the Global South, Latin and South America, and individuals with diverse lived experiences across the life course. Repeated application of this methodology will also be necessary to ensure that research priorities remain current in a rapidly evolving women’s health landscape.
Conclusion
Through an iterative and expert informed process, this study produced a topic map that offers a comprehensive conceptual framework for understanding the breadth and complexity of women’s health providing strategic priorities for this given moment. This framework served as the basis for identifying and ranking the top ten priority questions that can guide future research, policy development, and strategic investment. Together, the topic map and prioritized questions provide a structured foundation for advancing a more impactful women’s health research and innovation agenda. Operationalization of this research agenda will require sustained, cross-sectoral, and multilevel collaboration, alongside long-term investment, and institutional and political commitment.
Abbreviations
100Qs, the 100 Questions Initiative; The GovLab, the Governance Laboratory; HI, Hormone therapy; AI, Artificial Intelligence.
Acknowledgments
We extend our sincere thanks to the cohort of bilingual experts for their valuable contributions, insights, and recommendations, which were instrumental in shaping the outcomes of this research agenda. A full list of participating bilingual experts is provided here: https://womenshealth.the100questions.org/
Funding
This publication was supported by research funding from Gates Foundation. The findings and conclusions contained within are those of the authors and do not necessarily reflect positions or policies of the Gates Foundation.
Disclosure
Dr Stefaan Verhulst reports a joined project with the Centre for European Policy Studies. The authors have no other conflicts of interest in this work.
References
1. Irani SZ, Bishen S. The gender health gap: it’s about more than solving a women’s issue. World Economic Forum; 2024. Available from: https://www.weforum.org/stories/2024/02/women-health-gender-gap-equality/.
2. Willige A. The state of women’s health in numbers. World Economic Forum; 2026. Available from: https://www.weforum.org/stories/2026/03/womens-health-in-numbers/.
3. Innovation Equity Forum. Women’s health innovation opportunity map 2023 50 high-return opportunities to advance global women’s health R&D. Gates Foundation; 2023. Available from: https://cambercollective.com/wp-content/uploads/2025/01/Womens-Health-RD-Opportunity-Map-2023.pdf.
4. White J, Clayton J. The gender health innovation gap: a perspective from the NIH office of research on women’s health. Med. 2022;3(5):298–12. doi:10.1016/j.medj.2022.04.010
5. Ellingrud K, Pérez L, Petersen A, Sartori V. Closing the Women’s Health Gap. McKinsey; 2024. Available from: https://www.mckinsey.com/mhi/our-insights/closing-the-womens-health-gap-a-1-trillion-dollar-opportunity-to-improve-lives-and-economies.
6. Lancet T. A broader vision for women’s health. Lancet. 2023;402(10399):347. doi:10.1016/S0140-6736(23)01570-2
7. Camber Collective. Women’s health innovation opportunity map 2024 progress report. 2024. Available from: https://cambercollective.com/wp-content/uploads/2025/02/Womens-Health-Opportunity-Map-2024-Progress-Report.pdf.
8. Kirk UB, Bank-Mikkelsen AS, Rytter D, et al. Understanding endometriosis underfunding and its detrimental impact on awareness and research. Npj Womens Health. 2024;2(1):45. doi:10.1038/s44294-024-00048-6
9. Lego VD. Uncovering the gender health data gap. Cad Saúde Pública. 2023;39(7):e00065423. doi:10.1590/0102-311XEN065423
10. McFerran EF O, Quinney SK. Bridging the gap: inclusion of pregnant women in clinical drug trials. Clin Chem. 2025;72(1):7–10. doi:10.1093/clinchem/hvaf149
11. Musizvingoza R, Handforth C. The digital gender gap in healthcare progress, challenges and policy implications. 2021. Available from: https://genderhealthdata.org/wp-content/uploads/2024/01/The-Digital-Gender-Gap-in-HealthCare.pdf.
12. Nikghadam-Hojjati S, Marchetti E, Gustavsson M, et al. Gender-responsive research and innovation: issues and initiatives. Sustainability. 2025;17:6215. doi:10.3390/su17136215
13. Desai Z, Zhang Y. Climate change and women’s health: a scoping review. GeoHealth. 2021;5(9):e2021GH000386. doi:10.1029/2021GH000386
14. Batheja D, Goel S, Charani E. Understanding gender inequities in antimicrobial resistance: role of biology, behaviour and gender norms. BMJ Glob Health. 2025;10(1):e016711. doi:10.1136/bmjgh-2024-016711
15. Shirzad M, Kaufman MR. Missing piece: the imperative of gender-disaggregated data in unraveling health inequity. BMJ Glob Health. 2025;10(7):e018266. doi:10.1136/bmjgh-2024-018266
16. Patwardhan V, Gil GF, Arrieta A, et al. Differences across the lifespan between females and males in the top 20 causes of disease burden globally: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Public Health. 2024;9(5):e282–e294. doi:10.1016/S2468-2667(24)00053-7
17. Zakar R, Iqbal S. Editorial: social determinants of women’s health in low and middle income countries. Front Glob Womens Health. 2024;5. doi:10.3389/fgwh.2024.1482047
18. Onarheim KH, Iversen JH, Bloom DE. Economic benefits of investing in women’s health: a systematic review. PLoS One. 2016;11(3):e0150120. doi:10.1371/journal.pone.0150120
19. The GovLab. The 100 Questions Initiative - Women’s Health Innovation. 2025. Available from: https://womenshealth.the100questions.org.
20. Verhulst S, Vidal Bustamante CM, Carvajal-Velez L, et al. Toward a demand-driven, collaborative data agenda for adolescent mental health. J Adolesc Health. 2023;72(1, Supplement):S20–S26. doi:10.1016/j.jadohealth.2022.05.027
 © 2026 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2026 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.