Back to Journals » Patient Preference and Adherence » Volume 20
Factors Influencing Attendance to Physical Therapy Services Among Children with Cerebral Palsy in Saudi Arabia
Authors Alghamdi MS ![]() , Awali A
, Awali A ![]() , Alshehri MA
, Alshehri MA ![]() , Alonazi M, Alenazi AM
, Alonazi M, Alenazi AM
Received 22 January 2026
Accepted for publication 2 May 2026
Published 13 May 2026 Volume 2026:20 596418
DOI https://doi.org/10.2147/PPA.S596418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Mohammed S Alghamdi,1 Abdulaziz Awali,1 Mansour Abdullah Alshehri,1 Mushari Alonazi,2 Aqeel M Alenazi3
1Department of Medical Rehabilitation Sciences, Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, Saudi Arabia; 2Emergency Department, Pediatric Emergency, King Faisal Specialist Hospital & Research Center, Riyadh, Saudi Arabia; 3Department of Health and Rehabilitation Sciences, College of Applied Medical Sciences, Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia
Correspondence: Mohammed S Alghamdi, Department of Medical Rehabilitation Sciences, Faculty of Applied Medical Sciences, Umm Al-Qura University, Makkah, Saudi Arabia, Email [email protected]
Objective: To examine child, caregiver, and physical therapy (PT) service-related factors associated with regular versus irregular attendance to PT services among children with cerebral palsy (CP).
Methods: A cross-sectional study was conducted with 108 caregivers of children with CP aged 2– 12 years in Saudi Arabia. Caregivers completed an online survey about child and caregiver characteristics, PT characteristics, perceived difficulties related to PT services, and caregiver-reported burden. Attendance was categorized as regular or irregular based on caregiver report and differences were examined. Regular attendance reflected consistent participation in scheduled sessions, whereas irregular attendance reflected missed, delayed, or inconsistent attendance.
Results: Regular attendance was reported by 42.6% of participants. Regular attendance was associated with younger age of children (p = 0.003, d= 0.59) and lack of children’s educational enrollment (p = 0.014, &phis; = 0.24). No significant differences were found between groups for child sex, Gross Motor Function Classification System level, CP type, caregiver characteristics, or PT service characteristics. Irregular attendees reported greater difficulties related to appointment booking policies (r = 0.30), access to therapists (r = 0.26), agreement on treatment plans (r = 0.22), child behavior management (r = 0.25), and caregiver–child interaction during home exercises (r = 0.29), as well as higher financial (r = 0.21) and psychological burden (r = 0.19).
Conclusion: Attendance to PT services for children with CP was associated more with caregiver-perceived difficulties and burden than with demographic or service characteristics. Addressing service processes and caregiver experiences may support more consistent PT attendance.
Keywords: cerebral palsy, physical therapy attendance, caregiver burden, Saudi Arabia
Introduction
Children with cerebral palsy (CP) may require complex and multidisciplinary care because the condition is often associated with a range of functional difficulties affecting movement, daily activities, and participation.1 Physical therapy (PT) is a key component of rehabilitation services provided to children with CP, and PT interventions have been documented to promote outcomes such as mobility and daily life functioning.2–4 Pediatric rehabilitation is commonly guided by a family-centered care approach, which recognizes both the child and the family throughout the continuum of care and emphasizes support for families in their caregiving roles.5 Within this approach, collaboration between families and healthcare professionals in goal setting, decision making, and information sharing is viewed as fundamental to improving child and family outcomes.6 Thus, families of children with CP carry substantial responsibility for facilitating attendance to scheduled PT services (attendance) and following prescribed recommendations across clinic and home (adherence), which may impose considerable emotional, physical, and financial burden.7,8 Accordingly, attendance to PT services reflects not only the child’s clinical needs but also the extent to which service delivery aligns with family priorities, capacities, and experiences within the healthcare system.
Previous studies for children with disabilities have examined attendance to clinic-based services separately from participation in home-based therapy, demonstrating that clinic attendance is shaped primarily by service accessibility, scheduling processes, and caregiver-related constraints rather than by factors influencing home exercise participation.9,10 Research focusing specifically on clinic attendance has consistently identified service-related and caregiver-related barriers such as appointment scheduling difficulties, long waiting times, limited access to therapists, distance to clinics, and transportation or treatment costs.10–12 A large hospital-based study further showed that non-attendance at outpatient services was more strongly associated with service processes, prior missed appointments, and increasing child age than with clinical severity or CP subtype.13 Physical therapists similarly report frequent deviations from planned treatment schedules, often attributed to access limitations and system-level inefficiencies, highlighting the systemic nature of attendance challenges.14,15 In contrast, demographic variables such as caregiver education, income, or child functional severity have shown limited or inconsistent associations with attendance outcomes.9,13,16
Collectively, existing studies indicate that attendance to rehabilitation services for children with CP is influenced by service processes, access constraints, and caregiver burden. Evidence from a large hospital-based study identified predictors of non-attendance such as increasing child age and prior missed visits, yet these data do not capture caregiver-reported barriers that may explain attendance patterns.13 Qualitative studies and systematic reviews also described obstacles for non-attendance such as scheduling difficulties, limited therapist access, and caregiver strain.10,12 In addition, several studies focused on home program participation or therapist perspectives rather than caregiver-reported experiences of clinic attendance.9,11,14,17 Within Saudi Arabia, available evidence addresses elements of service delivery such as goal agreement and appointment planning, but it remains unclear how child factors, caregiver characteristics, and caregiver-perceived service barriers together relate to regular versus irregular attendance to PT services.9,14,18 Thus, specific investigation is needed because children with CP commonly depend on ongoing hospital-based rehabilitation, and attendance may be influenced by these factors.
Understanding attendance in this context aligns with healthcare utilization frameworks such as Andersen’s Behavioral Model, which proposes that service use is influenced by predisposing, enabling, and need-related factors.19 In this study, attendance at PT services was considered a form of healthcare utilization. Child and caregiver sociodemographic characteristics were conceptualized as predisposing factors, PT service access and caregiver-perceived barriers as enabling factors, and clinical characteristics such as motor severity and CP type as need-related factors. Within a hospital-based healthcare system, understanding attendance patterns is important for supporting continuity of care and optimizing service delivery for children with CP. Therefore, this study examined child, caregiver, and PT service-related variables associated with attendance to PT services among children with CP.
Methods
Design and Participants
A cross-sectional design was used for this study. Participants were a convenience sample of 108 caregivers of children with CP. The inclusion criteria were 1) caregiver aged 18 years or older; 2) able to read and write in Arabic; and 3) have a child with CP between 2 to 12 years of age. The exclusion criteria were 1) caregivers who are unable to communicate in Arabic; 2) caregivers of children with diagnoses other than CP. Participants were recruited from different regions in Saudi Arabia via social media platforms (X platform, WhatsApp, and Telegram) and were required to provide informed consent electronically prior to completing the survey. Prior to data collection, ethical approval was obtained from The Biomedical Research Ethics Committee at Umm Al-Qura University (Approval No. HAPO-02-K-012-2021-02-565). This study was conducted in accordance with the Declaration of Helsinki.
Survey Instrument
A survey designed for this study was used and consisted of four sections and completed by caregivers. The first section collected demographic and clinical information related to the child and caregiver. Child characteristics included age (in years or months if less than 1 year), sex, educational enrollment status (not enrolled, preschool, primary, or intermediate school), topographical distribution of motor involvement (quadriplegia, triplegia, diplegia, hemiplegia, and monoplegia), and functional mobility level using the Gross Motor Function Classification System (GMFCS).20 The GMFCS is a five-level system that describes gross motor function based on self-initiated movement: Level I (walks without limitations), Level II (walks with limitations), Level III (walks using a hand-held mobility device), Level IV (self-mobility with limitations, may use powered mobility), and Level V (transported in a manual wheelchair). Caregiver characteristics included caregiver role (mother, father, grandparent, or housemaid), age (reported in years), educational level (no formal education, less than secondary education, secondary education, bachelor’s degree, or postgraduate education), employment status (not employed, part-time employment [<30 hours/week], or full-time employment [≥30 hours/week]), and monthly household income (<6000 SAR, 6000–11,000 SAR, or ≥12,000 SAR). Family size was reported as the total number of individuals living in the household.
The second section included questions related to therapy characteristics. This included the type of rehabilitation services received (physical therapy, occupational therapy, and/or speech and language therapy), and the type of service provider (governmental, private, or home-based). Service intensity was described by the number of PT sessions per week, the duration of each session (<30 minutes, 30 minutes to 1 hour, or >1 hour), and the status of attending to PT services (regular attendance described as consistent participation in scheduled sessions, or irregular attendance described as missed, delayed, or inconsistent attendance).
The third section included 16 items to assess caregiver-perceived challenges encountered during the provision of PT services across three domains: PT center–related factors, session-related factors, and home exercise–related factors. The PT center–related items addressed the center’s policy of booking session appointments, availability of child-specific treatment rooms, waiting spaces, transportation to and from the center, and the cost of PT sessions. Session-related items included ease of access to the therapist for consultations, therapist’s ability to explain the child’s condition to the family, agreement between the therapist and the family on the treatment plan, therapist’s handling of the child and caregiver, therapist’s initiative in using various exercises and methods during the session, handling of the child’s behavior or crises during sessions, and communication with other departments to discuss the child’s condition. Home exercise–related items included the number and variety of therapeutic exercises prescribed, therapist’s ability to explain home exercises, availability of devices or equipment to support the child at home, and child interaction with the caregiver when performing home exercises. Items in this section were rated using a 4-point difficulty scale (1 = no difficulty at all; 2 = somewhat difficult; 3 = moderate difficulty; 4 = very difficult). The fourth section pertained to caregiver-reported burden related to PT services. These items addressed whether PT increased the family’s financial burden, whether commitment to PT sessions or home exercises contributed to increased physical burden, whether commitment to PT sessions reduced interaction with family and the community, and whether commitment to PT sessions adversely affected the caregiver’s mental health, including financial, physical, social, and psychological impact, using a 5-point agreement scale (1 = strongly disagree; 2 = disagree; 3 = not sure; 4 = agree; 5 = strongly agree). The survey was pilot tested with five caregivers of children with CP to assess clarity, readability, and appropriateness of items. The caregiver-perceived difficulty scale (16 items) demonstrated good internal consistency (Cronbach’s α = 0.88), while the caregiver-reported burden subscale (4 items) also showed good internal consistency (Cronbach’s α = 0.87).
Data Analysis
The primary outcome of this study was attendance to PT services, categorized as regular or irregular based on caregiver-reported attendance at scheduled PT sessions. Regular attendance reflected consistent participation in scheduled sessions, whereas irregular attendance reflected missed, delayed, or inconsistent attendance. Participants were classified into regular and irregular attendance groups for comparison across child, caregiver, and service-related variables.
Descriptive statistics were used to summarize participant characteristics and survey data. Comparisons between regular and irregular attendance groups were conducted using Chi-Square tests for categorical variables and independent-samples t-tests or Mann–Whitney U-tests for continuous variables, as appropriate after assessment of normality. Differences in caregiver-perceived difficulties related to PT services were examined using Mann–Whitney U-tests due to the ordinal nature of the response scales. Data were analyzed using the Statistical Package for the Social Sciences (SPSS), version (Mac Version 28). Statistical significance was set at p < 0.05.
Effect sizes were reported as phi coefficient (φ) for 2×2 chi-square tests, Cramér’s V for chi-square tests with variables containing more than two categories, Cohen’s d with 95% confidence intervals for independent-samples t-tests, and r for Mann–Whitney U-tests (r = |Z|/√N). Effect sizes were interpreted using conventional cut-off values.21 For phi coefficient (φ), Cramér’s V, and r derived from the Mann–Whitney U-test, values of 0.10, 0.30, and 0.50 were considered to indicate small, medium, and large effects, respectively. For Cohen’s d, values of 0.20, 0.50, and 0.80 were considered to indicate small, medium, and large effects, respectively. Because no a priori sample size calculation was conducted, post hoc power analyses were performed using G*Power (version 3.1.9.7) for to determine achieved statistical power.
Results
A total of 108 caregivers of children with CP were included in the analysis and were classified into regular attendance (42.6%) and irregular attendance (57.4%) groups based on attendance to PT services. Caregivers aged between 23 to 60 years, and 94.4% were mothers. Of the total sample, 82.4% of caregivers were not employed, 51.9% had an educational level of greater than high school. Children were 2 to 12 years of age and were classified using the GMFCS as follows: level I (3.8%), level II (22.9%), level III (31.4%), level IV (6.7%), and level V (35.2%). For statistical analyses, GMFCS levels were grouped into two categories: levels I–III (58.1%) and levels IV–V (41.9%) for ease of reporting.
Child and Caregiver Characteristics
Table 1 summarizes the demographic and clinical characteristics of regular and irregular attendees. The mean age of children who regularly attended PT sessions was significantly younger compared to irregular attendees, with a statistically significant difference t(106) = 3.02, p = 0.003, d = 0.59. Regular PT attendance was significantly associated with children’s educational enrollment χ2(1) = 5.99, p = 0.014, φ = 0.24, with a higher proportion of irregular attendees were enrolled in pre-school or school, whereas a higher proportion of regular attendees were not enrolled in school. No significant differences were found between groups in terms of child’s sex, GMFCS levels, or CP type. Caregiver demographics, including caregiver age, caregiver’s relation to the child, employment status, education level, household size, and household income, did not show statistically significant differences between regular and irregular attendees.
 |
Table 1 Demographic Data for Child and Caregiver |
PT Service Characteristics
Table 2 shows the differences between regular and irregular PT attendees concerning facility characteristics and session frequency. No significant differences were identified between regular and irregular attendees regarding the type of facility attended, with governmental versus non-governmental facilities showing comparable distributions. Similarly, the number of weekly PT sessions did not differ significantly. Further, there were no significant differences observed in the availability of occupational therapy and speech therapy services between the two attendance groups. The duration of PT sessions was also comparable between groups, with most sessions lasting between 30 minutes to one hour for both regular and irregular attendees.
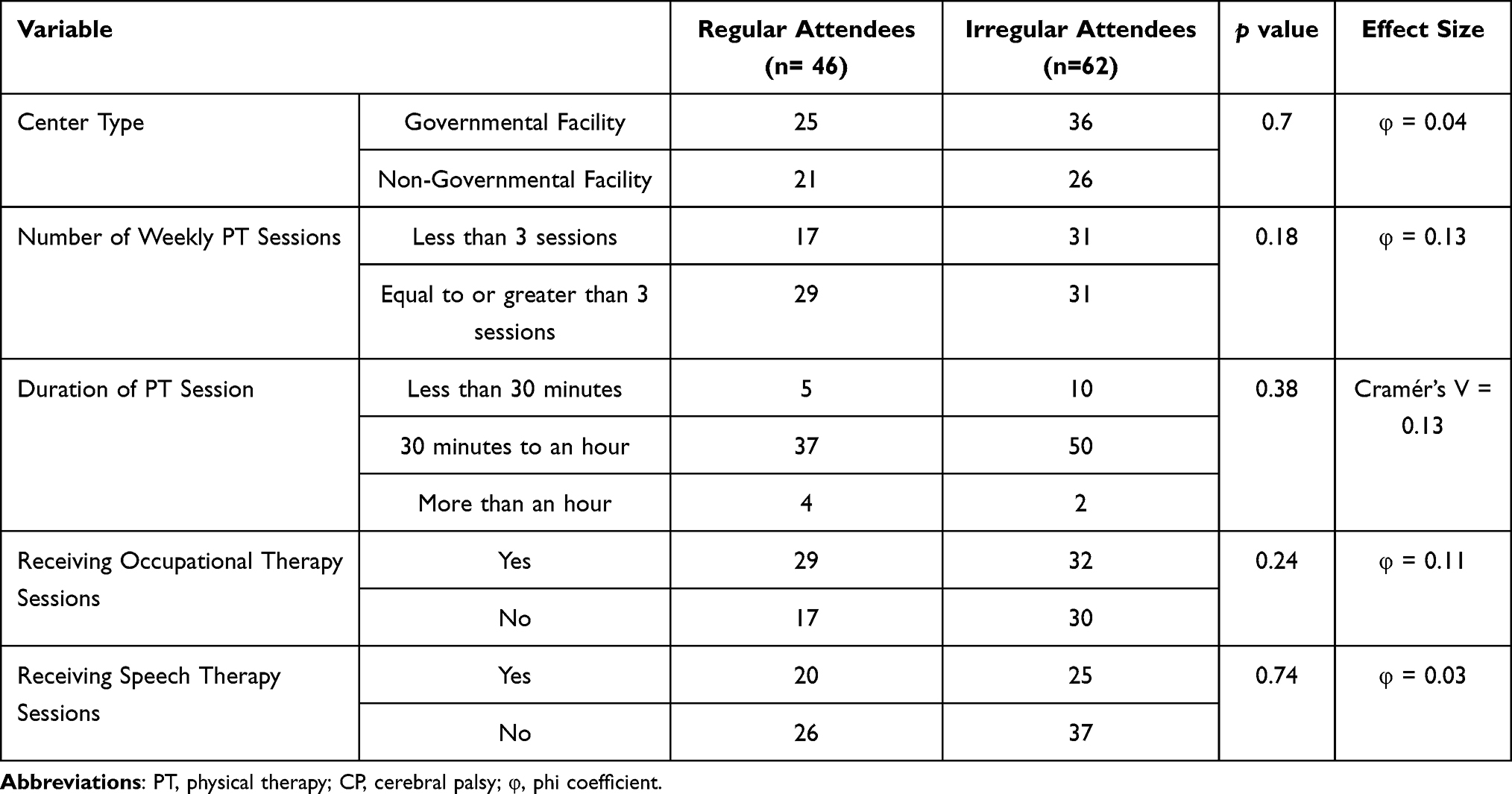 |
Table 2 Characteristics of PT Services for Children with CP |
Caregiver-Perceived Difficulties
Differences in caregiver-perceived difficulties were compared between the two groups: regular vs. irregular attendees. Significant differences were identified for five survey items (1, 6, 8, 11 and 16; Figure 1). Irregular attendees experienced significantly greater difficulty with the PT center’s booking policy for session appointments (U = 858, Z = −3.07, p = 0.002, r = 0.30) and ease of access to physical therapists for medical consultations (U = 987, Z = −2.74, p = 0.006, r = 0.26). Additionally, irregular attendees reported significantly more challenges in achieving agreement between physical therapists and families regarding treatment plans (U = 1048.5, Z = −2.33, p = 0.02, r = 0.22), managing children’s behavioral crises (U = 1060, Z = −2.65, p = 0.008, r = 0.25), and facilitating child-caregiver interaction during home exercises (U = 938, Z = −3.0, p = 0.003, r = 0.29). Figure 1 illustrates caregiver-perceived challenges encountered during the provision of PT services among regular and irregular attendees.
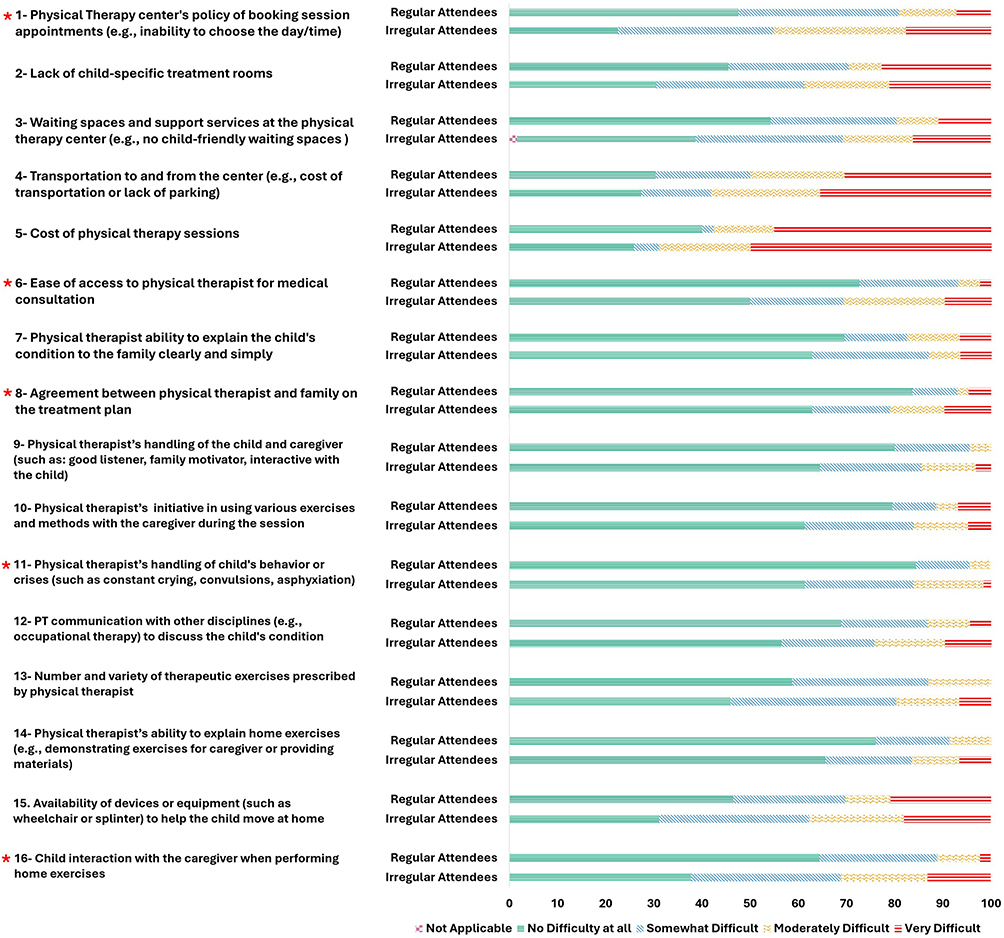 |
Figure 1 Caregiver-perceived challenges encountered during the provision of PT services among regular and irregular attendees. Asterisks (*) denote significant between-group differences: item 1 (r = 0.30), item 6 (r = 0.26), item 8 (r = 0.22), item 11 (r = 0.25), and item 16 (r = 0.29). |
Furthermore, caregivers in the irregular attendees group reported a significantly greater financial burden due to PT sessions (U = 1098.5, Z = −2.173, p = 0.030, r = 0.21) and adverse effects on mental health related to attending PT services (U = 1116.5, Z = −1.992, p = 0.046, r = 0.19). No statistically significant differences were observed between groups for perceived physical burden or reduced interaction with family and community (p > 0.05). Figure 2 shows caregiver-reported burden associated with attending PT services among regular and irregular attendees.
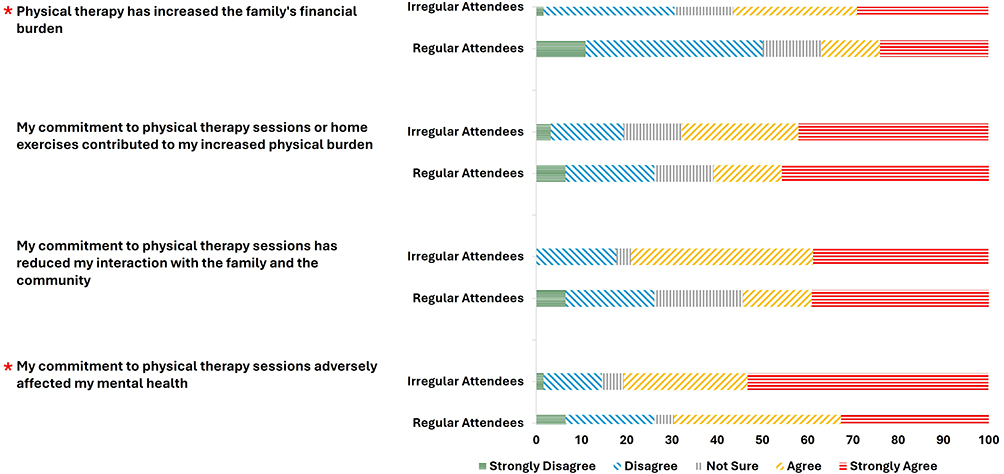 |
Figure 2 Caregiver-reported burden associated with attending PT services among regular and irregular attendees. Asterisks (*) denote significant between-group differences for financial burden (r = 0.21) and adverse effects on mental health (r = 0.19). |
Post hoc power analyses for selected key between-group comparisons indicated adequate power for analyses with moderate observed effects, with achieved power ranging from 0.84 to 0.88. In contrast, analyses with smaller observed effects were likely underpowered (ranging from 0.49 to 0.76), and these findings should therefore be interpreted with caution.
Discussion
The aim of this study was to examine child, caregiver, and PT–related factors associated with attendance to PT services among children with CP in Saudi Arabia by comparing caregivers with regular and irregular attendance. Overall, attendance was not associated with child clinical characteristics, caregiver demographic factors, or service structure such as facility type, session frequency, or session duration. Instead, regular attendance was more strongly related to child age, educational enrollment, and caregiver-perceived difficulties in accessing and sustaining PT services. In particular, challenges related to appointment booking, access to physical therapists for consultation, agreement on treatment plans, management of child behavioral crises, and financial and psychological burden distinguished families with irregular attendance, with the magnitude of these differences generally ranging from small to moderate effects. Together, these findings suggest that attendance to PT services is influenced less by what services are offered and more by how caregivers experience the process of obtaining and continuing care.
The observed association between younger child age and regular PT attendance aligns with evidence from large cohort studies showing that non-attendance at outpatient services increases as children with CP grow older.13 Although caregiver perceptions regarding developmental timing were not directly assessed in the present study, younger age may coincide with periods of more intensive service use or prioritization of therapy, which could support more consistent attendance.13 The association between educational enrollment and regular PT attendance may reflect greater routine and structure in daily schedules, which could help families maintain PT appointments more consistently. However, this should be interpreted with caution as the association was modest and did not assess family routines, dynamics, or other contextual factors that may underline this relationship. In contrast, the lack of association between attendance and GMFCS level or CP type in the present study differs from findings reported by Ligaya et al,16 who observed higher representation of children with more severe motor impairment in the non-adherent group and attributed this to increased transport burden and slower perceived progress This discrepancy may reflect differences in outcome definitions, as Ligaya et al16 examined adherence (participation in at least half of prescribed therapy sessions or completion of therapy sets across services) rather than clinic attendance alone. The present findings are, however, consistent with outpatient attendance studies indicating that clinical severity does not reliably predict missed appointments.13 Together, these results suggest that the influence of motor severity on rehabilitation participation may vary depending on whether attendance to scheduled services or broader treatment adherence is examined, highlighting the importance of clearly distinguishing between these constructs.
No significant differences were observed between regular and irregular attendance groups with respect to PT service characteristics, including facility type, session frequency, session duration, or availability of occupational and speech therapy services. This finding suggests that service structure and delivery alone may not be sufficient to explain variability in attendance. Studies examining service organization have shown that the presence or planned structure of services does not necessarily translate into consistent attendance, as deviations from scheduled care frequently occur due to access constraints rather than the number of sessions offered.14 Similarly, service redesign studies emphasize that improvements in access pathways and processes, rather than changes in service volume or duration, are more closely linked to reducing missed appointments.15 In the present study, the lack of differences between governmental and non-governmental facilities further indicates that attendance challenges may not be confined to a specific service sector. However, unlike some prior work that focused on access metrics such as waiting time or appointment availability, this study did not directly assess system-level processes, which limits direct comparison. Taken together, these findings suggest that attendance to PT services may be influenced less by the structural characteristics of services and more by factors related to access processes and caregiver experience, although further research is needed to clarify the relative contribution of these elements.
Caregiver-perceived difficulties were among the factors that distinguished families with regular and irregular attendance to PT services. Irregular attendance was associated with significantly greater difficulty related to appointment booking policies, limited access to physical therapists for consultation, lack of agreement on treatment plans, challenges in managing child behavioral crises during therapy sessions, and difficulties facilitating caregiver–child interaction during home exercises. Although this latter item relates to the home context, it reflects the broader caregiving demands associated with PT participation and may contribute to cumulative burden affecting sustained attendance to clinic-based services. These findings are consistent with qualitative and mixed-methods studies identifying scheduling constraints, limited therapist availability, and challenges in family–therapist collaboration as major barriers to attendance at rehabilitation services.10–12 Importantly, the observed challenges related to treatment agreement and behavior management align with evidence of limited family–therapist goal alignment and impairment-focused service delivery reported in pediatric rehabilitation settings,18 suggesting possible gaps in the application of family-centered care principles. In the current study, the largest differences were observed for appointment booking policy, caregiver–child interaction during home exercises, and access to therapists, supporting the view that attendance may be shaped not only by service availability but also by the quality of family–therapist interaction and responsiveness to family needs.
Caregivers of children with irregular attendance reported significantly greater financial and psychological burden associated with PT attendance, consistent with prior evidence linking caregiver strain and cumulative burden to difficulties maintaining participation in rehabilitation services.10,12 Although physical burden and reduced family or community interaction did not reach statistical significance, the overall response pattern suggested greater burden among caregivers in the irregular attendance group. This may reflect a cumulative strain process in which attendance becomes more difficult when caregiving demands exceed the family’s available resources. Future studies should examine whether caregiver burden has a threshold effect on attendance over time.
The findings of this study have implications for the design and delivery of pediatric PT services. Improving attendance may depend more on enhancing caregiver experience and access processes than on increasing service availability or modifying structural aspects such as session frequency. Addressing barriers related to appointment scheduling, therapist communication, and alignment on treatment plans, as well as reducing caregiver financial and psychological burden, may be more effective in promoting consistent attendance. This may include implementing more flexible and user-friendly appointment systems (simplified booking procedures, reminder systems, and easier rescheduling), as well as improving communication pathways by providing caregivers with greater access to therapists for consultation and discussion. Routine attention to caregiver stress and burden within PT services may help identify families who need additional support, including referral to counseling, social work, or other appropriate support services.
Several points should be considered when interpreting these findings. The nature of cross-sectional design, the use of convenience sampling, and online data collection may introduce selection bias and limit the generalizability of findings. Attendance was classified as regular or irregular based on caregiver report, which may not fully correspond with attendance documented in PT centers and may be affected by recall or overestimation bias. Information on prior missed appointments and the duration of PT services was not collected, despite their potential relevance to attendance patterns and attendance trajectories over time. The survey focused on caregiver-reported difficulties and burden but did not assess center-level factors such as therapist availability, appointment booking systems, or communication practices nor did it include therapists’ perspectives, which were identified as key challenges among caregivers with irregular attendance. The analyses were based on bivariate comparisons, and multivariate analysis was not conducted. Therefore, the observed associations do not account for potential confounding and should not be interpreted as independent predictors of attendance. In addition, post hoc power analyses suggested adequate power for comparisons with moderate observed effects, whereas analyses with smaller observed effects were likely underpowered and differences may not have been detected. Future studies should use multivariate models to clarify the relative contribution of child-, caregiver-, and service-related factors, and may also examine how attendance patterns relate to treatment progress, goal attainment, and discharge decisions, and whether regular attendance is associated with more favorable therapy outcomes or timely discharge from services.
Conclusion
This study examined child, caregiver, and PT service-related factors associated with regular versus irregular attendance to PT services among children with CP in Saudi Arabia. Attendance to PT services for children with CP was associated with child age, educational enrollment, and caregiver-perceived service difficulties than with clinical severity or caregiver demographic characteristics. Irregular attendance was mainly associated with challenges in appointment booking, access to physical therapists, agreement on treatment plans, management of child behavior during sessions, and child–caregiver interaction during home exercises, as well as greater financial and psychological burden on caregivers. In contrast, structural features of PT services, such as center type, session frequency, and session duration, did not differ between attendance groups. These findings may highlight the importance of addressing service processes and caregiver experiences when aiming to support regular attendance to PT services for children with CP in Saudi Arabia. The findings should be interpreted with consideration of the study design and the caregiver-reported attendance, which may limit generalizability and causal interpretation.
AI Declaration
Generative artificial intelligence (ChatGPT, OpenAI; version GPT-5.2) was used solely to assist with language editing and clarity of expression in this manuscript. All content was reviewed and approved by the authors, who take full responsibility for the manuscript.
Acknowledgment
The authors would like to acknowledge and thank all participants who contributed to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors report no conflict of interest.
References
1. Trabacca A, Vespino T, Di Liddo A, Russo L. Multidisciplinary rehabilitation for patients with cerebral palsy: improving long-term care. J Multidiscip Healthc. 2016;9:455–11. doi:10.2147/JMDH.S88782
2. Novak I, Honan I. Effectiveness of paediatric occupational therapy for children with disabilities: a systematic review. Austr Occupat Ther J. 2019;66(3):258–273. doi:10.1111/1440-1630.12573
3. Novak I, Morgan C, Fahey M, et al. State of the evidence traffic lights 2019: systematic review of interventions for preventing and treating children with cerebral palsy. Curr Neurol Neurosci Rep. 2020;20(2):3. doi:10.1007/s11910-020-1022-z
4. Manikandan M, Kerr C, Lavelle G, Walsh M, Walsh A, Ryan JM. Health service use among adults with cerebral palsy: a mixed-methods systematic review. Dev Med Child Neurol. 2022;64(4):429–446. doi:10.1111/dmcn.15097
5. Almasri NA, An M, Palisano RJ. Parents’ perception of receiving family-centered care for their children with physical disabilities: a meta-analysis. Phys Occup Ther Pediatr. 2018;38(4):427–443. doi:10.1080/01942638.2017.1337664
6. Brewer K, Pollock N, Wright FV. Addressing the challenges of collaborative goal setting with children and their families. Phys Occup Ther Pediatr. 2014;34(2):138–152. doi:10.3109/01942638.2013.794187
7. Raina P, O’Donnell M, Rosenbaum P, et al. The health and well-being of caregivers of children with cerebral palsy. Pediatrics. 2005;115(6):e626–e636. doi:10.1542/peds.2004-1689
8. Murphy NA, Christian B, Caplin DA, Young PC. The health of caregivers for children with disabilities: caregiver perspectives. Child Care Health Dev. 2007;33(2):180–187. doi:10.1111/j.1365-2214.2006.00644.x
9. Alwhaibi RM, Omer AB, Khan R. Factors affecting mothers’ adherence to home exercise programs designed for their children with cerebral palsy. Int J Environ Res Public Health. 2022;19(17):10792. doi:10.3390/ijerph191710792
10. Mtima-Jere P, Msowoya S, Chinyamu V, Kanduku T, Turkel R, Mughogho A. Facilitators and barriers to the adherence of physiotherapy clinic attendance and home programme by caregivers of children with cerebral palsy in Blantyre, Malawi. Dev Neurorehabilit. 2025;28:1–8. doi:10.1080/17518423.2025.2526356
11. Ikenna CU, Mirian CO, Paul CN, Onyekachi CO, Kingsley KO, Chidera LA. Towards developing a comprehensive treatment schedule for patients with cerebral palsy: factors influencing patient’s adherence to physiotherapy treatment. Afr Health Sci. 2022;22(2):573–580. doi:10.4314/ahs.v22i2.66
12. Medina-Valera MI, Fernández-Del Olmo A, Pinero-Pinto E. Barriers and facilitators of home programmes in children with cerebral palsy: a systematic review and a metasynthesis. Child Care Health Dev. 2025;51(2):e70049. doi:10.1111/cch.70049
13. Paget SP, McIntyre S, Goldsmith S, et al. Non-attendance at outpatient clinic appointments by children with cerebral palsy. Dev Med Child Neurol. 2022;64(9):1106–1113. doi:10.1111/dmcn.15197
14. Alhammad SA, Almuhanna OK, Aljumaah AR, Aldosari MS. Determinants of appointment planning in physical therapy: insights from Saudi Arabia.Healthcare (Basel). 2025; 13 (8):893. doi:10.3390/healthcare13080893
15. Harding KE, Camden C, Lewis AK, Perreault K, Taylor NF. Service redesign interventions to reduce waiting time for paediatric rehabilitation and therapy services: a systematic review of the literature. Health Soc Care Community. 2022;30(6):2057–2070. doi:10.1111/hsc.13866
16. Ligaya KGG, Ang-Muñoz CD, Dungca ML, Abiera JEH. Caregiver’s adherence to out-patient rehabilitation program of children with cerebral palsy in a tertiary government hospital. Philippine J Health Res Dev. 2025;29(2):25–34. doi:10.4103/PJHRD_20252902_25
17. Demeke ZD, Assefa YA, Abich Y, Chala MB, Samuel AJ. Home-based therapy and its determinants for children with cerebral palsy, exploration of parents’ and physiotherapists’ perspective, a qualitative study, Ethiopia. PLoS One. 2023;18(2):e0282328. doi:10.1371/journal.pone.0282328
18. Mashabi A, Saleh MN, Alharbi AA, Albalwi AA, Albalawi HF, Al-Bakri Q. Waiting time and focus of physical therapy for children with cerebral palsy in Saudi Arabia: parents’ report. Children. 2025;12(5):544. doi:10.3390/children12050544
19. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995;36(1):1–10. doi:10.2307/2137284
20. Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997;39(4):214–223. doi:10.1111/j.1469-8749.1997.tb07414.x
21. Cohen J. Statistical Power Analysis for the Behavioral Sciences, Rev. Lawrence Erlbaum Associates, Inc; 1977.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.