Back to Journals » Journal of Asthma and Allergy » Volume 19
Characteristics of Adult Severe Uncontrolled Asthma Patients in Primary Care and Modifications in Prescribed Inhalation Treatments
Authors Konradsen JR, Packham S, Vanfleteren LE, Syk J, Bossios A ![]() , Stridsman C
, Stridsman C ![]()
Received 21 December 2025
Accepted for publication 6 March 2026
Published 19 March 2026 Volume 2026:19 585933
DOI https://doi.org/10.2147/JAA.S585933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Jon R Konradsen,1,2,* Sylvia Packham,3,4,* Lowie EGW Vanfleteren,5– 7 Jörgen Syk,8– 10 Apostolos Bossios,11– 13 Caroline Stridsman3
1Department of Woman´s and Childrens Health, Karolinska Institutet, Stockholm, Sweden; 2Astrid Lindgren’s Children’s Hospital, Karolinska University Hospital, Stockholm, Sweden; 3Department of Public Health and Clinical Medicine, The OLIN and Sunderby Research Unit at Region Norrbotten, Umeå University, Umeå, Sweden; 4Medical Affairs, AstraZeneca AB, Stockholm, Sweden; 5Department of Respiratory Medicine and Allergology, COPD Center, Sahlgrenska University Hospital, Gothenburg, Sweden; 6Department of Internal Medicine and Clinical Nutrition, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden; 7Department of Respiratory Medicine, Ghent University Hospital, Ghent, Belgium; 8Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden; 9Academic Primary Health Care Centre, Stockholm, Sweden; 10Department of Women’s and Children’s health, Uppsala University, Uppsala, Sweden; 11Division for Lung and Airway Research, Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden; 12Department of Respiratory Medicine and Allergy, Karolinska Severe Asthma Center, Huddinge, Karolinska University Hospital, Stockholm, Sweden; 13Center for Molecular Medicine, Lung Laboratory, Karolinska University Hospital, Stockholm, Sweden
*These authors contributed equally to this work
Correspondence: Caroline Stridsman, Department of Public Health and Clinical Medicine, the OLIN and Sunderby Research Unit at Region Norrbotten, Umeå University, Umeå, 901 87, Sweden, Email [email protected]
Background: Severe asthma outcomes in primary care are poorly documented. This study characterizes adults with severe uncontrolled asthma and evaluates modifications of prescribed inhalation therapy and exacerbations over 12 months.
Methods: Adult primary care asthma patients, with visits recorded in the Swedish National Airway Register from July 2017 to February 2019 (index date), were included. Data were linked to National Prescribed Drug Register. Severe asthma was defined by adherence to high dose inhaled corticosteroids (ICS) ± long-acting beta-agonists (LABA) or ICS+LABA+long-acting muscarinic antagonists. Inhalation therapy was assessed 12 months pre- and post-index. All other variables were collected up to 24 months pre-index and 12 months post-index. Uncontrolled asthma was defined as Asthma Control Test ≤ 19.
Results: Severe asthma was identified in 2789 patients, of which, 1261 had uncontrolled disease. Severe uncontrolled asthma associated with regular OCS use 24 months pre-index (OR 1.77, 95% CI 1.42– 2.20), obesity (1.63, 1.32– 2.02), primary school education (1.55, 1.22– 1.96) and inversely associated with asthma management education (0.77, 0.66– 0.90). Post-index, 5%, 55% and 45% increased, maintained or reduced their inhalation therapy, respectively. Patients increasing inhalation therapy had lower mean FEV1% predicted (67.8 vs. 80.9 and 79.4), more regular OCS uses pre-index (34.8% vs. 17% and 21.9%), and high SABA use (33.3% vs. 27.3% and 21.3%). Post-index asthma exacerbations in severe uncontrolled asthma associated with rhinitis (1.46, 95% CI 1.14– 1.88), cardiovascular disease (1.38, 1.06– 1.80), high SABA use (1.79, 1.38– 2.34), and treatment increase (1.83, 1.08– 3.10).
Conclusion: In primary care, severe uncontrolled asthma was among other factors associated with regular OCS use, obesity, lower educational level and absence of asthma management education. Uncontrolled patients already adhering to high dose ICS medication and further increased inhalation therapy were at greater risk of exacerbations, indicating the need for referral to secondary care.
Keywords: treatment outcome, asthma management, inhalation adjustment
Introduction
Asthma is a chronic inflammatory respiratory disease affecting hundreds of millions of people worldwide with an estimated prevalence of 8–10% in high-income countries.1–4 It is a variable disease with symptoms such as wheezing, dyspnea, cough, mucus production and airway hyper-responsiveness.5 Disease severity, mild, moderate or severe asthma, is diagnosed retrospectively and defined according to treatment response.2 Severe asthma is estimated to 4–10% of the asthma population and is diagnosed in patients who, despite confirmed adherence, correct inhalation technique, and optimal management of comorbidities, require high-dose inhaled corticosteroids (ICS) plus at least one additional maintenance therapy to achieve symptom control.6,7 Severe uncontrolled asthma occurs despite these measures and is characterized by elevated symptom burden, frequent exacerbations, impaired lung function and comorbidities.8–13 However, if asthma control is not achievable in primary care, referral to specialist centers is advised for further evaluation.2,14 Despite that, it has been reported that 48–72% of patients with severe uncontrolled asthma patients are not being referred to secondary care, highlighting the unmet need for this patient group.6,15,16
Comorbidities related to severe asthma can be linked to the underlying type 2-high inflammation, such as allergic rhinitis and nasal polyposis.17 Some comorbidities may also be related to oral corticosteroid (OCS) treatment, including osteoporosis, psychiatric disorders, cardiovascular disease, obesity and type 2 diabetes.18–20 Severe uncontrolled asthma has a detrimental impact on the individual patient but also for the society with increased costs, including comorbidity related costs.4,21–23 Although severe uncontrolled asthma is rare, it has 1.7 to 5 times higher net cost compared to mild to moderate disease.21,23–25 Furthermore, healthcare resource utilization and societal costs are higher in patients treated with regular or periodic OCS compared to non-OCS users.26
Taken together, it is of utmost importance to recognize severe uncontrolled asthma patients in primary care and to identify barriers to enable the patient to reach controlled disease in a timely manner. This is crucial to avoid disease progression, long-term exposure of OCS treatment and reduce health care usage and costs.
Population-based nationwide data on well characterized severe asthma patients with longitudinal follow up are scarce. We therefore aimed to fill an evidence gap of severe uncontrolled asthma in primary care by utilizing multiple population registers, including disease specific register. The specific objectives were to: (I) describe the characteristics and clinical variables of severe uncontrolled asthma in primary care and to (II) investigate modifications in inhalation therapy and factors associated with exacerbations in severe uncontrolled asthma patients 12 months after a primary care visit.
Methods
Study Design and Population
In this observational, retrospective, cohort study, patients with a diagnosis of asthma (ICD-10 J45) and with a healthcare visit registered in the Swedish National Airway Register (SNAR) between July 2017 and February 2019 (index date) were identified (n = 42945). The overall study population, medication use, and variables have been described in detail previously.27 In the current study, we included adult patients with asthma, registered in primary care and adherent to inhalation treatment corresponding to modified GINA step 4–5. Patients younger than 18 years, patients registered in secondary care and/or with a concomitant COPD diagnosis were excluded (Figure 1A). The study was approved by the Swedish Ethical Review Authority (2019–04915; 2020–00508) and complies with the Declaration of Helsinki. Informed consent was not obtained as it is not required in Sweden when using anonymized register data.
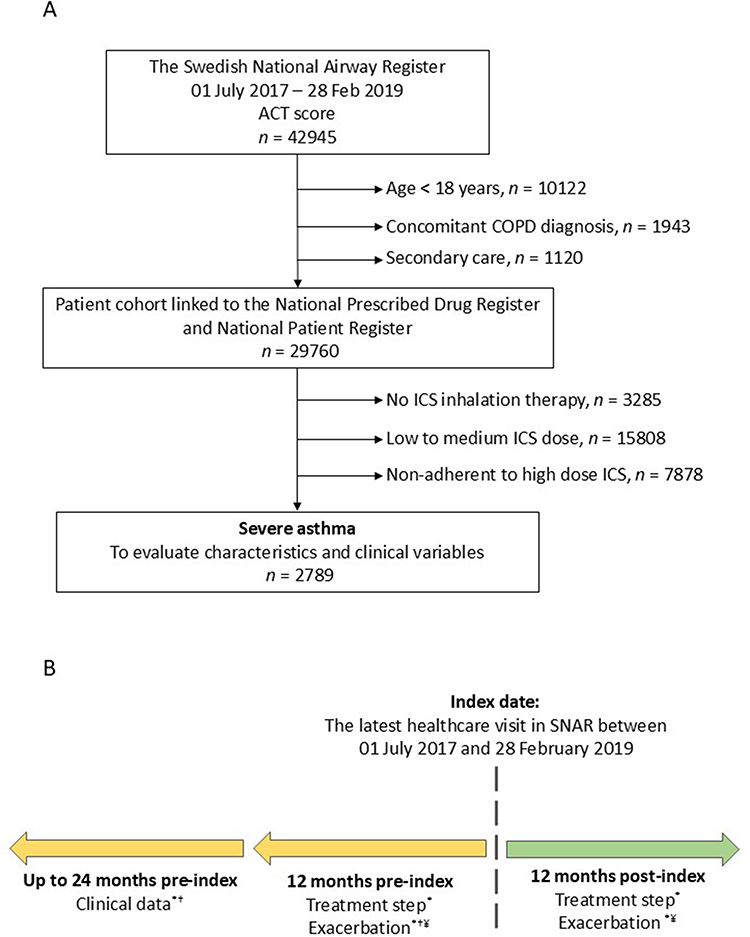 |
Figure 1 Schematic overview of the (A) study population and (B) Variables pre- and post-index. Abbreviations: ACT, asthma control test; COPD, chronic obstructive pulmonary disease; ICS, inhaled corticosteroid. Notes: (A) Severe asthma was defined by adherence to high dose ICS ± long-acting beta-agonists (LABA) or ICS+LABA+long-acting muscarinic antagonists. (B) *Data from Swedish Prescribed Drug Register † Data from Swedish National Airway Register. ¥ Data from National Patient Register. |
Clinical Data and Definitions
Severe asthma was defined as being adherent to prescribed inhalation treatment corresponding to modified GINA step 4; very high dose ICS (≥1600 µg daily budesonide eq) with or without long-acting beta agonist (LABA) or long-acting muscarinic antagonist (LAMA), or medium to high dose ICS (≥400–1599 µg daily budesonide eq) + LABA + LAMA and GINA step 5; very high dose ICS + LABA + LAMA.28
Drug adherence was calculated using Medication Possession Ratio (MPR); sum of days supply dispensed from the first fill until the end of the time period (12 months pre-index) divided by sum of the number of days from the first fill until the end of the time frame (inclusive of last prescription) [25]. Only patients with at least 80% MPR to prescribed treatment were included, n = 2789 (Figure 1A).
Clinical data were collected up to 24 months pre-index from the national registers SNAR, National Prescribed Drug Register (NPDR) and National Patient Register (NPR) (Figure 1B). Variables included from SNAR were level of care, sex, age, body mass index (BMI), smoking history, post-bronchodilator forced expiratory volume in 1 second as percent of predicted value (FEV1% pred), asthma management education and Asthma Control Test (ACT). Uncontrolled asthma was defined as having an ACT score of 19 or lower.
Asthma exacerbations were investigated 12 months post-index and defined as hospitalization with a primary diagnosis of asthma (ICD-10 classifications J45 and J46), alternatively J46 secondary care in NPR and/or any use of OCS in NPDR.
Inhalation treatment adjustments were investigated 12 months post-index and calculated from the earliest prescription of inhalation therapy followed by additional 3 months forward. Inhalation treatments were categorized into the following groups of ICS and add-on of LABA and/or LAMA; (I) high dose ICS + LABA + LAMA (II) high dose ICS ± LABA or LAMA or low to medium ICS + LABA + LAMA (III) Low to medium dose ICS ± LABA or LAMA (IV) low to medium dose ICS (V) other, eg. short-acting beta agonist (SABA) only and (VI) no prescribed inhalation treatment (Supplementary Figure 1). Low to medium and high dose ICS were defined based on the prescribed strength of the ICS dose in the inhaler (Supplementary Table 1).
Comorbidities were identified by pharmacy claims in the NPDR up to 24 months prior to index date and defined by Anatomical Therapeutic Chemical (ATC) codes; allergy (R06AX13/22/26-27, R06AE07), rhinitis (R01), cardiovascular disease (C01-03, C07-09), depression (N06) and diabetes (A10A, A10B).
In the 12 month pre-index period, high use of short-acting beta-antagonist (SABA) was considered having three or more pharmacy claims and regular OCS use was defined as having at least two pharmacy claims.
Level of education was classified into primary school (9 years of education), secondary school (12 years) and tertiary education (more than 12 years). Data were retrieved from Statistics Sweden.
Statistical Analysis
Baseline characteristics were reported for all patients included in the study. Continuous variables were described as mean and standard deviation (SD), and categorical data were presented as relative frequencies (%) observed. For comparisons between groups, t-tests were used for continuous data and Chi-square tests for categorical data. Odds ratios (OR) and 95% confidence intervals (CI) were estimated in bivariable and multivariable logistic regression analyses, including missing values as separate category. Independent variables with statistically significant associations in the bivariable analyses were included in the multivariable analyses. Statistical analyses were performed using SAS 9.4 for Windows and IBM SPSS statistics 29.
Results
Baseline Characteristics and Associations with Severe Uncontrolled Asthma
Out of 29760 adult asthma patients in primary care, severe asthma was identified in 2789 patients (9.4%). Most severe asthma patients, 93%, were in the step 4 treatment group. Uncontrolled severe asthma was identified in 1261 patients (45%), and there was a slightly higher proportion of patients with uncontrolled severe asthma in treatment step 5 compared to step 4 (Figure 2). Patient characteristics and bivariate comparative analysis of patients with controlled versus uncontrolled asthma are shown in Table 1. Severe uncontrolled patients were more often females (66.5% vs 59.0%), had a higher BMI (28.9 vs 27.5), lower FEV1% pred (79.6 vs 82.9), higher proportion of regular OCS users 24 months pre-index (19.9% vs 11.3%) and greater proportion of high SABA users (25.2% vs 14.5%) compared to controlled severe patients (all comparisons, p < 0.001). The severe uncontrolled group also included fewer patients who had received asthma management education (52.9% vs 59.1%), and fewer patients having completed tertiary level of education (36.3% vs 44.7%) (all comparisons, p < 0.001). Furthermore, there was a higher proportion of patients in the severe uncontrolled group that were current smoker or ex-smokers and a higher proportion of patients with comorbidities than in the severe controlled group (Table 1).
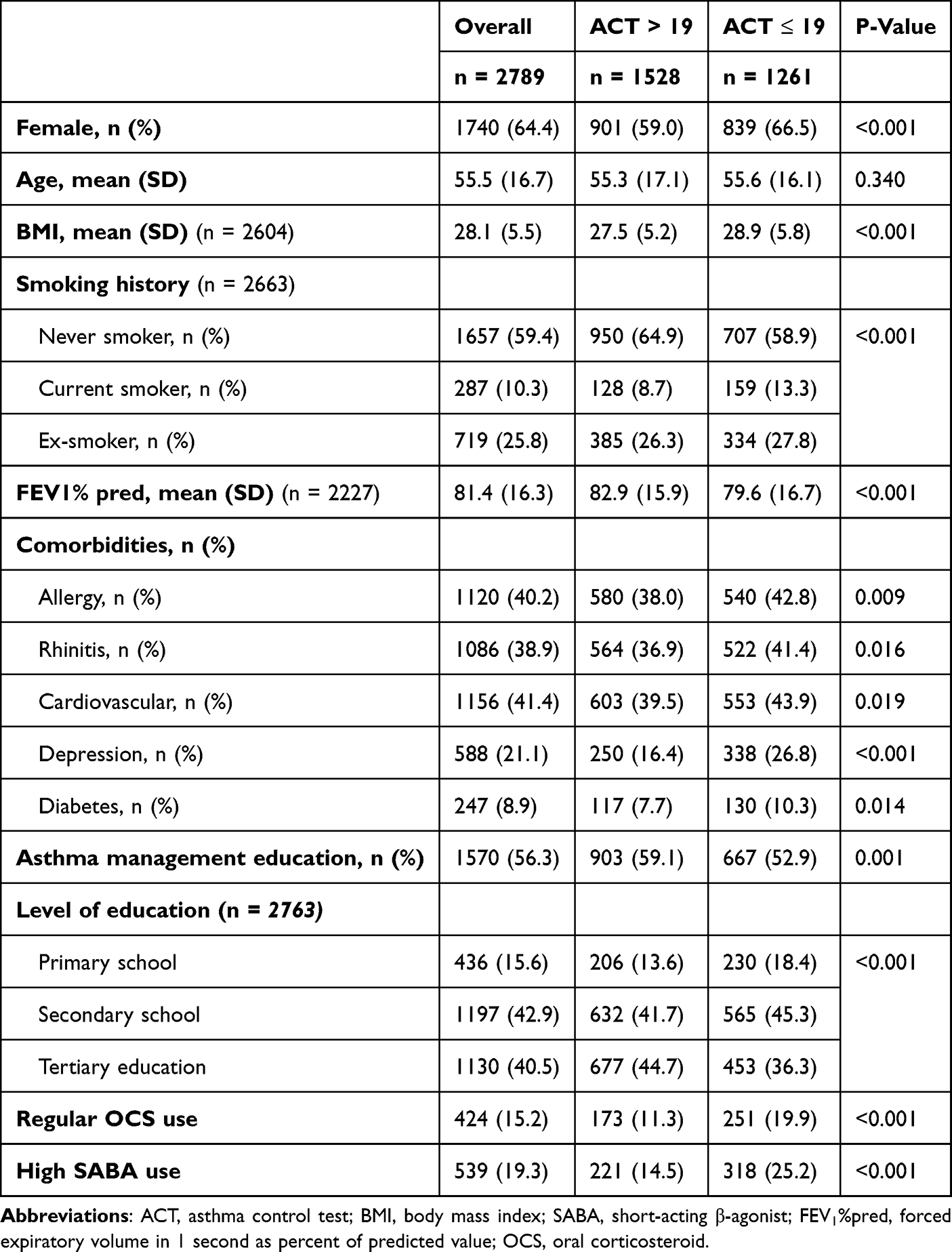 |
Table 1 Baseline Characteristics in Patients with Severe Asthma |
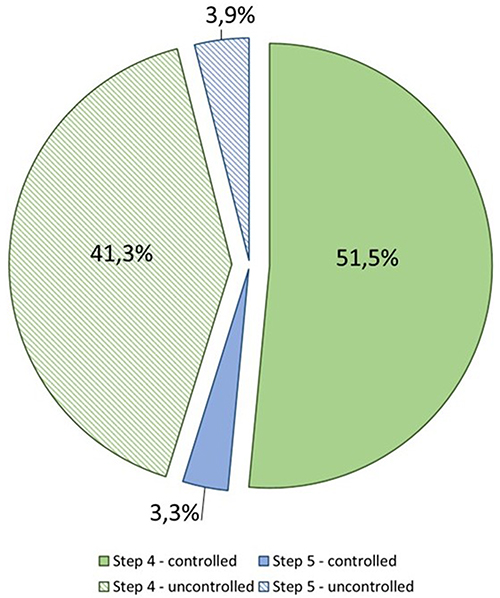 |
Figure 2 Proportions of severe asthma by treatment steps and asthma control in primary care. |
In adjusted analysis, severe uncontrolled asthma was associated with female sex (OR 1.27, 95% CI 1.08–1.50), obesity (1.63, 1.32–2.02), current smoking (1.43, 1.09–1.86), lower level of education; primary school (1.57, 1.24–1.99) and secondary school (1.23, 1.04–1.47) and regular OCS use 24 months pre-index (1.77, 1.42–2.22). Having received asthma management education was inversely associated with severe uncontrolled asthma (0.77, 0.66–0.90). Lower lung function was significant in crude analysis, and borderline significant in the adjusted analysis (1.24, 1.00–1.55, p = 0.055) (Figure 3).
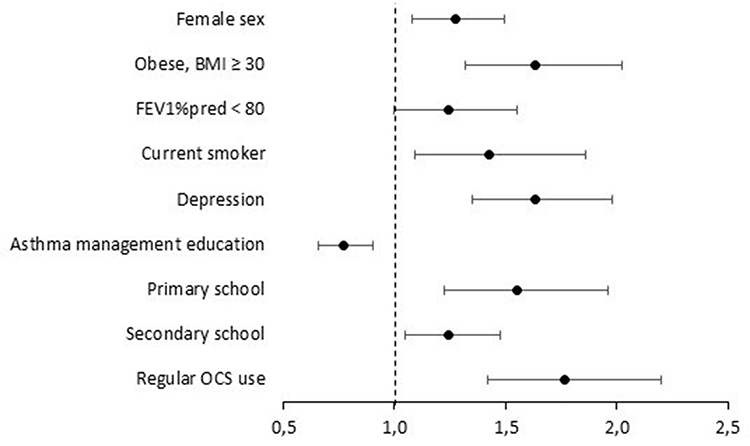 |
Figure 3 Adjusted model with poor asthma control as the dependent variable. The model was also adjusted for allergy, rhinitis, cardiovascular disease, diabetes, BMI groups underweight and overweight which were all non-significant. Reference groups within respective category; BMI 18.5–24.9; smoking habits, non-smoker; and level of education, tertiary education. Abbreviations: BMI, Body Mass Index; FEV1% pred, forced expiratory volume in 1 second as percent of predicted value. |
Changes in Inhalation Therapy and Exacerbations in Severe Uncontrolled Asthma
In the severe uncontrolled group, 55% remained within the same treatment strategy, 40% stepped down in treatment and 5% increased their inhalation treatment during the 12 months follow-up period (Figure 4). Of the 66 patients who increased their inhalation treatment, two patients initiated biologic treatment for severe asthma. Notably, 14.7% (n = 186) had no ICS prescribed during the follow-up period.
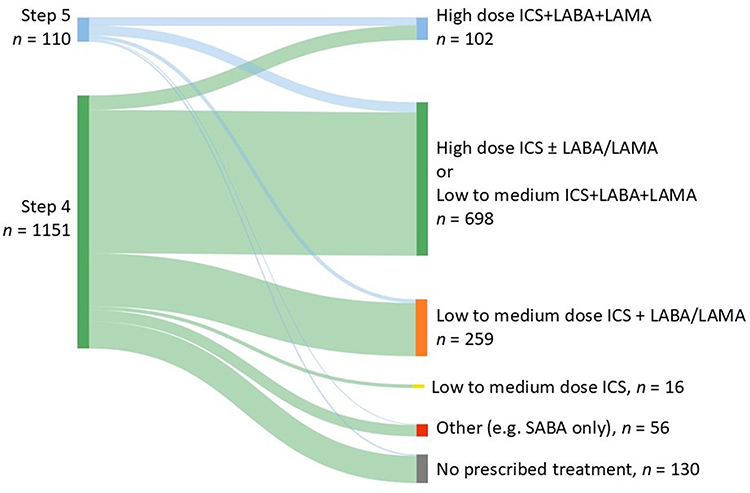 |
Figure 4 Treatment transitions of severe uncontrolled patients. |
Patients increasing their inhalation treatment were older with a mean age of 64.8 years versus staying within the same treatment category (56.4 years) or stepping down in treatment (53.4 years). Patients increasing therapy had lower mean FEV1% pred compared to patients staying on the same treatment step (67.8 vs 80.9) and the group stepping down in treatment (67.8 vs 79.4). The treatment group increasing inhalation therapy had significantly higher proportions of patients with a FEV1% pred <80 (75.5%), FEV1% pred <60 (32.1%), regular OCS use 24 months pre-index (34.8%) (all p < 0.001) and high SABA use (33.3%) (p = 0.018) compared to patients on the same treatment step or stepped down (Table 2). A higher proportion of patients stepping down in treatment were regular OCS users 24 months pre-index compared to patients staying on the same treatment step (21.9% vs 17.0%). There was no difference between the three groups in BMI, smoking history, comorbidities, having received asthma management education and level of education (Supplementary Table 2).
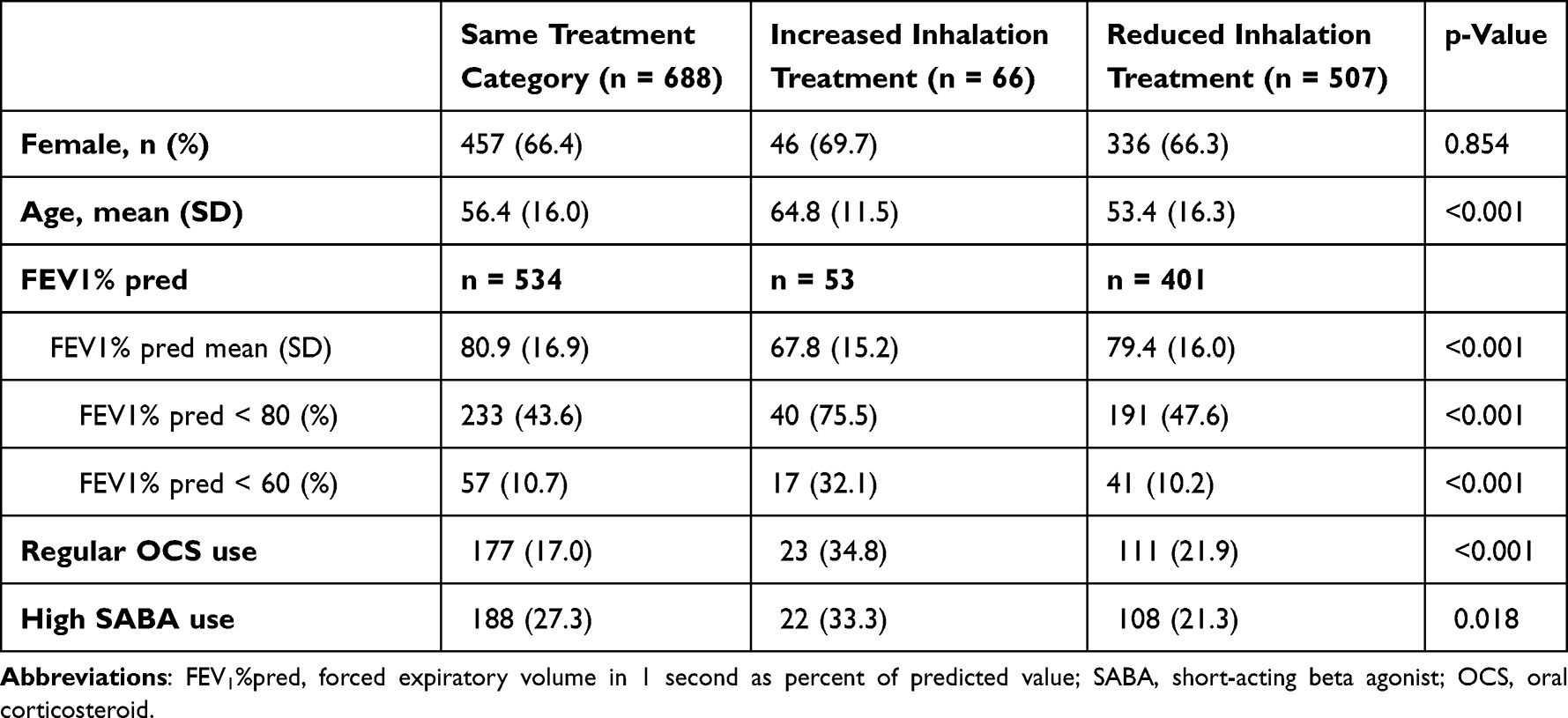 |
Table 2 Lung Function of Severe Uncontrolled Asthma Patients During Post-Index |
In adjusted analysis, post-index exacerbation in the severe uncontrolled group was associated with cardiovascular diseases (OR 1.38, 95% CI 1.06–1.80), rhinitis (1.46, 1.14–1.88), high SABA use (1.79, 1.38–2.34) and in patients increasing inhalation treatment (1.83, 1.08–3.1). In crude analysis, better lung function was inversely associated with post-exacerbation but was not significant in the adjusted model (Figure 5).
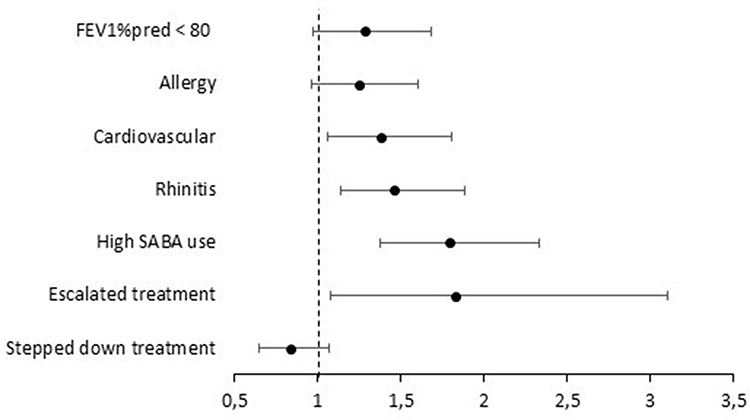 |
Figure 5 Independent predictors of post-index exacerbation in the uncontrolled group. The model was also adjusted for sex and age which were non-significant. Treatment transition; same treatment step was used as reference. Abbreviations: FEV1% pred, forced expiratory volume in 1 second as percent of predicted value; SABA, short-acting β-agonist. |
Discussion
This large nationwide register study, reflecting real-world primary care for patient with severe asthma, showed that almost half of these patients have uncontrolled disease. Despite their high risk for future exacerbations, treatment increase in inhalation therapy was rarely implemented during follow-up. Our study identified several treatment barriers, pharmacological and non-pharmacology, that need to be addressed to be able to achieve sustainable asthma control in primary care, and which represent a key issue requiring targeted attention from political stakeholders and healthcare leaders.
The overall prevalence of severe asthma and severe uncontrolled asthma in our primary care study was 9.4% and 4.2%, respectively, which is in line of what has been reported previously.7,8 Severe uncontrolled asthma was associated with female sex, obesity, current smoking, and depression. Our data strengthens previous findings from a smaller patient cohort including 140 patients with severe asthma showing that depression is associated with poorer asthma control and needs to be addressed in severe asthma management.10 Obesity has shown to be associated with disease progression into severe asthma and worse symptom control29 and a recent review addressed the complexity between these two diseases and that obesity and asthma both aggravate each other.30 Current guidelines emphasise the importance of investigating smoking habits and comorbidities to be able to achieve symptom control2 and our findings further highlight the need to focus on these parameters during asthma assessment.
Furthermore, severe uncontrolled asthma was also associated with lower education, which is an indirect measure of socioeconomic status. Previous studies, investigating asthma outcomes and socioeconomic status, have found a correlation between low socioeconomic status and worse asthma control, highlighting this as a vulnerable patient group which needs further attention to avoid uncontrolled asthma and associated costs with increased utilization of healthcare resources.31,32 Moreover, clinical benefit has been reported when providing tailored and repeated patient education in severe asthma in specialist care and in primary care.33–35 In our study, patients that had at least once received asthma management education were captured, indicating the benefit of patient education.
In patients with severe uncontrolled asthma, only 5% increased inhalation treatment therapy during follow-up. This patient group could possibly be classified as severe refractory asthma as we found an association between having an exacerbation during post-index and increased inhalation treatment. Furthermore, this group had the lowest lung function with 32% having an FEV1% pred below 60, compared to about 10% in the groups stepping down treatment or staying within the same treatment strategy during follow-up. As a consequence of not being able to reach controlled disease, patients may develop airway remodeling due to the underlying airway inflammation.36 Persistent airflow obstruction may indicate structural changes of the airways and has been shown to correlate with FEV1% pred below 60.37 Furthermore, a recent study investigated pre-biologic disease trajectories and response to biologics and found that patients with chronic severe asthma had the lowest prevalence of remission.38
An interesting finding is the high proportion of patients reducing their inhalation treatment. Asthma is a variable disease, and symptoms may fluctuate with seasonal variations such as weather change, pollen exposure and infections.39–41 This could partly explain the reduction in inhalation therapy, however, 14.6% of uncontrolled asthma patients did not have any prescribed ICS treatment during post-index. Today, ICS is fundamental in asthma management from mild to severe asthma and well established to prevent exacerbations and mortality.28,42 Within the group that reduced their inhalation therapy, more than 1 in 5 patients were regular OCS users 24 months pre-index, which might indicate dependency on systemic corticosteroid treatment rather than using ICS.
Our study identified several potential barriers of achieving asthma control in a primary care setting and suggests that improving asthma control requires a holistic patient approach; including both the patient (eg. asthma management education, weight management, and smoking cessation support), as well as improving healthcare adherence to guideline directed therapy (eg. patients with asthma symptoms in combination with high dose ICS+LABA should be referred to secondary care). For example, asthma control can be improved by nurse-led patient education or using digital home-monitoring tools43,44 and increased adherence to asthma treatment guidelines could potentially be achieved by clinical decision support system or artificial intelligence driven approach, which is yet to be optimized and verified on a large scale.43,45,46 By including both the patient and the healthcare system, there is a great potential in preventing exacerbations and OCS-related diseases which would improve the health for the patient, especially low to middle income individuals as suggested by our results, and simultaneously achieving long-term cost-savings for the healthcare.26,47
The strength of this study is that it is a large nationwide study including patients with a physician diagnosis of asthma. Further, by using multiple national registers, we could capture disease specific variables, medication use and demographic information. One limitation is the use of the asthma control test (ACT) to define uncontrolled asthma, which do not capture previous exacerbations or OCS use. A newly validated instrument, the Asthma Impairment and Risk Questionnaire (AIRQ), has been developed to capture these parameters and to better identify at-risk patients.48–50 Another limitation is that our study only focused on changes in inhalation therapy and did not include leukotriene receptor antagonist or azithromycin when investigating treatment modifications. This study includes the assumption of patients having pharmacy claims will use their inhalers as prescribed and could lead to misclassification of disease severity. This could, at least partly, explain why 40% of patients with severe uncontrolled asthma stepped down in inhalation treatment during follow-up.
Conclusions
Patients with severe asthma in primary care are commonly uncontrolled. Poor asthma control is associated with use of oral corticosteroids, comorbidities eg. obesity, socio-economic factors and absence of asthma management education. Current healthcare management of severe uncontrolled asthma in primary care is insufficient with only a minority of patients increasing inhalation treatment. The association between future exacerbation and patients having increased therapy may indicate severe refractory asthma and too late intervention. This patient group also had the lowest lung function and should be prioritized for secondary care referrals to prevent future exacerbations and disease deterioration.
Abbreviations
ACT, asthma control test; AIRQ, asthma impairment and risk questionnaire; BMI, Body Mass Index; CI, confidence intervals; FEV1% pred, forced expiratory volume in 1 second as percent of predicted value; ICD-10, International Classification of Diseases, Tenth Revision; ICS, inhaled corticosteroid; LABA, long-acting beta-agonist; LAMA, long-acting muscarinic antagonist; NPDR, National Prescribed Drug Register NPR, National Patient Register; OCS, oral corticosteroid; OR, odds ratio; SABA, short-acting beta-agonist; SNAR, Swedish National Airway Register.
Data Sharing Statement
The pseudonymized research database is held and managed by Region Norrbotten, Sweden, and is available from the corresponding author on reasonable request and with ethical permission. The study utilized data from the following sources: Swedish National Airway Register, National Prescribed Drug Register, National Patient Register, and Statistics Sweden.
Ethics Approval and Informed Consent
This non-interventional, retrospective register study was approved by the Swedish Ethical Review Authority (2019-04915; 2020-00508) and complies with the Declaration of Helsinki. Informed consent was not obtained as it is not required in Sweden when using secondary anonymized register data.
Acknowledgment
Acknowledgement is given to all the patients and healthcare professionals who contribute with registrations in SNAR. Further acknowledgements are given to the current SNAR steering committee and coordinators Anne Lindberg, Apostolos Bossios, Caroline Stridsman, Fredrik Nyberg, Frida Strömberg Celind, Henning Stenberg, Jon Konradsen, Jörgen Syk, Lowie Vanfleteren, Therese Sterner, Yvonne Sjöö, Kerstin Sundell Bergström together with representatives from the asthma- and allergy association and the Swedish heart and lung association as well as the founders of the register Ann Ekberg Jansson, Alf Tunsäter, Christophe Pedroletti and Thomas Gars.
Disclosure
The work was financially supported by AstraZeneca. SP is an employee of AstraZeneca and may or may not own stock or stock options in AstraZeneca. AB reports institutional fees from Chiesi, GSK, and AstraZeneca and institutional grants from AstraZeneca outside the submitted work. AB is supported by grants from the Swedish Heart-Lung Foundation (2022-0478). CS is supported through a regional agreement between Umeå University and Region Västerbotten (ALF) and the Swedish Heart-Lung Foundation (20230537, 20230473). JS has nothing to report. LEGWV reports personal payments for lectures and/or advisory boards from GSK, Astrazeneca, Chiesi, Pulmonx, Sanofi, Boehringer, Novartis. CS reports personal and institutional fees from AstraZeneca, Chiesi, GSK, and TEVA for lectures and/or advisory boards. JRK reports advisory board fees from Novartis and ALK and institutional fees and Thermo Fisher Scientific outside the submitted work. JRK is supported by a scholarship from Region Stockholm and by grants from the Freemason Child House Foundation, the Konsul Th. C. Bergh’s Foundation, the Swedish Asthma and Allergy Association’s Research Foundation, the Swedish Heart-Lung Foundation, and the Pediatric Research Foundation of Astrid Lindgren Children’s Hospital. The authors report no other conflicts of interest in this work.
References
1. To T, Stanojevic S, Moores G. et al. Global asthma prevalence in adults: findings from the cross-sectional world health survey. BMC Public Health. 2012;12(1):204. doi:10.1186/1471-2458-12-204
2. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2024. Available from: www.ginasthma.org.
3. Backman H, Raisanen P, Hedman L, et al. Increased prevalence of allergic asthma from 1996 to 2006 and further to 2016-results from three population surveys. Clin Exp Allergy. 2017;47(11):1426–11. doi:10.1111/cea.12963
4. Swed S, Sawaf B, Al-Obeidat F, et al. Asthma prevalence among United States population insights from NHANES data analysis. Sci Rep. 2024;14(1):8059. doi:10.1038/s41598-024-58429-5
5. Porsbjerg C, Melen E, Lehtimaki L, Shaw D. Asthma. Lancet. 2023;401(10379):858–873. doi:10.1016/S0140-6736(22)02125-0
6. Hansen S, von Bulow A, Sandin P, et al. Prevalence and management of severe asthma in the Nordic countries: findings from the NORDSTAR cohort. ERJ Open Res. 2023;9(2):00687–2022. doi:10.1183/23120541.00687-2022
7. Ronnebjerg L, Axelsson M, Kankaanranta H, et al. Severe Asthma in a General Population Study: prevalence and Clinical Characteristics. J Asthma Allergy. 2021;14:1105–1115. doi:10.2147/JAA.S327659
8. Larsson K, Stallberg B, Lisspers K, et al. Prevalence and management of severe asthma in primary care: an observational cohort study in Sweden (PACEHR). Respir Res. 2018;19(1):12. doi:10.1186/s12931-018-0719-x
9. Ding B, Chen S, Srivastava D, et al. Symptom Burden, Health Status, and Productivity in Patients with Uncontrolled and Controlled Severe Asthma in NOVELTY. J Asthma Allergy. 2023;16:611–624. doi:10.2147/JAA.S401445
10. Stubbs MA, Clark VL, Gibson PG, Yorke J, McDonald VM. Associations of symptoms of anxiety and depression with health-status, asthma control, dyspnoea, dysfunction breathing and obesity in people with severe asthma. Respir Res. 2022;23(1):341. doi:10.1186/s12931-022-02266-5
11. Sorkness RL, Bleecker ER, Busse WW, et al. Lung function in adults with stable but severe asthma: air trapping and incomplete reversal of obstruction with bronchodilation. J Appl Physiol. 2008;104(2):394–403. doi:10.1152/japplphysiol.00329.2007
12. Backman H, Jansson SA, Stridsman C, et al. Severe asthma-A population study perspective. Clin Exp Allergy. 2019;49(6):819–828. doi:10.1111/cea.13378
13. Mincheva R, Ekerljung L, Bossios A, Lundback B, Lotvall J. High prevalence of severe asthma in a large random population study. J Allergy Clin Immunol. 2018;141(6):2256–2264e2. doi:10.1016/j.jaci.2017.07.047
14. Läkemedelsverket. Behandlingsrekommendation: astma hos barn och vuxna. 2023. Available from: https://www.lakemedelsverket.se/astma.
15. Ryan D, Heatley H, Heaney LG, et al. Potential Severe Asthma Hidden in UK Primary Care. J Allergy Clin Immunol Pract. 2021;9(4):1612–1623e9. doi:10.1016/j.jaip.2020.11.053
16. Timmermann H, Milger K, Virchow JC, et al. Health Care Situation in the Treatment of Uncontrolled GINA Step 4/5 Patients in Germany. J Asthma Allergy. 2023;16:813–820. doi:10.2147/JAA.S418658
17. Scelo G, Torres-Duque CA, Maspero J, et al. Analysis of comorbidities and multimorbidity in adult patients in the International Severe Asthma Registry. Ann Allergy Asthma Immunol. 2024;132(1):42–53. doi:10.1016/j.anai.2023.08.021
18. Price DB, Trudo F, Voorham J, et al. Adverse outcomes from initiation of systemic corticosteroids for asthma: long-term observational study. J Asthma Allergy. 2018;11:193–204. doi:10.2147/JAA.S176026
19. Ekstrom M, Nwaru BI, Hasvold P, Wiklund F, Telg G, Janson C. Oral corticosteroid use, morbidity and mortality in asthma: a nationwide prospective cohort study in Sweden. Allergy. 2019;74(11):2181–2190. doi:10.1111/all.13874
20. Sweeney J, Patterson CC, Menzies-Gow A, et al. Comorbidity in severe asthma requiring systemic corticosteroid therapy: cross-sectional data from the Optimum Patient Care Research Database and the British Thoracic Difficult Asthma Registry. Thorax. 2016;71(4):339–346. doi:10.1136/thoraxjnl-2015-207630
21. Hakansson KEJ, Lokke A, Ibsen R, Hilberg O, Backer V, Ulrik CS. Beyond direct costs: individual and societal financial burden of asthma in young adults in a Danish nationwide study. BMJ Open Respir Res. 2023;10(1):e001437. doi:10.1136/bmjresp-2022-001437
22. Jansson SA, Backman H, Andersson M, et al. Severe asthma is related to high societal costs and decreased health related quality of life. Respir Med. 2020;162:105860. doi:10.1016/j.rmed.2019.105860
23. Kerkhof M, Tran TN, Soriano JB, et al. Healthcare resource use and costs of severe, uncontrolled eosinophilic asthma in the UK general population. Thorax. 2018;73(2):116–124. doi:10.1136/thoraxjnl-2017-210531
24. Nunes C, Pereira AM, Morais-Almeida M. Asthma costs and social impact. Asthma Res Pract. 2017;3:1. doi:10.1186/s40733-016-0029-3
25. Bahadori K, Doyle-Waters MM, Marra C, et al. Economic burden of asthma: a systematic review. BMC Pulm Med. 2009;9(1):24. doi:10.1186/1471-2466-9-24
26. Janson C, Lisspers K, Stallberg B, et al. Health care resource utilization and cost for asthma patients regularly treated with oral corticosteroids - a Swedish observational cohort study (PACEHR). Respir Res. 2018;19(1):168. doi:10.1186/s12931-018-0855-3
27. Packham S, Odling M, Bossios A, Konradsen JR, Stridsman C. Adherence to inhaled corticosteroid therapy and treatment escalation in the Swedish adult asthma population. Respir Med. 2024;231:107714. doi:10.1016/j.rmed.2024.107714
28. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2025. Available from: https://ginasthma.org/2025-gina-strategy-report/.
29. Backman H, Stridsman C, Hedman L, et al. Determinants of Severe Asthma - A Long-Term Cohort Study in Northern Sweden. J Asthma Allergy. 2022;15:1429–1439. doi:10.2147/JAA.S376806
30. Olejnik AE, Kuznar-Kaminska B. Association of Obesity and Severe Asthma in Adults. J Clin Med. 2024;13(12):3474. doi:10.3390/jcm13123474
31. Busby J, Price D, Al-Lehebi R, et al. Impact of Socioeconomic Status on Adult Patients with Asthma: a Population-Based Cohort Study from UK Primary Care. J Asthma Allergy. 2021;14:1375–1388. doi:10.2147/JAA.S326213
32. Hakansson KEJ, Backer V, Ulrik CS. Socioeconomic status is associated with healthcare seeking behaviour and disease burden in young adults with asthma - A nationwide cohort study. Chron Respir Dis. 2022;19:14799731221117297. doi:10.1177/14799731221117297
33. Laurence R, Ancel J, Devilliers MA, et al. Patient education needs in severe asthma, a pilot study. BMC Pulm Med. 2024;24(1):134. doi:10.1186/s12890-024-02960-8
34. Boulet LP, Boulay ME, Gauthier G, et al. Benefits of an asthma education program provided at primary care sites on asthma outcomes. Respir Med. 2015;109(8):991–1000. doi:10.1016/j.rmed.2015.05.004
35. Plaza V, Peiro M, Torrejon M, et al. A repeated short educational intervention improves asthma control and quality of life. Eur Respir J. 2015;46(5):1298–1307. doi:10.1183/13993003.00458-2015
36. Hough KP, Curtiss ML, Blain TJ, et al. Airway Remodeling in Asthma. Front Med Lausanne. 2020;7:191. doi:10.3389/fmed.2020.00191
37. Konstantellou E, Papaioannou AI, Loukides S, et al. Persistent airflow obstruction in patients with asthma: characteristics of a distinct clinical phenotype. Respir Med. 2015;109(11):1404–1409. doi:10.1016/j.rmed.2015.09.009
38. Soendergaard MB, Hjortdahl F, Hansen S, et al. Pre-biologic disease trajectories are associated with morbidity burden and biologic treatment response in severe asthma. Eur Respir J. 2025;65(4):2401497. doi:10.1183/13993003.01497-2024
39. RN Bauer, Yang X, TL Staton, et al. Seasonal variability of lung function and Asthma Quality of Life Questionnaire Scores in adults with uncontrolled asthma. BMJ Open Respir Res. 2019;6(1):e000406. doi:10.1136/bmjresp-2019-000406
40. D’Amato G, Annesi-Maesano I, Urrutia-Pereira M, et al. Thunderstorm allergy and asthma: state of the art. Multidiscip Respir Med. 2021;16(1):806. doi:10.4081/mrm.2021.806
41. Iikura M, Hojo M, Koketsu R, et al. The importance of bacterial and viral infections associated with adult asthma exacerbations in clinical practice. PLoS One. 2015;10(4):e0123584. doi:10.1371/journal.pone.0123584
42. O’Byrne P, Fabbri LM, Pavord ID, Papi A, Petruzzelli S, Lange P. Asthma progression and mortality: the role of inhaled corticosteroids. Eur Respir J. 2019;54(1):1. doi:10.1183/13993003.00491-2019
43. Matui P, Wyatt JC, Pinnock H, Sheikh A, McLean S. Computer decision support systems for asthma: a systematic review. NPJ Prim Care Respir Med. 2014;24(1):14005. doi:10.1038/npjpcrm.2014.5
44. Bjerg A, Ljungberg H, Dierschke K, et al. Shorter time to clinical decision in work-related asthma using a digital tool. ERJ Open Res. 2020;6(3):00259–2020. doi:10.1183/23120541.00259-2020
45. Tan LD, Nguyen N, Lopez E, et al. Artificial Intelligence in the Management of Asthma: a Review of a New Frontier in Patient Care. J Asthma Allergy. 2025;18:1179–1191. doi:10.2147/JAA.S535264
46. Herchline D, Mitchell M, Brannen S, et al. Improving Asthma Guideline Implementation in Hospital Medicine (ImAGINE): a Single-site Improvement Initiative. Pediatr Qual Saf. 2025;10(4):e818. doi:10.1097/pq9.0000000000000818
47. Canonica GW, Colombo GL, Bruno GM, et al. Shadow cost of oral corticosteroids-related adverse events: a pharmacoeconomic evaluation applied to real-life data from the Severe Asthma Network in Italy (SANI) registry. World Allergy Organ J. 2019;12(1):100007. doi:10.1016/j.waojou.2018.12.001
48. Chipps B, Zeiger RS, Beuther DA, et al. The Asthma Impairment and Risk Questionnaire enhances the assessment of asthma control. Ann Allergy Asthma Immunol. 2023;131(4):436–443e1. doi:10.1016/j.anai.2023.04.024
49. Chipps BE, Zeiger RS, Beuther DA, et al. Advancing assessment of asthma control with a composite tool: the Asthma Impairment and Risk Questionnaire. Ann Allergy Asthma Immunol. 2024;133(1):49–56. doi:10.1016/j.anai.2024.03.011
50. McCann W, Murphy KR, Zeiger RS, et al. Assessing meaningful change in the Asthma Impairment and Risk Questionnaire. Ann Allergy Asthma Immunol. 2024;133(2):152–158. doi:10.1016/j.anai.2024.02.013
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.