Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Skin Cancer Among Patients at a Major University Hospital in Saudi Arabia: A Retrospective, Single-Center Study
Authors Madkhali AM, Almarshoud GA ![]() , Alsanad LF, Alomar RO
, Alsanad LF, Alomar RO ![]() , Zawawi AA, Alrsheed SF, Alaidarous SR
, Zawawi AA, Alrsheed SF, Alaidarous SR ![]() , Alraddadi B, Almalki BB, Madani A
, Alraddadi B, Almalki BB, Madani A
Received 27 October 2025
Accepted for publication 22 January 2026
Published 10 February 2026 Volume 2026:19 576983
DOI https://doi.org/10.2147/CCID.S576983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jeffrey Weinberg
Abdossalam M Madkhali,1 Ghaida A Almarshoud,2 Layan F Alsanad,2 Rima Omar Alomar,2 Alia A Zawawi,2 Saud F Alrsheed,2 Sarah R Alaidarous,2 Bushra Alraddadi,3,4 Basel Bandar Almalki,4 Abdulaziz Madani4
1Department of Medicine, Oncology, Hematology and Radiation Oncology Unit, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2College of Medicine, King Saud University, Riyadh, Saudi Arabia; 3Department of Dermatology, Ohud Hospital, Ministry of Health, Madina, Saudi Arabia; 4Department of Dermatology, College of Medicine, King Saud University, Riyadh, Saudi Arabia
Correspondence: Abdossalam M Madkhali, Email [email protected]
Background: Skin cancer has two major types: melanoma and non-melanoma skin cancer. Melanoma is less prevalent than non-melanoma skin cancers but remains clinically significant due to its aggressive biological behavior. Numerous factors might increase an individual’s possibility of developing skin cancer. In addition to not being common, there are regional variations in the prevalence of skin cancer within Saudi Arabia.
Purpose: This study was conducted to describe the frequency, distribution, and clinical presentation of melanoma and non-melanoma skin cancers among university hospital patients in Saudi Arabia.
Methods: This retrospective study targeted adult patients diagnosed with any type of skin cancer at a major university hospital between 2016 and 2023. Data were collected from electronic medical records and then analyzed.
Results: A total of 91 patients diagnosed with skin cancer were included. Among them, 87 patients (95.6%) had primary skin cancer while 4 were recurrent. Non-melanoma basal cell carcinoma was the most prevalent subtype, affecting 49 patients (53.8%), followed by squamous cell carcinoma in 31 patients (34.1%). Most skin cancer cases (67%) were located on the head or face. Twenty-six patients (29%) presented to the hospital 36 months after the initial appearance of the lesion.
Conclusion: This study provides valuable information about the clinical outcomes of skin cancer, highlighting that non-melanoma basal cell carcinoma was the most common type. It also indicates that many patients delay seeking medical advice, emphasizing the importance of raising public awareness regarding skin cancer prevention and early recognition to reduce morbidity and mortality.
Keywords: skin cancer, cancer epidemiology, skin cancer screening
Introduction
Skin cancer has two major types: melanoma and non-melanoma skin cancer (NMSC). Melanoma skin cancer starts in the melanocytes, which are the cells that produce pigment, giving skin its color. NMSC includes basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), which are derived from epidermal cells and demonstrate common epidemiology, such as a high prevalence in White populations.1,2 Melanoma is less common than BCC and SCC, which are the most prevalent types.1 Although melanoma is less prevalent, it is known to be more aggressive and to have a higher death rate. Numerous factors, including lifestyle choices, exposure to ultraviolet (UV) radiation, and genetics, might increase an individual’s possibility of developing skin cancer. Although melanoma is more evenly distributed between genders, age and gender remain substantial risk factors, with men more likely than women to develop NMSC.1,3
There are regional variations in the prevalence of skin cancer in Saudi Arabia. According to a study conducted at King Khalid University Hospital in Riyadh, Saudi Arabia, between 2007 and 2018, NMSC, which includes SCC and BCC, accounted for the majority of skin cancer cases. In contrast, melanoma represented only 4.4% of such cases. Furthermore, melanoma was more commonly detected in the lower limbs, whereas NMSC most commonly manifested in the head and neck. The majority of patients were men. The study also revealed that the highest rate of metastasis was seen in melanoma, whereas metastatic spread is rare in both BCC and SCC, it occurs more frequently in SCC than in BCC.1
Additional research conducted in Saudi Arabia’s Aseer region and Taif City showed a marked increase in the number of skin cancer cases over the years; the incidence increased substantially from 1.6% in 2011 to 11.6% in 2017. The most frequently reported forms were SCC, with 230 cases (41.1%), and BCC, with 147 cases (26.3%).4 In addition, very few cases of melanoma were observed in Taif City, with SCC and BCC once again being the most common.3
Increased UV exposure, changes in lifestyle, or improvements in diagnostic methods could all be contributing factors to the increasing number of diagnosed cases, along with a better understanding of the disease and more accurate diagnosis. Understanding these changes and creating efficient preventive strategies requires ongoing research and surveillance. Moreover, addressing this issue may require public health initiatives that emphasize skin cancer awareness and sun protection.5
Worldwide, the incidence of skin cancer is consistently increasing, as demonstrated by a 33% rise in incidence between 2007 and 2017.6 Additionally, NMSC incidence has been noticeably increasing, reaching a 10% rise annually, with an estimated 2–3 million new cases globally each year.7 Although the prevalence of NMSC differs considerably worldwide, studies have shown it to be highest in White populations, with more than one million new cases reported annually.1 NMSC is particularly prevalent in White populations, with the highest rates in regions closer to the equator with high sun exposure, such as Australia, and lower rates in darker-skinned populations and regions with less sun exposure, such as parts of Africa.7,8
Most countries do not have cancer incidence rates specifically for NMSCs, but data from Poland revealed that 13,913 NMSCs occurred in 10,083 patients between 1999 and 2019, with 23% of patients having multiple NMSCs. The study also showed that BCC and SCC accounted for 99% of all NMSCs.9 Moreover, in the UK, a study conducted in 2011 reported 102,000 newly diagnosed NMSC cases, with BCCs accounting for 75%.10 Additionally, the incidence of melanoma in the US rose from 7.9 per 100,000 in 1975 to 25.3 per 100,000 in 2018, representing an increase of over 320%.11 However, as the vast majority of Saudi Arabians are not white, the risks are lower than in the mentioned studies, but they still require a deeper understanding.
In summary, NMSC and melanoma pose a major health risk both locally and globally. Therefore, since it is anticipated that the disease burden will increase, it is important to develop strategies to address this growing public health concern.12 This study thus aims to further enhance the assessment of skin cancer cases documented in a major West Asia university hospital between 2016 and 2023 to provide a more comprehensive understanding of the disease. Despite the descriptive nature of this study, updated institution-specific epidemiological data remain essential for understanding temporal patterns, clinical presentation, and healthcare utilization in populations with historically low reported incidence of skin cancer.
Material and Methods
This is a retrospective study approved by the Institutional Review Board at King Saud University (IRB No. E-24-8753), ensuring all ethical standards were followed during the research process. Informed consent to use data for research was obtained from all patients or legal guardians, allowing us to publish information as appropriate in accordance with the policies and procedures of the institution and local regulations. The study was conducted in accordance with the ethical guidelines of the Declaration of Helsinki. The study was conducted at a university hospital, a tertiary hospital in West Asia, utilizing data from adult patients diagnosed with BCC, SCC, or melanoma between 2016 and 2023. We identified the study cohort using the tumor database at the Research Unit of the Oncology Center at the hospital. The target population consisted of all adult patients aged 14 years and older; in accordance with institutional clinical and administrative guidelines whereby individuals aged 14 years and older are managed within adult medical services rather than pediatric care, who were diagnosed with any of the previously mentioned types of skin cancer at the hospital. Patients diagnosed with skin cancer before 2016 or pediatric and adolescent patients below the age of 14 were excluded from the study. The present analysis focused exclusively on basal cell carcinoma (BCC), squamous cell carcinoma (SCC), and malignant melanoma, as these represent the most consistently diagnosed and histopathologically confirmed primary skin cancers recorded in the institutional tumor registry during the study period.
Given the retrospective nature of the study, no formal sample size calculation was required. Instead, a comprehensive sampling approach was employed, including all eligible patients who met the inclusion criteria. This purposive sampling technique ensured that the study population was representative of BCC, SCC, and melanoma cases within the specified time frame. Data were obtained from the hospital’s electronic medical records, including histopathological and clinical information, to provide a detailed analysis of each case.
The data collected focused on several key variables. Demographic information included date of birth (age), sex, and nationality. Information related to the nature of the skin cancer lesions was also collected, including lesion type, size, anatomical site, borders, depth, and the presence of lymphovascular invasion.
Tumor size was measured according to the World Health Organization criteria, using the two-dimensional measurement method that involves multiplying the longest diameter by its perpendicular diameter.13
These factors are important in understanding the characteristics of skin cancer cases and determining possible prognostic factors. Moreover, various risk factors, such as a history of previous skin cancer, exposure to radiation, prolonged sunlight exposure, use of immunosuppressive medications, the presence of metastasis, family history of skin cancer, and smoking history, were noted when sufficient information was available.
Other important variables assessed included the pathological diagnosis of the cancer, clinical presentation of the patients, survivorship status, and recurrence of cancer following treatment, if applicable. These additional variables provided valuable insights into the overall outcomes and prognoses of the patients.
The data were aggregated using a secure online data collection form with industry-standard encryption. To maintain confidentiality, personal information was anonymized. No patient data were downloaded or shared outside the research team, and strict protocols were followed to ensure data privacy in compliance with ethical standards.
Statistical Analysis
The data were retrieved from medical records and entered into a secure, digital spread sheet. For statistical analysis, Statistical Package for the Social Sciences version 26.0 (IBM Inc., Chicago, IL, USA) was used to analyze the data. Descriptive analysis was performed for categorical data, which were presented as numbers and percentages. The chi-square test was used to assess overall associations between categorical variables and skin cancer type. Pairwise post hoc comparisons were not performed, and p-values represent global tests of association across categories. A P-value of <0.05 was considered statistically significant.
Results
This study included 91 patients diagnosed with skin cancer. Table 1 summarizes the demographic characteristics, indicating that 49 patients (53.8%) were aged between 66 and 85 years, with a mean (SD) age of 68.7 ± 15 years. The majority of the cohort were Saudi nationals (82.4%, 75 patients) and men (58.2%, 53 patients). The highest proportion of patients (42.9%) first presented through dermatology clinics (Figure 1). Most lesions measured between 2 and 100 mm2 (Table 2 and Figure 2). Data showed that 26 patients (29%) presented to the hospital 36 months after the initial appearance of the lesion and symptoms; this notable delay highlights a trend of late medical consultation (Figure 3).
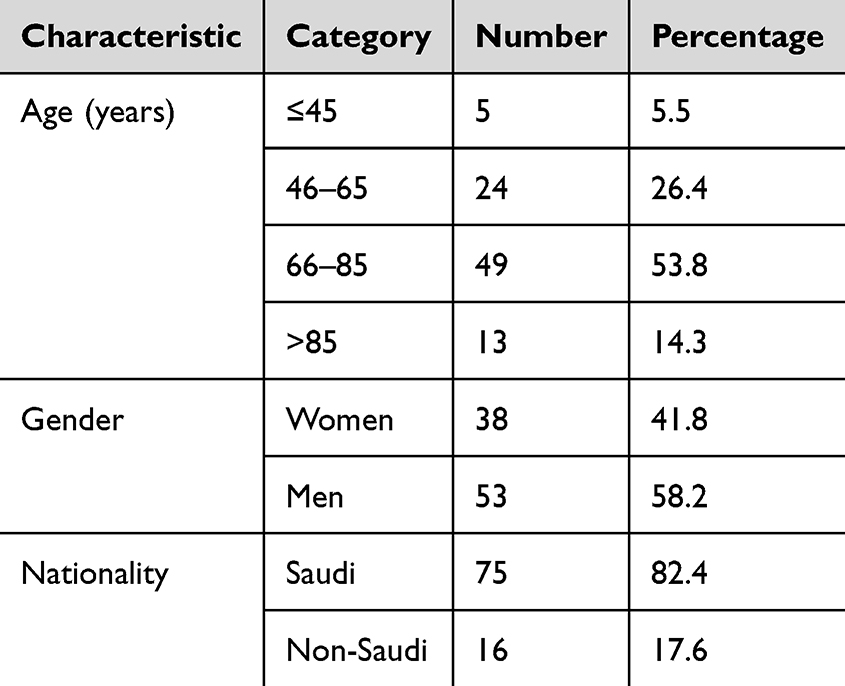 |
Table 1 Patients’ Demographics (N = 91) |
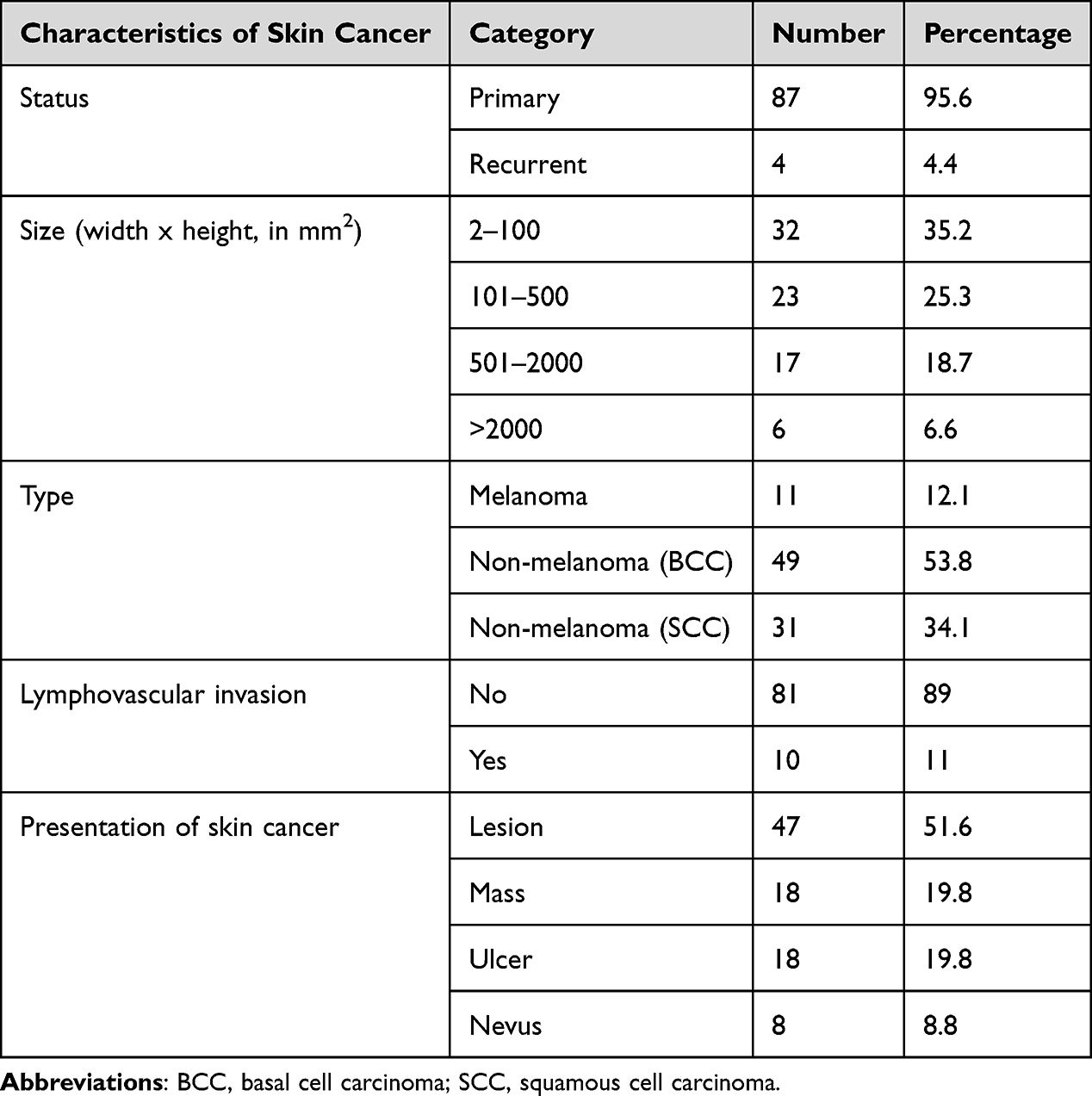 |
Table 2 Skin Cancer Characteristics Among 91 Patients |
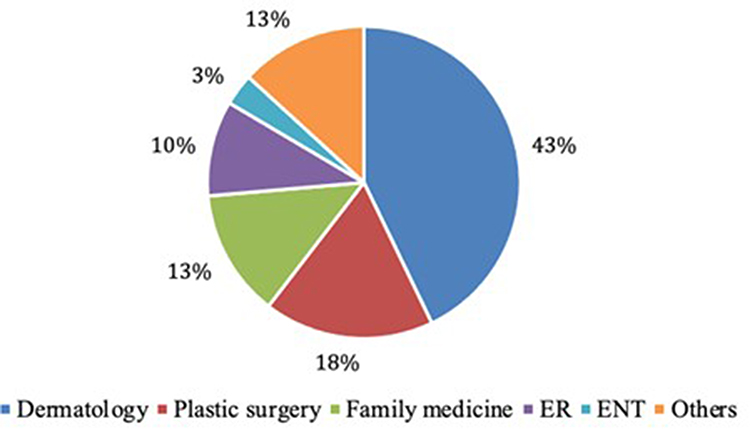 |
Figure 1 Distribution of patients with skin cancer across diagnostic clinics. |
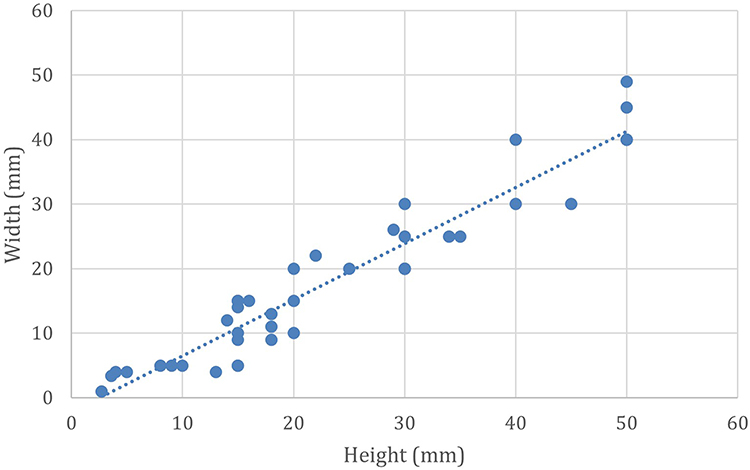 |
Figure 2 Distribution of skin lesion dimensions. |
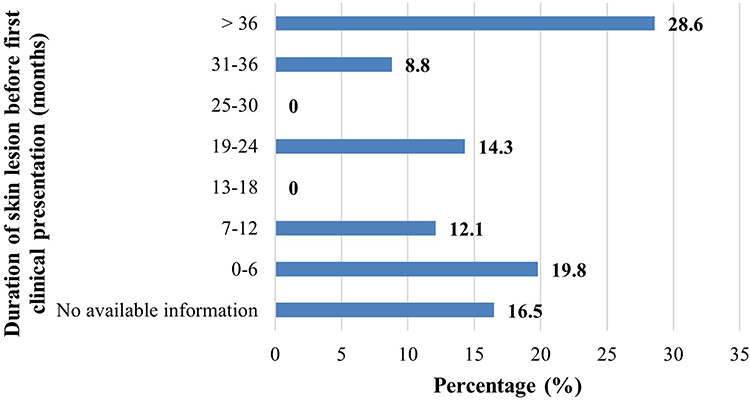 |
Figure 3 Duration of skin lesion before the first clinical presentation (months, N = 91). |
Table 2 outlines the clinical characteristics. Of the 91 patients, 87 (95.6%) had primary skin cancer. Non‑melanoma BCC was the most prevalent subtype, affecting 49 patients (53.8%), followed by non‑melanoma SCC in 31 patients (34.1%). No statistically significant associations were observed between skin cancer type and variables such as age, gender, cancer status, and presentation (Table 3).
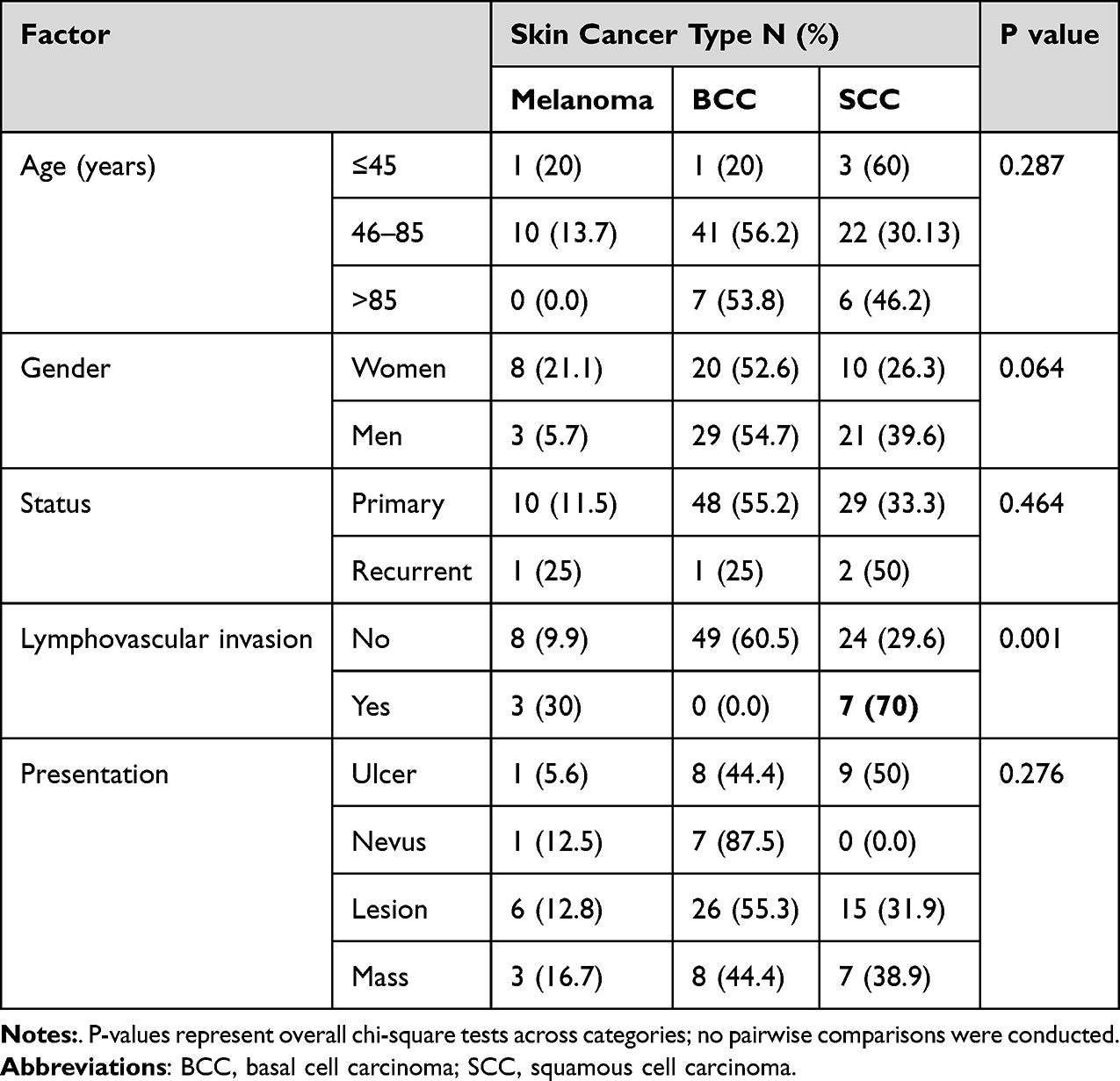 |
Table 3 Association of Patient Demographics with Skin Cancer Types |
Most skin cancer cases were located on the head or face (67%), with 51.7% occurring on the right side of the body (Figure 4). The highest proportion of patients (35.2%) had tumor sizes ranging from 2 to 100 mm2. Lesion-type skin-cancer presentation was the most common, affecting 47 patients (51.6%).
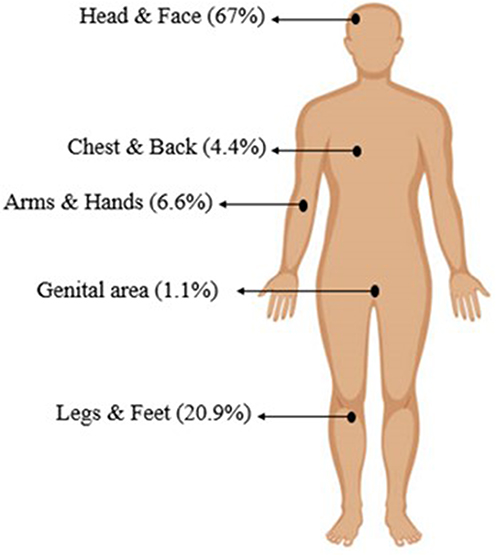 |
Figure 4 Site of skin cancer. |
Figure 5 depicts the temporal distribution of skin cancer cases at the hospital between 2016 and 2023. The highest proportion of diagnosed cases was recorded in 2016 (19.8%), whereas 2023 exhibited the lowest number of diagnoses (5.5%).
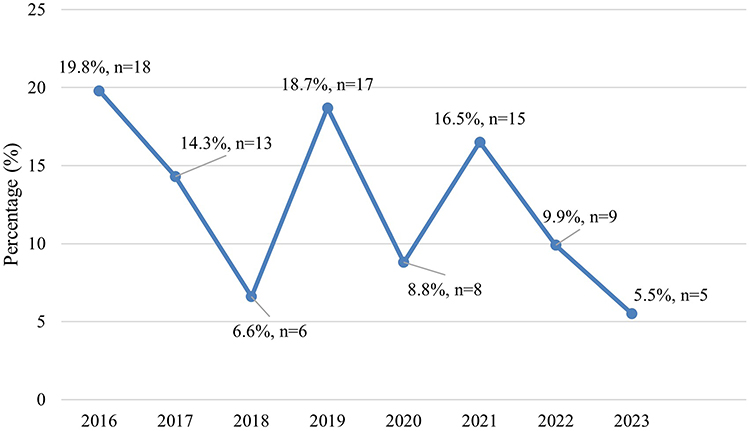 |
Figure 5 Distribution of the reported skin cancer from 2016 to 2023 in the Hospital. |
Among the 91 patients, 80 (87.9%) underwent therapeutic interventions, including surgery, radiation therapy, chemotherapy, or immunotherapy. The most common intervention was surgery, performed on 59 patients (64.8%). Following treatment, 22 patients (24.2%) experienced recurrence or progression, while four patients (4.4%) were referred to a palliative medicine specialist.
Discussion
Recently, skin cancer has been characterized by an increasing pattern worldwide as a result of heavy exposure to harmful UV radiation, exacerbated by ozone layer depletion.14 In Saudi Arabia, patients with skin cancer suffer an increasing risk of morbidity and mortality, mainly due to late reporting.15 Previous studies, such as those by Arab et al, documented the prevalence of melanoma skin cancer and NMSC over the period 2007–2018, revealing that BCC was the most common type of cancer reported at King Khalid University Hospital.1
While the observed patterns are consistent with international and regional reports, this agreement reinforces the external validity of the findings while providing updated insight from a Saudi tertiary academic center over a recent seven-year period. Such confirmatory data are particularly valuable in regions with historically low reported incidence and limited longitudinal datasets. The strength of this study lies in its focus on a population with a comparatively low incidence of skin cancer, a context that remains underrepresented in the dermatologic literature. Reporting epidemiological patterns from such settings is important for benchmarking disease burden and informing region-specific public health strategies.
Although the present study focused on BCC, SCC, and malignant melanoma, other cutaneous malignancies and precursor lesions such as cutaneous T-cell lymphoma (CTCL), Merkel cell carcinoma, and keratoacanthoma are recognized entities within dermatologic oncology. These conditions differ substantially in pathogenesis, clinical behavior, and management strategies. Including these rare entities would introduce substantial clinical and biological heterogeneity, while contributing very small numbers of cases. The present study aimed to assess the patterns and presentation among patients with skin cancer in the university hospital of interest from 2016 to 2023, building on the previous study. The study found that BCC was the most prevalent skin cancer type, accounting for 53.8% of the 91 patients diagnosed at the hospital. This result aligns with previous studies conducted in Saudi Arabia, such as that by Almaghrabi et al, who reported that 41% of cases from 1990 to 2003 in the Southwestern region of Saudi Arabia were BCC.16 Similarly, Almalki et al found that 39.5% of cases from 1987 to 2016 in the Western region of Saudi Arabia were BCC.17 Algarni et al, who conducted a similar study in the Aseer region, demonstrated that the majority of patients with skin cancer were men aged 61–80 years, consistent with our findings. However, their study found SCC to be the most common type of skin cancer (41.1%),4 which differs from our finding that this type was the second most common (31.9%).
The lesion-type skin cancer presentation was the most common among our included patients. It is worth noting that 29% of the patients waited more than 36 months between the onset of symptoms and seeking a medical opinion, which was longer than that reported by Han et al17 (12 months) but shorter than that reported by Chang et al18 (42 months). The prolonged delay observed in a subset of patients, with nearly one-third presenting more than 36 months after initial lesion appearance, may reflect multiple factors, including limited public awareness of early skin cancer signs, perceived benignity of slowly growing lesions, and delays in accessing specialized dermatologic care. While these explanations remain speculative due to the retrospective design, similar delays have been reported in regional and international studies and highlight the importance of targeted public education and early detection initiatives, and the development of more rapid and accurate diagnostic methods.
The face receives the greatest cumulative UV radiation throughout the day, making it the most common site for skin cancer, particularly BCC.19 This aligns with our findings, as 67% of the skin cancer cases were located on the head and face areas. These results are consistent with other studies,20 emphasizing the importance of protective measures against UV exposure. The higher proportion of male patients observed in this study may be partially explained by greater occupational and recreational outdoor exposure, resulting in increased cumulative ultraviolet radiation.
Our findings showed that most patients (N = 59, 64.8%) underwent surgical intervention, and a substantial proportion achieved a good prognosis with no recurrence or progression (N = 69, 75.8%). Surgical excision is considered the cornerstone and first-line therapy for skin cancer, specifically BCC and SCC, and is associated with high success rates.21
Excision was the most performed type of surgery (30.8%). Moreover, one study found that low recurrence rates (less than 5%) were linked to surgical excision, whereas radiotherapy showed a higher recurrence rate of 7.3%.22
Surgical excision was the predominant therapeutic modality in this cohort. Due to the retrospective nature of the study and variability in operative documentation, detailed surgical techniques—such as the use of Mohs micrographic surgery or frozen section margin assessment—were not uniformly recorded and could not be systematically analyzed. As such, treatment outcomes were evaluated based on the overall use of surgical intervention rather than technique-specific approaches.
Additionally, SCC is well documented to have a significant metastatic or invasion rate of 3.7%,23 which aligns with our study, as the lymphovascular invasion was significantly (P = 0.001) more prevalent in SCC compared with other types; however, due to the small number of cases, this may not be fully informative.
Although less prevalent, melanoma remains the deadliest form of skin cancer, accounting for 80% of skin cancer-related mortality.24 However, other studies, such as that by Zhong et al, reported lower mortality rates of 4%.25 Watts et al highlighted that routine skin examinations for melanomas were linked to considerably decreased mortality rates, emphasizing the need for implementing screening programs for early skin cancer detection.26
The observed differences in clinical behavior among BCC, SCC, and melanoma reflect well-established biological distinctions. BCC is characterized by slow growth and a very low metastatic potential, whereas SCC demonstrates a higher propensity for local invasion and metastasis, particularly in high-risk lesions. Malignant melanoma, although less prevalent, is biologically aggressive and associated with the highest rates of distant metastasis and mortality. These intrinsic differences help contextualize the patterns of lymphovascular invasion and clinical outcomes observed in the present cohort.
This study has several limitations. Its retrospective and single-center design limits generalizability, and missing data restricted the assessment of some clinical and pathological variables. Additionally, the relatively small sample size precluded robust subgroup analyses or the identification of independent predictors related to tumor subtype, anatomical site, size, or biological behavior. Consequently, the findings should be interpreted as descriptive rather than predictive. Future multicenter studies with larger cohorts are warranted to explore risk factors and prognostic determinants of skin cancer subtypes in the local population. While the study was not designed to identify causal risk factors, it provides an updated epidemiological overview of skin cancer patterns and clinical outcomes within a major Saudi tertiary care center, forming a foundation for future analytical and multicenter investigations.
Conclusion
This study provides valuable information on the patterns and clinical outcomes of skin cancer. It found that the most common type of skin cancer was NMSC (SCC and BCC), and that the condition was most prevalent in populations older than 65 years. These findings contribute updated epidemiological evidence that may inform institutional planning, public health awareness initiatives, and the design of future multicenter studies in similar populations. In agreement with international practice, surgery remains the most effective therapeutic intervention. As some cases of skin cancer are preventable, it is essential to raise public awareness regarding its epidemiology, preventive measures, and early recognition to facilitate timely treatment and reduce morbidity and mortality rates.
Data Sharing Statement
Anonymized data are available upon request from the corresponding author.
Funding
This research did not receive any external funding.
Disclosure
The authors declare that there is no conflict of interest in this work.
References
1. Arab KA, AlRuhaili A, AlJohany T, AlHammad RS. Melanoma and non-melanoma skin cancer among patients who attended King Khalid University Hospital in Riyadh, Saudi Arabia, from 2007 to 2018. Saudi Med J. 2020;41(7):709. doi:10.15537/smj.2020.7.25138
2. Cives M, Mannavola F, Lospalluti L, et al. Non-melanoma skin cancers: biological and clinical features. Int J Mol Sci. 2020;21(15):5394. doi:10.3390/ijms21155394
3. AlOtaibi MN, Basfar AS, Jawhari AM, et al. The burden of skin cancers in Saudi Arabia through 2011 to 2022. Cureus. 2023;15(9).
4. Algarni AM, Alshehri HS, Al Zomia AS, et al. The epidemiological pattern of skin cancer from 2011 to 2022 among the population of the Aseer region, Kingdom of Saudi Arabia. Cancers. 2023;15(18):4612. doi:10.3390/cancers15184612
5. Kornek T, Augustin M. Skin cancer prevention. J Dtsch Dermatol Ges. 2013;11(4):283–10. doi:10.1111/ddg.12066
6. Ciuciulete AR, Stepan AE, Andreiana BC, Simionescu CE. Non-melanoma skin cancer: statistical associations between clinical parameters. Curr Health Sci J. 2022;48(1):110–115. doi:10.12865/CHSJ.48.01.16
7. Samarasinghe V, Madan V. Non-melanoma skin cancer. J Cutan Aesthet Surg. 2012;5(1):3–10. doi:10.4103/0974-2077.94323
8. Lomas AL, Leonardi-Bee J, Bath‐Hextall F. A systematic review of worldwide incidence of non-melanoma skin cancer. Br J Dermatol. 2012;166(5):1069–1080. doi:10.1111/j.1365-2133.2012.10830.x
9. Pabianek M, Szczepaniak K, Hankiewicz A, Ułanska M. The incidence and clinical analysis of non-melanoma skin cancer. Sci Rep. 2021;11(1):4337. doi:10.1038/s41598-021-83502-8
10. Griffin LL, Ali FR, Lear JT. Non-melanoma skin cancer. Clin Med. 2016;16(1):62–65. doi:10.7861/clinmedicine.16-1-62
11. Saginala K, Barsouk A, Aluru JS, Rawla P. Epidemiology of melanoma. Med Sci. 2021;9(4):63. doi:10.3390/medsci9040063
12. Hu W, Fang L, Ni R, Zhang H, Pan G. Changing trends in the disease burden of non-melanoma skin cancer globally from 1990 to 2019 and its predicted level in 25 years. BMC Cancer. 2022;22(1):836. doi:10.1186/s12885-022-09940-3
13. Subbiah V, Chuang HH, Gambhire D, Kairemo K. Defining clinical response criteria and early response criteria for precision oncology: current state-of-the-art and future perspectives. Diagnostics. 2017;7(1):10. doi:10.3390/diagnostics7010010
14. Murphy M, Mabruk MJ, Lenane P, et al. Comparison of the expression of p53, p21, bax, and the induction of apoptosis between patients with basal cell carcinoma and normal controls in response to ultraviolet irradiation. J Clin Pathol. 2002;55(11):829–833. doi:10.1136/jcp.55.11.829
15. Al‐Dawsari NA, Amra N. Pattern of skin cancer among Saudi patients attending a tertiary care center in Dhahran, Eastern Province of Saudi Arabia: a 20‐year retrospective study. Int J Dermatol. 2016;55(12):1396–1401. doi:10.1111/ijd.13320
16. Al-Maghrabi JA, Al-Ghamdi AS, Elhakeem HA. Pattern of skin cancer in Southwestern Saudi Arabia. Saudi Med J. 2004;25(6):776–779.
17. Almalki S, Almalki AM, Allaf F, Alrougi A, Al-Marzouki AH, Farahat F. A retrospective chart review of skin cancer pattern and clinical outcomes among Saudi patients visiting a tertiary care hospital in Western Saudi Arabia from 1987–2016. Cureus. 2021;13(12).
18. Ch’ng CC, Wong SM, Lee YY. A 7-year retrospective review of skin cancer at University Malaya Medical Centre: a tertiary center experience. Malays J Dermatol. 2012;29:16–22.
19. Demirseren DD, Ceran C, Aksam B, Demirseren ME, Metin A. Basal cell carcinoma of the head and neck region: a retrospective analysis of completely excised 331 cases. J Skin Cancer. 2014;2014:858636. doi:10.1155/2014/858636
20. Unar A, Khan H, Zahid N, et al. Association of the depth of invasion with recurrence rates of basal cell carcinoma in a tertiary health care facility: a retrospective study over six years. Cureus. 2023;15(3). doi:10.7759/cureus.36276
21. Bichakjian C, Armstrong A, Baum C, et al. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540–559. doi:10.1016/j.jaad.2017.10.006
22. Smith V, Walton S. Treatment of facial basal cell carcinoma: a review. J Skin Cancer. 2011;2011:380371. doi:10.1155/2011/380371
23. Samarasinghe V, Madan V, Lear JT. Management of high-risk squamous cell carcinoma of the skin. Expert Rev Anticancer Ther. 2011;11(5):763–769. doi:10.1586/era.11.36
24. National Cancer Institute. Melanoma of the skin—cancer stat facts. National cancer institute surveillance, epidemiology, and end results program website. Available from: https://seer.cancer.gov/statfacts/html/melan.html.
25. Zhong CS, Coughlin CC, Hawryluk EB, et al. Characteristics of non-melanoma skin cancer in children without identifiable risk factors. J Am Acad Dermatol. 2021;84(5):1472–1476. doi:10.1016/j.jaad.2020.07.046
26. Watts CG, McLoughlin K, Goumas C, et al. Association between melanoma detected during routine skin checks and mortality. JAMA Dermatol. 2021;157(12):1425–1436. doi:10.1001/jamadermatol.2021.3884
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.