Back to Journals » Clinical Ophthalmology » Volume 19
Investigation of Age-Related Changes in Iris Curvature Among Japanese Participants
Authors Takagi Y ![]() , Asano R, Yamashita K, Sakai Y, Yokoyama S, Ichikawa K, Ichikawa K
, Asano R, Yamashita K, Sakai Y, Yokoyama S, Ichikawa K, Ichikawa K ![]()
Received 26 July 2025
Accepted for publication 1 December 2025
Published 8 December 2025 Volume 2025:19 Pages 4493—4503
DOI https://doi.org/10.2147/OPTH.S556391
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yuki Takagi,1,2 Ryo Asano,3,4 Kanna Yamashita,2 Yukihiro Sakai,2 Sho Yokoyama,4 Kei Ichikawa,2 Kazuo Ichikawa2
1Department of Ophthalmology, Japan Community Healthcare Organization Kanitounou Hospital, Kani, Gifu, Japan; 2Chukyo Eye Clinic, Nagoya, Aichi, Japan; 3Asano Eye Clinic, Nagoya, Aichi, Japan; 4Department of Ophthalmology, Japan Community Healthcare Organization Chukyo Hospital, Nagoya, Aichi, Japan
Correspondence: Yuki Takagi, Department of Ophthalmology, Japan Community Healthcare Organization Kanitounou Hospital, Kani, Gifu, Japan, Tel +81-574-25-3113, Fax +81-574-28-6382, Email [email protected]
Purpose: Angle-closure glaucoma is more common among Asians, including Japanese individuals, and iris curvature (I-Curv) is reportedly useful for its diagnosis. To investigate age-related changes in iris configuration and their associated factors in Japanese participants using I-Curv measured using anterior segment optical coherence tomography (AS-OCT).
Patients and Methods: A total of 480 healthy Japanese individuals aged 20– 99 years were enrolled. The anterior segment parameters of the anterior chamber, angle, and iris were measured using AS-OCT (CASIA2). The relationships between I-Curv and other parameters were assessed using Spearman’s rank correlation coefficient. Differences in the I-Curv among age groups were analyzed using the Kruskal–Wallis test, followed by pairwise comparisons with Bonferroni correction. Multiple regression analysis was performed with I-Curv as the dependent variable and age, refractive error, sex, axial length, and anterior segment parameters as the independent variables. Further, eyes were classified into concave and convex groups based on the sign of I-Curv, and clinical characteristics were compared between these groups.
Results: I-Curv tended to increase (become more anteriorly convex) with age, showing significant differences among age groups (P < 0.001). However, no significant differences were observed between the adjacent age groups. Spearman correlation revealed significant negative correlations between I-Curv and angle/anterior chamber parameters such as AOD500 and ACD, and positive correlations with LV, age, and refractive error. Multiple regression analysis identified AOD500, ARA500, LV, refractive error, age, and pupil diameter as significant factors influencing the I-Curv (R² = 0.824, P = 0.043). Compared with the convex group, the concave group was significantly younger, had greater myopia, wider anterior chambers and angles, and tended to include more males (P < 0.05).
Conclusion: The iris tended to become more anteriorly convex with increasing age, and these changes appeared to be strongly influenced by angle configuration.
Keywords: iris, iris curvature, I-Curv, anterior segment optical coherence tomography, AS-OCT
Introduction
Iris configuration, which is similar to the angle structure, is important in glaucoma management. Several studies have investigated iris configuration across various glaucoma subtypes.1–8 Among Asians, including Japanese individuals, a higher prevalence of angle-closure has been reported.9 Therefore, understanding the characteristics and age-related changes in the iris and angle structures in Asians, including Japanese populations, is important. One study comparing eyes with acute primary angle-closure (APAC) and their fellow eyes found a more linear iris configuration in the affected eyes.1 Another study comparing iris shapes among eyes with primary angle-closure suspect (PACS), primary angle-closure (PAC), and APAC reported that the iris becomes progressively more linear as the degree of angle closure advances.2 Conversely, other studies comparing iris configuration in eyes with open and closed angles reported a more convex iris shape in angle-closure eyes.3–5 Furthermore, iris configuration reportedly changes to a more convex shape following pupillary block onset.6 In contrast, a concave iris configuration has been observed in eyes with pigmentary glaucoma.7,8 In addition, some studies have reported age-related changes in iris configuration.10–12 Therefore, understanding these age-related changes may be useful for the subtype diagnosis of glaucoma. In addition to glaucoma, it has been reported that the structure of the anterior chamber angle changes after implantation of phakic intraocular lenses used for myopia correction.13 Thus, clarifying the age-related changes in these structures may also help determine the optimal lens size and have potential applications in other clinical fields.
Although slit-lamp examination and gonioscopy are useful for assessing iris configuration, quantitative evaluation using these methods is challenging. In contrast, ultrasound biomicroscopy10,11 and anterior segment optical coherence tomography (AS-OCT)12,14 have proven to be effective for evaluating iris configuration, with AS-OCT being particularly advantageous because of its noninvasive nature.
One parameter used to assess iris configuration with AS-OCT is iris curvature (I-Curv; Figure 1), which quantifies the degree of iris bowing. I-Curv is defined as the maximum perpendicular distance from a straight line connecting the iris root to the point of lens contact measured at the posterior surface of the iris pigment epithelium. I-Curv can be calculated automatically based on the AS-OCT device. Several studies have demonstrated the usefulness of the I-curve in evaluating iris morphology and assessing the risk of angle closure.1–5 Therefore, I-Curv may be helpful for classifying glaucoma subtypes. However, understanding age-related changes in iris configuration is essential for effective clinical application.
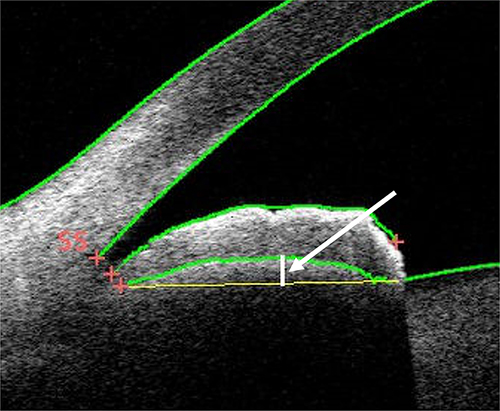 |
Figure 1 Location of I-Curv. I-Curv is defined as the maximum perpendicular distance (white arrow) from a straight line connecting the iris root to the point of contact with the lens measured at the posterior surface of the iris pigment epithelium. SS represents the position of the scleral spur. |
Although a previous study12 examined iris curvature, the data were obtained from a non-Japanese population and data specific to the Japanese population are currently unavailable. In that study, the I-Curv was manually calculated from images acquired using an AS-OCT device (3D OCT-200, Topcon, Japan). Therefore, no studies in Japan have examined age-related trends in iris configuration using automatically measured I-Curv via CASIA2 (TOMEY, Japan), nor have they investigated the factors influencing iris configuration in a Japanese population. Thus, this study aimed to evaluate age-related changes in iris configuration among Japanese participants and explore the influence of refractive error, age, sex, and anterior segment parameters measured by AS-OCT.
Materials and Methods
Participants
Participants included Japanese individuals aged 20–99 years with no history of refractive surgery, intraocular surgery, retinal detachment repair, or corneal shape abnormalities, such as keratoconus, and who had undergone AS-OCT imaging. For each decade of age, data from 60 cases were retrospectively extracted from medical records. The right eye was primarily selected for analysis; however, if the right eye met any exclusion criteria, the left eye was used instead.
AS-OCT imaging using CASIA2 was performed under dark-room conditions without pharmacologic dilation. The scleral spur and iris root positions were visually inspected and manually adjusted by a single examiner for all the images. The following parameters (Figure 2) were measured: anterior chamber parameters (anterior chamber depth [ACD], anterior chamber area [ACA], lens vault [LV], anterior chamber width [ACW]); angle parameters (angle opening distance at 500 μm [AOD500], angle recess area at 500 μm [ARA500], trabecular–iris space area at 500 μm [TISA500], and trabecular–iris angle at 500 μm [TIA500]); iris parameters (I-Curv, iris thickness at 750 and 2000 μm [IT750 and IT2000], and iris area [I-Area]); and pupil diameter. All angle and iris parameters were analyzed based on the nasal quadrant. The axial length was measured using an IOL Master 700 (Carl Zeiss Meditec, Jena, Germany).
 |
Figure 2 This image illustrates the parameters of the anterior chamber, angle, and iris. IR: iris root; AR: angle recess; SS: scleral spur, Angle open distance (AOD) 500: Distance from the scleral spur to the point where a perpendicular line drawn from the corneal endothelium at 500 μm intersects the iris, Angle recess area (ARA) 500: The cross-sectional area formed by the perpendicular line from the corneal endothelium 500 μm from SS to the iris and the anterior surface of the iris, Trabecular iris space area (TISA) 500: defined as the area of ARA500 minus the area bordered by a line from the scleral spur (SS) to the iris, the anterior iris surface, and the corneal endothelium, Trabecular iris angle (TIA500): the angle formed by two lines drawn from the AR to the two points on the corneal endothelium and the anterior iris surface defined by AOD500, Anterior chamber depth (ACD): the distance from the corneal endothelium to the anterior surface of the lens, Lens vault (LV): the perpendicular distance from the line connecting both SS points to the anterior surface of the lens, I-Area: the cross-sectional area of the iris. Iris thickness (IT500/2000): the thickness of the iris measured at the points where perpendicular lines drawn from the corneal endothelium at 500 μm and 2000 μm from the SS intersect the iris. |
This study was conducted as a retrospective analysis of the examination data extracted from electronic medical records. The study protocol was approved by the Institutional Review Board of Chukyo Eye Clinic (approval number: 20240701083). Informed consent was obtained using the opt-out method and the study was conducted in accordance with the Declaration of Helsinki.
Statistical Analysis
The normality of I-Curv and other AS-OCT parameters, as well as age, refractive error, pupil diameter, and axial length, was assessed using the Shapiro–Wilk test. Correlations between I-Curv, representing iris configuration, and AS-OCT parameters, age, refractive error, pupil diameter, and axial length, were assessed using Spearman’s rank correlation coefficient. I-Curv differences across age groups were analyzed using the Kruskal–Wallis test, followed by Bonferroni-corrected pairwise comparisons when significant differences were identified. Furthermore, multiple regression analysis using the stepwise method was performed with I-Curv as the dependent variable and AS-OCT parameters, age, sex (coded as 0 for females and 1 for males), refractive error, pupil diameter, and axial length as independent variables. Participants were categorized into concave (negative I-Curv; Figure 3) and convex (positive I-Curv) groups for the comparison of clinical characteristics. Fisher’s exact test was used for comparisons of categorical variables (sex), and the Mann–Whitney U-test for continuous variables. Similarly, the Mann–Whitney U-test was used to compare parameters between the male and female groups. Statistical significance was set at P < 0.05. All statistical analyses were performed using the SPSS software (Version 29.0; IBM Corp., Armonk, NY, USA).
 |
Figure 3 A case with negative I-Curv (concave iris configuration). In this anterior segment optical coherence tomography image obtained from the nasal quadrant (0°), the iris is bowed posteriorly toward the posterior chamber, demonstrating a concave configuration. SS represents the location of the scleral spur. |
An a prioripower analysis was conducted using G*Power (version 3.1.9.7). Assuming an effect size of 0.20, eight groups, a significance level (α) of 0.05, and a statistical power of 0.90, the minimum required total sample size was calculated to be approximately 472 participants (59 per group). To satisfy this requirement, we included 60 participants per age group, resulting in 480 participants.
Results
This study included 480 eyes of 480 Japanese participants (215 males and 265 females; 470 right eyes and 10 left eyes). The mean age of participants was 59.1 ± 22.5 years. The mean refractive error was −3.10 ± 4.59 diopters (D). Among the eyes, 306 (63.75%) were myopic (< −0.5 D), 78 (16.25%) were emmetropic (−0.5 D to +0.5 D), 89 (18.54%) were hyperopic (> +0.5 D), and 7 (1.46%) had missing refractive data. The mean values of other ocular parameters are presented in Table 1.
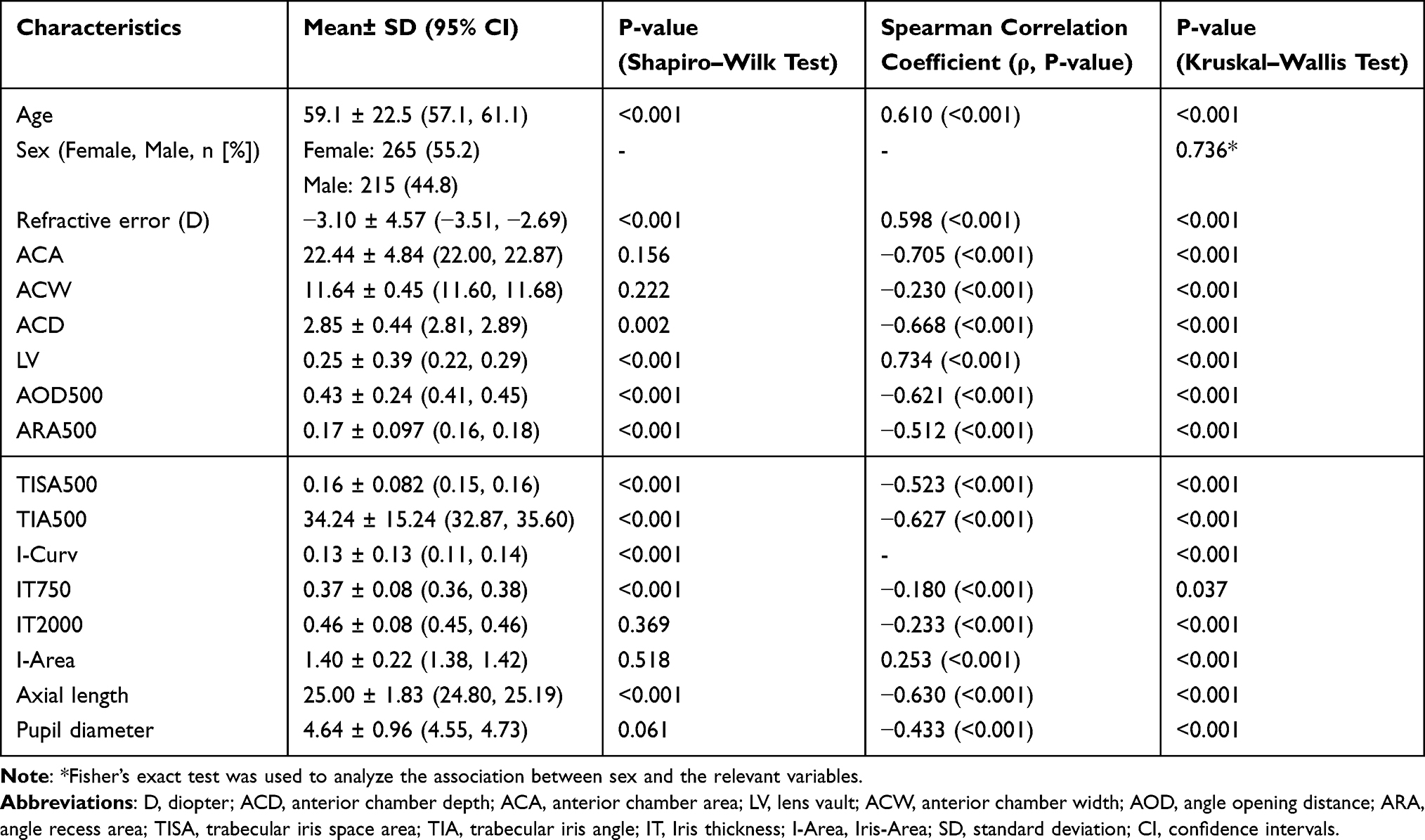 |
Table 1 Clinical Characteristics and Correlation with I-Curv |
In the assessment of normality, some parameters such as ACA and ACW showed normal distributions, whereas most parameters including I-Curv were not normally distributed. The correlations between the I-Curv and various parameters are summarized in Table 1. ARA500, TISA500, and pupil diameter showed moderate negative correlations with I-Curv (r = −0.433 to −0.523, P < 0.001), whereas AOD500, TIA500, ACA, ACD, and axial length demonstrated strong negative correlations (r = −0.621 to −0.705, P < 0.001). In contrast, age and LV exhibited strong positive correlations with I-Curv (r = 0.610 to 0.734, P < 0.001), and refractive error showed a moderate positive correlation (r = 0.598, P < 0.001).
The mean values of the I-Curv and other parameters according to age group are summarized in Table 2. Regarding I-Curv, the mean ± standard deviation for each age group was as follows: 20s, −0.01 ± 0.13; 30s, 0.04 ± 0.12; 40s, 0.08 ± 0.13; 50s, 0.13 ± 0.09; 60s, 0.12 ± 0.10; 70s, 0.19 ± 0.10; 80s, 0.24 ± 0.07; and 90s, 0.23 ± 0.09. A significant difference in the I-Curv was found among the age groups using the Kruskal–Wallis test (P < 0.001) (Figure 4). No significant differences were observed between the 20s, 30s, and 40s; 30s and 60s; 40s, 50s, and 60s; 50s and 70s; or 70s, 80s, and 90s (P > 0.05). However, all other age-group combinations showed significant differences (P < 0.05).
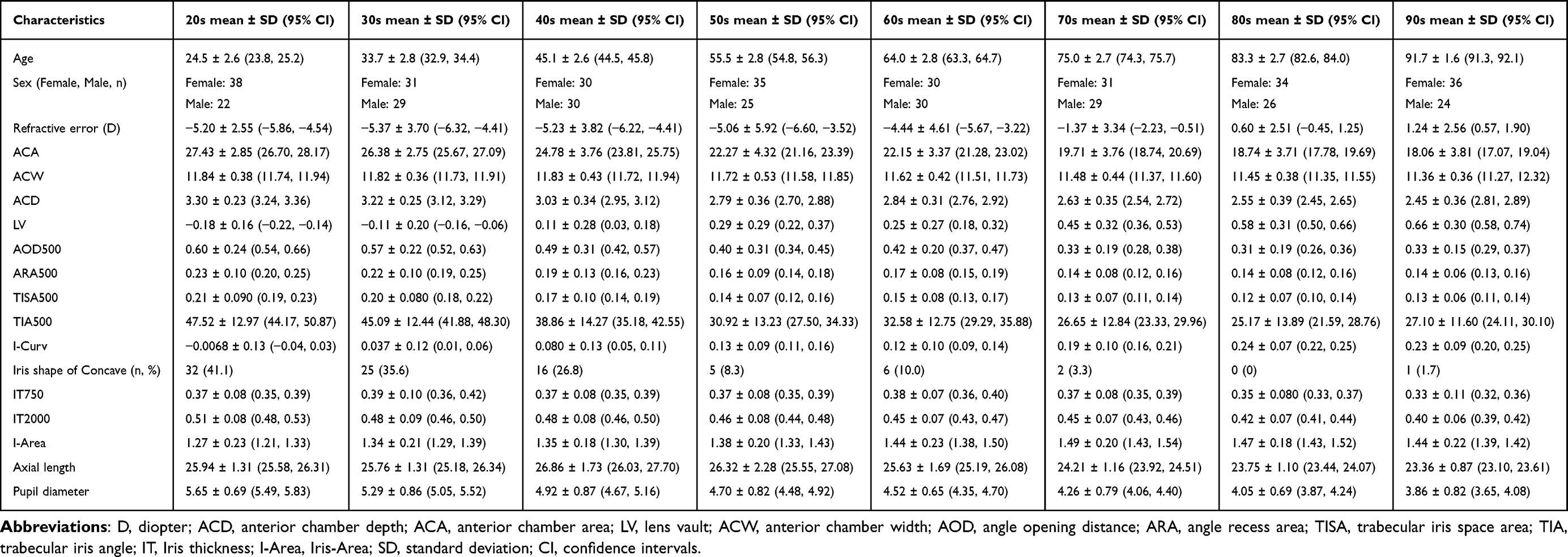 |
Table 2 Comparison of Clinical Characteristics Across Age Groups |
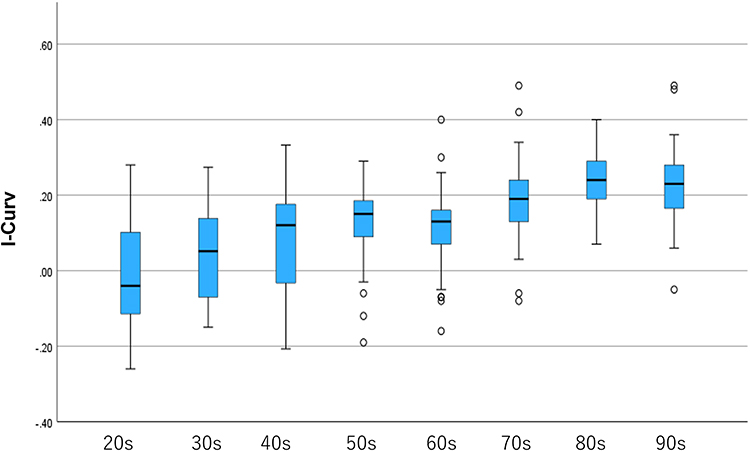 |
Figure 4 Age-related changes in I-Curv. I-Curv tends to increase with age, indicating progressive anterior bowing of the iris in older age groups. |
The results of the multiple regression analysis using the stepwise method to identify the factors influencing the I-Curv are presented in Table 3. Significant predictors included LV, AOD500, ARA500, refractive error, age, and pupil diameter (R² = 0.823, P = 0.043). As the AOD500 and ARA500 demonstrated high collinearity, we reanalyzed the multiple regression model after excluding the ARA500. The results are presented in Table 4 (R² = 0.603, P < 0.001).
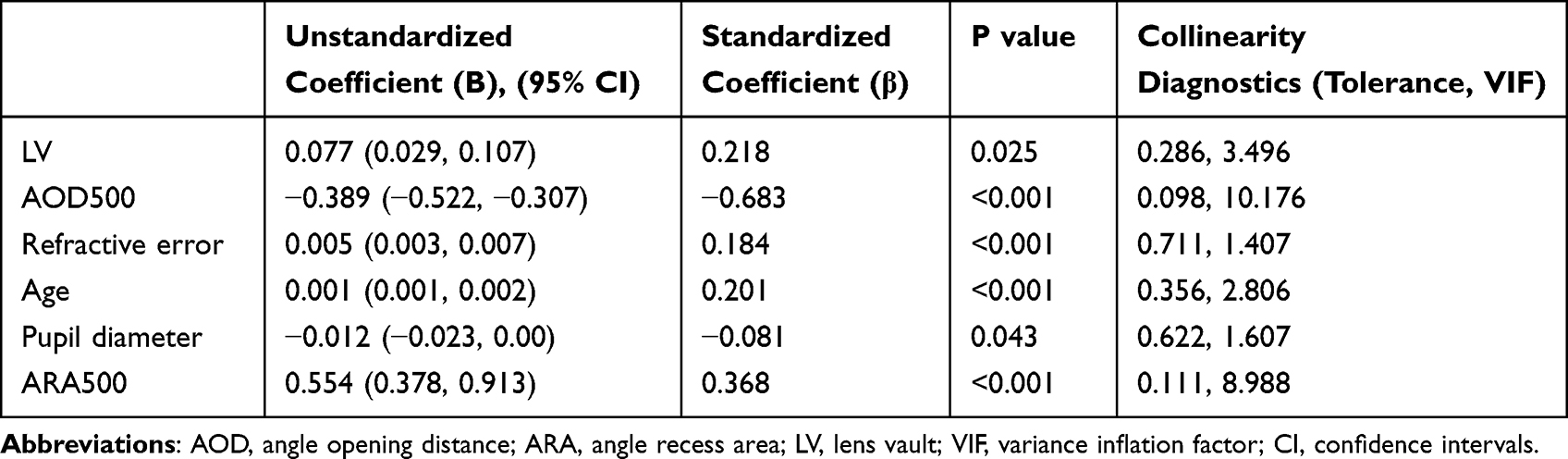 |
Table 3 Multiple Regression Analysis for Factors Associated with I-Curv |
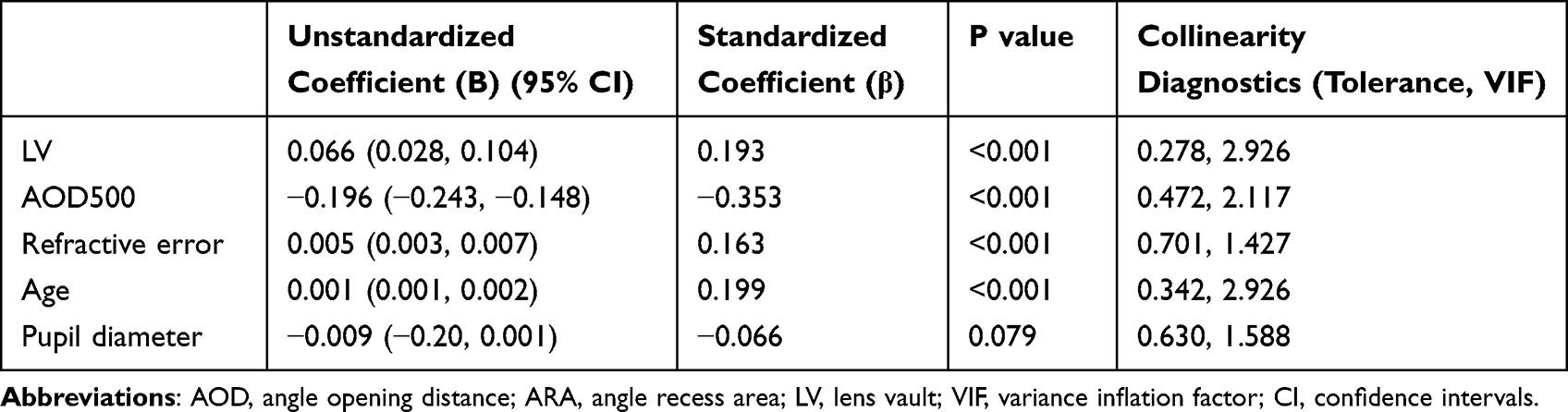 |
Table 4 Multiple Regression Analysis of Factors Associated with I-Curv After the Exclusion of ARA500 |
In the comparative analysis based on iris configuration, 87 eyes were classified as concave and 393 eyes as convex. The mean age and sex distribution were 37.3 ± 15.0 years (49 males, 38 females) in the concave group and 63.9 ± 20.9 years (166 males, 227 females) in the convex group, with significant differences observed (P < 0.001 and P = 0.017, respectively). The mean refractive errors were −6.47 ± 3.42 and −2.34 ± 4.48 D in the concave and convex groups, respectively, which also showed a significant difference (P < 0.001). Significant between-group differences were observed in angle parameters such as AOD500, as well as in ACA, ACD, ACW, axial length, and pupil diameter (P < 0.001). However, no significant differences were observed between IT750 and IT2000 (P = 0.261 and P = 0.150, respectively) (Table 5).
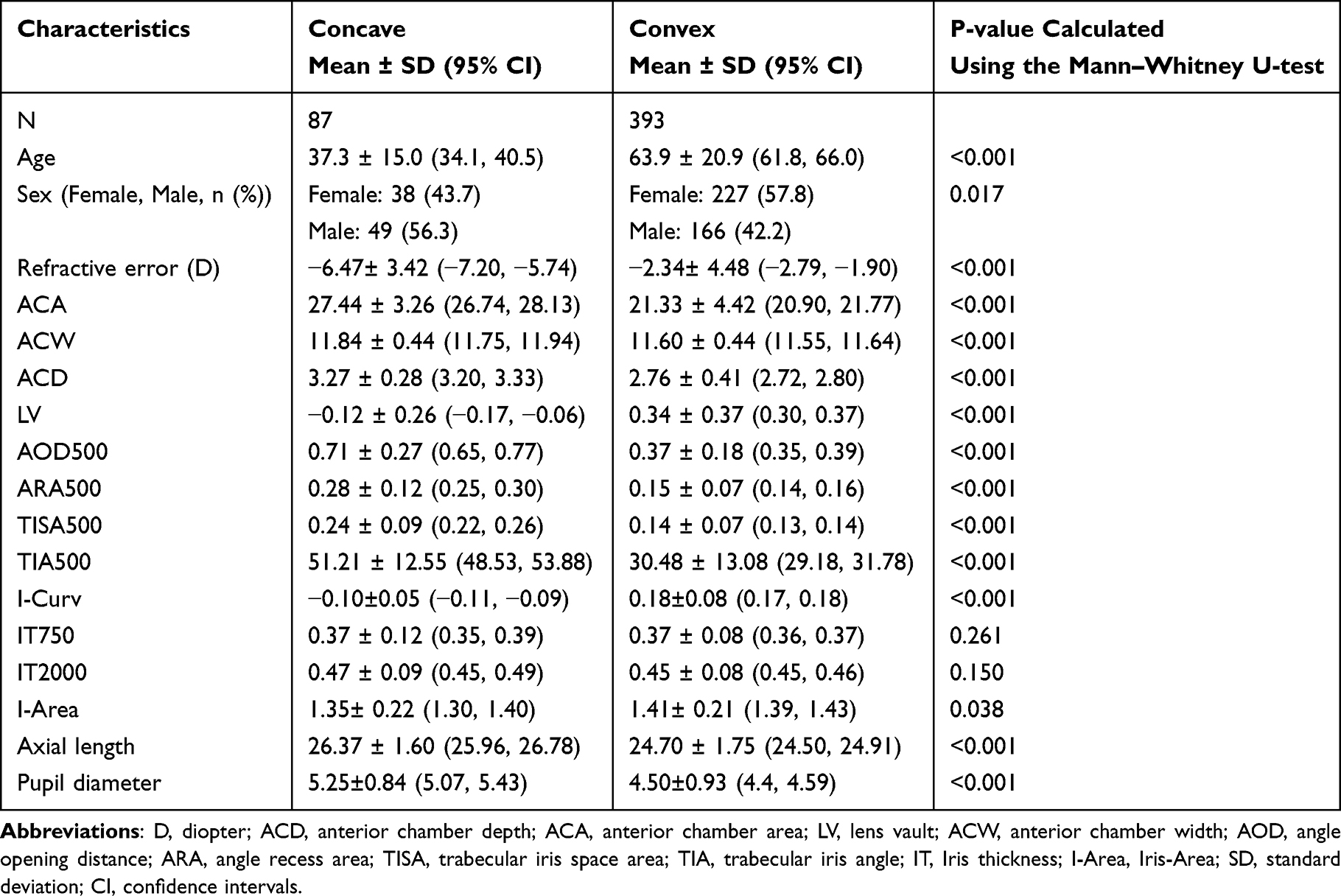 |
Table 5 Comparison Between Concave and Convex Iris Configuration Groups |
The results of sex-based comparisons are presented in Table 6. This study included 215 male and 265 female eyes. No significant differences were found in mean age (59.1 ± 21.7 years, males; 59.1 ± 23.1 years, females; P = 0.985) and mean refractive error (−2.83 ± 4.30 D, males; −3.31 ± 4.80 D, females; P = 0.345). I-Curv was 0.11 ± 0.14 in males and 0.14 ± 0.13 in females (P = 0.039), showing a significant tendency toward a more convex iris in females. Significant sex-based differences were also observed in ACA, ACD, ACW, AOD500, ARA500, TISA500, TIA500, IT750, I-Area, and axial length (P < 0.05). No significant differences were found in LV, IT2000, or pupil diameter (P > 0.05).
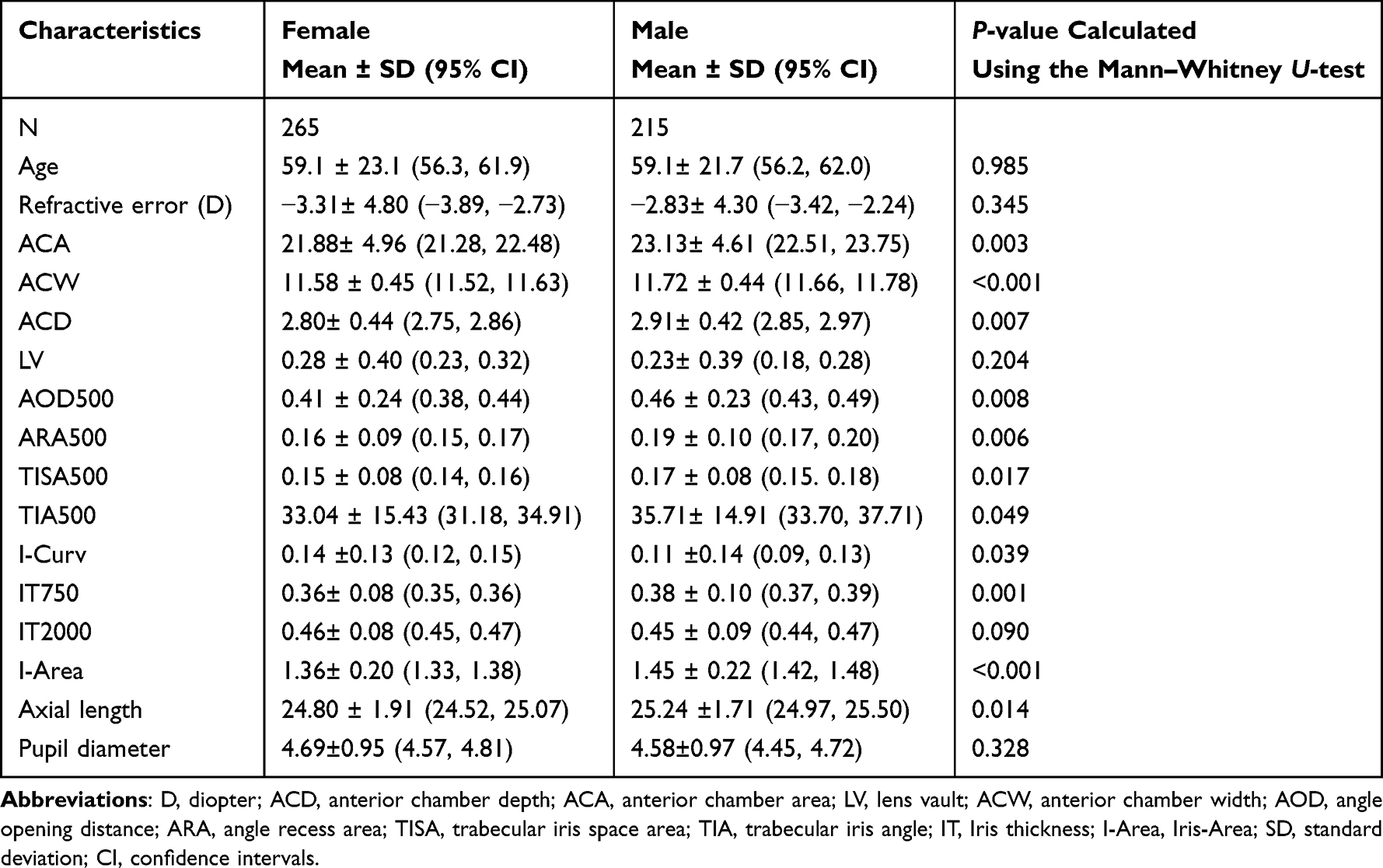 |
Table 6 Comparison Between Sex Groups |
Discussion
In this study, we investigated age-related changes in the I-Curv and its influencing factors in a Japanese population. I-Curv, which reflects anterior bowing of the iris, showed a significant tendency to increase with age, as indicated by the Kruskal–Wallis test. Pairwise comparisons between age groups revealed no significant differences among adjacent age groups, including 20s–40s, 40s–60s, and 70s–90s. However, significant differences tended to emerge between more widely separated age groups, such as between the 20s and 50s, probably because of the relatively small absolute values and gradual changes in I-Curv compared to other anterior chamber or angle parameters, which may have reduced the statistical power to detect differences between closely spaced age groups.
A study15 conducted in Korea examining age-related changes in anterior chamber parameters such as ACD and iris parameters, including I-Curv, in individuals aged 30–89 years, also reported that I-Curv tended to increase with age (indicating greater anterior bowing), which is consistent with our findings. This finding suggests that anterior bowing of the iris tends to increase with age, at least in individuals of Asian descent.
It is well established that the anterior chamber and angle narrow with age.15,16 In our study, significant age-related differences were also observed in angle parameters such as AOD500 and anterior chamber parameters, such as ACD, demonstrated a similar trend of progressive narrowing. Notably, previous studies15,16 included relatively few participants under the age of 40 and mainly focused on comparisons among older age groups. This differs from our study, which included a larger number of younger participants; however, the results were consistent. These findings suggest that even among younger individuals, the anterior chamber and angle gradually narrow with age, and the iris tends to bow anteriorly (becoming more convex), consistent with previous studies.
Based on the results of Spearman’s rank correlation analysis between the I-Curv and various parameters, eyes with a wider anterior chamber and angle, longer axial length, greater myopia, and younger age exhibited a more concave iris configuration. Consistent with our findings, a previous study12 also reported that age and refractive error influenced the iris configuration.
In the multiple regression analysis, AOD500, ARA500, LV, age, refractive error, and pupil diameter were identified as significant variables, with AOD500 showing the strongest influence on the I-Curv. However, the AOD500 and ARA500 showed high collinearity. As both parameters represent the configuration of the anterior chamber angle, this finding was considered reasonable. Therefore, we reanalyzed the data after excluding the ARA500. After exclusion, multicollinearity markedly improved (all VIF < 5), while the overall significance of the model was maintained. Even in the revised model, AOD500 remained a strong influencing factor for I-Curv, suggesting that I-Curv is highly affected by the angle structure. Although the statistical significance of pupil diameter was lost in the revised model, we retained it as a variable because previous studies have reported its association with the I-Curv.3,17
Conversely, axial length and sex were not selected as significant factors, in contrast to a previous study,12 which reported an association between sex and the iris curvature. Moreover, anterior chamber and angle structures are reportedly influenced by sex14,18 and axial length.3 Therefore, although sex and axial length may considerably influence anterior segment structures, such as ACD and AOD500, their direct impact on I-Curv itself may be limited. Furthermore, unlike previous studies, most cases in this study were myopic, regardless of sex, which may have influenced the results. Further studies including a larger number of emmetropic individuals will be necessary in future studies.
The pupil diameter was also selected as a significant factor and showed a negative association with iris curvature, indicating that larger pupil diameters are associated with a more concave iris. However, this finding contrasts with those of previous studies,3,17 which reported a positive correlation between pupil diameter and iris curvature, suggesting that larger pupils are associated with greater anterior bowing of the iris. These discrepancies may be attributed to differences in the study populations, including a smaller proportion of younger subjects, a higher proportion of female participants, and comparisons between eyes with angle closure and those with open angles in previous studies. Nevertheless, from the perspective of Poiseuille’s law, a smaller pupil diameter reduces the cross-sectional area available for aqueous humor to flow from the posterior to the anterior chamber, which could increase the resistance to aqueous flow, potentially elevating the pressure in the posterior chamber and leading to anterior bowing of the iris. Therefore, this mechanism may explain the more convex iris configuration observed in eyes with smaller pupils in our study.
In the comparison between the concave and convex groups, no significant differences were observed in IT750 and IT2000; however, all the other parameters differed significantly. The concave group was comprised of significantly younger male participants with longer axial lengths, greater degrees of myopia, and wider anterior chambers and angles. These findings are consistent with those of a previous study,12 which also reported correlations between iris configuration and age, refractive error, and sex. Although our study included a predominantly myopic population, in contrast to a previous study,12 the concave group exhibited significantly greater myopia, suggesting that greater degrees of myopia may be associated with a more concave iris configuration.
In the sex-based comparison, a significant difference in the I-Curv was observed, with female participants showing a tendency toward a more convex iris configuration. Although no significant differences were observed in age, refractive error, and LV, other anterior chamber and angle parameters showed significant differences. Male participants tended to have wider anterior chambers and angles as well as longer axial lengths. These findings are consistent with those of previous reports,14,18 which demonstrated that women have significantly narrower anterior chamber and angle parameters, such as ACD and AOD500, than men. Given that the multiple regression analysis identified the angle structure as a strong determinant of I-Curv, the narrower angle structure in females may contribute to their more convex iris configuration, despite the lack of significance in some parameters.
This study had some limitations. First, most of the included cases were myopic, which may have influenced our results. Consequently, the trends in iris configuration among emmetropic and hyperopic individuals in the Japanese population remain unclear. Future studies should include a greater number of emmetropic and hyperopic eyes for reevaluation to enable broader generalizability. Second, only nasal quadrant data were used to assess the angle parameters. In contrast, a previous study11 used temporal data, indicating methodological differences. Future investigations should include analyses that use data from all quadrants to provide a more comprehensive evaluation. Finally, this study was cross-sectional, and age-related changes were estimated by comparing the data among different age groups. However, to observe the actual changes, a longitudinal study in the same cohort would be necessary.
Conclusion
The iris tended to become increasingly anteriorly convex with increasing age, a change that appeared to be strongly influenced by alterations in angle configuration. Conversely, in younger participants with wider anterior chambers and angles, and greater degrees of myopia, the iris was more likely to exhibit a concave shape. The results of this study may serve as an indicator for the subtype diagnosis of glaucoma based on iris morphology. Furthermore, future studies involving multiple ethnic groups are warranted to clarify racial differences.
Abbreviations
APAC, Acute primary angle-closure; PACS, Primary angle-closure suspect; PAC, Primary angle-closure; ACD, Anterior chamber depth; ACA, Anterior chamber area; LV, Lens vault; ACW, Anterior chamber width; AOD, Angle opening distance; ARA, Angle recess area; TISA, Trabecular–iris space area; TIA, Trabecular–iris angle; I-Curv, Iris curvature; IV, Iris area.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol was approved by the Institutional Review Board of Chukyo Eye Clinic (approval number: 20240701083). Informed consent was obtained using the opt-out method, and the study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grants from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The author(s) declare (s) no conflict of interest.
References
1. Li X, Wang W, Huang W, et al. Difference of uveal parameters between the acute primary angle closure eyes and the fellow eyes. Eye. 2018;32(7):1174–1182. doi:10.1038/s41433-018-0056-9
2. Lee JR, Sung KR, Han S. Comparison of anterior segment parameters between the acute primary angle closure eye and the fellow eye. Invest Ophthalmol Vis Sci. 2014;55(6):3646–3650. doi:10.1167/iovs.13-13009
3. Cheung CY, Liu S, Weinreb RN, et al. Dynamic analysis of iris configuration with anterior segment optical coherence tomography. Invest Ophthalmol Vis Sci. 2010;51(8):4040–4046. doi:10.1167/iovs.09-3941
4. Guo JM, Li M, Xu XL, Zhang H, Wang JM. Anterior segment changes after pharmacologic mydriasis using Pentacam and optical coherence tomography in angle closure suspects. Int J Ophthalmol. 2015;8(5):980–984. doi:10.3980/j.issn.2222-3959.2015.05.23
5. Wang B, Sakata LM, Friedman DS, et al. Quantitative iris parameters and association with narrow angles. Ophthalmology. 2010;117(1):11–17. doi:10.1016/j.ophtha.2009.06.017
6. Wakako I, Takashi S, Namiguchi K, Mizoue S, Shiraishi A, Ohashi Y. Changes in anterior segment morphology of iris bombe before and after laser peripheral iridotomy in patients with uveitic secondary glaucoma. J Ophthalmol. 2016;2016(1):8496201. doi:10.1155/2016/8496201
7. Liebmann JM, Tello C, Chew SJ, Cohen H, Ritch R. Prevention of blinking alters iris configuration in pigment dispersion syndrome and in normal eyes. Ophthalmology. 1995;102(3):446–455. doi:10.1016/S0161-6420(95)31001-9
8. Yamashita T, Shiihara H, Terasaki H, Fujiwara K, Tanaka M, Sakamoto T. Characteristics of pigmentary glaucoma in Japanese individuals. PLoS One. 2022;17(6):e0268864. doi:10.1371/journal.pone.0268864
9. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262–267. doi:10.1136/bjo.2005.081224
10. Ochiai H, Chihara E, Chuman H, Sawada A, Akita J. Age and increased incidence of “forward bowing” of the iris in normal eyes. J Glaucoma. 1998;7(6):408–412.
11. Nonaka A, Iwawaki T, Kikuchi M, Fujihara M, Nishida A, Kurimoto Y. Quantitative evaluation of iris convexity in primary angle closure. Am J Ophthalmol. 2007;143(4):695–697.
12. Schuster AK, Fischer JE, Vossmerbaeumer U. Curvature of iris profile in spectral domain optical coherence tomography and dependency to refraction, age and pupil size - the MIPH eye&health study. Acta Ophthalmol. 2017;95(2):175–181. doi:10.1111/aos.13184
13. Elmohamady MN, Abdelghaffar W. Anterior chamber changes after implantable collamer lens implantation in high myopia using pentacam: a prospective study. Ophthalmol Ther. 2017;6(2):343–349. doi:10.1007/s40123-017-0109-3
14. Huang W, Gao X, Li X, et al. Anterior and posterior ocular biometry in healthy Chinese subjects: data based on AS-OCT and SS-OCT. PLoS One. 2015;10(3):e0121740. doi:10.1371/journal.pone.0121740
15. Hong S, Kyung RS, Yun SC, et al. Factors associated with anterior chamber narrowing with age: an optical coherence tomography study. Invest Ophthalmol Vis Sci. 2012;53(6):2607–2610. doi:10.1167/iovs.11-9359
16. Cheon MH, Sung KR, Choi EH, et al. Effect of age on anterior chamber angle configuration in Asians determined by anterior segment optical coherence tomography; clinic-based study. Acta Ophthalmol. 2010;88(6):e205–e210. doi:10.1111/j.1755-3768.2010.01960.x
17. Lee Y, Sung KY, Na JH, Sun JH. Dynamic changes in anterior segment (AS) parameters in eyes with primary angle closure (PAC) and PAC glaucoma and open-angle eyes assessed using AS optical coherence tomography. Invest Ophthalmol Vis Sci. 2012;53(2):693–697. doi:10.1167/iovs.11-8389
18. Xu L, Cao WF, Wang YX, Chen CX, Jonas JB. Anterior chamber depth and chamber angle and their associations with ocular and general parameters: the Beijing eye study. Am J Ophthalmol. 2008;145(5):929–936. doi:10.1016/j.ajo.2008.01.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.