Back to Journals » Clinical Ophthalmology » Volume 19
Expert Opinion to Optimize Clinical Outcomes of Bimatoprost Intracameral Implant Treatment
Authors Bovee C, Bacharach J, Singh IP, Swaminathan SS, Bovelle R ![]() , Lai H, Rivas M, Vera V
, Lai H, Rivas M, Vera V
Received 3 May 2025
Accepted for publication 29 September 2025
Published 31 October 2025 Volume 2025:19 Pages 4027—4042
DOI https://doi.org/10.2147/OPTH.S538141
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Patient Selection and Outcomes Following Bimatoprost Implant – Video S2 [538141]
Views: 46
Courtney Bovee,1 Jason Bacharach,2 Inder Paul Singh,3 Swarup S Swaminathan,4 Renee Bovelle,5 Hongxin Lai,6 Marcos Rivas,7 Vanessa Vera6
1Bovee Eye PLLC, Tampa, FL, USA; 2North Bay Eye Associates, Inc, Petaluma, CA, USA; 3Eye Centers of Racine & Kenosha, Racine, WI, USA; 4Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, USA; 5Envision Eye & Laser Center, Glenn Dale, MD, USA; 6AbbVie, Irvine, CA, USA; 7AbbVie, Madrid, Spain
Correspondence: Marcos Rivas, AbbVie, 91 Avenida de Burgos 28050, Madrid, Spain, Tel +34628759490, Email [email protected]
Abstract: Achieving a target intraocular pressure (IOP) in patients with ocular hypertension and open-angle glaucoma has many barriers, some treatment specific and others patient specific. Nonadherence to IOP-lowering eyedrops is one of the major barriers to effective glaucoma treatment. There is a wide range of patients who may benefit from non-topical treatment modalities such as selective laser trabeculoplasty and sustained-release drug delivery, including those who face challenges with topical eyedrops, and those who find benefit in independence from daily medication administration. Sustained-release drug delivery options for lowering IOP include the bimatoprost intracameral implant 10 μg (Bim-I), a relatively new treatment option. This article provides expert opinion on the use of the implant based on available literature, supplementary analysis of clinical trial data, and the experience of the authors who have performed thousands of Bim-I administrations. A single administration of Bim-I has demonstrated the potential to reduce IOP and the need for topical IOP-lowering medication for up to 2 years. Evidence suggests that the safety profile of the implant is most favorable in patients with wide-open (Shaffer grade 4) angles. Recommendations regarding the administration procedure and patient follow-up are provided. The objective of this expert opinion is to help optimize patient selection for Bim-I administration, the implantation procedure, follow-up management, and clinical outcomes while minimizing and addressing potential complications.
Keywords: bimatoprost intracameral implant, Durysta, intraocular pressure, open-angle glaucoma, treatment outcome, patient selection
Introduction
Open-angle glaucoma (OAG) is the most commonly diagnosed form of glaucoma worldwide.1 Although OAG is not always characterized by elevated intraocular pressure (IOP), IOP remains the only treatable risk factor for disease progression and irreversible vision loss in patients with OAG or ocular hypertension (OHT).2 Topical IOP-lowering medications (eyedrops) and laser therapy (eg, selective laser trabeculoplasty [SLT]) are commonly used as first-line treatment for OHT and OAG.3–5 The topical IOP-lowering medications that are most efficacious and most frequently used in initial treatment are the prostaglandin analog/prostamide (PGA) medications.6,7 Although procedures such as minimally invasive glaucoma surgery (MIGS) and minimally invasive bleb-forming surgery (MIBS) are typically considered when medications and/or laser treatment fail or are not well tolerated, the glaucoma treatment paradigm is starting to evolve towards a more proactive approach involving more procedural interventions.8
Newer treatment options in the form of sustained-release drug delivery platforms have emerged for patients who may benefit from a modality other than eyedrops or laser therapy. Among these, the bimatoprost intracameral implant 10 µg (Bim-I; Durysta®; AbbVie, North Chicago, IL) was approved in 2020 by the US Food and Drug Administration (FDA) for single administration in patients with OAG or OHT.9,10 Bim-I is a small cylindrical implant (approximately 200 µm in diameter and 1.1 mm in length) that is administered into the intracameral space with a single-use applicator.11 The implant is biodegradable and consists of 10 µg of bimatoprost in a matrix of poly-lactic acid and polylactic-co-glycolic polymers.11 Bimatoprost is slowly released as the implant polymers biodegrade.12 Although the implant was designed to release drug over 3–4 months, there is evidence from randomized clinical trials and real-world studies suggesting a longer duration of effect.13–21 In some patients, the implant has been shown to reduce IOP for 2 years without the need for additional IOP-lowering therapies.13,22
This article provides expert opinion on the use of the implant based on evidence from published studies, supplementary analysis of clinical trial data, and the experience of the authors (C.B., J.B., I.P.S., S.S.S., and R.B.) who have performed thousands of Bim-I implantations. The objective of this manuscript is to help optimize patient selection, the implantation procedure, follow-up management, and clinical outcomes while minimizing and addressing potential complications.
Evolution of Study Protocol Designs to Optimize Patient Outcomes
The clinical development program of Bim-I evolved to help optimize patient outcomes (Figure 1). In the prospective, randomized, 20-month, multicenter, evaluator-masked, Phase 3 ARTEMIS studies (1 and 2),10,12 all patients received a fixed regimen of three Bim-I administrations (once every 4 months). This fixed treatment regimen often led to accumulation of implant remnants in the anterior chamber. Further, corneal adverse events were more frequent after repeated administration of the implant, and their occurrence was thought to be related to the volume of accumulated implant material in the iridocorneal angle.11 With the fixed 16-week dosing interval used in the study, 10.2% and 8.1% of eyes treated with Bim-I exhibited ≥20% corneal endothelial cell density (CECD) loss (a threshold believed to be reliable and clinically meaningful23) during ARTEMIS 1 and ARTEMIS 2, respectively.10,12 As a result, the FDA approved the implant for a single administration per eye.
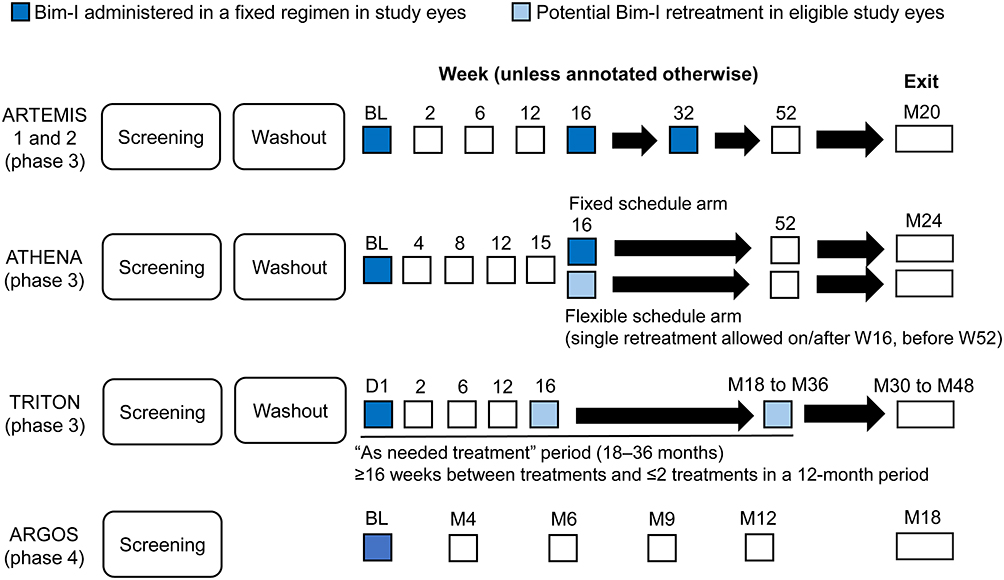 |
Figure 1 Improving clinical outcomes through study design. Only the Bim-I arm(s) of the studies are shown. Solid arrows indicate follow-up visits. Abbreviations: Bim-I, bimatoprost intracameral implant; BL, baseline; D, day; M, month; W, week. |
ATHENA was a prospective, randomized, 24-month, multicenter, patient- and efficacy evaluator–masked, paired-eye, phase 3 study comparing Bim-I with SLT.22 Considering the findings from the ARTEMIS studies, the ATHENA study protocol was eventually amended from two fixed administrations 4 months apart to a flexible treatment regimen of two administrations with a minimum retreatment interval of 4 months and a maximum of two administrations in a 12-month period.22 Overall, Bim-I met the primary endpoint of noninferiority to SLT in IOP change from baseline at 1, 4, and 6 months.22 The study also showed comparable efficacy and an improved safety profile with the flexible regimen compared with the fixed regimen.22 The proportion of eyes with ≥20% CECD loss during the study was 7.1% with the flexible regimen versus 9.0% with the fixed regimen.22
TRITON is an ongoing, prospective, open-label, multicenter phase 3b study evaluating the duration of effect of Bim-I.24 The study protocol allows up to three Bim-I administrations in a pro re nata, flexible regimen with a minimum retreatment interval of 4 months and a maximum of two administrations in a 12-month period.24 Results of an interim analysis have been reported. In survival analysis using the interim dataset, the probability of not having required a second administration or rescue treatment was 57.5% at day 360 and 33.4% at day 720, and the median time from the first implant administration to requiring either a second implant administration or rescue treatment was 392 days.24 The study results also showed a lower incidence of ≥20% CECD loss in eyes with Shaffer grade 4 (5.4%) versus Shaffer grade 3 (15.6%) inferior angles, as well as a trend for a lower incidence of ≥20% CECD loss in pseudophakic eyes (5.6%) compared with phakic eyes (11.1%).24
ARGOS was a prospective, observational, open-label, multicenter, 18-month, phase 4 study evaluating the effectiveness and safety of a single Bim-I administration in real-world clinical settings.21 In contrast to the ARTEMIS,10,12 ATHENA,22 and TRITON24 studies, the ARGOS study did not include a washout period before the baseline assessments; thus, the baseline was a medicated baseline, and many patients discontinued their topical IOP-lowering medications at the time of or after the implant administration. The proportion of primary eyes that had no new IOP-lowering medication or procedure (“additional treatment”) after the implant administration was 88.6% at month 6 (primary endpoint) and remained high at months 12 (83.7%) and 18 (77.7%).21 Among the 41 eyes that received additional treatment, the median time to the first additional treatment was 17.6 months.21 Implant removal was required in 3 of 340 implant-treated eyes (0.9%) because of corneal edema or endothelial cell loss.21
Patient Selection
Clinical trial findings and real-world evidence give us insight into how to optimize the outcomes of Bim-I treatment.
Patient Characteristics
Eliciting adherence issues can be difficult. Patients often try to please their physician or may be embarrassed to state their issues, and care providers may be subject to time constraints. Nonetheless, identifying adherence issues and understanding the reasons underlying nonadherence are key to individualizing and optimizing treatment.25 Patients who struggle with topical therapy (eyedrops) because of forgetfulness, tolerability issues, complexity of the prescribed regimen, or comorbidities hindering self-administration of eyedrops such as low vision or physical or cognitive conditions26 may benefit from sustained-release implants such as Bim-I. Patients who find their topical treatment regimen to be inconvenient may also benefit from Bim-I and independence from eyedrops. Any patient on a topical PGA may be considered to be a potential candidate for Bim-I.
The reasons to treat patients with the implant that were identified in clinical studies are shown in Figure 2. The most common reasons identified were related to topical medication side effects or to patient nonadherence to topical medications for reasons including memory problems/forgetfulness and medication cost. In the clinical experience of an author (C.B)., some patients who are doing well on topical drops may opt for Bim-I and independence from drops to simplify their glaucoma management and gain peace of mind.
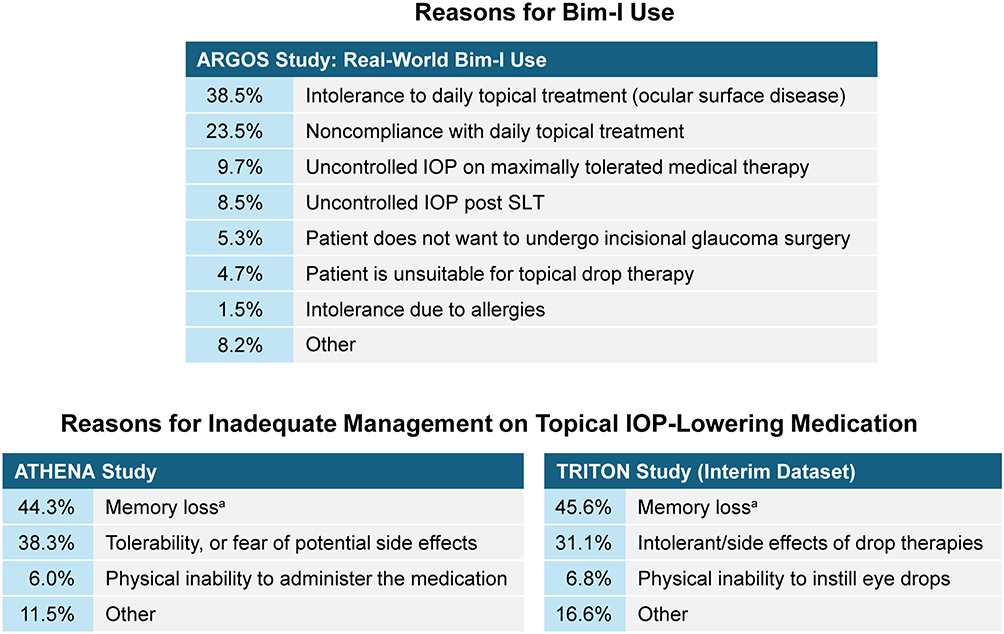 |
Figure 2 Reasons unrelated to efficacy for inadequate IOP management with topical medications and reasons for using Bim-I as identified in clinical studies of the implant. In each study, investigators selected reasons from among options that were available on the case report form. Data shown are the percentage of eyes treated with Bim-I for each reason in the ARGOS study,21 and the percentage of patients whose Bim-I–treated study eye was inadequately managed with topical IOP-lowering medication for each reason in the ATHENA22 and TRITON24 studies. The most common “other” reasons in the TRITON study were the cost of topical medications and nonadherence to topical medications. aForgetfulness could be categorized as memory loss. Abbreviations: Bim-I, bimatoprost intracameral implant; SLT, selective laser trabeculoplasty. |
Baseline IOP as a Predictor of Response
The duration of effective IOP management with Bim-I varies among patients from a few months to 2 years,13,22,24 and identifying predictors of long-term IOP management with the implant could help guide the decision of whether to use this treatment. In this regard, we conducted a post hoc analysis of data from the prospective, real-world ARGOS study to identify factors associated with the need for additional IOP-lowering treatment (a new medication or procedure) after Bim-I administration. Univariate Cox regression models of time to first additional IOP-lowering treatment were applied using covariates of baseline IOP as a continuous variable, baseline IOP as a categorical variable (<25 mmHg or ≥25 mmHg), sex (male or female), change in IOP from baseline at 12 weeks, number of IOP-lowering medications used at baseline (0, 1, 2, or ≥3), and baseline lens status (phakic or pseudophakic) (Supplementary Material 1).
The results of the analysis showed that each increment of 1 mmHg in baseline IOP increased the risk of requiring additional IOP-lowering treatment by 8% (hazard ratio [HR]: 1.08; 95% confidence interval [CI]: 1.02–1.14), and patients with a medicated baseline IOP <25 mmHg were less likely to require additional IOP-lowering treatment than those with a medicated baseline IOP ≥25 mmHg (HR: 0.38; 95% CI: 0.15–0.98). None of the other factors evaluated were significantly associated with the risk of needing additional treatment after Bim-I administration (Supplementary Material 1). The longer duration of IOP management without added treatment provided by the implant in patients with a lower baseline IOP may possibly be explained by physicians choosing to treat more aggressively when the baseline IOP is higher. Patients who have a higher baseline IOP likely require a greater IOP reduction to achieve the target pressure, and thus, may need additional treatment after the implant administration.
The degree of IOP reduction with Bim-I also may potentially be influenced by the baseline IOP. In a retrospective, single-center study of 156 patients with OAG, those with a baseline IOP ≥21 mmHg were shown to experience a larger IOP reduction (mean change from medicated baseline: −6.4 mmHg; p < 0.0001) than those with a baseline IOP <21 mmHg (mean change from medicated baseline: +0.9 mmHg).19 However, a difference between groups in how the implant was used likely caused or contributed to this difference in IOP lowering. In patients with baseline IOP ≥21 mmHg, the implant was generally added to ongoing medication, whereas in patients with baseline IOP <21 mmHg, the implant was typically used to replace 1 or more topical medications. The number of IOP-lowering medications used by patients with baseline IOP <21 mmHg was significantly reduced from baseline at 6 months after the Bim-I administration (mean change from baseline: −1.3; p < 0.0001), with no significant change in IOP.19
Target IOP and Reduction in Medication Burden
In the ARGOS study, the mean medicated baseline IOP was 2 mmHg higher than the population’s mean target IOP (15 mmHg). At 12 and 18 months after Bim-I administration, on average the target IOP was achieved (mean IOP of 15.3 and 15.0 mmHg, respectively). The mean medication count had decreased by 50% (from 1.8 to 0.9) and 44% (from 1.8 to 1.0), with 83.7% and 77.7% of eyes having added no new IOP-lowering treatment, at 12 and 18 months, respectively, after the Bim-I administration.21 In 4 of 5 retrospective, real-world studies with 12-month data published to date, mean IOP at 12 months mostly appeared in line with the aforementioned target, ranging from 13.3 to 16.3 mmHg.16–18,20 In the real-world study by Sarkisian et al,19 mean IOP was 18.0 mmHg at 12 months. Whether baseline characteristics of the study populations might explain the differences in mean IOP achieved in the studies is unclear as the level of detail provided varies across studies.
Real-world studies of Bim-I use have shown that implant administration frequently is associated with a reduction in the number of topical IOP-lowering medications used by patients. In fact, independence from eyedrop use can be a motivation for patients to receive the implant. In the study reported by Teymoorian et al20 in 197 eyes treated with Bim-I, the median number of topical IOP-lowering medications used was one before the implant administration and zero at all timepoints through 12 months of follow-up after the implant administration. All eyes that were being treated with a topical PGA discontinued the PGA when the implant was administered. In the ARGOS study,21 the mean number of topical IOP-lowering medications used was reduced from 1.8 at baseline to 0.9 at month 12 and 1.0 at month 18. Topical IOP-lowering medications were frequently stopped at the time of the implant administration or tapered after the effects of the implant on IOP were assessed.21
Diagnosis and Stage of Disease
Bim-I is currently indicated for lowering IOP in patients with OAG and OHT.27 In published studies of the implant that provided details of the diagnosis of the participants, most (77% to 86%)10,12,15,18,22,24 or all13 of the participants were diagnosed with primary OAG. However, none of the studies with a mixed population of patients reported the efficacy of Bim-I by diagnosis (type of OAG, or OAG vs OHT). It could be very informative to plan for such analyses in future studies or to perform post hoc analyses of completed studies.
The ability of Bim-I to control IOP without need for additional treatment could also potentially be influenced by the stage of glaucoma. Among the published real-world studies with information on glaucoma severity at baseline,16,18,20,28 only the study by Choi et al18 analyzed the potential relationship between glaucoma severity (which was based on International Classification of Diseases, Tenth Revision [ICD-10] codes documented at the initial study visit) and the effectiveness of Bim-I treatment. In that study, patients with severe glaucoma (54% of the total study population) showed a reduction in the number of IOP-lowering medications used at month 1 (p = 0.011) only, whereas the combined group of patients with mild (11%) or moderate (30%) glaucoma showed a reduction in the number of IOP-lowering medications used through 6 months (p ≤ 0.0016).18 However, there was no significant difference in medication reduction between the mild/moderate and severe glaucoma groups at any timepoint, and the apparent shorter duration of Bim-I’s effect in reducing topical medication use in severe glaucoma may have resulted from different treatment goals for the patients with severe glaucoma. Patients with severe disease may have a lower target IOP and need more intensive treatment or earlier surgical intervention.
Angle Dimensions and Space for the Implant
Evaluation of the iridocorneal angle and iris configuration to determine whether there is space to accommodate the implant without corneal touch is critical, because corneal contact of the implant could lead to endothelial cell loss. During this evaluation, it is important to keep in mind that implants can swell during the initial phase of biodegradation (weeks 2–28).11 Based on physician estimates of implant size relative to their initial size, approximately 40% of implants swell during this period, with the estimated size of the swollen implants typically up to 150% of the initial size, and in some cases, >200% of the initial size.11 An open inferior iridocorneal angle with Shaffer grade ≥3 was required for patient entry in the Bim-I clinical trials,10,12,22,24,29 and the product label contains a warning that Bim-I “should be used with caution in patients with narrow iridocorneal angles (Shaffer grade <3) or anatomical obstruction (eg, scarring) that may prohibit settling in the inferior angle.”27
Although Bim-I can be used successfully in eyes with Shaffer grade 3 angles, there is evidence suggesting that the safety profile of the implant is most favorable when the angle is wide open (Shaffer grade 4). The ATHENA22 and interim TRITON24 clinical trial results demonstrated a reduced incidence of ≥20% endothelial cell loss in eyes with Shaffer grade 4 angles (5.3%22 and 5.4%24) compared with eyes with Shaffer grade 3 angles (15.6%22 and 15.6%24). Results of real-world studies that provided information about the Shaffer grade and/or lens status in Bim-I–treated eyes have suggested that in clinical practice, the implant is usually used in patients with wide open angles. The proportion of treated eyes with grade 4 angles was 64%21 and 84%,20 and the proportion of treated eyes that were pseudophakic was 64%,17 67%,21 and 95%20 in these studies.
A case was reported of a patient who developed microcystic corneal edema in one eye after bilateral Bim-I treatment.30 The angle in the eye was open but had a steep iris configuration, causing the implant to be lodged between the cornea and the iris. This case highlights the importance of evaluating the iris configuration when considering treatment with Bim-I. The authors cautioned that “even in the presence of an open angle, a convex iris configuration or steep iris insertion could increase the risk of complications following Bim-I implantation, particularly in phakic individuals.”30
Race/Ethnicity
Most of the patients who were treated with Bim-I in the ATHENA22 and TRITON24 clinical trials were White (≥75.8%) or Black or African American (≥15.0%), and outcomes by race were not reported. Similarly, the majority of patients in the real-world studies16–21,28 discussed above were White; Black, Asian, and Native American patients were also included, and outcomes by race were not reported. However, we have now analyzed outcomes by race in the ARGOS study. Patients in the ARGOS study were White (68.6%), Black or African American (18.6%), Asian (4.3%), “other” race (0.5%), or did not report their race (8.1%). In a preplanned analysis based on observed values, the proportion of Bim-I–treated primary eyes that had not received a new added IOP-lowering treatment at 12 and 18 months after the implant administration, respectively, was 82.6% and 79.2% (White, N=144), 93.1% and 88.0% (Black or African American, N=39), 100% and 71.4% (other [mostly Asian], N=10), and 70.0% and 60.0% (race not reported, N=17) (AbbVie data on file). The high rate of effectiveness of Bim-I in Black or African American patients is encouraging, as individuals of African descent have a higher prevalence of primary OAG and faster rate of progression compared with individuals of European descent.31 There is also evidence suggesting a greater incidence and aggressiveness of OAG in individuals who are Hispanic;32,33 thus, additional studies evaluating Bim-I outcomes in Black versus non-Black patients and Hispanic versus non-Hispanic patients could be informative.
Age
There is some evidence that among adults with glaucoma, the risk of nonadherence to topical IOP-lowering treatment is highest for younger patients and those who are very elderly.34 Working-age patients who have a demanding work schedule may be particularly inconvenienced by eyedrop use and prefer a drop-free treatment. On the other hand, elderly patients are frequently polymedicated and most likely to have comorbidities that are barriers to eyedrop use,26 and may also benefit from alternatives to eyedrops.
Mean age at baseline ranged from 62–63 years in the ARTEMIS,10,12 ATHENA,22 and TRITON24 clinical trials, while it ranged from 73–80 years in real-world studies.16–21,28 To our knowledge, no studies have evaluated the potential impact of age on patient preferences for Bim-I treatment or on Bim-I’s effects.
Place in Treatment Algorithm
First-Line Option
Patients newly diagnosed with OAG/OHT potentially may benefit from Bim-I and freedom from eyedrop use. Some treatment-naïve patients were included in at least two real-world studies.17,21 However, efficacy analyses in the subgroup that used Bim-I as first-line treatment were not reported.
Transition from Eyedrops to Bim-I
Real-world studies16,17,19–21,28 have suggested that the majority of patients (78.8%–94.9% in these studies) use eyedrops before receiving Bim-I and require fewer eyedrops for IOP management after the implant administration. The mean reduction from baseline in the number of topical medications used by patients in these studies17,18,20,21 ranged from 0.5 to ≥1.0 at 12 months after Bim-I administration. In the ARGOS real-world study (with no washout), IOP-lowering medications were sometimes tapered off gradually after the implant administration.21 In contrast, in the single-site study by Teymoorian et al,20 topical PGAs used at baseline were discontinued at implantation in all Bim I–treated eyes.
We performed a post hoc analysis of the interim TRITON study dataset24 to evaluate the effects of replacing topical PGA monotherapy with Bim-I. Observed IOP data in the subset of patients who were on PGA monotherapy at screening were analyzed at screening, at baseline after washout, and at 3 and 6 months after a single Bim-I administration. Data from patients who received any additional IOP-lowering treatment after the Bim-I administration were excluded from analysis. The results showed that Bim-I can replace one topical PGA and further reduce IOP for at least 6 months (Figure 3). The mean (SD) change in IOP from screening was −1.7 (4.24) mmHg at 3 months after the Bim-I administration (n=136; p < 0.001, paired t-test) and −1.3 (3.60) mmHg at 6 months after the Bim-I administration (n=120; p < 0.001, paired t-test).
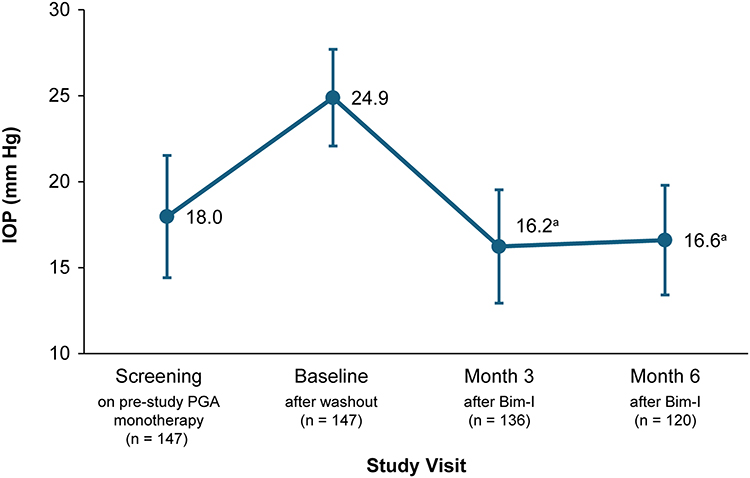 |
Figure 3 IOP-lowering effect of Bim-I in the TRITON study (interim dataset analysis) in eyes that were treated with topical PGA monotherapy at screening, were washed out before the Bim-I administration, and did not receive any added IOP-lowering treatment after the initial Bim-I administration. Mean ± standard deviation data are shown. ap < 0.001 vs screening (paired t-test). Abbreviations: Bim-I, bimatoprost intracameral implant; IOP, intraocular pressure; PGA, prostaglandin analog. |
The authors have had success in stopping more than one class of topical medication at the time of implant administration, with the realistic expectation that if necessary, medications can be restarted, or SLT can be considered to achieve the desired target pressure. They suspect that in the cases where the implant successfully replaced more than one topical medication, the patient may not have been properly administering the multiple medications, but additional evaluations would be needed to confirm this hypothesis.
Efficacy After or Between SLT Treatments
Retrospective, real-world studies by Wong et al28 (n=118) and Teymoorian et al20 (n=197) indicated that a history of prior SLT treatment did not affect the reductions in IOP or medication count from baseline observed following treatment with Bim-I. Teymoorian et al20 further showed that Bim-I can be used between two cycles of SLT, with the aim of keeping the patients off eyedrops. Prospective studies are needed to confirm these findings and draw definite conclusions.
Efficacy After Glaucoma Surgery
In a real-world study reported by Bowers et al,35 Bim-I was effective in reducing the number of topical IOP-lowering medications needed for IOP control in 41 eyes (in 31 patients) with a history of previous glaucoma surgery (incisional or MIGS). The patients were followed for a mean of 30.4 weeks after receiving Bim-I, and at both month 6 and the last available visit, the mean topical medication count was 1.2, compared with 1.9 at baseline before the implant administration (p < 0.001). The mean IOP was also reduced from 17.8 mmHg at medicated baseline to 16.6 mmHg at month 6 and the final visit, but this change in IOP was not statistically significant. These results indicate that Bim-I could be a good treatment option after glaucoma surgery including tube shunts and failed trabeculectomies (Figure 4).
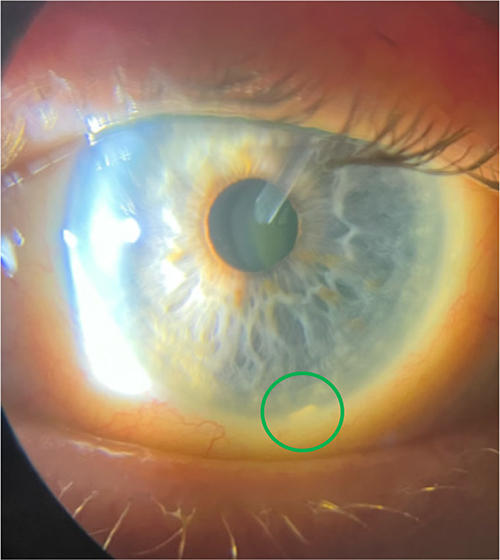 |
Figure 4 Bimatoprost intracameral implant (green circle) in the anterior chamber of a patient previously treated with a tube shunt. Image courtesy of Courtney Bovee. |
IOP Monitoring and Follow-Up
Along with appropriate patient selection, proper IOP monitoring and follow-up after Bim-I treatment are important to optimize outcomes. Follow-up visits should be scheduled similarly to the schedule after a new IOP-lowering medication is started or a laser treatment is performed to reduce the patient’s IOP, with the frequency of visits adjusted based on the patient’s risk factors and the physician’s clinical judgment.
The duration of effect of the implant is variable. In the authors’ experience, the efficacy typically wears off slowly and gradually over a period of 4 to approximately 24 months. When the IOP starts to rise above target because of the implant effect wearing off months post-administration, the authors re-evaluate adding topical or oral IOP-lowering medication, laser therapy, alternative sustained-release options, or surgical interventions. Increases in IOP after Bim-I administration have been reported in real-world studies,17,19–21,28 with the IOP elevated to levels above medicated baseline in rare cases.20,28 The increases in IOP were typically managed with the options mentioned above.
Elevations in IOP after Bim-I administration could be caused by the implant effect wearing off, the removal of topical IOP-lowering medications, a poor response to the implant, or a combination of these factors. In the experience of the authors, IOP elevations have occurred only when patients on multiple IOP-lowering medications (polypharmacy) stop using all of their medications when they receive the implant. The authors suggest that if a patient is on polypharmacy, has significant disease, and has Bim-I implanted, the treating physician should consider not stopping all eyedrops at that time, but instead, wait to see how the patient is doing clinically. In this situation, it may be best to discontinue only the topical PGA at the time of the implant, then taper other classes of topical medications, if appropriate, after follow-up evaluations.
Implant Location and Mobility
We have observed that following administration, the implant usually settles in the inferior angle between 5 and 7 o’clock (Figure 4). In agreement with these observations, at least 96% of the implants administered on day 1 in the ATHENA studies were reported to reside at 5–7 o’clock in the inferior angle at visits from week 2 through week 15.11 However, the implant can also be located at other clock hours, and in some cases may sit on the iris (with no corneal touch) rather than settling in the angle (Figure 5). In the authors’ experience, the implant’s final resting position can vary depending on the patient’s sleeping habits or activities performed during the first hours or days post-administration. It is important to monitor signs of implant mobility, such as pigment on the implant surface, as implant mobility may pose a threat to the integrity of the corneal endothelium.
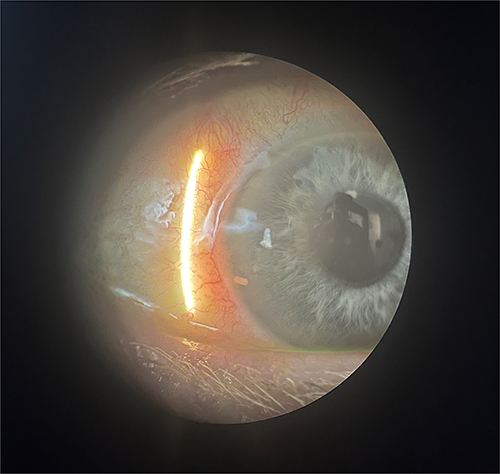 |
Figure 5 Bimatoprost intracameral implant sitting on the iris without corneal touch. Image courtesy of Jason Bacharach. |
Monitoring of Corneal Health
The risk of corneal adverse events with an intracameral implant is a safety concern. The ARGOS study showed a small mean decrease in CECD over the 18 months after a single Bim-I administration.21 At month 18, the mean percentage change in CECD from baseline in implant-treated eyes was −3.47% (n=131) based on central reading center evaluation and −3.23% based on autocounts.21 Three (1.2%) of the implant-treated eyes in ARGOS required implant removal because of treatment-emergent adverse events related to corneal edema or corneal endothelial cell loss.21 Consistent with the ARGOS study findings, in the interim dataset analysis of the TRITON study, the mean percentage change in CECD from baseline was −4.3% at 12 months after a single Bim-I administration.24
Because of the potential for corneal endothelial cell loss, the Bim-I label advises caution when administering the implant in patients with a limited corneal endothelial cell reserve, and the implant is contraindicated in patients with corneal endothelial cell dystrophy.27 In the authors’ opinion, CECD assessment by specular microscopy is generally not necessary if the implant is immobile and well placed (ie, deep in the angle without corneal touch). In real-world settings, slit lamp biomicroscopy is routinely used to examine the health of the cornea and endothelium to evaluate for abnormalities such as corneal guttae, and specular microscopy may be performed if corneal health is questioned, or patients are at higher risk.
Administration-Related Tips
Visual Inspection of the Applicator
Visual inspection of the applicator should include ensuring that the actuator button has not been depressed and the safety tab is in place.27 It is also important to check the needle tip; the applicator should not be used if the needle tip is burred or there is debris present (Figure 6). If the injector needle is damaged, the applicator should be returned to the manufacturer for analysis.
 |
Figure 6 Examples of functioning vs damaged injector needles. Images courtesy of AbbVie. |
Preparing the Patient for Bim-I Administration
Follow your standard protocol for aseptic preparation for intracameral procedures. A conventional eyelid speculum or Tegaderm transparent film dressing (3M; St. Paul, Minnesota, USA) can be used to allow for visualization of the anterior chamber without lid interference (Figure 7A and B). Preparing the eye with povidone iodine or any other standard antiseptic is essential to minimize the risk of endophthalmitis. The authors recommend numbing with proparacaine, then using povidone iodine diluted to 5% with a lid swab to properly clean the lashes and lid margin. They also note that evidence from studies evaluating physician masking during intravitreal injections suggests that wearing a mask could decrease the incidence of aerosolized bacteria, further decreasing the risk of endophthalmitis.36
 |
Figure 7 Administration procedure at the slit lamp using (A) eyelid speculum or (B) Tegaderm. Stabilization of the patient’s head (C and D) and eye (D) is important during administration of the bimatoprost intracameral implant. Images courtesy of Renee Bovelle (A and D) and Jason Bacharach (B and C). |
The administration procedure can be performed with the patient in supine position under a microscope (Video S1) or in upright position under the slit lamp (Video S2) with the patient’s head held in a stabilized position by an assistant (Figure 7C and D). The eye should not be dilated before the administration.
Administration
The intracameral administration procedure must be performed under magnification that allows clear visualization of the anterior chamber structures (Figure 7A and B; Video S1). It is important to both immobilize the patient’s head (Figure 7C and D) and stabilize the eye as the needle is advanced through the cornea; the latter can be done by applying counterpressure with a cotton-tipped applicator (Figure 7D).
The applicator needle should enter the anterior chamber with the needle bevel visible through clear cornea. The needle should enter the anterior chamber parallel to the iris plane, adjacent to the limbus through clear cornea. Following the injection, the eye should be washed, and a drop of topical antibiotic can be instilled.
When bilateral treatment is required, the eyes are usually treated separately, 1 or 2 weeks apart.
Post-Administration Instructions and Follow-Up
Following Bim-I administration, patients should be instructed to remain upright for at least 1 hour, so the implant can settle (Figure 4).27 To avoid corneal contact of the implant, it is also advisable to instruct patients to sleep face up (not on their side or face down) for a few days after the procedure.
Some degree of eye redness and discomfort from the prep solutions is expected following administration, and patients should be informed accordingly. The redness or discomfort is generally transient (lasting approximately 1 day). Moreover, patients should be instructed to contact the treating physician immediately if they experience any of the following symptoms in the treated eye: progressive redness, sensitivity to light, pain, or change in vision. Additional instructions should be provided regarding physical activities and ocular medications, and a follow-up appointment should be scheduled to check on the patient’s response to the implant.
The side effect profile of Bim-I includes adverse effects related to the PGA class of medications such as iris pigmentation, inflammation of the anterior segment, and cystoid macular edema (CME), as well as adverse effects related to the administration procedure (eg, endophthalmitis) and to the implant itself (eg, corneal events and implant migration).27 Current evidence suggests that the incidence of CME after a single administration of Bim-I is low (<0.2%) and similar to the 0.09% incidence of CME reported for topical PGAs.37 In large prospective clinical studies, among the 988 study eyes treated with Bim-I in the ARTEMIS 1 and 2, ATHENA, and interim dataset TRITON studies, CME was reported in 2 (0.2%) eyes; in those two eyes, the CME occurred after a second and third administration of Bim-I. There were no reports of CME in the real-world studies16–21,28,35 discussed above, in which 1200 eyes received a single administration of Bim-I. Three case reports of CME following Bim-I administration have been published.38–40 Bettach et al38 reported a case of unilateral CME in a patient who had received Bim-I in both eyes; the eye that developed CME had a probable history of CME after prior cataract surgery. Patel et al39 reported a case of bilateral CME in a patient who had received Bim-I in both eyes; both eyes had previously developed CME after cataract surgery. Finally, Jiao et al40 reported a case of bilateral sclerouveitis with associated CME in a patient who had received Bim-I in both eyes. Both eyes were pseudophakic, but the patient had no other known risk factors for PGA-related inflammation and CME.40
Troubleshooting Scenarios
The troubleshooting scenarios presented below are not found in the prescribing information. The insights provided in this section have been gained through clinical experience and, therefore, consideration of the suggestions provided is ultimately at the discretion of the physician.
Bim-I Adheres to the Needle Tip During the Administration Procedure
If the implant adheres to the needle tip during the administration procedure (Figure 8), wait 5 seconds to allow the implant to disengage from the needle tip. If this is unsuccessful, withdraw the needle from the anterior chamber. Contact with the inner lip of the administration track should release the implant from the needle tip.
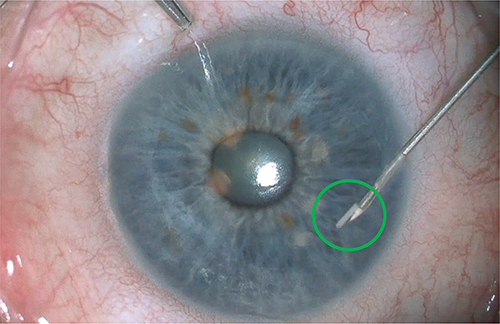 |
Figure 8 Image of a bimatoprost intracameral implant (green circle) adhering to the needle tip during the administration procedure. Image courtesy of AbbVie. |
To avoid this potential issue, some physicians have implemented a slightly modified administration technique. They start by partially depressing the actuator button, then fully pressing it after a second or two (Video S2). Doing so seems to consistently allow the implant to separate from the loader/injector. In addition, some physicians have found that removing the Bim-I from refrigerated storage 30 minutes prior to administration decreases the incidence of Bim-I adhering to the needle tip.
Bim-I Becomes Lodged in the Corneal Administration Track
Implants should not be allowed to remain lodged in or in contact with the administration track (Figure 9), as this may trigger an inflammatory response. To dislodge the implant, gently tap the cornea over the administration track to cause the implant to drop down. If that does not work, use an anterior chamber probe to dislodge the implant from the administration track by advancing it approximately 4 mm into the anterior chamber.
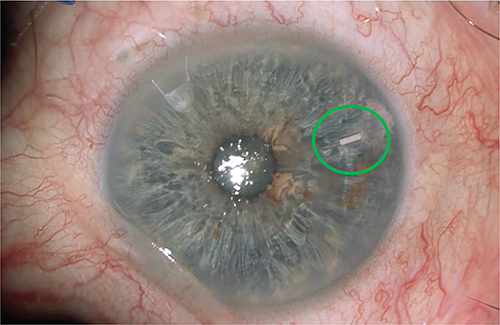 |
Figure 9 Image of a bimatoprost intracameral implant (green circle) lodged in the corneal administration track. Image courtesy of AbbVie. |
Bim-I Floats in the Anterior Chamber
When the implant is released, it sometimes adheres to an air bubble, causing the implant to float (Figure 10). The air bubble should dissipate quickly on its own, and the implant will settle down. For additional information, please see Video S2.
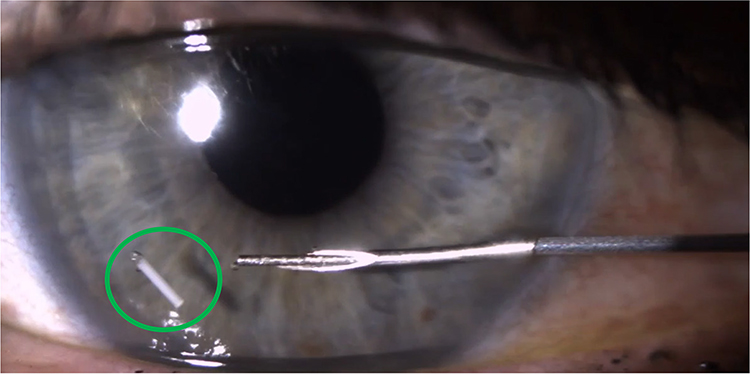 |
Figure 10 Image of a bimatoprost intracameral implant (green circle) floating in the anterior chamber. Image courtesy of Paul Singh. |
Bim-I Removal from the Anterior Chamber
Occasionally an implant needs to be removed from the anterior chamber because of corneal events or implant mobility. To remove the implant, an anterior chamber washout procedure should be performed with a sterile intraocular irrigating solution. After creating a wound with a keratome, viscoelastic can be used to burp the device out of the wound, taking care to compress the lower lip of the wound when ready to express out the implant (to ensure the implant does not get stuck in the angle under the wound itself). Attempting to grab the implant with forceps is not recommended, as the degrading implant is brittle and can break into pieces.
Intracorneal deployment of the implant can occur if the patient’s head moves or the bevel of the needle injector is not fully within the anterior chamber during the deployment. If this occurs, implant removal must be performed as soon as possible, through enlargement of the corneal track or creation of a small corneal incision (partial thickness) over the implant location, using standard aseptic technique for intraocular procedures. Incisions can be closed using your preferred closure method.
Summary
The lessons learned from the literature and the authors’ clinical experience with Bim-I are as follows. Bim-I can help overcome eyedrop-related nonadherence issues. It can also help reach a target IOP around 15 mmHg and typically eliminates the need for one topical medication. Sometimes more than one medication can be replaced by Bim-I if there are adherence problems with the eyedrops. The duration of IOP management with Bim-I may be longer for patients with a lower baseline IOP (<25 mmHg) and an earlier stage of disease, although more studies are required to confirm these findings and to identify predictors of long-term response. In addition, prior treatment with SLT or glaucoma surgery does not seem to negatively impact outcomes of Bim-I treatment. The time to return to baseline IOP can vary widely (from months to years), but in some patients, the IOP-lowering effect of Bim-I can last over 2 years.
Treating physicians should select patients with open angles and flat iris insertions (where the implant can settle away from the cornea) and avoid use in patients with any signs of compromised corneal health or active ocular inflammation, and well as patients unsuitable for PGAs. There are currently no data regarding the efficacy of Bim-I in non-responders to a PGA. Follow-up visits to monitor the implant and the response to treatment should be planned as when any new IOP-lowering medication or treatment is introduced.
Conclusion
Evidence from clinical studies and clinical experience has helped us better understand the potential of Bim-I and how to use it to optimize patient outcomes. Considering the increasing prevalence of glaucoma in the aging population and the increasing use of procedural interventions as the glaucoma treatment paradigm evolves, Bim-I has potential to be an important treatment option to help overcome nonadherence issues and reduce both IOP and medication burden.
Data Sharing Statement
AbbVie is committed to responsible data sharing regarding the clinical trials we sponsor. This includes access to anonymized, individual, and trial-level data (analysis data sets), as well as other information (eg, protocols, clinical study reports, or analysis plans), as long as the trials are not part of an ongoing or planned regulatory submission. This includes requests for clinical trial data for unlicensed products and indications. These clinical trial data can be requested by any qualified researchers who engage in rigorous, independent, scientific research, and will be provided following review and approval of a research proposal, Statistical Analysis Plan (SAP), and execution of a Data Sharing Agreement (DSA). Data requests can be submitted at any time after approval in the US and Europe and after acceptance of this manuscript for publication. The data will be accessible for 12 months, with possible extensions considered. For more information on the process, or to submit a request, visit the following link: https://www.abbvieclinicaltrials.com/hcp/data-sharing/.
Ethics Approval and Informed Consent
This study was compliant with the principles of the Declaration of Helsinki. All patients provided written informed consent before undergoing treatment. All data and videos presented in this manuscript were acquired in accordance with the Health Insurance Portability and Accountability Act with patient consent for the use of identifiable images and videos. The ARGOS and TRITON studies were approved by an institutional review board (IRB) or ethics committee (EC) at each participating site. A central IRB, the WIRB-Copernicus Group, was used for ARGOS. For TRITON, the IRBs/ECs were Bellberry Limited Human Research Ethics Committee; Bioethics Committee at the District Medical Chamber in Gdańsk; Central Ethics Committee of the IRCCS – IFO-Bietti Foundation Section; Clinical Research Ethics Committee – CEIC; Clinical Research Ethics Committee of Cork Teaching Hospitals; East Midlands – Leicester South Research Ethics Committee; Ethics Committee of the Albert Ludwig University of Freiburg; Ethics Committee of the Calabria Region, Central Area Section; Ethics Committee for Clinical Trials; Ethics Committee of the Faculty Hospital Kralovské Vinohrady; Ethics Committee of the General Teaching Hospital in Prague; Ethics Committee of the Hamburg Medical Association; Ethics Committee for the Pavia Area; Ethics Committee of the University Medical Center Göttingen; Independent Ethics Committee Integrated Consulting Rooms CEIC; Health and Disability Ethics Committee; Institutional Evaluation Committee of the Austral University Hospital; LAZIO 2; Research Ethics Committee of the Italian Hospital of Buenos Aires; SAMAREC; The Scientific Ethics Committees for the Capital Region of Denmark; Umbria Regional Ethics Committee; WCG IRB; Western Institutional Review Board.
Funding
AbbVie sponsored the development of this publication and participated in review and approval of the publication. Medical writing support was provided by Michele Jacob, PhD of Evidence Scientific Solutions (Raleigh, NC) and funded by AbbVie.
Disclosure
Courtney Bovee is a consultant for AbbVie, Bausch + Lomb, Glaukos, Harrow, Ocular Therapeutix, Radius XR, and Tarsus; sits on an advisory board for AbbVie and Radius XR; is a speaker for AbbVie, Glaukos, Harrow, New World Medical, Radius XR, and Sight Science; has served as a principal investigator or sub-investigator for AbbVie, Acelyrin, Alcon, Alimera, Alkeus, AstraZeneca, Bausch + Lomb, EyePoint, Genentech, Glaukos, Kodiak, Novartis, Ocular Therapeutix, Oculis, Opthea, Oxurion, Roche, Ocular Therapeutix, and Radius XR; and has financial interest through ETF or stock ownership in AbbVie, Glaukos, Harrow, Radius XR, and Sight Sciences. Jason Bacharach is a consultant for Alcon, Allergan, Bausch + Lomb, CBCC, Eyenovia, Glaukos, Humphrey-Zeiss, Iantrek, Imprimis, Injectsense, Ocular Therapeutix, Polyactiva, Santen, Sun, Tarsus, Théa, Topcon, Vialase, and Viatris; has received grant or research support from Alcon, AimMax, Bausch + Lomb, Biorasi, CBCC, Cloudbreak, Elios, Equinox, Glaukos, Injectsense, Kowa, Lenz, Nicox, Oasis, Ocular Therapeutix, Oculis, Oculos, Ocuphire, Ora, Orasis, Radius, Santen, Sight Science, Surface, Symbio, Tarsier, Tarsus, TearClear, Théa, Trefoil, Viatris, and Vivavision; has received lecture fees from Allergan, Bausch + Lomb, Bryn Mawr Communications, Dompe, Evolve, and Sun; and has equity/stock ownership in Iantrek, OnPace, and Radius. Inder Paul Singh is a speaker and consultant for AbbVie, Alcon, AVG, Bausch + Lomb, Glaukos, Iantrek, iStar Medical, Lumibird, New World Medical, Nova Eye, Ocular Therapeutix, PLU Ophthalmic, Sight Sciences, and Théa. Swarup S. Swaminathan is a consultant for AbbVie and Lumata Health; has received honoraria from Elios Vision and Heidelberg Engineering; and has equity in Lumata Health. Renee Bovelle is a speaker for Allergan/AbbVie, Bausch + Lomb, Ocular Therapeutics, PRN Vision Group, and Sun Ophthalmics, Inc.; and sits on advisory boards for Johnson & Johnson and Tarsus. Hongxin Lai, Marcos Rivas, and Vanessa Vera are employees of AbbVie and may hold AbbVie stock. The authors report no other conflicts of interest in this work.
References
1. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
2. Lee HP, Tsung TH, Tsai YC, Chen YH, Lu DW. Glaucoma: current and new therapeutic approaches. Biomedicines. 2024;12(9):2000. doi:10.3390/biomedicines12092000
3. Gedde SJ, Vinod K, Wright MM, et al. Primary open-angle glaucoma preferred practice pattern®. Ophthalmology. 2021;128(1):P71–P150. doi:10.1016/j.ophtha.2020.10.022
4. European Glaucoma Society Terminology and Guidelines for Glaucoma, 5th Edition. Br J Ophthalmol. 2021;105(Suppl 1):1–169. doi:10.1136/bjophthalmol-2021-egsguidelines
5. Rhee DJ, Sancheti H, Rothman AL, et al. Primary practice patterns for the initial management of open angle glaucoma. J Glaucoma. 2024;33(9):671–678. doi:10.1097/ijg.0000000000002453
6. van der Valk R, Webers CA, Lumley T, Hendrikse F, Prins MH, Schouten JS. A network meta-analysis combined direct and indirect comparisons between glaucoma drugs to rank effectiveness in lowering intraocular pressure. J Clin Epidemiol. 2009;62(12):1279–1283. doi:10.1016/j.jclinepi.2008.04.012
7. Schwartz GF, Patel A, Naik R, Lunacsek O, Ogbonnaya A, Campbell J. Characteristics and treatment patterns of newly diagnosed open-angle glaucoma patients in the United States: an administrative database analysis. Ophthalmol Glaucoma. 2021;4(2):117–125. doi:10.1016/j.ogla.2020.09.002
8. De Francesco T, Bacharach J, Smith O, Shah M. Early diagnostics and interventional glaucoma. Ther Adv Ophthalmol. 2024;16:25158414241287431. doi:10.1177/25158414241287431
9. Shirley M. Bimatoprost implant: first approval. Drugs Aging. 2020;37(6):457–462. doi:10.1007/s40266-020-00769-8
10. Bacharach J, Tatham A, Ferguson G, et al. Phase 3, randomized, 20-month study of the efficacy and safety of bimatoprost implant in patients with open-angle glaucoma and ocular hypertension (ARTEMIS 2). Drugs. 2021;81(17):2017–2033. doi:10.1007/s40265-021-01624-9
11. Weinreb RN, Bacharach J, Brubaker JW, et al. Bimatoprost implant biodegradation in the phase 3, randomized, 20-month ARTEMIS studies. J Ocul Pharmacol Ther. 2023;39(1):55–62. doi:10.1089/jop.2022.0137
12. Medeiros FA, Walters TR, Kolko M, et al. Phase 3, randomized, 20-month study of bimatoprost implant in open-angle glaucoma and ocular hypertension (ARTEMIS 1). Ophthalmology. 2020;127(12):1627–1641. doi:10.1016/j.ophtha.2020.06.018
13. Craven ER, Walters T, Christie WC, et al. 24-month Phase I/II clinical trial of bimatoprost sustained-release implant (Bimatoprost SR) in glaucoma patients. Drugs. 2020;80(2):167–179. doi:10.1007/s40265-019-01248-0
14. Medeiros FA, Sheybani A, Shah MM, et al. Single administration of intracameral bimatoprost implant 10 µg in patients with open-angle glaucoma or ocular hypertension. Ophthalmol Ther. 2022;11(4):1517–1537. doi:10.1007/s40123-022-00527-6
15. Weinreb RN, Christie WC, Medeiros FA, et al. Single administration of bimatoprost implant: effects on 24-hour intraocular pressure and 1-year outcomes. Ophthalmol Glaucoma. 2023;6(6):599–608. doi:10.1016/j.ogla.2023.06.007
16. Xu W, Zhou P, Kansara ND, Frankfort BJ, Blieden LS, Chang PT. Intraocular pressure and eyedrop usage reduction with intracameral bimatoprost implant. J Ocul Pharmacol Ther. 2023;39(6):398–403. doi:10.1089/jop.2023.0013
17. Ali AA, Avilés Elescano D, Grover DS. Bimatoprost SR for glaucoma therapy implanted at the slit-lamp in a real-world setting. Clin Ophthalmol. 2024;18:1371–1377. doi:10.2147/opth.S450220
18. Choi EY, Johnson NA, Stinnett S, Rosdahl J, Moya F, Herndon LW. The effect of bimatoprost implant on glaucoma patients: an observational study. J Glaucoma. 2024;33(6):431–436. doi:10.1097/ijg.0000000000002368
19. Sarkisian SR Jr, Mitchell EC. Real-world analysis of the efficacy of bimatoprost sustained-release glaucoma implant where American Indians comprise the largest minority population. Clin Ophthalmol. 2024;18:917–927. doi:10.2147/opth.S452159
20. Teymoorian S, Craven ER, Nguyen L, Werts E. Real-world study of the effectiveness and safety of intracameral bimatoprost implant in a clinical setting in the United States. Clin Ophthalmol. 2024;18:187–199. doi:10.2147/opth.S445005
21. Mann E, Kammer JA, Sawhney G, et al. Prospective 18-month study of bimatoprost intracameral implant in patients with open-angle glaucoma or ocular hypertension in US clinical practice. Drugs. 2025;85(3):397–414. doi:10.1007/s40265-025-02157-1
22. Kolko M, Tatham AJ, Lim KS, et al. Phase 3, randomized, comparison study of intracameral bimatoprost implant 10 µg and selective laser trabeculoplasty. Am J Ophthalmol. 2025;272:19–37. doi:10.1016/j.ajo.2024.12.026
23. McCarey BE, Edelhauser HF, Lynn MJ. Review of corneal endothelial specular microscopy for FDA clinical trials of refractive procedures, surgical devices, and new intraocular drugs and solutions. Cornea. 2008;27(1):1–16. doi:10.1097/ICO.0b013e31815892da
24. Silverstein SM, Oddone F, Kolko M, et al. Safety and longevity of intraocular pressure control after bimatoprost implant administration: interim analysis of a phase 3b clinical trial (TRITON). Drugs. 2025;85(4):557–570. doi:10.1007/s40265-025-02154-4
25. Newman-Casey PA, Rhee DJ, Robin AL, Mansberger SL. Patient challenges with glaucoma eye drops: a need to identify nonadherence and facilitate appropriate support and disease management. Ophthalmol Glaucoma. 2025;S2589-4196(2524):00217. doi:10.1016/j.ogla.2024.12.002
26. Cordeiro MF, Denis P, Astarita C, Belsey J, Rivas M, García-Feijoo J. Prevalence of comorbidities with the potential to increase the risk of nonadherence to topical ocular hypotensive medication in patients with open-angle glaucoma. Curr Med Res Opin. 2024;40(4):647–655. doi:10.1080/03007995.2024.2322048
27. Allergan. Durysta (bimatoprost implant) prescribing information. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/211911s002lbl.pdf.
28. Wong MK, Bowers ME, Ventimiglia J, et al. Short-term outcomes of bimatoprost sustained-release intracameral implant in glaucoma. J Glaucoma. 2023;32(9):738–743. doi:10.1097/ijg.0000000000002271
29. Lewis RA, Christie WC, Day DG, et al. Bimatoprost sustained-release implants for glaucoma therapy: 6-month results from a phase I/II clinical trial. Am J Ophthalmol. 2017;175:137–147. doi:10.1016/j.ajo.2016.11.020
30. Gallo Afflitto G, Swaminathan SS. Role of iris configuration in patient selection for Durysta implantation. Ophthalmol Glaucoma. 2022;5(6):586. doi:10.1016/j.ogla.2022.08.011
31. Sample PA, Girkin CA, Zangwill LM, et al. The African Descent and Glaucoma Evaluation Study (ADAGES): design and baseline data. Arch Ophthalmol. 2009;127(9):1136–1145. doi:10.1001/archophthalmol.2009.187
32. Varma R, Wang D, Wu C, et al. Four-year incidence of open-angle glaucoma and ocular hypertension: the Los Angeles Latino Eye Study. Am J Ophthalmol. 2012;154(2):315–325.e311. doi:10.1016/j.ajo.2012.02.014
33. Ciociola EC, Sekimitsu S, Smith S, et al. Racial disparities in glaucoma vision outcomes and eye care utilization: an IRIS Registry analysis. Am J Ophthalmol. 2024;264:194–204. doi:10.1016/j.ajo.2024.03.022
34. Friedman DS, Okeke CO, Jampel HD, et al. Risk factors for poor adherence to eyedrops in electronically monitored patients with glaucoma. Ophthalmology. 2009;116(6):1097–1105. doi:10.1016/j.ophtha.2009.01.021
35. Bowers ME, Wong MK, Ventimiglia J, et al. Effect of bimatoprost sustained-release intracameral implant on intraocular pressure and medication burden in patients with prior glaucoma surgery. J Fr Ophtalmol. 2024;47(2):103996. doi:10.1016/j.jfo.2023.07.016
36. Tao BK, Li X, Chen N, et al. Face masking and risk of endophthalmitis after intravitreal injection: a network meta-analysis of 2.6 million injections. Ophthalmology. 2024;S0161-6420(0124):00756. doi:10.1016/j.ophtha.2024.12.006
37. Hu J, Vu JT, Hong B, Gottlieb C. Uveitis and cystoid macular oedema secondary to topical prostaglandin analogue use in ocular hypertension and open angle glaucoma. Br J Ophthalmol. 2020;104(8):1040–1044. doi:10.1136/bjophthalmol-2019-315280
38. Bettach E, Wiener R, Brosh K, Zadok D, Goldberg M. Cystoid macular edema occurring after intracameral bimatoprost implantation. Eur J Ophthalmol. 2024;34(4):NP20–NP24. doi:10.1177/11206721241247588
39. Patel SH, Badar A, Bakhsh S, Jusufbegovic D. Bilateral cystoid macular edema after bimatoprost implants. Retin Cases Brief Rep. 2024;18(2):218–220. doi:10.1097/icb.0000000000001346
40. Jiao C, Prabakaran G, Berk T, Hossain HA, Arepalli S. Persistent bilateral sclerouveitis following bimatoprost implantation and removal. Am J Ophthalmol Case Rep. 2025;37:102240. doi:10.1016/j.ajoc.2024.102240
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.