Back to Journals » Patient Preference and Adherence » Volume 19
The Effectiveness of a Mindfulness-Based Art Therapy Program on Sleep Quality among Urban Older Adults in Thailand: A Quasi-Experimental Study
Authors Makkabphalanon K, Thangkratok P, Bunnaphasitthasothin C, Pramnoi P, Madsong C ![]()
Received 7 July 2025
Accepted for publication 13 September 2025
Published 16 October 2025 Volume 2025:19 Pages 3183—3195
DOI https://doi.org/10.2147/PPA.S551988
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Video abstract of “Effectiveness of Mindfulness-Based Art Therapy Program on Sleep Quality” [551988].
Views: 62
Khunatpakorn Makkabphalanon,1 Pramote Thangkratok,2,* Chedhakitd Bunnaphasitthasothin,3 Pornpimon Pramnoi,2 Chalermkwan Madsong2,*
1Boromarajonani College of Nursing, Nakhon Ratchasima, Thailand; 2Srisavarindhira Thai Red Cross Institute of Nursing, Bangkok, Thailand; 3Faculty of Nursing Srinakharinwirot University, Nakhon Nayok, Thailand
*These authors contributed equally to this work
Correspondence: Chalermkwan Madsong, Srisavarindhira Thai Red Cross Institute of Nursing, 1873 Rama IV Road, Pathum Wan, Bangkok, Thailand, Email [email protected]
Background: Approximately 50% of older adults experience sleep disturbances. The preservation of high-quality sleep is essential; consequently, there is a pressing need for effective interventions to enhance sleep quality.
Purpose: This study aimed to determine the effectiveness of the Mindfulness-Based Art Therapy (MBAT) on sleep quality, depression anxiety stress, and mindful attention awareness among older adults in urban contexts.
Patients and Methods: A quasi-experimental study with a one-group pretest-posttest design was conducted from March to May 2025. A random sample of 35 older adults with sleep problems was selected from 98 volunteers in Bangkok to participate in a six-week MBAT program using Mandala coloring. Data collection included a Personal Information Questionnaire, the Pittsburgh Sleep Quality Index (PSQI), the Depression Anxiety Stress Scales (DASS-21), and the Mindful Attention Awareness Scale (MAAS) at baseline (pre-test), 6 weeks (post-test), and 10 weeks (follow-up). Data were analyzed using descriptive statistics, one-way repeated measures ANOVA, and the Friedman test.
Results: Significant changes in PSQI scores (p < 0.001) and DASS-21 scores (p < 0.050), were observed over the 10 weeks study. Multiple comparisons revealed that participants showed significant improvements in PSQI scores from baseline to the 6 weeks and from baseline to 10 weeks (p < 0.001 and < 0.001, respectively) and DASS-21 scores were significantly different between the 6 weeks and 10 weeks (p < 0.050). Effect sizes indicated large effects for PSQI scores and DASS-21 scores. MAAS scores showed medium effects that were not statistically significant.
Conclusion: The MBAT program enhances relaxation for older adults, improving their sleep quality and mental health. It incorporates education on sleep hygiene, stimulus control, sleep restriction, relaxation techniques, and weekly telenursing sessions. The findings suggest it should be integrated into standard nursing care, and future research should consider extending the program’s duration to better change the MAAS score.
Trial Registry Number: Thai Clinical Trials Registry (TCTR20250409001).
(https://www.thaiclinicaltrials.org/show/TCTR20250409001).
Keywords: cognitive behavioral therapy, insomnia, CBT-I, aging, telehealth, mandala
Introduction
Aging is linked to a decline in physiological function, often leading to poorer sleep quality. Around 50% of older adults’ worldwide report experiencing poor sleep quality and shorter sleep durations. Moreover, about 20% of older adults indicate challenges such as excessive sleep, insomnia, and increased sleep disturbances.1 Thailand is currently facing a significant an older adult population challenge. The prevalence of insomnia among the Thai elderly reported to be 46.30%.2 Additionally, previous studies have found that between 35.91% and 66.30% of them experience poor sleep quality.3,4 This trend underscores the need for targeted policies and strategies to address the needs of this growing demographic.
As individuals age, their bodies frequently undergo a range of alterations that can substantially influence their overall quality of life. Notably, decreasing hormone levels such as estrogen in women and testosterone in men, are associated with risk of depression, which may linked to various sleep-related health concerns including obstructive sleep apnea hypoventilation syndrome and impaired sleep quality5,6 Furthermore, chronic illnesses such as diabetes, heart disease, and osteoarthritis can lead to significant discomfort and pain, which adversely impacts the capacity of older adults to attain restorative sleep.7,8 In addition to experiencing physical changes, older adults undergo psychological transformations that can significantly impact their mental and emotional well-being. Conditions such as depression and anxiety may develop because of bereavement, alterations in social roles, or the transition into retirement. The loss of interpersonal relationships can lead to heightened feelings of loneliness and despair, subsequently increasing stress levels among older adults. Such stressors have the potential to exacerbate sleep disturbances, as persistent ruminations and anxieties may trigger nighttime awakenings. The interplay of both physical and psychological changes profoundly affects the quality of sleep-in older adult.8–10 It is essential to understand these issues to develop effective therapeutic interventions that support older adults in managing transitions.
The sleep issues are often underrecognized and inadequately addressed in clinical settings.11 However, it is common for older adults to encounter various sleep-related challenges, including insomnia, frequent awakenings throughout the night, and early morning arousals. The natural sleep cycle is often disrupted due to declines in sleep-wake function in the brain, leading to a decrease in deep sleep, which compromises physical recovery.12 To enhance sleep quality in the elderly, various techniques such as cognitive behavioral therapy for insomnia (CBT-I),13,14 art therapy (ie, Mandala coloring),15 and mindfulness meditation16 have demonstrated effectiveness. These methods can substantially improve the quality of life for older adults in a sustainable manner.
Cognitive Behavioral Therapy for Insomnia (CBT-I) serves as a potent, non-drug intervention for insomnia among older adults, endorsed as a primary treatment option by the American College of Physicians.17 CBT-I assists older individuals in cultivating healthier sleep practices by addressing the thoughts and behaviors that disrupt sleep, including feelings of anxiety. This approach follows a systematic method that empowers them to enhance sleep through increased awareness and self-care.18 The core components of CBT-I include Sleep Restriction Therapy (SRT), Stimulus Control Therapy (SCT), Sleep Hygiene (SH), and Cognitive Therapy (CT).14,19 These components aim to help older adult initiate and maintain sleep and are typically delivered over six sessions. Previous study demonstrated that this six-session CBT-I intervention leads to improvements in insomnia severity, sleep efficiency, sleep onset latency, wake time after sleep onset, total sleep time, and anxiety disorders.18 Additionally, a study has shown that CBT-I can reduce both insomnia and depression severity in older adults suffering from depression.20 Consequently, researchers were integrating activities into the MBAT program based on the core components of CBT-I to improve sleep quality in older adult.
Mindfulness-based art therapy (MBAT) combines mindfulness practices with artistic expression to enhance awareness of emotions and promote self-reflection.21 This approach encourages being present without judgment, using art as a means for self-expression, which can reduce anxiety and depression while improving emotional stability.22 The therapeutic process typically involves foundational mindfulness exercises, such as breath awareness, emotional exploration, and the recognition of present-moment experiences, alongside various artistic activities. Participants engage with art in a spontaneous and non-aesthetic manner, employing techniques such as drawing, painting, or sculpting. This approach facilitates non-verbal connections with thoughts and feelings, leading to enhanced self-awareness and the release of suppressed emotions. Furthermore, the MBAT fosters a constructive relationship with oneself by encouraging self-acceptance and minimizing judgmental comparisons.23–25 A review of the literature indicates that MBAT, specifically through mandala coloring, can significantly reduce stress, anxiety, and depression while enhancing daily functioning in elderly. Interventions have a single session of 20 minutes twice a week over a span of eight weeks.26–28
A recent systematic review and meta-analysis examined the impact of mindfulness meditation on sleep quality. The review found that mindfulness meditation has been studied in various clinical populations with sleep disturbances, but there are relatively few studies involving older adults. Most of the programs conducted lasted 6 to 8 weeks and included CBT-I, mind-body bridging (MBB), and mindfulness-based stress reduction (MBSR), among others. Additionally, the analysis indicated that there was no significant difference in effectiveness between mindfulness meditation and established sleep treatments. Thus, more research is needed, especially focused on older adult populations.16 Consequently, this study seeks to investigate whether the MBAT program, utilizing mandala coloring, can effectively improve sleep quality and mindfulness awareness attention.
The significant benefits of improved sleep quality and mindful attention for older adults, derived from the MBAT program utilizing mandala coloring, are not widely recognized in Thailand or internationally. This study aims to evaluate the effectiveness of the MBAT program, which is rooted in CBT-I19 and relevant prior research. We utilized the LINE application for health communication and information dissemination to compare levels of sleep quality, depression anxiety stress, and mindful attention awareness scores among older adults before (week 1) and after (week6) the MBAT program, as well as during follow-up assessments (week 10).
Materials and Methods
A single group repeated measures trial was conducted to examine the effects of the MBAT program. This study was registered at the Thai Clinical Trials Registry (TCTR20250409001).
Participants
The study focused on older adults residing in urban Bangkok, Thailand. Data collection occurred between March and May 2025. To reduce potential selection bias and enhance comparability, a total of 35 participants were randomly chosen from 98 volunteers who met the inclusion criteria. The criteria for inclusion were as follows: (1) participants must be aged 60 or older; (2) they must experience sleep quality issues, indicated by scores exceeding 5 on the Pittsburgh Sleep Quality Index (PSQI); (3) participants should not be enrolled in any therapy programs that could influence the study outcomes; (4) they should not have severe health conditions, such as heart disease or uncontrolled diabetes, that would prevent them from participating in activities; (5) participants must be able to understand and follow instructions for both online and onsite activities; and (6) they must be willing to participate in the study. The effect size of this study was calculated using the equation,29 with a minimum effect size of each variable from relevant studies.26,30 A power analysis conducted using G-Power software version 3.1.9 determined that an effect size of −0.63, a desired power of 0.95, and a significance level of 0.050, a sample size of 29 participants per group is sufficient. To account for potential attrition, an additional 20% was added, bringing the total number of participants to 35.
Intervention
The 6-week MBAT program implemented in this study was structured into three sessions, as shown in Table 1.
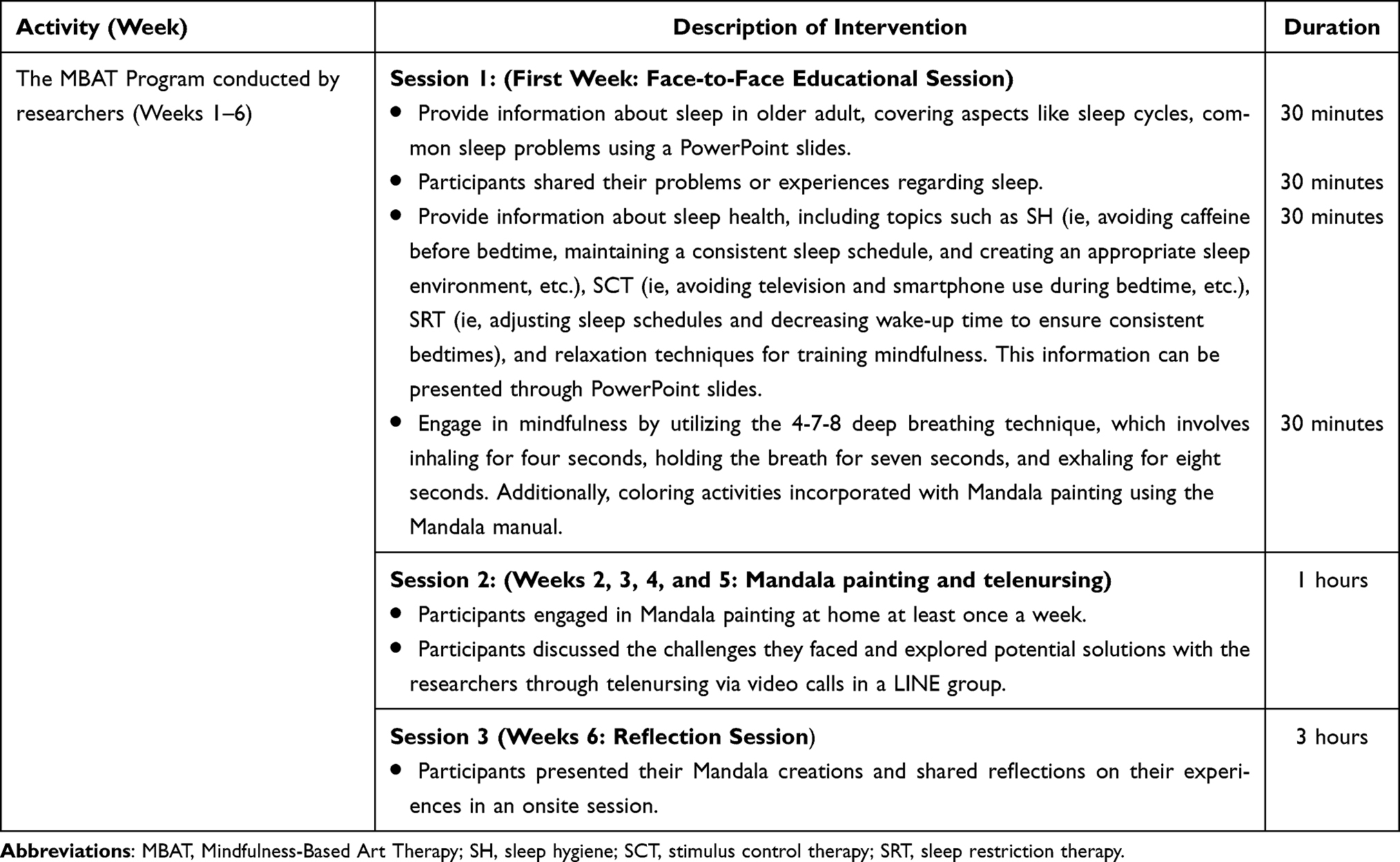 |
Table 1 The MBAT Program Protocol |
The MBAT program is a comprehensive research intervention developed based on the principles of CBT-I, as detailed by Walker et al19 and prior study.13–16 This program is designed to address the challenges older adults face when initiating and sustaining sleep, making it particularly relevant for those suffering from insomnia. The intervention focused on five core treatment components: (1) Cognitive Therapy (CT) to address negative thought patterns and beliefs related to sleep. It emphasizes identifying cognitive distortions and involves participants described the situations that trigger these thoughts and their emotional reactions and using mandala painting to express their feelings. This approach aims to reduce anxiety related to sleep performance and promote more restful sleep; (2) Sleep Hygiene (SH) education: participants received education on the practices that contribute to healthy sleep habits. This includes guidance on maintaining a conducive sleep environment, establishing consistent sleep schedules, and avoiding stimulants close to bedtime, which can significantly enhance overall sleep quality; (3) Stimulus Control Therapy (SCT): this strategy helps participants create positive associations with their sleep environment. SCT recommends specific behaviors, such as using the bed only for sleep and intimacy, to strengthen the mental connection between the bed and sleep, which can lead to improved sleep onset; (4) Sleep Restriction Therapy (SRT): by initially limiting the amount of time participants spent in bed, this approach aims to increase sleep efficiency. Participants gradually adjust their sleep schedules to find the optimal amount of sleep they need, which can lead to deeper and more restorative sleep; (5) Relaxation Therapy by using mandala painting. This innovative approach incorporates mandala painting as a form of relaxation therapy. This creative activity can help participants reduce stress and anxiety, fostering a calm mental state conducive to sleep. Additionally, weekly follow-up telenursing sessions were conducted via video group calls on LINE over four weeks to enhance the program’s effectiveness. These sessions serve not only to reinforce the skills learned but also to provide participants with ongoing social support. This supportive environment encourages individuals to share their experiences, celebrate successes, and address any challenges they face in adopting healthier sleep behaviors, ultimately reinforcing their commitment to improving their sleep health.
The MBAT program was implemented over a six-week period. In the first week, researchers educated participants on sleep health topics such as sleep in older adults, sleep hygiene, stimulus control, sleep restriction, and relaxation techniques through Mandala painting. From weeks two to five, participants attended weekly Mandala painting sessions, discussing sleep problem, shared feeling, and solutions with researchers by using telenursing via one-hour video calls in a LINE group. In the final week, participants presented their Mandala creations and shared reflections (week6). A follow-up was held one month later to evaluate ongoing impact (week 10) (Table 1).
Outcomes and Measurement
The research employed two types of instruments: one for data collection and the other for intervention. To assess content validity, the Item-Objective Congruence (IOC) index score was evaluated by three experts, all of whom were nursing instructors with expertise in older adult and mental health care. Permission was obtained from the developer to use all instruments. The data collection instruments included:
The Personal Information Questionnaire, which was comprised of six items, was developed by the researcher to collect demographic data, including gender, age, level of education, marital status, underlying, and history of sleeping pill use.
The Pittsburgh Sleep Quality Index (PSQI), developed by Buysse et al.31 The Thai version was translated by Sitasuwan et al.32 This index comprises seven components: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. Each component is assessed using a 4-point Likert scale, reflecting sleep behaviors, where a score of “0” indicates optimal sleep behavior and a score of “3” signifies poor sleep behavior. The cumulative score ranges from 0 to 21 points. A total score of 5 or less indicates good sleep quality, whereas a score exceeding 5 denotes poor sleep quality.
Depression Anxiety Stress Scales (DASS-21), originally developed by Lovibond and Lovibond,33 was culturally adapted for Thai populations by Oei et al.34 DASS-21 encompasses 21 items categorized into three dimensions: depression, anxiety, and stress, each containing seven items. Responses for each dimension are measured on a 4-point Likert scale, representing the prevalence of emotional states. A score of “0” corresponds to “ Did not apply to me at all”, while a score of “3” indicates “ Applied to me very much or most of the time”. For older adults, the classification of DASS-21 scores is as follows: normal (0–9), mild (10–13), moderate (14–20), severe (21–27), and extremely severe (28 or higher).
The Mindful Attention Awareness Scale (MAAS), developed by Brown and Ryan,35 was translated into a Thai version by Santivong.36 This scale consists of 15 items. Responses are evaluated on a 6-point Likert scale, which reflects individuals’ experiences and their sensitive awareness of what is happening in the present moment. The scale emphasizes measuring the level of awareness and mindfulness in everyday life. A score of “1” indicates “Almost Always”, while a score of “6” represents “Almost Never.” The total score ranges from 15 to 90 points, with higher scores indicating greater awareness and mindfulness among older adults.
In this study, the average IOC score of the PSQI, DASS-21, and MAAS was 0.67–1.00, indicating an acceptable level, while the Cronbach’s Alpha was 0.80, representing an acceptable reliability coefficient.
Ethical Considerations
This research received approval from the Human Ethics Committee of Boromarajonani College of Nursing in Nakhon Ratchasima (COA No. 38/2567) located in Nakhon Ratchasima, Thailand. The study was conducted in accordance with the principles of the Declaration of Helsinki. Prior to their participation in the study, the researcher provided a comprehensive explanation of the research objectives, data collection methods, potential benefits, and the rights of participants, which included the option to withdraw without any repercussions on their care. Participants were actively encouraged to ask questions and willingly signed informed consent documents prior to their decision-making. All data collected remained confidential and was reported solely in terms of overall findings.
Data Collection
Researchers conducted a thorough review of the application materials submitted by volunteers to identify individuals who satisfied the study’s inclusion criteria. From an initial pool of 98 volunteers, 35 participants were selected at random. Those who expressed interest and met the eligibility requirements were formally invited to take part in the study. Researchers provided a verbal overview of the informal consent process (ie, the right to participate, the ability to withdraw at any time, the benefits they received, and the program’s process), after which participants completed and signed the informed consent form. Data collection was facilitated using Google Forms, allowing participants to independently record their responses before the commencement of the program (week 1), following the program’s conclusion (week 6), and during a follow-up period (week 10). The data included Personal Information (collected only during the first week), PSQI, DASS-21, and MAAS (Figure 1).
 |
Figure 1 Study Flow Chart. |
Statistical Analysis
Data were analyzed utilizing SPSS version 29. The demographic data were presented using descriptive statistics, which included frequency, percentage, mean, and standard deviation (SD), based on the scale of the variables. Following the verification of the normal distribution of the dependent variables through the Shapiro–Wilk test (for sample sizes less than 50). To assess the normality of the data, we used skewness and kurtosis metrics (ie, standardized values within the range of −1.96 to 1.96 indicate a normal distribution). When the normality assumptions were confirmed, we conducted a one-way repeated measures analysis of variance (ANOVA) to evaluate changes in the hypothesized outcomes at three time points: baseline, 6 weeks, and 10 weeks. If the data did not meet the criteria for normal distribution, we employed the Friedman test as an alternative method.
Results
Demographic Data
Participants in this study were 35 older adults (N =35) and were in urban areas in Bangkok, Thailand. The sample predominantly comprised females, accounting for 97.10%, with a mean age of 67.03 years (SD = 4.17). In terms of marital status, 37.10% of participants were either single or in a relationship. The highest educational attainment among the respondents was a bachelor’s degree (74.30%). Hypertension was identified as the most common underlying health condition (28.60%), followed by dyslipidemia (25.70%). Furthermore, 62.90% of sample opted not to use sleeping medication. Prior to their participation in the study, it was observed that 31.40% of individuals went to bed between 11:00 PM and midnight, while 51.40% reported waking between 4:00 AM and 6:00 AM. Additionally, 48.60% of participants took more than 30 minutes to initiate sleep, and 51.40% indicated they slept for fewer than 6 hours per night (Table 2).
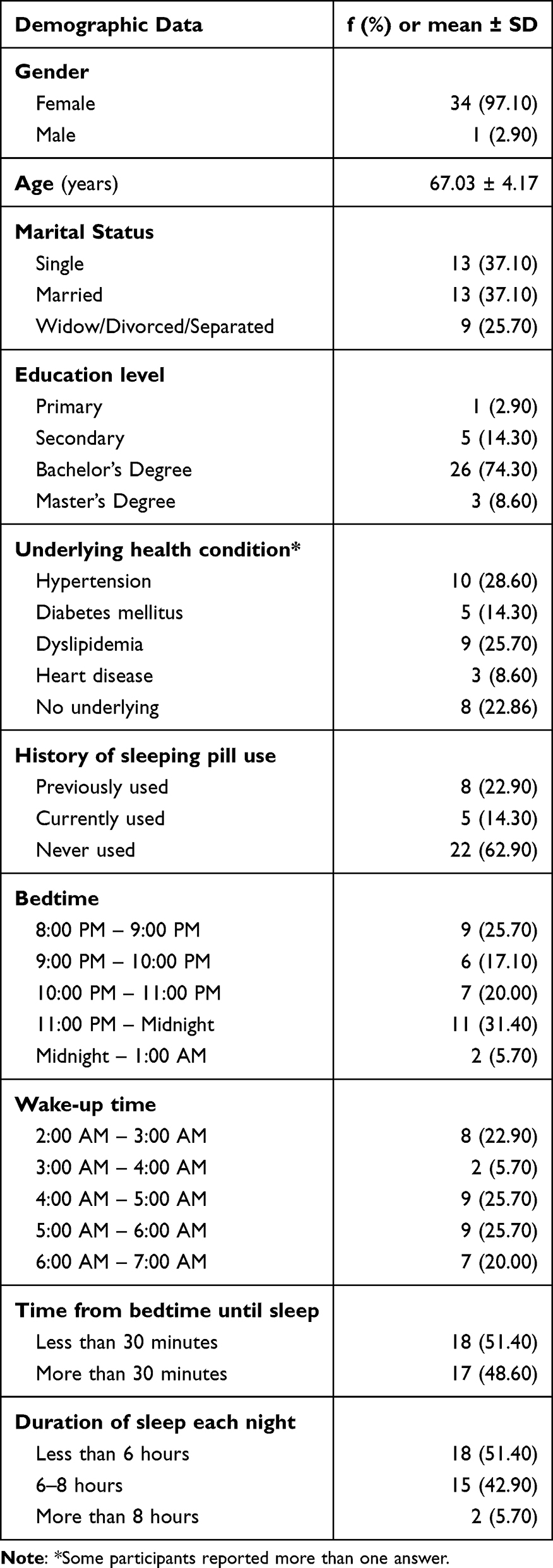 |
Table 2 Demographic Data of Participants (N = 35) |
Intervention Effects
Table 3 presents the outcomes of the intervention, which encompassed patient-reported measures such as sleep quality, depression anxiety stress, and mindful attention awareness.
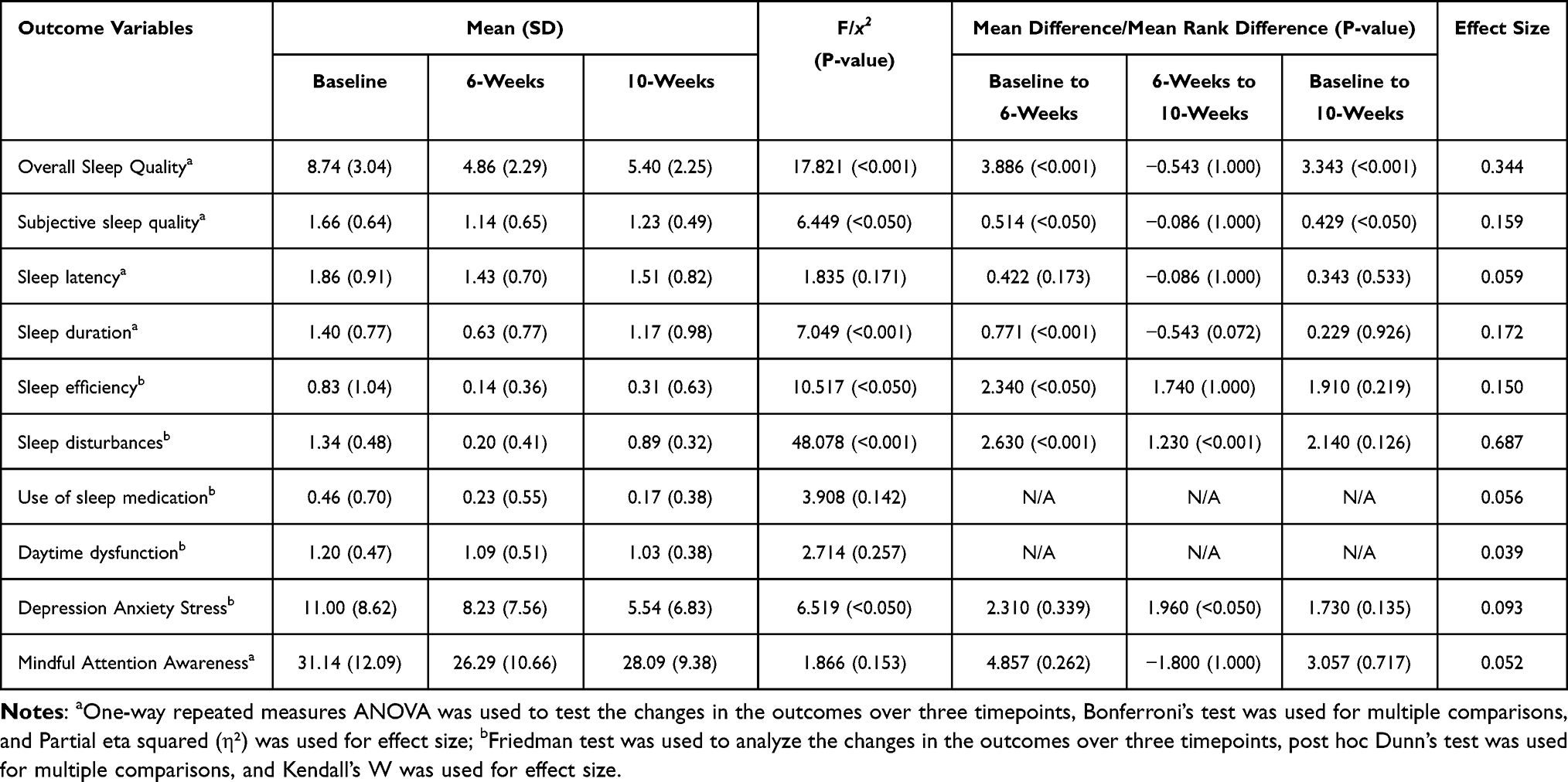 |
Table 3 Means and Mean Differences at Baseline, 6-Weeks, and 10-Weeks (N = 35) |
Sleep Quality
The findings indicated a significant improvement in the overall sleep quality scores by using the PSQI (F = 17.821, p < 0.001), as well as in specific PSQI components, including subjective sleep quality (F = 6.449, p < 0.050), sleep duration (F = 7.049, p < 0.001), sleep efficiency (χ² = 10.517, p < 0.050), and sleep disturbances (χ² = 48.078, p < 0.001). However, some components did not show significant differences, including sleep latency (F = 1.835, p > 0.050), use of sleep medication (χ² = 3.908, p > 0.050), and daytime dysfunction (χ² = 2.714, p > 0.050).
Multiple comparisons revealed that participants showed significant improvement in overall sleep quality scores from baseline to the 6 weeks and from baseline to 10 weeks (p < 0.001 and < 0.001, respectively). For each sleep quality component, the multiple comparisons for sleep latency demonstrated no statistically significant differences between baseline and 6 weeks (p > 0.050). However, significant improvements were observed in subjective sleep quality, sleep duration, sleep efficiency, and sleep disturbances (p < 0.050, < 0.001, < 0.050, and < 0.001, respectively). When comparing scores between 6 weeks and 10 weeks, there were no statistically significant differences in overall sleep quality scores, subjective sleep quality, sleep latency, sleep duration, and sleep efficiency (p > 0.050). However, there was a significant difference in sleep disturbances (p < 0.001). Comparing scores between baseline and 10 weeks revealed statistically significant differences in subjective sleep quality (p < 0.050), but no significant differences in sleep latency, sleep duration, sleep efficiency, and sleep disturbances (p > 0.050). Additionally, the components related to the use of sleep medication and daytime dysfunction did not show significant changes across the three time points, suggesting that the program may need to be extended for greater impact.
Depression Anxiety Stress
The findings demonstrated a significant improvement in depression anxiety stress scores as assessed by the DASS-21 over 10 weeks (F = 6.519, p < 0.050). Multiple comparisons indicated that participants exhibited significant improvement from the 6 weeks to the 10 weeks (p < 0.050). Effect sizes, as measured by Kendall’s W, revealed a large effect size. However, there were no statistically significant differences observed between baseline and the 6 weeks assessment, as well as no significant differences between baseline and the 10 weeks assessment.
Mindful Attention Awareness
The findings indicated no significant improvement in mindful attention awareness scores, as assessed by MAAS over the 10 weeks (p > 0.050). Multiple comparisons showed that participants did not exhibit significant improvements across the three time points (p > 0.050). Effect sizes, as measured by Partial eta squared (η²), revealed a medium effect size.
Discussion
In this study, we aimed to examine the effects of the MBAT program, integrating principles of CBT-I along with Mandala painting and telenursing, on several psychological and sleep-related outcomes among older adults (ie, sleep quality, depression anxiety stress, and mindful attention awareness). We assessed participants at three different time points: baseline, 6 weeks, and 10 weeks, to evaluate any changes over time.
Our findings demonstrated that the MBAT program led to significant improvements in depression anxiety stress (p < 0.050) and overall sleep quality (p < 0.001), These improvements suggest a meaningful impact of the program on the psychological well-being of older adults. The findings suggest that the MBAT program, with a particular emphasis on Mandala coloring, has a positive impact on the emotional well-being of older adults. This conclusion is consistent with previous studies conducted in Taiwan,26 Indonesia,27 and Iran.28 These studies demonstrated that older adults who participated in Mandala coloring sessions for 20 minutes per week (either once or twice a week), over a duration of 6 to 8 weeks, experienced significant improvements in their levels of depression, anxiety, and stress. Such outcomes underscore the effectiveness of this approach in enhancing emotional health among older adults. A fundamental component of this therapeutic approach is the practice of mindfulness, wherein individuals concentrate on the present moment without judgment, employing art as a medium for self-expression and introspection. This methodology has the potential to foster relaxation and alleviate mental stress, which may lead to physiological effects such as a decrease in cortisol levels, the hormone associated with stress.37 Elevated cortisol levels can disrupt hormonal balance and accelerate the aging process. By facilitating relaxation and the release of emotions, the MBAT program may contribute to the normalization of cortisol levels.38 These findings indicate that the MBAT program can enhance self-awareness and promote the expression of repressed emotions, resulting in a significant reduction in symptoms related to depression, anxiety, and stress.
Moreover, participants who engaged in the MBAT program reported notable improved in sleep quality. Specific areas of enhancement included subjective sleep quality (p < 0.050), sleep duration (p < 0.001), sleep efficiency (p < 0.050), and reductions in sleep disturbances (p < 0.001). These results highlight the potential of the MBAT program to foster healthier sleep patterns and overall mental health in older individuals. The finding aligns with a study of older adults in the USA who had moderate sleep disturbances.30 The 6-week mind-body medicine intervention included six 2-hour sessions featuring mindfulness exercises such as mindful sitting, eating, and walking. Participants spent 10 to 30 minutes on experiential practice each class, along with teacher-led instruction and group discussions. The study found significant improvements in sleep quality and a reduction in depression symptoms. Additionally, CBT-I (ie, education on sleep hygiene, stimulus control, sleep restriction, relaxation techniques, and weekly telenursing sessions) along with mindfulness is an effective approach that assists individuals in establishing a consistent sleep routine. This structured therapy may influence serotonin levels in the brain, which mainly produced in the dorsal raphe nucleus, is known to promote wakefulness and inhibit REM sleep.39 The findings are consistent with a study conducted on older adults in Australia,20 which examined three groups: a standard CBT-I group, a CBT-I group plus mood strategies, and a control group receiving psychoeducation over an eight-week period. The results indicated that both the standard CBT-I group and the CBT-I plus mood strategies group experienced significantly greater improvements in insomnia and depression severity compared to the psychoeducation group. These outcomes suggest that both CBT-I and the inclusion of mood strategies may effectively enhance sleep quality and mental health among aging individuals. Therefore, the MBAT program may play a role in enhancing serotonin activity. Through practices that combine mindfulness techniques with creative expression, individuals may experience greater emotional awareness and engagement. This combination can lead to improved mood and increased alertness, making MBAT a valuable complement to CBT-I in promoting overall sleep quality.
The findings revealed that there were no significant changes in certain aspects of sleep quality (ie, sleep latency, the use of sleep medication, and daytime dysfunction) and mindful attention awareness scores at three different time points (p > 0.050). In comparing the baseline (pre-intervention) and six weeks (post-intervention), which showed an improvement in those components of sleep quality. These findings are consistent with prior studies, which have shown mixed outcomes in these areas. For instance, Black et al30 reported that mindfulness meditation improved overall sleep quality, although the improvements in sleep latency were modest. Similarly, González-Martín et al40 noted small effect sizes for sleep onset latency among older adults participating in mindfulness-based cognitive therapy. Although our study did not find significant improvements in quantitative measures of mindfulness awareness attention scores, participants shared qualitative feedback indicating increased emotional insight and relaxation during Mandala painting. They reflected that the color red represents anger, while green and blue symbolize calmness. While coloring, many participants felt more relaxed and even sleepy. In the initial week, the shapes of the mandala are simple; a week later, they become more complex, providing participants with deeper meditation and time to reflect on their feelings. However, a few participants struggled with coloring and found it difficult to adjust their sleep routines due to work commitments. Thus, this indicates that although the program offered various benefits, challenges related to sleep maintenance and medication use may continue. This observation aligns with the findings of Campenni and Hartman,41 who noted enhanced state mindfulness through art-based interventions. These results suggest that while MBAT may not result in immediate changes to certain sleep parameters or mindfulness metrics, it fosters subjective improvements in emotional regulation and relaxation, both of which are important for long-term mental health. Future research might consider longer intervention periods or alternative measurement tools to more effectively capture these nuanced effects.
The MBAT program, which combines CBT-I, Mandala painting, and telenursing, showed significant improvements in both sleep quality and psychological well-being among older adults. Participants reported increased emotional awareness and relaxation through mindfulness-based creative expression. Despite some limitations, the program offers a promising holistic approach to enhancing mental health and sleep in the older adults. Thus, the program offers a practical, cost-effective, and culturally sensitive approach to improving sleep and mental health in older adults. It should be implemented in rural or remote areas, particularly where access to mental health services is limited. Trained nurses can facilitate the program, which promotes emotional awareness and relaxation through creative expression using Mandala painting. These findings suggest that the MBAT program could be integrated into primary health care to enhance sleep quality among the elderly and could also be adapted for other vulnerable populations.
Strengths
The strengths of the MBAT program include its innovative approach that combines CBT-I with Mandala painting and telenursing, making it accessible and engaging for older adults. The integration of telenursing allows for flexible participation, ensuring that individuals can engage in sessions from the comfort of their homes. Furthermore, the focus on creative expression provides a unique avenue for processing emotions and enhancing mental health. Moreover, the longitudinal design of the study allows for the observation of changes over time, offering insights into the sustained effects of the MBAT program.
Limitations
Despite these strengths, the study has limitations that should be acknowledged. The small sample size may limit the generalizability of the findings. Additionally, the lack of significant results in mindful attention awareness suggests that further exploration is needed to determine the factors contributing to these outcomes. There may also be individual differences in participants’ openness to art therapy that could influence the program’s effectiveness. Additionally, self-reported measures may introduce response biases, as participants may have differing interpretations of the scales used.
Recommendations
To enhance the efficacy of the MBAT program, future research should consider a larger and more diverse sample size to assess its effectiveness across different demographics. Additionally, incorporating additional measures follow-up assessments beyond 10 weeks to evaluate mindfulness explicitly and exploring the long-term effects of the program on mental health would also be beneficial. Moreover, integrating feedback from participants can help refine the program’s components, ensuring it meets the evolving needs of older adults seeking mental health support.
Conclusion
The findings of this study suggest that the MBAT program, which incorporates CBT-I with Mandala painting and telenursing, can significantly enhance sleep quality and depression anxiety stress among older adults both at the conclusion of the program and during a follow-up assessment. Therefore, the MBAT program should be considered an effective intervention for addressing sleep disorders in this population. Future studies should extend a longer period of intervention and follow-up.
Data Sharing Statement
Data supporting this study are available from the corresponding author.
Acknowledgments
We would like to express our sincere gratitude to all participants for their dedicated time and effort throughout the various stages of this study. Additionally, we would like to acknowledge the generous funding provided by Boromarajonani College of Nursing, Nakhon Ratchasima.
Funding
This study was funded by Boromarajonani College of Nursing, Nakhon Ratchasima.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Du M, Liu M, Wang Y, Qin C, Liu J. Global burden of sleep disturbances among older adults and the disparities by geographical regions and pandemic periods. SSM Popul Health. 2024;25:101588. doi:10.1016/j.ssmph.2023.101588
2. Aunjitsakul W, Pitanupong J, Werachattawan N. Sleep quality among elderly people in Songkhla Province, Thailand: a two-stage cluster sampling study. J Med Assoc Thailand. 2018;101(1):137–144.
3. Siripanich C, Somrongthong R, Kanthawee P. Health status and behavior influencing sleep quality among community-dwelling elderly in Chanthaburi province, Thailand. J Health Res. 2018;32(Suppl 2):S151–S158. doi:10.14456/jhr.2018.17
4. Jamwong P, Borisuth P, Chaiwoot K, et al. Prevalence and predictive factors of poor sleep quality among the elderly in the urban areas of Lampang Province, Northern Thailand. J Health Res. 2024;38(4):311–321. doi:10.56808/2586-940X.10882
5. Morssinkhof MWL, van Wylick DW, Priester-Vink S, et al. Associations between sex hormones, sleep problems and depression: a systematic review. Neurosci Biobehav Rev. 2020;118:669–680. doi:10.1016/j.neubiorev.2020.08.006
6. Zhou P, Li H, Li H, Chen Y, Lv Y. A possible important regulatory role of estrogen in obstructive sleep apnea hypoventilation syndrome. Front Med Lausanne. 2025;12:1369393. doi:10.3389/fmed.2025.1369393
7. Eslami V, Zimmerman ME, Grewal T, Katz M, Lipton RB. Pain grade and sleep disturbance in older adults: evaluation the role of pain, and stress for depressed and non-depressed individuals. Int J Geriatr Psychiatry. 2016;31(5):450–457. doi:10.1002/gps.4349
8. Koffel E, McCurry SM, Smith MT, Vitiello MV. Improving pain and sleep in middle-aged and older adults: the promise of behavioral sleep interventions. Pain. 2019;160(3):529–534. doi:10.1097/j.pain.0000000000001423
9. Brouwer A, van de Ven PM, Kok A, Snoek FJ, Beekman ATF, Bremmer MA. Symptoms of depression and insomnia in older age: a within-individual analysis over 20 years. J Am Geriatr Soc. 2022;70(7):2051–2059. doi:10.1111/jgs.17765
10. Irwin MR, Boyle CC, Cho JH, et al. Sleep and Healthy Aging Research on Depression (SHARE-D) randomized controlled trial: protocol overview of an experimental model of depression with insomnia, inflammation, and affect mechanisms in older adults. Brain Behav Immun Health. 2023;28:100601. doi:10.1016/j.bbih.2023.100601
11. Gulia KK, Kumar VM. Sleep disorders in the elderly: a growing challenge. Psychogeriatrics. 2018;18(3):155–165. doi:10.1111/psyg.12319
12. Cohen ZL, Eigenberger PM, Sharkey KM, Conroy ML, Wilkins KM. Insomnia and other sleep disorders in older adults. Psychiatr Clin North Am. 2022;45(4):717–734. doi:10.1016/j.psc.2022.07.002
13. Huang K, Li S, He R, et al. Efficacy of cognitive behavioral therapy for insomnia (CBT-I) in older adults with insomnia: a systematic review and meta-analysis. Australas Psychiatry. 2022;30(5):592–597. doi:10.1177/10398562221118516
14. Rossman J. Cognitive-behavioral therapy for insomnia: an effective and underutilized treatment for insomnia. Am J Lifestyle Med. 2019;13(6):544–547. doi:10.1177/1559827619867677
15. Jakobsson Støre S, Jakobsson N. The effect of Mandala coloring on state anxiety: a systematic review and meta-analysis. Art Ther. 2022;39(4):173–181. doi:10.1080/07421656.2021.2003144
16. Rusch HL, Rosario M, Levison LM, et al. The effect of mindfulness meditation on sleep quality: a systematic review and meta-analysis of randomized controlled trials. Ann N Y Acad Sci. 2019;1445(1):5–16. doi:10.1111/nyas.13996
17. Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD. Management of chronic insomnia disorder in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2016;165(2):125–133. doi:10.7326/m15-2175
18. Hinrichsen GA, Leipzig RM. Efficacy of cognitive behavioral therapy for insomnia in geriatric primary care patients. J Am Geriatr Soc. 2021;69(10):2993–2995. doi:10.1111/jgs.17319
19. Walker J, Muench A, Perlis ML, Vargas I. Cognitive Behavioral Therapy for insomnia (CBT-I): a primer. Klin Spec Psihol. 2022;11(2):123–137. doi:10.17759/cpse.2022110208
20. Sadler P, McLaren S, Klein B, Harvey J, Jenkins M. Cognitive behavior therapy for older adults with insomnia and depression: a randomized controlled trial in community mental health services. Sleep. 2018;41(8). doi:10.1093/sleep/zsy104
21. Jang SH, Lee JH, Lee HJ, Lee SY. Effects of mindfulness-based art therapy on psychological symptoms in patients with coronary artery disease. J Korean Med Sci. 2018;33(12):e88. doi:10.3346/jkms.2018.33.e88
22. Geiger PJ, Boggero IA, Brake CA, et al. Mindfulness-based interventions for older adults: a review of the effects on physical and emotional well-being. Mindfulness. 2016;7(2):296–307. doi:10.1007/s12671-015-0444-1
23. Beerse ME, Van Lith T, Pickett SM, Stanwood GD. Biobehavioral utility of mindfulness-based art therapy: neurobiological underpinnings and mental health impacts. Exp Biol Med. 2020;245(2):122–130. doi:10.1177/1535370219883634
24. Jalambadani Z. The Effectiveness of Mindfulness-Based Art Therapy (MBAT) on healthy lifestyle in iranian menopausal women. J Lifestyle Med. 2020;10(1):44–48. doi:10.15280/jlm.2020.10.1.44
25. Rieger KL, Lobchuk MM, Duff MA, et al. Effectiveness of mindfulness-based arts interventions on psychological wellbeing and fatigue in adults with a physical illness: a systematic review protocol. JBI Database System Rev Implement Rep. 2018;16(7):1476–1484. doi:10.11124/jbisrir-2017-003446
26. Koo M, Chen HP, Yeh YC. Coloring activities for anxiety reduction and mood improvement in Taiwanese community-dwelling older adults: a randomized controlled study. Evid Based Complement Alternat Med. 2020;2020:6964737. doi:10.1155/2020/6964737
27. Hasnida H, Meutia A. The effectiveness of Mandala therapy on coping stress. In: Proceedings of the 2nd International Conference on Social and Political Development (ICOSOP 2017); October 25–26, 2017; Medan, Indonesia. Atlantis Press. doi:10.2991/icosop-17.2018.45
28. Ahmadi P, Alaee N, Foroughan M. The effect of coloring mandalas on depression, anxiety and stress in elderly people referred to daily rehabilitation center for the elderly in Tehran: a clinical trial. Iran J Nurs. 2023;35:642–655. doi:10.32598/ijn.35.140.3242
29. Glass GV. Primary, secondary, and meta-analysis of research. Educ Researcher. 1976;5(10):3–8. doi:10.2307/1174772
30. Black DS, O’Reilly GA, Olmstead R, Breen EC, Irwin MR. Mindfulness meditation and improvement in sleep quality and daytime impairment among older adults with sleep disturbances: a randomized clinical trial. JAMA Intern Med. 2015;175(4):494–501. doi:10.1001/jamainternmed.2014.8081
31. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
32. Sitasuwan T, Bussaratid S, Ruttanaumpawan, P, Chotinaiwattarakul, W. Reliability and validity of the Thai version of the Pittsburgh Sleep Quality Index. J Med Assoc Thai. 2014, Mar;97(Suppl 3):S57–67
33. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety Stress Scales
34. Oei TP, Sawang S, Goh YW, Mukhtar F. Using the depression anxiety stress scale 21 (DASS-21) across cultures. International J Psychol. 2013;48(6):1018–1029. doi:10.1080/00207594.2012.755535
35. Brown KW, Ryan RM. The benefits of being present: Mindfulness and its role in psychological well-being. J Pers Soc Psychol. 2003;84(4):822–848. doi:10.1037/0022-3514.84.4.822
36. Santivong R. Mindfulness-based cognitive therapeutic intervention in caring for depression. Thesis for Master of Nursing Sciences (Chonburi, Thailand: Burapha University). 2007.
37. Zhang MQ, Liu X, Huang Y. Does Mandala art improve psychological well-being in patients? A systematic review. J Integr Complement Med. 2024;30(1):25–36. doi:10.1089/jicm.2022.0780
38. Van Lith T, Cheshure A, Pickett SM, Stanwood GD, Beerse M. Mindfulness based art therapy study protocol to determine efficacy in reducing college stress and anxiety. BMC Psychology. 2021;9(1):134. doi:10.1186/s40359-021-00634-2
39. Strasser E. The Neuroscience of Mindfulness Based Art Therapy: A Literature Review. Lesley University; 2024. https://digitalcommons.lesley.edu/expressive_theses/904.
40. González-Martín AM, Aibar-Almazán A, Rivas-Campo Y, Marín-Gutiérrez A, Castellote-Caballero Y. Effects of mindfulness-based cognitive therapy on older adults with sleep disorders: a systematic review and meta-analysis. Front Public Health. 2023;11:1242868. doi:10.3389/fpubh.2023.1242868
41. Campenni CE, Hartman A. The effects of completing Mandalas on mood, anxiety, and state mindfulness. Art Ther. 2020;37(1):25–33. doi:10.1080/07421656.2019.1669980
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.