Back to Journals » Nutrition and Dietary Supplements » Volume 18
The Role of Interpersonal Communication in Promoting Adolescent Health and Nutrition: A Systematic Review
Authors Sari DN ![]() , Sunjaya DK
, Sunjaya DK ![]() , Sari P
, Sari P ![]() , Hilmanto D
, Hilmanto D ![]()
Received 18 October 2025
Accepted for publication 22 February 2026
Published 15 May 2026 Volume 2026:18 575328
DOI https://doi.org/10.2147/NDS.S575328
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Ara Kirakosyan
Video abstract of “Interpersonal Communication in Adolescent Health and Nutrition” [575328].
Views: 24
Dewi Nurlaela Sari,1,* Deni Kurniadi Sunjaya,2 Puspa Sari,3,* Dany Hilmanto4
1Doctoral Study Program, Faculty of Medicine, Universitas Padjadjaran, Bandung, Jawa Barat, Indonesia; 2Department of Public Health, Faculty of Medicine, Universitas Padjadjaran, Bandung, Jawa Barat, Indonesia; 3Vocational School, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 4Department of Child Health, Hasan Sadikin Hospital, Faculty of Medicine, Universitas Padjadjaran, Bandung, Jawa Barat, Indonesia
*These authors contributed equally to this work
Correspondence: Dany Hilmanto, Department of Child Health, Hasan Sadikin Hospital, Faculty of Medicine, Universitas Padjadjaran, Bandung, Jawa Barat, 45363, Indonesia, Email [email protected]
Objective: Adolescent health and nutrition remain critical global public health priorities. Interpersonal communication (IPC) is increasingly utilized as a strategy to influence adolescents’ health-related behaviors across peer, family, school, healthcare, and digital contexts. However, evidence regarding its effectiveness remains heterogeneous. This systematic review synthesizes recent evidence on IPC interventions targeting adolescent health and nutrition outcomes.
Methods: This systematic review followed PRISMA 2020 guidelines. Four databases (PubMed, Scopus, Web of Science, and CINAHL) were searched for studies published between January 2021 and March 2025. Of 4430 identified records, 3,912 titles and abstracts were screened after duplicate removal (n=518), and 126 full texts articles were assessed for eligibility. Fourteen studies met the inclusion criteria. Due to heterogeneity in study designs and outcome measures, findings were synthesized narratively.
Results: Studies conducted across Asia, Africa, Europe and North America examined IPC delivered through peer-led communication, family-based discussions, teacher-facilitated programs, healthcare provider counseling, and digitally mediated exchanges. Most studies reported improvements in intermediate outcomes, including knowledge, self-efficacy, behavioral intentions, and attitudes. Several quasi-experimental and longitudinal studies suggested potential behavioral improvements; however, many cross-sectional and digital communication studies demonstrated associative rather than causal relationships.
Conclusion: IPC interventions are consistently associated with favorable intermediate outcomes in adolescent health and nutrition promotion. However, robust evidence on sustained behavioral and objective health outcomes remains limited. Future research should employ rigorous longitudinal and experimental designs and integrate objective health indicators to strengthen causal inference and translational impact.
Keywords: adolescent health, komunikasi antarpribadi, health promotion, nutrition behavior
Introduction
Adolescence is a critical transitional period between childhood and adulthood, encompassing individuals aged 10–19 years as defined by the World Health Organization.1 This life stage represents a sensitive development window during which rapid biological, cognitive, emotional and social changes interact to shape health behaviors with long-term consequences. Behaviors established during adolescence, including dietary practices and lifestyle choices, often persist into adulthood and contribute to future risks of non-communicable diseases and other adverse health outcomes.2–4
Puberty is characterized by substantial physiological changes driven by hormonal fluctuations, including increases in testosterone, estrogen, and growth hormone. These changes contribute to accelerated growth and increased muscle mass and are associated with elevated nutritional and energy requirements. Concurrently, adolescents experience ongoing maturation of executive function, heightened emotional reactivity, and increased sensitivity to social influences, particularly from peers. These developmental characteristics shape decision-making processes and may increase susceptibility to both health-promoting and health-compromising behaviors.5
A defining feature of adolescence is the progressive increase in autonomy, which enables greater independence in health-related behaviors such as dietary choices, physical activity, and substance use. While increased autonomy supports identity formation and self-regulation, it may also heighten vulnerability to unhealthy behaviors. Lifestyle factors such as tobacco use and alcohol consumption frequently emerge during adolescence and are often associated with unhealthy dietary patterns, underscoring this developmental stage as a critical period for preventive interventions.6
Late adolescence, particularly among individuals aged 18 years and above, overlaps with the phase of emerging adulthood. This transition is characterized by increased independence, reduced parental oversight, and shifts in educational and social environments. Evidence suggests that health-related behaviors adopted during this stage, including dietary habits, are likely to persist into later adulthood, highlighting the importance of targeted health promotion during this transition.7
Within these developmental contexts, interpersonal communication plays a central role in shaping adolescent health behaviors. In this review, interpersonal communication (IPC) is defined as interactive, bidirectional exchanges of information, meanings, and social support occurring through face-to-face or digitally mediated interactions between individuals, including peers, family members, educators, and healthcare providers.8 Drawing on behavioral and communication theories such as the Health Belief Model and social learning theory, IPC may influence adolescent health outcomes by enhancing knowledge, shaping social norm, strengthening perceived benefits and risks, improving self-efficacy, and ultimately supporting behavior change related to nutrition and other health practice.9
Although communication-based approaches are widely used in adolescent health promotion, the existing evidence remains fragmented. Previous reviews have primarily focused on individual behavioral interventions, school-based programs, mass media campaigns, or digital health interventions. However, the specific role of interpersonal communication across diverse relational contexts, such as peer, family, school, healthcare, and technology-supported interactions, has not been systematically mapped. As a result, there is limited understanding of how IPC in conceptualized, implemented, and evaluated in relation to nutrition-related health outcomes among adolescents.10,11
For the purpose of this review, interpersonal communication (IPC) is operationalized in two forms: (1) Structured IPC, referring to planned, theory-informed communication embedded within formal interventions (eg., peer-led programs, counseling sessions, teacher-facilitated discussions); and (2) Naturally occurring IPC, referring to spontaneous or routine exchanges among peers, family members, educators, healthcare providers outside structured intervention frameworks.
This review addresses this gap by focusing specifically on interpersonal communication as a cross-cutting mechanism influencing adolescent nutrition related health outcomes across multiple contexts. This review aims to (1) Identify the forms and modalities of interpersonal communication used in adolescent nutrition-related health promotion; (2) map the contexts In which these communication processes occur, including peer, family, school, healthcare, and digital settings; and (3) examine the types of nutrition-related outcomes assessed, such as knowledge, attitudes, self-efficacy and behavioral change.
Material and Methods
A comprehensive literature search was conducted using several electronic databases, including PubMed, Scopus, Web of Science, and CINAHL, as well as the search engine Google Scholar to identify relevant studies.11 The search covered publications published between 2021 and 2025 and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.12 The review was guided by a modified PICO framework. Population (P): adolescents aged 10–19 years. Intervention/Exposure (I): interpersonal communication (IPC) occurring within peer, family, school, healthcare, or digital relational contexts. Comparison (C): Usual practice, alternative interventions, or absence of structured IPC exposure (where applicable), and Outcomes (O): Intermediate cognitive and psychosocial outcomes (eg., knowledge, attitudes, intentions, self-efficacy), behavioral outcomes (eg., dietary practices, physical activity), and where reported, clinical or physiological indicators.13,14
The population comparised adolescents aged 10–19 years. The concept focused on interpersonal communication (IPC), defined as reciprocal, interactive communication processes occurring between adolescents and peers, family members, teachers, healthcare providers, or through technology-supported platforms (eg., digital messaging or online peer interaction). The primary context was health promotion and nutrition-related settings, including schools, families, healthcare facilities, communities and digital environments. Studies were eligible if they examined IPC related to nutrition knowledge, dietary behaviors, nutritional status, or health-related behaviors among adolescents. The keywords used in the search included combinations such as Adolescent, Youth, Teenager, Peer communication, Peer education, Peer-to-peer, Peer support, Health promotion, Health education, Nutrition, Physical activity, and Mental health. Boolean operators (AND, OR) and truncation techniques were applied to ensure a sensitive and comprehensive search across all selected databases.
A comprehensive search strategy was developed using a combination of keywords and controlled vocabulary terms related to interpersonal communication, adolescents, and nutrition. The full Boolean search strategies for each database are provided in the Supplementary Materials to ensure reproducibility.
Selection Criteria
Although early conceptual framing emphasized peer-to-peer communication, the inclusion criteria were intentionally broadened to capture interpersonal communication across multiple relational contexts, including family, school, healthcare, and digital environments. This broader scope reflects the social ecological influences shaping adolescent health behaviors.
Studies were included if they met the following criteria:
- Focused on adolescents aged 10–19 years.
- Investigated the role and impact of interpersonal communication (IPC) on health and/or nutrition outcomes.
- Employed qualitative, quantitative, or mixed methods study designs (eg.,Randomized controlled Trial (RCT), quasi-experimental, cohort, cross-sectional, ethnographic studies).
- Published in peer-reviewed journals in English.
- Reported measurable or observable outcomes related to adolescent health (eg., dietary behavior, mental health, physical activity, nutritional status).
Studies were excluded if they:
- Focused solely on mass media, social media, or non-interpersonal interventions without a component of direct person-to-person communication.
- Targeted populations outside the adolescent age range.
- Were editorials, reviews, commentaries, or conference abstracts without full data.
Literature Search
The initial search yielded 4.430 records. After removing duplicates, titles and abstracts were screened independently by two reviewers. Full-text articles were retrieved and assessed for eligibility based on the predefined inclusion criteria. Any disagreements between reviewers were resolved through discussion or consultation with a third reviewer. The final selection of studies is presented in a PRISMA flow diagram developed for this review (Figure 1), adapted from the PRISMA 2020 guidelines.
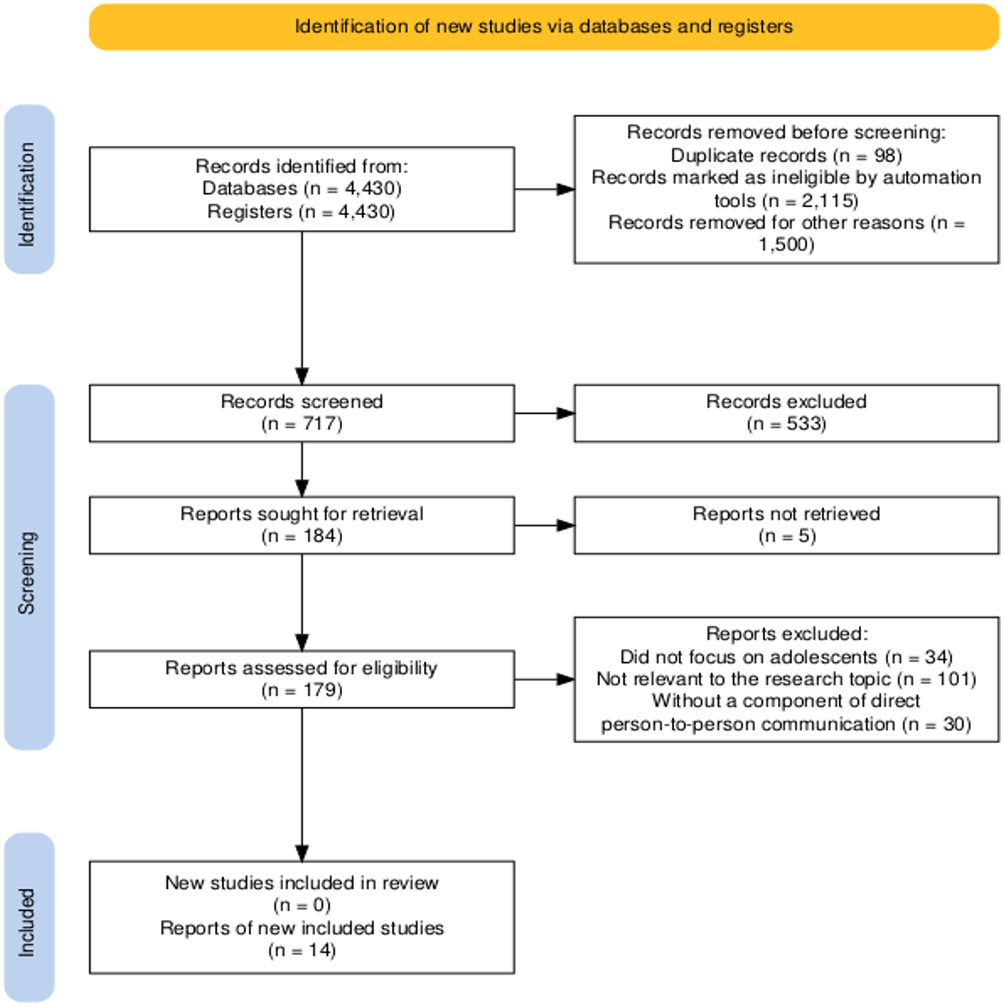 |
Figure 1 PRISMA flow diagram of study selection, adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.12 |
Quality Assessment
The methodological quality of included studies was assessed using appropriate Joanna Briggs Institute (JBI) Critical Appraisal Tools, tailored to each study designs (eg., RCTs, qualitative studies, cross-sectional surveys). Studies receiving full scores met all applicable methodological criteria according to the JBI checklist, however, a full score does not imply absence of contextual, behavioral, or implementation-related limitations, particularly in complex interpersonal communication interventions.
Each study was evaluated independently by two reviewers (NS and DS). Studies were categorized as high, moderate, or low quality based on the total score obtained from the checklist. Discrepancies in scoring were discussed until consensus was reached. The completed appraisal checklist is provided as Tables 1–4. Although study screening was conducted independently by two reviewers with discrepancies resolved through discussion, inter-rater agreement statistics (eg, Cohen’s kappa) were not calculated.
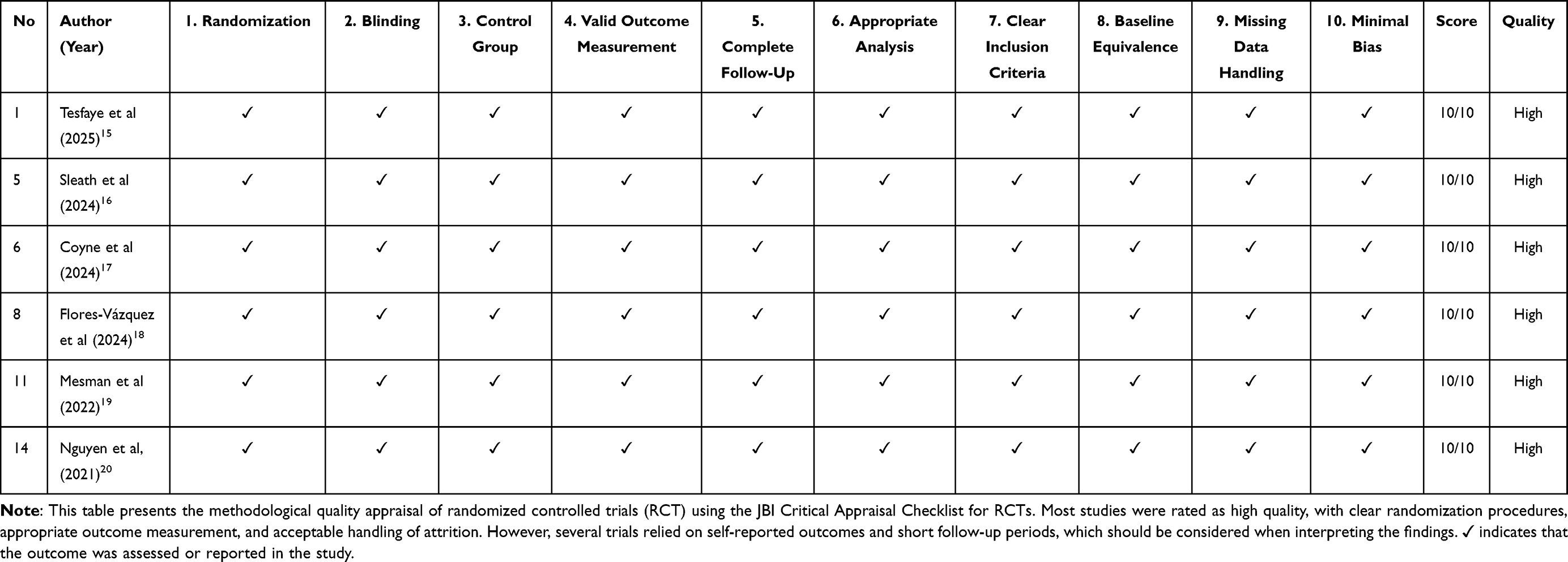 |
Tabel 1 JBI Critical Appraisal Checklist – RCT and Similar Study Designs |
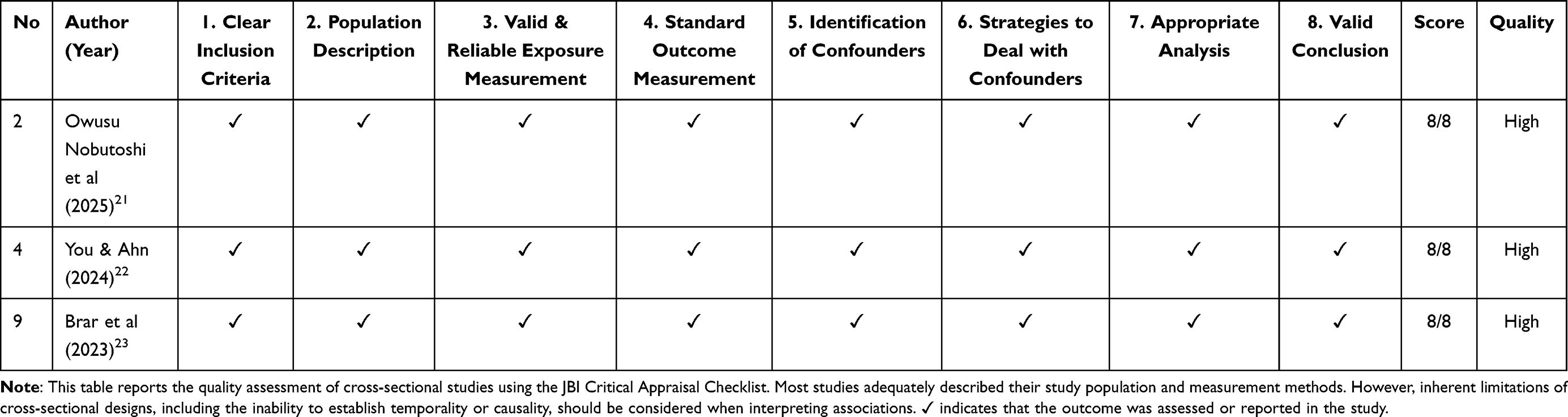 |
Tabel 2 Cross-Sectional Survey |
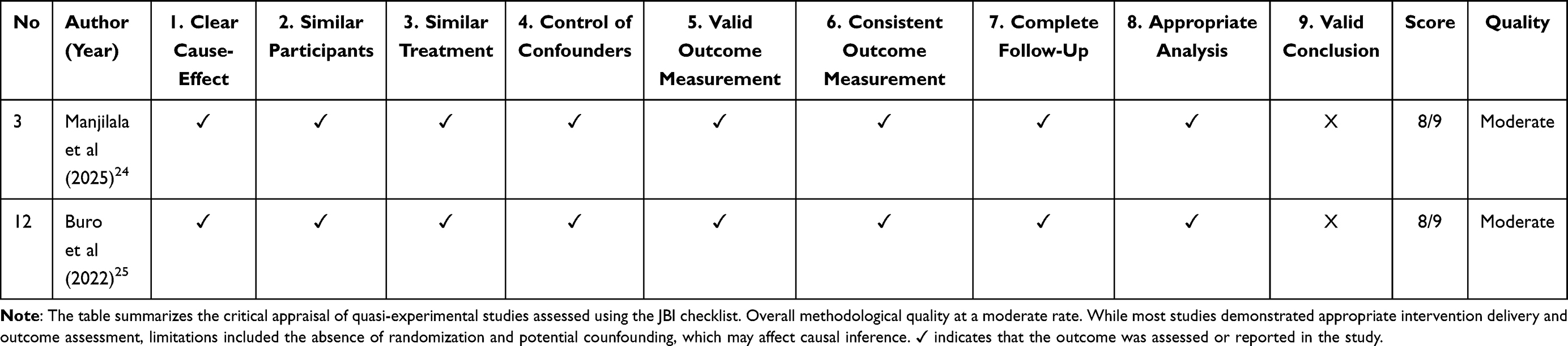 |
Table 3 Quasi-Experimental |
 |
Table 4 Mixed-Methods |
Synthesis of Study Results
Given the substantial heterogeneity across study designs, IPC contexts, outcome measures, and analytical approaches, no statistical pooling or meta-analysis was conducted. Instead, a narrative synthesis approach was used to summarize findings across studies. Results were synthesized by IPC context (peer, family, school, healthcare, and technology-supported communication) and outcome domain (knowledge, attitudes, behaviors, and nutritional or health indicators). Quantitative results were-extracted as reported in the original studies, and no re-estimation of effect size or additional statistical analyses were performed. To enhance analytical transparency, descriptive summaries were used to indicate whether studies reported positive, mixed, or null associations between IPC and adolescent health nutrition outcomes.
Results
Study Selection
The included studies demonstrated substantial heterogeneity in terms of study designs, population characteristics, interpersonal communication (IPC) contexts, and outcomes measures. Given this diversity, a narrative synthesis approach was considered the most appropriate method to summarize and interpret the findings, allowing for structured comparison across IPC contexts rather than statistical aggregation. A total of 14 studies were included in this systematic review after screening and eligibility assessment, representing diverse geographical settings, study designs, and forms of interpersonal communication targeting adolescent health and nutrition outcomes.
Characteristics of Included Studies
The including studies were published between 2021 and 2025 and represented a range of geographical region and settings, including school-based, family-based, healthcare, community, and digital environments. Study designs varied widely and included randomized controlled trials, quasi-experimental studies, cohort studies and cross-sectional designs.
Substantial heterogeneity was observed across studies with respect to participant characteristics, interpersonal communication (IPC) contexts, intervention formats, outcome measures, and analytical approaches. Given this diversity, findings were synthesized using a narrative synthesis approach, allowing structured comparison across IPC contexts rather than statistical aggregation.
This review included 14 studies from diverse geographical contexts, including Europe (Netherlands n = 2; Germany n = 1; Spain n = 1), Asia (Korea n = 1; Japan n = 1; Indonesia n = 1; Vietnam n = 1), Africa (Ethiopia n = 1), North America (USA n = 3; Mexico n = 1), with no studies identified from Oceania. The studies employed various research designs, including cluster randomised controlled trials (RCTs) (n = 2), pilot cluster-RCTs (n = 3), prospective surveys (n = 1), cross-sectional surveys (n = 4), one-group pretest–posttest designs (n = 2), and mixed-methods evaluations (n = 2).
Sample sizes were reported in most studies; however, several pilot or feasibility studies particularly cluster randomized trials, did not explicitly report sample size in the published manuscripts. These studies are indicated as “not reported” in the summary tables.
Peer communication was categorized into two related but distinct formats: face-to-face peer communication and technology supported or digital peer communication. While some studies examined exclusively in-person peer interactions, other focused on online or social media-mediated peer communication. No included study formally combined both formats within a single intervention arm; therefore, these contexts are presented separately in the results tables and narrative synthesis. An overview of study characteristics, including designs, population, IPC context, outcomes, and methodological quality, is provided in Table 5.
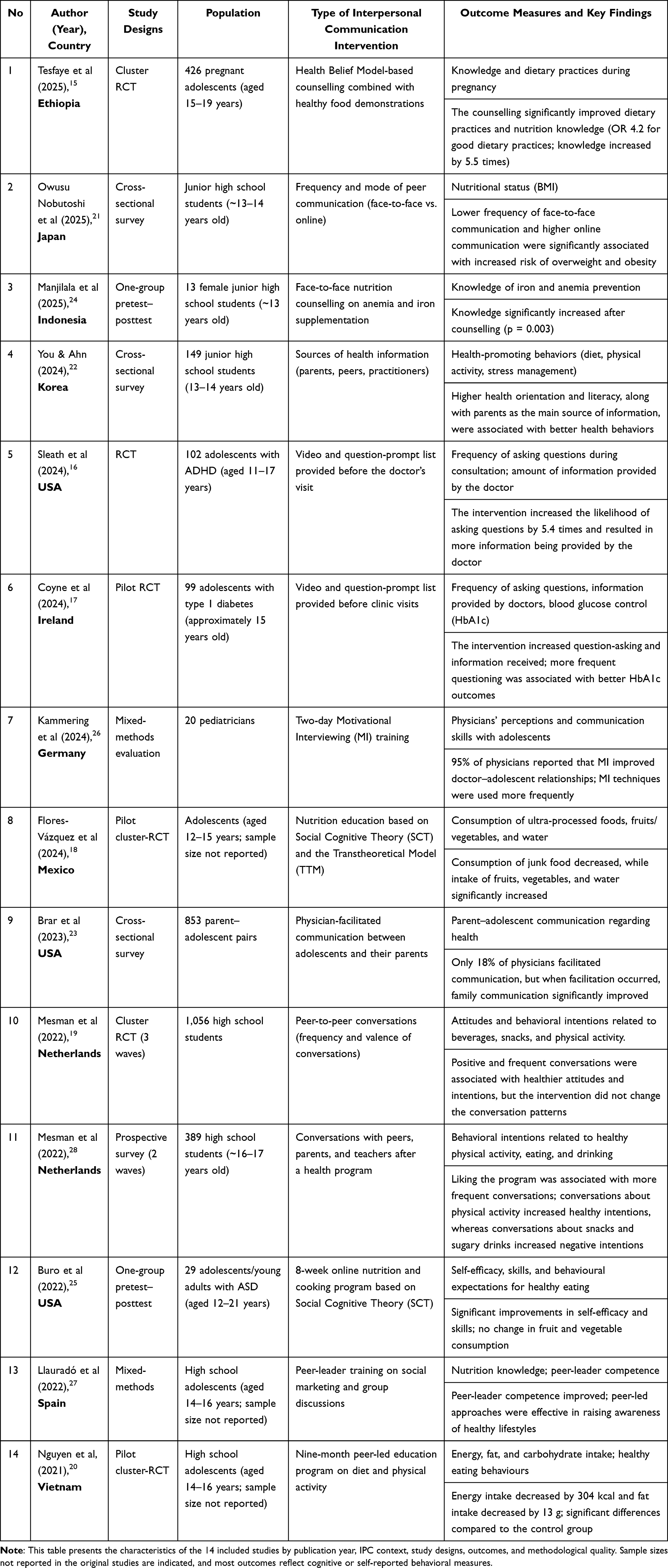 |
Table 5 Characteristics of Included Studies on Interpersonal Communication and Adolescent Health and Nutrition |
Quality Assessment
The methodological quality of the included studies was assessed using appropriate JBI Critical Appraisal Tools_RCT and Similar Study Designs are summarized in Table 1. The results of this appraisal are presented in Table 2 for cross-sectional studies, Table 3 for quasi-experimental studies, Table 4 for mixed-methods studies, and Table 6 for the overall risk-of-bias summary.
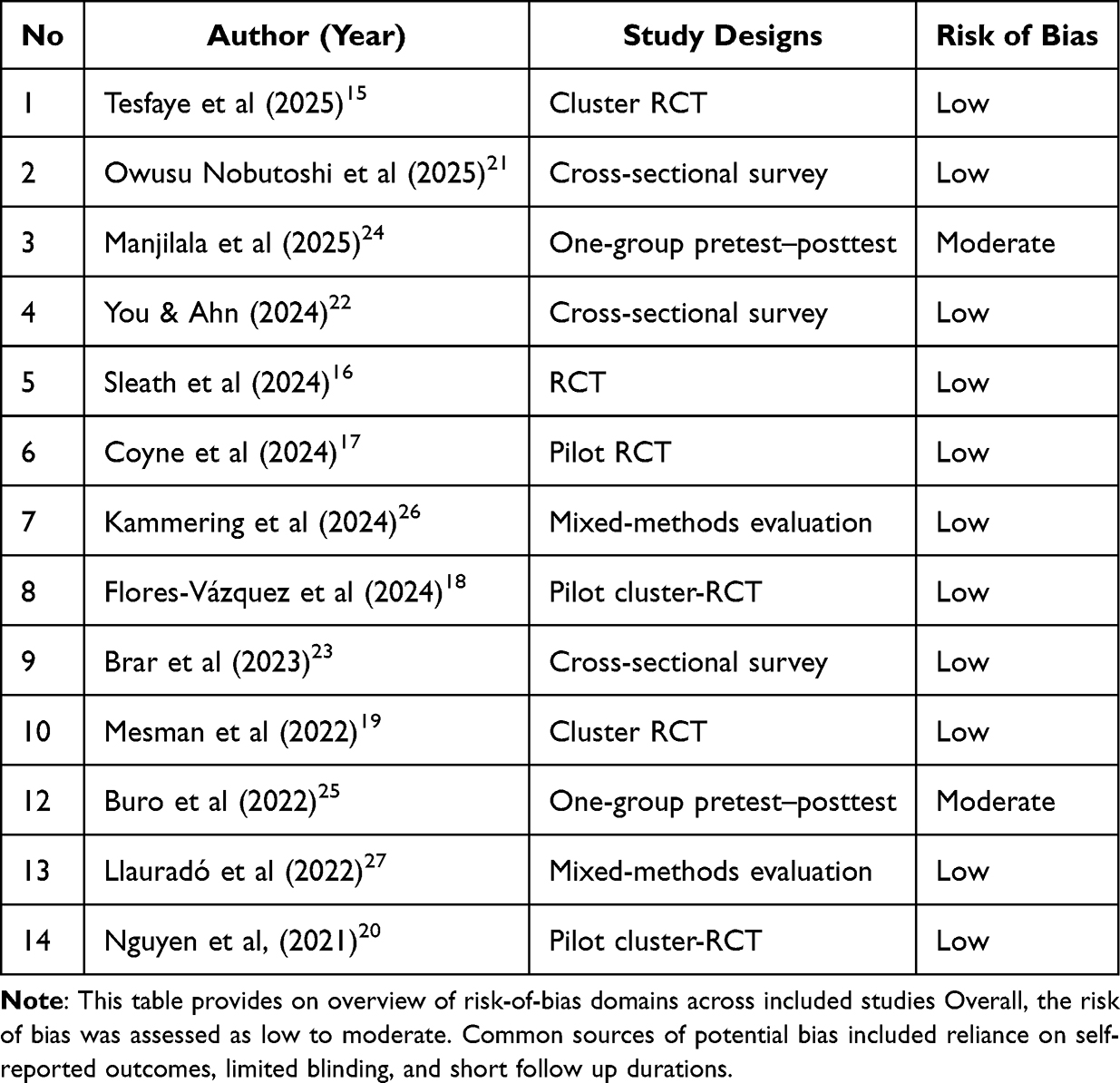 |
Table 6 Risk Of Bias Summary |
Randomised Controlled Trials (RCTs) and Similar Designs
Six studies were categorised as RCTs, cluster RCTs, or pilot RCTs and were appraised using the 10-item JBI checklist for experimental studies. All six studies achieved a perfect score of 10/10, indicating high methodological quality. These studies adequately reported randomisation procedures, blinding, valid outcome measures, appropriate analysis, and minimal risks of bias.
Cross-Sectional Studies
As presented in Table 2, all cross-sectional studies demonstrated high methodological quality. Three cross-sectional studies were assessed using the 8-item JBI checklist. All studies met all appraisal criteria with a score of 8/8, reflecting high quality. These studies clearly described their inclusion criteria, provided sufficient population details, and appropriately addressed potential confounding factors.
Quasi-Experimental Studies (One-Group Pretest–Posttest)
The detailed appraisal result for the quasi-experimental studies are shown in Table 3. Two quasi-experimental studies were assessed using the 9-item checklist. Both studies scored 8/9, with the limitation being insufficient clarity regarding the validity of conclusions drawn. Consequently, these studies were rated as having moderate quality, indicating acceptable but not optimal methodological rigour.
Mixed-Methods Studies
The appraisal outcomes for mixed-methods studies are summarized in Table 4. Two studies employing mixed-methods designs were evaluated using the adapted 10-item JBI checklist for mixed-methods research. Both studies received a perfect score of 10/10, demonstrating high quality in terms of designs justification, integration of quantitative and qualitative components, triangulation, and interpretation of findings.
Risks of Bias Summary
An overview of the risk-of-bias evaluation for all included studies is presented in Table 6. The overall risks of bias across the included studies was low to moderate. The majority of studies, particularly those with randomised controlled designs and mixed-methods approaches, demonstrated a low risks of bias, supported by rigorous methodology, clear reporting of inclusion criteria, appropriate outcome measurements, and strategies to address confounding factors.
In contrast, the quasi-experimental studies (one-group pretest–posttest) presented a moderate risks of bias due to potential limitations in causal inference and incomplete reporting regarding the validity of conclusions. A comprehensive summary of the risks of bias for all included studies is presented in Table 6.
Forms and Contexts of Interpersonal Communication
The included studies explored a diverse range of interpersonal communication (IPC) approaches implemented across various relational and institutional contexts. These approaches demonstrated both positive impacts and areas of concern regarding adolescent health, nutrition, and behavior.
Peer Communication (Face-to-Face)
Studies examining face-to-face peer communication primarily focused on structured group-based interactions delivered in school or community settings. These interventions commonly targeted nutrition knowledge, dietary attitudes, and health-related behaviors through peer-led discussions, mentoring, or group activities.18,20,27,28
Most studies reported positive associations between peer communication and improvements in nutrion-related knowledge and self-reported dietary behaviors. However, effects on anthropometric outcomes were less consistently reported, and follow-up durations were generally short. Methodological quality across these studies was predominantly high, although outcome measures frequently relied on self-reported data.14
Digital Peer Communication
Digital peer communication interventions were delivered through online platforms, social media, or mobile applications and emphasized peer interaction in virtual environments. These studies demonstrated mixed findings. While some reported increased engagement and awareness related to nutrition and health behaviors, others identified potential unintended consequences.16
Notably, at least one study reported an association between unstructured online peer communication and a higher risks of overweight or obesity, highlighting the importance of intervention structure and content moderation. Overall, findings suggest that digital peer communication may offer both opportunities and risks, depending on implementation and context.28
Family Communication
Family-based IPC studies explored parent-adolescent communication related to nutrition practices, dietary decision-making, and health behaviors. These studies consistently demonstrated positive associations between supportive family communication and healthier dietary patterns, improved nutritional knowledge and more favorable health-related attitudes among adolescents.27
Interventions emphasizing parental involvement and bidirectional communication tended to report stronger effect than those focusing solely on information provision. However, variability in outcome measures and study designs limited direct comparison across studies.19
Health Provider Communication
Studies examining communication between adolescents and healthcare providers focused on counseling, guidance, and interpersonal support delivered in clinical or primary care settings. These interventions were associated with improved health-related knowledge, risks perception, and in some cases, behavior change.
Provider-led communication was particularly effective when it incorporated individualized counseling and adolescent-centered communication strategies. However, the number of studies in this category was relatively small compared with peer-and family-based interventions.
Multiple studies underscored the value of effective communication between adolescents and healthcare providers: Counseling interventions grounded in the Health Belief Model notably improved nutrition knowledge and dietary practices among pregnant adolescents in Ethiopia.15 Question-prompt-list (QPL) and video interventions significantly enhanced adolescent engagement during medical consultations, leading to improved information exchange and, in the case of youth with type 1 diabetes, better clinical outcomes such as glycemic control.17,26 Training in Motivational Interviewing (MI) for pediatricians improved healthcare providers’ communication skills and strengthened relationships with adolescent patients.25
School and Teacher-Based Communication
School-based IPC interventions typically involved communication between students and teachers or structured curricula incorporating interactive discussion. These studies commonly targeted nutrition education and health promotion within formal educational settings.16,18
Overall, school-based communication interventions were associated with improvements in nutrition knowledge and, in some cases, dietary behaviors. Effects on longer-term health outcomes were less frequently assessed. The quality appraisal indicated generally high methodological quality, although heterogeneity in intervention content and duration was evident.16,18,19
Teachers and school staff played a facilitative role in adolescent health dialogue, particularly through structured educational programs: Health education interventions incorporating peer-led approaches, social marketing, and behavioral change theories such as Social Cognitive Theory (SCT) and the Transtheoretical Model (TTM) effectively improved health knowledge, dietary patterns, and health literacy.
Technology-Enhanced Interpersonal Communication
One study explored the integration of technology within IPC strategies: Among adolescents with autism spectrum disorder, an online nutrition and culinary education program improved self-efficacy, behavioral skills, and outcome expectations for healthy eating, although direct dietary behavior changes were limited.25
Health and Nutrition Outcomes
The various IPC interventions and interactions yielded the following health-related outcomes among adolescents:
- Dietary Improvements: Significant reductions in ultra-processed food consumption and increased intake of fruits, vegetables, and water were-observed.29
- Behavioral Change and Health Literacy: Enhanced health knowledge, intentions, self-efficacy, and peer leader competence were documented, particularly among peer-led and special needs groups.25,27
- Clinical Outcomes: Improved nutritional status among pregnant adolescents and better glycemic control in youth with type 1 diabetes were achieved through counseling and structured engagement.21,30
- Mental and Social Health: Increased adolescent participation during healthcare encounters, improved family dialogue, and positive peer influence on health attitudes were reported.23
- Negative Associations: Increased reliance on online peer communication during the COVID-19 pandemic was associated with higher risks of overweight and obesity.23
Discussion
This systematic review synthesizes evidence from 14 studies published between 2021 and 2025 that examined the role of interpersonal communication (IPC) in adolescent health and nutrition across diverse contexts, including peer, family, school, healthcare, and technology-supported settings (Table 5). Overall, the findings indicate that IPC is most consistently associated with improvements in nutrition-related knowledge, attitudes, intentions, and self-efficacy, while evidence for sustained behavioral change and clinical outcomes remains more limited and heterogeneous.16,26
These patterns align with the narrative synthesis approach adopted in this review, as substantial heterogeneity was observed across study designs, population, IPC formats, and outcome measures, precluding quantitative pooling. Importantly, no effect sizes were re estimated, and all interpretations rely on the analyses reported in the original studies, in accordance with established guidance for scoping and narrative reviews.
Interpretation of Findings by IPC Context
Across IPC contexts, the strongest and most consistent associations were observed for family-based and healthcare provider communication. Peer communication was particularly influential in shaping dietary attitudes.20,26,29 These findings align with behavioral and social learning theories, which emphasize the influence of trusted authority figures and role models in shaping health-related beliefs and decision-making during adolescence.
In contrast, peer communication, defined as direct interactions between adolescents of similar age or social status, demonstrated more variable effects. Structured, face-to-face peer interventions, often embedded in school or community programs, were generally associated with positive changes in knowledge and self-reported behaviors.23,30 However, evidence for sustained behavioral change or objective health outcomes was limited, reflecting both short follow-up periods and reliance on self-reported measures.22,30
School-based communication, typically involving teacher-student interactions or curriculum-based discussions, showed moderate and relatively consistent benefits for nutrition knowledge and awareness.18,23 However, fewer studies assessed longer-term behavioral or clinical outcomes, limiting conclusions regarding durability of effects. Communication delivered by healthcare providers, although examined in a smaller number of studies, appeared particularly effective when adolescent-centered and individualized, suggesting the importance or relational quality and trust in clinical interactions.29
Importantly, across all IPC contexts, the majority of included studies assessed cognitive and psychosocial outcomes (eg., knowledge, intentions, self-efficacy) rather than objective clinical indicators. As such, claims regarding “improvements in health outcomes” should be interpreted primarily as improvements in intermediate determinants of behavior, with more limited evidence for downstream health effects.20,24,30
Peer Communication: Benefits and Contextual Risks
Peer communication emerged as a prominent and complex influence on adolescent health behaviors. Seven studies examined peer-based IPC, including face-to-face peer discussions and structured peer-led education programs (Table 5).18,23,30 Positive and frequent peer conversations were associated with healthier attitudes and behavioral intentions, particularly related to physical activity and dietary choices. Peer-led interventions grounded in behavioral theories such as Social Cognitive Theory demonstrated reductions in energy and fat intake and improvements in healthy eating behaviors, particularly in school-based settings.22,23
However, the findings also underscore that peer communication is not uniformly beneficial. One large observational study reported that snack and sugar-sweetened beverage related peer discussions were associated with less healthy intentions, highlighting the importance of message content and emotional valence.30 Additionally, a cross-sectional study found that higher exposure to online peer communication was associated with increased risks of overweight and obesity, whereas more frequent face-to-face communication showed protective associations.22 Rather than indicating harm per se, these findings suggest that unstructured or digitally mediated peer interactions may amplify existing norms and behaviors, underscoring the need for guided and context-sensitive peer engagement strategies.
Consistent with the result section, peer communication was therefore presented in two distinct formats; face-to-face and technology-supported peer communication, with no studies combining both modalities within a single intervention arm. Technology-mediated communication, encompassing online peer interaction, social media engagement, and digital messaging platforms. Represents a rapidly evolving IPC context. Findings in this domain were notably mixed. While some studies reported increased engagement and accessibility of health information, others highlighted potential unintended consequences.22
In particular, the association between unstructured digital peer communication and higher overweight or obesity risks was reported in a single cross-sectional study.22 This finding should be interpreted with caution, as cross-sectional designs do not establish causality and may reflect confounding by underlying behavioral or social factors. This finding should not be interpreted as evidence of harm, but rather highlights the need to consider how unstructured digital peer communication may operate under certain conditions. This result underscores the importance of structure, moderation, and content quality in digital IPC interventions. Overall, digital communication appears to hold promise when deliberately designed and integrated with broader support systems, but its effectiveness and safety likely depend on implementation features.
Health Provider Communication and Clinical Engagement
Communication between adolescents and healthcare providers was associated with improvement in both communicative processes and selected clinical indicators. Interventions incorporating counseling frameworks such as the Health Belief Model significantly improved nutrition knowledge and dietary practices among pregnant adolescent.26 Similarly, communication-support tools including question-prompt lists and video-based preparatory materials enhanced adolescents’ active participation during clinical encounters, resulting in improved information exchange and engagement.27 In one pilot randomized controlled trial, such as a intervention was also associated with improved glycemic control among adolescents with type 1 diabetes, suggesting potential benefits for selected clinical indicators when communication is effectively structured.19
Training healthcare providers in Motivational Interviewing further strengthened provider adolescent relationship and communication quality, underscoring the importance of relational and developmental alignment in clinical interactions.31 Collectively, these findings suggest that structured, adolescent-centered provider communication appears particularly effective when tailored to specific clinical contexts. However, evidence regarding sustained behavioral or clinical outcomes remains limited, largely due to short follow-up periods and modest sample sizes.
School and Teacher-Supported Communication
School-based IPC interventions, often delivered through peer-led or teacher-facilitated programs, contributed to improvements in nutritional knowledge, awareness, and selected dietary behaviors. Interventions integrating behavioral change theories such as Social Cognitive Theory and the Transtheoretical Model were particularly effective in promoting healthier food choices and reducing ultra processed food consumption.18,22,23
Nevertheless, most school-based studies primarily assessed intermediate outcomes such as knowledge, intentions, and self-efficacy, with relatively few evaluating objective dietary intake or longer-term health indicators. These limitations constrain the strength of causal inference. It is important to note that several included studies employed cross-sectional designs; therefore, reported associations should not be interpreted as causal effects.
Strengths and Limitations
This review has several strengths, including adherence to PRISMA-ScR guidelines, transparent reporting of study selection and quality appraisal, and inclusion of multiple IPC contexts relevant to adolescent health promotion. The use of Joanna Briggs Institute (JBI) appraisal tools allowed systematic assessment of methodological quality across diverse study designs.
However, several limitations should be acknowledged. Although many randomized controlled trials achieved high JBI quality scores, these ratings primarily reflect methodological reporting standards rather than certainty regarding effect magnitude. The substantial heterogeneity in study designs, outcomes, and IPC formats precluded meta-analysis and necessitates cautious interpretation of findings. Additionally, reliance on self-reported outcomes, short follow-up periods, and limited reporting of long-term effects constrain conclusions about sustained health impact. The restriction to English-language publications and studies published from 2021 onward may also have excluded earlier or non-English research, potentially limiting the comprehensiveness of the evidence base.
Implication for Practice and Future Research
Despite these limitations, the findings have practical implications. Interventions that leverage structured interpersonal communication, particularly involving families and healthcare providers, appear promising for supporting adolescent nutrition and health-related behaviors. Policymakers and practitioners should be cautious in assuming benefits from unstructured digital peer communication and prioritize designs features that promote supportive, evidence-based interaction.
Future research should focus on longitudinal and experimental designs to clarify causal pathways between IPC and health outcomes, incorporate objective or biomarker-based measures where feasible, and examine differential effects across cultural contexts. Additionally, advances in digital health tools may complement IPC strategies. Emerging research from continuous glucose monitoring (CGM) analytics has demonstrated the value of dynamic glycemic metrics and machine-learning-based pattern detection in identifying early metabolic dysregulation among adolescents.31,32 Integrating such digital biomarkers with structured interpersonal communication may enable more timely, personalized, and data-informed discussions between adolescents, families, and healthcare providers. Future research should explore how CGM-supported communication strategies can enhance clinical engagement and preventive nutrition counseling in adolescent populations.
Conclusion
This systematic review synthesizes evidence from fourteen studies examining the role of interpersonal communication (IPC) in adolescent health and nutrition across peer, family, school, healthcare, and technology-supported contexts. IPC was most consistently associated with improvements in nutrition-related knowledge, attitudes, behavioral intentions, and self-efficacy, particularly when communication was structured and facilitated by parents, teachers, or healthcare providers. However, evidence for sustained behavioral change or objective clinical outcomes remains limited and heterogeneous.
Peer and digital communication demonstrated more variable associations. Structured, face-to-face peer interventions were generally linked to positive cognitive and behavioral intentions, whereas unstructured or poorly moderated digital peer interactions showed mixed findings and warrant cautious interpretation. Importantly, these observations reflect associations rather than causal effects, especially in studies using cross-sectional designs or self-reported outcomes.
This review highlights the potential of IPC as a complementary strategy for adolescent health and nutrition promotion, while underscoring critical evidence gaps. Future research should prioritize longitudinal and experimental designs, incorporate objective outcome measures where feasible, and examine how emerging digital health tools can be effectively integrated with interpersonal communication to support timely, context-sensitive, and equitable adolescent health interventions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. UNICEF & WHO. Improving the Health and Wellbeing of Children and Adolescents: Guidance on Scheduled Child and Adolescent Well-Care Visits; 2023.
2. Patton GC, Sawyer SM, Santelli JS, et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet. 2016;387(10036):2423–18. doi:10.1016/S0140-6736(16)00579-1
3. Azzopardi PS, Hearps SJC, Francis KL, et al. Progress in adolescent health and wellbeing: tracking 12 headline indicators for 195 countries and territories, 1990–2016. Lancet. 2019;393(10176):1101–1118. doi:10.1016/S0140-6736(18)32427-9
4. WHO. Global Strategy on Digital Health 2020–2025. Licence: CC BY-NC-SA 3.0 IGO. Geneva: World Health Organization; 2021.
5. Cheng TW, Mills KL, Pfeifer JH. Revisiting adolescence as a sensitive period for sociocultural processing. Neurosci Biobehav Rev. 2024;164:105820. doi:10.1016/j.neubiorev.2024.105820
6. Robert G, Kahn NF. Promoting Positive Adolescent Health Behaviors and Outcomes: Thriving in the 21st Century. National Academies Press; 2020.
7. Chong CY, Tan CX, Tsai MC, Tan SS, Hariyono H, Tan ST. Gender differences in dietary intake and physical activity among university students: a post-COVID-19 pandemic study. Nutr Food Sci. 2024;54(7):1190–1201. doi:10.1108/NFS-01-2024-0015
8. Prasanna SAS, Abeysena HTCS, Alagiyawanna MAAP. Development and validation of the interpersonal communication assessment tool for assessing the interpersonal communication skills of public health midwives. BMC Health Serv Res. 2023;23(1). doi:10.1186/s12913-023-09511-7
9. Parhiala P, Ranta K, Gergov V, et al. Interpersonal Counseling in the Treatment of Adolescent Depression: a Randomized Controlled Effectiveness and Feasibility Study in School Health and Welfare Services. School Ment Health. 2020;12(2):265–283. doi:10.1007/s12310-019-09346-w
10. Tock WL, Gauvin L, Hudon F, Tremblay F, Bélanger RE, Turcotte-Tremblay AM. Scoping review of interventions aimed at promoting healthy screen use among adolescents. BMJ Open. 2025;15(9):e103772. doi:10.1136/bmjopen-2025-103772
11. Bramer WM, Rethlefsen ML, Kleijnen J, Franco OH. Optimal database combinations for literature searches in systematic reviews: a prospective exploratory study. Syst Rev. 2017;6(1). doi:10.1186/s13643-017-0644-y
12. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906. doi:10.1016/j.ijsu.2021.105906
13. Roberts K, Casey M, Coghlan D, et al. A scoping review protocol to map the evidence on the use of action research methodology by healthcare professionals and in healthcare team settings. HRB Open Res. 2021;4:68. doi:10.12688/hrbopenres.13275.1
14. Pollock D, Peters MDJ, Khalil H, et al. Recommendations for the extraction, analysis, and presentation of results in scoping reviews. JBI Evid Synth. Lippincott Williams Wilkins. 2022;21(3):520–532. doi:10.11124/JBIES-22-00123
15. Tesfaye A, Belete KT, Tamiru D, Belachew T. Effect of nutrition behavior change communication on nutrition knowledge and dietary practices of pregnant adolescents in West Arsi, Central Ethiopia: a cluster randomized controlled trial. Front Nutr. 2025;12. doi:10.3389/fnut.2025.1541415.
16. Sleath B, Beznos B, Carpenter D, et al. A pre-visit video/question prompt list intervention to increase youth question-asking about attention deficit hyperactivity disorder during pediatric visits. Patient Educ Couns. 2024;127:108320. doi:10.1016/j.pec.2024.108320
17. Coyne I, Sleath B, Surdey J, et al. Intervention to promote adolescents’ communication and engagement in diabetes clinic encounters: a pilot randomized controlled trial. Patient Educ Couns. 2024;126:108322. doi:10.1016/j.pec.2024.108322
18. Flores-Vázquez AS, Rodríguez-Rocha NP, Macedo-Ojeda G. Educational Nutritional Intervention Program for Adolescents Based on Social Cognitive Theory: pilot Study of a Cluster Randomized Controlled Trial. Health Serv Insights. 2024;17. doi:10.1177/11786329241249011.
19. Mesman M, Hendriks H, Onrust S, van den Putte B. The Intervening Role of Conversational Frequency and Valence in a School-Based Health Intervention. Health Commun. 2022;37(13):1590–1599. doi:10.1080/10410236.2021.1909245
20. Thi Nguyen NT, Tang HK, Nguyen MN, Dibley MJ, Alam NA. Effect of a peer-led education intervention on dietary behaviour and physical activity among adolescents in Ho Chi Minh City, Vietnam: a pilot study. Eur J Clin Nutr. 2022;76(11):1590–1593. doi:10.1038/s41430-022-01140-3
21. Owusu FM, Nawa N, Nishimura H, et al. Association of communication methods and frequency with BMI among adolescents during the COVID-19 pandemic: findings from A-CHILD study. Front Public Health. 2025;13. doi:10.3389/fpubh.2025.1433523
22. You MA, Ahn JA. Health information orientation and health literacy as determinants of health promotion behaviors in adolescents: a cross-sectional study. Front Public Health. 2024;12. doi:10.3389/fpubh.2024.1522838.
23. Brar P, Sieving RE, Steiner RJ, et al. Provider Facilitation of Parent-Adolescent Health Communication: findings From a National Survey. J Pediatric Health Care. 2023;37(3):253–261. doi:10.1016/j.pedhc.2022.11.003
24. Manjilala M, Idris N, Rauf S, Sirajuddin S. Effectiveness of Interpersonal Communication in Nutrition Education on Iron Supplement Knowledge in Adolescent Girls at SMP Muhammadiyah Maros. J Health Nutr Res. 2025;4(1):358–364. doi:10.56303/jhnresearch.v4i1.359
25. Buro AW, Gray HL, Kirby RS, et al. Pilot Study of a Virtual Nutrition Intervention for Adolescents and Young Adults With Autism Spectrum Disorder. J Nutr Educ Behav. 2022;54(9):853–862. doi:10.1016/j.jneb.2022.01.008
26. Kammering H, Cruz JA, Platzbecker AL, et al. Motivational interviewing from the paediatricians’ perspective: assessments after a 2-day training for physicians caring for adolescents with chronic medical conditions (CMCs). BMC Pediatr. 2024;24(1). doi:10.1186/s12887-024-04794-z
27. Llauradó E, Aceves-Martins M, Prades-Tena J, et al. Adolescents encouraging healthy lifestyles through a peer-led social marketing intervention: training and key competencies learned by peer leaders. Health Expectations. 2022;25(1):455–465. doi:10.1111/hex.13406
28. Mesman M, Hendriks H, Onrust S, Neijens P, van den Putte B. The Antecedents and Consequences of Interpersonal Communication during a School-based Health Intervention. Health Commun. 2022;37(1):114–124. doi:10.1080/10410236.2020.1824664
29. Budhawani N, Naar S. Training Providers in Motivational Interviewing to Promote Behavior Change. Pediatric Clinics of North America. 2022;69(4):779–794. doi:10.1016/j.pcl.2022.04.008
30. Harianti R, Nurjanah T, Hasrianto N. Peer education as a method in sexual, reproductive health promotion and risk communication for adolescent. J Kajian Komunikasi. 2021;9(2):213–223. doi:10.24198/jkk.v9i2.32280
31. Montaser E, Farhy L, Kovatchev B. Novel Detection and Progression Makers for Diabetes Based on Continuous Clucose Monitoring Data Dynamics. J Clin Endocrinol Metab. 2024;110(1):254–262. doi:10.1210/clinem/dgae379
32. Montaser E, Farhy L, Rich S. Enhancing Type 1 Diabetes Immunological Risk Prediction with Continuous Glucose Monitoring and Genetic Profiling. Diabetes Technol Ther. 2025;27(4):292–300. doi:10.1089/dia.2024.0496
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.