Back to Journals » Nature and Science of Sleep » Volume 17

Association Between Obstructive Sleep Apnea and Prostate Cancer: NHANES and the Mendelian Randomization Study
Authors Liu Y, Jiang B, Xia L ![]() , Bao E, Wang L
, Bao E, Wang L ![]() , Zhu PY
, Zhu PY
Received 16 September 2024
Accepted for publication 10 October 2025
Published 24 October 2025 Volume 2025:17 Pages 2783—2795
DOI https://doi.org/10.2147/NSS.S496540
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Ying Liu,1,2,* Binglei Jiang,3,* Long Xia,2,* Erhao Bao,4 Li Wang,5 Ping-Yu Zhu2
1Department of Transfusion, Zigong First People’s Hospital, Zigong, Sichuan, People’s Republic of China; 2Department of Urology, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China; 3Department of Ultrasound, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China; 4Department of Urology, Sichuan Provincial People’s Hospital East Sichuan Hospital & Dazhou First People’s Hospital, Dazhou, Sichuan, People’s Republic of China; 5Department of Urology, The Second Hospital of Lanzhou University, Lanzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ping-Yu Zhu, Email [email protected]
Background: Obstructive sleep apnea is a common condition worldwide, and prostate cancer is the most prevalent cancer among men. However, the link between OSA and prostate cancer remains unclear. This study aims to explore the relationship between OSA and prostate cancer.
Methods: Initially, a multivariable regression analysis was conducted to control for potential confounders and assess the impact of OSA on the risk of developing prostate cancer. Subsequently, age-stratified analyses were performed to further investigate the relationship between OSA and prostate cancer across different age groups. Finally, Mendelian randomization was employed to evaluate the causal relationship between OSA and prostate cancer risk.
Results: The multivariable regression analysis of the NHANES data showed no significant association between OSA and prostate cancer after controlling for age, smoking habits, hypertension, diabetes, cardiovascular diseases, stroke, alcohol consumption, body mass index (OR = 0.83; 95% CI: 0.46– 1.48; p = 0.49). However, age-stratified analysis revealed a significant negative correlation between OSA and prostate cancer in the younger population (< 60 years) (OR = 0.07; 95% CI: 0.01– 0.74; p = 0.03), whereas no significant association was found in the elderly population (≥ 60 years) (OR = 1.01; 95% CI: 0.69– 1.49; p = 0.96). Finally, our Mendelian randomization results did not find a causal relationship between OSA and prostate cancer (OR = 0.992; 95% CI: 0.876– 1.124; p = 0.906).
Conclusion: The findings indicate that while there is no significant association between OSA and prostate cancer in the overall analysis, a significant negative correlation exists in the younger population. The lack of significant association in the Mendelian randomization analysis may be due to the inability to perform age stratification. Further prospective studies and mechanistic research are needed to better understand the biological mechanisms underlying this association.
Keywords: obstructive sleep apnea, prostate cancer, national health and nutrition examination survey, mendelian randomization
Introduction
Prostate cancer is the most prevalent cancer among men. The etiology of prostate cancer is multifactorial, involving genetic, environmental, and lifestyle factors.1 Obstructive sleep apnea (OSA) is a prevalent condition worldwide, affecting over 4% of men and 2% of women, characterized by recurrent partial or complete upper airway obstruction during sleep. This condition is associated with various adverse health outcomes, including cardiovascular diseases, and metabolic disorders.2,3
Several studies have investigated the potential link between OSA and cancer, suggesting that one of the key features of OSA—intermittent hypoxia—might promote tumor progression and metastasis through mechanisms such as increased angiogenesis, oxidative stress, and inflammation.4,5 However, the relationship between OSA and prostate cancer remains unclear, with conflicting results reported in the literature. Fang et al indicated that, based on data from the National Health Insurance database in Taiwan, the risk of prostate cancer in patients with obstructive sleep apnea is significantly higher than that in the control group.6 In contrast to Fang et al, Wu et al’s study found no significant impact of obstructive sleep apnea on the risk of prostate cancer.7 Conversely, in a nationwide large health insurance database, OSA appeared to increase the risk of only a few cancer types, including pancreatic cancer, kidney cancer, and melanoma, while the risk of prostate cancer was lower among OSA patients.8
The National Health and Nutrition Examination Survey (NHANES) provides valuable datasets for epidemiological studies, offering comprehensive health information representative of the US population. Utilizing the NHANES database, we aim to investigate the association between OSA and prostate cancer, employing multivariate regression analysis to adjust for potential confounding factors. Additionally, we seek to explore the impact of stratifying this relationship by different factors.
To complement the observational findings from NHANES, we employ Mendelian Randomization (MR) as an analytical method. MR uses genetic variations as instrumental variables to infer causal relationships between exposures and outcomes, thereby reducing the likelihood of confounding and reverse causality.9
Therefore, to explore the relationship between the two, we analyzed data from the NHANES database spanning from 2001 to 2010. Additionally, to determine if there is a causal relationship, we conducted a two-sample Mendelian Randomization analysis.
Materials and Methods
Study Population in NHANES
NHANES is a cross-sectional survey that has been updated and released every two years since 1999, employing a rigorous, stratified, multistage probability sampling design to ensure national representativeness. In the current observational study, we used data from the NHANES 2001–2010 cycles, spanning five survey periods. Detailed inclusion and exclusion criteria are provided in Figure 1.
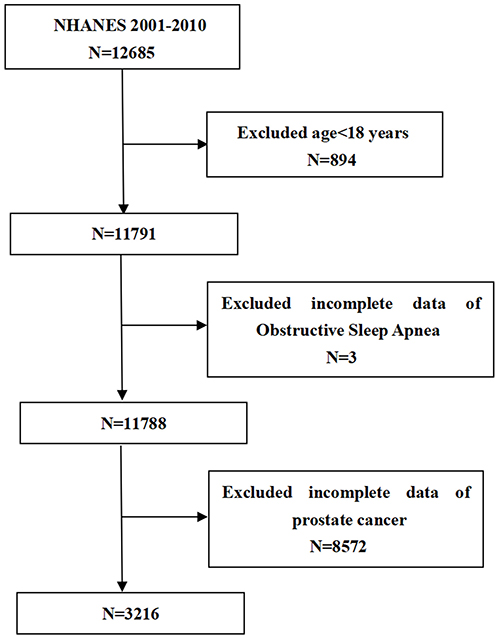 |
Figure 1 Flowchart of NHANES. |
Exposure and Outcome Definitions
In this study, OSA was used as the exposure variable. The presence of obstructive sleep apnea symptoms was determined using answers to three yes/no questions: (1) frequent snoring (three or more nights weekly); (2) episodes of snorting, gasping, or breath stopping (three or more nights weekly); and (3) excessive daytime sleepiness occurring 16–30 times a month despite sleeping at least seven hours on average during weekdays or work nights. Participants who reported any of these symptoms were considered to have OSA. The identification of prostate cancer was based on responses to a single question: “Have you ever been told by a doctor or health professional that you have prostate cancer?”
Covariates
The multivariable-adjusted models encompassed a summary of the potential covariates that could introduce confounding factors into the relationship between OSA and prostate cancer. The covariates included age (years), smoking status (never/former/current), hypertension, diabetes, cardiovascular disease (CVD), stroke, alcohol intake (never/former/mild/moderate/heavy), body mass index. Comprehensive information regarding the measurement procedures for the study variables can be accessed publicly at www.cdc.gov/nchs/nhanes/.
Assumptions and Data Sources of Two-Sample MR
In Mendelian Randomization (MR) studies, it is critical that the instrumental variables (IVs) used meet three criteria: (1) they must be strongly associated with OSA, (2) they should not relate to any confounders between the exposure and the outcome, and (3) they must affect prostate cancer only through their interaction with the exposure.10 We sourced the genetic instruments for OSA from FinnGen’s latest release 10 (https://r10.fnngen.fi/), with data including 43,901 cases and 366,484 controls. We obtained genetic data on prostate cancer from the PRACTICAL Consortium (https://gwas.mrcieu.ac.uk/), which conducted a large study including 79,148 cases and 61,106 controls of European ancestry, ultimately including 20,346,368 SNPs.11
Selection of Genetic Instruments
In our study, we selected single-nucleotide polymorphisms (SNPs) that showed a robust correlation with obstructive sleep apnea (OSA) to serve as instrumental variables (IVs), applying a significance threshold of p < 5x10^-8. To ensure the independence of these SNPs, linkage disequilibrium (LD) clumping was conducted. This involved identifying SNPs with r2 less than 0.01 and at least 50,00 kb apart. SNPs that were palindromic were excluded, and harmonization was achieved between alleles affecting the exposure and outcome in our datasets. Additionally, we utilized the Phenoscanner database (http://www.phenoscanner.medschl.cam.ac.uk/) to remove any SNPs that exhibited pleiotropic effects, thereby addressing potential confounders in the exposure-outcome relationship.
Statistical Analysis
Cross-Sectional Study
We applied the NHANES sampling weights to address the intricacies of the complex multistage cluster survey design according to CDC protocol. Odds ratios (ORs) and 95% confidence intervals (CIs) for the relationship between obstructive sleep apnea (OSA) and prostate cancer were estimated using two distinct multivariable logistic regression models. The first model did not adjust for any covariates, and the second model included adjustments for age, smoking habits, hypertension, diabetes, cardiovascular diseases, stroke, alcohol consumption and body mass index. We also conducted a subgroup analysis using stratified multivariate regression, which considered a range of demographic and health-related factors. An interaction term was used to examine the variability in associations across different subgroups using the log-likelihood ratio test model. Statistical significance was determined using a p-value of 0.05. All statistical analyses and graphical representations were performed using Stata version 17 and R version 4.3.1.
MR
Our Mendelian randomization study used a variety of research methods, including the inverse variance weighting (IVW) method, MR-Egger, weighted median, and MR-Pleiotropy residuals and outliers (MR-PRESSO) test. IVW is used as the predominant analytical method used to verify causality because of its robust causal estimation, which is chosen as the primary method for all Mendelian randomization.12 We used MR-Egger regression and weighted medians to enhance the credibility of the IVW results.13,14 In addition to this, we used the Cochran Q test to test for the presence of heterogeneity in the selected SNPs and the MR-Egger intercept to test for the presence of horizontal pleiotropy.15,16 The MR-PRESSO test provides a comprehensive assessment of heterogeneity to identify potential outliers in the SNP data in order to exclude these outliers from distorting the results.17
BWMR is an efficient statistical method for causal inference based on summary statistics. To address the prevalence of polygenic structure as well as pleiotropy, we adopted Bayesian-weighted Mendelian randomization (BWMR) to remove the uncertainty associated with weak effects as well as pleiotropy for the purpose of enhancing the robustness of IVW results.18
All statistical analyses were conducted using the“Two Sample M” package (version 0.5.6) in R software (version 4.3.1).
Results
Baseline Characteristics of Participants
Table 1 shows the participants’ baseline demographic characteristics. A total of 3216 participants were enrolled in our study. The average age of the participants was 56.35 ± 0.38 years. The overall mean incidence of prostate cancer was 3.28%, and varying rates of prostate cancer were based on the presence of OSA. (prostate cancer: 3.7% without OSA and 2.49% With OSA; p = 0.02).
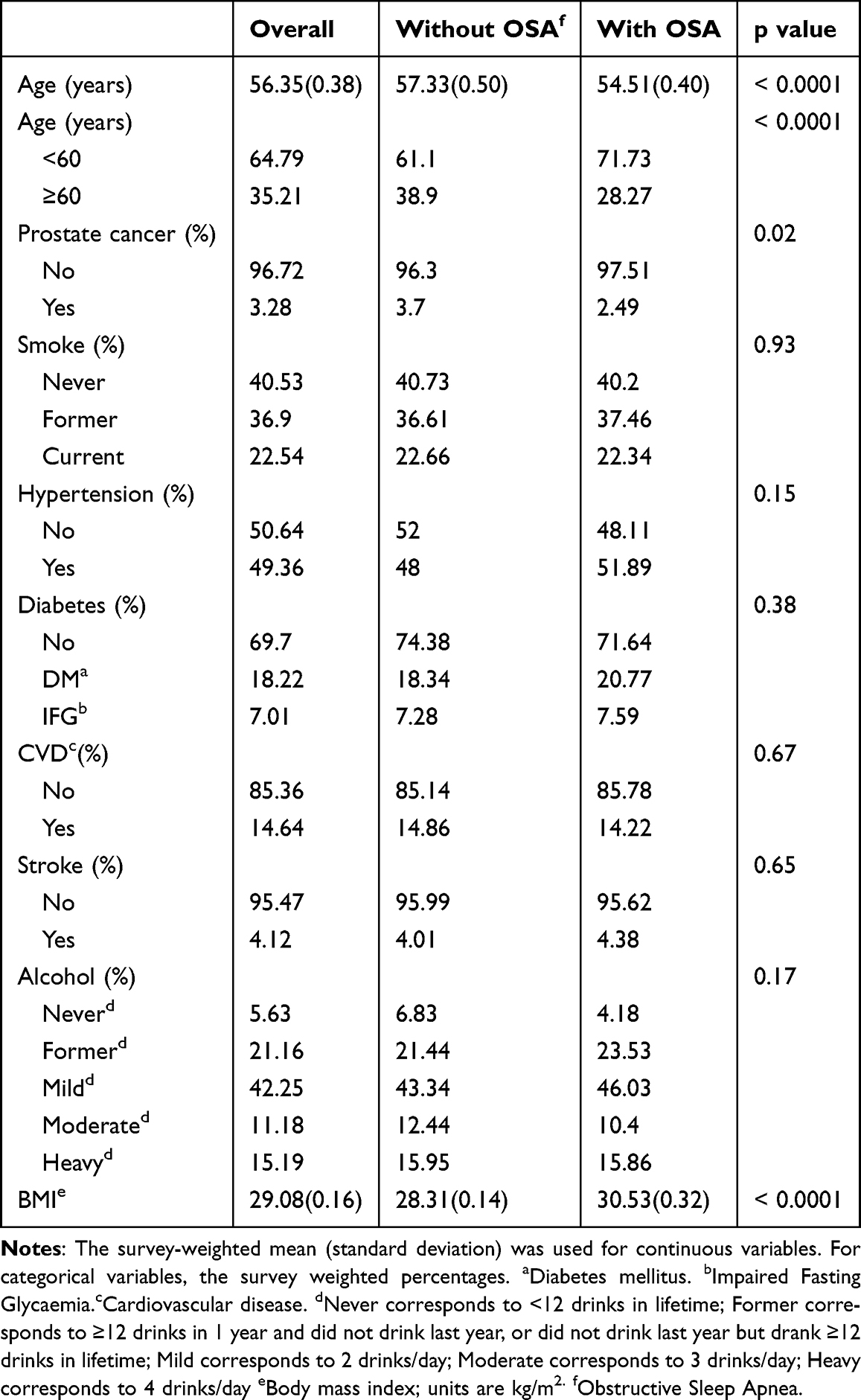 |
Table 1 Baseline Characteristics of Participants |
NHANES of Obstructive Sleep Apnea and Prostate Cancer
In Model 1, which did not include any adjustments for variables, there was a negative link between obstructive sleep apnea (OSA) and prostate cancer (OR = 0.66; 95% CI: 0.47–0.93; p=0.02). However, in Model 2, after adjusting for age, smoking habits, hypertension, diabetes, cardiovascular diseases, stroke, alcohol consumption, and body mass index, no significant association was found between OSA and prostate cancer (OR = 0.83; 95% CI: 0.46–1.48; p = 0.49) (Table 2).
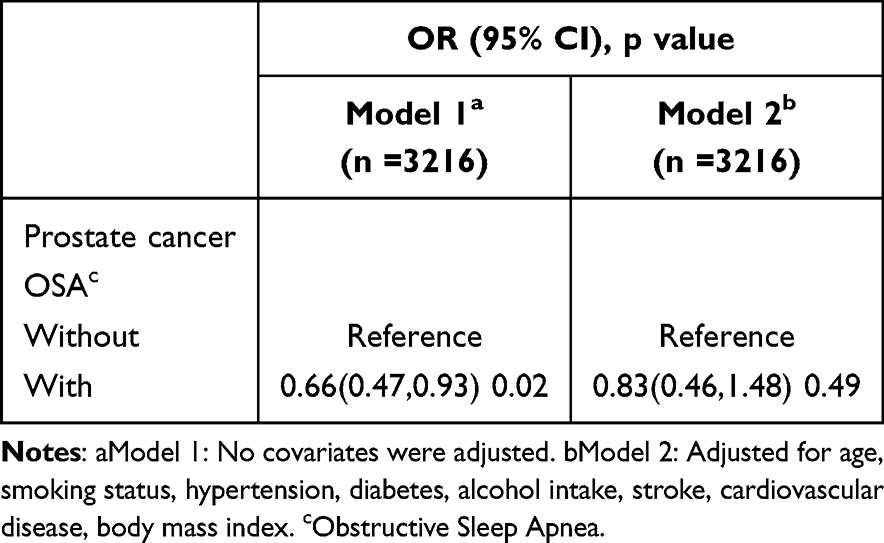 |
Table 2 Association of Obstructive Sleep Apnea with Prostate Cancer |
Subgroup Analysis
A subgroup analysis was conducted to assess the strength of the relationship between OSA and prostate cancer (Figure 2). We detected interactions between age, smoking habits, hypertension, diabetes, cardiovascular diseases, stroke, and alcohol consumption. The age-stratified analysis revealed a significant negative correlation between OSA and prostate cancer in the younger population (OR = 0.07; 95% CI: 0.01–0.74; p = 0.03), whereas no significant association was found in the elderly population (OR = 1.01; 95% CI: 0.69–1.49; p = 0.96). No statistically significant correlation with the p-value for interaction was observed, suggesting that there was no dependency on factors such as smoking habits, hypertension, diabetes, cardiovascular diseases, stroke, and alcohol consumption (p for interaction >0.05).
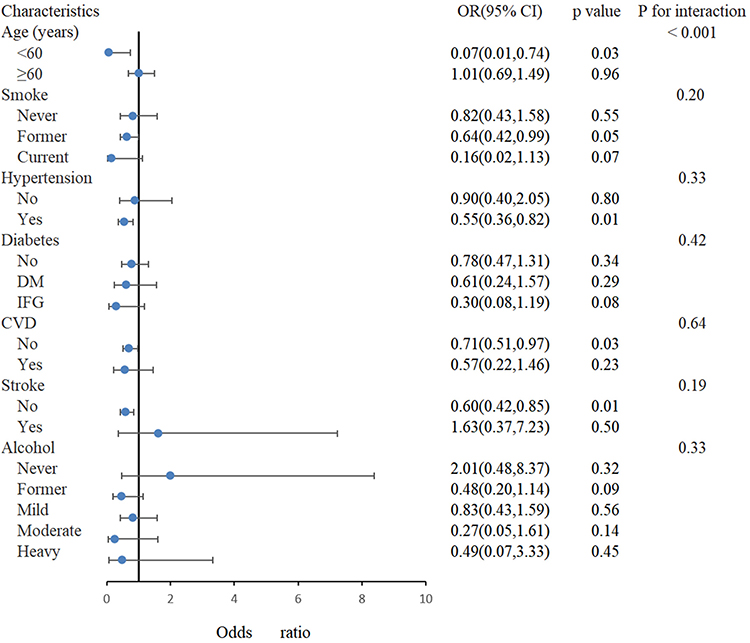 |
Figure 2 Subgroup analysis (forest plots). |
Results of Two-Sample MR Analysis
We rigorously screened all data and the final genetic instrumental variables included in the analyses had F-values greater than 10, indicating that the genetic instrumental variables of OSA are less likely to be affected by bias from weak instrumental variables. Subsequently, a selected set of SNPs was used as genetic instrumental variables in Mendelian randomization (MR) studies, as detailed in Supplementary Table 1. We did not observe a significant causal relationship between OSA and prostate cancer (OR = 0.992; 95% CI: 0.876–1.124; p = 0.906) and the results of our Bayesian Mendelian randomization analysis remained consistent (OR = 0.993; 95% CI: 0.881–1.121; p = 0.916). The results of the analyses for all methods can be found in Figure 3. Although our Cochran’s Q statistic showed presence of heterogeneity, both MR-Pleiotropy residuals as well as MR-PRESSO suggested the absence of horizontal pleiotropy, as shown in Table 3. Scatter plots, leave-one-out plots, forest plots and funnel plots pertinent to MR are available in Figures 4–7.
 |
Table 3 Heterogeneity and Pleiotropy Test |
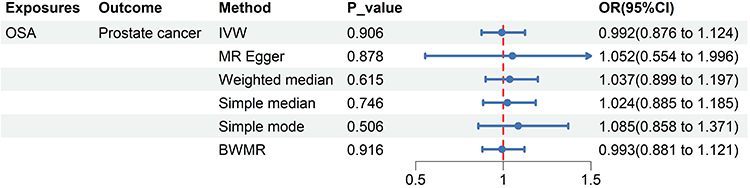 |
Figure 3 Causal relationship between Obstructive sleep apnea with prostate cancer. |
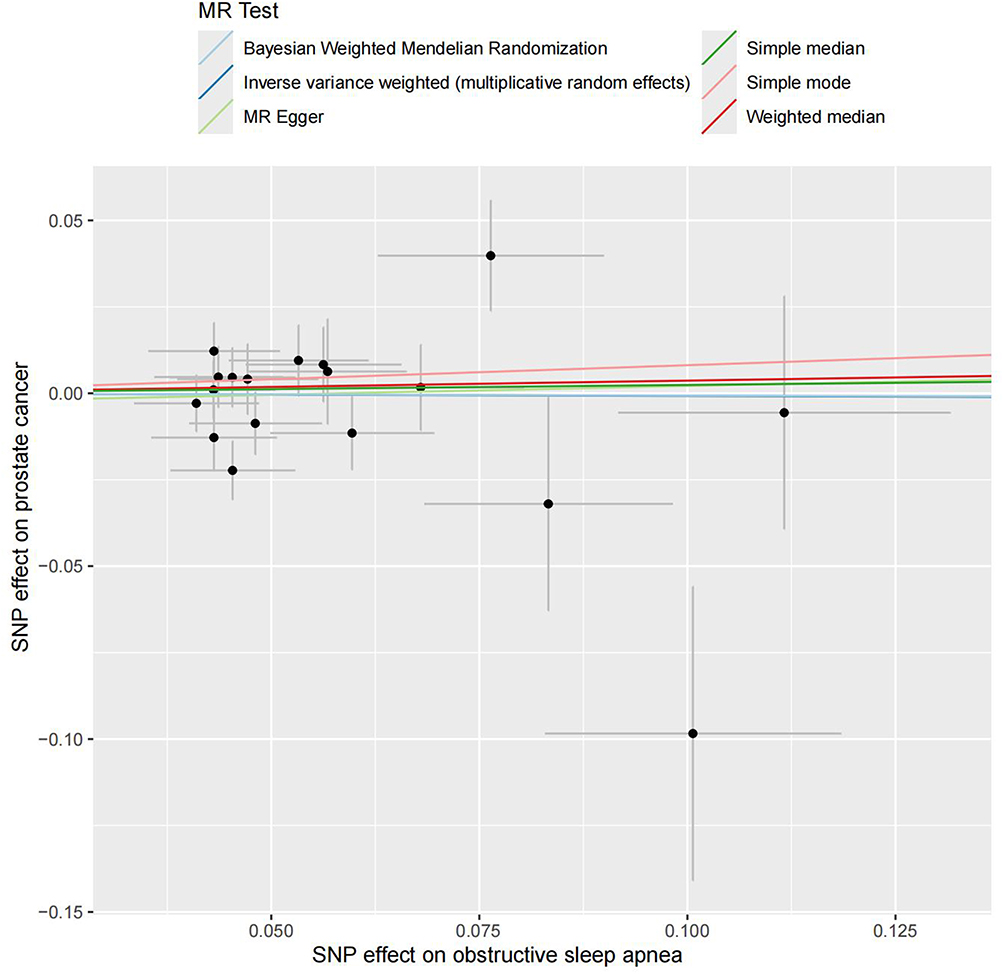 |
Figure 4 The scatter plot for MR analyses of causal associations between obstructive sleep apnea SNPs and prostate cancer. |
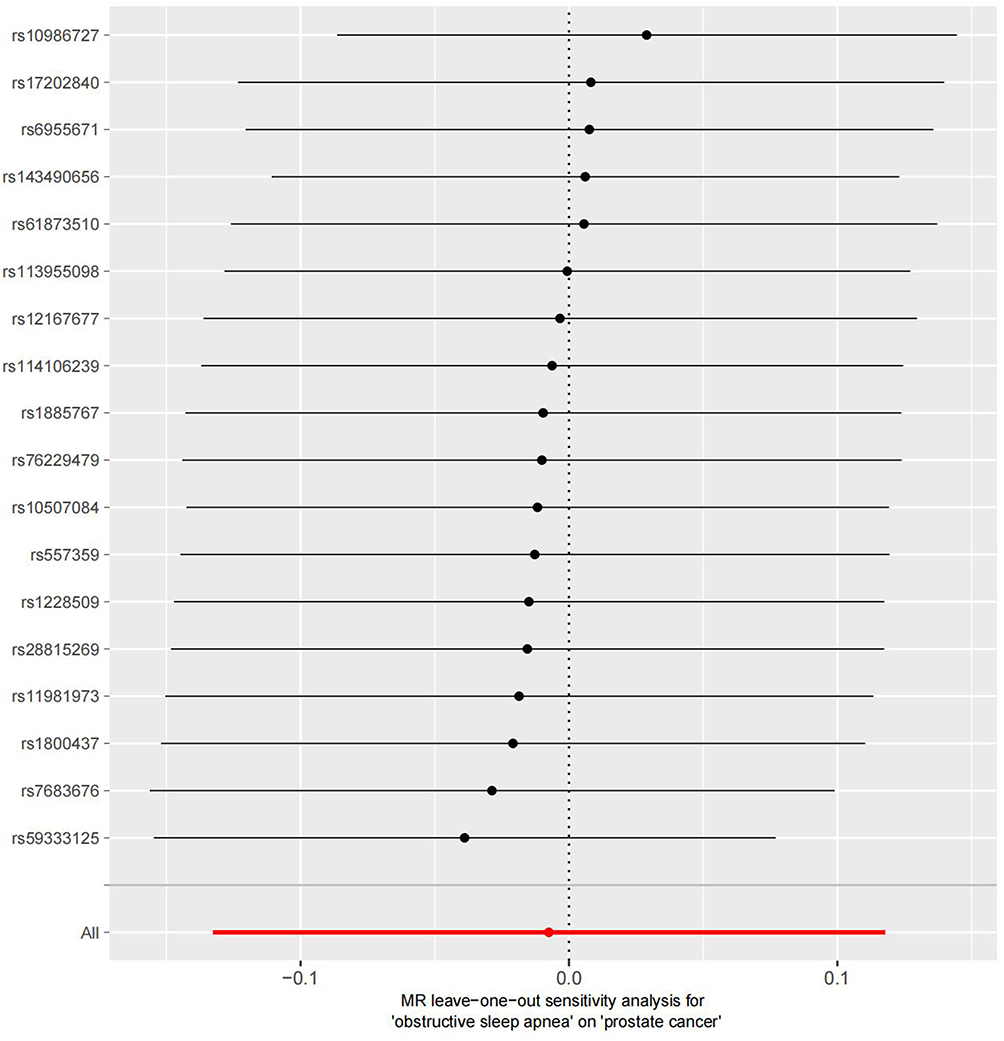 |
Figure 5 Leave-one-out sensitivity analysis for prostate cancer using SNPs associated obstructive sleep apnea. |
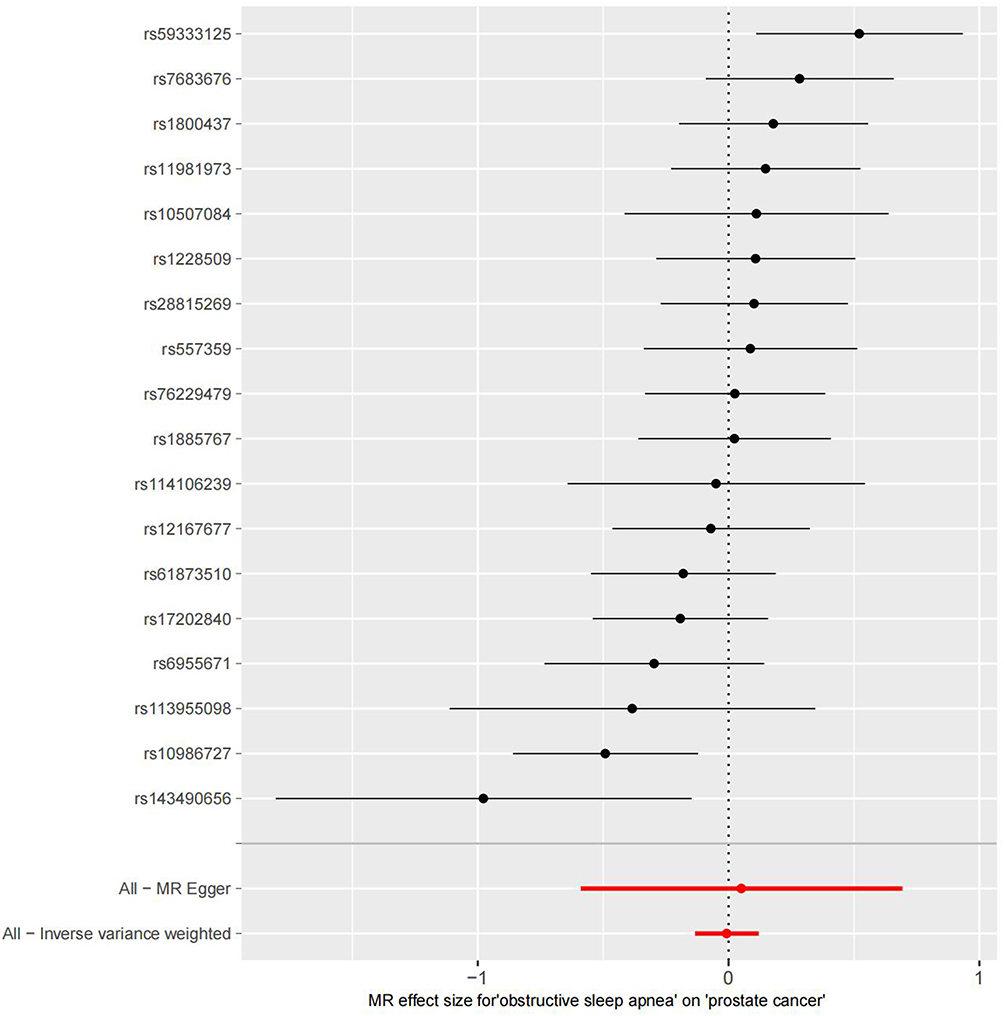 |
Figure 6 The forest plots for MR analyses of causal associations between obstructive sleep apnea SNPs and prostate cancer. |
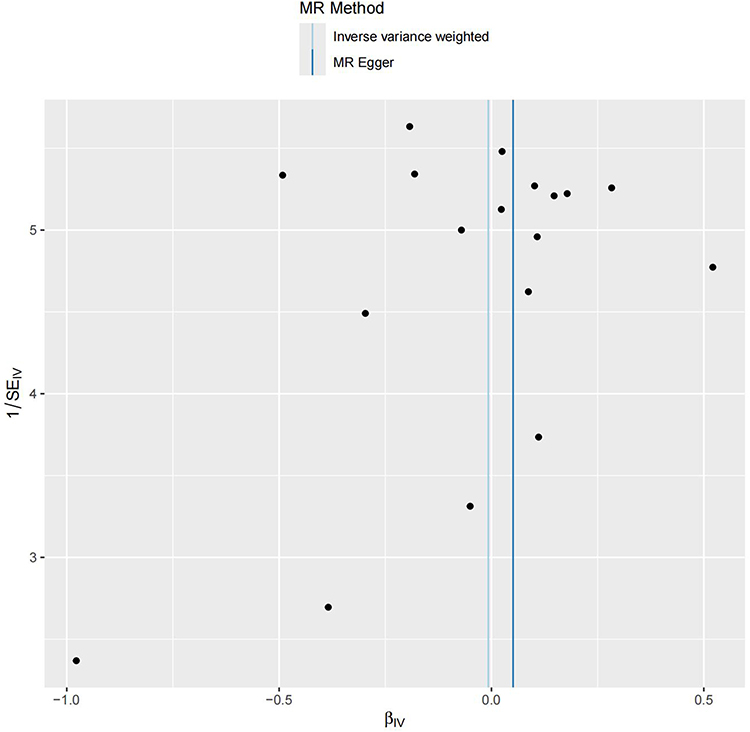 |
Figure 7 The funnel plot for MR analyses of causal associations between obstructive sleep apnea SNPs and prostate cancer. |
Discussion
This study used the NHANES database to explore the relationship between OSA and prostate cancer. Multivariable regression analysis showed no significant association between OSA and prostate cancer after controlling for confounders. However, age-stratified analysis revealed a negative correlation between OSA and prostate cancer in individuals under 60, while no significant relationship was found in those over 60. The lack of significant association in the Mendelian randomization analysis may be due to the inability to perform age stratification. These findings offer new insights into the OSA-prostate cancer connection.
Intermittent hypoxia (IH) is a core feature of obstructive sleep apnea (OSA) in clinical pathophysiology. Chronic cyclical severe hypoxia (30–90 seconds) is considered a primary mechanism leading to the adverse systemic outcomes of OSA. Intermittent hypoxia (IH) can induce the production of hypoxia-inducible factor-1α (HIF-1α), which plays a crucial role in tumor metastasis and angiogenesis. The overexpression of HIF-1α in prostate cancer cells further suggests a potential link between obstructive sleep apnea (OSA) and prostate cancer.19,20 In addition, chronic hypoxic conditions are also involved in the early development of prostate cancer, playing a key role in tumor proliferation and hormone-refractory progression.21–24
The desaturation-reoxygenation sequence results in oxidative stress and the production of reactive oxygen species (ROS).25 Elevated ROS levels lead to increased expression of adhesion molecules,26 leukocyte activation,27 and systemic inflammation.28 Oxidative stress, systemic inflammation, and sympathetic activation underlie the significant cardiovascular and metabolic complications in OSA. Thus, OSA should be regarded as a systemic disease, with IH causing detrimental effects throughout the organism.
However, some arguments suggest that hypoxia exposure may also lead to beneficial adaptations in the body, protecting it from various pathological conditions. For decades, athletes have used hypoxic training as a strategy to enhance performance, with methods and techniques becoming increasingly sophisticated.29 Interestingly, epidemiological data indicate that living at moderate altitudes may be associated with lower obesity rates.30–32 Although IH is generally considered harmful in OSA, some findings suggest that moderate OSA might offer protection against ischemia-reperfusion events.33,34 In this context, IH could enhance the number and function of endothelial progenitor cells, promoting angiogenesis and coronary collateral vessels.35 These factors could potentially reduce the incidence of prostate cancer.
In elderly men, the ratio of estrogen to androgen increases significantly parallel to the decrease in testosterone (T) levels.36 Recent studies suggest that not only low T levels but also an increase in estrogen may promote the progression of prostate cancer.37 This may obscure age-specific associations observed in younger populations. Specifically, age-related hormonal differences may play an important role: younger men typically have higher levels of testosterone and dihydrotestosterone, and endocrine alterations related to OSA at this stage may not exert strong pro-carcinogenic effects.38 In addition, younger individuals generally have fewer comorbidities and more active immune surveillance, which may counteract some of the tumor-promoting effects of intermittent hypoxia. By contrast, older men are more susceptible to immunosenescence, and the cumulative burden of hypoxia and oxidative stress may amplify cancer risk.39,40 Furthermore, the higher prevalence of comorbidities and metabolic dysfunction in older populations could further contribute to cancer development.41 These mechanisms provide a plausible biological explanation for the observed age-specific associations.
Compared to the findings of Fang et al, who reported a significantly higher risk of prostate cancer in OSA patients based on data from the Taiwan National Health Insurance Database,6 this may be due to the lack of adjustment for certain confounding factors in their study. In contrast, our overall results align with Wu et al, who found no significant impact of OSA on prostate cancer.7 This discrepancy might be due to the lack of age-stratified analysis in their study. When we stratified by age, we discovered a negative correlation between OSA and prostate cancer in individuals under 60, consistent with findings from a large, nationally representative health insurance database.8
Although our MR analyses did not provide evidence for a causal relationship, these null findings are still clinically informative. They suggest that the associations observed in previous observational studies may be due to confounding or bias rather than a direct causal link, and therefore should be interpreted with caution in clinical practice. Further large-scale and well-designed studies are warranted before firm clinical recommendations can be made.
This study has several strengths: First, it utilizes the nationally representative NHANES data, providing a large sample size and good external validity. Second, it employs Mendelian Randomization to systematically explore the relationship between OSA and prostate cancer, offering more robust causal inferences. However, there are limitations: The cross-sectional design limits causal determination, and despite Mendelian Randomization, statistical power constraints remain, such as the inability to perform age stratification. NHANES data reliance on self-reporting introduces potential bias, future studies incorporating objective diagnostic approaches are warranted to validate and strengthen our findings. Future GWAS using objectively defined OSA phenotypes based on polysomnography could provide more accurate and reliable insights into the genetic architecture of the disorder. This study is based on cross-sectional prevalence data and lacks stratification by OSA severity, which may introduce selection bias. Future studies using longitudinal incidence data and incorporating OSA severity will help to better elucidate the age- and severity-dependent associations between OSA and prostate cancer. Additionally, small subgroup sample sizes in stratified analyses may affect the stability and reliability of statistical results.
Conclusion
The findings indicate that while there is no significant association between OSA and prostate cancer in the overall analysis, a significant negative correlation exists in the younger population. This suggests that age may play a crucial moderating role in the relationship between OSA and prostate cancer. The lack of significant association in the Mendelian randomization analysis may be due to the inability to perform age stratification. Further prospective studies and mechanistic research are needed to better understand the biological mechanisms underlying this association.
Data Sharing Statement
This study utilized publicly available datasets for analysis. The original contributions made to the research are outlined in the article/Supplementary material; for additional inquiries, please contact the corresponding author.
Ethics Approval
The Ethics Committee of the affiliated hospital of North Sichuan Medical College strictly adheres to the Declaration of Helsinki and the International Ethical Guidelines for Health-related Research Involving Humans, performing independent ethical review responsibilities. This study uses legally obtained publicly available data, meeting the conditions for exemption from review as stated in the Ethical Review Methods for Life Sciences and Medical Research Involving Humans.
Acknowledgments
Ying Liu, Binglei Jiang and Long Xia are co-first authors for this study. We sincerely thank everyone who contributed to and took part in the National Health and Nutrition Examination Survey. Additionally, we extend our appreciation to the researchers from the PRACTICAL Consortium and FinnGen database for making genome-wide association study data available for this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that there are no financial or non-financial interests that could have influenced the manuscript.
Disclosure
The authors have no relevant conflicts of interest for this work.
References
1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.21590
2. Punjabi NM. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):136–143. doi:10.1513/pats.200709-155MG
3. Somers VK, White DP, Amin R, et al. Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, stroke council, and council on cardiovascular nursing. J Am Coll Cardiol. 2008;52(8):686–717. doi:10.1016/j.jacc.2008.05.002
4. Rankin EB, Giaccia AJ. The role of hypoxia-inducible factors in tumorigenesis. Cell Death Differ. 2008;15(4):678–685. doi:10.1038/cdd.2008.21
5. Almendros I, Montserrat JM, Torres M, et al. Intermittent hypoxia increases melanoma metastasis to the lung in a mouse model of sleep apnea. Respir Physiol Neurobiol. 2013;186(3):303–307. doi:10.1016/j.resp.2013.03.001
6. Fang HF, Miao NF, Chen CD, Sithole T, Chung MH. Risk of cancer in patients with insomnia, parasomnia, and obstructive sleep apnea: a nationwide nested case-control study. J Cancer. 2015;6(11):1140–1147. doi:10.7150/jca.12490
7. Wu D, Zhao Z, Chen C, et al. Impact of obstructive sleep apnea on cancer risk: a systematic review and meta-analysis. Sleep Breath. 2023;27(3):843–852. doi:10.1007/s11325-022-02695-y
8. Gozal D, Ham SA, Mokhlesi B. Sleep apnea and cancer: analysis of a nationwide population sample. Sleep. 2016;39(8):1493–1500. doi:10.5665/sleep.6004
9. Smith GD, Ebrahim S. “Mendelian randomization”: can genetic epidemiology contribute to understanding environmental determinants of disease? Int J Epidemiol. 2003;32(1):1–22. doi:10.1093/ije/dyg070
10. Vanderweele TJ, Tchetgen TE, Cornelis M, Kraft P. Methodological challenges in mendelian randomization. Epidemiology. 2014;25(3):427–435. doi:10.1097/EDE.0000000000000081
11. Schumacher FR, Al OA, Berndt SI, et al. Association analyses of more than 140,000 men identify 63 new prostate cancer susceptibility loci. Nat Genet. 2018;50(7):928–936. doi:10.1038/s41588-018-0142-8
12. Hemani G, Zheng J, Elsworth B, et al. The MR-base platform supports systematic causal inference across the human phenome. Elife. 2018;7. doi:10.7554/eLife.34408
13. Burgess S, Thompson SG. Erratum to: interpreting findings from mendelian randomization using the MR-egger method. Eur J Epidemiol. 2017;32(5):391–392. doi:10.1007/s10654-017-0276-5
14. Bowden J, Davey SG, Haycock PC, Burgess S. Consistent Estimation In Mendelian Randomization With Some Invalid Instruments Using A Weighted Median Estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
15. Ren Z, Simons P, Wesselius A, Stehouwer C, Brouwers M. Relationship between NAFLD and coronary artery disease: a mendelian randomization study. Hepatology. 2023;77(1):230–238. doi:10.1002/hep.32534
16. Bowden J, Del GMF, Minelli C, et al. Improving the accuracy of two-sample summary-data Mendelian randomization: moving beyond the NOME assumption. Int J Epidemiol. 2019;48(3):728–742. doi:10.1093/ije/dyy258
17. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
18. Zhao J, Ming J, Hu X, Chen G, Liu J, Yang C. Bayesian weighted Mendelian randomization for causal inference based on summary statistics. Bioinformatics. 2020;36(5):1501–1508. doi:10.1093/bioinformatics/btz749
19. Zhong H, De Marzo AM, Laughner E, et al. Overexpression of hypoxia-inducible factor 1alpha in common human cancers and their metastases. Cancer Res. 1999;59(22):5830–5835.
20. Ghafar MA, Anastasiadis AG, Chen MW, et al. Acute hypoxia increases the aggressive characteristics and survival properties of prostate cancer cells. Prostate. 2003;54(1):58–67. doi:10.1002/pros.10162
21. Stewart GD, Ross JA, Mclaren DB, Parker CC, Habib FK, Riddick AC. The relevance of a hypoxic tumour microenvironment in prostate cancer. BJU Int. 2010;105(1):8–13. doi:10.1111/j.1464-410X.2009.08921.x
22. Butterworth KT, Mccarthy HO, Devlin A, et al. Hypoxia selects for androgen independent LNCaP cells with a more malignant geno- and phenotype. Int, J, Cancer. 2008;123(4):760–768. doi:10.1002/ijc.23418
23. Fraga A, Ribeiro R, Principe P, Lopes C, Medeiros R. Hypoxia and prostate cancer aggressiveness: a tale with many endings. Clin Genitourin Cancer. 2015;13(4):295–301. doi:10.1016/j.clgc.2015.03.006
24. Hakim F, Wang Y, Zhang SX, et al. Fragmented sleep accelerates tumor growth and progression through recruitment of tumor-associated macrophages and TLR4 signaling. Cancer Res. 2014;74(5):1329–1337. doi:10.1158/0008-5472.CAN-13-3014
25. Lavie L. Obstructive sleep apnoea syndrome--an oxidative stress disorder. Sleep Med Rev. 2003;7(1):35–51. doi:10.1053/smrv.2002.0261
26. Baguet JP, Barone-Rochette G, Tamisier R, Levy P, Pepin JL. Mechanisms of cardiac dysfunction in obstructive sleep apnea. Nat Rev Cardiol. 2012;9(12):679–688. doi:10.1038/nrcardio.2012.141
27. Schulz R, Mahmoudi S, Hattar K, et al. Enhanced release of superoxide from polymorphonuclear neutrophils in obstructive sleep apnea. Impact of continuous positive airway pressure therapy. Am J Respir Crit Care Med. 2000;162(2 Pt 1):566–570. doi:10.1164/ajrccm.162.2.9908091
28. Garvey JF, Taylor CT, Mcnicholas WT. Cardiovascular disease in obstructive sleep apnoea syndrome: the role of intermittent hypoxia and inflammation. Eur Respir J. 2009;33(5):1195–1205. doi:10.1183/09031936.00111208
29. Millet GP, Roels B, Schmitt L, Woorons X, Richalet JP. Combining hypoxic methods for peak performance. Sports Med. 2010;40(1):1–25. doi:10.2165/11317920-000000000-00000
30. Sherpa LY, Stigum H, Chongsuvivatwong V, Thelle DS, Bjertness E, Bjertness E. Obesity in Tibetans aged 30-70 living at different altitudes under the north and south faces of Mt Everest. Int J Environ Res Public Health. 2010;7(4):1670–1680. doi:10.3390/ijerph7041670
31. Santos JL, Perez-Bravo F, Carrasco E, Calvillan M, Albala C. Low prevalence of type 2 diabetes despite a high average body mass index in the Aymara natives from Chile. Nutrition. 2001;17(4):305–309. doi:10.1016/s0899-9007(00)00551-7
32. Voss JD, Masuoka P, Webber BJ, Scher AI, Atkinson RL. Association of elevation, urbanization and ambient temperature with obesity prevalence in the United States. Int J Obes. 2013;37(10):1407–1412. doi:10.1038/ijo.2013.5
33. Steiner S, Schueller PO, Schulze V, Strauer BE. Occurrence of coronary collateral vessels in patients with sleep apnea and total coronary occlusion. Chest. 2010;137(3):516–520. doi:10.1378/chest.09-1136
34. Lavie L, Lavie P. Ischemic preconditioning as a possible explanation for the age decline relative mortality in sleep apnea. Med Hypotheses. 2006;66(6):1069–1073. doi:10.1016/j.mehy.2005.10.033
35. Lavie L. Oxidative stress in obstructive sleep apnea and intermittent hypoxia--revisited--the bad ugly and good: implications to the heart and brain. Sleep Med Rev. 2015;20:27–45. doi:10.1016/j.smrv.2014.07.003
36. Belanger A, Candas B, Dupont A, et al. Changes in serum concentrations of conjugated and unconjugated steroids in 40- to 80-year-old men. J Clin Endocrinol Metab. 1994;79(4):1086–1090. doi:10.1210/jcem.79.4.7962278
37. Corona G, Vignozzi L, Rastrelli G, Lotti F, Cipriani S, Maggi M. Benign prostatic hyperplasia: a new metabolic disease of the aging male and its correlation with sexual dysfunctions. Int J Endocrinol. 2014;2014:329456. doi:10.1155/2014/329456
38. Luboshitzky R, Lavie L, Shen-Orr Z, Herer P. Altered luteinizing hormone and testosterone secretion in middle-aged obese men with obstructive sleep apnea. Obes Res. 2005;13(4):780–786. doi:10.1038/oby.2005.88
39. Ovadya Y, Landsberger T, Leins H, et al. Impaired immune surveillance accelerates accumulation of senescent cells and aging. Nat Commun. 2018;9(1):5435. doi:10.1038/s41467-018-07825-3
40. Guo X, Liu Y, Kim JL, et al. Effect of cyclical intermittent hypoxia on Ad5CMVCre induced solitary lung cancer progression and spontaneous metastases in the KrasG12D+; p53fl/fl; myristolated p110fl/fl ROSA-gfp mouse. PLoS One. 2019;14(2):e0212930. doi:10.1371/journal.pone.0212930
41. Ip MS, Lam B, Ng MM, Lam WK, Tsang KW, Lam KS. Obstructive sleep apnea is independently associated with insulin resistance. Am J Respir Crit Care Med. 2002;165(5):670–676. doi:10.1164/ajrccm.165.5.2103001
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.