Back to Journals » Nature and Science of Sleep » Volume 17

Excessive Screen Time Associated with Emotional and Behavioral Problems Mediated by Sleep Disturbance Among Young Children
Authors You Y, Chen Y, Shang J, Tan L, Yu M, Wu Y, Li B, Guo P, Zhang Q ![]()
Received 26 June 2025
Accepted for publication 12 October 2025
Published 21 October 2025 Volume 2025:17 Pages 2757—2770
DOI https://doi.org/10.2147/NSS.S549178
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Valentina Alfonsi
Yingbin You,1,* Yuhui Chen,2,* Jianhui Shang,2 Leyun Tan,2 Mingtao Yu,2 Yueyang Wu,2 Boya Li,2 Pi Guo,2 Qingying Zhang2
1Department of Administrative, Affiliated Hospital Group of Guangdong Medical University Shenzhen Baoan Central Hospital (Baoan Central Hospital of Shenzhen), Shenzhen, Guangdong, People’s Republic of China; 2Department of Preventive Medicine, Shantou University Medical College, Shantou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qingying Zhang, Department of Preventive Medicine, Shantou University Medical College, Shantou, Guangdong, People’s Republic of China, Tel +86-754-88900445, Fax +86-754-88566774, Email [email protected]
Objective: We examined whether excessive screen time (ST) is associated with emotional and behavioral problems (EBPs) in young school children mediated by sleep disturbance.
Methods: This was a cross-sectional survey of 3883 children aged 7– 9 years at 18 primary schools in Shenzhen. Data on children’s ST on weekdays and weekends as well as household environment, parental ST, and parental accompaniment time were collected. Sleep disturbance and EBPs were assessed with the Sleep Disturbance Scale for Children and the Strengths and Difficulties Questionnaire (SDQ), respectively. Odds ratios (ORs) and 95% confidence intervals (CIs), the average causal mediation effects and the average direct effects were estimated.
Results: Overall, 15.7% of children had ST in excess of the recommended 2 hr/day, and 24.1% of parents reported that their child had a sleep disturbance. The total SDQ score was higher for children with than without ST ≥ 2 hr/day and sleep disturbance (P< 0.001). After adjustment for potential confounders, children with ST ≥ 2 hours/day had increased odds of sleep disturbances (OR 1.99, 95% CI 1.65– 2.33). The odds of EBPs were increased for children with ST ≥ 2 hr/day (OR 1.34, 95% CI 1.11– 1.64) and sleep disturbance (OR 2.77, 95% CI 2.23– 3.22). Mediation analysis indicated that sleep disturbance partially explained the association between ST and EBPs (all effects statistically significant, P < 0.001).
Conclusion: Excessive ST was significantly associated with EBPs and may be mediated by sleep disturbance. Reducing children’s ST and encouraging good sleep practices may enhance mental health.
Keywords: children, electronic products, sleep, emotional and behavioral problem
Introduction
With the rapid proliferation of information and communication technologies in China, both children and adults increasingly use electronic devices throughout the day and night. Excessive screen time (ST) has been linked to various adverse health outcomes in children, including myopia, obesity, and insufficient sleep.1–3 A Chinese study showed that ST of more than 60 minutes was associated with poor performance on development tests.4 According to the recommendations of the American Academy of Pediatrics,5 excessive ST (≥2 hr/day) was considered when the average ST per day was >2 hr. Guo et al’s study found that 36.8% of the children and adolescents exceeded the recommended ST of 2 hr/day.6 However, this study did not include school children aged 7–9 years old in first grade to second grade. We need to know the current state of the ST of children in this age group because children’s screen habits tend to develop during age 5–12 years. The detrimental effects of excessive ST may persist from childhood into adulthood.7 International systematic reviews have indicated that excessive ST adversely affects psychophysiological health, including its role in inducing sleep disturbances and contributing to emotional and behavioral problems (EBPs) in children.8,9
Sleep disturbance refers to “the perceived or actual alterations in nighttime sleep (quantity and quality) with subsequent daytime impairment”.10 A systematic review conducted in Western populations has demonstrated that screen use behaviors can induce sleep disturbances,11 and another study reported a dose–response relationship between ST and sleep disturbances.12 A comparable study on sleep disturbances and EBPs in Chinese and Japanese preschoolers demonstrated that sleep disturbances were associated with EBPs.13 Furthermore, a prospective cohort study indicated that sleep disturbances identified in late childhood may contribute to the development of EBPs in adolescence, with a dose–response relationship observed between the two.14 Studies in Western populations have further shown that increased ST and sleep disturbances are linked to persistent and distressing psychotic-like experiences, which are themselves associated with EBPs.15,16 Moreover, sleep disturbances constitute a risk factor for suicidal behaviors among individuals with severe EBPs.17,18 Based on this body of evidence, we conceptualize a mediation framework in which excessive ST serves as the independent variable, sleep disturbance functions as the mediating variable, and EBPs act as the dependent variable. Within this framework, excessive ST may first induce an increase in sleep disturbances; subsequently, these elevated sleep disturbances, as an intermediate mechanism, may further contribute to the exacerbation of EBPs.19
Strengths and Difficulties Questionnaire (SDQ) is an effective tool to identify children’s psychosocial problems.20 A study of SDQ use in 5959 school students in grades 3 to 8 from 4 cities in China showed that ST and negative life events were significantly correlated with EBPs.21 However, there have been few studies using SDQ to investigate the relationship between ST and sleep duration associated with EBPs in children.
While numerous studies have investigated the link between ST, sleep disturbances, and EBPs, the outcomes have been inconsistent due to differences in study populations and methodologies. Moreover, whether sleep disturbance plays a mediating role between excessive ST and EBPs in young school-age children remains unclear, and this relationship warrants further investigation. As the financial center of China, Shenzhen is at the forefront of science and technology. Children in Shenzhen have easy access to electronic products. Therefore, this study aimed to investigate the prevalence of excessive ST in children aged 7–9 years in Shenzhen, explore the link between excessive ST and EBPs, and to assess whether sleep disturbances mediate this connection. At the same time, we considered the family environment, parents’ behavior and other information as possible factors. The findings may inform targeted interventions to foster healthy screen and sleep habits and to promote mental health in children.
Methods
Study Design and Data Collection
The Children Lifeway Cohort was developed to investigate lifestyle and related metabolic disease in a prevention and treatment program for children in the Baoan district of Shenzhen, China. This cohort recruited second-grade students from 19 of the 134 local primary schools by using cluster sampling in September 2018. In the end, 18 schools were willing to participate. In September 2019, the study administered a questionnaire about the current situation of electronic products use in children in this cohort. ST was measured as the average screen time during the week preceding the survey to minimize recall bias, whereas sleep disturbance and EBPs were assessed using the Sleep Disturbance Scale for Children (SDSC) and SDQ, respectively, both of which specify a six-month recall period as defined in the official instruments. Given the cross-sectional design, these measurements limit the ability to infer causality or the temporal directionality of the associations.
Electronic questionnaires were sent to the parents or guardians of 4829 children, 4593 were returned (response rate: 95.1%). All questionnaires were completed by the children’s parents or guardians on their behalf. Specifically, the parent or guardian designated as the “first” parent or guardian (ie, the parent or guardian who completed the main questionnaire) was also asked to provide the ST information on behalf of the child. Questionnaires with too much missing information, children who were not aged 7–9, lacked information on ST, or had severe organic diseases or had been hospital-diagnosed EBPs were excluded. Finally, 3883 children were included in the analyses (Figure 1). Informed consent was received from a parent or guardian of each participant, and this project was approved by the medical ethics committee of the Baoan Central Hospital of Shenzhen (no. IRB-PJ-2018-002).
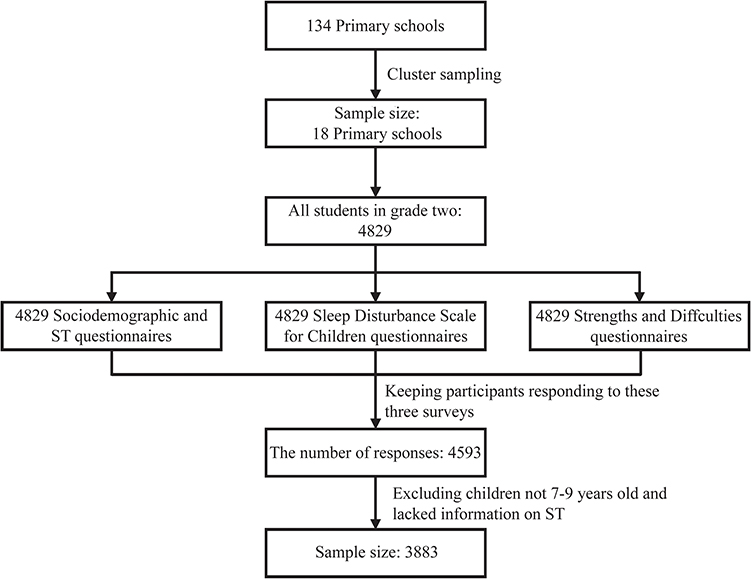 |
Figure 1 Participant recruitment diagram. |
Socio-Demographic Variable and Exposure
The questionnaire included socio-demographic information such as the child’s sex, date of birth, family economic status, family structure and parents’ educational level. The exact questions from the ST-related survey are provided in the Supplementary Material. Average daily ST was calculated as (5/7 × [ST on weekdays] + 2/7 × [ST during the weekend]). The questionnaire showed good reliability and validity with high consistency among measurement items after analyses (Cronbach’s α = 0.866).
Outcome Assessment
Sleep Disturbance
SDSC was used to investigate the status of sleep disturbance in children. The SDSC contains 26 items of six dimensions: disorders of initiating and maintaining sleep, sleep breathing disorder, disorders of arousal, sleep-wake transitions disorders, disorders of excessive somnolence, and sleep hyperhidrosis.13,22 Each item was scored from 1 to 5, with a total score of ≥39 considered a sleep disorder. The Cronbach’s α coefficient was 0. 866. The Kaiser-Meyer-Olkin statistic was 0.811, and the Bartlett spherical test P < 0.001.
EBPs
Children’s emotional problems, behavioral problems, peer interaction and other psychological development characteristics were assessed with the revised SDQ (parental version). The total difficulties score (range 0—40) was calculated as the sum of emotional symptom, conduct problems, hyperactivity, and peer relationship problems scores, excluding the prosocial behavior score. The score was divided into 80th and 90th percentiles; 90th percentiles with a corresponding cutoff value of 17 were considered abnormal, <80th percentiles with a corresponding cutoff value of 14 were considered normal, and 80th to 90th percentiles were considered borderline.23 The SDQ is a dimensional measure without a strict threshold. Previous studies have shown that each additional point on the SDQ total difficulties score is associated with an increased odds of adverse outcomes (OR range: 1.14–1.28).24 To improve statistical power and ensure stability of estimates, we combined children scoring in the “borderline” range with those in the “abnormal” range into a single “at-risk” group, consistent with prior studies.25 Accordingly, the total difficulties score and each subscale were dichotomized as either healthy (normal) or at-risk (borderline and abnormal). The Cronbach’s α was 0.766. The KMO statistic was 0.865, and the Bartlett spherical test P<0.001.
Covariates
Numerous variables such as demographic characteristics (sex, parental educational level, family structure and family economic status), household environment (whether the child sleeps in a bedroom with a TV/computer, whether the child uses electronic devices in a dark environment) and the condition of parental accompaniment (parental ST, parental accompaniment time). The calculation of parental ST was similar to that for children.
Statistical Analysis
Data are described with mean (SD) for continuous variables and number (%) for categorical variables. The chi-squared test was used to assess differences in socio-demographic variables and Mann–Whitney U-test for quantitative data with non-normal distribution. Spearman correlation coefficients (r) were used assess the association of ST and sleep disturbance with SDQ scores. Logistic regression models were used to test the association of exposure variables with risk of EBPs. The package “mediation” of R software was used to analyze the mediating effect of sleep disturbance. We fit a mediator model in which SDSC score ≥39 (mediator) was modeled as a function of the ST ≥ 2 hr/day (treatment) and pre-treatment covariates (socio-demographic variable, covariates) and modeled the outcome variable, which was a binary variable, indicating whether or not the child’s SDQ score was borderline or abnormal (at-risk). The explanatory variables of the outcome model included the mediator, treatment, and the same set of pre-treatment variables as those used in the mediator model. Logistic regression was used to fit the mediator and outcome models, and we used nonparametric bootstrap rather than the quasi-Bayesian Monte Carlo simulation for variance estimation via the boot = TRUE argument, with the default (1000). The average causal mediation effects (ACMEs) and average direct effects (ADE) were estimated by the mediate function. The a priori level of significance was defined as P<0.05. All statistical analyses involved using SPSS 24.0 (IBM Corp., Armonk, NY, USA) and RStudio v1.2.5042.
Results
Participant Characteristics and Proportion by ST
Among the participants, 14.4% of boys and 17.4% of girls had ST ≥ 2 hr/day. Sleep disturbance was reported in 24.3% of boys and 23.8% of girls. The proportion of children at risk of EBPs was 24.7% for boys and 23.6% for girls. The sample characteristics stratified by ST, sleep disturbance and EBPs (at-risk) are in Table 1. The proportion of the children with ST ≥ 2 hr/day varied significantly by sex, family structure, family economic status, parental educational level, maternal accompaniment time, paternal ST ≥ 2 hr/day, maternal ST ≥ 2 hr/day, TV/computer in the child’s bedroom and use of electronic devices in a dark environment. The prevalence of sleep disturbance differed by family structure and parental educational level, etc. Risk of EBPs was related to paternal educational level, parental accompaniment time, TV/computer accessibility in children’s bedroom, and use of electronic devices in a dark environment but did not vary significantly by sex, family structure, or family economic status. We found significant differences in the rate of EBPs among ST and sleep disturbance groups (P < 0.001 for all).
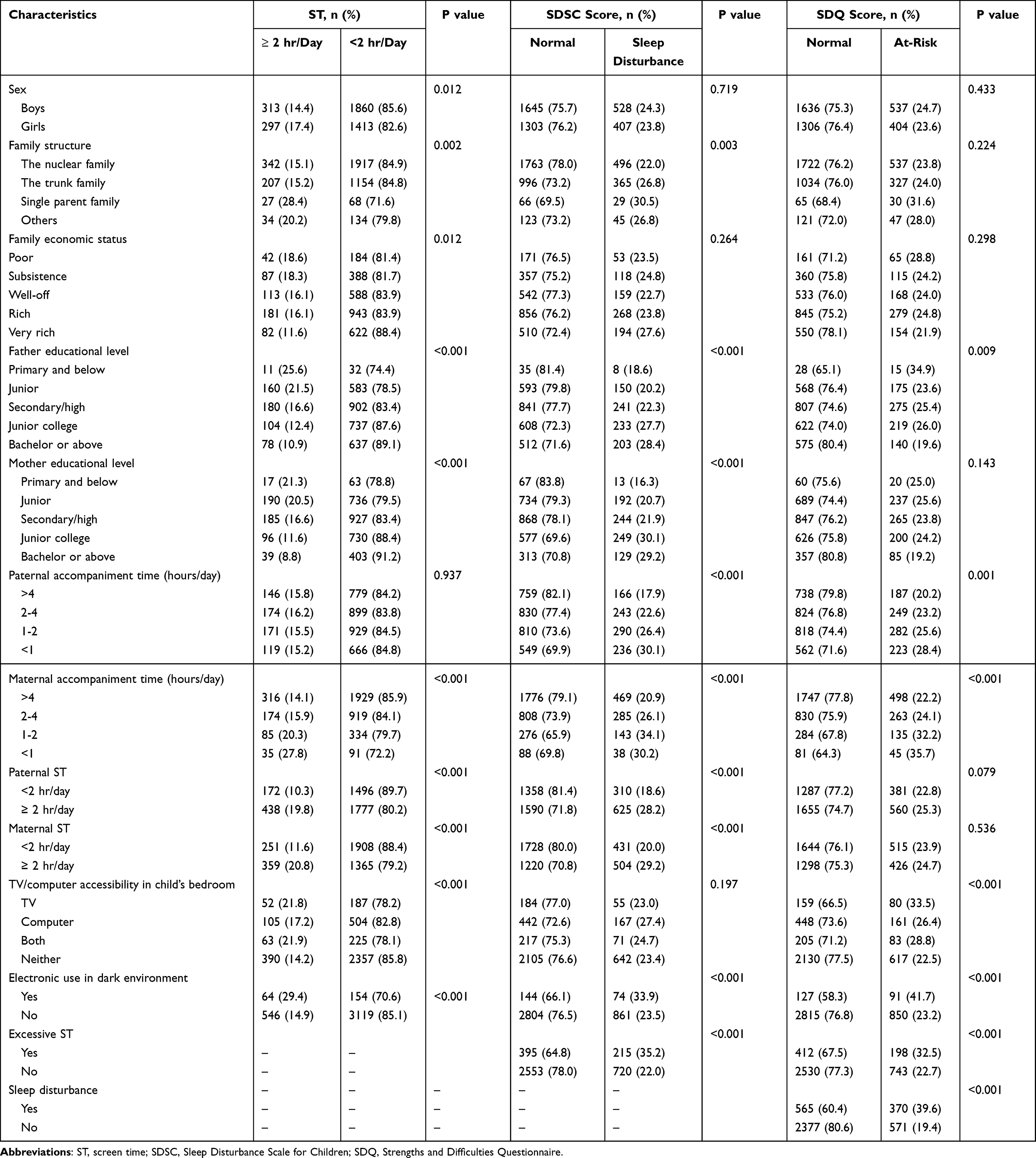 |
Table 1 Characteristics of Children Aged 7–9 years |
Differences Between ST, SDQ and Behavioral Problems
Table 2 reports the mean scores for total and subscale SDQ scores for the different ST and sleep-disturbance groups. Except for the prosocial subscale score, the total and subscale SDQ scores were higher for children with than without ST ≥ 2 hr/day (P < 0.05). The prosocial subscale scores were lower for children with than without ST ≥ 2 hr/day (P < 0.001). Similar results were found for the associations between the total and subscale SDQ scores and sleep disturbance (P < 0.001 for all). For the ST grouping, Cohen’s d was approximately 0.266, which indicates a small effect size, and for the SDSC score grouping, Cohen’s d was approximately 0.595, suggesting a medium effect size.
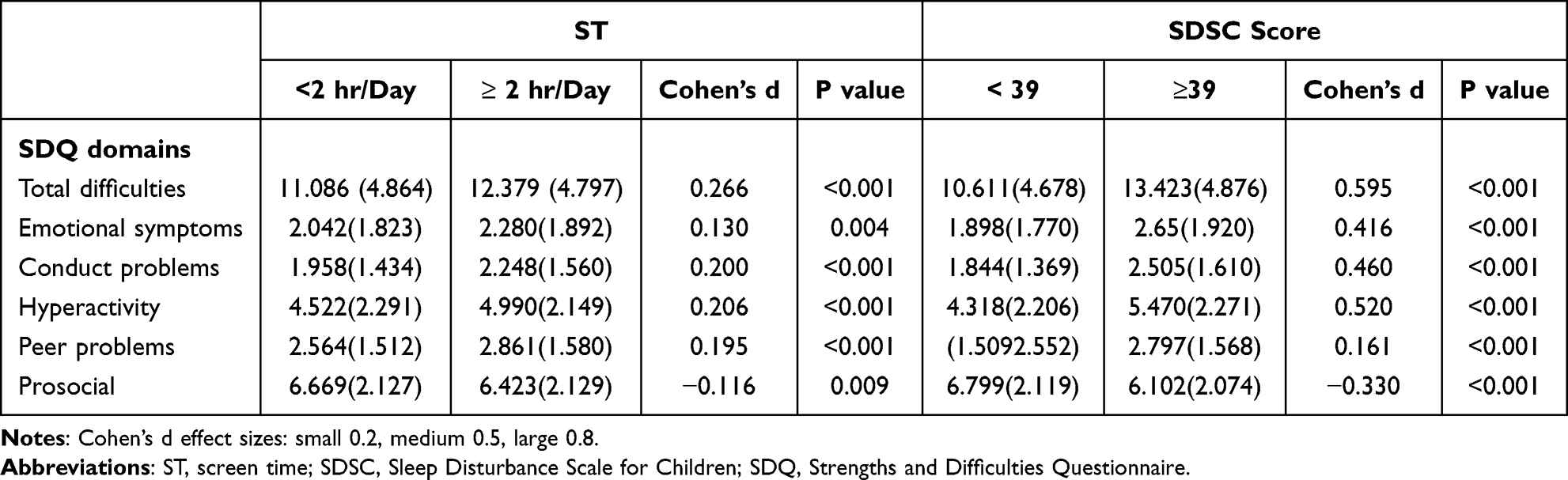 |
Table 2 SDQ Total and Subscale Scores for ST and Sleep Disturbance Groups |
Correlation of ST and SDSC Score with SDQ Score
The correlations of the total and subscale SDQ scores with the continuous predictor variables ST and SDSC score are in Table 3. The mean (SD) total SDQ score was 11.3 (4.9). ST was positively correlated with the total SDQ score (r = 0.118, P < 0.05) and with SDQ subscale scores, except for the prosocial subscale (r = −0.095, P < 0.001). Squaring this correlation coefficient (ie, calculating R²) showed that ST explained approximately 1.4% of the variance in total SDQ scores. Similarly, the SDSC score was positively correlated with the total SDQ score (r = 0.306, P < 0.05) as well as SDQ subscale scores; its R² indicated that SDSC accounted for around 9.4% of the variance in total SDQ scores. Conversely, the SDSC score was negatively correlated with the prosocial subscale score (r = –0.173, P < 0.001).
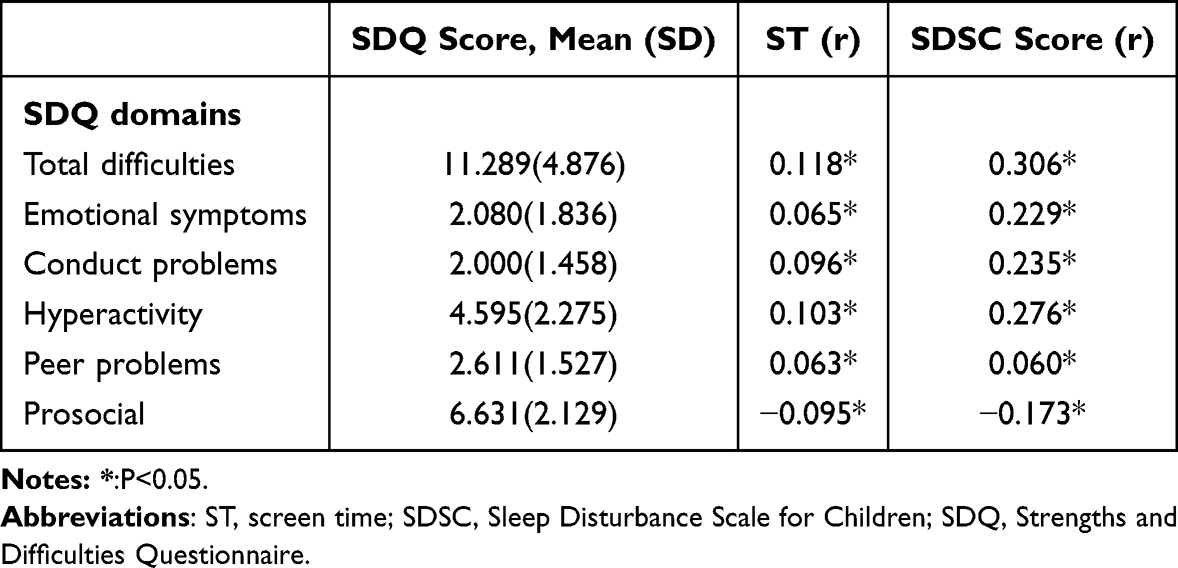 |
Table 3 Correlation of ST and SDSC Score with SDQ Score as a Continuous Variable |
Associations Between Excessive ST and Sleep Disturbance
Table 4 shows the associations between excessive ST and risk of sleep disturbance. All associations were evident in both crude and adjusted models. The probability of sleep disturbance was positively associated with ST ≥ 2 hr/day (OR 1.93, 95% CI 1.60–2.32, P < 0.001, Model 1: not adjusted). ST ≥ 2 hr/day remained a risk factor after adjusting for sex, family structure and parental educational level (Model 2: OR 2.10, 95% CI 1.71–2.58, P < 0.001) and additional variables such as parental ST and parental accompaniment time (Model 3: OR 1.98, 95% CI 1.55–2.36, P < 0.001). In Model 4, additional covariates such as TV/computer accessibility in child’s bedroom and electronic use in the dark were controlled, and the results continued to show that ST ≥ 2 hr/day was a risk factor for sleep disturbance in children (Model 4: OR 1.85, 95% CI 1.50–2.29, P < 0.001), thus indicating that excessive ST had harmful effects on the condition of sleep.
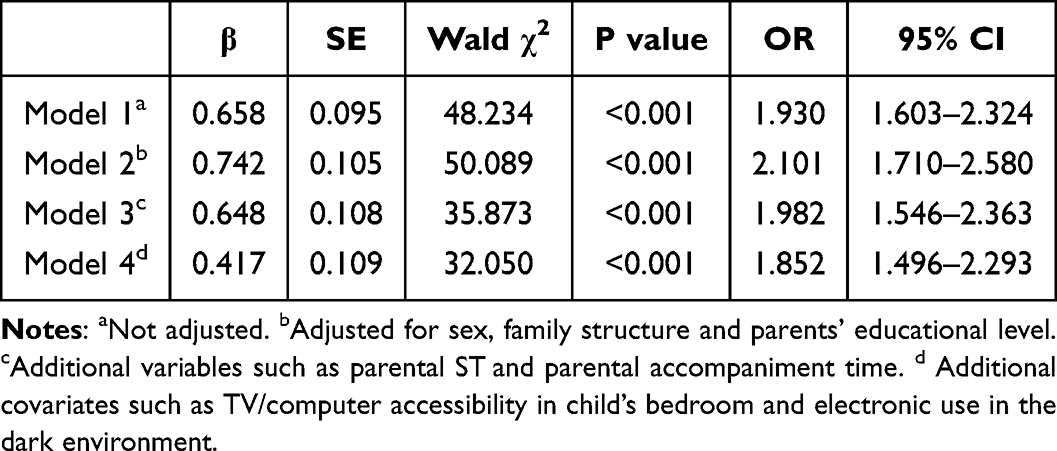 |
Table 4 Association Between ST and Risk of Sleep Disturbance |
Associations Between Excessive ST, Sleep Disturbance and Risk of EBPs
Table 5 shows the analysis of the associations between ST ≥ 2 hr/day and sleep disturbance and risk of EBPs. We adjusted the same covariables in each of the four models as in the mediator model. Probability of EBPs was increased with excessive ST (Model 1: OR 1.45, 95% CI 1.20–1.76, P < 0.001; Model 2: OR 1.33, 95% CI 1.07–1.64, P = 0.011; Model 3: OR 1.35, 95% CI 1.11–1.65, P = 0.011; Model 4: OR 1.34, 95% CI 1.10–1.64, P = 0.004). Children with sleep disturbance showed significantly increased risk of behavioral problems in all models (Model 1: OR 2.64, 95% CI 2.25–3.10; Model 2: OR 2.79, 95% CI 2.34–3.33; Model 3: OR 2.70, 95% CI 2.26–3.23; Model 4: OR 2.66, 95% CI 2.26–3.18; P < 0.001 for all). These findings were inconsistent for each of the SDQ subscales. In model 1, both ST ≥ 2 hr/day and sleep disturbance increased the risk of emotional symptoms (OR 1.23, 95% CI 1.00–1.51 and OR 2.16, 95% CI 1.83–2.57), conduct problems (OR 1.32, 95% CI 1.09–1.58 and OR 2.31, 95% CI 1.98–2.70), hyperactivity (OR 1.35, 95% CI 1.13–1.62 and OR 2.26, 95% CI 1.94–2.63), and peer problems (OR 1.49, 95% CI 1.24–1.79 and OR 1.30, 95% CI 1.09–1.50), whereas sleep disturbance was associated with prosocial behavior (OR 1.62, 95% CI 1.32–1.99). In Model 2, after adjusting for demographic variables, the results changed. The associations were no longer statistically significant between ST ≥ 2 hr/day and emotional symptoms (P = 0.240) and prosocial problems (P = 0.544). In Model 3, sleep disturbance increased the risk of emotional symptoms (OR 2.22, 95% CI 1.84–2.67), conduct problems (OR 2.27, 95% CI 1.92–2.69), hyperactivity (OR 2.29, 95% CI 1.93–2.71), peer problems (OR 1.38, 95% CI 1.16–1.65), and prosocial behavior problems (OR 1.61, 95% CI 1.29–2.01), whereas the association remained non-statistically significant between ST ≥ 2 hr/day and emotional symptoms (P = 0.262) and prosocial problems (P = 0.577). Model 4 results were similar to Model 3 results.
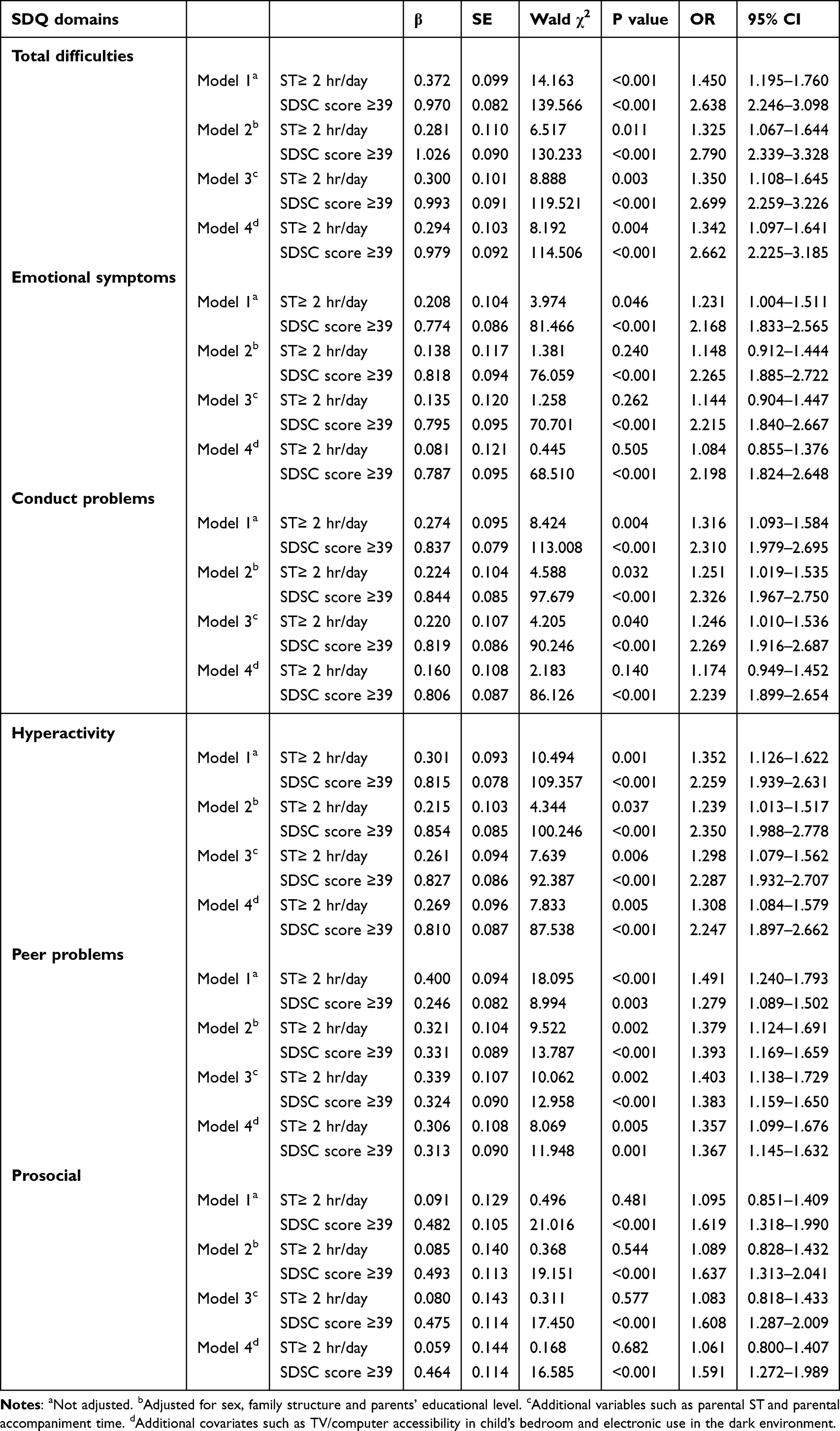 |
Table 5 Associations Between ST, Sleep Disturbance and Risk for Emotional and Behavioral Problems (EBPs) |
The Mediating Effect of Sleep Disturbance
We adjusted for demographic characteristics and covariates to analyze the mediating role of sleep disturbance in the relation between ST ≥ 2 hr/day and SDQ total score ≥39. The estimated ACMEs, ADEs, and total effects were statistically different from zero (P<0.001) (Table 6). The results suggest that ST ≥ 2 hr/day may increase the risk of sleep disturbance, which in turn increased the odds of EBPs. Here, because the outcome was binary, all estimated effects were expressed as an increase in probability. The ACME was 0.0193 and ADE 0.0567, so the mediating effect model could be considered valid, and sleep disturbance partially mediated the correlation between ST ≥ 2 hr/day and risk of EBPs. The proportion of mediation was 25.4% (Figure 2).
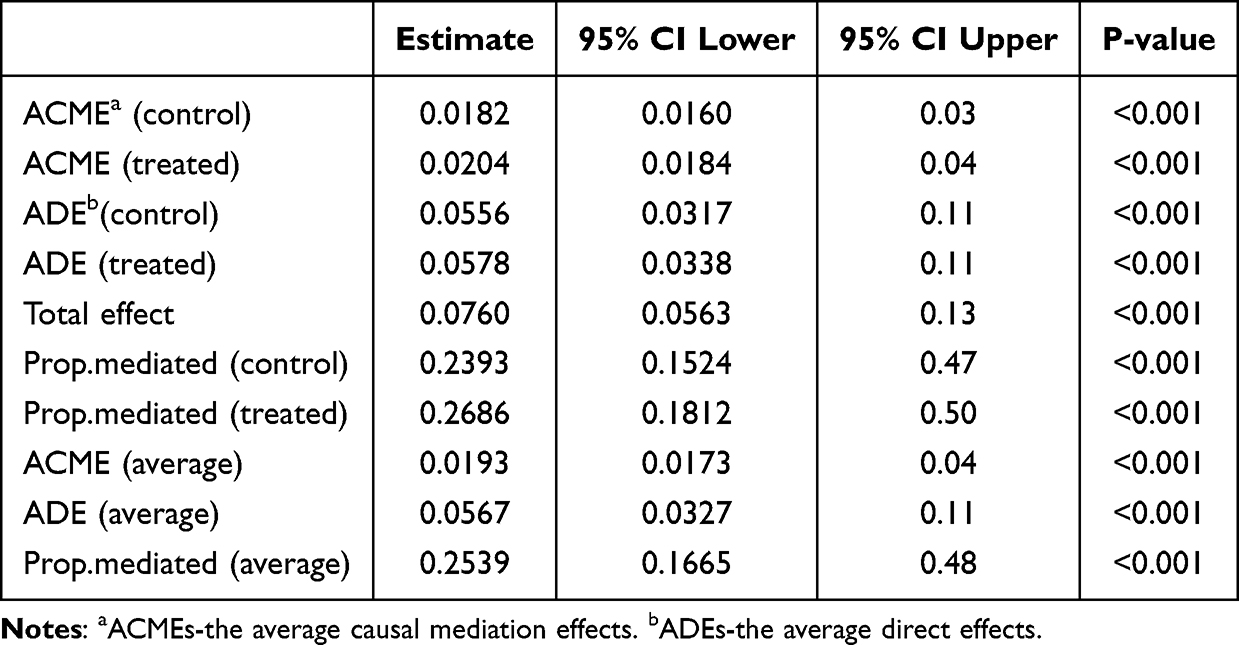 |
Table 6 Mediation Analysis: Excessive ST, Sleep Disturbance and EBPs |
 |
Figure 2 Mediation of sleep disturbance in the association between screen time (ST) and emotional-behavioral problems (EBP) among children. |
Discussion
The present study offered insights into the associations of excessive ST with sleep disturbance and risk of EBPs among school children aged 7–9 in China and further explored whether sleep disturbance plays a mediating role between ST and EBPs. Our results show increased odds of EBPs in young school children with ST ≥ 2 hr/day and sleep disturbance, and sleep disturbance was a significant mediator. Specifically, children with ST ≥ 2 hr/day and sleep disturbance had higher scores on SDQ total difficulties, emotional symptoms, conduct problems, hyperactivity, and peer problems but lower prosocial scores.
As hypothesized, the present study found that children aged 7–9 with ST ≥ 2 hr/day and sleep disturbance were significantly more likely to have EBPs. Sleep disturbance was a significant mediator, although the effect sizes were small. About 15.7% of children had ST in excess of the recommended 2 hr/day, and 24.1% of parents reported that their child had a sleep disturbance. The rate of sleep disturbance was higher for children with ST > 2 hr/day than < 2 hr/day. Logistic regression analysis revealed that excessive ST increased the risk of sleep disturbance in children. ST may affect children by displacing their sleep habits.
A total of 3883 children aged 7–9 in Shenzhen were screened by the SDQ scale for abnormal and borderline total difficulties score, with a positive detection rate of 24.1%. This proportion exceeds the 20% threshold corresponding to the “at risk” category of the SDQ in the general Chinese population, suggesting a higher prevalence of EBPs in the Shenzhen area. Total and subscale SDQ scores were positively correlated with SDSC scores. The present study provides evidence that ST ≥ 2 hr/day was significantly associated with EBPs among children aged 7–9 years, even after adjustment for potential confounders, perhaps because children at this age are at a stage of poor self-control. If they spend too much time watching TV, using mobile phones or computers, they will spend less time interacting with the outside world and playing with their peers, which is not conducive to the development of social functions.
The relation between sleep problems and behavioral problems in children is well established. Lima Santos et al26 reported an association of shorter night-time sleep duration in preschool children with increased likelihood of externalizing behavioral symptoms (overactivity, anger, aggression, impulsivity, tantrums, and annoying behaviors) based on parental reports. Previous studies showed that ST may be associated with increased EBPs in children, including aggression,27 decreased prosocial behavior28 and attention problems.29 A study conducted in Tongling, China, showed a dose-response relation between children’s TV and computer use time and risk of sleep disorders.12 The relation between the time of watching TV and risk of sleep disorders was non-linear J-shaped; that is, the risk of sleep disorders increased with increasing time of watching TV when the time of watching TV exceeded the threshold. When the time of watching TV increased by 1 hr every day, the risk of sleep disorders in children increased by 12.4%. For computer use, the relation was broad linear between the use time and the risk of sleep disorders. Mulla et al30 found that ST of 670 children aged 6 to 14 years in Saudi Arabia and Bahrain was significantly correlated with adverse mental health outcomes, especially emotional symptoms and depressive symptoms. A prospective cohort study in Finland found that ST from childhood were associated with perceived stress and depressive symptoms in adolescence.31 A previous study investigated the relation between ST and mental health of 10,829 school-age children aged 10–12 in Iceland.32 Children with long ST were more likely to feel lonely and depressed, especially those with ST > 4 hr/day. However, the studies cited used different assessments of behavioral problems, but did not link ST, sleep disturbance and EBPs.
In our study, we focused on studying the relationship between excessive ST and sleep disturbance and risk of EBPs among school children, and further explored whether sleep disturbance plays a mediating role between ST and EBPs. After adjusting for demographic characteristics and covariates, we still found that children with ST ≥ 2 hr/day had an increased risk of developing sleep disorders, which acted as a significant mediator of the impact of ST on children’s EBPs, explaining 25.39% of the total effect. A few studies also had similar results.33,34 Several possible mechanisms may explain how sleep disturbances play an intermediary role between screen and EBPs. For children, the time spent using electronic products was at the cost of sleep time, thus shortening sleep time and reducing sleep quality.35 Another possible mechanism is that bright light inhibits the melatonin, which interferes with sleep.36 Moreover, not all types of screen use exert the same impact on sleep. In particular, interactive screen-based activities such as video gaming have been shown to induce higher levels of physiological arousal and cognitive engagement compared to more passive media forms such as watching videos, which may strengthen their association with sleep disturbances.37 Sleep loss reduced prefrontal activity and reduced functional connectivity between the prefrontal cortex and limbic regions.38 Sleep loss also reduces rapid eye movement sleep, which is implicated in the processing of emotional memories.39 Finally, sleep deprivation has a negative impact on cognitive function, and many of these processes are involved in emotion monitoring, reasoning, and emotional regulation.40 Besides, the screen content such as playing games, watching videos, and chatting, may cause psychophysiological arousal.41 Of note, the mechanisms of sleep disturbance mediated on EBPs in children are complex, especially for young school-age children. More mechanism research underlying these associations would be required.
In rapidly developing, high-tech cities like Shenzhen, where electronic devices are pervasive, our findings highlight the importance of implementing public health and school-based interventions. Such interventions may include limiting ST both at school and at home, promoting sleep hygiene education, all of which aim to promote healthy screen use habits and sleep routines, and reduce subsequent EBPs in young school-aged children. The strengths of this study include the large representative sample and the statistical adjustment for a large number of potential covariates. In addition to gathering information on the child, parental accompaniment time, parental ST, we assessed TV/computer accessibility in the child’s bedroom and use of electronic products in the dark environment as potential confounders to better estimate the associations between ST and sleep disturbance and behavioral problems.
Our study has several limitations. Firstly, the data on ST were retrospective and reported by parents and might have been subject to recall bias. Also, parents are likely reporting the time their child goes to bed, not necessarily the time the child falls asleep. Secondly, although this study focused on the hypothesized pathway from ST to sleep disturbance and subsequently to EBPs, it is important to acknowledge that the observed associations do not establish causality. Existing literature indicates that the relationship between ST and EBPs may be bidirectional, children with EBPs may engage in more screen-based activities, while excessive ST may, in turn, exacerbate EBPs.42 However, the evidence regarding the directionality between sleep disturbance and EBPs remains inconsistent across studies, suggesting the possibility of reverse causality in our findings.14 Given these discrepancies and the cross-sectional nature of our data, we cannot determine temporal precedence or rule out the possibility that pre-existing EBPs influenced children’s screen use or sleep patterns. Therefore, prospective studies with repeated measurements are needed to further clarify these associations. Thirdly, social desirability bias may prompt parental underreporting of screen exposure and sleep problems.43 Finally, although some confounders were controlled in this study, the influence of other unmeasured confounders cannot be excluded. For example, we focused on overall screen time without differentiating content types (eg, educational, entertainment, or violent), which may have distinct effects on children’s sleep and emotional and behavioral outcomes. Further studies are needed to clarify these associations more precisely. Moreover, cultural factors and the specific technology environment of Shenzhen, including high levels of digital device penetration, intensive academic competition, and rapid lifestyle transitions, may limit the generalizability of our findings to other contexts. Further studies are needed to examine whether similar associations are observed in regions with different sociocultural backgrounds and patterns of technology use.
Conclusions
Our findings suggest that children with prolonged ST were significantly more likely to have behavioral problems, and sleep disturbance mediated this association. Importantly, persistent EBPs in childhood may lead to prolonged screen exposure and sleep disturbances, which in turn can heighten the risk of developing more severe mental health difficulties in adolescence, such as depression, anxiety, or social withdrawal. While causal conclusions cannot be drawn from a cross-sectional design, the identified associations highlight the necessity for further longitudinal or interventional studies. Accordingly, coordinated efforts among parents, educators, and healthcare providers to identify and address EBPs at an early stage, alongside the promotion of healthy screen-use habits and sleep routines, are essential to mitigate long-term psychosocial risks.
From a public health and clinical perspective, our findings support current recommendations to limit children’s daily ST to no more than 2 hours, avoid screen use in dark environments, and promote healthy sleep routines. Pediatricians and school health professionals should routinely assess both sleep quality and behavioral functioning in children with high screen exposure, as early detection may enable timely and targeted interventions.
For parents and educators, establishing structured screen-use guidelines and encouraging healthy sleep hygiene practices may be particularly beneficial. For younger children, who are more vulnerable to environmental influences, parents should act as role models by reducing their own screen use and fostering healthy screen-time habits. For older children, parental supervision and structured planning of screen use may help balance the benefits of digital engagement with the risks of overexposure.
Data Sharing Statement
The datasets used or analyzed during the current study are available from the corresponding author upon reasonable request.
Consent Statement and Ethics Approval
Informed consent was received from a parent or guardian of each participant, and this project was approved by the medical ethics committee of the Baoan Central Hospital of Shenzhen (no. IRB-PJ-2018-002). The procedures used in this study adhered to the tenets of the Declaration of Helsinki.
Acknowledgments
We are grateful to all the doctors and nurses in Baoan Central Hospital of Shenzhen. We also thank all the school doctors and teachers in Baoan District who participated in the survey.
Author Contributions
Yingbin You and Yuhui Chen share first authorship. Yingbin You: Investigation, Writing – Original Draft. Yuhui Chen: Conceptualization, Methodology, Writing – Original Draft, Writing – Review & Editing. Jianhui Shang: Data Curation, Writing – Review & Editing. Leyun Tan: Methodology, Data Curation. Writing – Original Draft. Mingtao Yu: Conceptualization, Formal analysis. Writing – Review & Editing. Yueyang Wu: Investigation. Writing – Review & Editing. Boya Li: Investigation. Writing – Original Draft. Pi Guo: Formal analysis. Writing – Review & Editing. Qingying Zhang: Supervision, Conceptualization, Methodology, Writing – Original Draft, Writing – Review & Editing. All authors agreed to submitting this article to Nature and Science of Sleep, agreed to the final version accepted for publication, and agree to be accountable for the contents of this paper.
Funding
This research was funded by the Metabolic Disease in Prevention and Treatment Program of Occupational Groups and Adolescents (2019–2020) and Baoan District Social Construction Special Fund Project (2017–2018), which was sponsored by the government of Baoan District of Shenzhen.
Disclosure
The authors have no conflicts of interest relevant to this article to disclose.
References
1. Pandey S, Agarwal M. Lifestyle factors associated with childhood obesity in South Asian expatriates of Dubai: a cross-sectional study. Cureus. 2024;16(12):e74924. doi:10.7759/cureus.74924
2. Wu F, Tham YC, Sabanayagam C, Saw SM. From evidence to action: public health approaches to reducing screen time and mitigating myopia risk. Asia-Pac J Ophthalmol Phila Pa. 2025;14(2):100177. doi:10.1016/j.apjo.2025.100177
3. Hartley S, Royant-Parola S, Zayoud A, Gremy I, Matulonga B. Do both timing and duration of screen use affect sleep patterns in adolescents? PLoS One. 2022;17(10):e0276226. doi:10.1371/journal.pone.0276226
4. Chen H, Sun Y, Luo S. Association of screen content with early development among preschoolers in shanghai: 7-day monitoring study with auto intelligent technology. J Med Internet Res Mar. 2025;5(27):e65343. doi:10.2196/65343
5. Hill D, Ameenuddin N, Reid Chassiakos Y, Council on Communications and Media. Media and young minds. Pediatrics. 2016;138(5):e20162591. doi:10.1542/peds.2016-2591
6. Guo M, Zhu Y, Wang X. Physical activity and recreational screen time among Chinese children and adolescents: a national cross-sectional study. Front Public Health. 2024;12:1376330. doi:10.3389/fpubh.2024.1376330
7. MacDonell N, Hancox RJ. Childhood and adolescent television viewing and metabolic syndrome in mid-adulthood. Pediatrics. 2023;152(2):e2022060768. doi:10.1542/peds.2022-060768
8. Lissak G. Adverse physiological and psychological effects of screen time on children and adolescents: literature review and case study. Environ Res. 2018;164:149–157. doi:10.1016/j.envres.2018.01.015
9. Brautsch LA, Lund L, Andersen MM, Jennum PJ, Folker AP, Andersen S. Digital media use and sleep in late adolescence and young adulthood: a systematic review. Sleep Med Rev. 2023;68:101742. doi:10.1016/j.smrv.2022.101742
10. Matthews EE. Sleep disturbances and fatigue in critically ill patients. AACN Adv Crit Care. 2011;22(3):204–224. doi:10.1097/NCI.0b013e31822052cb
11. Lund L, Sølvhøj IN, Danielsen D, Andersen S. Electronic media use and sleep in children and adolescents in western countries: a systematic review. BMC Public Health. 2021;21(1):1598. doi:10.1186/s12889-021-11640-9
12. Zhu R, Fang H, Chen M, et al. Screen time and sleep disorder in preschool children: identifying the safe threshold in a digital world. Public Health. 2020;186:204–210. doi:10.1016/j.puhe.2020.07.028
13. Wang G, Takahashi M, Wu R, et al. Association between sleep disturbances and emotional/behavioral problems in Chinese and Japanese preschoolers. Behav Sleep Med. 2020;18(3):420–431. doi:10.1080/15402002.2019.1605995
14. Cooper R, Di Biase MA, Bei B, Quach J, Cropley V. Associations of changes in sleep and emotional and behavioral problems from late childhood to early adolescence. JAMA Psychiatry. 2023;80(6):585–596. doi:10.1001/jamapsychiatry.2023.0379
15. Cooper R, van der Ven E, Jalbrzikowski M. Trajectories of psychotic-like experiences in youth and associations with lifestyle factors. J Child Psychol Psychiatr. 2025. doi:10.1111/jcpp.14179
16. Bolhuis K, Koopman-Verhoeff ME, Blanken LME, et al. Psychotic-like experiences in pre-adolescence: what precedes the antecedent symptoms of severe mental illness? Acta Psychiatr Scand. 2018;138(1):15–25. doi:10.1111/acps.12891
17. Baldini V, Gnazzo M, Maragno M, et al. Suicidal risk among adolescent psychiatric inpatients: the role of insomnia, depression, and social-personal factors. Eur Psychiatry J Assoc Eur Psychiatr. 2025;68(1):e42. doi:10.1192/j.eurpsy.2025.29
18. Baldini V, Gnazzo M, Santangelo G, et al. Are sleep disturbances a risk factor for suicidal behavior in the first episode of psychosis? Evidence from a systematic review. J Psychiatr Res. 2025;185:186–193. doi:10.1016/j.jpsychires.2025.03.053
19. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. doi:10.1037//0022-3514.51.6.1173
20. Murray CA, Hastings RP, Totsika V. Clinical utility of the parent-reported strengths and difficulties questionnaire as a screen for emotional and behavioural difficulties in children and adolescents with intellectual disability. Br J Psychiatry J Ment Sci. 2021;218(6):323–325. doi:10.1192/bjp.2020.224
21. Song Y, Li L, Xu Y, Pan G, Tao F, Ren L. Associations between screen time, negative life events, and emotional and behavioral problems among Chinese children and adolescents. J Affect Disord. 2020;264:506–512. doi:10.1016/j.jad.2019.11.082
22. Bruni O, Ottaviano S, Guidetti V, et al. The Sleep Disturbance Scale for Children (SDSC). construction and validation of an instrument to evaluate sleep disturbances in childhood and adolescence. J Sleep Res. 1996;5(4):251–261. doi:10.1111/j.1365-2869.1996.00251.x
23. Du Y, Kou J, Coghill D. The validity, reliability and normative scores of the parent, teacher and self report versions of the strengths and difficulties questionnaire in China. Child Adolesc Psychiatr Ment Health. 2008;2(1):8. doi:10.1186/1753-2000-2-8
24. Goodman A, Goodman R. Strengths and difficulties questionnaire as a dimensional measure of child mental health. J Am Acad Child Adolesc Psychiatry. 2009;48(4):400–403. doi:10.1097/CHI.0b013e3181985068
25. Casas L, Tiesler C, Thiering E, et al. Indoor factors and behavioural problems in children: the GINIplus and LISAplus birth cohort studies. Int J Hyg Environ Health. 2013;216(2):146–154. doi:10.1016/j.ijheh.2012.03.006
26. Lima Santos JP, Soehner AM, Ladouceur CD, Versace A. The impact of insufficient sleep on white matter development in late childhood and early adolescence. J Adolesc Health off Publ Soc Adolesc Med. 2025;76(2):220–227. doi:10.1016/j.jadohealth.2024.10.007
27. Takahashi I, Obara T, Ishikuro M, et al. Prospective associations of screen time at age 2 with specific behavioral subscales at age 3: a cohort study. J Public Health Oxf Engl. 2024;46(4):477–486. doi:10.1093/pubmed/fdae240
28. Poulain T, Ludwig J, Hiemisch A, Hilbert A, Kiess W. Media use of mothers, media use of children, and parent-child interaction are related to behavioral difficulties and strengths of children. Int J Environ Res Public Health. 2019;16(23):4651. doi:10.3390/ijerph16234651
29. Nagata JM, Al-Shoaibi AAA, Leong AW, et al. Screen time and mental health: a prospective analysis of the Adolescent Brain Cognitive Development (ABCD) Study. BMC Public Health. 2024;24(1):2686. doi:10.1186/s12889-024-20102-x
30. Mulla W, Ahmed W, Radhi M, et al. Exploring screen time and its effects on children’s mental health: a cross-sectional study. Cureus. 2024;16(10):e71215. doi:10.7759/cureus.71215
31. Haapala EA, Leppänen MH, Kosola S, et al. Childhood lifestyle behaviors and mental health symptoms in adolescence. JAMA Network Open. 2025;8(2):e2460012. doi:10.1001/jamanetworkopen.2024.60012
32. Yang F, Helgason AR, Sigfusdottir ID, Kristjansson AL. Electronic screen use and mental well-being of 10-12-year-old children. Eur J Public Health. 2013;23(3):492–498. doi:10.1093/eurpub/cks102
33. Guerrero MD, Barnes JD, Chaput JP, Tremblay MS. Screen time and problem behaviors in children: exploring the mediating role of sleep duration. Int J Behav Nutr Phys Act. 2019;16(1):105. doi:10.1186/s12966-019-0862-x
34. Li X, Buxton OM, Lee S, Chang AM, Berger LM, Hale L. Sleep mediates the association between adolescent screen time and depressive symptoms. Sleep Med. 2019;57:51–60. doi:10.1016/j.sleep.2019.01.029
35. Borfe L, Sehn AP, Reuter CP, et al. Associations between body mass index and sleep duration in Brazilian children and adolescents: the moderating role of screen time. J Pediatr Endocrinol Metab JPEM. 2025;38(4):326–332. doi:10.1515/jpem-2024-0302
36. Hartstein LE, Behn CD, Akacem LD, Stack N, Wright KP, LeBourgeois MK. High sensitivity of melatonin suppression response to evening light in preschool-aged children. J Pineal Res. 2022;72(2):e12780. doi:10.1111/jpi.12780
37. Brosnan B, Haszard JJ, Meredith-Jones KA, Wickham SR, Galland BC, Taylor RW. Screen use at bedtime and sleep duration and quality among youths. JAMA Pediatr. 2024;178(11):1147–1154. doi:10.1001/jamapediatrics.2024.2914
38. Kitano E, Ueno H, Takahashi Y, et al. Postnatal sleep restriction in male mice impairs the development of parvalbumin-positive neurons in the prefrontal cortex and increases anxiety-like behaviour. Neuroscience. 2025;573:127–142. doi:10.1016/j.neuroscience.2025.03.029
39. Ong JL, Lo JC, Gooley JJ, Chee MWL. EEG changes across multiple nights of sleep restriction and recovery in adolescents: the need for sleep study. Sleep. 2016;39(6):1233–1240. doi:10.5665/sleep.5840
40. Mukherjee U, Sehar U, Brownell M, Reddy PH. Mechanisms, consequences and role of interventions for sleep deprivation: focus on mild cognitive impairment and Alzheimer’s disease in elderly. Ageing Res Rev. 2024;100:102457. doi:10.1016/j.arr.2024.102457
41. King DL, Delfabbro PH, Zwaans T, Kaptsis D. Sleep interference effects of pathological electronic media use during adolescence. Int J Ment Health Addict. 2014;12(1):21–35. doi:10.1007/s11469-013-9461-2
42. Vasconcellos RP, Sanders T, Lonsdale C, et al. Electronic screen use and children’s socioemotional problems: a systematic review and meta-analysis of longitudinal studies. Psychol Bull. 2025;151(5):513–543. doi:10.1037/bul0000468
43. Scharkow M. The accuracy of self-reported internet use—a validation study using client log data. Commun Methods Meas. 2016;10(1):13–27. doi:10.1080/19312458.2015.1118446
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.