Back to Journals » ClinicoEconomics and Outcomes Research » Volume 17
Are Nutritional Interventions Worthwhile in Cancer Patients? A Systematic Review on Economic Evaluation
Authors Nguyen HTT ![]() , Riewpaiboon A
, Riewpaiboon A ![]() , Tran HTB, Youngkong S, Vo TQ
, Tran HTB, Youngkong S, Vo TQ ![]() , Turongkaravee S
, Turongkaravee S ![]()
Received 14 July 2025
Accepted for publication 31 October 2025
Published 2 December 2025 Volume 2025:17 Pages 865—882
DOI https://doi.org/10.2147/CEOR.S553676
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Hieu Thi Thanh Nguyen,1,* Arthorn Riewpaiboon,2 Hien Thi Bich Tran,3 Sitaporn Youngkong,2 Trung Quang Vo,3 Saowalak Turongkaravee2,*
1Social, Economic and Administrative Pharmacy (SEAP) Graduate Program, Faculty of Pharmacy, Mahidol University, Bangkok, 10400, Thailand; 2Social and Administrative Pharmacy Division, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok, 10400, Thailand; 3Department of Economic and Administrative Pharmacy, Faculty of Pharmacy, Pham Ngoc Thach University of Medicine, Ho Chi Minh, 700000, Vietnam
*These authors contributed equally to this work
Correspondence: Saowalak Turongkaravee, Social and Administrative Pharmacy Division, Department of Pharmacy, Faculty of Pharmacy, Mahidol University, 447 Sri-Ayuthaya Road, Phayathai, Ratchathewi, Bangkok, 10400, Thailand, Tel +6626448964 extension 5309, Email [email protected]
Purpose: Malnutrition in cancer patients may stem from both tumor progression and treatment regimens. Nutritional interventions have shown potential for enhancing treatment efficacy and overall quality of life, but their cost-effectiveness requires exploration. Accordingly, this study systematically investigated research on economic evaluations of nutritional interventions implemented as either preventive or therapeutic strategies in cancer patients.
Methods: PubMed and Scopus databases were searched from inception to September 9, 2025. Following study selection and data extraction, the reporting quality of included studies was evaluated using the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) checklist, while risk of bias was assessed using the ECOBIAS checklist.
Results: Eight studies, published between 1989 and 2022, primarily focused on gastrointestinal cancers and were conducted in high-income countries. Most of these investigations (6 out of 8) performed cost–utility analyses. Four indicated that combining oral supplements or parenteral nutrition with nutritional counseling was more cost-effective, although these studies differed in terms of time horizons, types of interventions evaluated, and types of comparators used. Most of the studies adhered to the CHEERS standards, but no reported on characterizing heterogeneity, and none discussed approaches to stakeholder involvement in study design. Based on the ECOBIAS framework, the three most frequently encountered risks of bias were limited sensitivity analysis bias, bias related to quality-of-life weights, and limited scope bias.
Conclusion: The findings offer physicians valuable guidance for optimizing treatments and potentially support policy decision-making.
Keywords: cancer, cost-effectiveness, economic evaluation, nutritional intervention, systematic review
Introduction
Cancer is a major public health issue that accounted for nearly 20 million new cases and 10 million deaths in 2022.1 The disease has malnutrition as a common symptom in patients, caused by both the presence of a tumor and medical and surgical anticancer therapies.2 This result finds support in a prospective observational study, which reported that 51% of all cancer patients experience dietary impairment and that 64% lose weight six months after diagnosis.3 Malnutrition negatively impacts quality of life (QoL) and treatment effectiveness, with an estimated 10% to 20% of cancer patients dying due to its consequences rather than from tumors themselves.2 It also contributes to financial burdens. In Spain, for example, total hospitalization expenses rise by up to €2,000 per episode because of extended hospital stays among malnourished cancer patients.4
Robust evidence has dictated that nutritional issues be taken into account from the time of cancer diagnosis, within a diagnostic and therapeutic pathway, and in parallel to the implementation of antineoplastic treatments.2 The European Society for Clinical Nutrition and Metabolism (ESPEN), an oncology expert group, has highlighted three key steps in enhancing the quality of nutritional care and the overall well-being of individuals navigating the challenges of cancer: (1) early nutritional risk screening for all cancer patients, irrespective of their body mass indices or weight histories; (2) nutrition‐related assessment (measures of anorexia, body composition, inflammatory biomarkers, resting energy expenditure, and physical function); and (3) multimodal nutritional intervention.5 Nutritional interventions are essential avenues that prevent and/or reverse malnutrition by maintaining neutral or positive energy and protein balance as well as ensuring adequate vitamin, mineral, trace element, and electrolyte levels.6 Those intended for cancer patients should cover both oral and medical nutrition, according to the ESPEN’s practical guidelines.2 Oral nutritional interventions include the provision of dietary advice or nutritional counseling, the treatment of symptoms and derangements that impair food intake (nutrition impact symptoms), and the administration of oral nutritional supplements (ONSs). Nutritional counseling aids symptom management and promotes the consumption of well-tolerated protein- and energy-rich meals and drinks. The additional use of ONSs containing the essential calories or nutrients that individuals need (carbohydrates, proteins, vitamins, and minerals) is advised when an enriched diet ineffectively satisfies nutritional goals. Medical nutritional intervention (also known as artificial nutritional intervention) is recommended for patients who are unable to eat adequately. It encompasses enteral nutrition (EN) if oral nutrition remains insufficient despite the implementation of nutritional interventions (counseling, ONS administration) and parenteral nutrition (PN) if EN-based regimens are insufficient or infeasible.
Appropriate nutrition has been shown to enhance the clinical outcomes of malnourished cancer patients. The nutritional intervention that accompanies curative treatment also increases tolerance for and response to oncology treatment, decreases the frequency of complications, shortens the length of stay in hospitals, and possibly reduces morbidity by optimizing the balance between energy expenditure and food intake.6 A recent meta-analysis suggested that nutritional intervention drives statistically significant improvements in weight (1.89 kg, 95% confidence interval 0.25–3.47) and energy intake (432 kcal/d, 95% confidence interval 172–693) compared with those achieved through routine care.7 Such an intervention also enhances various QoL aspects, such as emotional functioning, dyspnea, loss of appetite, and overall QoL.7 Despite these benefits, however, regimens based on nutrition have no effect on mortality.7
Nutritional interventions can considerably improve the health outcomes of cancer patients, but they are costly, and economic constraints substantially affect nutritional intervention choices. In the United States, for instance, adult cancer survivors spend $6.8 billion on nutritional supplements annually.8 In-hospital nutritional support for a period of six months can cost up to over $60,000 per patient.9 These realities highlight the need to explore the cost-effectiveness of such regimens. Economic evaluations may help decision-makers determine the value for money of nutritional interventions, but there is currently no evidence that guides policy decision-making or the optimization of treatment by physicians, particularly in resource-constrained settings.
In consideration of the abovementioned issues, the present study systematically investigated research on economic evaluations of nutritional interventions for cancer patients. To the best of our knowledge, this review is the first to focus on economic evaluations of preventive or therapeutic nutritional interventions to address malnutrition in cancer patients. Because healthcare providers, researchers, and policymakers are inundated with unmanageable amounts of nutritional information, systematic reviews such as the current research are essential to efficiently integrating existing insights and providing data on rational decision-making for cancer interventions. In addition, the findings can aid the design and improvement of future economic evaluation of nutritional interventions.
Materials and Methods
The protocol underlying this systematic review was registered on PROSPERO, an international prospective registry of systematic reviews (ID number CRD42022380168). The review was also conducted in accordance with the guidelines indicated in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).
Identification of Studies
A comprehensive and systematic search of the PubMed and Scopus databases was undertaken to identify relevant articles that were published from the inception of the databases to September 9, 2025. The search terms, developed based on the PICOS framework (ie, population, intervention, comparison, outcomes, and study type), comprised those related to the population domain (ie, cancer) and intervention (ie, nutritional intervention, nutritional counseling, enteral nutrition, parenteral nutrition, dietary supplements) of interest as well as study type (ie, cost-utility analysis [CUA] or cost-effectiveness analysis [CEA]). This systematic review included CEA and CUA as these are the predominant approaches for assessing intervention efficiency in healthcare economic evaluation. CEA employs disease-specific or clinical outcomes (eg, life-years gained, hospitalizations prevented), while CUA uses composite measures such as quality-adjusted life years (QALYs), enabling broader cross-intervention comparisons.10 Cost-benefit analysis (CBA) was excluded due to methodological and ethical limitations inherent in monetizing health outcomes, including valuation heterogeneity, equity concerns, and limited applicability in healthcare decision-making.11 To maintain methodological consistency and align with the extra-welfarist perspective prioritizing health maximization within budget constraints, we focused on CEA and CUA approaches that directly inform health policy decisions. No restrictions were imposed on the domains of comparison and outcomes. Search terms were combined within the same domain using “OR” and between domains using “AND.” The search was updated every three months, and the reference lists of the relevant studies were also examined.
Study Selection
The first reviewer (HTTN) screened all the articles identified during the database searches by looking at their titles/abstracts following the inclusion criteria, after which a second reviewer (HTBT) carried out a double screening of 10% of the titles and abstracts. Disagreements were resolved via discussion with a third reviewer (ST), and studies failing to meet the inclusion criteria were regarded as ineligible for analysis. The inclusion criteria were original articles on the cost-effectiveness or cost-utility (S) of nutritional interventions (I) for adult cancer patients (P). The nutritional interventions of interest were the oral and medical nutritional regimens defined by the ESPEN.2 The types of outcome (O) measures considered were the incremental cost-effectiveness ratio (ICER), incremental cost per QALY, incremental cost per disability-adjusted life year, net monetary benefit, and incremental net benefit. Non-English or inaccessible full-text publications were also excluded from the study.
Data Extraction
Data were derived independently by two reviewers (HTTN and HTBT) using a data extraction form. The extracted data were as follows:
- General information (ie, author, year of publication)
- Study characteristics (ie, country, country income level, study type, trial or model-based EE, sources of cost and effectiveness, perspective, time horizon, discounting, currency, currency year reference, uncertainty analysis)
- Patient characteristics (ie, target populations)
- Characteristics of interventions and comparators
- Study results (ie, strategy compared, willingness-to-pay threshold, ICER, and conclusion)
- Funding information (ie, pharmaceutical companies and other resources)
The conclusions drawn regarding cost-effectiveness results were categorized into four groups: “cost-effective”, “not cost-effective”, “cost-saving”, and “no conclusion.” If the cost year of a given study was unspecified, it was assumed to be the year of publication. In cases of missing data and/or additional details, we reached out to the corresponding authors of the articles. Country income levels were categorized according to the World Bank’s income classifications (2024): Low-income economies are countries with a gross national income (GNI) per capita of $1,135 or less; lower- middle-income economies are nations with a GNI per capita between $1,136 and $4,465; upper-middle-income economies are those with a GNI per capita between $4,466 and $13,845; and high-income economies are those with a GNI per capita of $13,846 or more.12 Reported funding sources were classified into predefined categories as industry (corporate or for-profit), government (public or governmental grants), non-profit (charitable, foundational, or internal academic funding), and not reported. The data were documented in a Microsoft Excel spreadsheet. Any disagreements regarding classifications in data extraction was resolved by the third reviewer (ST).
Quality Assessment of Economic Evaluation Reporting
The quality of reporting was assessed using the 2022 checklist of the Consolidated Health Economic Evaluation Reporting Standards (CHEERS 2022).13 This checklist consists of 28 items subdivided into seven categories: title, abstract, introduction, methods, results, discussion, and other relevant information. Quality standards were labeled as “fulfilled”, “unfulfilled”, “unreported”, or “not applicable.” The quality of reporting was assessed by two independent reviewers (HTTN and HTBT), and any disagreements were resolved through discussion with the third reviewer (ST). Inter-reviewer reliability was assessed using simple percentage agreement, calculated as the number of agreements divided by the total number of items assessed, multiplied by 100.
Risk of Bias Assessment
The risk of bias was assessed using the ECOBIAS checklist, a tool designed to evaluate bias in model-based economic studies.14 The checklist comprises 22 items divided into two sections: Part A, which assesses overall bias in economic evaluations, and Part B, which focuses on model-specific aspects of bias. Each item on the ECOBIAS checklist was assigned “yes”, indicating fully achieved; “no”, indicating unachievable; “partially yes”, indicating partially achieved; “unclear”, indicating insufficient information, and “not applicable”, if that item was not relevant. For non-model-based economic evaluations, only the first part of the checklist was applied. The risk of bias was assessed by two independent reviewers (HTTN and HTBT), and any disagreements were resolved through discussion with the third reviewer (ST). Inter-reviewer reliability was assessed using simple percentage agreement, calculated as the number of agreements divided by the total number of items assessed, multiplied by 100.
Results
Search Results
We identified 2,924 articles, of which 792 were found on PubMed, and 2,132 were discovered on Scopus. The removal of duplicates left us with 2,401 articles eligible for title or abstract screening, which further eliminated 2,321 articles based on the exclusion criteria. The ineligible studies were eliminated mostly because they were non-original works (eg, review, systematic review, meta-analysis, letter, commentary) and because none of the interventions of interest to the current review were explored. The remaining 80 articles were subjected to full-text screening and eligibility assessment, yielding a final sample of eight articles15–22 from which to extract data. Figure 1 shows the PRISMA-based study selection process.
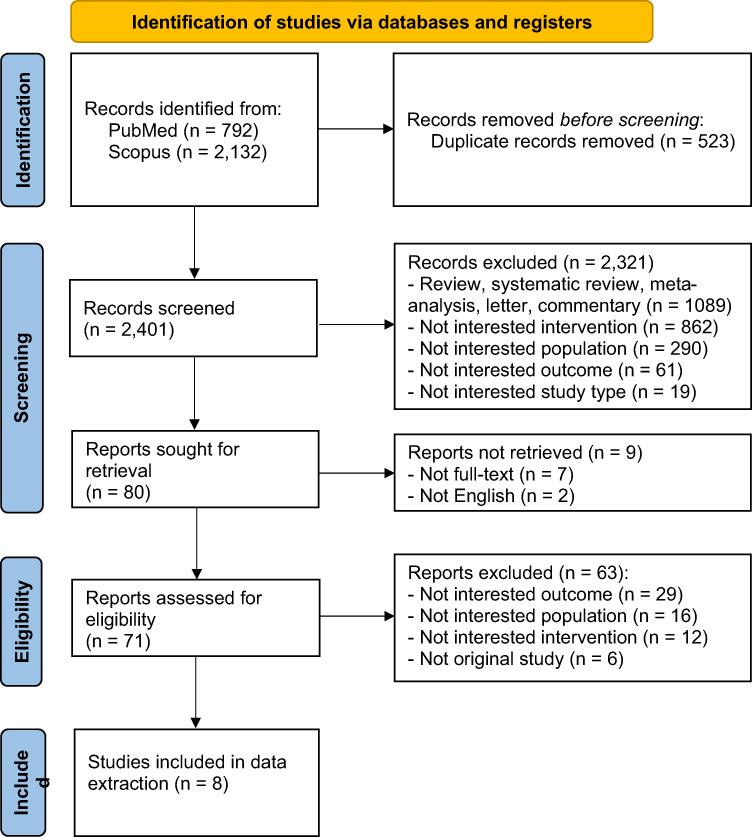 |
Figure 1 PRISMA flow of study selection process. |
General Characteristics of Eligible Studies
Table 1 provides an overview of the general characteristics of the studies examined in this work. These studies were conducted in the United States (n=3),16,18,21 United Kingdom (n=2),17,22 Italy,19 Canada,15 and China,19 which are mostly high-income regions, except for China (upper middle income). These studies were carried out within the period 1989 to 2022.
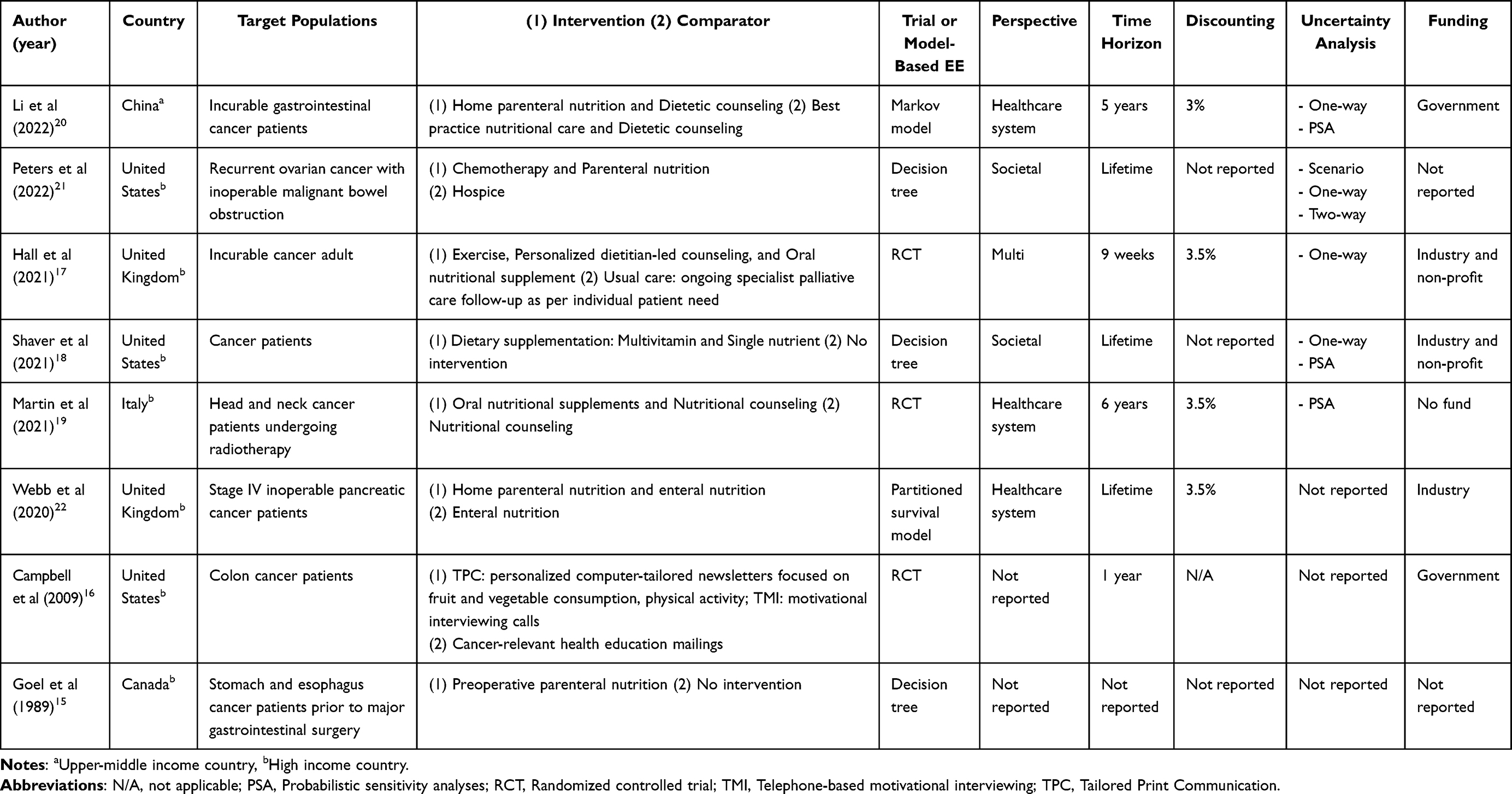 |
Table 1 General Characteristics of the Reviewed Studies |
The target population was composed mostly of gastrointestinal cancer patients (n=3).15,16,20 The various nutritional interventions evaluated included combined nutritional counseling and oral or PN (n=3),17,19,20 PN combined EN,22 PN,15,21 nutritional counseling,16 and the administration of ONSs.18 In terms of perspective, three studies were carried out based on a perspective toward the healthcare system,19,20,22 two were underlain by a societal perspective,18,21 one adopted multiple perspective,17 and two did not state a perspective.15,16 Six studies involved CUAs.15,17,18,20–22 Three studies obtained clinical effect sizes based on RCTs,16,17,19 while five derived such results from models, including decision trees, Markov models, or partitioned survival model.15,18,20–22 The time horizons used in seven studies ranged from nine weeks to a lifetime,16–22 and the discount rate used was 3% to 3.5% in four studies.17,19,20,22 With respect to uncertainty analysis, four studies performed one-way sensitivity analyses,17,18,20,21 three conducted probabilistic sensitivity analyses,17,18,20 and one carried out a scenario analysis.21 Four studies were funded by non-profit or government organizations,16–18,20 three received financial support from pharmaceutical companies,17,18,22 and that of Martin et al indicated no funding source.19 There was no information about funding in the studies conducted by Goel et al15 and Peters et al.21
Results of Economic Evaluations of Nutritional Interventions
The economic outcomes derived by the examined studies are summarized in Table 2. They found an overall incremental QALY range of 0.00018 to 0.48 and the smallest QALY gain in an adult with incurable cancer.17 In the oral nutrition group, one study assessed only nutritional counseling for colon cancer patients and associated an ICER of $106 to $128 with each 35-item block of the food frequency question score.16 Other studies in which ONSs were administered to cancer patients indicated the cost-effectiveness of the intervention.18
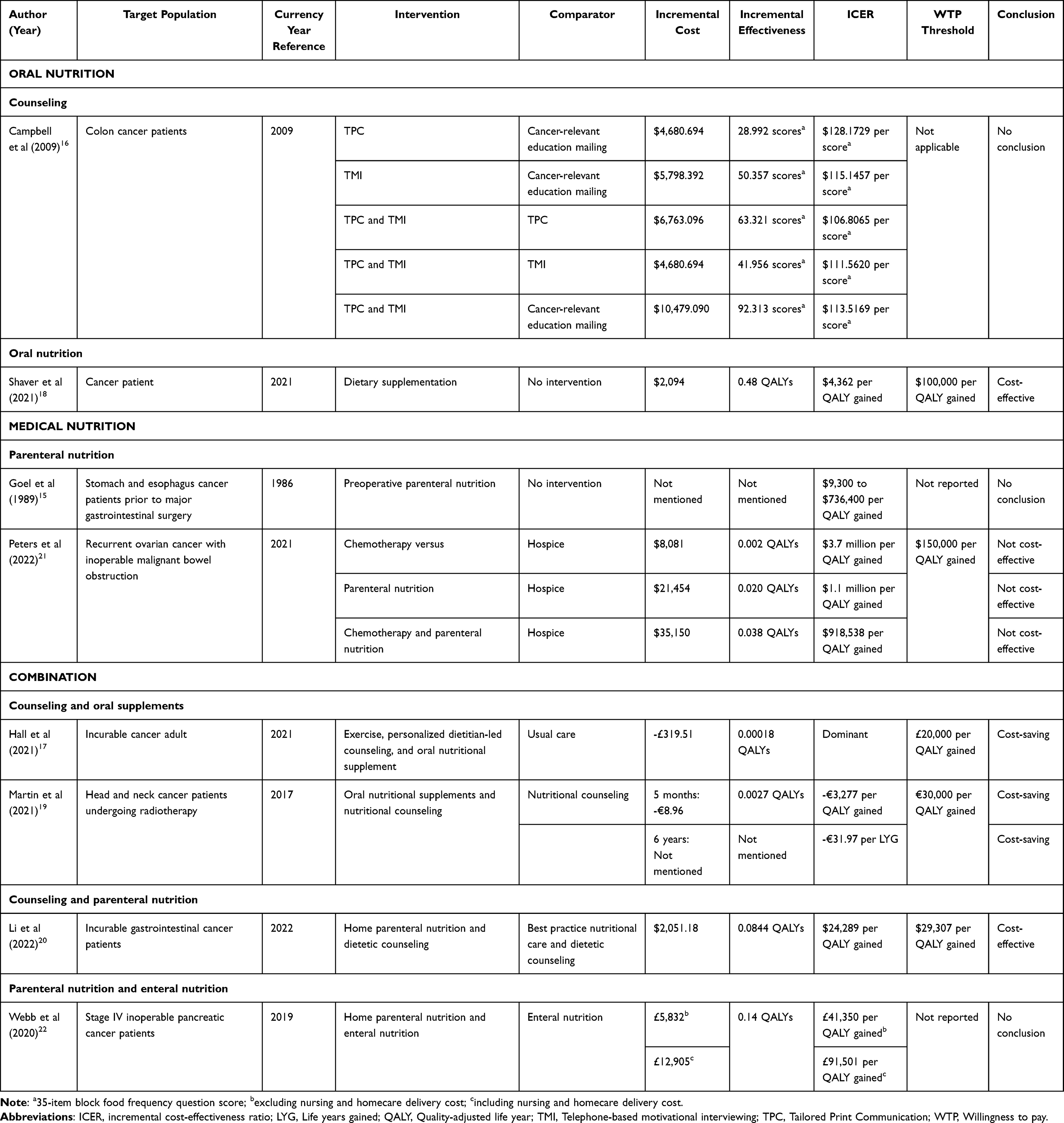 |
Table 2 Cost-Effectiveness Results of the Reviewed Studies |
In the medical nutrition group, one study was devoted to patients afflicted with stomach and esophageal cancer before major gastrointestinal surgery and found an ICER of $9,300 to $736,400 per QALY.15 Research on recurrent ovarian cancer with inoperable malignant bowel obstruction evaluated the intervention involved as not cost-effective.21 In the group combining nutritional counseling with oral supplements, the interventions for head and neck cancer patients undergoing radiotherapy were evaluated as cost-effective,19 as was the combination of nutritional counseling with PN for incurable gastrointestinal cancer patients.20 The regimens administered to adults with incurable cancer were assessed as cost-saving.17 A cost-effective analysis of combination PN and EN in patients with stage IV inoperable pancreatic cancer yielded ICER of £41,350 per QALY gained when excluding nursing and homecare delivery costs, and £91,501 per QALY gained when including these delivery costs.22
CHEERS-Based Quality Assessment of Economic Evaluation Reporting
All the studies reviewed presented clearly written abstracts, backgrounds and objectives, settings and locations, outcomes, main results, and discussions of uncertainty. Most of the studies identified the perspectives, discount rates, and time horizons that they used but without justifying their choices. Regarding the health economic analysis plan, three RCT-based studies reported that the analysis was conducted according to a pre-developed plan.16,17,19 Approaches to engagement with patients or stakeholders on research design and heterogeneity of population were not reported in all studies. While two studies addressed distributional effects,15,18 most studies failed to report on these critical aspects. Overall, the percentage of agreement between two independent reviewers in the present research ranged from 57% to 100%, suggesting that the quality assessment was reliable (Table 3).
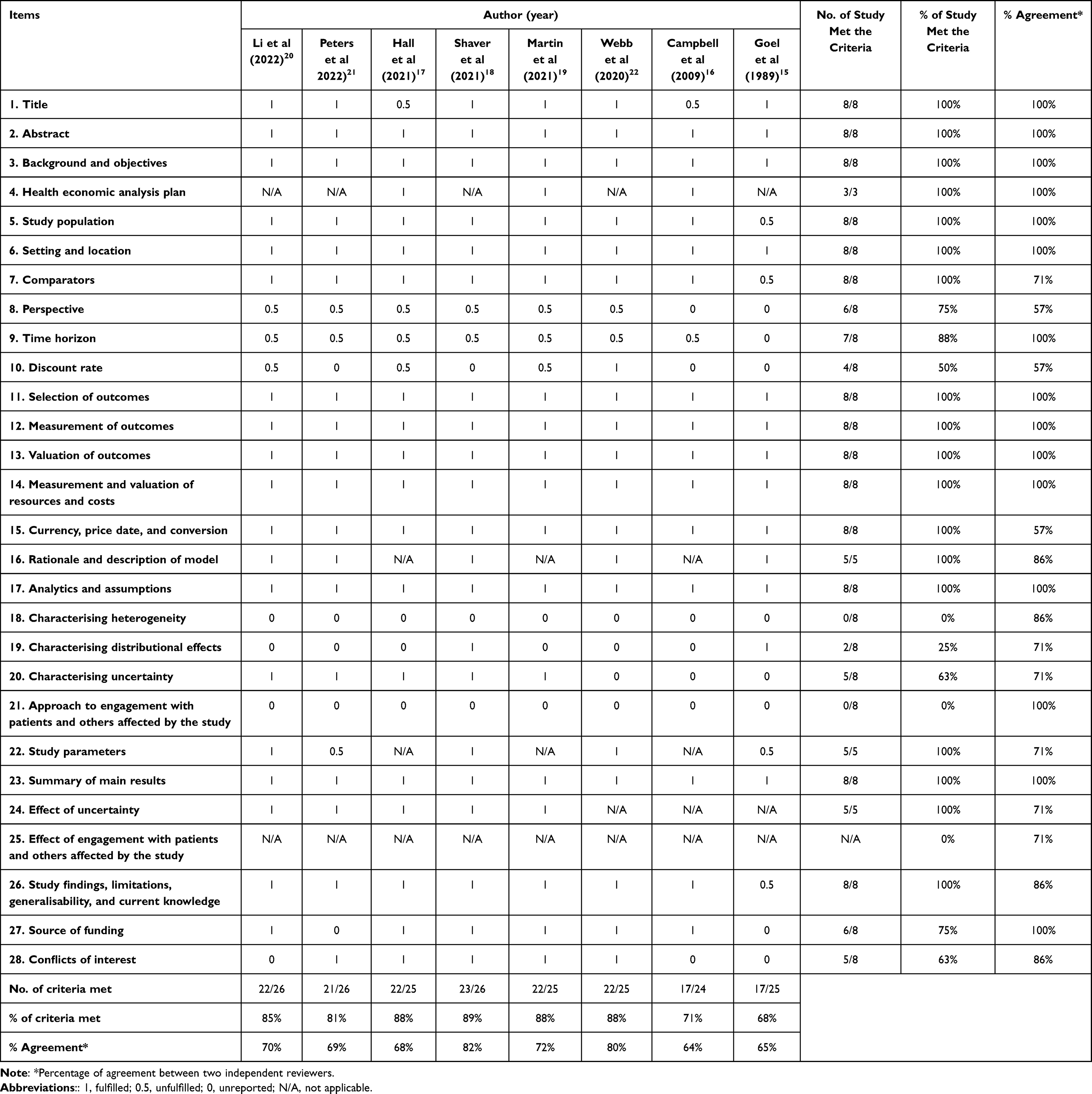 |
Table 3 Results of the Quality Assessment of Economic Evaluation Reporting (CHEERS Based) |
In addition, the percentages of criteria that each study met ranged from 68% to 89%, indicating an overall good quality of reporting. The highest-quality study is Shaver et al (2021),18 with 89% of criteria fulfilled. Studies such as Goel et al (1989)15 and Campbell et al (2009),16 while meeting a moderate to high percentage of criteria, have lower agreement rates. Agreement rates among reviewers vary, with the lowest being 64% (Campbell et al)16 and the highest 82% (Shaver et al).18 For each study, the number of criteria with a recorded outcome (fulfilled or not fulfilled) and the total number of applicable criteria (excluding those marked as not applicable) were recorded.
ECOBIAS-Based Risk of Bias Assessment
Following ECOBIAS, the three highest sources of risk of bias were “Limited sensitivity analysis bias” (0/8), “Bias related to quality-of-life weights (utilities)” (0/8), and “Limited scope bias” (0/8) (see Table 4). Items of “Cost measurement omission bias”, “Invalid valuation bias”, “Ordinal ICER bias”, “Reporting and dissemination bias”, “No treatment comparator bias”, “Bias related to data identification”, “Bias related to baseline data”, “Bias related to treatment effects”, and “Bias related to internal consistency” were met by all studies. Overall, the studies met 6 and 17 of the 22 ECOBIAS criteria. For each included study, both the number of assessed criteria (yes) and the total number of relevant criteria were recorded, with non-applicable items excluded. The study by Campbell et al (2009)16 demonstrated the highest risk of bias among the economic evaluations reviewed (55%), whereas Webb et al (2020)22 exhibited the lowest risk of bias (77%).
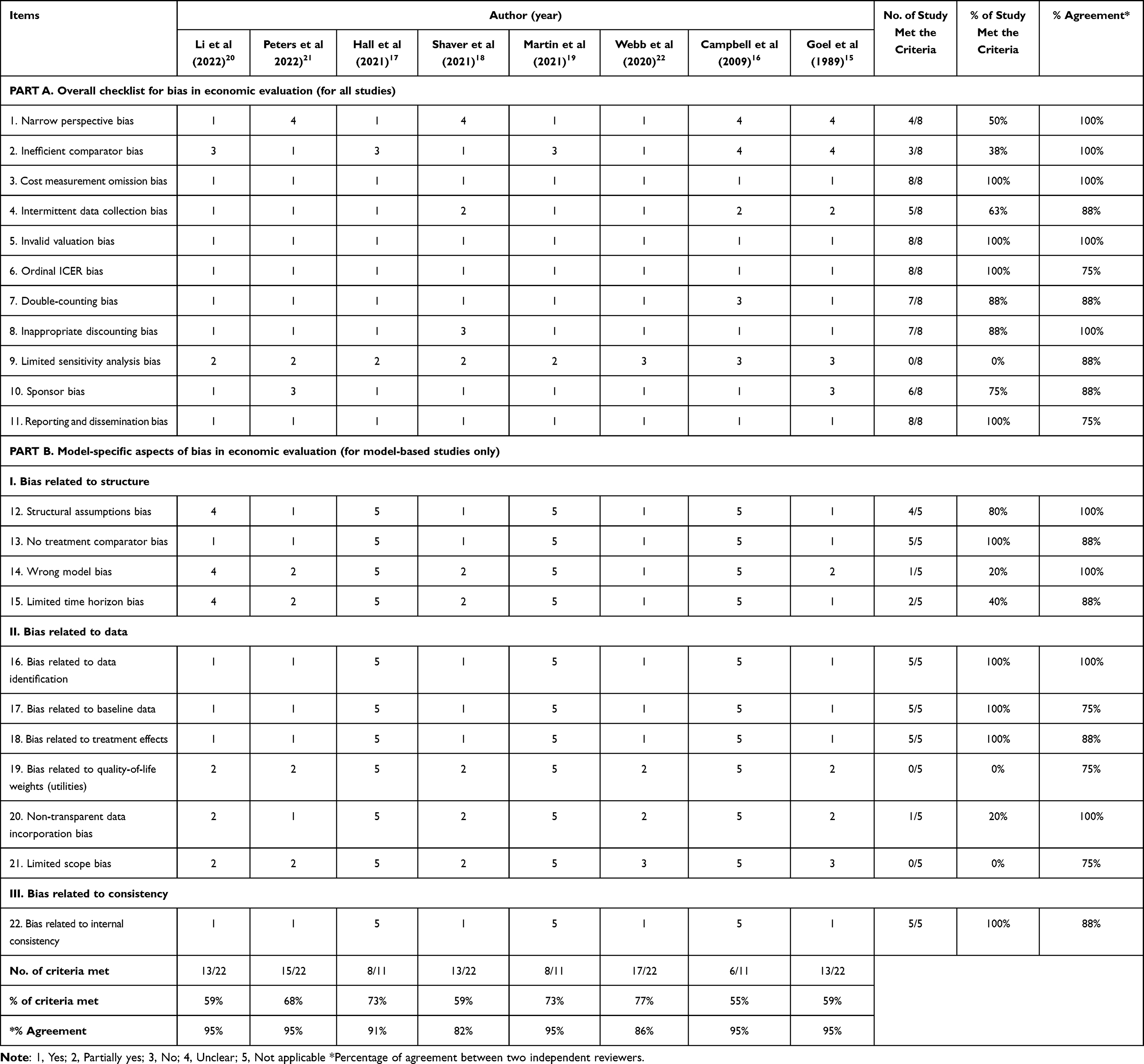 |
Table 4 Results of Risk of Bias Assessment (ECOBIAS Based) |
Discussion
To the best of our knowledge, this is the first systematic review focusing on economic evaluations of nutritional interventions for cancer patients. The analysis was directed toward eight such assessments, which involved a broad range of nutritional interventions, reference populations, methodologies (eg, perspective, trial, and model-based EE), and time horizons. Six studies applied CUAs, and one carried out both CEA and CUA.
Cancer management presents significant nutritional challenges that require systematic intervention throughout the disease trajectory. Contemporary clinical guidelines recognize nutritional care as an individualized, evidence-based component integral to comprehensive cancer treatment rather than a standardized approach. The ESPEN Clinical Nutrition Guidelines for Cancer Care establish a structured framework for nutritional intervention from diagnosis through survivorship phases, emphasizing proactive nutritional assessment and intervention strategies.2 Initial management focuses on individualized dietary counseling and symptom management to optimize oral intake. When conventional dietary measures prove insufficient, progressive nutritional support modalities are implemented, including ONSs, EN, or PN as clinically indicated. This systematic, multimodal approach aligns with economic evaluation findings demonstrating that slightly more than half of the studies analyzed found nutritional interventions cost-effective18,20 or cost-saving17,19 because they addressed nutrient deficiencies and potentially reduced hospital stays in malnourished patients, leading to improved patient outcomes and substantial cost savings for healthcare systems.23,24 All regimens involving the combination of counseling with ONSs/parenteral supplements were also assessed as cost-effective20 or cost-saving.17,19 These positive results can be attributed to the comprehensiveness offered by counseling, which is considered the primary approach in nutrition therapy. This dedicated and recurrent communication process extends over several months, aiming to equip patients with exhaustive knowledge about nutrition-related subjects, ultimately fostering long-term improvements in their dietary behaviors.25 In the studies reviewed, as well, complementing nutritional counseling, ONSs, and PN effectively addressed nutrient deficiencies, offering complete nutrient mixtures that supplement inadequate food intake.23,24,26 While there was a reduction in hospital stays observed among malnourished patients receiving ONSs,23,24 PN brought benefits to certain patient populations, especially those with functional impairment of the gastrointestinal tract.15,20,21 PN also improved QoL and reduced the need for separate treatments targeting nutrition-related symptoms, indicating the achievement of superior health outcomes under combined approaches.27 This evidence supports the clinical guideline recommendation for combined nutritional approaches to achieve superior health outcomes in cancer care. Beyond nutritional intervention combinations, the ESPEN guidelines advocate for a comprehensive approach incorporating foundational principles and supportive therapies.2 Key recommendations include systematic malnutrition screening from diagnosis, standardized energy (25–30 kcal/kg/day) and protein requirements (1.0–1.5 g/kg/day), and physical activity integration with moderate-intensity exercise and resistance training across all cancer stages. Pharmacological support encompasses selective appetite stimulants, n-3 fatty acid supplementation for advanced malnourished patients, and prokinetic agents for early satiety. The guidelines discourage restrictive diets and fasting during chemotherapy due to insufficient evidence and malnutrition risks. This evidence-based framework emphasizes individualized care tailored to treatment phases and patient needs, achieving superior health outcomes through integrated oncology care.
The reliability of the included studies strengthens confidence in these findings. The majority of studies included in this review adhered to the CHEERS 2022 guidelines and demonstrated high reporting quality, reflecting the researchers’ commitment to transparency and reproducibility. However, the reporting quality in the research methods section remains inadequate. The absence of patient or stakeholder involvement in the study design represents a significant limitation. Engaging the wider community and involving stakeholders in the research process could enhance the relevance, acceptability, and appropriateness of the studies.28 Community engagement, which directly involves local populations in decision-making, implementation, and policy development, has the potential to strengthen local capacities, community structures, and ownership. This approach promotes greater transparency, accountability, and optimal resource allocation across diverse settings. Unfortunately, none of the studies reported any involvement of patients or stakeholders in the design process. Overall, high-quality of reporting and agreement among reviewers provide robust evidence of nutritional interventions’ economic and clinical benefits. By combining reliable study quality with favorable cost-effectiveness outcomes, these results provide a strong basis for incorporating nutritional interventions into routine care for cancer patients. The studies analyzed derived reliable evidence that can inform decisions about funding and reimbursements of expenses related to nutritional interventions for cancer patients in specific contexts.
The ECOBIAS assessment of reviewed economic evaluations revealed significant methodological heterogeneity, with notable strengths coexisting alongside critical systematic deficiencies. The universal absence of adequate sensitivity analysis indicates insufficient exploration of model uncertainty across four fundamental dimensions: methodological, structural, heterogeneity, and parameter uncertainty. Most critically, all studies failed to evaluate population heterogeneity, representing a substantial limitation for evidence-based clinical decision-making. While economic models typically generate population-averaged results for hypothetical average patients, the consistent failure to assess cost-effectiveness variation across patient subpopulations constitutes a fundamental analytical flaw.29 The absence of subgroup analyses or individual-level simulation modeling provides single, population-averaged estimates that lack clinical applicability for personalized treatment decision-making. This limitation forces binary population-wide decisions based on averages potentially applicable to no individual patient, risking both resource misallocation and inequitable care access. The universal failure to address utility-related bias, compounded by absent reporting of quality-of-life weight derivation methods, represents a critical validity threat undermining result credibility. Utilities constitute the foundation of CUA, generating QALYs as primary outcome measures.30 Inappropriate utility sources, unrepresentative patient populations, or inconsistent application render QALY calculations—and consequently incremental cost-effectiveness ratios—questionable. Given the substantial impact of utility variations on economic outcomes, transparent reporting of utility sources and derivation methods represents essential methodological requirements rather than technical details. Conversely, universal compliance with cost measurement, valuation, and treatment effect criteria demonstrates strong foundational competency in core economic modeling domains, including accurate cost identification and robust clinical data utilization, providing baseline analytical credibility for the reviewed studies.
The majority of the studies were conducted in high-income countries, namely, the United States,16,18,21 Canada,15 United Kingdom,17 and Italy,19 whereas only one was undertaken a middle-income country20 (China). The collection of data from high-income countries may limit transferability and applicability to other nations due to differences in clinical practice, patterns of resource use, costs, survival, and/or utilities.31 The methods of economic evaluation used, which vary particularly on the basis of income levels in countries, range from cost data collection, outcome measurement, and modeling to the use of cost-effectiveness thresholds and uncertainty analyses.32 High-income countries often benefit from robust health information systems, sophisticated technologies such as electronic medical records, and extensive research infrastructure, enabling excellent data collection for economic evaluations. In contrast, low- and middle-income countries (LMICs) may encounter challenges that include incomplete data, a lack of standardized recordkeeping, and limited research funding, which can compromise the reliability of evaluations. These problems point to the need for more research involving economic evaluations in LMICs. By adopting context-appropriate methodologies and leveraging available resources, researchers can improve the quality of such assessments in LMICs, ultimately informing decision-making on healthcare and policy development for nutritional interventions for cancer patients.
The distribution of declared funding sources presents a nuanced picture. The plurality of studies being supported by non-profit or government organizations is a positive indicator, as this type of funding is typically associated with research priorities set by scientific and public health needs rather than commercial interests.33 Studies from this category are often perceived as having a lower risk of bias in their design and conclusions. However, it is noteworthy that two studies (Hall et al,2021; Shaver et al, 2021)17,18 reported mixed funding, receiving support from both pharmaceutical companies and non-profit sources. Two studies showed positive outcomes which were cost-saving and cost-effective. This dual sponsorship creates a complex interplay of interests. While the non-profit involvement may support methodological rigor, the pharmaceutical funding could potentially influence the study’s focus towards a proprietary intervention or a favorable comparative analysis.33
This study has several strengths, among which is the fact that it is the first systematic review of CUAs of nutritional interventions for cancer patients. A comprehensive search and up-to-date review of all types of nutritional interventions for cancer patients were conducted. This review summarized the results of the economic evaluations of interest, which can help clinicians, researchers, and policymakers acquire an extensive overview of available evidence, thereby facilitating informed decision-making.
As with all types of research, this systematic review is encumbered with certain limitations. First, the number of studies reviewed was limited. Since our literature search was restricted to economic evaluations published in English, we may have missed research conducted elsewhere. Second, the limited number of identified studies (n=8) primarily reflects the nascent field of economic evaluation in cancer nutrition, which remains an underdeveloped area of health economic research. The majority of identified economic evaluations were conducted in high-income countries, representing a substantial evidence gap from LMICs despite their disproportionate burden of cancer-related malnutrition. While our systematic search strategy utilized comprehensive databases and search terms to minimize the risk of omitting relevant publications, several limitations warrant consideration. Publication bias cannot be entirely discounted, as economic evaluations with neutral or unfavorable cost-effectiveness findings may remain unpublished or be confined to grey literature sources. Additionally, our restriction to English-language publications may have excluded relevant studies published in other languages, potentially limiting the global representativeness of our findings. This constrained evidence base highlights a critical knowledge gap and underscores the pressing need for additional methodologically rigorous economic evaluations with standardized reporting in cancer nutrition research, particularly in resource-limited settings. Third, due to the heterogeneity of the methodologies used in the examined studies, a meta-analysis could not be performed, preventing us from drawing synthetic and general conclusions about cost-effectiveness analyses. This also challenged the systematic comparison of the studies.
Future research should include a broader range of settings, with a particular focus on LMICs, to fill critical evidence gaps and support better-informed decision-making on nutritional interventions for cancer care globally. Future studies should prioritize robust economic evaluations of comprehensive nutritional interventions, incorporating standardized outcome measures and longer follow-up periods to capture sustained benefits. Research gaps requiring investigation include cost-effectiveness analyses of personalized nutrition protocols, economic impact of integrated physical activity programs, and comparative effectiveness of pharmacological nutritional support strategies across diverse cancer populations and treatment modalities. Such studies can also report on approaches to including stakeholders and patients in economic evaluations of interventions to clarify the contribution of community engagement to research. Based on ECOBIAS assessment, future economic evaluations must prioritize comprehensive sensitivity analyses, justify and transparently report utility values, and adopt a sufficiently broad perspective to minimize these critical biases and provide more reliable evidence for healthcare decision-making. To improve the quality and transparency of health economics evaluation research, future studies should strengthen compliance with guidelines like CHEERS 2022 and ECOBIAS checklist, thereby improving the overall quality, reliability and applicability of research outcomes.
Conclusions
This is the first systematic review of the cost-effectiveness of oral and medical nutritional interventions for cancer patients. Most of the studies analyzed revolved around cost-effective nutritional interventions for cancer patients. The evidence indicates that combined nutritional interventions are more likely to achieve cost-effectiveness or cost-savings compared to standard care or nutritional counseling alone. These findings provide critical evidence to inform healthcare policymakers in resource allocation decisions and guide clinicians in developing evidence-based treatment protocols, supporting the systematic integration of multimodal nutritional support into standard oncology care pathways. Future studies should prioritize diverse settings, especially in LMICs, evaluate outcomes in heterogeneous patient populations, and actively integrate stakeholder and patient engagement in economic evaluations to enhance the relevance, inclusivity, and global applicability of research on nutritional interventions in cancer care.
Ethics Approval and Informed Consent
Not applicable as this systematic review uses publicly available data from previously studies and does not involve human participants.
Acknowledgments
This work is a part of a study in Doctor of Philosophy program in Social, Economic and Administrative Pharmacy (SEAP), Faculty of Pharmacy, Mahidol University, Bangkok.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent for Publication
Not applicable. This study is a systematic review and does not involve individual data requiring consent for publication.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. International Agency for Research on Cancer. Global cancer observatory: cancer today. World Health Organization. Available from: https://gco.iarc.fr/today.
2. Muscaritoli M, Arends J, Bachmann P, et al. ESPEN practical guideline: clinical nutrition in cancer. Clin Nutr. 2021;40(5):2898–2913. doi:10.1016/j.clnu.2021.02.005
3. Muscaritoli M, Lucia S, Farcomeni A, et al. Prevalence of malnutrition in patients at first medical oncology visit: the PreMiO study. Oncotarget. 2017;8(45):79884–79896. doi:10.18632/oncotarget.20168
4. Planas M, Álvarez-Hernández J, León-Sanz M, Celaya-Pérez S, Araujo K, García de Lorenzo A. Prevalence of hospital malnutrition in cancer patients: a sub-analysis of the PREDyCES® study. Support Care Cancer. 2016;24(1):429–435. doi:10.1007/s00520-015-2813-7
5. Arends J, Baracos V, Bertz H, et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin Nutr. 2017;36(5):1187–1196. doi:10.1016/j.clnu.2017.06.017
6. Caro MMM, Laviano A, Pichard C. Nutritional intervention and quality of life in adult oncology patients. Clin Nutr. 2007;26(3):289–301. doi:10.1016/j.clnu.2007.01.005
7. Baldwin C, Spiro A, Ahern R, Emery PW. Oral nutritional interventions in malnourished patients with cancer: a systematic review and meta-analysis. J National Cancer Inst. 2012;104(5):371–385. doi:10.1093/jnci/djr556
8. John GM, Hershman DL, Falci L, Shi Z, Tsai W-Y, Greenlee H. Complementary and alternative medicine use among US cancer survivors. J Cancer Survivorship. 2016;10(5):850–864. doi:10.1007/s11764-016-0530-y
9. Schuetz P, Sulo S, Walzer S, et al. Cost savings associated with nutritional support in medical inpatients: an economic model based on data from a systematic review of randomised trials. BMJ open. 2021;11(7):e046402. doi:10.1136/bmjopen-2020-046402
10. Drummond MF, Sculpher MJ, Claxton K, Stoddart GL, Torrance GW. Methods for the Economic Evaluation of Health Care Programmes. Oxford university press; 2015.
11. Turner HC, Archer RA, Downey LE, et al. An introduction to the main types of economic evaluations used for informing priority setting and resource allocation in healthcare: key features, uses, and limitations. Front Public Health. 2021;9:722927. doi:10.3389/fpubh.2021.722927
12. The World Bank. World. bank country and lending groups https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
13. Husereau D, Drummond M, Augustovski F, et al. Consolidated health economic evaluation reporting standards (CHEERS) 2022 explanation and elaboration: a report of the ISPOR CHEERS II Good Practices Task Force. Value Health. 2022;25(1):10–31. doi:10.1016/j.jval.2021.10.008
14. Adarkwah CC, van Gils PF, Hiligsmann M, Evers SMAA, van Gils SM. Risk of bias in model-based economic evaluations: the ECOBIAS checklist. Expert Rev Pharmacoecon Outcomes Res. 2016;16(4):513–523. doi:10.1586/14737167.2015.1103185
15. Goel V, Detsky AS. A cost-utility analysis of preoperative total parenteral nutrition. Int J Technol Assess Health Car. 1989;5(2):183–194. doi:10.1017/S0266462300006413
16. Campbell MK, Carr C, DeVellis B, et al. A randomized trial of tailoring and motivational interviewing to promote fruit and vegetable consumption for cancer prevention and control. Ann Behav Med. 2009;38(2):71–85. doi:10.1007/s12160-009-9140-5
17. Hall CC, Skipworth RJ, Blackwood H, et al. A randomized, feasibility trial of an exercise and nutrition‐based rehabilitation programme (ENeRgy) in people with cancer. J Cachexia, Sarcopenia Muscle. 2021;12(6):2034–2044. doi:10.1002/jcsm.12806
18. Shaver AL, Tufuor TA, Nie J, et al. Cost-Effectiveness of nutrient supplementation in cancer survivors. Cancers. 2021;13(24):6276. doi:10.3390/cancers13246276
19. Martin B, Cereda E, Caccialanza R, Pedrazzoli P, Tarricone R, Ciani O. Cost-effectiveness analysis of oral nutritional supplements with nutritional counselling in head and neck cancer patients undergoing radiotherapy. Cost Eff Resour Alloc. 2021;19(1):1–9. doi:10.1186/s12962-021-00291-7
20. Li W, Guo H, Li L, Cui J. Cost-effectiveness analyses of home parenteral nutrition for incurable gastrointestinal cancer patients. Article Front Oncol. 2022;12858712. doi:10.3389/fonc.2022.858712
21. Peters PN, Moyett JM, Davidson BA, Cantrell S, Bliss SE, Havrilesky LJ. Cost-effectiveness of management strategies for patients with recurrent ovarian cancer and inoperable malignant bowel obstruction. Gynecologic Oncol. 2022;167(3):523–531. doi:10.1016/j.ygyno.2022.10.013
22. Webb N, Fricke J, Hancock E, et al. The clinical and cost-effectiveness of supplemental parenteral nutrition in oncology. ESMO Open. 2020;5(3):e000709. doi:10.1136/esmoopen-2020-000709
23. Neelemaat F, Bosmans JE, Thijs A, Seidell JC, van Bokhorst-de van der Schueren MAE. Oral nutritional support in malnourished elderly decreases functional limitations with no extra costs. Clin Nutr. 2012;31(2):183–190. doi:10.1016/j.clnu.2011.10.009
24. Wilson B, Fernandez-Madrid A, Hayes A, Hermann K, Smith J, Wassell A. Comparison of the effects of two early intervention strategies on the health outcomes of malnourished hemodialysis patients. J Ren Nutr. 2001;11(3):166–171. doi:10.1053/jren.2001.24364
25. Arends J, Bachmann P, Baracos V, et al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr. 2017;36(1):11–48. doi:10.1016/j.clnu.2016.07.015
26. Naghibi M, Smith T, Elia M. A systematic review with meta-analysis of survival, quality of life and cost-effectiveness of home parenteral nutrition in patients with inoperable malignant bowel obstruction. Clin Nutr. 2015;34(5):825–837. doi:10.1016/j.clnu.2014.09.010
27. Caro M, Laviano A, Pichard C, Candela CG. Relationship between nutritional intervention and quality of life in cancer patients. Nutricion hospitalaria. 2007;22(3):337–350.
28. van Voorn GA, Vemer P, Hamerlijnck D, et al. The missing stakeholder group: why patients should be involved in health economic modelling. Appl Health Econ Health Policy. 2016;14:129–133. doi:10.1007/s40258-015-0200-7
29. Espinoza MA, Manca A, Claxton K, Sculpher MJ. The value of heterogeneity for cost-effectiveness subgroup analysis: conceptual framework and application. Med Decis Mak. 2014;34(8):951–964. doi:10.1177/0272989X14538705
30. Sanders GD, Neumann PJ, Basu A, et al. Recommendations for conduct, methodological practices, and reporting of cost-effectiveness analyses: second panel on cost-effectiveness in health and medicine. JAMA. 2016;316(10):1093–1103. doi:10.1001/jama.2016.12195
31. Drummond M, Barbieri M, Cook J, et al. Transferability of economic evaluations across jurisdictions: ISPOR good research practices task force report. Value Health. 2009;12(4):409–418. doi:10.1111/j.1524-4733.2008.00489.x
32. Griffiths UK, Legood R, Pitt C. Comparison of economic evaluation methods across low‐income, middle‐income and high‐income countries: what are the differences and why? Health Economics. 2016;25:29–41. doi:10.1002/hec.3312
33. Lundh A, Lexchin J, Mintzes B, Schroll JB, Bero L. Industry sponsorship and research outcome. Cochrane Database Syst Rev. 2017;2. doi:10.1002/14651858.MR000033.pub3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.