Back to Journals » Clinical Ophthalmology » Volume 15
Are Dilated Fundus Examinations Needed for OCT-Guided Retreatment of Exudative Age-Related Macular Degeneration? A Prospective, Randomized, Pilot Study
Authors Solomon SD, Kyerematen V, Qutab M, Wenick AS, Wang J, Hawkins BS
Received 9 May 2021
Accepted for publication 23 July 2021
Published 12 August 2021 Volume 2021:15 Pages 3401—3417
DOI https://doi.org/10.2147/OPTH.S315554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sharon D Solomon,1 Victoria Kyerematen,2 Madiha Qutab,3 Adam S Wenick,1 Jiangxia Wang,4 Barbara S Hawkins1,4
1Department of Ophthalmology, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 2Bloomfield Court Hospital, National Health Services, London, UK; 3Department of Neurology, Johns Hopkins University School of Medicine, Baltimore, MD, USA; 4Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, USA
Correspondence: Sharon D Solomon Email [email protected]
Purpose: To report findings when dilated fundus examination (DFE) is omitted from follow-up of patients receiving anti-VEGF injections for neovascular age-related macular degeneration (NVAMD).
Design: Randomized pilot study.
Participants: NVAMD patients with two or more injections of anti-VEGF within prior six months who were expected to require treatment for at least eight more months.
Methods and Interventions: Participants were assigned to either retinal imaging and DFE or retinal imaging without a DFE except at 16 weeks and 32 weeks and at study completion.
Outcomes: Primary safety outcomes were change in usual-corrected visual acuity (UCVA) and central subfield thickness (CST). Primary efficacy outcomes included time spent in clinic and patient satisfaction with clinic visits.
Results: The 66 participants had mean baseline UCVA of 20/50 in the study eye. Median change in UCVA from baseline to each clinic visit in each arm was “no change”. Mean change in CST was less than 15 microns from baseline to any follow-up clinic visit. Time spent in the clinic at follow-up visits averaged 20 minutes less for participants in the Imaging Only group than those in the Full Exam group. More participants in the Imaging Only group were satisfied with the time spent in clinic and with the clinic visits overall than participants in the Full Exam group: means of 71 vs 91 minutes, respectively, per clinic visit.
Conclusion: Based on findings from this randomized pilot study, follow-up retina clinic visits for established patients who have NVAMD and are under treatment with intravitreous injection of anti-VEGF agents could be streamlined by implementing longer intervals between DFE and by relying on imaging alone to make most decisions regarding the need for retreatment, thereby reducing the time spent by patients in clinic and increasing their satisfaction with care received, without excess adverse events.
Trial Registration: NCT02251366.
Keywords: neovascular age-related macular degeneration, anti-VEGF injection, time in clinic
Plain Language Summary
Patients who had neovascular age-related macular degeneration and were assigned randomly to follow-up with OCT imaging but less frequent dilated fundus examination spent on average 20 minutes less in clinic than patients who had dilated fundus examination performed at each follow-up. Usual-corrected visual acuity, central subfield thickness, changes in these measurements, and levels of physician and patient satisfaction with clinic visits were similar in the two groups.
Introduction
Intravitreous delivery of anti-vascular endothelial growth factor (VEGF) has revolutionized the management of neovascular age-related macular degeneration (NVAMD).1–4 However, the requirement for frequent monitoring of response to treatment and repeat injections coupled with the growing number of patients needing treatment pose a challenge to efficient delivery of care by retina specialists, under normal circumstances. Prior to the COVID-19 pandemic, the time patients spent in clinic for evaluation and treatment might span more than 2 hours. Based on a survey of 57 retina specialists selected randomly and data from clinic diaries for 221 patients, Prenner et al5 calculated the mean length of clinic visits for NVAMD patients to be 90 minutes, with an upper limit of more than 4 hours. As many patients also require assistance with transportation because of visual impairment, age, or co-morbidities, the adult family members or friends of these patients often miss hours from work each month to transport or accompany patients to clinic visits. In an attempt to maximize treatment efficiency, many retina specialists have adopted a treat-and-extend regimen where patients are brought into the office to be assessed a certain number of weeks to months following their last treatment when it is suspected repeat treatment may be necessary. While this may decrease the number of required visits for any individual patient over one year, it does not decrease the wait time any one patient has during a particular visit.
Now, during the era of COVID-19, when social-distancing in waiting rooms and an appropriate trend toward greater utilization of telemedicine are recommended, it has become even more important to have a streamlined alternative to current clinical practice for evaluation of patients with NVAMD to determine whether intravitreal therapy with an anti-VEGF agent is indicated at a particular clinic visit. In a recent publication in Ophthalmology Retina, Dr. Patel and colleagues asked, “Are dilated fundus examinations needed for OCT-guided retreatment of exudative age-related macular degeneration?”6 The authors performed a post hoc analysis of ranibizumab-treated patients in the HARBOR study to determine whether dilated fundus examination (DFE) was required in addition to spectral-domain (SD) OCT imaging at each visit to guide retreatment decisions. While the authors’ observations did suggest that DFE may not be needed for retreatment decisions during follow-up of NVAMD patients, they admitted that the data were limited by its retrospective nature and by its inability to comment on safety, as the frequency of adverse events such as posterior inflammation, retinal tear, or retinal detachment could not be analyzed. They concluded that evidence from prospective, randomized clinical trials is needed to address these issues and to determine the appropriate frequency of the DFE in patients receiving anti-VEGF injections for NVAMD.6
In a multi-site, prospective, randomized, pilot study, we compared standard-of-care assessment, defined as retinal imaging with at least OCT and DFE by a retina specialist, versus immediate evaluation of OCT images by the retina specialist with less frequent DFE in the management of NVAMD. A pro re nata (PRN) regimen of treatment with monthly evaluation was used for the sake of standardization across sites and to facilitate data analysis in this pilot study; however, in a real-world scenario, any follow-up regimen, including treat-and-extend, could be utilized, as the goal was to compare clinical outcomes and patient and physician satisfaction to ascertain whether either was affected by our attempt to decrease the amount of time patients spent in retina clinics during any one visit.
Methods
The randomized pilot study was conducted at five satellite retina clinics of the Wilmer Eye Institute, Johns Hopkins School of Medicine. Residents and fellows did not participate in patient care at these satellite clinics. The Johns Hopkins University School of Medicine Institutional Review Board reviewed and approved the study protocol. The study adhered to the tenets of the Declaration of Helsinki and was conducted in compliance with the regulations set forth by the Health Insurance Portability and Accountability Act.
Patient Screening and Enrollment
The study coordinator traveled to each participating site on the day of the week when the participating retina specialist at that site scheduled NVAMD patients for follow-up examinations. During the period of participant accrual, prior to her weekly visit to attend each retina clinic, the study coordinator screened the electronic medical records of all patients scheduled for a return visit to identify those who appeared to meet inclusion criteria for the pilot study. Patients with an established diagnosis of NVAMD in one or both eyes who had been given 2 or more intravitreous anti-VEGF injections by a pilot study investigator during the previous 6 months and who were anticipated to need continued PRN therapy during the next 8 months or longer were designated for screening for eligibility by the participating ophthalmologist. Patients who had systemic diseases that could affect the retina, such as diabetes mellitus or sickle cell disease, were not eligible. Patients with a recent history of symptomatic posterior vitreous detachment or a history of retinal tear, retinal detachment, or retinal surgery also were not eligible. The study eye was required to have usual-corrected visual acuity (UCVA) of 20/200 or better. Patients who gave written consent were assigned randomly to either the DFE plus Diagnostic Images arm, hereafter referred to as the “Full Exam” arm, or to the Diagnostic Images Only arm, hereafter referred to as the “Imaging Only ” arm. The patient’s care during the clinic visit at which consent was obtained occurred per usual clinic routine; that enrollment visit was deemed to be the newly enrolled participant’s baseline visit for the pilot study. The study coordinator obtained the random assignment from prepared randomization schedules stored electronically after she had documented signed consent and entered the required identifying information, including an assigned study identifier, into the electronic study database. The randomization schedule for each participating site was generated using randomly permuted blocks of randomly selected sizes. The study participant was informed of the assignment. The next clinic visit, which would be the first follow-up visit for the pilot study, was scheduled in the interval prescribed by the ophthalmologist and on the day of the week the study coordinator was scheduled to be in the satellite retina clinic.
Participant Follow-Up
Follow-up visits typically occurred at 4-week to 8-week intervals, as recommended by the treating retina specialist. Visits were assigned to 4-week windows for data reporting purposes based on the actual visit completion date. Each participant was scheduled for the final pilot study visit 32 weeks after enrollment.
At each follow-up clinic visit, each pilot study participant was screened by the ophthalmic technician, including measurement of UCVA and intraocular pressure (IOP), and had imaging as ordered by the retina specialist. UCVA was recorded as the line of smallest letters read without error on the logMAR chart while the participant was wearing usual distance correction and with pinhole whenever that device resulted in reading a line of smaller letters correctly. After images were available for review, each participant in the Full Exam arm had a retinal examination by the retina specialist and intravitreous anti-VEGF injection whenever recommended.
Once retinal images were available for participants in the Imaging Only arm, the study coordinator displayed them on a computer monitor in one of the examination rooms for review by the ophthalmologist with the participant present. The study coordinator provided the ophthalmologist with the participant’s current UCVA and IOP measurements and interim ocular and relevant medical history. During review of the digital images, the retina specialist had access to pertinent clinical information in the electronic medical record. Immediately after interpreting the digital images to make a treatment decision for the participant at this visit, the retina specialist instructed the study coordinator either to have the participant prepared for intravitreous injection of an anti-VEGF agent, chosen at the physician’s discretion, or to schedule the participant’s next follow-up visit because treatment was not required at this time.
At each follow-up clinic visit, the study coordinator recorded the time at which the ophthalmic technician escorted the participant for screening and the time she escorted the participant to the check-out desk for discharge and scheduling of the next clinic visit. These two times were used to calculate the length of the clinic visit. Other study-related procedures required of study personnel or participants in both study arms were completion of a 4-item online questionnaire about each participant’s clinical status by the study ophthalmologist after making the treatment decision and telephone administration of a questionnaire regarding satisfaction with the clinic visit7 by the study coordinator to each participant within 48 hours after completion of each follow-up clinic visit. Although the Visit-Specific Satisfaction Instrument (VSQ-9) contained 11 items, our primary interest was the participant’s rating of 3 items: length of time waiting, time spent with the physician/healthcare provider, and the visit overall. Respondents rated each item as poor, fair, good, very good, or excellent.
Regardless of the random assignment of each pilot study participant, a mandatory full retinal examination was performed 16 weeks and 32 weeks after enrollment to ensure participant safety and to address any non-urgent concerns of study participants or ophthalmologists. Participants in the Imaging Only arm who missed the Week 16 clinic visit were scheduled for a DFE at the Week 20 visit. Participants who missed the Week 32 visit were scheduled for an additional study visit at which a DFE was performed. Treatment recommendations for all participants at these mandatory visits were made by the ophthalmologist based on the DFE and interpretation of images. In addition, any participant assigned to the Imaging Only arm or the study ophthalmologist of such a patient could elect a DFE at any other follow-up clinic visit. Participants who requested a DFE or reported symptoms between scheduled follow-up visits were examined promptly.
After each scheduled clinic visit by a study participant, the study coordinator recorded the examination findings in the study database along with information from the electronic medical record. That information included interim clinic visits and examinations by ophthalmic care providers and other medical personnel and procedures and hospitalizations or other potential indicators of adverse events.
Statistical Issues and Methods
A data and safety monitoring committee, with two non-study retina specialists and a clinical trials methodologist as voting members, provided oversight of the study. Their twice-yearly reviews of reports of accumulated data focused on performance of participating sites and, using unmasked data, participant safety.
Because of the pilot nature of this investigation, we did not calculate a formal sample size. We examined change in UCVA and CST measurements from baseline to scheduled follow-up times as the primary safety outcomes. The primary efficacy outcomes compared between Full Exam and Imaging Only arms were the length of follow-up clinic visits and satisfaction of study participants and ophthalmologists with the clinic visits. Analyses focused on estimation of mean differences between groups for UCVA, CST, and length of clinic visits and on risk ratios for proportions of participants in each arm who experienced adverse events and proportions of physicians and participants who reported satisfaction; 95% confidence intervals were calculated for all estimates.
We compared the baseline characteristics between groups of participants in the study arms using Student’s t-test, the χ2 test, or Fisher’s exact test, as appropriate. We used similar tests to compare follow-up UCVA, CST, and changes in these measurements from baseline. Because the distribution of the length of follow-up clinic visits was skewed, we used the nonparametric Kruskal–Wallis equality-of-populations rank test to compare lengths of clinic visits between the two study arms. The proportion of participants who reported satisfaction with each aspect of the clinic visit as “excellent” or “very good” was calculated and compared between study arms at each clinic visit. We anticipated that the proportions who reported “very good” or “excellent” in the two study arms at 16 weeks and 32 weeks would be similar.
Statistical analyses were performed using Stata, version 14.2, software (StataCorp LP, College Station, Texas). We deemed probabilities (p-values) from statistical comparisons less than or equal to 0.05 to be of interest but not to indicate statistical significance because of the multiple times the data were reviewed during the course of the pilot study.
Results
The first participant enrolled in October 2014. When accrual ended in December 2015, 66 participants had enrolled, 32 assigned to the Full Exam arm and 34 assigned to the Imaging Only arm. The last study follow-up clinic visit was completed in July 2016.
Characteristics of Pilot Study Participants
Baseline characteristics of pilot study participants and their eyes are summarized in Tables 1 and 2, respectively. Sociodemographic characteristics of the two groups were similar at baseline; no comparison yielded a p-value smaller than 0.10. The mean age of participants was 81 years; 59% of the participants were women. As expected in a study of NVAMD in the United States, the participants were predominantly (92%) non-Hispanic White.
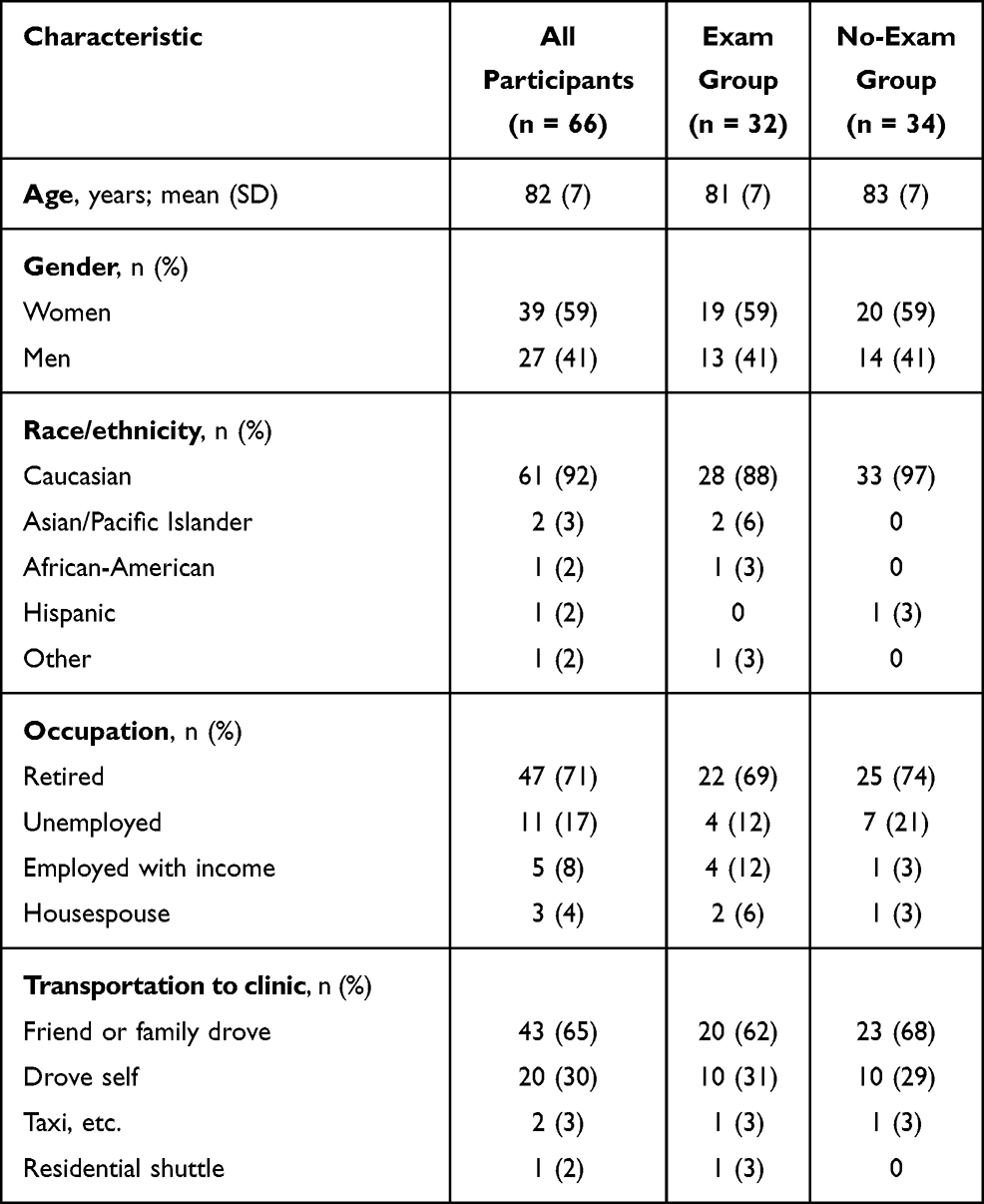 |
Table 1 Number (%) of Study Participants with Specified Baseline Sociodemographic Characteristics |
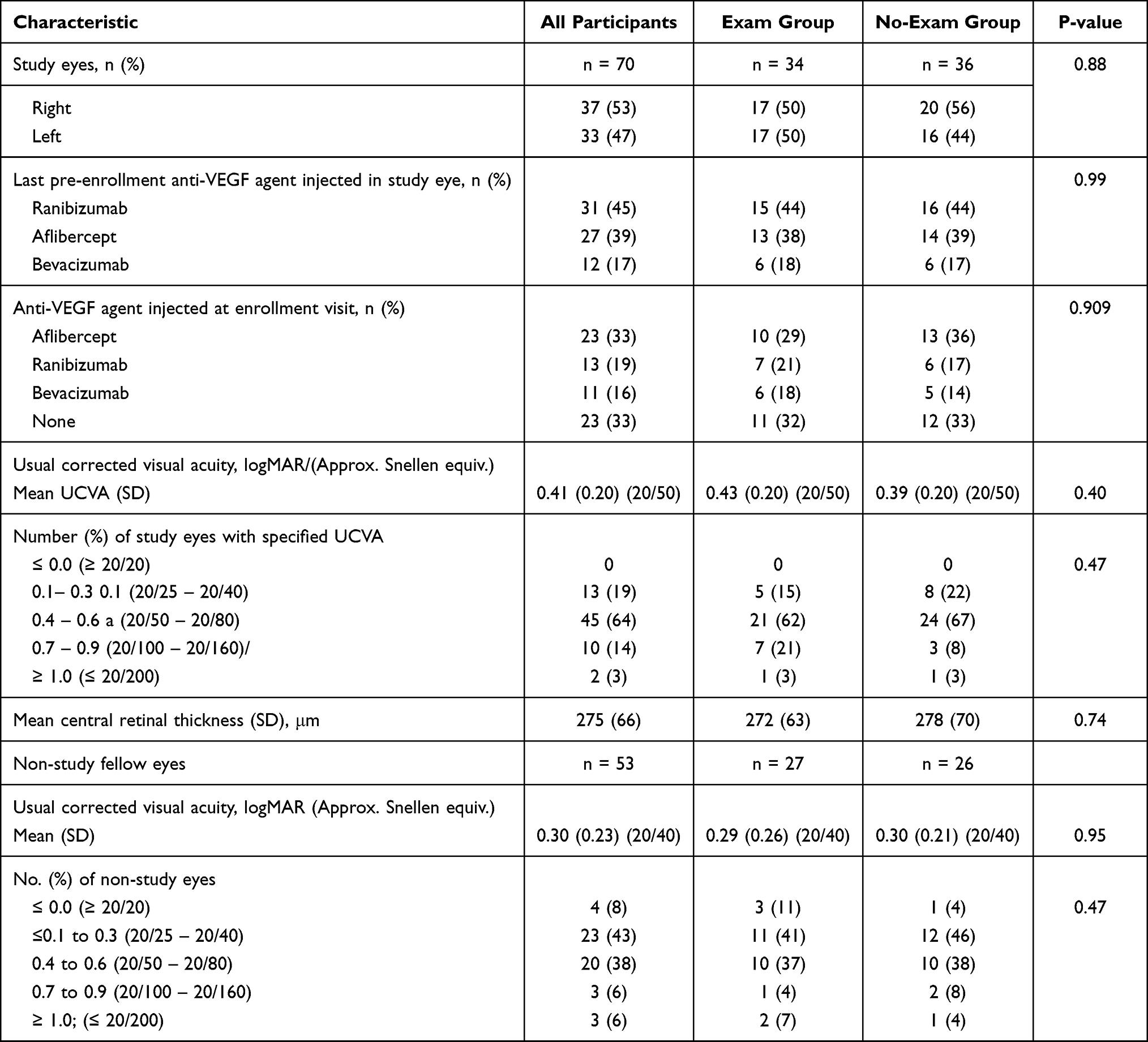 |
Table 2 Specified Baseline Characteristics of Eyes of Pilot Study Participants |
Of the 66 participants, both eyes of four participants met the eligibility criteria for the pilot study and were followed as study eyes; thus, the Full Exam arm contained 34 study eyes and the Imaging Only arm contained 36 study eyes. The most recently administered anti-VEGF agent in the study eye prior to enrollment was ranibizumab (Lucentis, Genentech, Inc.) in 31 of 70 study eyes (45%), aflibercept (Eylea, Regeneron, Inc.) in 27 study eyes (39%), and bevacizumab (Avastin, Genentech, Inc.) in the remaining 12 study eyes (17%). At the enrollment visit, 33% of study eyes did not have an intravitreous injection of an anti-VEGF agent. Of the eyes that were treated at that visit, 33% received aflibercept and 19% and 16%, respectively, received injections with ranibizumab or bevacizumab.
The mean (SD) logMAR UCVA at baseline was 0.43 (0.20) in the Full Exam arm and 0.39 (0.20) in the Imaging Only arm, ie, approximately 20/50 in each group (Table 2). One eye in each group had UCVA at baseline of 1.0 logMAR or worse (≤ 20/200). CST, as measured on OCT, was similar between the two groups of study eyes; the mean values (SD) were 272 µm (63 µm) in the Full Exam group and 278 µm (70 µm) in the Imaging Only arm. The mean logMAR UCVA of non-study fellow eyes is also shown in Table 2 for all participants by random assignment. The study eye was the better eye of 16 (26.2%) of the 61 participants who had only one study eye and had UCVA measured in the non-study eye at the baseline visit.
Compliance with Follow-Up Schedules
Table 3 provides the numbers of participants who completed clinic visits during 4-week intervals. Of 256 clinic visits that potentially could have been completed by participants in the Full Exam arm, 21 were not required based on the judgement of the retina specialist. Thus, 198 of 235 (84%) clinic visits expected were completed by Full Exam arm participants. Participants in the Imaging Only arm potentially could have returned at 4-week intervals for 272 follow-up clinic visits; 23 clinic visits were judged by the study ophthalmologist to be unnecessary. Thus, participants in the Imaging Only arm completed 203 of 249 (82%) scheduled clinic visits. The proportion of participants in the two groups who missed scheduled study visits was similar: 16% and 18% in the Full Exam and Imaging Only arms, respectively.
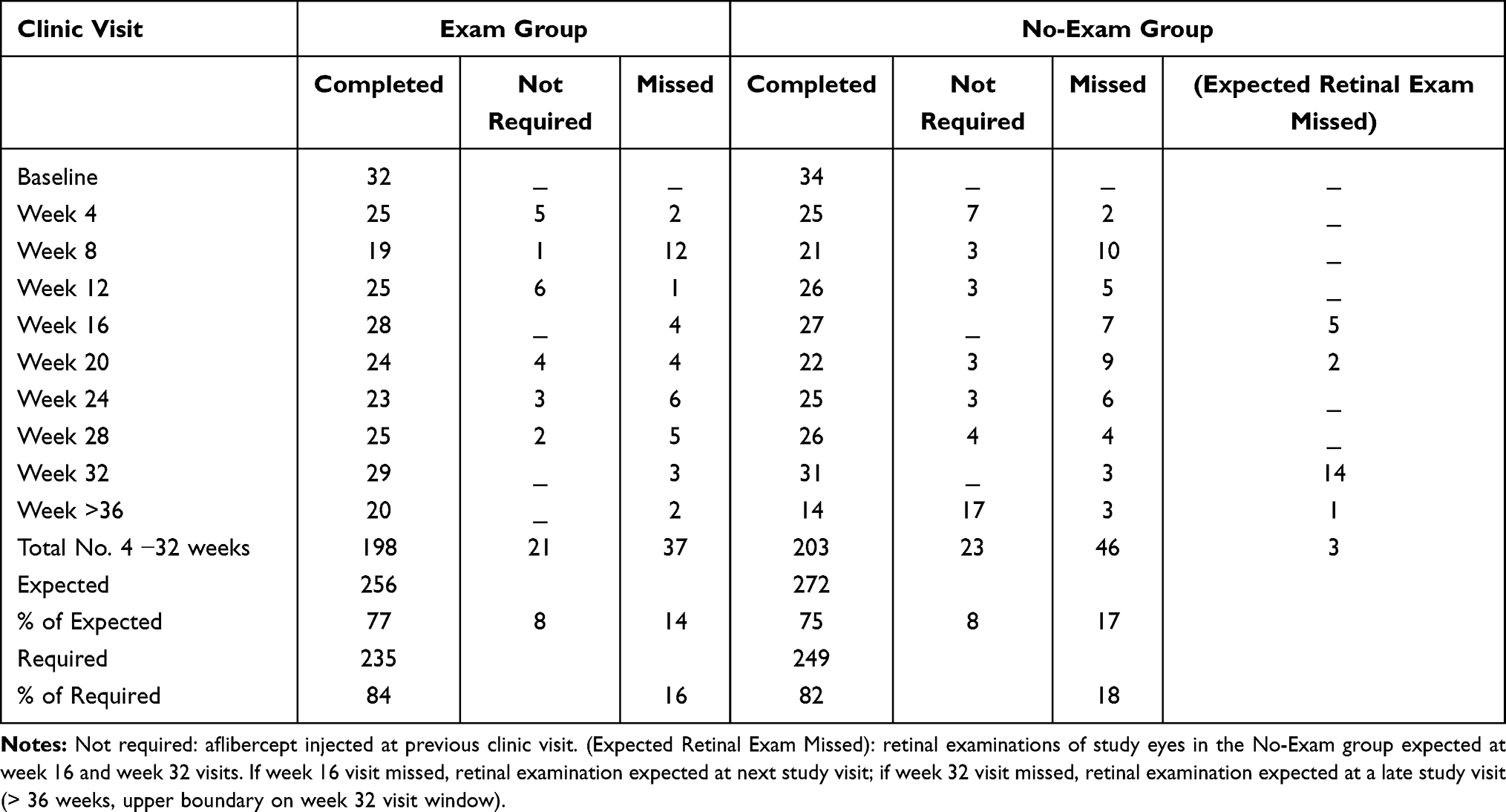 |
Table 3 Number of Participants by Randomly Assigned Study Arm and Completion of Study Visits |
Twenty-eight participants in the Full Exam arm and 27 participants in the Imaging Only arm completed the 16-week clinic visit. Three participants in each group missed the 32-week clinic visit, the final scheduled follow-up visit under the pilot study protocol. All participants in the Full Exam arm who missed the 16-week visit had a DFE at the next clinic visit, but 2 participants who missed the 32-week visit were not examined later as part of the pilot study. In addition to the 7 participants in the Imaging Only arm who missed the 16-week visit, 5 who completed the visit did not have the required DFE; 2 of these 12 participants did not have a DFE at the next clinic visit. Of the 17 participants in the Imaging Only arm who did not have a retinal examination at 32 weeks, 16 had DFE by the ophthalmologist at a delayed final study visit. In addition to these DFEs, out of 192 clinic visits when a DFE was not required, the retina specialist performed 26 total additional DFEs of the study eye on 18 participants in the Imaging Only arm.
Clinical Outcomes
UCVA and CST were measured at each clinic visit. Distributions of UCVA as measured at each visit are given in Table 4; changes in UCVA from baseline are summarized in Table 5. Mean UCVA of study eyes remained at or near 0.4 logMAR (20/50) at each follow-up visit in both groups of participants (Table 4). Mean and median change in UCVA from baseline was less than 0.06 logMAR (< 3 letters in both groups at each clinic visit; SD=0.22 or less). However, one participant in the Full Exam group lost ≥0.5 logMAR (5 or more lines; 25 or more letters) from baseline UCVA to counting fingers at the 16-week and remaining study visits. Mean difference in change in UCVA between study groups (Full Exam vs Imaging Only) from baseline to the 32-week clinic visit was 0.05 (95% CI: −0.03 to 0.14), ie, 2.5 letters; the mean changes in the Full Exam and Imaging Only arms were +0.02 and −0.03 respectively (Table 5). At no follow-up visit was the mean difference between groups for UCVA change > 0.05, ie, 3 letters or more.
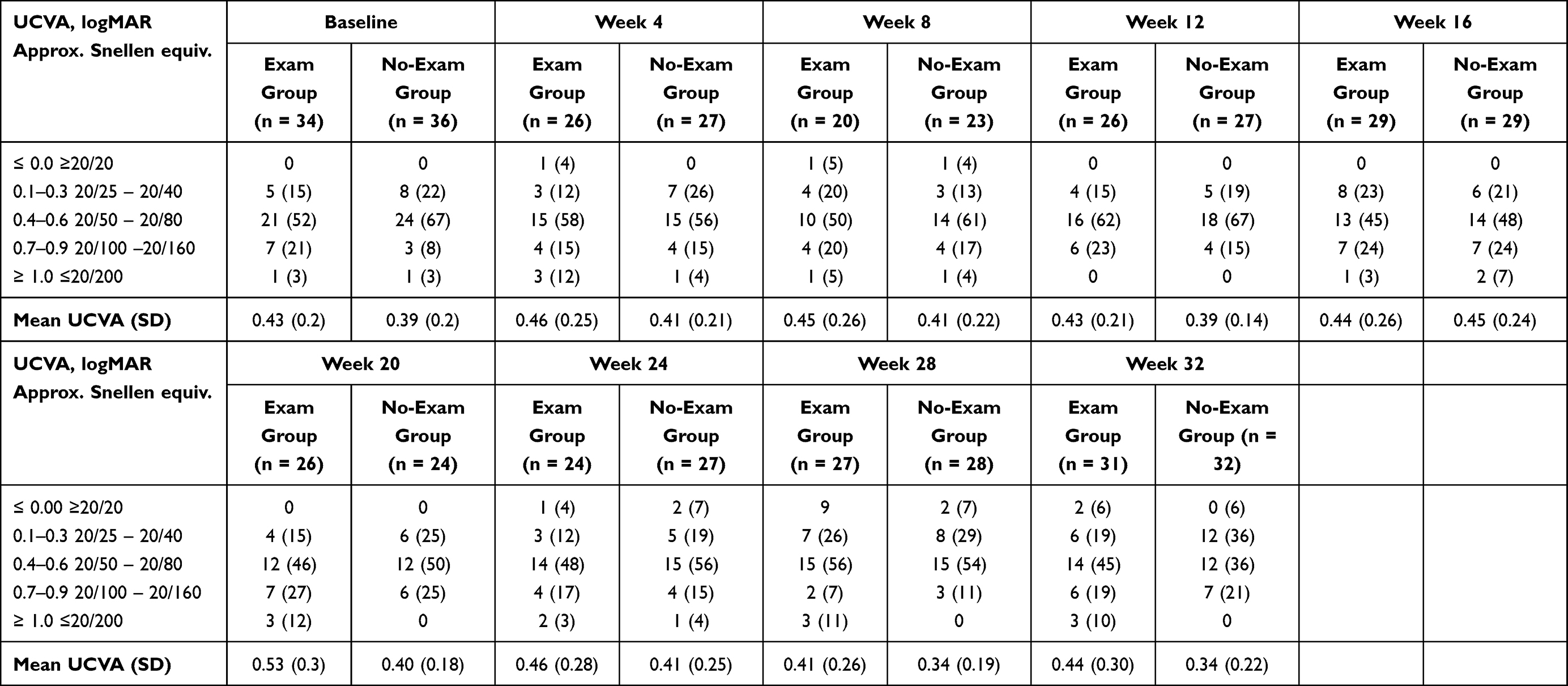 |
Table 4 Number (Percent) of Study Eyes with Specified Usual-Corrected Visual Acuity (UCVA) at Baseline and Each Scheduled Follow-Up Clinic Visit |
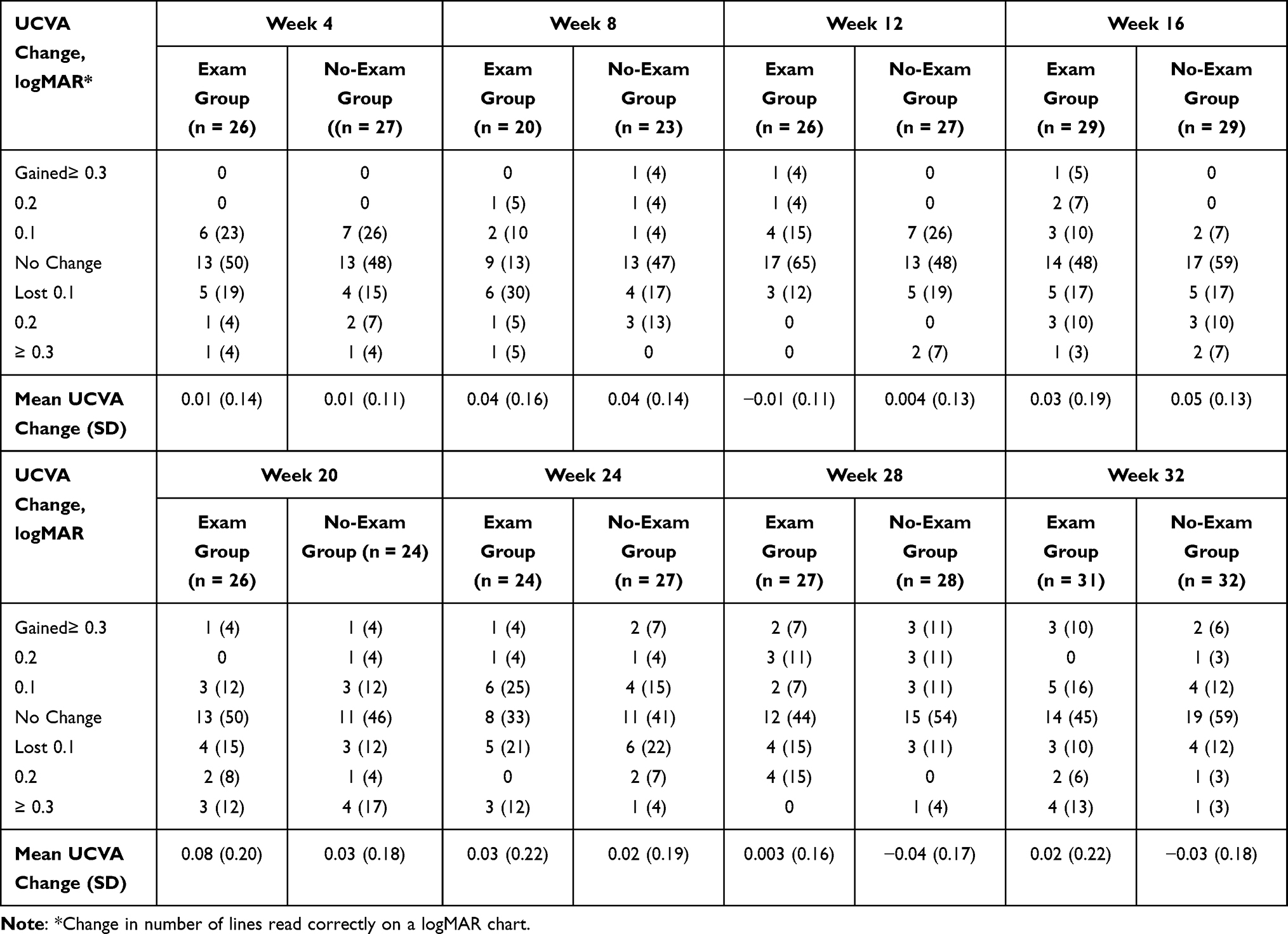 |
Table 5 Number (Percent) of Study Eyes with Specified Change in Usual-Corrected Visual Acuity (UCVA) from Baseline to Each Scheduled Follow-Up Clinic Visit |
Study ophthalmologists administered intravitreous anti-VEGF injections to one half to two thirds of study eyes at each follow-up clinic visit. The mean number of eyes treated per visit was 19.6 (58%) in the Full Exam arm and 21.0 (58%) in the Imaging Only arm. The mean numbers of repeat injections were 5.6 in Full Exam arm study eyes and 5.4 in Imaging Only arm study eyes out of 9 possible monthly injections.
Both mean and median CST measurements remained close to baseline levels. Mean and median changes in CST measurements from baseline were smaller than 15 μm at each follow-up visit. Few participants in either group had changes of more than 50 μm from baseline at any visit (Table 6). However, one participant in the Imaging Only arm had an increase of more than 200 μm from baseline CST based on OCT imaging at the 20-week visit.
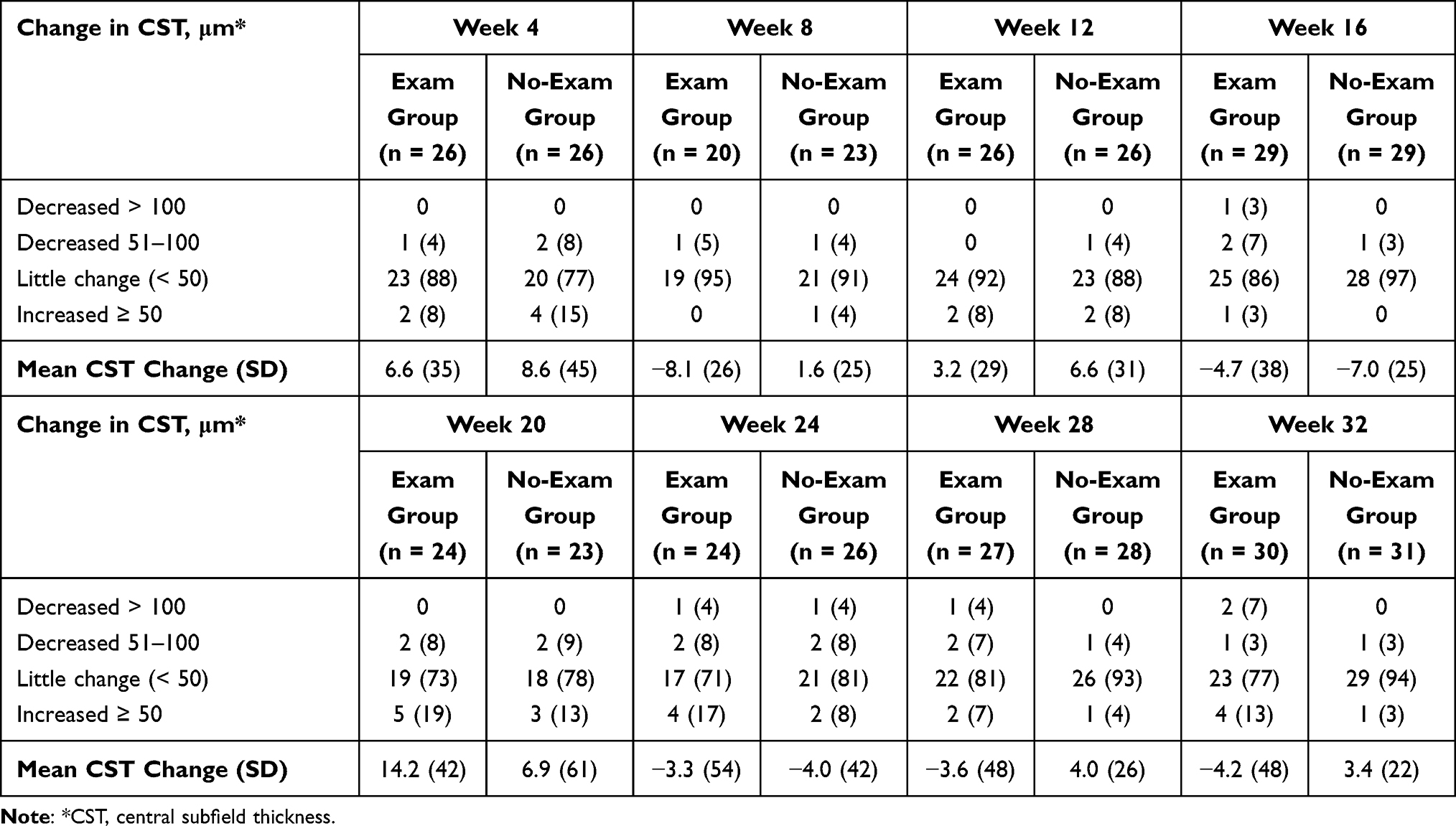 |
Table 6 Number (Percent) of Study Eyes with Specified Change in Central Subfield Thickness from Baseline to Each Follow-Up Clinic Visit |
Nine participants (10 eyes), six in the Full Exam arm and 3 in the Imaging Only arm, initiated interim clinic visits. Six of these visits, three in each group, were deemed “emergency visits”. Six study eyes, three in each group, received an intravitreous injection of an anti-VEGF agent at an interim clinic visit.
Effect of Streamlining Follow-Up Clinic Visits
Based on beginning and end times of follow-up clinic visits for pilot study participants recorded by the study coordinator, there was an overall mean difference of 20 minutes in the length of clinic visits between Full Exam and Imaging Only participants, with shorter clinic visits for participants in the Imaging Only arm, at all follow-up times, including the 16-week and 32-week visits when all participants were expected to have DFEs (Figure 1). To ensure that the difference in visit length at the 16- and 32-week visits was not due to missed DFEs of Imaging Only participants who made clinic visits, we compared length of clinic visits both for all participants examined in each group and for Imaging Only participants examined at the 16-week and 32-week visits. There was no substantive difference between the two time advantages for the Imaging Only participants. For example, when all 29 Imaging Only participants who had a 16-week clinic visit were compared to the 29 Full Exam participants, the mean difference in visit length was 19 minutes. When only the 24 Imaging Only participants who had the expected DFE were considered, the mean difference in length of the clinic visits was 20 minutes (Table 7). Variability in length of clinic visits was considerably greater at most visits in the Full Exam arm than in the Imaging Only arm, as indicated by the standard deviations given in Table 7.
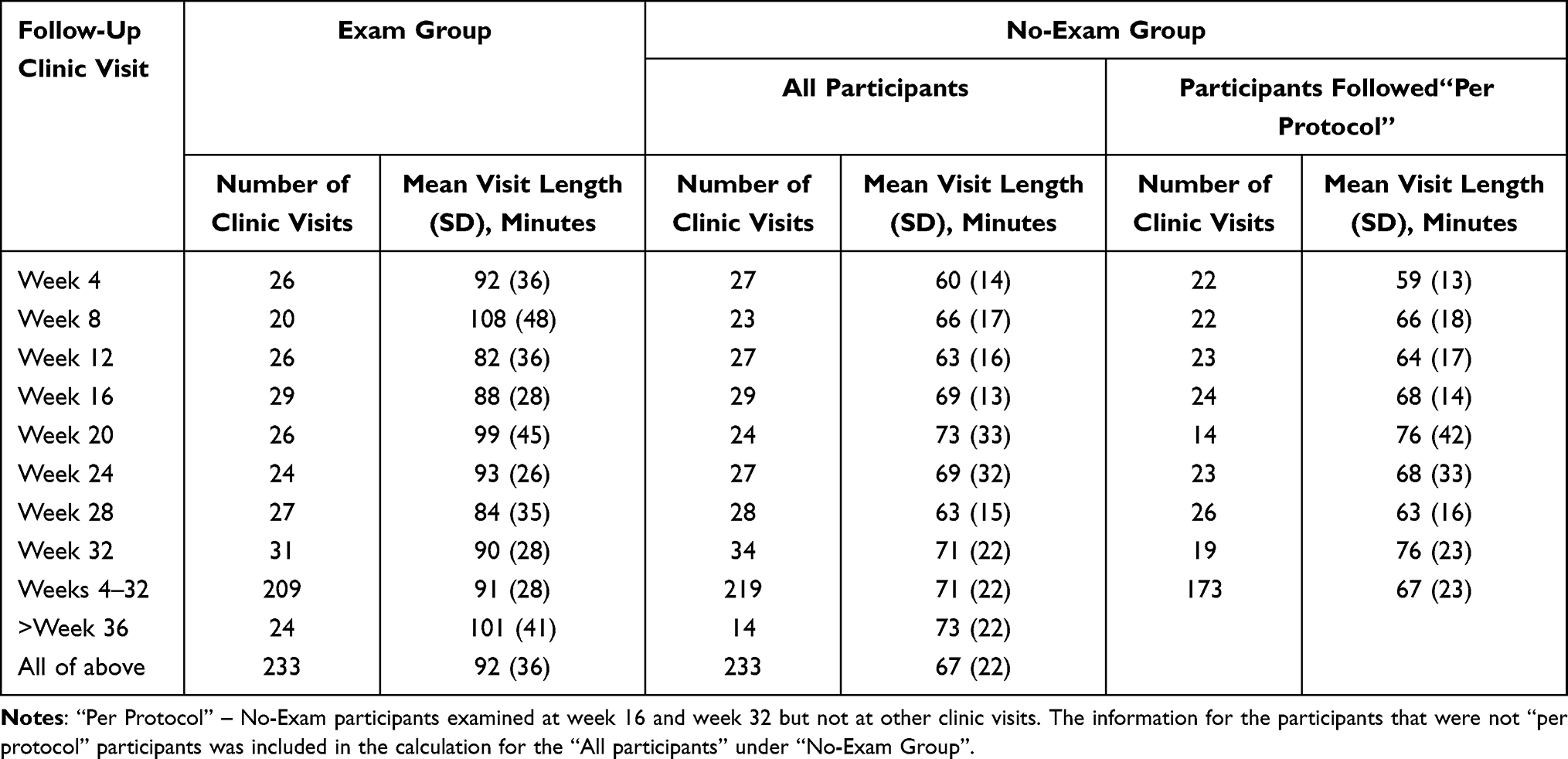 |
Table 7 Mean (Standard Deviation) Length of Scheduled Follow-Up Visits, in Minutes |
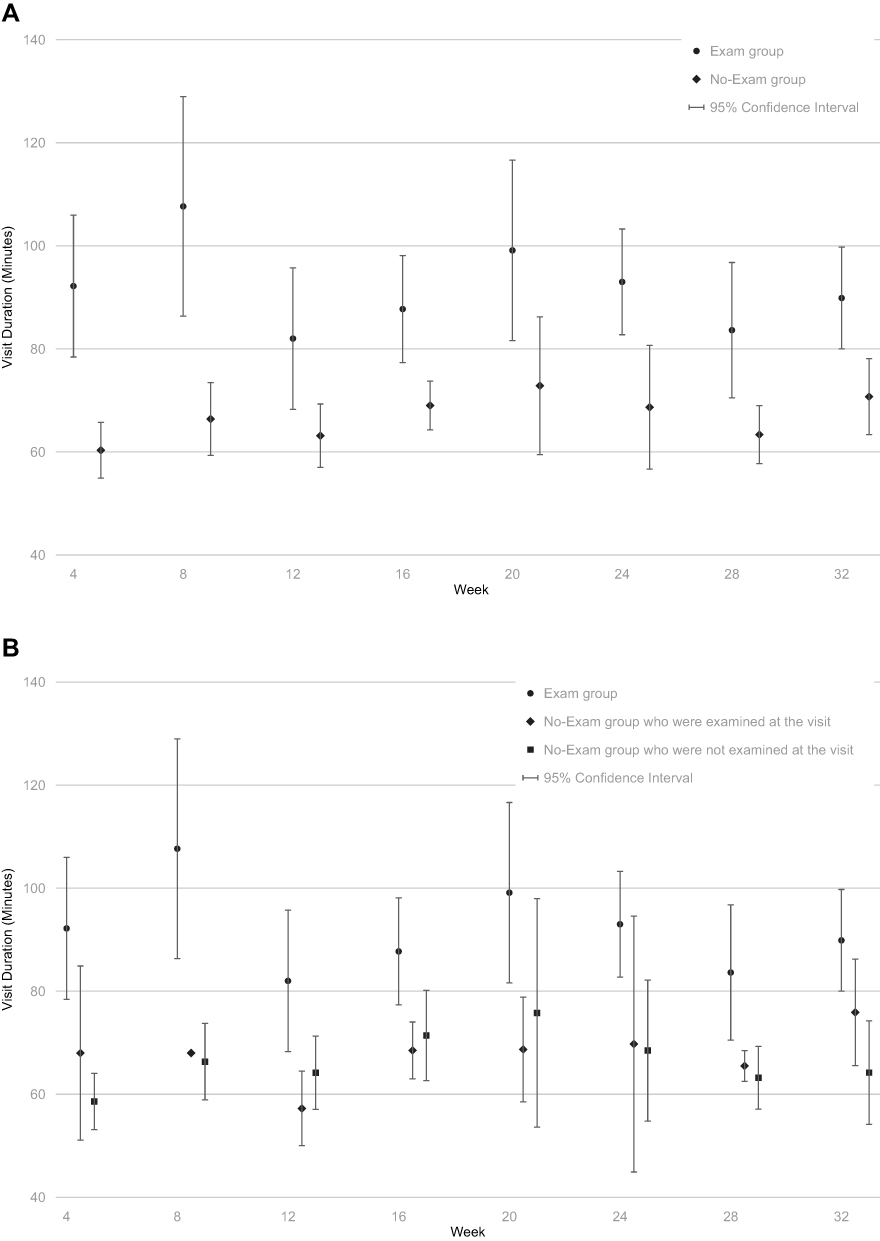 |
Figure 1 (A) Mean length of each follow-up clinic visit for participants for whom a retinal examination was required at each clinic visit (Exam Group) and those for whom a retinal examination was required at only the 16-week and 32-week visits (No-Exam Group) . (B) Mean length of each follow-up clinic visit for participants from Exam Group at each clinic visit, those from No-Exam group who were examined at the visit, and those from No-Exam Group who were not examined at the visit. |
Physician and Patient Satisfaction
Based on the 4-item questionnaire completed for each pilot study participant at each follow-up examination, the study ophthalmologists were satisfied that participants had been assessed adequately at more than 90% of all follow-up clinic visits, whether based on DFEs and imaging of all participants at the 16- and 32-week visits or based on review of images alone for the Imaging Only participants at those and other clinic visits.
The proportion of pilot study participants in the Imaging Only arm who responded that the length of the clinic visit waiting time was “excellent” or “very good” was larger at all follow-up visits than of participants assigned to the Full Exam arm (Figure 2). For example, following the 4-week visit, 64% and 52% of participants, respectively, gave one of these responses. The largest difference between the two groups was at the 20-week visit when 86% of the Imaging Only arm but only 42% of the Full Exam arm judged the length of the clinic visit to be “excellent” or “very good”. When all participants in the two groups who had a 16-week clinic visit were considered, the proportions who gave positive responses regarding waiting time were 48% of Full Exam arm participants and 85% of Imaging Only arm participants. When the comparison was restricted to the 22 Imaging Only participants who had a DFE at 16 weeks, the proportion for the Imaging Only arm was 86% (Tables 8–10). The differences between the two methods of comparison of satisfaction of Full Exam and Imaging Only participants yielded only trivial differences. At the 16-week and 32-week clinic visits, more participants in the Imaging Only arm than in the Full Exam arm judged the waiting time in clinic to be “excellent” or “very good”: 85% versus 48%, respectively at the 16-week visit and 81% versus 58% at the 32-week visit. Ratios of proportions who responded “excellent” or “very good” ranged from 1.16 (CI: 0.80, to 1.68) at the 28-week visit to 1.92 (CI: 1.22 to 3.03) at the 20-week visit, with ratios greater than 1.0 favoring the Imaging Only group and those with the lower boundary of the confidence interval greater than 1.0 indicating statistically significantly greater satisfaction with clinic waiting times among Imaging Only participants.
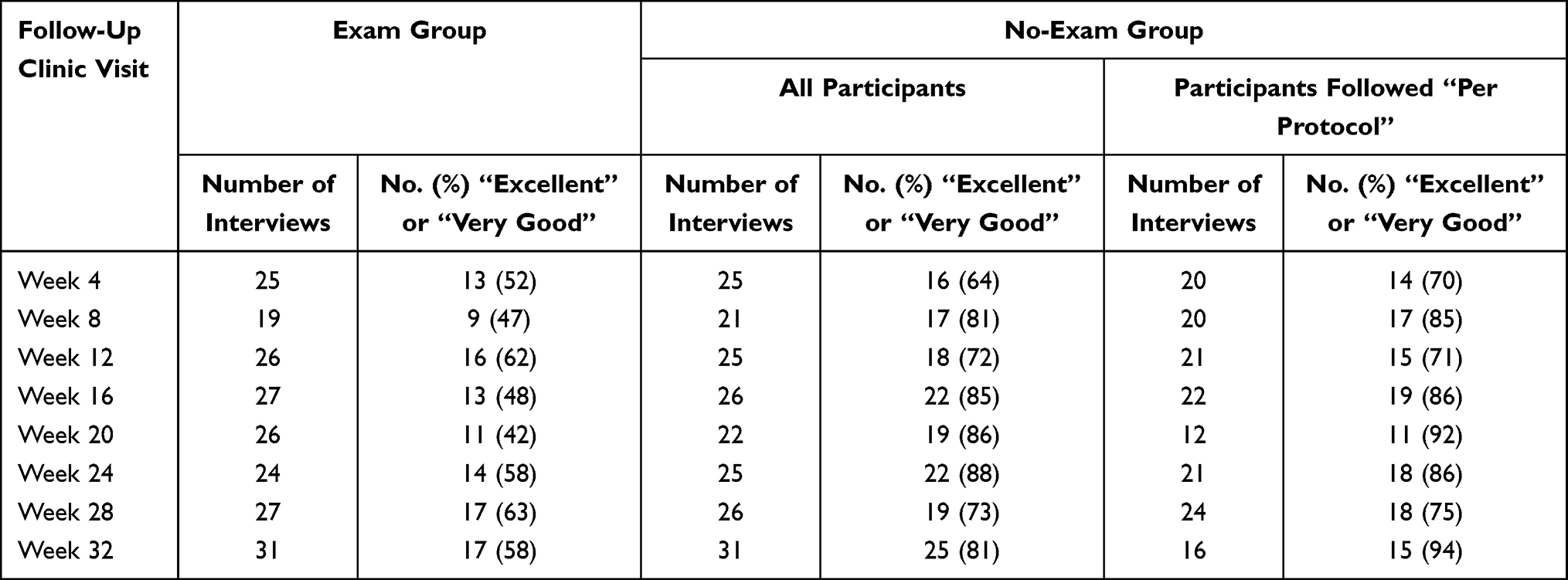 |
Table 8 Number (Percentage) of Participants Who Rated “Clinic Waiting Time” as “Excellent” or “Very Good” When Interviewed After Specified Scheduled Follow-Up Visits |
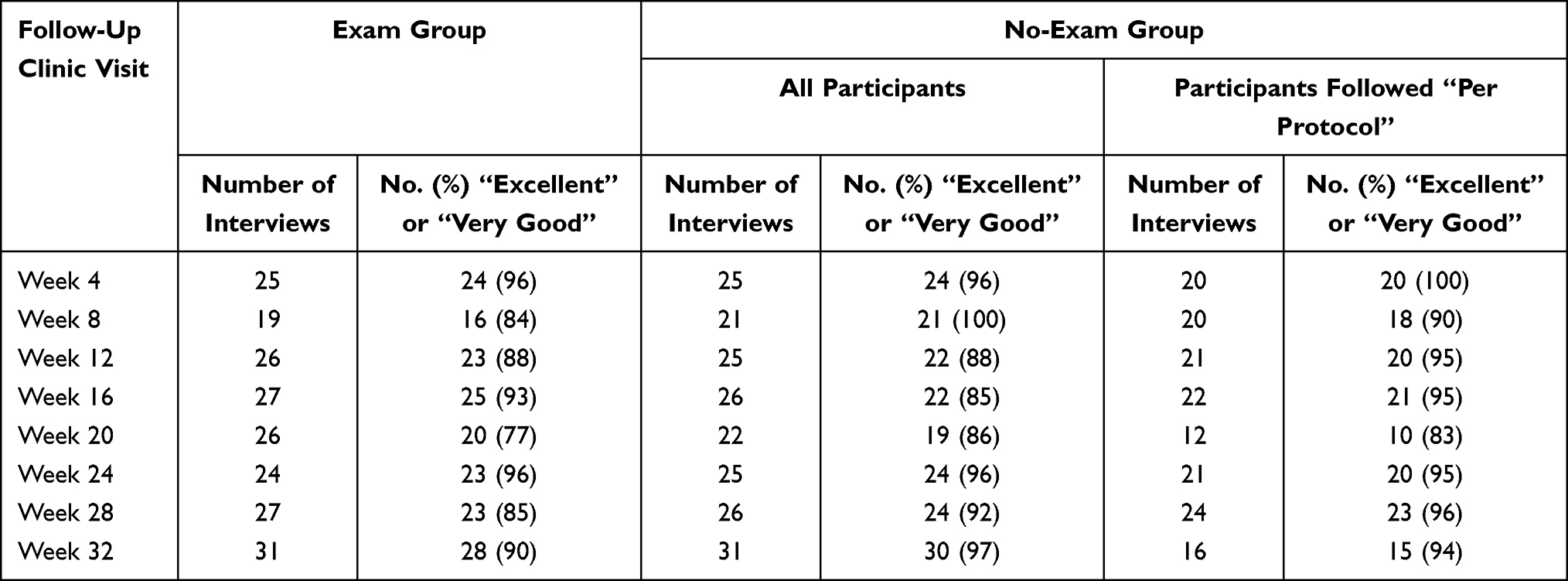 |
Table 9 Number (Percentage) of Participants Who Rated “Time Spent with Healthcare Professionals” as “Excellent” or “Very Good” During Interviews After Specified Scheduled Follow-Up Visits |
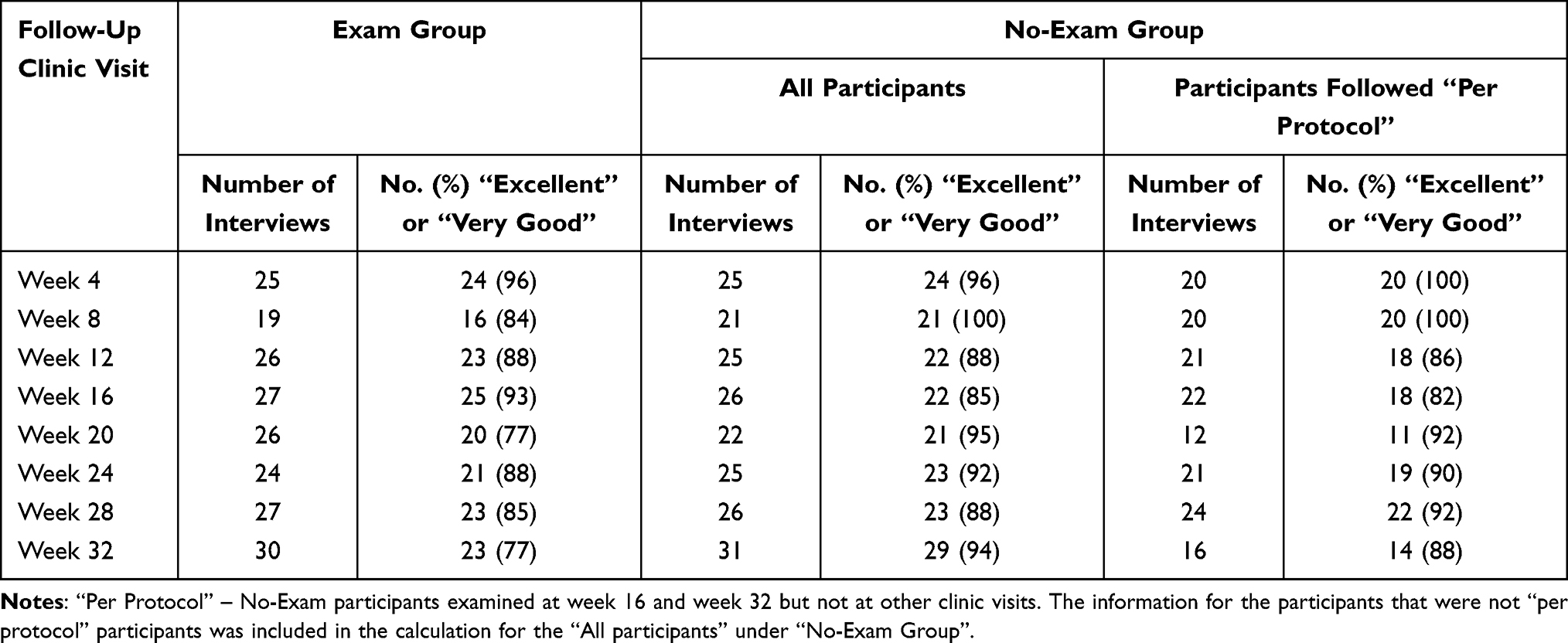 |
Table 10 Number (Percentage) of Participants Who Rated “Visit Overall” as “Excellent” or “Very Good” During Interviews After Specified Scheduled Follow-Up Visits |
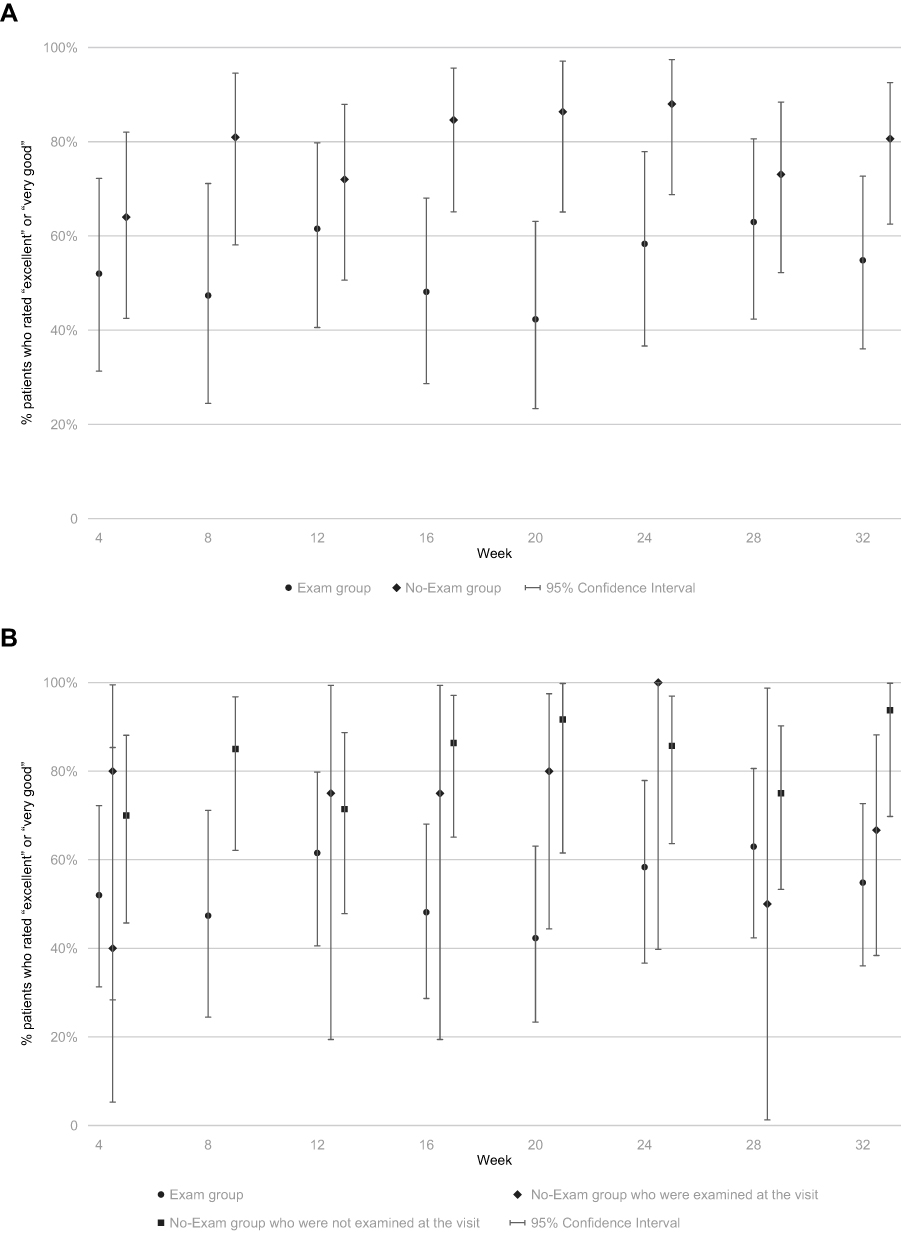 |
Figure 2 (A) Percentage of participants in each group who responded “excellent” or “very good” to the question regarding satisfaction about “Length of waiting time(s)” with aspects of each follow-up clinic visit scheduled in the pilot study. (B) Percentage of participants in each group (Exam Group, No-Exam group who were examined at the visit, and No-Exam Group who were not examined at the visit), who responded “excellent” or “very good” to the question regarding satisfaction about “Length of waiting time(s)” with aspects of each follow-up clinic visit scheduled in the pilot study. |
With respect to time spent with the ophthalmologist and other health-care providers, 90% or more of participants in both arms rated it as “excellent” or “very good” at almost all clinic visits (Figure 3). There was no consistent pattern regarding which group reported greater satisfaction, whether all participants with the specified clinic visits were compared or Full Exam participants were compared with Imaging Only participants followed “per protocol”. Differences between groups in proportions with high levels of satisfaction at all visits were 10% or less. Ratios of proportions ranged from 0.91 (CI: 0.76 to 1.08) at the 20-week visit to 1.09 (CI: 0.90 to 1.32) at the 28-week visit. The confidence intervals all included 1.0, indicating no statistically significant difference between Full Exam and Imaging Only participants.
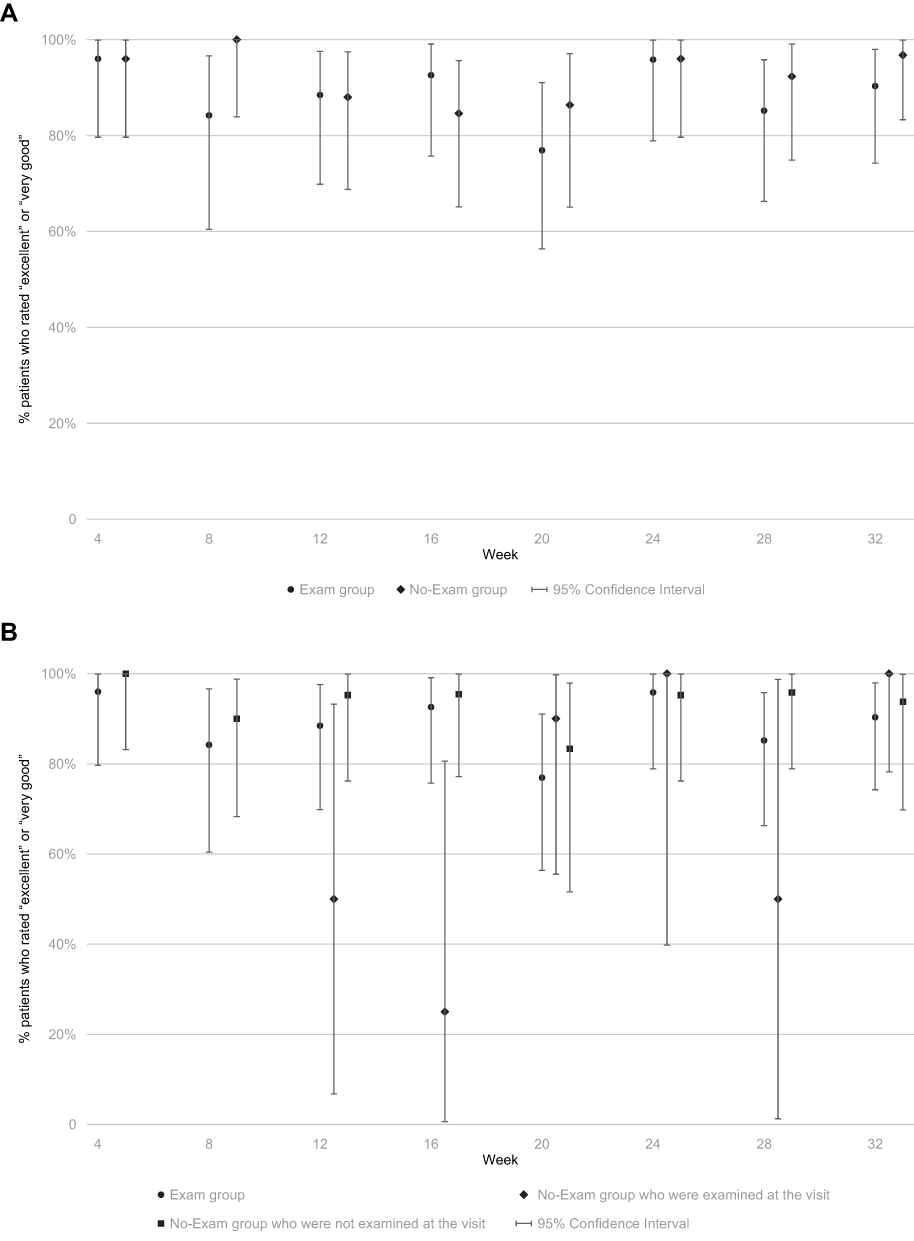 |
Figure 3 (A) Percentage of participants in each group who responded “excellent” or “very good” to the question regarding satisfaction about “Time spent with the ophthalmologist and other health care providers” with aspects of each follow-up clinic visit scheduled in the pilot study. (B) Percentage of participants in each group (Exam Group, No-Exam group who were examined at the visit, and No-Exam Group who were not examined at the visit), who responded “excellent” or “very good” to the question regarding satisfaction about “Time spent with the ophthalmologist and other health care providers” with aspects of each follow-up clinic visit scheduled in the pilot study. |
Finally, overall satisfaction with follow-up clinic visits was rated “excellent” or “very good” by 85% or more of participants in both groups at most visits, with no consistent difference between the Full Exam and Imaging Only arms (Figure 4). Exceptions were the 20-week and 32-week visits, judged to be “excellent” or “very good” overall by 95% and 94% of the Imaging Only arm but by only 77% of the Full Exam arm (ratio of proportions highly satisfied = 1.24, 95% CI: [0.99 to 1.54]).
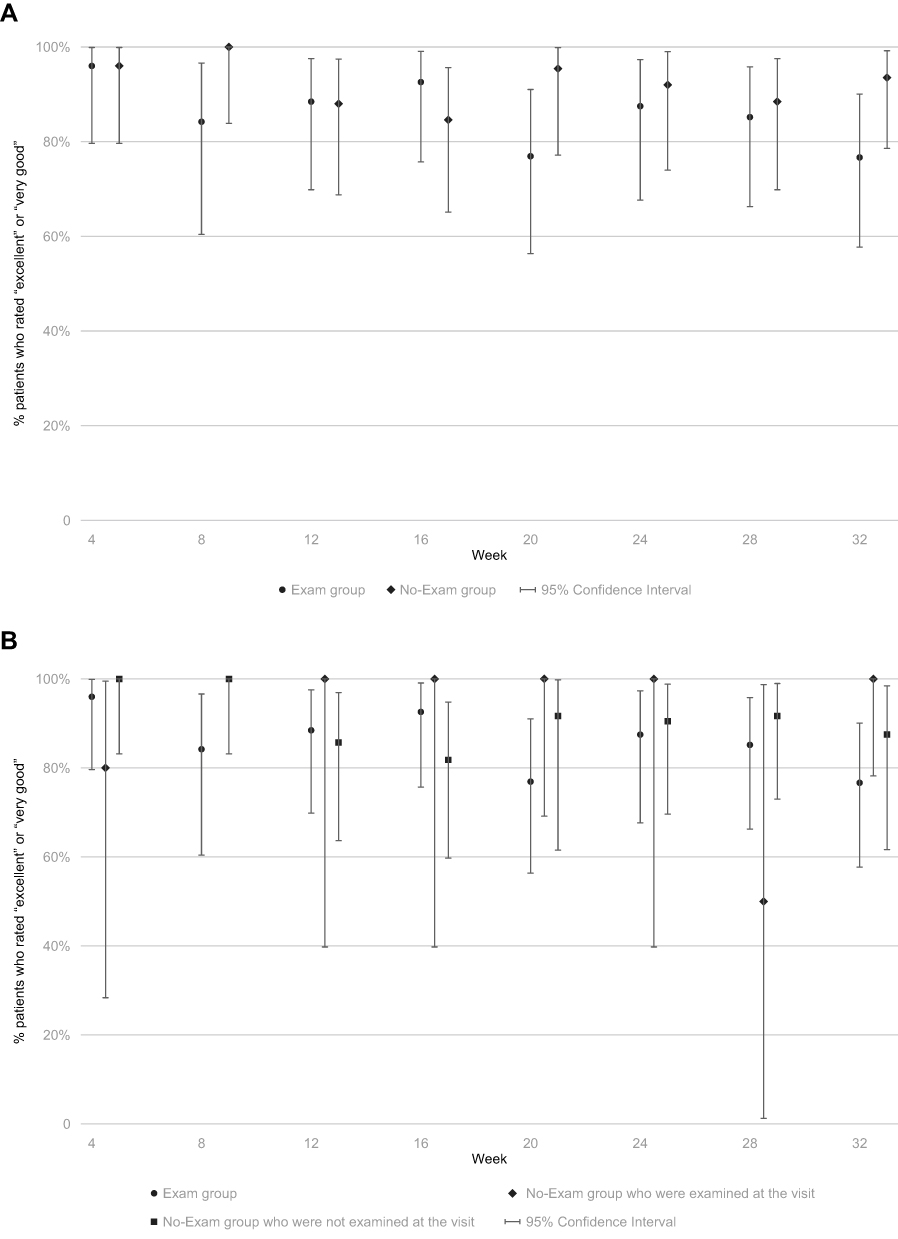 |
Figure 4 (A) Percentage of participants in each group who responded “excellent” or “very good” to the question regarding satisfaction about “Overall clinic visit” with aspects of each follow-up clinic visit scheduled in the pilot study. (B) Percentage of participants in each group (Exam Group, No-Exam group who were examined at the visit, and No-Exam Group who were not examined at the visit), who responded “excellent” or “very good” to the question regarding satisfaction about “Overall clinic visit” with aspects of each follow-up clinic visit scheduled in the pilot study. |
Discussion
In a pilot study designed to explore the potential of streamlined clinic visits in patients with NVAMD, 66 participants (70 study eyes) with NVAMD and a recent history of treatment with anti-VEGF agents were randomly assigned to 8 monthly follow-up visits with OCT imaging and DFE by a retina specialist at each clinic visit (Full Exam group) or to 6 of 8 monthly visits with imaging and ophthalmologist evaluation of images only to judge the need for repeat intravitreous injection of an anti-VEGF agent (Imaging Only arm). All participants were scheduled for DFE by a retina specialist at the 16- and 32-week clinic visits. Adherence to scheduled clinical follow-up was good, more than 80% of required visits were completed in each group. The primary safety measurements of usual-corrected visual acuity and central subfield thickness were similar in the two groups of participants at each follow-up visit, based on comparison of means and distributions. There was little change from baseline UCVA values or CST measurements to each follow-up clinic visit in either group. The mean number of PRN injections was similar in the two groups. Mean time in clinic during follow-up visits averaged 20 minutes shorter for participants in the Imaging Only arm. Somewhat more participants in the Imaging Only arm rated the waiting time in clinic, the time spent with the ophthalmologist and other personnel, and the clinic visit overall as “very good” or “excellent” at most clinic visits. These findings suggest that a streamlined follow-up examination protocol for NVAMD patients who are receiving PRN intravitreous anti-VEGF injections is acceptable to patients, does not compromise patient safety, and reduces the time such patients spend in clinic at each visit.
Thus, the reduction in the length of clinic visits for participants in the Imaging Only arm was supported with a high degree of satisfaction with clinic waiting times. Given the absence of safety concerns for the Imaging Only arm, further streamlining of visits for patients undergoing treatment for NVAMD can be envisioned. For instance, in this pilot study, participants were placed in rooms to wait for the retina specialist to review the images in their presence, as the investigators were concerned that enrollment might be difficult if patients feared randomization to an arm where they would have absolutely no interaction with their retina specialist after enrollment, except at the 4 months and 8 months clinic visits. Eliminating this step and replacing it with a telemedicine interpretation of the imaging would further reduce wait times for patients who do not require anti-VEGF therapy at a particular clinic visit. Additionally, at the majority of clinic visits, treating physicians requested OCT imaging alone rather than also requesting fundus photography and fluorescein angiography; thus, pupillary dilation could be avoided at many visits, further reducing clinic visit times. In an era where artificial intelligence is being utilized to assess images of the fundus and where COVID-19 concerns put more pressure on clinics to assess patients with even greater efficiency, it is easy to envision a new standard-of-care by which OCT images are interpreted in real-time in a reading center and patients shuttled either to treatment by the retina specialist or to discharge with follow-up as prescribed by the retina specialist.
The absence of safety concerns for participants who did not receive monthly DFE in this pilot study also indicates that a telemedicine strategy could be considered for the treatment of NVAMD patients who live in rural areas or areas that are underserved by retina specialists. OCT imaging could be obtained by a local comprehensive ophthalmologist and then interpreted by a retina specialist at an OCT reading center at a distant location to judge whether anti-VEGF treatment was necessary. When indicated, treatment could then be carried out by the local ophthalmologist.
Applicability of our findings is limited by the small number of participants, the inability to mask ophthalmologists and participants to the random assignment, and inadequate resources to provide an on-site study coordinator to remind clinic personnel of the assignment of each participant and to monitor adherence to the protocol for UCVA measurements and other procedures. Imaging Only participants missed a few more follow-up visits and, those who returned for clinic visits, were not always interviewed after the visits, possibly biasing estimates of time spent in clinic and interview responses regarding satisfaction with visits. Strengths of the pilot study include random assignment to the follow-up strategies compared, the study was conducted in existing retina clinics with established NVAMD patients under treatment with anti-VEGF agents, and assessment of both clinical and patient-reported outcomes.
In summary, our findings suggest that it is feasible and acceptable to patients for their ophthalmologists to follow their NVAMD based on imaging and less frequent DFEs than were mandated in the randomized trials that demonstrated the benefits of intravitreous injections of anti-VEGF agents without sacrificing visual acuity benefits or incurring additional harm.
Data Sharing Statement
The authors do not plan to share individual deidentified participant data.
Acknowledgments
Retina specialists at satellite clinics: Adam Wenick, MD, PhD; Ingrid Zimmer-Galler, MD; Adrienne Scott, MD; Akrit Sodhi, MD, PhD; Sharon D. Solomon, MD.
Data and Safety Monitoring Committee: Janet Holbrook, PhD, Chair; Catherine Meyerle, MD; Syed Mahmood Shah, MD.
Central Study Team: Sharon D. Solomon, MD, principal investigator; Victoria Kyerematen, MS, study coordinator 5/2014–8/2015; Madiha Qutab, BS, study coordinator, 8/2015–9/2016; Jiangxia Wang, MS, statistician; Kurt Dreger, systems analyst; Barbara S. Hawkins, PhD, consulting clinical trialist/epidemiologist.
This submission has not been published anywhere previously and is not simultaneously being considered for any other publication.
Disclosure
Ms. Kyerematen and Ms. Qutab were supported by a grant from the Wilmer Pooled Professors Research Fund, 2014–2016. Dr. Hawkins and Dr. Solomon received support from an unrestricted institutional grant to the Wilmer Eye Institute from Research to Prevent Blindness, New York, NY. Dr. Solomon also received support from the Katharine M. Graham Professorship in Ophthalmology. Ms. Wang and Mr. Dreger received support from a core grant, P30EY001765, to the Wilmer Eye Institute from the National Eye Institute, National Institutes of Health, US Department of Health and Human Services, Bethesda, Maryland. Dr Adam S Wenick reports personal fees from Genentech, outside the submitted work. Ms Jiangxia Wang reports grants from NEI, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
2. Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432–1444. doi:10.1056/NEJMoa062655
3. Maguire MG, Martin DF, Ying G-S; Comparison of Age-related Macular Degeneration Treatments Trials (CATT) Research Group. Five-Year outcomes with anti-vascular endothelial growth factor treatment of neovascular age-related macular degeneration: the comparison of age-related macular degeneration treatments trials. Ophthalmology. 2016;123(8):1751–1761. doi:10.1016/j.ophtha.2016.03.045
4. Solomon SD, Lindsley K, Vedula SS, Krzystolik MG, Hawkins BS. Anti-vascular endothelial growth factor for neovascular age-related macular degeneration. Cochrane Database Syst Rev. 2014;8:CD005139.
5. Prenner JL, Halperin LS, Rycroft C, et al. Disease burden in the treatment of age-related macular degeneration: findings from a time-and-motion study. Am J Ophthalmol. 2015;160(4):725–731. doi:10.1016/j.ajo.2015.06.023
6. Patel Y, Miller DM, Fung AE, Hill LF, Rosenfeld PJ. Are dilated fundus examinations needed for OCT-guided retreatment of exudative age-related macular degeneration? Ophthalmol Retina. 2020;4(2):141–147. doi:10.1016/j.oret.2019.09.006
7. Rand Corporation: Visit-Specific Satisfaction Instrument (VSQ-9). Available from: https://www.rand.org/health-care/surveys_tools/vsq9.html.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.