Back to Journals » International Medical Case Reports Journal » Volume 19
Arachnoid Cyst in the Posterior Fossa and Its Contested Association with Mania and Psychotic Symptoms in a Prepubertal Child: A Case Report
Authors AL Lihabi AA ![]()
Received 30 January 2026
Accepted for publication 30 June 2026
Published 16 July 2026 Volume 2026:19 598563
DOI https://doi.org/10.2147/IMCRJ.S598563
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Abeer Ayad AL Lihabi
Psychiatry, Medicine Department, Taibah University, Madinah Almonawara, Saudi Arabia
Correspondence: Abeer Ayad AL Lihabi, Email [email protected]
Abstract: Bipolar affective disorder presenting as a primary diagnosis in prepubescent children remains a contentious issue. Studies examining how common it is have yielded mixed, sometimes contradictory findings. One might argue that many of the rare cases described could actually be secondary to underlying neurological problems. In this report, we describe a 10-year-old girl with a posterior fossa arachnoid cyst who displayed a cluster of manic and psychotic symptoms. The clinical picture was marked by a sudden onset of irritability and hyperactivity, along with paranoid delusions. Of particular interest was a relapse after stopping medication. An initial EEG raised the possibility of epileptiform activity, but thorough follow-up testing failed to confirm this. Treatment with olanzapine and oxcarbazepine brought about some improvement, though not complete remission. Surgery was ultimately not pursued, as the cyst was deemed incidental. This case really discusses the difficulty in differentiating primary psychiatric illness from neuroimaging findings that may or may not be relevant. We propose that this might be a rare example of very early-onset mania, with the arachnoid cyst merely an incidental finding. It is worth noting that while there is some literature hinting at links between posterior fossa abnormalities and psychopathology, the evidence remains inconclusive. For a fuller picture, we include a one-year follow-up to shed light on the course of this complex presentation.
Keywords: mania, bipolar disorder, arachnoid cyst, early onset, psychosis
Introduction
Bipolar affective disorder is a type of mood disorder with a complex etiology. Bipolar I disorder (BPI) is characterized by the occurrence of at least one manic episode, in which an individual’s mood is abnormally and persistently elevated, expansive, or irritated and accompanied by four or more additional symptoms. These symptoms could include grandiosity, a decreased need for sleep, pressured speech, flight of ideas or racing thoughts, distractibility, increased goal-directed activity or psychomotor agitation, and excessive participation in pleasurable but risky activities.1
Mania or hypomania in prepubescents is considered rare. Prevalence values of 0.2–0.4% in children and roughly 1% in teenagers have been proposed by certain meta-analyses.2,3 However, longitudinal high-risk offspring studies have found that mania or hypomania typically only appears around mid-adolescence,4 and re-analyses of epidemiological studies have found no evidence of bipolar disorder before puberty.5
Arachnoid cysts (ACs) are collections of cerebrospinal fluid (CSF). The prevalence of arachnoid cysts is 2.6% in pediatrics, and over 90% are asymptomatic.6 The etiology of most arachnoid cysts is unclear.7,8 ACs are typically located in the middle cranial fossa and tend to be on the left side in the retrocerebellar region, with respective incidences of 34% and 33%. Only 5% of cases are reported to be symptomatic; the most common symptoms associated with AC are headache, hydrocephalus, ataxia, seizures, and dizziness.7 They can co-exist with psychiatric illnesses with varying presentations, depending on the location and size of the cyst, with some cysts being asymptomatic. These reports are limited, particularly when concerning pediatric patients.9–11 In this article, very-early-onset mania combined with a posterior fossa cyst is extremely rare.
Statement of Ethics
The patient’s legal guardian provided written informed consent for publication of the case details and images.
Case Presentation
Patient Information
This case presents a 10-year-old female in grade 5 whose school performance is average. She has quite a sensitive and shy personality and is prone to bullying at home and school. Seven months before presentation, she experienced repeated events of bullying. The first assessment in the psychiatry clinic was in March 2024, and the last follow-up was in March 2025.
History of Illness
Seven months before attending her first appointment, the child started to have an irritable mood and cried over seemingly insignificant events. She was unable to sleep due to high levels of activity. She would talk and sing to herself. Her mother had tried to force her to sleep, but she would scream and had difficulty settling down. She would wander around the house or exit the home with no identifiable plan or purpose. The child later reported hearing voices and became paranoid regarding her mother’s behavior and her sibling’s intentions. Due to troubling behavior and psychotic symptoms, her mother decided to keep her home from school, only allowing her to go to school on exam days. Her condition became more severe, particularly regarding hyperactivity, lack of sleep, and hallucinations. The family went to a neurologist, where she was diagnosed with epilepsy after an EEG report showed some epileptic activity despite her having no abnormal movement, disturbed level of consciousness, or orientation. The first EEG was conducted overseas, and although the findings indicated the presence of epileptiform activity, there was no information available about the qualifications of the reporting personnel or their interpretation methods for verification. She was prescribed olanzapine 5mg once daily and oxcarbazepine 300mg two times per day, after which some symptoms improved. However, she was still hyperactive, unable to focus, self-talking, and crying. Both medications are commonly used for epilepsy and mood disorders. She never returned to her baseline during the 7 months before her first appointment. No depressive episode reported.
Concerning personal history, the child’s birth followed a normal pregnancy and delivery. Her developmental milestones and academic performance were appropriate for her age; however, because of her recent condition, she could not attend school regularly. Her vaccines were up to date, her parents are not consanguineous, and there is no family history of epilepsy, mental health issues, or genetic disease.
Examination
She was conscious, alert, interactive, and oriented to time, place, and person. She had normal speech with short answers. She appeared detached, perplexed, and anxious, and asked her parents for help in providing information for the interview. Her examination showed normal cranial nerves,2–12 normal muscle tone, and symmetric deep tendon reflexes (+2). She had normal power in all limbs (5/5), normal down-going plantar response, and no ankle clonus. She had a normal cerebellar assessment and gait.
Investigations
Brain CT showed an arachnoid cyst at the level of the cerebellar region, with no abnormal brain parenchyma. A brain MRI (Figures 1 and 2) showed an approximately 2.5×2 x 1.8 cm (AP, T & CC dimensions) cystic mass, ovoid in shape with a smooth outline, located just infratentorial, and showed CSF intensity in all sequences - most likely a benign arachnoid cyst causing mild mass effect on the upper aspect of the cerebellar vermis and medial aspect of nearby occipital lobes. Repeated EEG in a trusted institute (awake and asleep) was normal, even when she was symptomatic. Blood work was normal, which included CBC, renal and liver panel, ANA, C3/C4, ESR, TSH, vitamin D, vitamin B12, folate, lactate, amino acid, and organic acid tests.
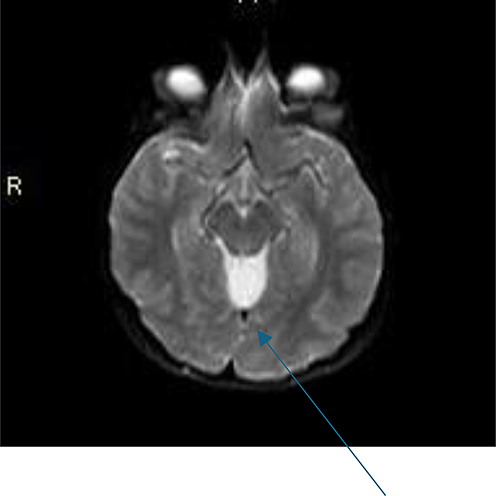 |
Figure 1 Axial T2-weighted MRI sequence showing a well-defined, ovoid arachnoid cyst in the posterior fossa. The cyst exerts a mild mass effect on the superior aspect of the cerebellar vermis and displays cerebrospinal fluid (CSF) signal intensity. The cyst’s location is indicated by an arrow. |
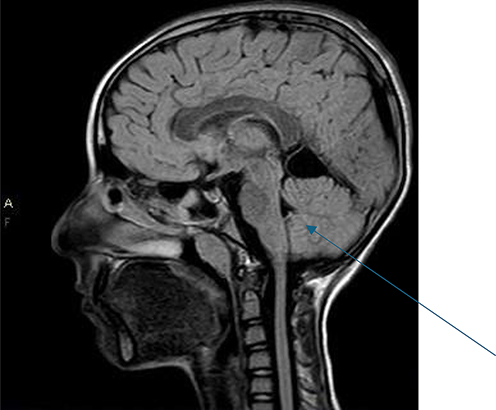 |
Figure 2 Sagittal T1-weighted MRI sequence providing an additional view of the posterior fossa arachnoid cyst, highlighting its infratentorial position and its relationship with adjacent occipital and cerebellar structures. The cyst’s location is marked by an arrow. |
Diagnostic Assessment
- Mixed affective vs manic state: mixed features were recognized, but the dominance of manic characteristics supported the diagnosis of mania.
- Disruptive Mood Disorder (DMDD): ruled out (episodic nature + presence of psychosis).
- Delirium/NCSE: evaluated; dismissed because of preserved cognitive function and normalization of EEG.
- Psychosis related to an arachnoid cyst: although thought to be possible, psychosis brought on by the cyst was judged less plausible because affective symptoms predominated.
Extended Differential Diagnosis
- Attention-Deficit/Hyperactivity Disorder (ADHD): While there was clear hyperactivity, we felt the diagnosis did not quite fit. The sudden onset of symptoms, the decreased need for sleep, and especially the psychotic features all point away from ADHD. It seems more consistent with something beyond just a hyperactivity disorder.
- Trauma-Related Disorders: Bullying was certainly a major psychosocial factor here, no doubt. That said, the symptom pattern—those episodic manic episodes coupled with psychosis—leans more towards a primary mood disorder rather than trauma-related.
Diagnostic Assessment
Mapping DSM-5 Criteria
When we looked closely at the patient’s presentation through the lens of DSM-5 criteria for a manic episode, several points stood out. She clearly exhibited a distinct and sustained period of abnormally elevated, expansive, or irritable mood, paired with heightened activity that lasted longer than a week—criteria A, basically. Then, diving deeper into the symptom checklist, we found at least three features: she showed a decreased need for sleep, was speaking more rapidly and at greater length than usual, appeared easily distracted, and demonstrated both increased goal-directed behavior and noticeable psychomotor agitation. These signs align with criterion B. What seemed particularly striking was how these symptoms culminated in a mood disturbance severe enough to significantly disrupt her social interactions and work life, meeting criterion C. It is worth noting that, while no formal diagnosis of a depressive episode was documented, the overall clinical picture fitted best with a manic episode. One might argue that this constellation of symptoms leaves little room for alternative explanations.
Limitation
We acknowledge that this case study lacks standardized psychiatric assessment tools like the Young Mania Rating Scale or the Kiddie Schedule for Affective Disorders and Schizophrenia (Kiddie-SADS). Instead, our diagnosis relied heavily on thorough clinical interviews combined with prolonged longitudinal observation. It seems this approach, while detailed, may introduce some subjectivity that standardized measures might have helped mitigate. Still, given the complexity of the presentation, we felt careful clinical judgment was essential.
Therapeutic Interventions and Outcome
The patient was initially administered olanzapine [5mg] and oxcarbazepine [300 mg] two times per day. Due to excessive sleepiness and increased appetite, the olanzapine dosage was lowered to 2.5 mg, leading to an improvement in mood, sleep quality, and a decrease in psychotic symptoms. Nevertheless, some anxiety and clingy behaviors continued, prompting the addition of paroxetine at 12.5 mg.
She maintained a relatively stable condition over the following months, but she did not regain her previous level of functioning. In December 2024, her family discontinued all medications, and within a week, she experienced a relapse characterized by feelings of suspicion, heightened activity, nighttime wandering, and a decrease in appetite.
The patient exhibited significant improvement in her symptoms with the use of medication, especially regarding her mood and psychotic issues. However, she did not completely return to her pre-illness state and continued to experience lingering anxiety and dependence. Periods in which the medication regimen was followed were linked with relative stability, whereas the stopping of treatment resulted in a relapse. During the last check-in in March 2025, she was stable on olanzapine 5 mg, although she had developed nocturia. A consultation with neurosurgery took place, but surgery was deemed unnecessary since the cyst was relatively small, only produced mild pressure effects, and did not result in any specific neurological deficits. As a result, conservative management was preferred, consistent with contemporary neurosurgical guidelines that suggest reserving surgical decompression for cases with evident neurological issues or worsening symptoms. No formal psychosocial interventions were offered during that time. Table 1 outlines the timeline of care.
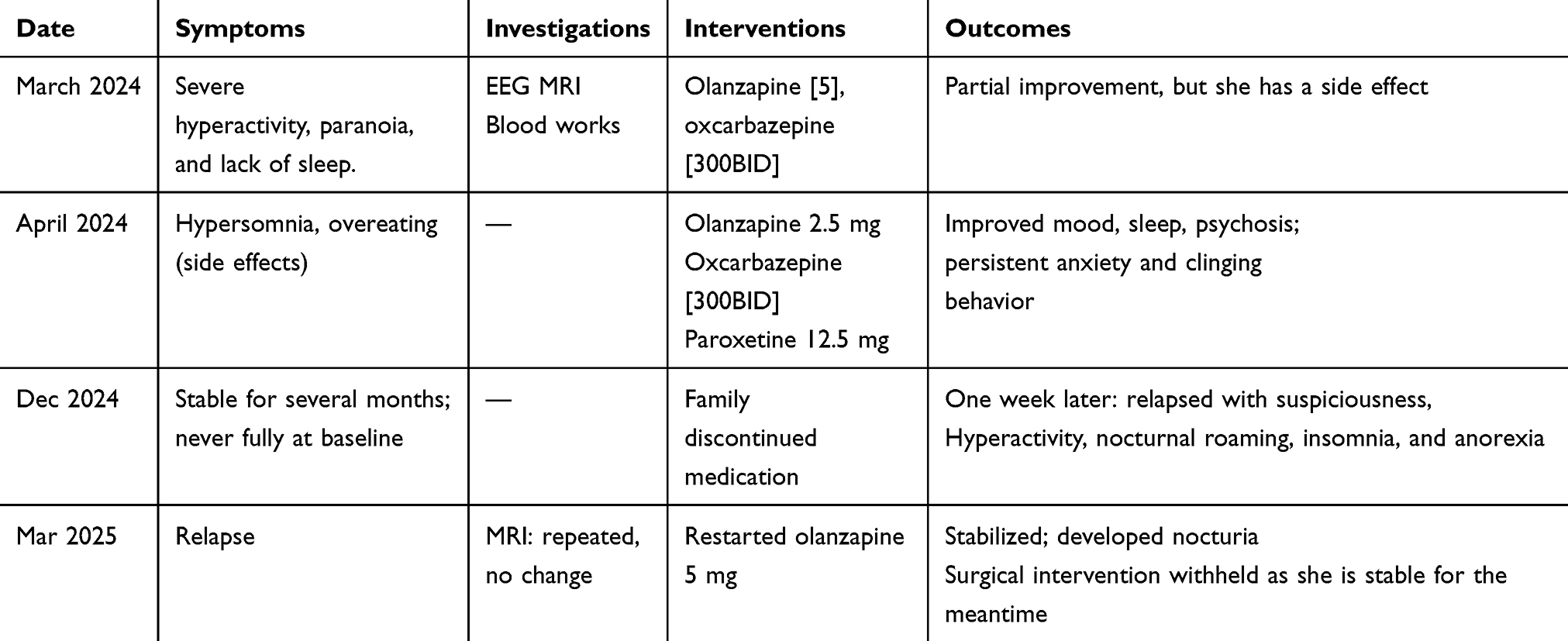 |
Table 1 Timeline of Care |
Patient Perspective
The patient’s mother stated, “the hardest part has been her trouble sleeping and her persistent wandering throughout the night. Although I experienced some relief after medication, I remain concerned about her recovery”.
Discussion
This case really puts us in a diagnostic grey zone: are the symptoms genuinely linked to the posterior fossa arachnoid cyst, or could this be an unusual manifestation of pre-pubertal primary bipolar disorder? The timing certainly raises questions, but it’s hard to say for sure if one caused the other. What stands out is that the patient’s symptoms got better with psychiatric meds—not surgery—and then worsened when the meds were stopped. Meanwhile, the cyst itself caused only a mild mass effect, and there were no neurological deficits to speak of. Given all this, it seems reasonable that the neurosurgical team recommended a watch-and-wait approach, supporting the simpler idea that the cyst is just an incidental finding.12,13
Although arachnoid cysts are uncommon, there are reports of people with related psychotic symptoms, which could be explained by the pressure the cyst puts on the temporal lobe and other surrounding structures. Depression and frontal arachnoid cysts have been linked,13 and psychosis has been linked to left temporal lobe cysts.14,15 Alexithymia symptoms have been previously reported with a left frontotemporal cyst,14 and individuals with left temporal lobe cysts have been known to exhibit outward hostility and experience mood disorders akin to manic depression (bipolar illness).16 Furthermore, hypomanic symptoms and marked cognitive impairment have been reported in middle-aged women.17 An overview of instances with posterior fossa cysts and documented psychiatric conditions can be seen in Table 2.
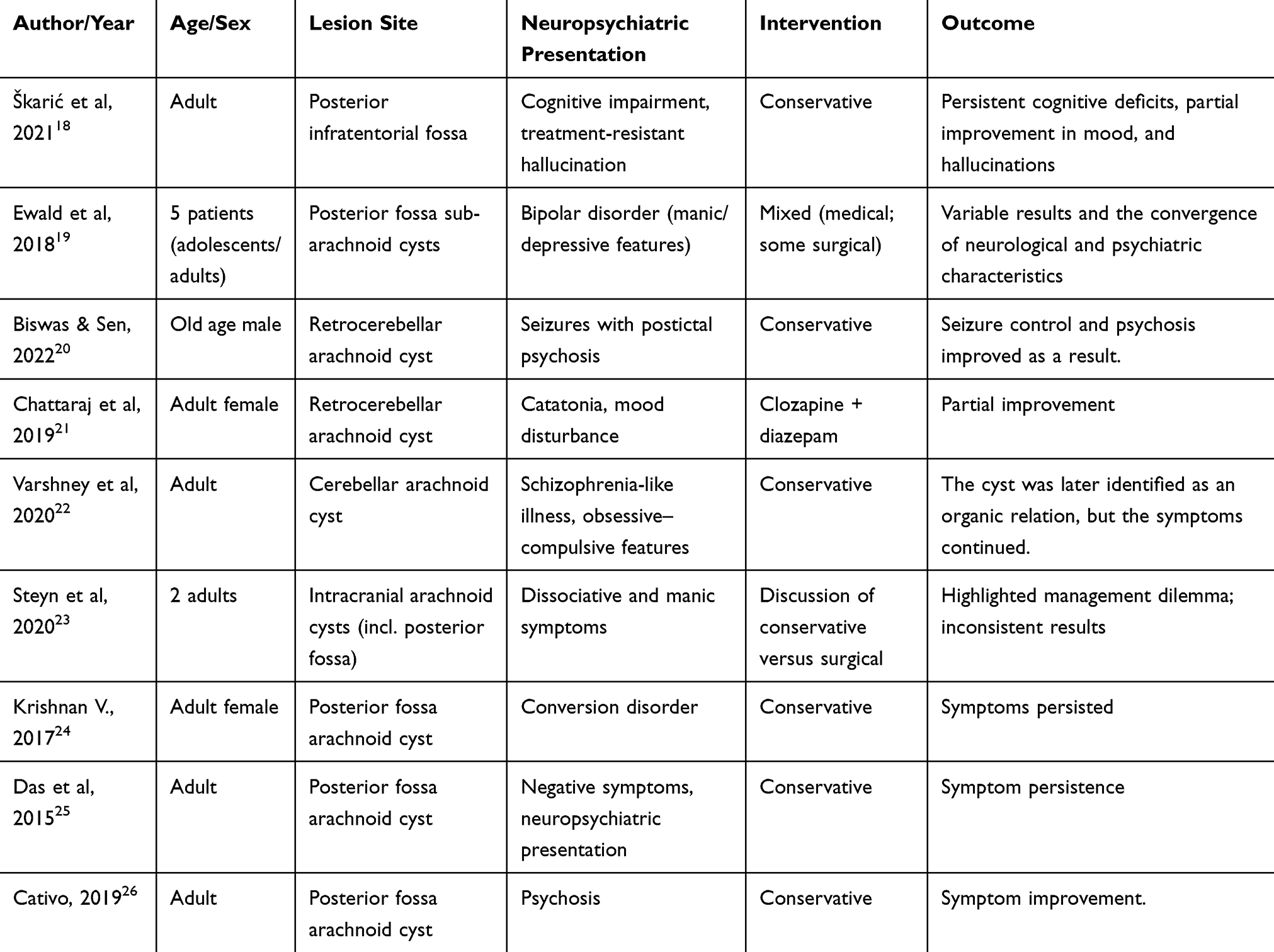 |
Table 2 Reported Posterior Fossa Arachnoid Cysts with Psychiatric Presentations |
The frontal and limbic cortices have been the primary sites of brain abnormalities in patients with bipolar disorders.27 According to recent research, the cerebellum is one of the key brain regions involved in processing emotions.28 The emergence of mood disorders following cerebellar injury and the identification of anomalies in cerebellar and cerebellar-cortical connections in BP patients provide evidence in favor of this theory.
The cerebellum can be anatomically separated into anterior and posterior lobes. The posterior lobe of the cerebellum is believed to be engaged in cognitive and affective processes like attention, language, awareness, and emotional reactions, whereas the anterior lobe is primarily linked to motor control and learning.29 Reduced gray matter volume (GMV) in the anterior and posterior cerebellar lobes, as well as microstructural abnormalities in the cerebellar peduncles and dentate nuclei, have been found in structural MRI investigations.30,31
Furthermore, functional MRI research has demonstrated reduced activity in the cerebral cortex, impaired intercerebellar coordination, and disrupted functional connectivity (FC) between the cerebellum and the limbic system, which is the default mode network.32 These results imply that the etiology and progression of bipolar disorder may be related to anatomical and functional abnormalities of the cerebellum. There is increasing evidence that the cerebellum has a role in affective and cognitive processes; its exact function in mood regulation is still being studied. These variations may contribute to some variability in bipolar disorder presentations.
In the case described, the onset of mania with psychotic symptoms in a 10-year-old child without personal or family antecedents of psychosis enables us to evaluate the possibility of a causal relationship between the arachnoid cyst discovered by magnetic resonance imaging (MRI) and the set of symptoms. Bipolar disorder is very rare at this age, especially without genetic contribution. Our patient had manic symptoms plus psychosis at a very young age. It is possible that the patient’s cerebellar lesion was incidental to an underlying psychiatric disorder and that the brain lesion was an incidental finding without functional importance. However, we cannot exclude the possibility that the infratentorial-located arachnoid cyst caused thinning of the adjacent cortex and reorganization of cortical functions.
Diagnosing bipolar disorder in prepubertal children is still a hotly debated topic. The challenge largely lies in the overlapping symptoms, the often-inconsistent ways the disorder can present, and the fact that bona fide bipolar disorder is relatively uncommon in this age group. Irritability and behavioral problems are frequent complaints among younger patients, but these signs can just as easily point toward other diagnoses—disruptive mood dysregulation disorder (DMDD) being a prime example. That said, in this case, the episodic nature of the symptoms alongside psychotic features seems to tilt the scales in favor of bipolar disorder rather than DMDD. It is worth noting that these nuances make the diagnosis anything but straightforward.
Looking over the case reports summarized in Table 2, it seems that psychiatric symptoms in many adult patients did not reliably clear up after surgery. That said, the link between the surgical intervention and the psychiatric manifestations often felt more correlational than definitively causal.15,16 One might argue that this ambiguity complicates how we interpret outcomes in these cases.
To sum up, there’s growing evidence pointing to a connection between arachnoid cysts and cognitive or psychiatric symptoms. That said, in our case, the clinical trajectory, how the patient responded to treatment, and the absence of neurological signs all seem to support the diagnosis of a primary psychiatric disorder. It’s worth emphasizing how crucial a detailed diagnostic workup is, especially when incidental findings show up on neuroimaging in patients presenting with early-onset psychiatric issues. At the same time, one might argue that more functional studies are needed to really clarify what role, if any, these cystic lesions play in psychiatric presentations.
Conclusion
This case illustrates the complexity of diagnosing bipolar disorder in a pre-pubertal child, the necessity of considering organic contributions, such as posterior fossa arachnoid cysts, and the importance of cautious management decisions. Follow-ups with the patient over time and the gathering of related cases are required to establish causality. This case adds to the limited literature on posterior fossa arachnoid cysts in relation to psychiatric symptoms, especially within the pediatric population, marking it as a rare and significant finding. However, there are limitations, including the lack of surgical intervention, which hinders the ability to establish causality, and the relatively brief follow-up period, which limits assessment of long-term effects. These aspects emphasize the necessity for more extensive longitudinal and functional research to gain a clearer understanding of the connection between arachnoid cysts and psychiatric manifestations.
Data Sharing Statement
Included in the main manuscript.
Funding
There is no funding to report.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Substance Abuse and Mental Health Services Administration. DSM-5 Changes: Implications for Child Serious Emotional Disturbance. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2016.
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 2013.
3. Van meter AR, Burke C, Youngstrom EA, Faedda GL, Correll CU. The bipolar prodrome: meta-analysis of symptom prevalence prior to initial or recurrent mood episodes. J Am Acad Child Adolesc Psych. 2016;55(7):543–8. PMID: 27343882. doi:10.1016/j.jaac.2016.04.017
4. Duffy A, Carlson G, Dubicka B, Hillegers MHJ. Pre-pubertal bipolar disorder: origins and current status of the controversy. Int J Bipolar Disord. 2020;8(1):18. PMID: 32307651; PMCID: PMC7167382. doi:10.1186/s40345-020-00185-2
5. Parry P, Allison S, Bastiampillai T. ‘Pediatric bipolar disorder’ rates are still lower than claimed: a re-examination of eight epidemiological surveys used by an updated meta-analysis. Int J Bipolar Disord. 2021;9(1):21. PMID: 34170440; PMCID: PMC8233426. doi:10.1186/s40345-021-00225-5
6. Sarwar S, Rocker J. Arachnoid cysts in paediatrics. Curr Opin Pediatr. 2023;35(2):288–295. PMID: 36692001. doi:10.1097/MOP.0000000000001219
7. Schmahmann JD, Sherman JC. The cerebellar cognitive affective syndrome. Brain. 1998;121(Pt4):561–579. PMID: 9577385. doi:10.1093/brain/121.4.561
8. Al-Holou WN, Terman S, Kilburg C, Garton HJ, Muraszko KM, Maher CO. Prevalence and natural history of arachnoid cysts in adults. J Neurosurg. 2013;118(2):222–231. PMID: 23140149. doi:10.3171/2012.10.JNS12548
9. Ahmed AK, Cohen AR. Intracranial arachnoid cysts. Childs Nerv Syst. 2023;39(10):2771–2778. PMID: 37466684. doi:10.1007/s00381-023-06066-0
10. Boomkens HR, van der Cammen TJM, Mattace-Raso FUS. Primary arachnoid cyst mimicking depressive symptoms in an elderly woman. Int Psychogeriatr. 2010;22(5):832–833. Epub 2010 May 25. PMID: 20497622. doi:10.1017/S1041610210000670
11. Mironov A, John S, Auerbach J, Jamaleddine G. Acute onset of psychosis in a patient with a left temporal lobe arachnoid cyst. Case Rep Med. 2014;2014:204025. Epub 2014 Feb 11. PMID: 24715905; PMCID: PMC3970447. doi:10.1155/2014/204025
12. Wester K. Intracranial arachnoid cysts--do they impair mental functions? J Neurol. 2008;255(8):1113–1120. Epub 2008 Jul 28. PMID: 18677648. doi:10.1007/s00415-008-0011-y
13. Gelabert-González M. Quistes aracnoideos intracraneales [Intracranial arachnoid cysts]. Rev Neurol. 2004;39(12):1161–1166. Spanish. PMID: 15625636.
14. Blackshaw S, Bowen RC. A case of atypical psychosis associated with alexithymia and a left fronto-temporal lesion: possible correlations. Can J Psychiatry. 1987;32(8):688–692. PMID: 3690485. doi:10.1177/070674378703200809
15. Vakis AF, Koutentakis DI, Karabetsos DA, Kalostos GN. Psychosis-like syndrome associated with intermittent intracranial hypertension caused by a large arachnoid cyst of the left temporal lobe. Br J Neurosurg. 2006;20(3):156–159. PMID: 16801049. doi:10.1080/02688690600776986
16. Heinrichs W. In search of madness: schizophrenia and neuroscience; 2001. doi:10.1093/acprof:oso/9780195122190.001.0001
17. Shettar M, Karkal R, Misra R, Kakunje A, Chandran V, Mendonsa R. Arachnoid cyst causing depression and neuropsychiatric symptoms: a case report. East Asian Archiv Psych. 2018;28:64–67. doi:10.12809/eaap181690
18. Škarić M, Aukst Margetić B, Bogović Dijaković A, Karlović D. Cognitive and psychotic symptoms in a patient with infratentorial arachnoid cyst: case report. Acta Clin Croat. 2021;60(2):304–308. PMID: 34744282; PMCID: PMC8564833. doi:10.20471/acc.2021.60.02.18
19. Ewald VAM, Purnell JR, Bruss JE, et al. Posterior fossa sub-arachnoid cysts observed in patients with bipolar disorder: a retrospective cohort study. Cerebellum. 2023;22(3):370–378. Epub 2022 May 14. PMID: 35568792; PMCID: PMC9659668. doi:10.1007/s12311-022-01408-1
20. Biswas R, Sen I. Seizures and postictal psychosis in a patient with retrocerebellar arachnoid cyst: a case report. Cureus. 2022;14(5):e24935. PMID: 35698697; PMCID: PMC9187137. doi:10.7759/cureus.24935
21. Chattaraj S, Mukherjee D, Kundu PS. A unique case of catatonia in a background of retrocerebellar arachnoid cyst responding to clozapine and diazepam treatment. Ann Indian Psych. 2025. doi:10.4103/aip.aip_196_24
22. Varshney P, Raghuraman BS, Ganjekar S, Sharma M, Chaturvedi S. Cerebellar arachnoid cyst masquerading initially as schizophrenia and later as obsessive compulsive disorder. Asian J Psychiatr. 2020;47:101838. Epub 2019 Oct 14. PMID: 31706227. doi:10.1016/j.ajp.2019.10.018
23. Steyn PJ, Jordaan GP. Case series: intracranial arachnoid cysts and neuropsychiatric presentations. BMJ Case Rep. 2020;13(5):e233345. doi:10.1136/bcr-2019-233345
24. Krishnan V, Khandelwal SK, Bhatia MS. Conversion disorder in a patient with posterior fossa arachnoid cyst. J Neuropsychiatry Clin Neurosci. 2017;29(3):297–298. doi:10.1176/appi.neuropsych.16090117
25. Das S, Srivastava A, Ghosh A. Posterior fossa arachnoid cyst presenting as negative symptoms. Indian J Psychol Med. 2015;37(2):228–230. doi:10.4103/0253-7176.155621
26. Cativo M. The link between arachnoid cysts and psychosis: a case report and review of the literature. Clin Case Rep Int. 2019;3:1139. doi:10.25107/2638-4558
27. Fournier JC, Chase HW, Almeida J, Phillips ML. Within- and between-session changes in neural activity during emotion processing in unipolar and bipolar depression. Biol Psychiatry Cogn Neurosci Neuroimaging. 2016;1(6):518–527. PMID: 28083566; PMCID: PMC5220672. doi:10.1016/j.bpsc.2016.03.005
28. Chen L, Wang Y, Niu C, et al. Common and distinct abnormal frontal-limbic system structural and functional patterns in patients with major depression and bipolar disorder. Neuroimage Clin. 2018;20:42–50. PMID: 30069426; PMCID: PMC6067086. doi:10.1016/j.nicl.2018.07.002
29. Zhao L, Wang Y, Jia Y, et al. Microstructural abnormalities of basal ganglia and thalamus in bipolar and unipolar disorders: a diffusion kurtosis and perfusion imaging study. Psychiatry Invest. 2017;14(4):471–482. PMID: 28845175; PMCID: PMC5561406. doi:10.4306/pi.2017.14.4.471
30. Schmahmann JD, Caplan D. Cognition, emotion and the cerebellum. Brain. 2006;129(Pt 2):290–292. PMID: 16434422. doi:10.1093/brain/awh729
31. Kim D, Cho HB, Dager SR, et al. Posterior cerebellar vermal deficits in bipolar disorder. J Affect Disord. 2013;150(2):499–506. Epub 2013 Jun 12. PMID: 23769608; PMCID: PMC5510461. doi:10.1016/j.jad.2013.04.050
32. Luo X, Chen G, Jia Y, et al. Disrupted cerebellar connectivity with the central executive network and the default-mode network in unmedicated bipolar II disorder. Front Psychiatry. 2018;9:705. PMID: 30618876; PMCID: PMC6305495. doi:10.3389/fpsyt.2018.00705
33. Phillips ML, Swartz HA. They offer a thoughtful critique of neuroimaging studies in bipolar disorder, pushing us toward rethinking the neural circuits involved and suggesting directions for future investigations. American J Psych. 2014;171(8):
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.