Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Aquagenic Palmoplanta keratoderma: Response to Topical Pimecrolimus and Literature Review
Received 28 September 2025
Accepted for publication 11 January 2026
Published 21 January 2026 Volume 2026:19 566532
DOI https://doi.org/10.2147/CCID.S566532
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michela Starace
Jinpeng Shan, Rukang Chen
Department of Dermatology, The Second Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, Zhejiang, 310005, People’s Republic of China
Correspondence: Rukang Chen, Department of Dermatology, The Second Affiliated Hospital of Zhejiang Chinese Medical University, No. 318, Chaowang Road, Hangzhou, People’s Republic of China, Tel +86 15757194107, Fax +86 15757194107, Email [email protected]
Abstract: Aquagenic palmoplantar keratoderma (APK) is a rare skin disease characterized by temporary papules and macerated plaques triggered by contact with water. Failure to receive timely and proper treatment may seriously damage the patient’s daily life. The precise pathogenesis of APK (Aquagenic Palmoplantar Keratoderma) remains poorly understood, and safe and efficacious therapeutic options are currently lacking. The conventional therapy mainly involves topical application of aluminum chloride, followed by botulinum toxin injection, topical corticosteroids, topical salicylic acid, barrier agents, and oral antihistamines. This case report presents an APK patient who showed improvement after tw1o months of treatment with pimecrolimus cream, slight symptom recurrence following water exposure or sweating.
Keywords: aquagenic palmoplantar keratoderma, water contact test, pimecrolimus
Introduction
Aquagenic palmoplantar keratoderma (APK) is a rare skin disease, which is characterized by the rapid appearance of white papules, excessive wrinkling and swelling of the palm after brief contact with water. Under normal circumstances, wrinkles appear on the palms within an average of 12 minutes when soaked in water.1,2 We described a female patient who was treated with pimecrolimus for affected hands and wrists.
Case Presentation
A 50-year-old woman presented to the outpatient dermatology department with an over 20-years history of rapid appearance of white papules, excessive wrinkling and swelling of the palm after brief exposure to warm water or sweating,but there were no symptoms of itching, burning, or pain. Upon water removal, the symptoms disappeared rapidly. She denies having a history of atopic dermatitis or hyperhidrosis, smoking, or a history of special medications, as well as denying engaging in long-term frequent hand washing work, and no other family members have experienced similar symptoms.
On examination, after soaking both hands in hot water or sweat, diffuse white spots were visible on the dorsal of the hands and wrists, with skin lines remaining. The palmar skin exhibited a pebbly appearance and slight edema, accompanied by excessive swelling (Figure 1A and B). Approximately half an hour after the sweat evaporated, the skin keratinization of the dorsal of the hands and wrists subsided, leaving behind a few white spots, and only a few erythematous spots were visible on the palms (Figure 1C and D). Due to the patient’s clinical symptoms, a biopsy was not taken. Based on her history,the appearance of her hands and an otherwise normal physical examination, we diagnosed aquagenic palmoplanta keratoderma(APK). She applied topical Pimelomos ointment twice a day and was advised to continue her daily routine, including weekly moisturizing and follow-up. Her palm texture and symptoms improved within a week (Figure 2). When she stopped treatment and was exposed to sweat or hot water again after 2 months, the symptoms recurred but also responded to retreatment with pimecrolimus.
 |
Figure 1 Clinical images of aquagenic plamoplantar keratoderma in a 50-year-old woman. (A) Diffuse white spots were visible on the dorsal aspects of the hands and wrists, with skin lines remaining. (B) Visible erythema on the palm, diffuse white spots were visible on the wrists. (C) Upon the removal of water, the skin keratinization on the dorsal aspects of the hands subsided, leaving behind a few white spots. (D) After the palm dries,only a few erythematous spots were visible on the palms. |
 |
Figure 2 Substantial improvement noted in skin texture and wrinkling of hand skin 1 week after treatment with pimecrolimus ointment. |
Discussion
APK is triggered on the palms and soles after brief immersion in water, and is characterized by the rapid appearance of translucent papules or macerated plaques.1 The pathogenesis is still unclear; in atopic dermatitis, impaired barrier function leading to increased skin water absorption, and hyperhidrosis, cystic fibrosis, or drug-induced increase in sweat salt concentration may play a role.1–6 While there has been a strong association between APK and cystic fibrosis(CF), APK has also been shown to be drug-induced independent of CF history. In this case, the patient has no history of medication,we plan to further investigate whether it is related to cystic fibrosis, as APK may be a skin manifestation of CF.
Most treatment strategies aimed at preventing water exposure, reducing any related hyperkeratosis, and alleviating symptoms have proven ineffective and disappointing results in APK.7 The experience of using Vaseline and/or the use of gloves is still mostly frustrating, as pointed out in our case. In her case, repeated treatment with urea cream did not yield any benefits, and avoiding contact with water in daily work and life was impractical and could cause serious psychological and social problems.7 We observed that the patient’s skin symptoms were relieved in one week of topical pimecrolimus. Mild recurrence occurred after stopping treatment for two months, and the therapeutic effect was good after retreatment that the topical pimecrolimus was perhaps remittive therapy.
As a clinically approved calcineurin inhibitor for atopic dermatitis, the immune mechanism of pimecrolimus is often used for off label therapy, and its efficacy is comparable to that of topical corticosteroids. It is speculated that COX-2 inhibitors induce APK by inhibiting sodium reabsorption in epidermal cells and increasing sodium retention, analogous to renal effects. In a randomized study, calcineurin inhibitors inhibited COX-2 activity, thereby suppressing sodium transport in epidermal cells.8 In the experimental model, calcineurin inhibitors selectively regulate the renal cyclooxygenase subtype COX-1 and more selectively regulate COX-2 dependent prostaglandin synthesis, thereby regulating the homeostasis of keratinocytes.9–11 These mechanisms extending beyond immunomodulation—may elucidate topical pimecrolimus efficacy in APK pathogenesis.
We searched PubMed for eligible articles related to APK from 2015 to 2025 using the following keywords: “Aquagenic palmoplanta keratoderma”; “treatment” and “case report”. After screening, 10 articles meet the eligibility criteria and have been included.9,12–20 Table 1 shows the characteristics of patients and data on treatment and response. Overall, four patients experienced recurrence symptoms or treatment failure. These patients showed slight improvement in symptoms after local application of urea cream, aluminum chloride, Vaseline and intradermal injections botulinum toxin, but relapsed after discontinuation of the medication. Five patients showed improvement in symptoms after receiving urea, oral oxybutynin, and endoscopic thoracic sympathetic nerve examination, but no long-term treatment observation results were mentioned.
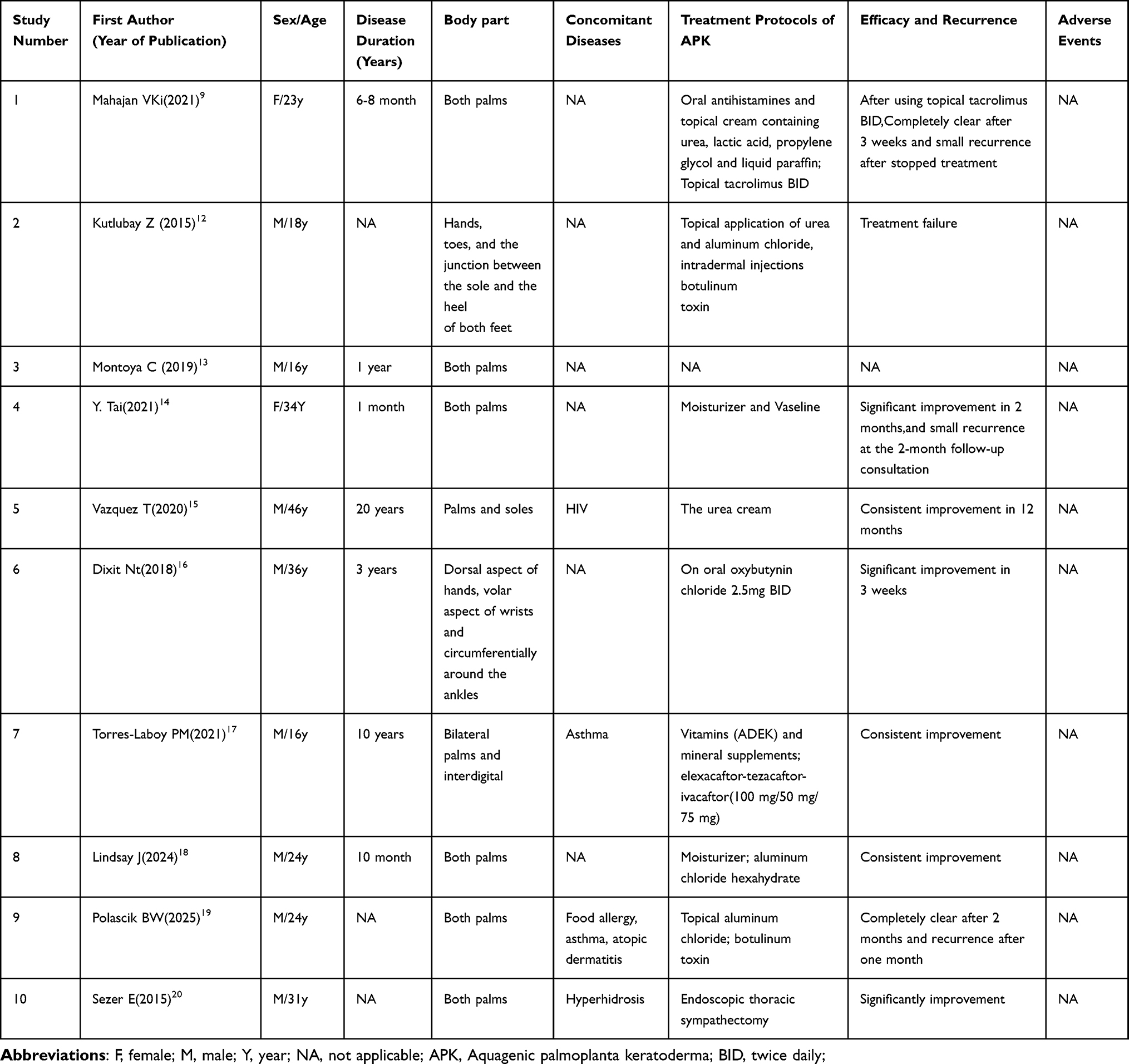 |
Table 1 Treatment in Reported APK Cases |
Although patients usually experience symptoms such as burning, pain, or itching after immersion in water, this patient did not have similar symptoms. As in our case, physical findings typically resolve promptly after water removal. Lesions on the dorsal fingers are rarer than palmar involvement.4,5 Many APK cases may be overlooked clinically without a water contact test.1
In conclusion, we report a case of hand involvement in a healthy female APK patient treated with pimecrolimus. It is worth noting that clinicians use water contact testing as a screening test for suspected APK patients; furthermore skin biopsy and cystic fibrosis transmembrane conductance receptor mutation testing are recommended.
Ethical Statement and Informed Consent
This patient in this manuscript has given written informed consent to publication of her case details. The study was approved by The Second Affiliated Hospital of Zhejiang Chinese Medical University ethical and review board.
Consent Statement
In this study, this patient provided written informed consent for the publication of this case information and accompanying images.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Park L, Khani C, Tamburro J. Aquagenic wrinkling of the palms and the potential role for genetic testing. Pediatr Dermatol. 2012;29(3):237–5. doi:10.1111/j.1525-1470.2011.01609.x
2. Gild R, Clay CD, Morey S. Aquagenic wrinkling of the palms in cystic fibrosis and the cystic fibrosis carrier state: a case–control study. Br J Dermatol. 2010;163(5):1082–1084. doi:10.1111/j.1365-2133.2010.09914.x
3. Seitz CS, Gaigl Z, Bröcker EB, Trautmann A. Painful wrinkles in the bathtub: association with hyperhidrosis and cystic fibrosis. Dermatology. 2008;216(3):222–226. doi:10.1159/000112929
4. Angra D, Angra K, Rodney IJ. Aquagenic palmoplantar keratoderma with dorsal hand involvement in an adolescent female. JAAD Case Rep. 2016;2(3):239–240. doi:10.1016/j.jdcr.2016.05.016
5. Yoon TY, Kim KR, Lee JY, Kim MK. Aquagenic syringeal acrokeratoderma: unusual prominence on the dorsal aspect of fingers? Br J Dermatol. 2008;159(2):486–488. doi:10.1111/j.1365-2133.2008.08633.x
6. Rongioletti F, Tomasini C, Crovato F, Marchesi L. Aquagenic (pseudo) keratoderma: a clinical series with new pathological insights. Br J Dermatol. 2012;167(3):575–582. doi:10.1111/j.1365-2133.2012.11003.x
7. Syed Z, Wanner M, Ibrahimi OA. Aquagenic wrinkling of the palms: a case report and literature review. Dermatology Online J. 2010;16:7. doi:10.5070/D35D57W5ZZ
8. Øzbay LA, Stubbe J, Jespersen B, Jensen BL. The effects of calcineurin inhibitors on prostanoid synthesis: a randomized cross-over study in healthy humans. Transpl Int. 2013;26(2):131–137. PMID: 23190385. doi:10.1111/tri.12004
9. Mahajan VK, Negi R, Thakur P, Kukreja A. Aquagenic wrinkling of the palms: response to topical tacrolimus. Indian Dermatol Online J. 2022;13(3):380–383. doi:10.4103/idoj.idoj_657_21
10. Khuu PT, Duncan KO, Kwan A, Hoyme HE, Bruckner AL. Unilateral aquagenic wrinkling of the palms associated with aspirin intake. Arch Dermatol. 2006;142:1661–1662. doi:10.1001/archderm.142.12.1661
11. Robida AM, Xu K, Ellington ML, Murphy TJ. Cyclosporin A selectively inhibits mitogen-induced cyclooxygenase-2 gene transcription in vascular smooth muscle cells. Mol Pharmacol. 2000;58(4):701–708. doi:10.1124/mol.58.4.701
12. Kutlubay Z, Engin B, Baglam S, Khatib R, Demirkesen C, Aydemir EH. Case report: treatment failure in a case of aquagenic syringeal acrokeratoderma. J Cosmet Laser Ther. 2015;17(4):224–226. doi:10.3109/14764172.2014.1003240
13. Montoya C, Arias LM, Salazar M, Restrepo R. Water-induced dermatosis: aquagenic keratoderma. A case report. Biomedica. 2019;39(2):247–251. English, Spanish. doi:10.7705/biomedica.v39i2.4524
14. Tai Y, Fukumoto T, Oka M, Nishigori C. Frequent handwashing and disinfection: a potential new trigger for aquagenic wrinkling of the palms caused by COVID-19 outbreak. J Eur Acad Dermatol Venereol. 2021;35(1):e9–e10. doi:10.1111/jdv.16906
15. Vazquez T, Zarei M, Herskovitz I, Price A, Villada G, Keri J. Atypical familial aquagenic syringeal acrokeratoderma. J Cutan Pathol. 2020;47(11):991–996. doi:10.1111/cup.13704
16. Dixit N, Sardana K, Tandon S, Singh Y. Atypical aquagenic keratoderma treated with oxybutynin chloride. An Bras Dermatol. 2018;93(2):308–309. doi:10.1590/abd1806-4841.20187262
17. Torres-Laboy PM, Melendez-Montañez JM, De Jesús-Rojas W. Aquagenic wrinkling of the palm: a rare diagnostic clue of cystic fibrosis and the response to CFTR-modulating therapy. Cureus. 2021;13(4):e14425. doi:10.7759/cureus.14425
18. Lindsay J, Incristi AR, Arnett B, Costa M, Chong C. A case of aquagenic syringeal acrokeratoderma in a male patient undergoing treatment with an angiotensin-converting enzyme inhibitor. Cureus. 2024;16(11):e74157. doi:10.7759/cureus.74157
19. Polascik BW, Karklins SP, Johnson MC, Hammert WC, McMichael AJ. Acquired aquagenic syringeal keratoderma following COVID-19 infection. Hand. 2025;20(1):NP12–NP19. doi:10.1177/15589447241233371
20. Sezer E, Durmaz EÖ, Çetin E, Şahin S. Permanent treatment of aquagenic syringeal acrokeratoderma with endoscopic thoracic sympathectomy. Indian J Dermatol Venereol Leprol. 2015;81(6):648–650. doi:10.4103/0378-6323.168331
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.