Back to Journals » Drug Design, Development and Therapy » Volume 19
Applying the Lasso Model to Identify Risk Factors for Piperacillin-Tazobactam-Induced Leukopenia
Authors Liu J, Yuan X ![]() , Liu X
, Liu X ![]() , Liu L
, Liu L ![]() , Wen L, Zheng F
, Wen L, Zheng F
Received 2 June 2025
Accepted for publication 18 November 2025
Published 5 December 2025 Volume 2025:19 Pages 10765—10773
DOI https://doi.org/10.2147/DDDT.S544195
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Jiheng Liu,1,* Xuefeng Yuan,2,* Xiaohui Liu,3 Lihua Liu,4 Long Wen,5 Fang Zheng6
1Department of Hematology & Oncology, The First Hospital of Changsha (The Affiliated Changsha Hospital of Xiangya School of Medicine, Central South University), Changsha, Hunan, People’s Republic of China; 2Department of Nosocomial Infection Management, The First Hospital of Changsha (The Affiliated Changsha Hospital of Xiangya School of Medicine, Central South University), Changsha, Hunan, People’s Republic of China; 3Department of Pharmacy, The First Hospital of Changsha (The Affiliated Changsha Hospital of Xiangya School of Medicine, Central South University), Changsha, Hunan, People’s Republic of China; 4Department of Pharmacy, The Third Hospital of Changsha, The Affiliated Changsha Hospital of Hunan University, Changsha, Hunan, People’s Republic of China; 5Department of Respiratory and Critical Care Medicine, The First Hospital of Changsha(The Affiliated Changsha Hospital of Xiangya School of Medicine, Central South University), Changsha, Hunan, People’s Republic of China; 6Department of Infectious Diseases, The First Hospital of Changsha (The Affiliated Changsha Hospital of Xiangya School of Medicine, Central South University), Changsha, Hunan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaohui Liu, Department of Pharmacy, The First Hospital of Changsha (The Affiliated Changsha Hospital of Xiangya School of Medicine, Central South University), Changsha, Hunan, People’s Republic of China, Tel +86 731 84667573, Fax +86 731 84667680, Email [email protected]
Objective: We conducted a retrospective study to investigate the prevalence, clinical characteristics, and risk factors for leukopenia in patients receiving piperacillin-tazobactam (TZP) therapy.
Methods: This observational study was conducted from January to December 2022 at a tertiary general hospital in China. All patients over 18 years old who received TZP for more than 48 hours were included. Patients were stratified into adverse drug reactions (ADR) (n=41, TZP-induced leukopenia or neutropenia) and Control (n=8014, no ADR) groups. To balance covariates, 1:2 propensity score matching (PSM) was applied using age, infection type, gender, and comorbidity index, resulting in 82 matched controls for comparative analysis. We employed least absolute shrinkage and selection operator (LASSO) regression to identify risk factors for TZP-induced leukopenia.
Results: A total of 123 patients were analyzed. The average duration of treatment was 10 days (IQR: 7, 19). In 41 patients with TZP-induced leukopenia, the mean onset time was 17.7 ± 6.6 days. Among these, 29 (70.7%) developed neutropenia (including 1 severe case), and 3 (7.3%) had drug-induced fever. Therapy duration (odds ratio (OR) = 1.53, 95% confidence interval (CI) 1.32– 1.76) was identified as a significant influencing factor for leukopenia caused by TZP through the LASSO regression screening process.
Conclusion: Clinicians should recognize the potential association between TZP administration and leukopenia. Routine hematologic monitoring should emphasize leukocyte trends to assess both therapeutic response and drug safety.
Keywords: piperacillin-tazobactam, TZP, leukopenia, neutropenia, adverse effect, least absolute shrinkage and selection operator, LASSO
Introduction
Piperacillin-tazobactam (TZP) is a combination therapy consisting of a semisynthetic urea-penicillin and a β-lactamase inhibitor, boasting broad-spectrum antimicrobial activity. It is efficacious in treating a variety of infections caused by β-lactamase-producing Gram-positive and Gram-negative bacteria, as well as anaerobes. These infections include pneumonia, urinary tract infections, gynecological and pelvic infections, abdominal infections, skin and soft tissue infections, bone and joint infections, sepsis, and mixed infections resulting from both aerobic and anaerobic bacteria.1–3 A 2024 meta-analysis incorporating 39 randomised controlled trials suggests that TZP, when used as empirical antibiotic therapy for adults with non-ventilator-associated hospital-acquired pneumonia targeting Pseudomonas aeruginosa and other gram-negative bacteria, may demonstrate superior efficacy in reducing treatment failure.4 In the context of clinical practice, TZP is widely used in hospitals at all levels across China. As demonstrated by the statistical data of 2023, the sales volume of TZP in China’s graded hospitals has reached 7.34 billion Yuan, thus surpassing cefoperazone-sulbactam in usage.5
The most frequently encountered adverse reactions to TZP include gastrointestinal disturbances and skin reactions, along with additional adverse effects such as leukopenia, neurotoxicity, hepatotoxicity, electrolyte imbalances, acid-base disturbances, bleeding disorders, as well as hematologic adverse effects such as neutropenia, leukopenia, thrombocytopenia, and hemolytic anemia.6 Case reports on post-market adverse drug reactions (ADR) of TZP,7,8 in combination with the results of retrospective studies, have pointed to leukopenia as being linked to bone marrow suppression,9,10 typically occurring more than ten days after the initiation of TZP therapy.
ln this context, we conducted a retrospective analysis leveraging the propensity score matching analysis and Lasso regression models to assess the likelihood of leukopenia linked to TZP administration and to identify key clinical indicators that can predict an increased risk of these adverse events during treatment, with the ultimate objective of developing a risk prediction model.
Materials and Methods
Patients
This retrospective, single-center study was conducted at the First Hospital of Changsha, a tertiary general hospital with 1,800 beds, situated in Changsha, Hunan Province—a pivotal city within the Yangtze River Economic Belt in China, boasting a population of approximately 10.5 million inhabitants. The study covered a one-year period, from January to December 2022. This study was conducted in accordance with all relevant tenets of the Declaration of Helsinki. This study was approved by the Medical Ethics Committee of the First Hospital of Changsha (China) (Approval Number: 2023lks[ly]122). In light of the retrospective nature of the study and the utilisation of anonymized clinical data (with no personally identifiable information), the Medical Ethics Committee explicitly waived the requirement for written informed consent. The data were extracted from routine clinical records and transferred to an anonymised, password-protected database. This database was securely maintained and did not contain any personally identifiable information.
Inclusion and Exclusion Criteria
A comprehensive search of the hospital information system was conducted, resulting in the retrieval of the medical records of all patients who received treatment with TZP during their respective hospitalizations from January to December 2022. The inclusion criteria for this study were: (1) age ≥18 years; (2) TZP treatment duration >48 hours; (3) the completion of routine blood tests and other relevant index measurements is to be conducted prior to, during, and following TZP treatment. The exclusion criteria were as follows: (1) patients with hematological diseases (such as hematological malignancies, idiopathic thrombocytopenia, hemophilia, etc.); (2) patients using systemic steroid therapy or chemotherapy within the last 3 months; (3) patients with leukopenia (leukocyte count of < 4×109/L) and neutropenia (neutrophil count of < 2×109/L); and (4) the clinical data of the patients were incomplete. If the interval between two instances of TZP therapy surpassed one month, those instances were assessed separately. In this study, we defined two separate patient populations: the ADR group, comprising 41 patients who underwent TZP and subsequently experienced leukopenia or neutropenia, and the Control group, encompassing 8014 patients who underwent TZP but did not encounter any adverse drug reactions. To ensure comparable demographics and clinical characteristics between the groups, we employed 1:2 propensity score matching, considering factors such as age, infection type, gender, and comorbidity index. Ultimately, we identified and selected 82 patients from the Control group for the purpose of this comparison. Refer to Figure 1 for the flowchart outlining the case collection process.
 |
Figure 1 Case collection process diagram. |
Data Collection
We conducted a cross-sectional study to explore the differences in the occurrence of adverse drug reactions among patients with different demographic characteristics, disease characteristics and drug treatment regimens. Demographic information (age, gender), laboratory and clinical data (including comorbidity status, age-adjusted Charlson Comorbidity Index (ACCI), estimated glomerular filtration rate (eGFR) calculated using the Cockcroft–Gault formula, site and type of infection), as well as medication details (dosage, duration of treatment, concomitant medications, and adverse reactions during TZP therapy) were gathered through the hospital information system. During TZP treatment, We collected clinical laboratory test results at various time points, including at baseline, every 2 days during administration, and at any time point within 7 days post-discontinuation. According to the package insert of TZP, the usual daily dose is 4.5 g administered every 6 or 8 hours. For patients with renal insufficiency, the dosage should be adjusted to 4.5g every 8 hours for those with an creatinine clearance of 20mL/min to 40mL/min, and further reduced to 4.5g every 12 hours for those with severe renal insufficiency (creatinine clearance < 20mL/min).11 We defined the total therapeutic dose as the cumulative amount of TZP administered continuously throughout one treatment cycle, and leukopenia as an absolute leukocyte count below 4×109/L, with neutropenia as an absolute neutrophil count below 2×109/L, and severe neutropenia as an absolute neutrophil count below 0.5×109/L.9 Clinical pharmacists examined the collected records individually and assessed the causality of adverse drug reactions based on the World Health Organization-Uppsala Monitoring Centre (WHO-UMC) system.12
Statistical Analysis
The data were initially recorded in Microsoft Word and subsequently summarised in Microsoft Excel to create a database. Data were initially selected for 32 variables, and after inclusion and exclusion, 17 variables were used for further analysis. Following the auditing process, Data were analyzed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Categorical variables were expressed as frequency (percentage), with comparisons between unordered categorical variable groups using either the Chi-square test or Fisher’s exact test; Ordered categorical variables (ordinal variables) were compared using the rank-sum test. Continuous variables undergo normality testing using the Kolmogorov–Smirnov method. If they followed a normal distribution, they were described as mean ± standard deviation (±s), with comparisons between groups using the t-test. If they did not follow a normal distribution, they were described using median (interquartile range) [M(P25, P75)], with comparisons between groups using the Mann–Whitney U-test. All p values were two-tail and p < 0.05 was considered significant.
R version 4.4.2 “glmnet” package (R Foundation for Statistical Computing, Vienna, Austria) was used to build the LASSO prediction model. At the traditional statistical analysis level, we replaced the columns with continuous values in the dataset with the average value of the remaining values in the column. If the missing value came from the classification column (string or value), we replaced the missing value with the most common category. For data variables with longitudinal behavior (time variables in this study), the last valid observation value was used to fill in the missing value. In training set, LASSO regression was used to screen variables. We utilized tenfold cross-validation to select the penalty term, λ. The binomial deviance was computed for the test data as measures of the predictive performance of the fitted models. Logistic regression analysis was used to calculate the odds ratio (OR) of variables.
Results
Demographics and Clinical Characteristics
Among a total of 8055 patients who received TZP treatment, 41 (0.5%) developed leukopenia. A total of 123 patients who received TZP at the First Hospital of Changsha were identified as eligible for inclusion in the study. The demographic and clinical characteristics of all patients enrolled in the study, presented as median [M (P25, P75)] or mean (± SD), are summarized in Table 1. There were more males (61.0%) than females, with a median age of 61 years (IQR: 53, 69) and a mean weight of 58.53 ± 9.78 kg. Additionally, the Age-adjusted Charlson Comorbidity Index was 5 (IQR: 3, 8). The most common site of infection was lower respiratory tract (50%), followed by abdominal (30.8%) and skin and soft tissues (12.6%). The average duration of treatment for 123 patients on TZP was 10 days (IQR: 7, 19).
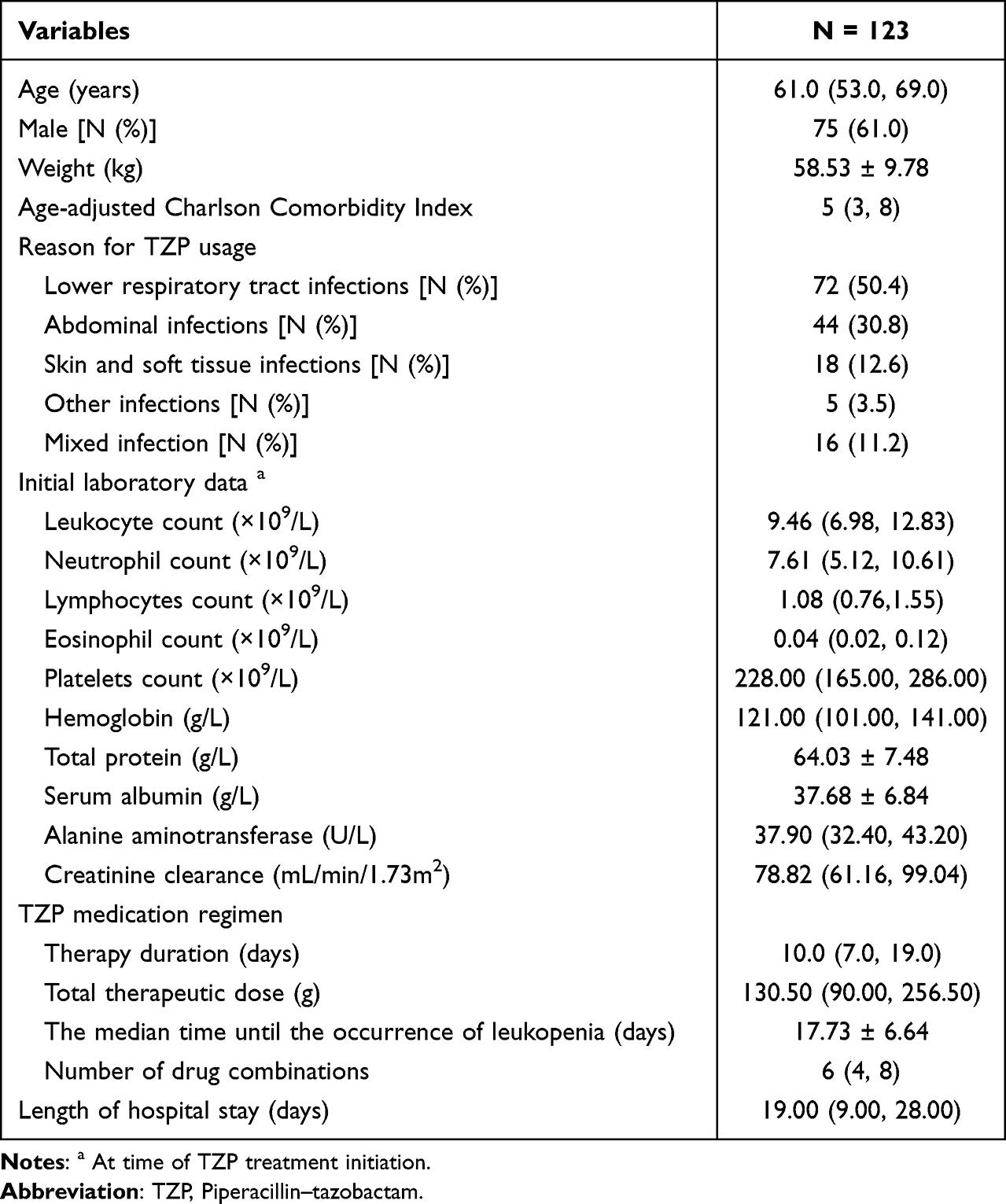 |
Table 1 Demographic and Clinical Data for All Patients Included in the Study [ |

Among the 41 patients who developed leukopenia following treatment with TZP, 29 cases developed neutropenia, including one case of severe neutropenia. Additionally, 3 cases were complicated by drug-induced fever. Among these 41 patients, 18 cases exhibited a decreased lymphocyte count. Moreover, 11 cases had concurrent leukopenia and neutropenia, while 7 cases had a normal neutrophil count. The mean time to onset of leukopenia was 17.73 ± 6.64 days. In these 41 patients, the white blood cell count and absolute neutrophil count returned to normal ranges following discontinuation of the medication. Lastly, the average length of hospital stay for the patients was 19 days (IQR: 9, 28).
We have identified 16 factors associated with TZP-induced leukopenia. Among these factors, statistically significant differences (P < 0.05) were observed in initial leukocyte count, initial neutrophil count, initial albumin levels, duration of TZP therapy, total TZP dose, number of drug combinations, and length of hospital stay between the ADR group and the Control group (Table 2). Specifically, compared to patients without adverse reactions, those in the ADR group exhibited lower leukocyte counts, neutrophil counts, and albumin levels prior to treatment. Additionally, they had longer durations of TZP therapy and hospital stays, as well as higher total TZP doses and more number of drug combinations.
 |
Table 2 Comparison of the Differences Between the Group Experiencing Leukopenia and the Group Without Adverse Drug Reactions After TZP Exposure [ |

Establishment of the LASSO Regression Prediction Model
In the training sample, TZP-induced neutropenia was used as the dependent variable. We utilized the Least Absolute Shrinkage and Selection Operator (LASSO) regression algorithm to screen the variables and determined the optimal lambda (λ) value through 10-fold cross-validation (as illustrated in Figure 2). Figure 2 features two dashed lines, representing λmin and λ1se, respectively. λmin denotes the λ value at which the model error is minimized, while λ1se indicates the range of model error within one standard error of λ. At this juncture, the fit was ensured by incorporating the minimal number of variables necessary to achieve the most streamlined prediction model. We presented the estimated coefficients from a logistic LASSO regression analysis, the relationship between various factors (length of stay, therapy duration, accumulated dose, number of drug combinations, creatinine clearance before treatment, leukocyte count and neutrophil count before treatment) and neutropenia induced by TZP was examined. Among these factors, therapy duration (odds ratio (OR) = 1.53, 95% confidence interval (CI) 1.32–1.76) was identified as a significant influencing factor for leukopenia caused by TZP through the LASSO regression screening process. The estimated coefficient for therapy duration is 0.1047 (with bootstrap standard error).
 |
Figure 2 LASSO Regression and Five-Fold Cross-Validation for Predictor Screening (A): Coefficient Plot from LASSO Regression. The plot shows the coefficients of 17 variables as a function of the log (λ) parameter in LASSO regression. The horizontal axis represents the log (λ) value, and the vertical axis represents the coefficients of the independent variables. As λ increases, the coefficients of the variables are gradually compressed to zero. Variables that become zero later are considered more important for the model.(B): Ten-Fold Cross-Validation for LASSO Regression. The plot shows the binomial deviance (or mean squared error) of the LASSO regression model as a function of log (λ).The two vertical dashed lines represent: The left dashed line indicates the value of log (λ) that minimizes the model error. The right dashed line indicates the value of log (λ) where the model error is within one standard error of the minimum. The red line represents the binomial deviance, and the shaded area represents the standard error of the cross-validation. |
Discussion
In our retrospective study of 8055 patients, TZP therapy was induced with leukopenia in 41 cases (0.51%) and neutropenia in 29 cases (0.36%), findings that align with a meta-analysis of 13,816 non-neutropenic fever trial participants where piperacillin-related neutropenia occurred in only 0.04% (5 cases),13 collectively underscoring the rare incidence of these hematologic adverse events across diverse clinical contexts. Despite the relatively low incidence, vigilance remains critical regarding the potential risks of secondary neutropenia and drug fever, necessitating proactive monitoring and early intervention strategies.
Our findings indicating that the median duration until the onset of leukopenia following medication administration was 17.73 ± 6.64 days, which is consistent with the timeframe reported in a review article.14 The recovery of the white blood cell and neutrophil counts following treatment discontinuation provides further evidence of a causal relationship between TZP exposure and leukopenia, aligning with findings from prior studies.9,10,13,14
Possible Mechanisms of Drug Adverse Reactions
The underlying mechanisms for TZP-induced leukopenia or neutropenia may involve bone marrow suppression or immune-mediated processes.14–17 In relation to bone marrow-related factors, piperacillin, a component of TZP, has been observed to induce a cessation in the proliferation of myeloid cells. In two cases of neutropenia following TZP treatment, bone marrow aspirate examinations were conducted. The results obtained demonstrated granulocytic maturation arrest, thus providing further evidence for the involvement of bone marrow-associated mechanisms in TZP-induced neutropenia.18,19 Such bone marrow suppression can directly lead to a decline in both neutrophils and overall WBC counts, given that neutrophils constitute a major part of WBCs. In addition to factors related to bone marrow, immune-mediated reactions have been identified as a potential mechanism leading to TZP-induced leukopenia or neutropenia. Such immune-mediated reactions are categorised as immune-mediated hematological adverse event, with an incidence rate of approximately 1–4 cases per million people per year.14,17 Immune responses triggered by TZP can result in the destruction of hematopoietic progenitor cells in the bone marrow or circulating blood cells. This can cause a generalized decrease in WBCs, including neutrophils and lymphocytes.14,17 In our study, 29 out of the 41 patients with leukopenia developed neutropenia, and 18 showed a decreased lymphocyte count. The occurrence of decreased neutrophil and lymphocyte counts in some patients indicates an immune-mediated attack on multiple types of white blood cells. In order to diagnose TZP-induced leukopenia, a comprehensive evaluation of bone marrow function, immune markers, and drug-specific antibody tests may be necessary.
Risk Factors of TZP-Induced Leukopenia or Neutropenia
In this study, prolonged TZP therapy (ie, therapy duration) was identified as the sole independent predictor for the incidence of leukopenia or neutropenia, with a median latency of above 17 days from treatment initiation. A recent systematic review with meta-analysis demonstrated that TZP-induced neutropenia typically manifests approximately 14 days post-therapy initiation.14 Early retrospective studies demonstrated a significant inverse correlation between absolute neutrophil count at treatment completion and cumulative piperacillin exposure.20 In a recent retrospective study, multivariate analysis identified four independent risk factors for leukopenia: lower Charlson Comorbidity Index (CCI) score, reduced baseline leukocyte count, concurrent use of TZP with another antibiotic agent, and prolonged total duration of TZP therapy.9 Regarding combination therapy, early retrospective studies identified concurrent antibiotic use as a risk factor for neutropenia development post-TZP exposure,18 while recent retrospective analyses have similarly implicated this association in leukopenia occurrence.9
In the retrospective cohort analysis conducted, it was determined that, despite the ADR group exhibiting lower baseline leukocyte counts, neutrophil counts, and albumin levels in comparison to the control group. In addition, Lasso regression analysis did not support the hypothesis that these variables function as risk factors. From a theoretical standpoint, baseline leukocyte and neutrophil counts are regarded as pivotal indicators of the body’s immune status. The hypothesis that lower baseline levels of these counts may signify a relatively weaker immune system is one that merits further investigation. Furthermore, low albumin levels may be indicative of poor nutritional status or impaired liver synthetic function, which, in turn, may have a detrimental effect on the body’s drug metabolism and tolerance. In clinical practice, the determination of potential critical thresholds for these parameters may be of great significance. Furthermore, despite observing a statistically significant difference in the number of drug combinations between the leukopenia occurrence group and the control cohort following TZP therapy, Lasso regression analysis did not retain this variable in the final model, suggesting potential confounding in univariate comparisons. This discrepancy may be attributable to the restricted frequency of concomitant antibiotic utilisation observed in the study population.
Advantages of LASSO Regression in the Analysis of Adverse Drug Reactions
Considering the substantial influence of ADR on clinical outcomes and treatment adherence, to rigorously evaluate the association between TZP exposure and leukopenia development, we employed LASSO, which addresses multicollinearity.21,22 This approach enabled simultaneous variable selection and coefficient estimation while controlling for established clinical risk factors for leukopenia (eg, baseline neutrophil count, renal dysfunction). Through 10-fold cross-validated λ selection, the LASSO model automatically eliminated non-predictive variables, retaining only TZP therapy duration (OR 1.53, 95% CI 1.32–1.76) as independent predictors in the final parsimonious model. To the best of our knowledge, this represents the first pharmacoepidemiological investigation to apply LASSO for simultaneous evaluation of both the TZP therapy and the collective impact of clinical risk factors on leukopenia incidence. This methodological advancement introduces a robust analytical paradigm leveraging LASSO to deconvolute multifactorial pathways contributing to adverse drug reactions, enabling precise risk stratification through simultaneous variable selection, confounder control, and effect size estimation. By integrating penalized regression with cross-validated feature selection, this framework surpasses traditional multivariate approaches in disentangling collinear risk factors (eg, drug exposure metrics, comorbidities) while maintaining interpretability through retained variable coefficients.
Limitations
This study has several methodological limitations requiring cautious interpretation. First, the retrospective observational design limited comprehensive evaluation of all potential influencing factors associated with leukopenia development, particularly regarding specific pharmacotherapies and stratified analyses of baseline leukocyte thresholds. Second, clinical heterogeneity within the inpatient cohort—encompassing diverse departments, comorbidity profiles, and treatment protocols—introduced unmeasured variability that may have constrained statistical precision. Third, the single-center derivation framework restricts generalizability, necessitating external validation in prospective multicenter settings. Notably, while this analysis represents the larger cohort examined to date (n=8055) and successfully identified therapy duration as risk factor for TZP-induced leukopenia, the observed associations require confirmation through randomized controlled trials. Such trials should incorporate predefined stratification by baseline leukocyte levels and employ standardized hematotoxicity grading criteria (eg, NCI-CTCAE v5.0) to enhance clinical applicability. Despite these constraints, our findings provide critical methodological groundwork for developing predictive risk models in antibiotic-induced hematotoxicity research.
Conclusions
Leukopenia induced with TZP therapy remains a rare adverse drug reaction with incompletely elucidated pathophysiology. The analysis revealed that cumulative exposure duration is an independent modifiable risk factor for TZP-induced leukopenia. In clinical practice, heightened vigilance is required when prescribing TZP courses exceeding 14 days, especially for patients with preexisting hematologic vulnerabilities. Monitoring alterations in WBC, neutrophil, and lymphocyte counts over time during TZP treatment can also provide significant information for the early detection and management of these adverse reactions.
Acknowledgments
We would like to express our gratitude to Wenxin Yiyan (ERNIE Bot version 4.5) for its valuable assistance in enhancing the readability and fluency of the language in this article. The AI tool’s contributions have been instrumental in improving the overall quality of our manuscript. We maintain full responsibility for the content and accuracy of the work presented under our names.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Science and Health Joint Project of the Natural Science Foundation of Hunan Province (No. 2021JJ70056), the Project of Hunan Provincial Health Commission (No.202103020580, No.D202303028856) and Natural Science Foundation of Hunan Province (NO.2023JJ60067, No.2023JJ60396).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Paul M, Carrara E, Retamar P, et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine). Clin Microbiol Infect. 2022;28(4):521–547. doi:10.1016/j.cmi.2021.11.025
2. Tamma PD, Heil EL, Justo JA, Mathers AJ, Satlin MJ, Bonomo RA. Infectious Diseases Society of America 2024 guidance on the treatment of antimicrobial-resistant gram-negative infections. Clin Infect Dis. 2024;ciae403. doi:10.1093/cid/ciae403
3. Sy CL, Chen PY, Cheng CW, et al. Recommendations and guidelines for the treatment of infections due to multidrug resistant organisms. J Microbiol Immunol Infect. 2022;55(3):359–386. doi:10.1016/j.jmii.2022.02.001
4. Ghadimi M, Siemieniuk RAC, Guyatt G, et al. Empiric antibiotic regimens in adults with non-ventilator-associated hospital-acquired pneumonia: a systematic review and network meta-analysis of randomized controlled trials. Clin Microbiol Infect. 2024;30(11):1351–1363. doi:10.1016/j.cmi.2024
5. The billion dollar market has undergone changes, with 7.3 billion varieties experiencing two consecutive jumps, and the price of centralized procurement has dropped by another 55% (attached ranking). Available from: https://finance.sina.com.cn/stock/med/2024-05-14/doc-inavewzh1231569.shtml.
6. Perry CM, Markham A. Piperacillin/tazobactam: an updated review of its use in the treatment of bacterial infections. Drugs. 1999;57(5):805–843. doi:10.2165/00003495-199957050-00017
7. Gupta A, Bastiampillai T, Moore B. Clozapine or antibiotic induced neutropenia? Austr Psychiatry. 2016;24(4):400. doi:10.1177/1039856216647253
8. Darwiche D, Iskandar K, Azar R, Hallit R, Hallit S. piperacillin–tazobactam-induced neutropenia: a case report. J Med Cases. 2017;8(9):280–282. doi:10.14740/jmc2889w
9. Aysun B, Serap Ş-Y, Seniha B, et al. Hematologic adverse effects of prolonged piperacillin-tazobactam use in adults. Turk J Haematol. 2018;35
10. Lemieux P, Grégoire JP, Thibeault R, Bergeron L. Higher risk of neutropenia associated with piperacillin-tazobactam compared with ticarcillin-clavulanate in children. Clin Infect Dis. 2015;60(2):203–207. Epub 2014 Oct 9. PMID: 25301207. doi:10.1093/cid/ciu780
11. Pfizer Incorporated. TAZOCIN (Piperacillin-tazobactam) full prescribing information. Available from: https://labeling.pfizer.com/ShowLabeling.aspx?id=12876.
12. Behera SK, Das S, Xavier AS, Velupula S, Sandhiya S. Comparison of different methods for causality assessment of adverse drug reactions. Int J Clin Pharm. 2018;40:903–910. doi:10.1007/s11096-018-0694-9
13. Scheetz MH, Mckoy JM, Parada JP, et al. Systematic review of piperacillin-induced neutropenia. Drug Safety. 2007;30(4):295–306. doi:10.2165/00002018-200730040-00002
14. Wang Q, He Z, Wu X, et al. Hematologic adverse effects induced by piperacillin–tazobactam: a systematic review of case reports. Int J Clin Pharm. 2020;42:1026–1035. doi:10.1007/s11096-020-01071-8
15. Wu Y, Wu Y, Guo G, Zeng J, Liu Y, Wu Y. Piperacillin-tazobactam induced immune hemolytic anemia led to increased renal impairment and eventual death from multiple organ failure in a patient with hypertensive nephropathy: case report and literature review. BMC Nephrol. 2023;24(1):173. doi:10.1186/s12882-023-03235-w
16. Arndt PA. Drug-induced immune hemolytic anemia: the last 30 years of changes. Immunohematology. 2014;30(2):44–54. doi:10.21307/immunohematology-2019-098
17. Gerhardy B, Bowler S. Piperacillin-tazobactam-induced haemolytic anaemia after multiple courses of therapy. Intern Med J. 2021;51(3):458. doi:10.1111/imj.15243
18. Khan F. Severe neutropenia secondary to piperacillin/tazobactam therapy. Indian J Pharmacol. 2005;37:192–193. doi:10.4103/0253-7613.16222
19. Ruiz-Irastorza G, Barreiro G, Aguirre C. Reversible bone marrow depression by high-dose piperacillin/tazobactam. Br J Haematol. 1996;95:611–612. doi:10.1046/j.1365-2141.1996.d01-1952.x
20. Peralta FG, Sánchez MB, Roíz MP, Pena MA, Tejero MA, Arjona R. Incidence of neutropenia during treatment of bone-related infections with piperacillin-tazobactam. Clinl Infect Dis. 2003;37(11):1568–1572. doi:10.1086/379519
21. Wang Z, Sun X, Wang B, Shi S, Chen X. Lasso-Logistic regression model for the identification of serum biomarkers of neurotoxicity induced by strychnos alkaloids. Toxicol Mech Methods. 2023;33(1):65–72. doi:10.1080/15376516.2022.2086088
22. Liu Y, Shen Y, Wei B. The Clinical Risk factors of adenovirus pneumonia in children based on the logistic regression model: correlation with lactate dehydrogenase. Int J Clin Pract. 2022;2022:3001013. doi:10.1155/2022/3001013
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.