Back to Journals » Patient Preference and Adherence » Volume 20
Application of Positional Nursing Combined with Positive Suggestion in Patients Undergoing Sedated Gastroscopy
Received 6 November 2025
Accepted for publication 5 February 2026
Published 23 March 2026 Volume 2026:20 579630
DOI https://doi.org/10.2147/PPA.S579630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Liying Mu,1 Yuanshi Wang,2 Jinyu Duan2
1Endoscopy Center, Beihua University Affiliated Hospital, Jilin, 132000, People’s Republic of China; 2Department of Gastroenterology, Beihua University Affiliated Hospital, Jilin, 132000, People’s Republic of China
Correspondence: Yuanshi Wang, Email [email protected]
Purpose: To investigate the effects of positional nursing combined with positive suggestions on anxiety, procedural outcomes, and patient comfort in patients undergoing painless gastroscopy.
Patients and Methods: This retrospective cohort study enrolled 153 patients undergoing sedated gastroscopy between March 2024 and August 2025. Patients were assigned to the conventional nursing group (n=73, March–October 2024) or the comprehensive nursing group (n=80, November 2024–August 2025). The comprehensive group received individualized positioning optimization and standardized positive psychological suggestions. Primary outcomes included State-Trait Anxiety Inventory-State subscale (STAI-S), examination success rate, examination duration, and General Comfort Questionnaire (GCQ). Secondary outcomes included hemodynamic stability, adverse events, recovery time, and patient satisfaction.
Results: Baseline characteristics were comparable between groups. The comprehensive nursing group demonstrated significantly lower STAI-S scores (43.23± 7.68 vs 48.67± 8.45, P < 0.001) and shorter examination duration (6.54± 1.62 min vs 7.23± 1.87 min, P =0.016). GCQ scores were significantly higher in the comprehensive group (P < 0.001). The comprehensive group maintained better intra-procedural hemodynamic stability with lower heart rates (P =0.002), higher oxygen saturation (P < 0.001), and higher blood pressure levels (systolic BP: P =0.020; diastolic BP: P =0.008). Comprehensive group had lower overall adverse event incidence, shorter recovery time and higher modified Patient Satisfaction Questionnaire scores (modified PSQ-18) (all P < 0.05).
Conclusion: Positional nursing combined with positive suggestion may help reduce pre-procedural anxiety, improve hemodynamic stability, decrease adverse events, and enhance patient comfort and satisfaction in painless gastroscopy. This non-pharmacological intervention shows promise for integration into routine endoscopy nursing protocols.
Keywords: gastroscopy, patient positioning, psychological intervention, anxiety, nursing care
Introduction
Gastroscopy remains the gold standard diagnostic procedure for upper gastrointestinal disorders, with millions of examinations performed annually worldwide.1 The introduction of sedation-based sedated gastroscopy has substantially improved patient tolerance and procedural acceptance compared to conventional non-sedation examination.2 Despite advances in anesthetic techniques and endoscopic equipment, patients undergoing sedated gastroscopy frequently experience procedural anxiety, discomfort, and suboptimal cooperation, which may compromise examination quality and increase sedation requirements.3
Pre-procedural anxiety affects approximately 60–80% of patients scheduled for gastrointestinal endoscopy.4 This psychological distress stems from fear of choking, pain anticipation, concerns about sedation safety, and uncertainty regarding potential diagnoses. Heightened anxiety triggers sympathetic nervous system activation, manifesting as elevated heart rate, increased blood pressure, and enhanced muscle tension.5 These physiological responses not only intensify patient discomfort but also elevate anesthetic medication requirements and prolong recovery time.6 The interplay between psychological stress and physical tension creates a cycle wherein anxiety amplifies perceived discomfort, further compromising patient cooperation during critical procedural moments.
Patient positioning during endoscopic procedures significantly influences examination success and patient comfort. The left lateral decubitus position, widely adopted for gastroscopy, facilitates instrument passage through the esophagus and provides optimal visualization of gastric structures.7 However, standard positioning protocols often overlook individual anatomical variations and comfort preferences. Poor positioning may result in neck strain, airway compromise, and increased patient restlessness during sedation.8 Recent evidence suggests that optimized positional adjustments—including individualized head elevation, cervical alignment, and limb support—can reduce procedural complications and enhance patient comfort.9 Despite these findings, standardized approaches to position optimization remain underutilized in routine clinical practice.
Psychological interventions have gained recognition as valuable adjuncts to procedural sedation in various medical settings. Positive suggestion, rooted in principles of cognitive-behavioral therapy, involves delivering reassuring verbal cues that reshape patients’ cognitive appraisal of threatening situations.10 Studies in surgical and procedural contexts demonstrate that positive verbal guidance reduces anxiety, diminishes pain perception, and improves patient satisfaction.11,12 The neurobiological mechanisms underlying these effects involve modulation of the limbic system and prefrontal cortex, brain regions governing emotional processing and pain perception.13 By redirecting attention away from fear-inducing stimuli and fostering a sense of safety, positive suggestion may attenuate stress responses and facilitate smoother procedural experiences.
Despite growing interest in non-pharmacological interventions for endoscopic procedures, research examining combined positional and psychological approaches remains limited. Most existing studies have evaluated positioning techniques or psychological support in isolation, without investigating their potential synergistic effects.14,15 The few studies that have explored combined interventions often lacked standardized protocols or focused on different patient populations, limiting generalizability to sedated gastroscopy settings. Furthermore, previous research has predominantly relied on single outcome measures such as anxiety scores or sedation dosages, without comprehensively assessing multiple dimensions of procedural quality including examination success rates, physiological stability, patient comfort, and satisfaction.16
This retrospective study addresses these gaps by investigating the effects of combined positional nursing and positive suggestion on patients undergoing painless gastroscopy. We will explore the impact of incorporating positional nursing and positive suggestions into endoscopy procedures, compared to traditional approaches, on various aspects of patient experience during sedated gastroscopy.
Methods
Study Design and Participants
A retrospective cohort study was conducted at the Endoscopy Center of Beihua University Affiliated Hospital between March 2024 and August 2025. Patients scheduled for sedated gastroscopy were sequentially assigned to two groups based on the nursing protocol implemented during their hospitalization period. The conventional nursing group (n=73) received standard care between March and October 2024, while the comprehensive nursing group (n=80) received positional nursing combined with positive suggestion from November 2024 to August 2025 (Figure 1). The study protocol was approved by the hospital’s Institutional Review Board (approval number: 20240081).
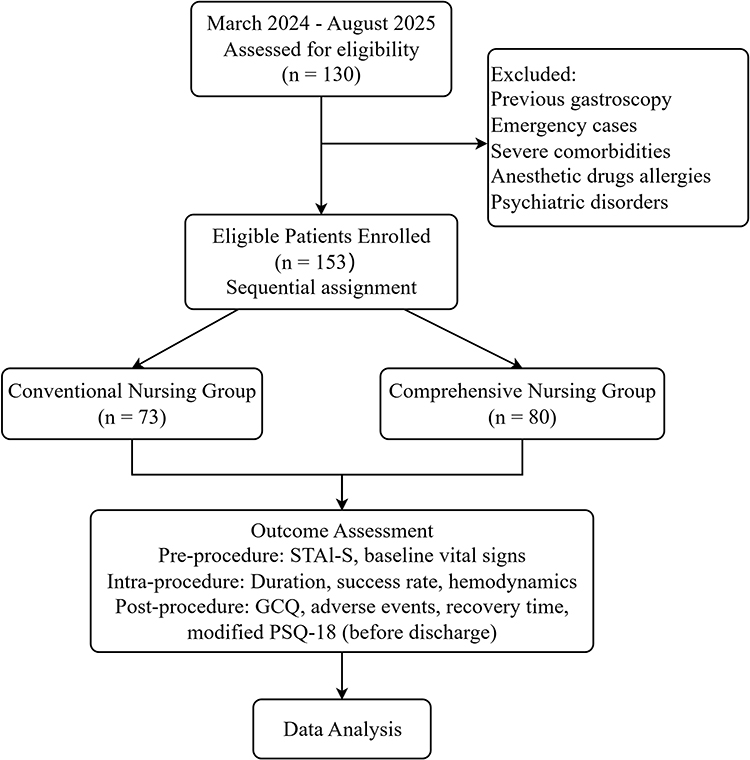 |
Figure 1 Study Flow. Workflow for patient screening, grouping, intervention, and outcome assessment involving 153 patients undergoing painless gastroscopy. Abbreviations: STAI-S, State-Trait Anxiety Inventory-State subscale; GCQ, General Comfort Questionnaire; Modified PSQ-18, Modified Patient Satisfaction Questionnaire. |
Patients were included if they met the following criteria: age 18–70 years; scheduled for sedated gastroscopy under propofol; American Society of Anesthesiologists physical status classification I–II; ability to communicate effectively and complete questionnaires. Exclusion criteria included: previous gastroscopy experience within the past year; emergency examinations; severe cardiopulmonary disease (New York Heart Association class III–IV or chronic obstructive pulmonary disease requiring home oxygen); known allergies to propofol; psychiatric disorders or cognitive impairment affecting comprehension; current use of anxiolytic medications or antidepressants.
Treatment Strategies
The standardized endoscopic equipment used is OLYMPUS (EVIS LUCERA-ELITE-CV-290, GIF-H290Z). All patients in both groups received standardized pre-procedural preparation and anesthetic management. One day before the examination, patients received a written information sheet detailing fasting requirements (solid food for ≥8 hours, clear fluids for ≥2 hours), items to bring, and procedural overview. Propofol sedation was administered by an anesthesiologist using a target-controlled infusion system, with initial dosing of 1.5–2.5 mg/kg adjusted according to patient response.17 Supplemental oxygen was provided via nasal cannula at 3–5 L/min throughout the procedure. Continuous monitoring included electrocardiography, pulse oximetry, and non-invasive blood pressure measurement at 3-minute intervals.18 Vital signs were monitored during the surgical procedure.
Conventional Nursing Group
On the examination day, upon arrival at the endoscopy center, nursing staff verified patient identity, confirmed adherence to fasting guidelines, and measured baseline vital signs. Intravenous access was established using a 20-gauge or 22-gauge catheter. Patients received brief verbal instructions regarding the procedure: “Please lie on your side, and the doctor will insert the endoscope through your mouth. The medication will help you sleep comfortably”. Patients were assisted into the left lateral position on the examination table with a standard 10-cm pillow under the head. Lower limbs were positioned with natural flexion, and a bite block was placed after topical oropharyngeal anesthesia with lidocaine gel. Communication was limited to essential instructions such as “Please relax” or “Try to breathe slowly”. All examinations were performed by experienced endoscopists with over 5 years of practice.
Post-procedure care included standard recovery room monitoring until patients achieved a Modified Aldrete Score of at least 9.19 Standard discharge instructions regarding diet resumption and activity restrictions were provided to all patients.
Comprehensive Nursing Group with Positional Nursing Combined with Positive Suggestion
The comprehensive nursing group received enhanced postural care and positive cues in addition to conventional nursing. The comprehensive nursing protocol was developed through a multidisciplinary collaborative process involving endoscopy nurses, anesthesiologists, and gastroenterologists, with consideration of patient feedback from clinical practice. A pilot phase was conducted to refine the protocol, during which staff training procedures were optimized and workflow integration challenges were addressed. Implementation required no additional staffing; the intervention was incorporated into standard pre-procedural preparation time. The hospital had established standard operating procedures (SOPs) for patient positioning nursing and standardized scripts for positive cues. All nursing staff implementing the intervention had completed standardized training. Nursing staff acceptance was high following completion of the standardized training program.
About 15 minutes before examination, the designated nurse established rapport through greeting and introduction. A calm, reassuring tone was maintained during all interactions. Patients received individualized education adapted to their comprehension level, using accessible language and easy-to-understand metaphors to explain the procedure. Positive verbal suggestions were delivered using standardized phrases designed to reduce anxiety and establish expectations of safety and comfort. Patients were taught diaphragmatic breathing techniques as a self-regulation strategy. This exercise was repeated 3–5 times. STAI-S was administered to assess baseline anxiety levels.20
Upon entering the examination room, personalized position adjustments were made by trained nursing staff. Position optimization followed a systematic approach tailored to individual patient anatomy. After assisting the patient into the left lateral position, the nurse adjusted pillow height (8–12 cm) to maintain neutral cervical alignment, avoiding excessive flexion or extension that might compromise airway patency. The patient’s head was positioned with slight anterior tilt (approximately 15–20 degrees) to facilitate endoscope passage. Upper extremities were positioned comfortably in front of the torso or supported with a small pillow. Lower extremities were flexed at the hip and knee joints (approximately 90–120 degrees), with the right leg positioned over the left and a cushion placed between the knees to prevent pressure discomfort. Lumbar support was provided if any gap was detected between the patient’s back and the examination table The nurse verbally confirmed comfort: “Is this position comfortable for you? Would you like any adjustments?”
Positive verbal suggestions were delivered following a structured protocol developed based on cognitive-behavioral principles and refined during pilot testing. All suggestions were delivered in a calm, warm, and reassuring tone at moderate pace. Before sedation induction, the patient was given positive psychological suggestions and gentle words to induce breathing and deep breathing as follows: “The medication will help you relax. Most patients find this much easier than expected”. “You will soon fall into a comfortable sleep, and the examination will be completed shortly”. Breathing Exercise and Relaxation Induction Diaphragmatic breathing was taught using the following script: “Let’s practice a simple breathing technique”. “Breathe in slowly through your nose for 4 counts, letting your abdomen rise”. “Notice how your body feels more relaxed with each breath”. Throughout the examination, even after loss of consciousness, the nurse continued to provide gentle verbal reassurance in a low, calm voice, as evidence suggests that auditory processing may persist during light sedation:21 “You will soon fall into a comfortable sleep, and the examination will be completed quickly”. “We are right here with you. You are safe”. “You are doing very well”. “Everything is progressing smoothly”. “We are almost finished”. If the patient showed signs of light sedation with minor movement, the nurse provided tactile comfort through gentle shoulder contact while repeating calming phrases.
After the procedure, nurses gently called the patient to wake up and give positive feedback as follows: “the examination was successful”. “You did wonderfully”. “Everything went smoothly”. “Take your time waking up. There’s no rush”. Nurses asked if there was any discomfort and solved them accordingly. Patients were given detailed instructions on postoperative precautions and modified PSQ-18 and GCQ were distributed.22
Outcome Measures and Data Collection
Primary Outcome Measures
Anxiety levels were assessed 30 minutes before examination using the State Anxiety subscale of STAI-S.20 This 20-item instrument uses a 4-point Likert scale (total scores 20–80), with higher scores indicating greater anxiety. The STAI-S demonstrates excellent internal consistency (Cronbach’s α=0.86–0.95) and adequate test-retest reliability (r=0.65–0.75) appropriate for situational assessment.23,24 Examination success rate was defined as the proportion of patients completing gastroscopy in a single attempt without premature termination due to patient intolerance, inadequate sedation, or technical difficulties.8 And procedural time was measured in minutes from endoscope insertion through the mouth to complete withdrawal, recorded using standardized electronic timers. GCQ was administered before discharge.25 This 48-item instrument evaluates physical, psychospiritual, and sociocultural comfort on a 4-point Likert scale (total scores 48–192), with higher scores indicating greater comfort. The GCQ demonstrates strong internal consistency (Cronbach’s α=0.88–0.91) and good test-retest reliability (r=0.81).26
Secondary Outcome Measures
Intra-Procedural Hemodynamic Stability
Heart rate, systolic and diastolic blood pressure, and oxygen saturation were recorded at baseline, procedure midpoint, and immediately post-procedure. Hemodynamic fluctuation was calculated as the maximum deviation from baseline for each parameter.27,28
Recovery Time
Emergence time was measured from propofol cessation to full consciousness, defined as coherent verbal responses, orientation to person/place/time, and spontaneous eye opening.19
Adverse Events
Procedure-related complications were documented including nausea, vomiting, abdominal bloating, and throat discomfort. Additional safety outcomes included hypoxemia (SpO2<90% for >30 seconds), bradycardia (<50 bpm), hypotension (systolic BP<90 mmHg), and paradoxical agitation.29
Patient Satisfaction
Patient satisfaction was assessed before discharge using a modified satisfaction questionnaire adapted from the PSQ-18 framework. The questionnaire was simplified to suit the clinical workflow of the endoscopy recovery setting and employed a 0–10 numeric rating scale (0 = completely dissatisfied, 10 = completely satisfied) to evaluate overall satisfaction with the endoscopy experience, which is more intuitive and customary for local patients.
Assessment Timeline
Baseline demographic data was recorded at enrollment. STAI-S was administered 30 minutes pre-procedure. Hemodynamic parameters were recorded at three time points during the procedure. Procedural outcomes were documented intra-procedurally. The GCQ, adverse event checklist, and modified PSQ-18 were completed before discharge (60–90 minutes post-procedure). All assessments were conducted by trained research nurses not involved in direct patient care.
Statistical Analysis
Statistical analysis was performed using SPSS 26.0 software (IBM Corp., Armonk, NY, USA). Data in each group were tested for normality using the Shapiro–Wilk test. For between-group comparisons, independent samples t-tests were used for normally distributed continuous data, while Mann–Whitney U-tests were employed for non-normally distributed data. Chi-square tests or Fisher’s exact test were used for categorical variables. A significant level of P <0.05 was considered statistically significant for all tests.
Results
Baseline Characteristics
As shown in Table 1, this study included 153 patients who completed the entire study protocol, comprising 73 patients in the conventional nursing group and 80 patients in the comprehensive nursing group. All baseline demographic and clinical characteristics were comparable between the two groups. Age distributions were similar (45.23±11.87 years vs 46.15±12.34 years, P =0.628), with male patients accounting for 54.79% and 52.50% in the conventional and comprehensive groups, respectively (P =0.759). Body mass index showed no significant difference between groups (22.45±2.73 kg/m2 vs 22.68±2.91 kg/m2, P =0.603). American Society of Anesthesiologists classification distribution was comparable (P =0.710), with approximately 60% of patients classified as ASA Class I in both groups. Indications for examination, including epigastric pain/discomfort, acid reflux/heartburn, nausea/vomiting, and anemia/occult blood positive, showed similar distributions across groups (P =0.729). Medical history profiles, including prevalence of hypertension, diabetes mellitus, and cardiovascular disease, demonstrated no statistically significant differences (all P >0.05). Current medication use, encompassing proton pump inhibitors, antihypertensive drugs, and hypoglycemic agents, was also similar between groups (all P >0.05).
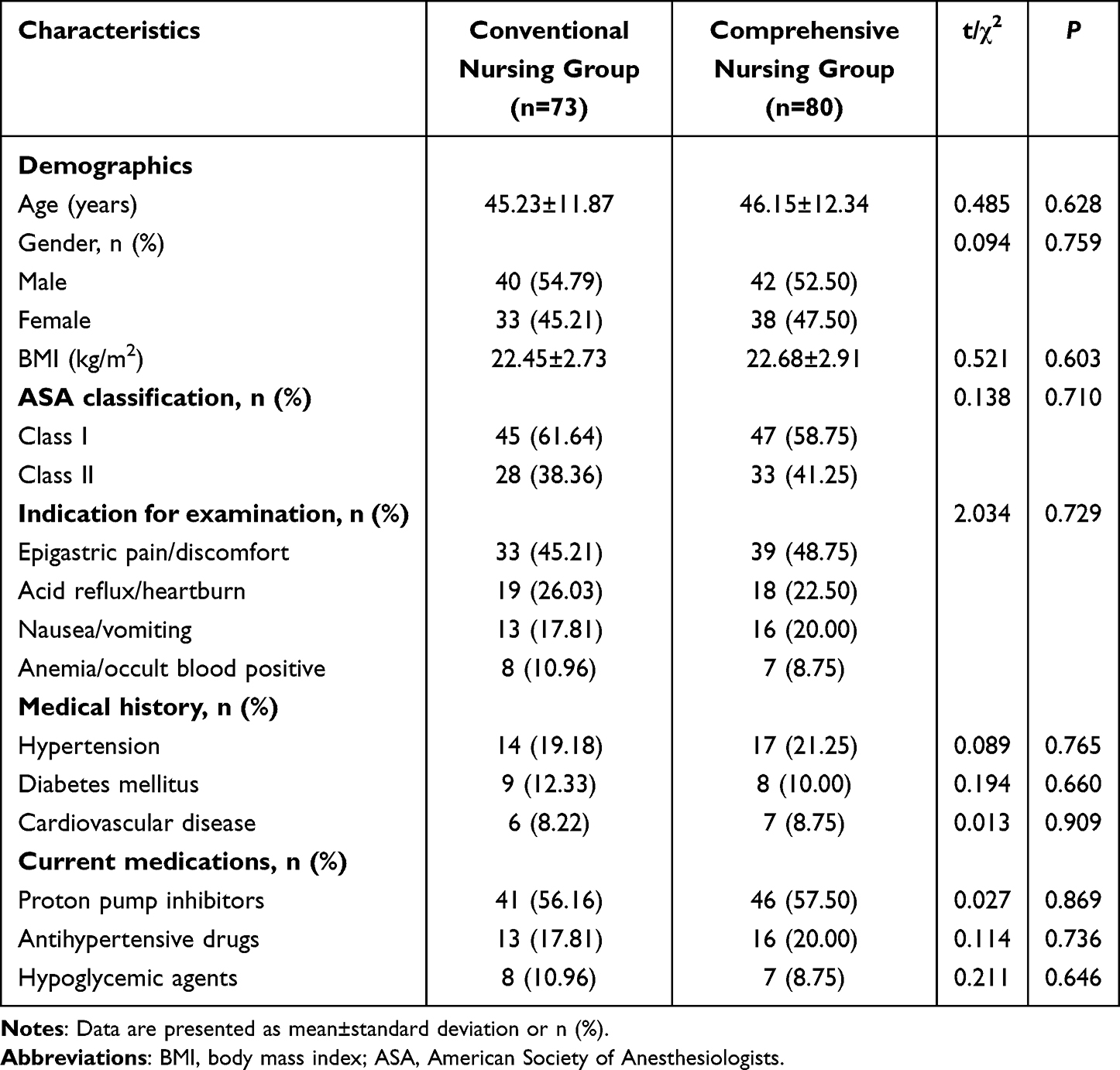 |
Table 1 Baseline Characteristics of Two Groups |
Primary Outcomes
As demonstrated in Table 2, examination success rates were high in both groups (95.89% in conventional group vs 98.75% in comprehensive group), with no statistically significant difference (P =0.239). Examination duration was significantly shorter in the comprehensive nursing group compared to the conventional group (6.54±1.62 min vs 7.23±1.87 min, P =0.016).
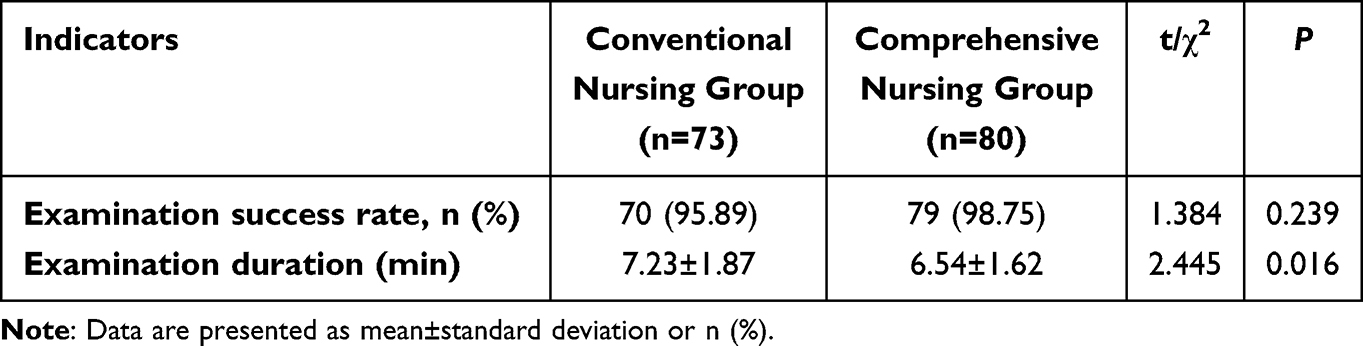 |
Table 2 Comparison of Examination-Related Indicators Between Two Groups |
Figure 2 presents the comparison of anxiety and comfort scores between the two groups. Pre-procedural anxiety assessed by STAI-S revealed significantly lower scores in the comprehensive nursing group (43.23±7.68) compared to the conventional nursing group (48.67±8.45, P <0.001). Post-procedural comfort evaluated using the GCQ demonstrated significantly higher scores in the comprehensive nursing group (156.82±16.43) relative to the conventional nursing group (142.35±18.67, P <0.001).
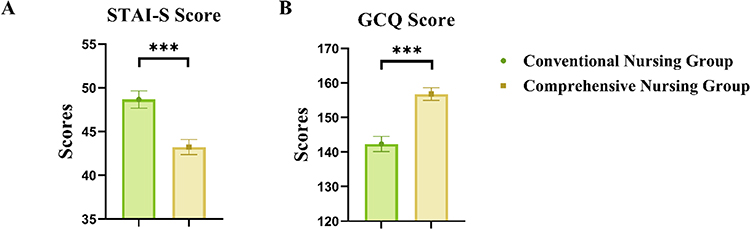 |
Figure 2 Comparison of STAI-S and GCQ Score between Two Groups. (A) The State-Trait Anxiety Inventory (STAI-S) score between two groups before procedure; (B) The General Comfort Questionnaire (GCQ) score between two groups after procedure. ***P < 0.001 compared with the conventional nursing group. |
Secondary Outcomes
Table 3 presents the secondary outcome measures including hemodynamic parameters, adverse events, recovery time, and patient satisfaction. Baseline heart rate measurements showed no difference between groups (76.45±9.23 bpm vs 75.87±8.96 bpm, P >0.05). During the procedure, the comprehensive nursing group maintained significantly lower heart rates (78.63±9.38 bpm) compared to the conventional group (83.67±10.54 bpm, P =0.002). Post-procedure heart rates returned to similar levels in both groups (P >0.05).
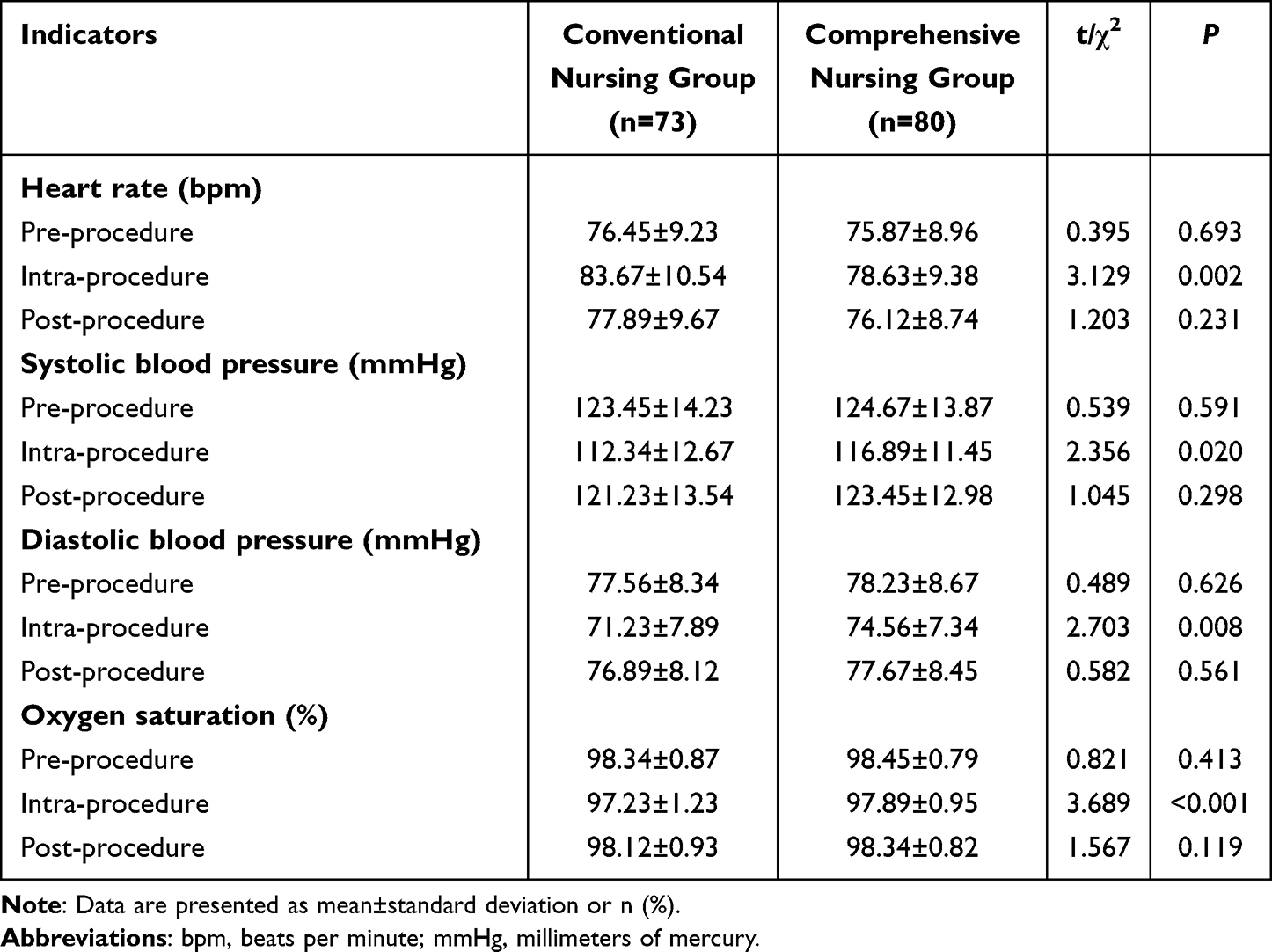 |
Table 3 Comparison of Vital Signs |
Systolic blood pressure measurements revealed comparable baseline values between groups (123.45±14.23 mmHg vs 124.67±13.87 mmHg, P >0.05). Intra-procedural systolic blood pressure was significantly higher in the comprehensive nursing group (116.89±11.45 mmHg) compared to the conventional group (112.34±12.67 mmHg, P =0.020). Post-procedure systolic blood pressure showed no significant difference (P >0.05). Diastolic blood pressure followed a similar pattern, with comparable baseline values (P >0.05), significantly higher intra-procedural values in the comprehensive group (74.56±7.34 mmHg vs 71.23±7.89 mmHg, P =0.008), and similar post-procedure recovery (P >0.05).
Oxygen saturation remained high throughout the procedure in both groups. Baseline measurements were equivalent (P >0.05), while intra-procedural oxygen saturation was significantly higher in the comprehensive nursing group (97.89±0.95%) compared to the conventional group (97.23±1.23%, P =0.001). Post-procedure oxygen saturation showed no significant difference (P >0.05).
As shown in Table 4, Adverse event incidence varied significantly between groups. Nausea occurred in 18 patients in the conventional nursing group and 11 in the comprehensive nursing group (P =0.042). Vomiting was reported in 8 conventional group patients compared to 3 in the comprehensive group (P =0.035). Abdominal bloating affected 22 patients in the conventional group and 15 in the comprehensive group (P =0.046). Throat discomfort was experienced by 31 conventional group patients versus 21 comprehensive group patients (P =0.016). Overall adverse event rates showed significant difference, with 45 patients in the conventional group experiencing at least one adverse event compared to 35 in the comprehensive group (P =0.013).
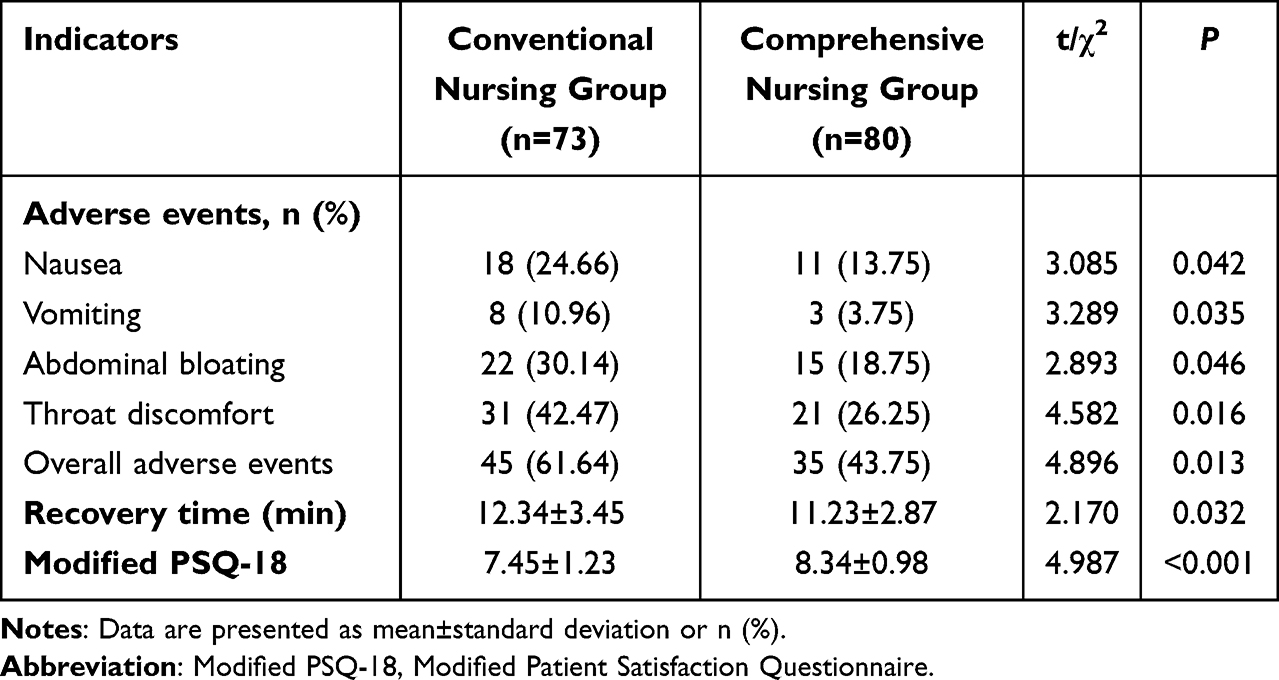 |
Table 4 Comparison of Adverse Events, Recovery Time and Patient Satisfaction |
Recovery time was significantly shorter in the comprehensive nursing group (11.23±2.87 min) compared to the conventional nursing group (12.34±3.45 min, P =0.032). Patient satisfaction scores were significantly higher in the comprehensive nursing group (8.34±0.98) than in the conventional nursing group (7.45±1.23, P <0.001).
Discussion
This retrospective study investigated the effects of positional nursing combined with positive suggestion on patients undergoing painless gastroscopy. Our findings demonstrate that this integrated nursing approach significantly reduces pre-procedural anxiety, shortens examination duration, improves intra-procedural hemodynamic stability, decreases adverse events, and enhances patient comfort and satisfaction compared to conventional care. These results suggest that optimized positioning and psychological support represent valuable adjuncts to standard sedation protocols in endoscopy settings.
Pre-procedural anxiety constitutes a significant challenge in gastrointestinal endoscopy, affecting patient cooperation, sedation requirements, and overall procedural quality.30,31 STAI-S scores in our comprehensive nursing group were significantly lower than those in the conventional group, indicating effective anxiety reduction through standardized positive suggestions delivered during the pre-procedural phase. This finding aligns with previous research demonstrating that structured psychological preparation reduces anticipatory anxiety in procedural settings.13,32 The neurobiological mechanisms underlying anxiety reduction through positive suggestion likely involve modulation of the amygdala and prefrontal cortex, brain regions central to fear processing and emotional regulation.14 By reframing patients’ cognitive appraisal of the procedure from threatening to manageable, positive verbal cues may attenuate activation of the hypothalamic-pituitary-adrenal axis, thereby reducing physiological manifestations of stress.33 The approximately 5-point reduction in STAI-S scores observed in our comprehensive group represents a clinically meaningful decrease, as changes of 4–5 points on this scale are associated with perceptible improvements in subjective anxiety and physiological stress markers.34 While the comprehensive group showed lower anxiety, they exhibited higher intra-procedural blood pressure. This could be explained by propofol’s dose-dependent cardiovascular effects: propofol causes hypotension through sympathetic inhibition and vasodilation, occurring in approximately 36% of endoscopy procedures.35 Previous studies showed that music therapy reduced sedative requirements by 50% during regional anesthesia,36 and anxiety reduction through premedication decreased propofol consumption during endoscopic retrograde cholangiopancreatography.37 The comprehensive group demonstrated lower heart rate combined with more stable blood pressure fluctuation, representing genuine hemodynamic stability rather than stress-induced changes. The shorter recovery time in the comprehensive group further supports reduced propofol exposure.
The significantly shorter examination duration in the comprehensive nursing group merits attention, as procedural efficiency directly impacts endoscopy center throughput and resource utilization. Although the absolute time difference of approximately 40 seconds may appear modest, this reduction likely reflects enhanced patient cooperation and reduced involuntary movements during endoscope manipulation.38,39 Patients experiencing lower anxiety and greater physical comfort are more likely to remain still and tolerate instrumentation, facilitating smoother endoscope passage and optimal mucosal visualization.40 Our standardized positioning optimization approach—including adjusting pillow height, cervical spine alignment, limb placement, and lumbar support—helps maintain airway patency and reduces musculoskeletal discomfort.41 The higher intra-procedural oxygen saturation in the comprehensive group supports improved airway management.9
Nausea, vomiting, abdominal distension, and throat discomfort are common complaints following endoscopy, while lower anxiety levels may attenuate vagal stimulation and reduce susceptibility to nausea.42 Postural improvements, particularly adequate lumbar support and limb positioning, can decrease abdominal pressure sensations and mitigate discomfort caused by insufflation.43 Furthermore, providing continuous intraoperative reassurance to patients in the integrated care group may influence their perception and reporting of discomfort, as psychological factors significantly modulate symptom experience during medical procedures.21,44 Additionally, the comprehensive care group experienced approximately 2 minutes shorter recovery times, potentially related to lower cumulative propofol exposure. This improvement in hemodynamic stability reduced the need for supplemental sedation to control patient movement or discomfort. However, we acknowledge that our study did not directly measure propofol dosage, limiting our ability to establish a definitive causal relationship between nursing interventions and sedation requirements. Future prospective studies should incorporate precise tracking of sedative doses to elucidate these relationships.
Several limitations warrant acknowledgment. The retrospective cohort design limits our ability to establish causation and introduces potential for selection bias, despite the temporal separation strategy employed to minimize contamination. The single-center nature of the study may restrict generalizability. A significant limitation is that propofol dosages were not prospectively recorded in this retrospective study so we cannot directly confirm whether the nursing intervention resulted in lower propofol consumption. If standardized data such as the dosage of propofol and infusion parameters are recorded, it will be helpful to quantify the pharmacological impact of comprehensive nursing. Additionally, the study period spanned different seasonal timeframes for the two groups, potentially introducing unmeasured confounding variables.
From a statistical perspective, while baseline characteristics were comparable between groups, more sophisticated multivariate approaches would better account for within-subject correlations across time points and adjust for potential residual confounding. Post-hoc power analysis indicated that our sample size (n=153) provided >80% power to detect the observed differences in primary outcomes at α=0.05. However, the study may have been underpowered to detect smaller differences in rare adverse events as sample size calculation was not performed. Future research should employ randomized controlled trial designs, incorporate objective sedation depth monitoring and medication tracking, extend follow-up to assess longer-term outcomes, and evaluate implementation across multiple centers to establish external validity.
Despite these limitations, our findings provide evidence supporting the integration of optimized positioning and positive psychological suggestion into routine gastroscopy nursing protocols. This intervention requires minimal additional resources beyond nursing staff training and represents a practical, low-cost approach to improving multiple dimensions of procedural quality. The concurrent improvements across anxiety, efficiency, hemodynamic stability, adverse events, and patient satisfaction suggest that this nursing approach addresses fundamental aspects of the patient experience rather than isolated outcomes. As healthcare systems increasingly emphasize patient-centered care and non-pharmacological interventions, nursing-led initiatives such as the protocol evaluated in this study offer promising avenues for quality enhancement in procedural settings.
Conclusion
This retrospective study suggests that positional nursing combined with positive suggestion may reduce pre-procedural anxiety, shorten examination duration, enhance intra-procedural hemodynamic stability, decrease adverse event incidence, and improve patient comfort and satisfaction. These findings validate the clinical value of this integrated care approach as a practical, non-pharmacological adjunct to standard sedation protocols. Given its favorable safety profile, minimal resource requirements, and beneficial impact on multiple quality indicators, this nursing intervention may merit wider implementation in endoscopy centers.
Ethics Statement
This study was approved by the Ethics Committee of Beihua University Affiliated Hospital (Approval No. 20240081). Informed consent was obtained from all the participants. All methods were carried out in accordance with Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was conducted with no external funding, and its costs have been assumed by researchers.
Disclosure
The authors declare that they have not competing interests.
References
1. Peery AF, Crockett SD, Murphy CC, et al. Burden and cost of gastrointestinal, liver, and pancreatic diseases in the United States: update 2021. Gastroenterology. 2022;162(2):621–12. doi:10.1053/j.gastro.2021.10.017
2. Cohen LB, Delegge MH, Aisenberg J, et al. AGA Institute review of endoscopic sedation. Gastroenterology. 2007;133(2):675–701. doi:10.1053/j.gastro.2007.06.002
3. Albayrak T, Torun Göktaş A, Eyüpoğlu S, Muhtaroğlu A, Dulger AC. Patient anxiety in endoscopy: a comparative analysis of single vs. dual procedure effects. Cureus. 2024;16(3):e57237. doi:10.7759/cureus.57237
4. Yu X, Deng H, Xiong Z, et al. A scale to measure the worry level in gastrointestinal endoscopy with sedation: development, reliability, and validity. Int J Clin Health Psychol. 2023;23(4):100410. doi:10.1016/j.ijchp.2023.100410
5. Khan AA, Ali A, Khan AS, et al. Effects of visual aid on state anxiety, fear and stress level in patients undergoing endoscopy: a randomized controlled trial. Ann Med. 2023;55(1):1234–1243. doi:10.1080/07853890.2023.2191000
6. Kiecolt-Glaser JK, McGuire L, Robles TF, Glaser R. Emotions, morbidity, and mortality: new perspectives from psychoneuroimmunology. Annu Rev Psychol. 2002;53:83–107. doi:10.1146/annurev.psych.53.100901.135217
7. Tang S, Zheng Y, Li X, Zhang Y, Zhang Z. Optimizing sedation in gastroscopy: a study on the etomidate/propofol mixture ratio. Front Med. 2024;11:1392141. doi:10.3389/fmed.2024.1392141
8. Early DS, Lightdale JR, Vargo JJ, et al. Guidelines for sedation and anesthesia in GI endoscopy. Gastrointest Endosc. 2018;87(2):327–337. doi:10.1016/j.gie.2017.07.018
9. Amornyotin S. Sedation-related complications in gastrointestinal endoscopy. World J Gastrointest Endosc. 2013;5(11):527–533. doi:10.4253/wjge.v5.i11.527
10. Liu X, Xiao Q, Zhuang S. Comparison of propofol-esketamine versus propofol for anesthesia in gastroscopy: a double-blind, randomized controlled clinical trial. Front Med. 2023;10:1184709. doi:10.3389/fmed.2023.1184709
11. Yang Y, Xia Q, Wu L, et al. Examination tolerance, pre-examination anxiety, knowledge needs and cooperation in gastroscopic examinees: a prospective, correlational analysis in a health screening population. Nurs Open. 2024;11(8):e70006. doi:10.1002/nop2.70006
12. Kim Y, Yoo SH, Chun J, Kim JH, Youn YH, Park H. Relieving anxiety through virtual reality prior to endoscopic procedures. Yonsei Med J. 2023;64(2):117–122. doi:10.3349/ymj.2022.0319
13. Tefikow S, Barth J, Maichrowitz S, Beelmann A, Strauss B, Rosendahl J. Efficacy of hypnosis in adults undergoing surgery or medical procedures: a meta-analysis of randomized controlled trials. Clinic Psychol Rev. 2013;33(5):623–636. doi:10.1016/j.cpr.2013.03.005
14. Rainville P, Duncan GH, Price DD, Carrier B, Bushnell MC. Pain affect encoded in human anterior cingulate but not somatosensory cortex. Science. 1997;277(5328):968–971. doi:10.1126/science.277.5328.968
15. Aslan K, Özer Z, Yöntem MK. Effect of virtual reality on pain, anxiety, and vital signs in endoscopy. Pain Manage Nurs. 2025;26(4):e371–e380. doi:10.1016/j.pmn.2024.11.009
16. Hidalgo-Cabanillas M, Laredo-Aguilera JA, Cobo-Cuenca AI, et al. Patient satisfaction and safety in the administration of sedation by nursing staff in the digestive endoscopy service: a cross-sectional study. BMC Nurs. 2024;23(1):953. doi:10.1186/s12912-024-02644-y
17. Leslie K, Absalom A, Kenny GN. Closed loop control of sedation for colonoscopy using the Bispectral Index. Anaesthesia. 2002;57(7):693–697. doi:10.1046/j.1365-2044.2002.02572_2.x
18. Sarraj R, Theiler L, Vakilzadeh N, Krupka N, Wiest R. Propofol sedation in routine endoscopy: a case series comparing target controlled infusion vs manually controlled bolus concept. World J Gastrointest Endosc. 2024;16(1):11–17. doi:10.4253/wjge.v16.i1.11
19. Aldrete JA. The post-anesthesia recovery score revisited. J Clin Anesth. 1995;7(1):89–91. doi:10.1016/0952-8180(94)00001-k
20. Spielberger C, Gorsuch R, Lushene R, Vagg PR, Jacobs G. Manual for the State-Trait Anxiety Inventory (Form Y1 – Y2). Vol. IV. 1983.
21. Lubke GH, Kerssens C, Phaf H, Sebel PS. Dependence of explicit and implicit memory on hypnotic state in trauma patients. Anesthesiology. 1999;90(3):670–680. doi:10.1097/00000542-199903000-00007
22. Polese L, Giugliano E, Valmasoni M. Patient position in operative endoscopy. J Clin Med. 2023;12(21):6822. doi:10.3390/jcm12216822
23. Knowles KA, Olatunji BO. Specificity of trait anxiety in anxiety and depression: meta-analysis of the state-trait anxiety inventory. Clinic Psychol Rev. 2020;82:101928. doi:10.1016/j.cpr.2020.101928
24. Barnes LLB, Harp D, Jung WS. Reliability generalization of scores on the spielberger state-trait anxiety inventory. Educ Psychol Meas. 2002;62:603–618. doi:10.1177/0013164402062004005
25. Kolcaba KY. A theory of holistic comfort for nursing. J Adv Nurs. 1994;19(6):1178–1184. doi:10.1111/j.1365-2648.1994.tb01202.x
26. Kolcaba K, Tilton C, Drouin C. Comfort Theory: a unifying framework to enhance the practice environment. J Nurs Adm. 2006;36(11):538–544. doi:10.1097/00005110-200611000-00010
27. Amornyotin S, Chalayonnawin W, Kongphlay S. Deep sedation for endoscopic retrograde cholangiopancreatography: a comparison between clinical assessment and Narcotrend(TM) monitoring. Med Devices. 2011;4:43–49. doi:10.2147/mder.S17236
28. Mason KP, Green SM, Piacevoli Q. Adverse event reporting tool to standardize the reporting and tracking of adverse events during procedural sedation: a consensus document from the World SIVA International Sedation Task Force. Br J Anaesth. 2012;108(1):13–20. doi:10.1093/bja/aer407
29. Cotton PB, Eisen GM, Aabakken L, et al. A lexicon for endoscopic adverse events: report of an ASGE workshop. Gastrointest Endosc. 2010;71(3):446–454. doi:10.1016/j.gie.2009.10.027
30. Lv LL, Zhang MM. Up-to-date literature review and issues of sedation during digestive endoscopy. Wideochirurgia i inne techniki maloinwazyjne. 2023;18(3):418–435. doi:10.5114/wiitm.2023.127854
31. Sneyd JR. Developments in procedural sedation for adults. BJA Educ. 2022;22(7):258–264. doi:10.1016/j.bjae.2022.02.006
32. Montgomery GH, Bovbjerg DH, Schnur JB, et al. A randomized clinical trial of a brief hypnosis intervention to control side effects in breast surgery patients. J National Cancer Inst. 2007;99(17):1304–1312. doi:10.1093/jnci/djm106
33. Faymonville ME, Boly M, Laureys S. Functional neuroanatomy of the hypnotic state. J Physiol Paris. 2006;99(4–6):463–469. doi:10.1016/j.jphysparis.2006.03.018
34. Zhou Y, Li YP. Safety and efficacy of etomidate in combination with oxycodone in painless gastroscopic procedures in the elderly: a prospective randomized controlled trial study. Medicine. 2023;102(1):e32612. doi:10.1097/md.0000000000032612
35. Sneyd JR, Absalom AR, Barends CRM, Jones JB. Hypotension during propofol sedation for colonoscopy: a retrospective exploratory analysis and meta-analysis. Br J Anaesth. 2022;128(4):610–622. doi:10.1016/j.bja.2021.10.044
36. Lepage C, Drolet P, Girard M, Grenier Y, DeGagné R. Music decreases sedative requirements during spinal anesthesia. Anesthesia Analg. 2001;93(4):912–916. doi:10.1097/00000539-200110000-00022
37. Paspatis GA, Manolaraki MM, Vardas E, Theodoropoulou A, Chlouverakis G. Deep sedation for endoscopic retrograde cholangiopancreatography: intravenous propofol alone versus intravenous propofol with oral midazolam premedication. Endoscopy. 2008;40(4):308–313. doi:10.1055/s-2007-995346
38. Alam L, Khan RSA, Saeed F, Sher F, Khan RZA. Does patient’s position count during endoscopic retrograde cholangio-pancreatography? Left lateral decubitus versus prone position. Pak J Med Sci. 2023;39(5):1232–1237. doi:10.12669/pjms.39.5.6932
39. Meeusen V, Kim M, Ma R, et al. A randomized controlled trial of patient positioning during Endoscopic Retrograde Cholangiopancreatography (ERCP) procedures: a comparison between semi-prone- and prone-positioned patients. Gastroenterol Nurs. 2025;48(1):51–61. doi:10.1097/sga.0000000000000849
40. Rex DK, Imperiale TF, Latinovich DR, Bratcher LL. Impact of bowel preparation on efficiency and cost of colonoscopy. Am J Gastroenterol. 2002;97(7):1696–1700. doi:10.1111/j.1572-0241.2002.05827.x
41. Hu B, Jiang K, Shi W, et al. Effect of remimazolam tosilate on respiratory depression in elderly patients undergoing gastroscopy: a multicentered, prospective, and randomized study. Drug Des Devel Ther. 2022;16:4151–4159. doi:10.2147/dddt.S391147
42. Koch KL, Andrews PLR, Stern RM. Nausea: Mechanisms and Management. 2011.
43. Takahashi Y, Tanaka H, Kinjo M, Sakumoto K. Prospective evaluation of factors predicting difficulty and pain during sedation-free colonoscopy. Dis Colon Rectum. 2005;48(6):1295–1300. doi:10.1007/s10350-004-0940-1
44. Schnur JB, Bovbjerg DH, David D, et al. Hypnosis decreases presurgical distress in excisional breast biopsy patients. Anesthesia Analg. 2008;106(2):440–4, table of contents. doi:10.1213/ane.0b013e31815edb13
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of the Online Mindfulness-Based Stress Reduction on Anxiety and Depression Status of COVID-19 Patients Treated in Fangcang Hospitals: A Randomized Controlled Trial
Li H, Chen H, Ye Z, Li X, Yang L, Wang S, Yang S, Liu S, Chen S, Li R, Yang J, Li H, Bao Y, Shi Y, Wang J, He Y, Liu M
Psychology Research and Behavior Management 2023, 16:2735-2745
Published Date: 18 July 2023