Back to Journals » Journal of Asthma and Allergy » Volume 18
Application of Magnetic Particle Chemiluminescence Technology to Detect Sensitization in Patients in Guangzhou, China: A Study Based on Real-World Medical Data
Authors Huang H, Chen Y, Hu H, Zheng P ![]() , Luo W, Fang Y, Lin Y, Sun B
, Luo W, Fang Y, Lin Y, Sun B ![]()
Received 12 May 2025
Accepted for publication 21 August 2025
Published 12 September 2025 Volume 2025:18 Pages 1255—1267
DOI https://doi.org/10.2147/JAA.S534408
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Huimin Huang,1,2,* Yifan Chen,1,* Haisheng Hu,1 Peiyan Zheng,1 Wenting Luo,1 Yanting Fang,1 Yinghong Lin,1 Baoqing Sun1,2
1Department of Clinical Laboratory, State Key Laboratory of Respiratory Disease, National Center for Respiratory Medicine, National Clinical Research Center for Respiratory Disease, Guangzhou Institute of Respiratory Health, The First Affiliated Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China; 2Guangzhou National Laboratory, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Baoqing Sun, Department of Clinical Laboratory, State Key Laboratory of Respiratory Disease, National Center for Respiratory Medicine, National Clinical Research Center for Respiratory Disease, Guangzhou Institute of Respiratory Health, the First Affiliated Hospital of Guangzhou Medical University, 28 Qiaozhongzhong road, Guangzhou, People’s Republic of China, Email [email protected]
Objective: Magnetic particle chemiluminescence is a novel allergen detection technology recently introduced in clinical practice in China. This study analyzed the application of the ALLEOS assay using real-world clinical data from Guangzhou to identify regional allergen sensitization patterns.
Methods: A retrospective review of 20,406 suspected allergy patients, tested for 28 specific allergens using the ALLEOS 2000 system at the First Affiliated Hospital of Guangzhou Medical University from June 2021 to January 2024.
Results: The highest positive rate was observed for Dermatophagoides farinae (53.4%), followed by D. pteronyssinus (43.2%) and tropical mites (20.4%). Children showed significantly higher positivity rates for most allergens compared to adults, except for dog dander and German cockroach (P < 0.05). Among allergic diseases, children predominated in rhinitis (84.9%), while adults predominated in asthma (56.5%). In terms of severity, asthma and rhinitis patients exhibited higher sensitization levels (Class 3– 6) to D. pteronyssinus (81.6% and 86.3%) and D. farinae (86.7% and 87.3%), while dermatitis patients were more sensitized to egg (19.7%) and milk (17.9%) allergens. Allergen positivity rates varied by season, with children showing significantly higher sensitization to both daisy and dandelion in autumn (11.1% and 8.8%) and winter (11.8% and 16.7%). In childhood (ages 0– 4), egg (31.4%) and milk (27.1%) sensitization rates peaked and declined with age, whereas animal dander showed lower rates (< 10.0%). Multiple sensitizations were observed in 22.2% of patients. Analysis of sensitization patterns revealed three main categories for inhalation allergens: mite-dominant, animal dander-dominant, and pollen-dominant sensitizations, with a Cronbach’s α of 0.889. Similarly, food allergies were categorized into egg and milk-dominant, nut-dominant, and seafood-dominant patterns, with a Cronbach’s α of 0.932.
Conclusion: This real-world study revealed age-, disease-, and season-specific allergen sensitization patterns in southern China. Inhalant and food allergens formed three major sensitization clusters each. These findings support region- and population-specific testing strategies and may inform clinical decision-making.
Keywords: allergen, sIgE, magnetic particle chemiluminescence, diagnostic technology, real-world study
Introduction
Allergic diseases have become a significant global public health concern, affecting individuals of all ages. The prevalence of allergies has increased over the past few decades, particularly in urban areas. Current estimates indicate that approximately 30% to 40% of the global population is affected by allergic conditions.1,2 These conditions impose a significant burden not only on individuals but also on society as a whole. For patients, the burden of allergic diseases extends beyond the physical symptoms like wheezing, itchy skin, and watery eyes.3 Our preliminary research shows that many allergic patients experience worsening symptoms due to delayed diagnosis and treatment.4,5 This delay is often caused by two main factors: doctors working in primary healthcare settings underestimateing the importance of allergens in causing symptoms, and patients failing to provide complete symptom information to their doctors. The indirect costs caused by factors such as missed diagnosis or misdiagnosis have greatly increased the social burden of allergic disease.6 Allergen detection is an important step in the diagnosis, prevention, and treatment of allergic diseases. In China, this challenge is amplified by its vast, diverse population and regional climatic variations. Guangzhou, a subtropical metropolis with high humidity and warm temperatures, fosters pervasive allergens like Dermatophagoides mites, mold, and pollen, contributing to disproportionately high sensitization rates.
The recent introduction of the ALLEOS assay, a magnetic particle chemiluminescence technology, offers promise. Its enhanced sensitivity and specificity—attributed to improved target binding and reduced nonspecific signals—could address gaps in detecting polysensitization and age-specific allergen profiles.7 However, real-world validation in Chinese populations is lacking.8,9 Leveraging data from 20,406 patients in Guangzhou (July 2021–June 2024), this study evaluates the clinical utility of the ALLEOS system and delineates regional sensitization patterns. We aim to bridge critical gaps in allergy management by informing precision diagnostics, seasonal prevention strategies, and domestically relevant guidelines.
Method
Study Design
This is a retrospective study based on real-world medical data. The analysis included patients with suspected allergies who have undergone serum allergen-specific IgE (sIgE) determination using magnetic particle luminescence technology (ALLEOS 2000, China) in the First Affiliated Hospital of Guangzhou Medical University from July, 2021 to January, 2024. Patients with cancer, immunodeficiency, parasitic infection, and autoimmune diseases were excluded. The following symptoms were considered as indications of a suspected allergy by doctors: dyspnea, wheezing and/or cough not attributable to common cold, runny nose, sneezing, nasal itching/obstruction, rashes, wheal, urticaria, abdominal pain, diarrhea, indigestion, and itchy eyes. For these patients, serum allergen sIgE tests panel were selected to confirm causative allergen(s).
Twenty eight common allergens were tested on the ALLEOS system: Tropical mites (D201); Horse dander (E3); Cow dander (E4); Codfish (F3); Hazelnut (F17); Brazil nut (F18); Almond (F20); Beef (F27); Coconut (F36); Daisy (W7); Dandelion (W8); Plantain (W9); D. pteronyssinus (D1); Dog dander (E5); Egg white (F1); Milk (F2); Wheat (F4); Shrimp (F24); German cockroach (I6); Alternaria alternata (M6); Cat dander (E1); Aspergillus fumigatus (M3); Mugwort (W6); Sesame (F10); Peanut (F13); Soybean (F14); Crab (F23); D. farinae (D2). The diagnosis of asthma, rhinitis, and dermatitis is based on the Global Initiative for Asthma (GINA),10 the Allergic Rhinitis and Its Impact on Asthma (ARIA),11 and Clinical Diagnostic Guidelines for Dermatitis,12 respectively. Participants were divided into two age groups: children (0–18 years) and adults (≥19 years). Ethical approval was obtained from the Ethics Committee of The First Affiliated Hospital of Guangzhou Medical University. The initial approval (Reference number: GYFYY-2016-73) covered the secondary analysis of de-identified data from the Guangzhou Medical Database for multiple research purposes during the period of 2016 to 2021. An extension of this approval was granted under a new reference number (GYFYY-2022-85), allowing continued use of the database for related studies from 2022 onward. The current analysis of allergy-related data collected between 2021 and 2024 falls within the scope of these approvals. No additional ethical review was required.
Detection Method
All samples were collected with a vacuum blood collection tube with separated gel. A venous blood sample of 5 mL was drawn and centrifuged for 10 minutes at 3000 r/min. Sera were analyzed using magnetic particle luminescence technology (ALLEOS 2000, China) by trained technicians and the results were reported in kU/L, with ≥ 0.35 kU/L as a positive cutoff. Based on the quantitative sIgE levels, the reactivity was categorized into six classes: Class 1 (≥ 0.35 kU/L to < 0.70 kU/L), Class 2 (≥ 0.70 kU/L to < 3.50 kU/L), Class 3 (≥ 3.50 kU/L to < 17.50 kU/L), Class 4 (≥ 17.50 kU/L to < 50.00 kU/L), Class 5 (≥ 50.00 kU/L to < 100.00 kU/L), and Class 6 (≥ 100.00 kU/L).
Statistical Method
Data was analyzed using SPSS 22.0 (IBM Corp, Armmonk, NY, USA). Normally distribution data, such as age were presented as mean ± standard deviation. Quantitative information such as positive rate was presented as percentage or frequency. Inter-group difference was assessed using the chi-square test (χ2). Correlations between non-parametric data were analyzed using Spearman’s tests, with correlation coefficients presented as “rs”. Interrelationship between allergens was analyzed using optimal scale analysis, and statistical significance was defined as P < 0.05.
Result
Demographic and Clinical Characteristics of Patients
A total of 20,406 patients were included in this study, with 56.3% male (n = 11,497) and 43.7% female (n = 8909), and the average age was 31 ± 26 years. Among them, 1,0918 were adults (≥ 18 years), with an average age of 51 ± 17 years, and 9488 were children (< 18 years), with an average age of 6 ± 4 years. Among the 20,406 patients, 6743 were definitively diagnosed with allergic diseases, including 3666 (17.9%) with asthma, 2087 (10.2%) with rhinitis, and 990 (4.8%) with atopic dermatitis. The remaining patients could not be clearly diagnosed with a specific allergic disease. Among the inhaled allergens, the highest sensitization rate was D. farinae (53.4%), followed by D. pteronyssinus (43.2%), tropical mites (20.4%), and cat dander (9.1%). For food allergens, the highest sensitization rate was egg white (17.0%), followed by milk (15.2%), shrimp (4.4%), and crab (4.1%) (Table 1).
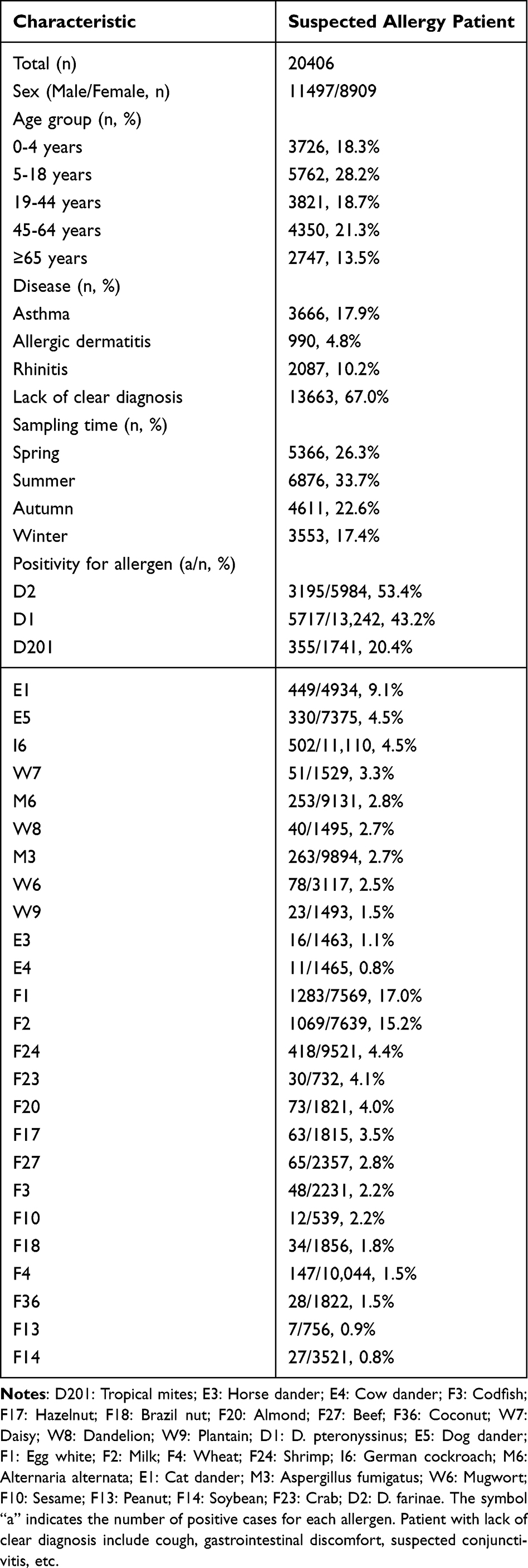 |
Table 1 Demographic and Clinical Characteristics of 20,406 Patients from Southern China |
Differences in Positive Rate Among Adults and Children
The three allergens with the highest positive rate among both adults and children were D. farinae (39.7% vs56.2%, χ2 = 92.1, P < 0.001), D. pteronyssinus (29.5% vs 52.8%, χ2= 712.4, P < 0.001), and tropical mites (17.0% vs 35.6%, χ2= 54.5, P < 0.001), with children showing significantly higher rates than adults. Additionally, compared to adults, children had significantly higher positive rate for egg white (20.3% vs 1.3%, χ2= 285.3, P < 0.001) and milk (16.7% vs 1.3%, χ2= 220.7, P < 0.001). Only two allergens showed higher positive rate in adults compared to children: dog dander (5.4% vs 4.2%, χ2= 4.893, P < 0.01) and German cockroach (5.4% vs 3.9%, χ2= 13.964, P < 0.001) (Figure 1a).
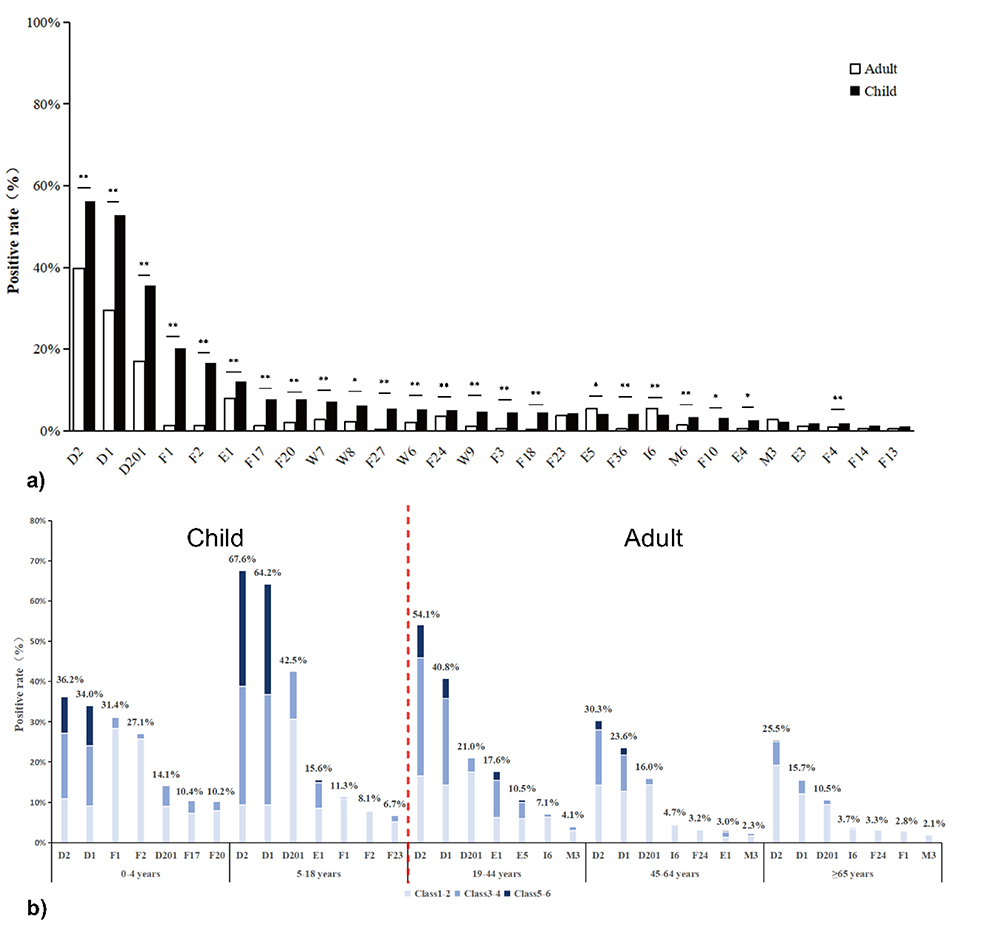 |
Figure 1 The distribution of allergen positive rate across different age groups. (a) Comparison of allergen positive rate differences between adults and children, Chi square test, *P < 0.05; **P < 0.001. (b) The top seven allergies with the highest positive rate among patients of different age groups. Based on the quantitative sIgE levels, the reactivity was categorized into six classes: Class 1 (≥ 0.35 kU/L to < 0.70 kU/L), Class 2 (≥ 0.70 kU/L to < 3.50 kU/L), Class 3 (≥ 3.50 kU/L to < 17.50 kU/L), Class 4 (≥ 17.50 kU/L to < 50.00 kU/L), Class 5 (≥ 50.00 kU/L to < 100.00 kU/L), and Class 6 (≥ 100.00 kU/L). Participants were divided into two age groups: children (0–18 years) and adults (≥19 years) and the red cutoff line indicates the boundary between adult and child groups. D201: Tropical mites; D1: D. pteronyssinus; E5: Dog dander; E1: Cat dander; F1: Egg white; F2: Milk; F24: Shrimp; I6: German cockroach; M3: Aspergillus fumigatus; D2: D. farinae. |
The positive rate of D. farinae, D. pteronyssinus, and tropical mites consistently ranked in the top three allergens across all age groups, peaking during adolescence (ages 5–18) at 67.6%, 64.2%, and 42.5%, respectively. In children (ages 0–4), the highest positive rates were observed for egg white (31.4%) and milk (27.1%), which gradually declined with age. The positivity rate for cat dander significantly increased during adolescence and young adulthood (ages 19–44), reaching 15.6% and 17.6%, respectively, while remaining lower in other age groups. Additionally, the positive rate for most allergens gradually decreased after adolescence, though the rate for German cockroach reached its highest in young adulthood and continued to rise in subsequent age groups, peaking in middle-aged (ages 45–64) and elderly (≥ 65 years) populations at 4.7% and 3.7%, respectively (Figure 1b).
Differences in Positive Rate Between Adults and Children with Rhinitis, Asthma, and Dermatitis
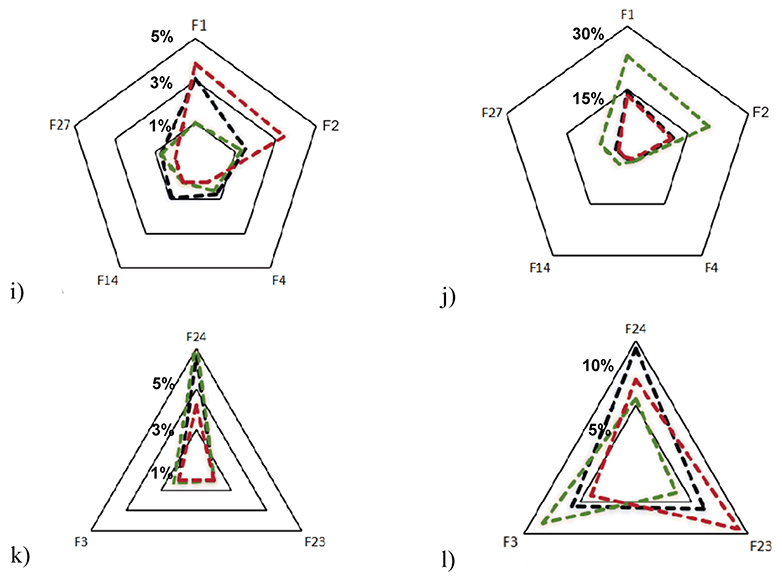
In the disease, pediatric patients with rhinitis accounted for 84.9%, and asthma patients accounted for 43.5%; adult rhinitis patients accounted for 15.1%, and asthma patients accounted for 56.5%. Across all disease types, D. farinae was the primary allergen, with positive rate of 77.5% in asthma, 49.7% in dermatitis, and 75.1% in rhinitis. The second most common allergen was D. pteronyssinus, with positive rate of 58.5% in asthma, 38.4% in dermatitis, and 67.7% in rhinitis. Among pediatric patients with dermatitis, the positive rate for egg white (23.0% vs 1.0%, χ2 = 87.0, P < 0.001) and milk (20.2% vs 1.3%, χ2 = 53.5, P < 0.001) were significantly higher than in adult patients. Dog dander showed a significantly higher positive rate in adults with asthma (13.5% vs 7.8%, χ2 = 7.4, P < 0.01) and rhinitis (16.7% vs 4.9%, χ2= 10.988, P < 0.001) compared to children. For nut allergens, both adults and child were primarily sensitized to hazelnut (1.3% and 7.8%, respectively) and almond (2.1% and 7.7%, respectively). For pollen allergens, adult dermatitis patients were mainly sensitized to daisy (8.2%), while pediatric asthma patients showed higher sensitization to dandelion (13.9%), and pediatric dermatitis patients to plantain (9.5%). For animal hair allergens, adult patients were mainly sensitized to cat and dog dander, while child were primarily sensitized to cat dander alone (Figure 2a–l).
Figure 2 Continued. Figure 2 The distribution of allergen positive rate across different diseases in adults and children. The distribution of mite allergen positive rate in adults (a) and children (b); the distribution of animal dander allergen positive rate in adults (c) and children (d); the distribution of nut allergen Positive rate in adults (e) and children (f); the distribution of pollen allergen positive rate in adults (g) and children (h); the distribution of common food allergen Positive rate in adults (i) and children (j); the distribution of seafood allergen positive rate in adults (k) and children (l). D201: Tropical mites; E3: Horse dander; E4: Cow dander; F3: Codfish; F17: Hazelnut; F18: Brazil nut; F20: Almond; F27: Beef; F36: Coconut; W7: Daisy; W8: Dandelion; W9: Plantain; D1: D. pteronyssinus; E5: Dog dander; F1: Egg white; F2: Milk; F4: Wheat; F24: Shrimp; I6: German cockroach; M6: Alternaria alternata; E1: Cat dander; M3: Aspergillus fumigatus; W6: Mugwort; F10: Sesame; F13: Peanut; F14: Soybean; F23: Crab; D2: D. farinae.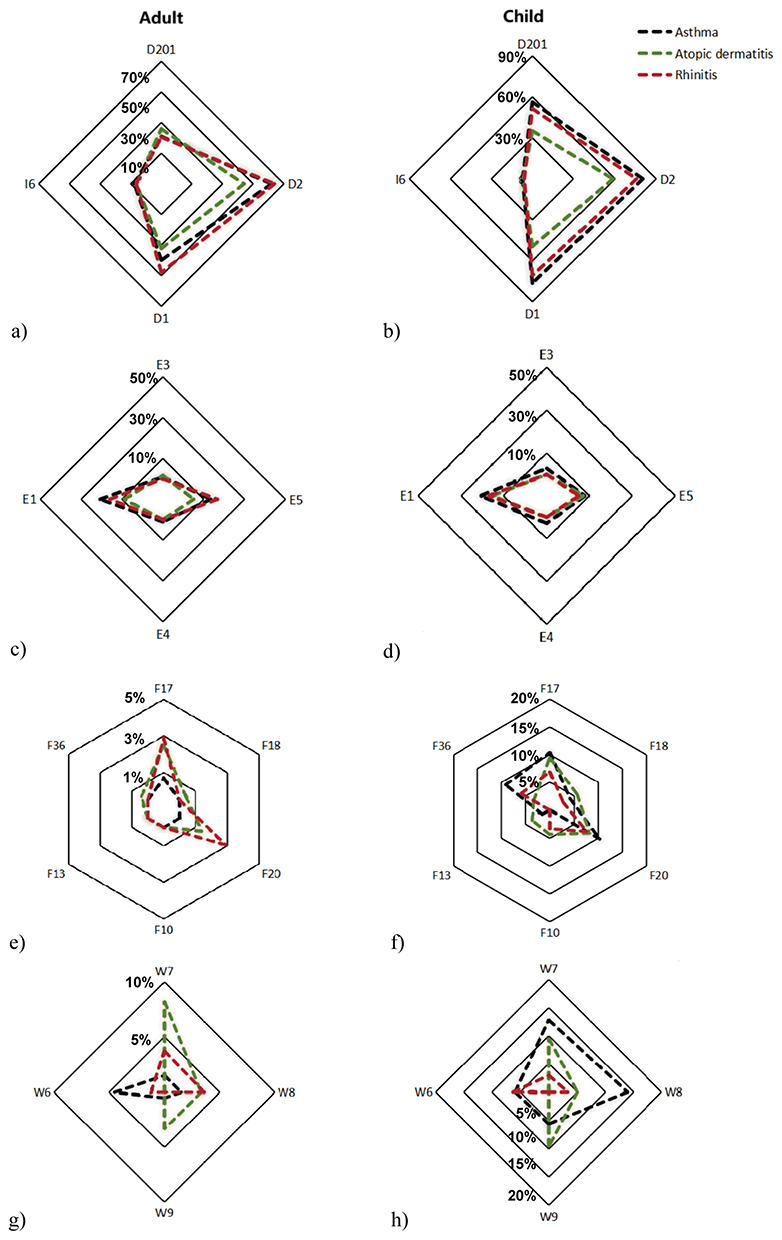
The analysis of sensitization levels for allergens with an overall positivity rate ≥4.5% across different diseases is shown in Table 2. In adult patients with asthma, dermatitis, and rhinitis, the proportions of severe sensitization (Class 5–6) to D. pteronyssinus and D. farinae were 15.1%, 13.8%, 15.5% and 20.2%, 22.7%, 26.7%, respectively, while the proportions of moderate sensitization (Class 3–4) were 53.4%, 40.0%, 53.5%, and 56.1%, 40.9%, 46.7%, respectively. In pediatric patients with asthma, dermatitis, and rhinitis, the proportions of severe sensitization to D. pteronyssinus and D. farinae were 46.9%, 32.0%, 43.6%, and 44.9%, 39.5%, 45.0%, respectively, while the proportions of moderate sensitization were 41.2%, 41.6%, 44.5%, and 43.3%, 47.4%, 43.0%, respectively. Additionally, in rhinitis and asthma patients, sensitization patterns to egg white and milk was primarily concentrated in Class 1–2 (both above 95%). In pediatric dermatitis patients, the proportions of moderate sensitization to milk and egg white were 13.7% and 14.0%, respectively. In adult dermatitis patients, the proportions of severe and moderate sensitization to milk were 40.0% and 20.0%, respectively, higher than in rhinitis (0.0%) and asthma (0.0%). Tropical mites were the only allergen without any cases of Class 5–6 sensitization.
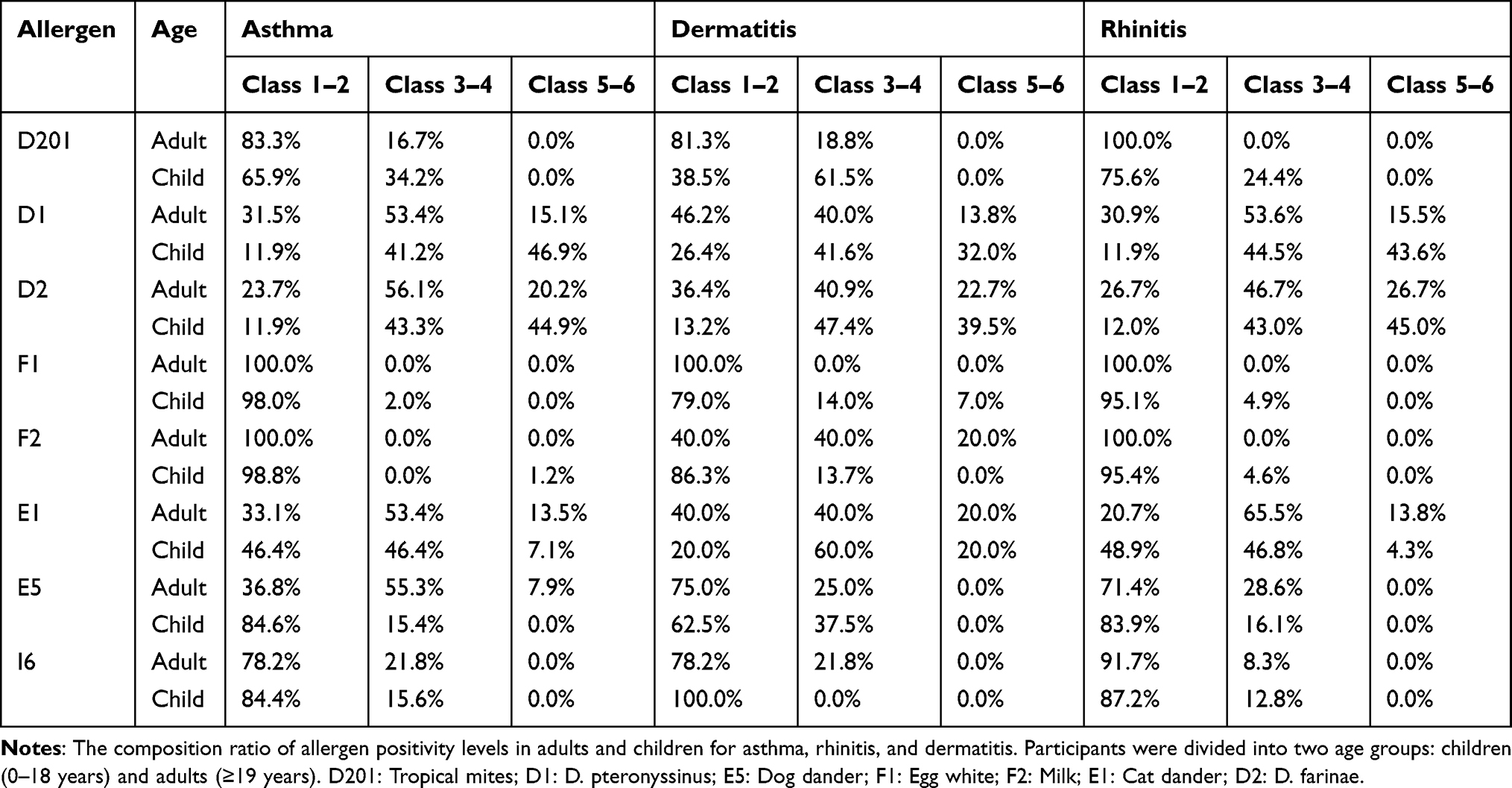 |
Table 2 The Distribution of Sensitization Patterns to Allergens Across Different Diseases in Adults and Children |
Differences in Positive Rate Between Adults and Child Patients in Different Seasons
The seasonal variation characteristics of inhalant allergens with an overall positivity rate > 2.5% are shown in Figure 3. The positive rates for allergens to D. pteronyssinus and D. farinae remained high throughout the year for both adults and children. In children, the positive rates for tropical mites, D. pteronyssinus, and D. farinae showed the highest in the summer, reaching 38.5%, 58.0%, and 62.6%, respectively (Figure 3a–c). Among adults, the German cockroach was the only tested allergen showed a higher positive rate than children throughout the year, and both adults and child showed peak positive rates for the German cockroach in the summer at 6.6% and 4.8%, respectively (Figure 3d). The positive rates for cat dander in both adults and children increased from summer to winter, with the lowest levels observed in the summer (5.9%). Unlike cat dander, the positive rate of adult dog dander allergens is higher than children. The seasonal trend of adult positive rates is similar to that of cat dander, peaking in winter (8.5%) and reaching its lowest point in summer (3.7%) (Figure 3e and f). For children, the positive rates for daisy and dandelion allergens increased in autumn and winter, which were higher compared to those in adults (Figure 3g and h). The seasonal variation in the positive rate of Alternaria alternata is not significant; however, the positive rate in children is noticeably higher than in adults (Figure 3i).
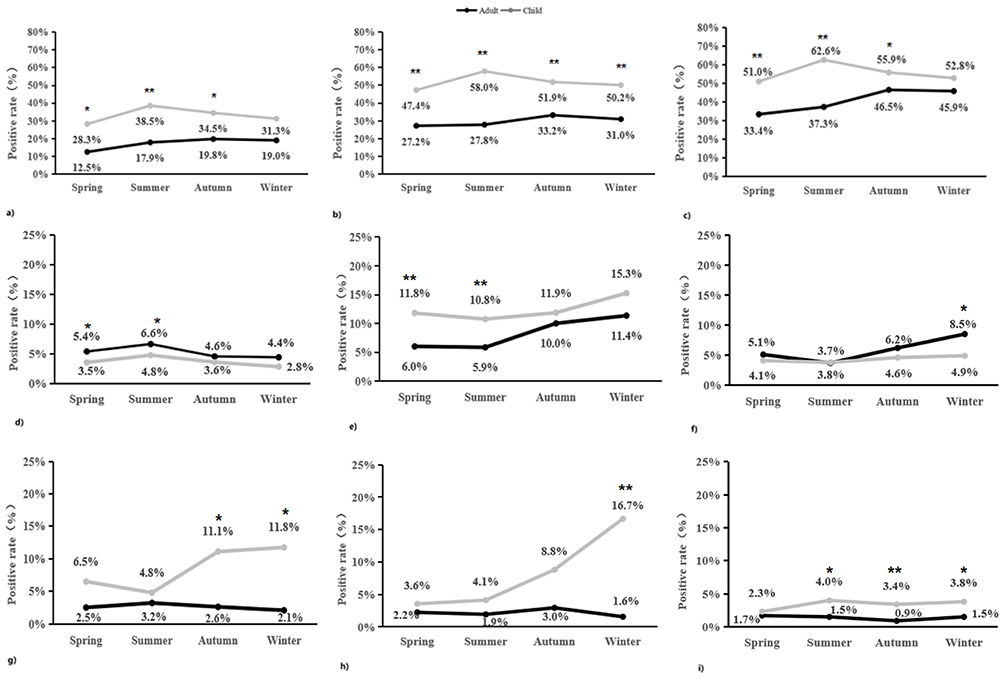 |
Figure 3 The distribution of allergen Positive rate in adults and children across different seasons. The seasonal differences in allergen positive rate between adults and children for (a) D201 tropical mites, (b) D1: D. pteronyssinus, (c) D2: D. farinae, (d) I6: German cockroach, (e) E1: cat dander, (f) E5: dog dander, (g) W7: daisy, (h) W8: dandelion, and (i) M6: Alternaria alternata, Chi square test, *P < 0.05; **P < 0.001. |
The Correlation Between Allergens and Patients’ Sensitization Patterns
Overall, 37.2% of patients were positive for at least one allergen, with 22.2% showing polysensitization, and only 7.5% testing positive for more than three allergens. Polysensitization, defined as sensitivity to multiple allergens simultaneously, is a common phenomenon in allergic diseases and may contribute to the observed differences in sensitization patterns across age groups. Additionally, children generally exhibited higher positive rates than adults (Figure 4a). The Spearman’s analysis revealed strong correlations among specific allergens. Tropical mites showed strong correlations with horse dander (rs = 0.901, P < 0.01), cow dander (rs = 0.902, P < 0.01), daisy (rs = 0.885, P < 0.01), dandelion (rs = 0.893, P < 0.01), and plantain (rs = 0.894, P < 0.01). Strong correlations were observed between horse dander and cow dander (rs = 0.996, P < 0.01), daisy (rs = 0.970, P < 0.01), dandelion (rs = 0.982, P < 0.01), and plantain (rs = 0.980, P < 0.01); between cow dander and daisy (rs = 0.970, P < 0.01), dandelion (rs = 0.982, P < 0.01), and plantain (rs = 0.982, P < 0.01); between daisy and dandelion (rs = 0.981, P < 0.01), and plantain (rs = 0.978, P < 0.01); between dandelion and plantain (rs = 0.990, P < 0.01). For food allergens, correlations were observed between brazil nut and codfish (rs = 0.896, P < 0.01), hazelnut (rs = 0.983, P < 0.01), almond (rs = 0.980, P < 0.01), beef (rs = 0.870, P < 0.01), and coconut (rs = 0.974, P < 0.01) (Figure 4b). The optimal scale analysis further indicated three main sensitization patterns for inhalant allergens: I. mite-dominated [D. pteronyssinus, D. farinae, tropical mite, German cockroach]; II. animal dander-dominated [cat dander, horse dander, cow dander, dog dander]; III. pollen-dominated [mugwort, daisy, dandelion, plantain], Cronbach’s α = 0.889) (Figure 4c). For food allergens, the pattern included: I. egg and milk-dominated [egg white, milk, soybean]; II. nut-dominated [hazelnut, Brazil nut, almond, sesame]; III. seafood-dominated [crab, shrimp], Cronbach’s α = 0.932) (Figure 4d).
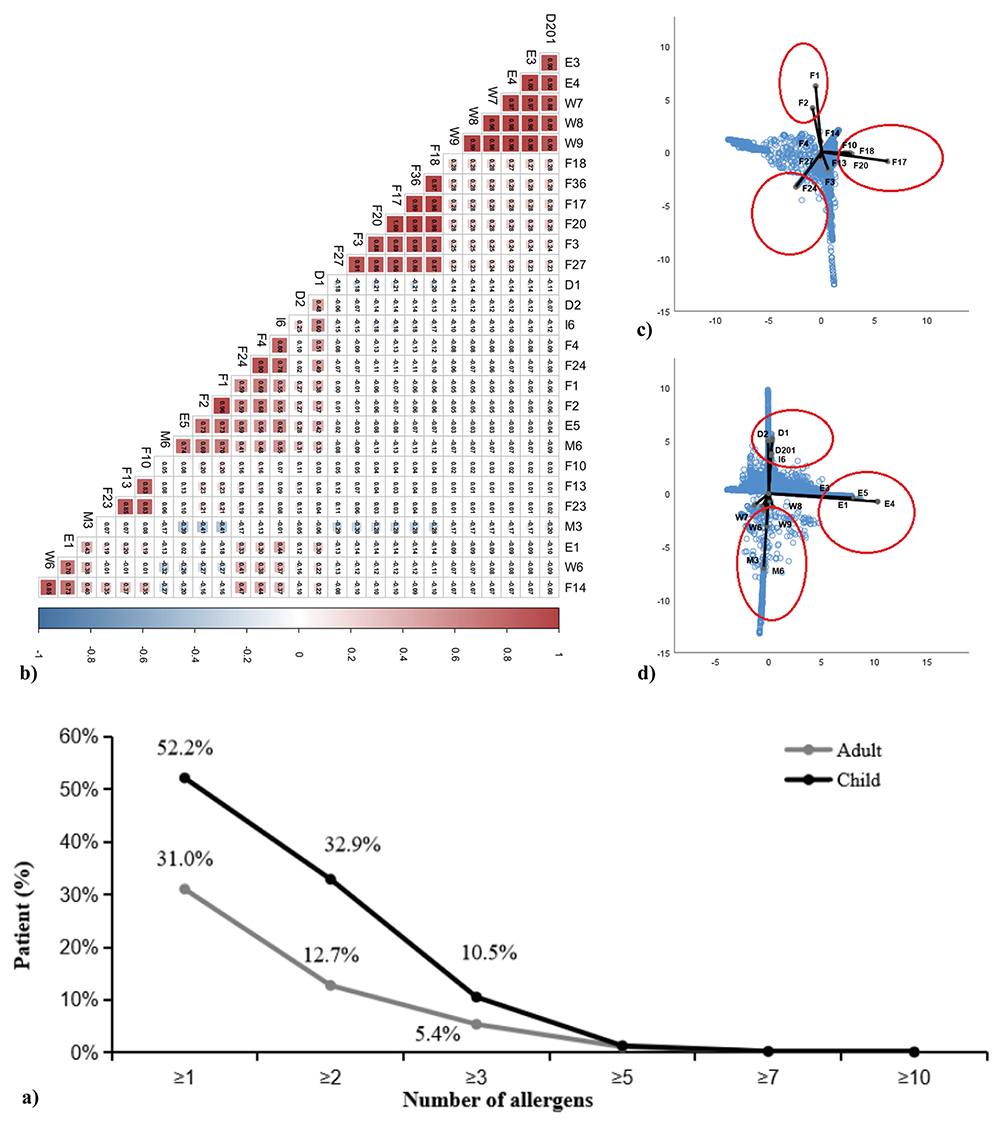 |
Figure 4 The relationship between allergens and the sensitization patterns of patients. (a) The percentage of polysensitized patients among adults and children; (b) Spearman`s test was used to analyze the correlation between allergens; (c and d) A dimensional reduction analytical method was used for optimal scale analysis. Using the serum specific immunoglobulin E concentration of allergens as the continuous variable, the closer the two points, the higher the correlation between the two factors. Allergens enclosed within the same red circle represent a shared sensitization pattern. D201: Tropical mites; E3: Horse dander; E4: Cow dander; F3: Codfish; F17: Hazelnut; F18: Brazil nut; F20: Almond; F27: Beef; F36: Coconut; W7: Daisy; W8: Dandelion; W9: Plantain; D1: D. pteronyssinus; E5: Dog dander; F1: Egg white; F2: Milk; F4: Wheat; F24: Shrimp; I6: German cockroach; M6: Alternaria alternata; E1: Cat dander; M3: Aspergillus fumigatus; W6: Mugwort; F10: Sesame; F13: Peanut; F14: Soybean; F23: Crab; D2: D. farinae. |
Discussion
For a new technology widely used in clinical practice, it is necessary to evaluate its application value based on real-world medical data and compare it to the detection situation of old technologies. This study found that dust mites have the highest positivity rates among inhaled allergens, while eggs and milk have the highest positivity rates among food allergens. A study in China showed that in inhalation allergen, the highest positivity rate was D. pteronyssinus (33.7%). Among food allergens, the highest positivity rates were egg white (10.9%) and milk (11.6%). This results, obtained using PhadiaCAP (Thermo Fisher, USA) aligned with our findings.13 A multicenter study using skin prick tests (SPT) as the detection method found that the three allergens with the highest positive rates were D. pteronyssinus, dust mites, and tropical mites, and the ranking of allergen positivity rates were coincide with our results.14 Our study utilized magnetic particle luminescence technology, which employs magnetic particles as solid-phase carriers to provide a larger surface area, significantly enhancing the binding efficiency between antigens and antibodies. Compared to SPT, this technology is non-invasive and safe, avoiding direct contact with the patient’s skin and thus eliminating the risk of severe allergic reactions, making it particularly suitable for children and high-risk populations. Compared to ELISA, magnetic particle luminescence technology offers more precise quantification of specific IgE levels, with a broader dynamic range, ensuring more accurate measurements, especially at low IgE concentrations.
Different patients showed different sensitization characteristics. Children had higher positive rate for egg white and milk, while adults had higher positive rate for dog dander and German cockroach. A study conducted in southern China, which included 39,831 patients revealed that the positivity rate for German cockroach was significantly higher in adults compared to children, while the positivity rate for dog dander was similar (3.4%) across both groups, which are consistent with our study.15 Meanwhile, a study involving 12,321 patients in southern China focused on food allergens demonstrated that egg white and milk were the most prominent allergens during childhood, while the positivity rates for shrimp and crab surpassed those of milk and egg white in individuals aged 18 years and older, which is generally consistent with our findings.16 A possible explanation for this trend is that milk and egg allergies are typically triggered by specific proteins in these foods, such as whey protein and ovalbumin. During childhood, the immune system is not fully developed, making children more sensitive to these external proteins. As the immune system matures with age, many children develop immune tolerance, reducing allergic reactions to these food proteins.
In addition, for nut allergens, patients with asthma and rhinitis were primarily sensitized to hazelnut and almond. For pollen allergens, pediatric patients with asthma were mainly sensitized to daisy, while adult patients were more commonly sensitized to mugwort. Almonds are a popular food choice for humans, however they are also one of the nuts most likely to trigger allergies. Its main sensitizing proteins are Pru du 3 (a non-specific lipid transfer protein 1, nsLTP1), Pru du 4 (a profiling protein), Pru du 5 (60S acidic ribosomal protein 2), Pru du 6 (a 11S legume protein called prunin), and Pru du 8 (an antibacterial protein with cC3C repeat sequence).17,18 Daisy is a common plant in daily life, which also plays an important role in allergic diseases. A study conducted in Guangdong involving 254 pediatric patients found that children with rhinitis had a very high sensitization rate to daisies (14.6%).19 Therefore, the ALLEOS technology incorporates these regional characteristic allergens, increasing the comprehensiveness of allergen detection.
The positive rate of allergens may vary in different seasons. In this study, dust mites consistently exhibited the highest positivity rates throughout the year. For children, the positive rates for daisy and dandelion allergens increased in autumn and winter, which were higher compared to those in adults. Guangzhou’s climate increases pollen concentrations from plants like dandelions and daisies in spring and autumn. However, the highest sensitization rates occur in autumn and winter, likely due to sustained immune hypersensitivity rather than immediate exposure. Cumulative pollen exposure in earlier seasons may prolong sensitization and exacerbate respiratory symptoms, such as allergic rhinitis and asthma. In autumn and winter, lower temperatures and reduced rainfall extend pollen suspension in the air, increasing respiratory exposure. Additionally, the higher prevalence of respiratory illnesses during these seasons may lead to more allergen testing, contributing to the rise in sensitization rates. However, there was a lack of international report about the seasonal changes in the positivity rate of Daisy and Dandelion allergens in China. IgE antibodies to cross-reactive carbohydrate determinants (CCD) can cause false positive results in allergen sIgE tests. The ALLEOS allergen detection system uses paramagnetic microparticles, which is specifically designed to eliminate solid-phase related CCD interferences in sIgE tests. This technology enhances diagnostic specificity, particularly for pollen allergens.20 Therefore, we can obtain accurate results of pollen allergen testing and supplement the insufficient of international study.
Interestingly, the optimal scale analysis shows three main sensitization patterns for inhalant allergens (I. mite-dominated; II. animal dander-dominated; III. pollen-dominated) and for food allergens (I. egg and milk-dominated; II. nut-dominated; III. seafood-dominated). In clinical practice, due to the sensitization mode being stable for a certain period of time, doctors can select different allergen testing panels based on the patient’s age, region, and lifestyle. However, including too many allergens in the testing panel can increase the patient’s economic burden, while an insufficient number of allergens may lead to incomplete testing.21 Our study results suggest that, for each sensitization patterns, it is sufficient to test one or two common allergen from the pattern for initial screening. For example, in seafood-dominated sensitization patterns, testing for shrimp alone maybe sufficient. Of course, additional potential allergens must be tested according to the patient’s main complaints. This targeted screening approach ensures comprehensive testing while effectively controlling costs and avoiding overdiagnosis. Nonetheless, the allergen screening strategies for different regions still need to be refined through further epidemiological research.22
This study analyzed allergen sensitization patterns in a large real-world cohort of suspected allergy patients from southern China. A major strength of the study lies in the inclusion of over 20,000 individuals and the assessment of 28 common inhalant and food allergens, providing a comprehensive and representative overview of allergen exposure across the region. This allowed detailed characterization of sensitization profiles across different age groups, disease types, and seasons. The findings contribute valuable epidemiological insights and may support the development of stratified allergen testing strategies in clinical settings. However, this study has certain limitations. Detailed clinical information, such as lung function and induced sputum results, was not available, and some potential allergens were not included in the current panel. Future studies incorporating broader allergen coverage and clinical parameters are warranted.
Conclusion
This real-world study revealed age-, disease-, and season-specific allergen sensitization patterns in southern China. Inhalant and food allergens formed three major sensitization clusters each. These findings support region- and population-specific testing strategies and may inform clinical decision-making.
Data Sharing Statement
The datasets are not publicly available due to confidentiality agreements, but may be requested from the corresponding author with appropriate approvals from the Ethics Committee of The First Affiliated Hospital of Guangzhou Medical University. All materials described in this study are commercially available or can be provided by Huimin Huang upon request.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Ethics Committee of The First Affiliated Hospital of Guangzhou Medical University. The initial approval (Reference number: GYFYY-2016-73) covered the secondary analysis of de-identified data from the Guangzhou Medical Database for multiple research purposes during the period of 2016 to 2021. An extension of this approval was granted under a new reference number (GYFYY-2022-85), allowing continued use of the database for related studies from 2022 onward. The current analysis of allergy-related data collected between 2021 and 2024 falls within the scope of these approvals. No additional ethical review was required.
The informed consent of patients was obtained by Biobank for Respiratory Diseases in the National Clinical Research Center for Respiratory Disease (BRD-NCRCRD, Guangzhou, Southern China), which informed each patient that their clinical examination data would be used for possible future studies. For participants aged <18 years, written informed consent was obtained from parents/legal guardians in accordance with national regulations and institutional guidelines.
This study adheres to the principles of the Declaration of Helsinki (2013 revision), including:
Independent ethical review and approval by accredited institutional boards
Voluntary participation with right to withdraw at any time
Strict confidentiality protocols for personal data
Age-appropriate consent procedures aligned with national legislation
Acknowledgments
We thank everyone involved in the collection, storage, transportation, and management of the serum samples from BRD-NCRCRD.
Author Contributions
Conceived and designed the experiments: BQS. Performed the experiments: HMH. Analyzed the data: YFC. Wrote the paper: HSH, YFC, HMH. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Guangdong Zhongnan Mountain Medical Foundation (ZNSXS-20220015). The funders had no role in study design, data analysis, preparation of the manuscript, or decision to publish.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Hou X, Huang H, Hu H, Wang D, Sun B, Zhang XD. Short-term exposure to ambient air pollution and hospital visits for IgE-mediated allergy: a time-stratified case-crossover study in southern China from 2012 to 2019. EClinicalMedicine. 2021;37:100949. doi:10.1016/j.eclinm.2021.100949
2. Li Y, Hu H, Zhang T, et al. Increase in indoor inhalant allergen sensitivity during the COVID-19 pandemic in South China: a cross-sectional study from 2017 to 2020. J Asthma Allergy. 2021;14:1185–1195. doi:10.2147/JAA.S322034
3. Wu G, Hu H, Zhang T, Zhang XD, Sun B. Profiles of sensitization and comorbidity in asthma patients with markedly increased serum total IgE (>1000kU/L). Allergy Asthma Proc. 2022;43(2):124–132. doi:10.2500/aap.2022.43.210123
4. Hu H, Huang Z, Luo W, et al. Allergen diagnosis strategy: an experimental application of different methods in Guangzhou, Southern China. Sci Prog. 2021;104(1):36850421997277. doi:10.1177/0036850421997277
5. Weidner J, Hu H, Hou X, Sun B. Editorial: the application of new technology in the diagnosis of allergic diseases. Front Allergy. 2024;5:1484624. doi:10.3389/falgy.2024.1484624
6. Stróżek J, Samoliński BK, Kłak A, et al. The indirect costs of allergic diseases. Int J Occup Med Environ Health. 2019;32(3):281–290. doi:10.13075/ijomeh.1896.01275
7. Huang J, Xiang R, Tan L, et al. Dust mite component analysis: identifying key allergens components for effective immunotherapy in allergic rhinitis. Int Immunopharmacol. 2023;125(Pt A):111111. doi:10.1016/j.intimp.2023.111111
8. Chen W, Jie WU, Chen ZO, Jie XU, Huang-Xian JU. Chemiluminescent immunoassay and its applications. Chin J Anal Chem. 2012;40(1):3–10. doi:10.1016/S1872-2040(11)60518-5
9. Iranifam M. Analytical applications of chemiluminescence-detection systems assisted by magnetic microparticles and nanoparticles. TRAC-Trends Anal Chem. 2013;51:51–70. doi:10.1016/j.trac.2013.05.014
10. Boulet LP, Reddel HK, Bateman E, Pedersen S, FitzGerald JM, O’Byrne PM. The global initiative for asthma (GINA): 25 years later. Eur Respir J. 2019;54(2):1900598. doi:10.1183/13993003.00598-2019
11. Brożek JL, Bousquet J, Agache I, et al. Allergic rhinitis and its impact on asthma (ARIA) guidelines-2016 revision. J Allergy Clin Immunol. 2017;140(4):950–958. doi:10.1016/j.jaci.2017.03.050
12. Kulthanan K, Tuchinda P, Nitiyarom R, et al. Clinical practice guidelines for the diagnosis and management of atopic dermatitis. Asian Pac J Allergy Immunol. 2021;39(3):145–155. doi:10.12932/AP-010221-1050
13. Luo W, Wang D, Zhang T, et al. Prevalence patterns of allergen sensitization by region, gender, age, and season among patients with allergic symptoms in mainland China: a four-year multicenter study. Allergy. 2021;76(2):589–593. doi:10.1111/all.14597
14. Li J, Sun B, Huang Y, et al. A multicentre study assessing the prevalence of sensitizations in patients with asthma and/or rhinitis in China. Allergy. 2009;64(7):1083–1092. doi:10.1111/j.1398-9995.2009.01967.x
15. Luo W, Hu H, Tang W, et al. Allergen sensitization pattern of allergic adults and children in southern China: a survey based on real life data. Allergy Asthma Clin Immunol. 2019;15:42. doi:10.1186/s13223-019-0357-y
16. Liu M, Liu L, Qi W, et al. Interpreting epidemiologic distribution of total and specific IgE levels for food allergy in Southern China from 2004 to 2023: understanding the mechanisms and focusing on prevention. BMC Public Health. 2024;24(1):3022. doi:10.1186/s12889-024-20470-4
17. Costa J, Mafra I, Carrapatoso I, Oliveira MBPP. Almond allergens: molecular characterization, detection, and clinical relevance. J Agric Food Chem. 2012;60(6):1337–1349. doi:10.1021/jf2044923
18. Zhang Y, Jin T. Almond allergens: update and perspective on identification and characterization. J Sci Food Agric. 2020;100(13):4657–4663. doi:10.1002/jsfa.10417
19. Liao CX, Huang DM, Hu HS, et al. Analysis of serum allergen-specific IgE in children with respiratory allergic disease in Guangdong. Zhonghua Yu Fang Yi Xue Za Zhi. 2021;55(5):613–619. doi:10.3760/cma.j.cn112150-20201217-01467
20. Zhu ZC, Peng Y, Chen Z, Qiu QH. Analysis and dynamic observation of inhaled and food allergens for people in Pearl River Delta. Lin Chuang Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2017;31(5):343. doi:10.13201/j.issn.1001-1781.2017.05.004
21. Hu H, Huang H, Liao C, et al. A study of allergen detection panel in Guangzhou, southern China based on real-world data from the past 7 years. Sci Rep. 2023;13(1):14855. doi:10.1038/s41598-023-41949-x
22. Chen H, Li J, Cheng L, et al. China consensus document on allergy diagnostics. Allergy Asthma Immunol Res. 2021;13(2):177–205. doi:10.4168/aair.2021.13.2.177
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.